Colorectal carcinoma anatomy to management
99
COLORECTAL CARCINOMA- ANATOMY TO MANAGEMENT By Dr. Ayush Garg
-
Upload
drayush-garg -
Category
Healthcare
-
view
112 -
download
1
Transcript of Colorectal carcinoma anatomy to management
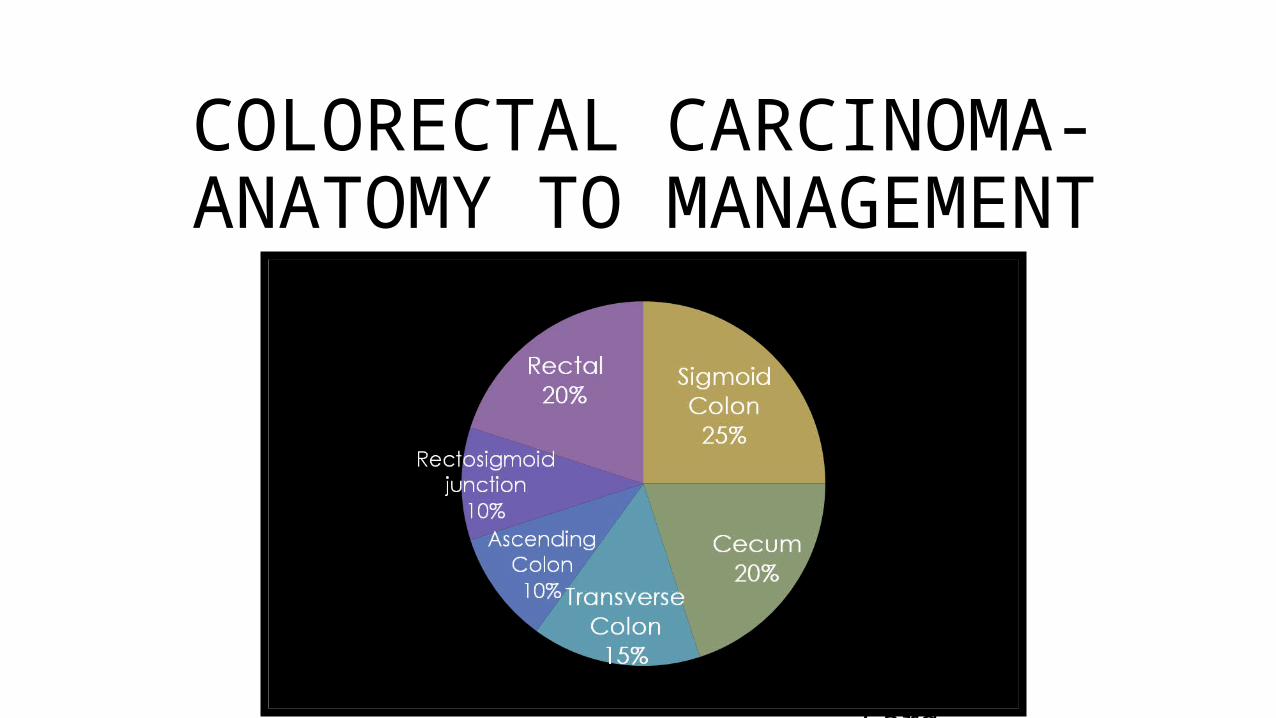
COLORECTAL CARCINOMA- ANATOMY TO MANAGEMENT
ByDr. Ayush Garg

1. Anatomy2. Epidemiology3. Risk Factors4. Clinical Features5. Screening6. Pathology7. Pathway of Spread8. Staging9. Diagnostic Work Up10.Treatment

ANATOMY• Embryology
• Starts the fourth week of gestation
• Derived from the endoderm
• Three segments: foregut, midgut, and hindgut
• Midgut and Hindgut contribute to the colon, rectum, and anus
• Hindgut - distal transverse colon, descending colon, rectum, and proximal anus all blood supply from IMA
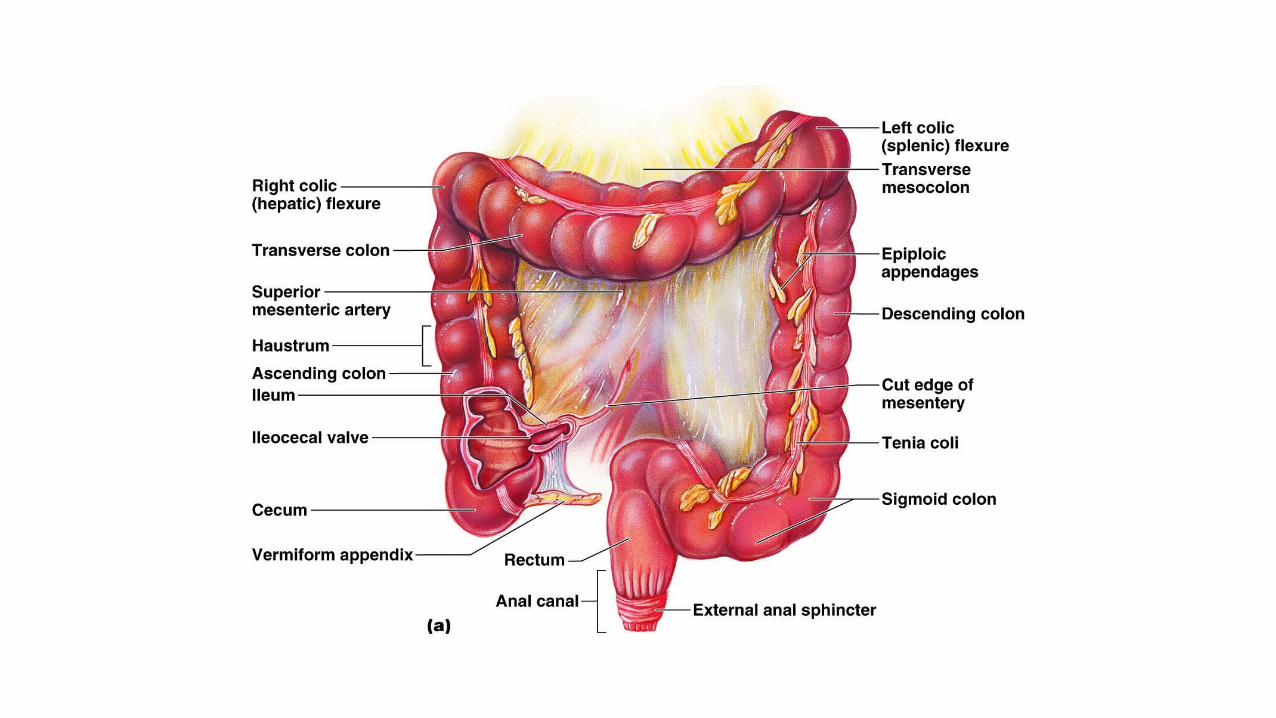

Colon/Rectum and Peritoneum
• Colon/Rectum covered by serosa• Cecum• Transverse• Sigmoid• Anterior descending• Anterior ascending• Rectosigmoid• Upper third and anterior wall of middle third of rectum
• Colon/Rectum without serosa• Posterior ascending• Posterior descending• Lower third of rectum (rectal ampulla)

Arterial Supply• SMA -
• Ileocolic artery (absent in up to 20% of people),
terminal ileum and proximal ascending colon
• Right colic artery - ascending colon
• Middle colic artery - transverse colon • IMA -
• Left colic artery - descending colon
• Sigmoidal branches - sigmoid colon
• Superior rectal artery - proximal rectum
• Communicate via the marginal artery of Drummond,
complete in only 15 to 20% of people
Veins• Veins of the colon parallel their corresponding arteries (except IMV) and
bear the same terminology • Inferior mesenteric vein ascends in the retroperitoneal plane over the
psoas muscle, posterior to the pancreas to join the splenic vein.
Nerve Supply• Sympathetic (inhibitory) and parasympathetic (stimulatory) nerves, which
parallel the course of the arteries. • Sympathetic nerves arise from T6–T12 and L1–L3. • Vagus nerve ->parasympathetic innervation to the right and transverse
colon; • Parasympathetic nerves to the left colon arise from sacral nerves S2–S4 to
form the nervi erigentes.
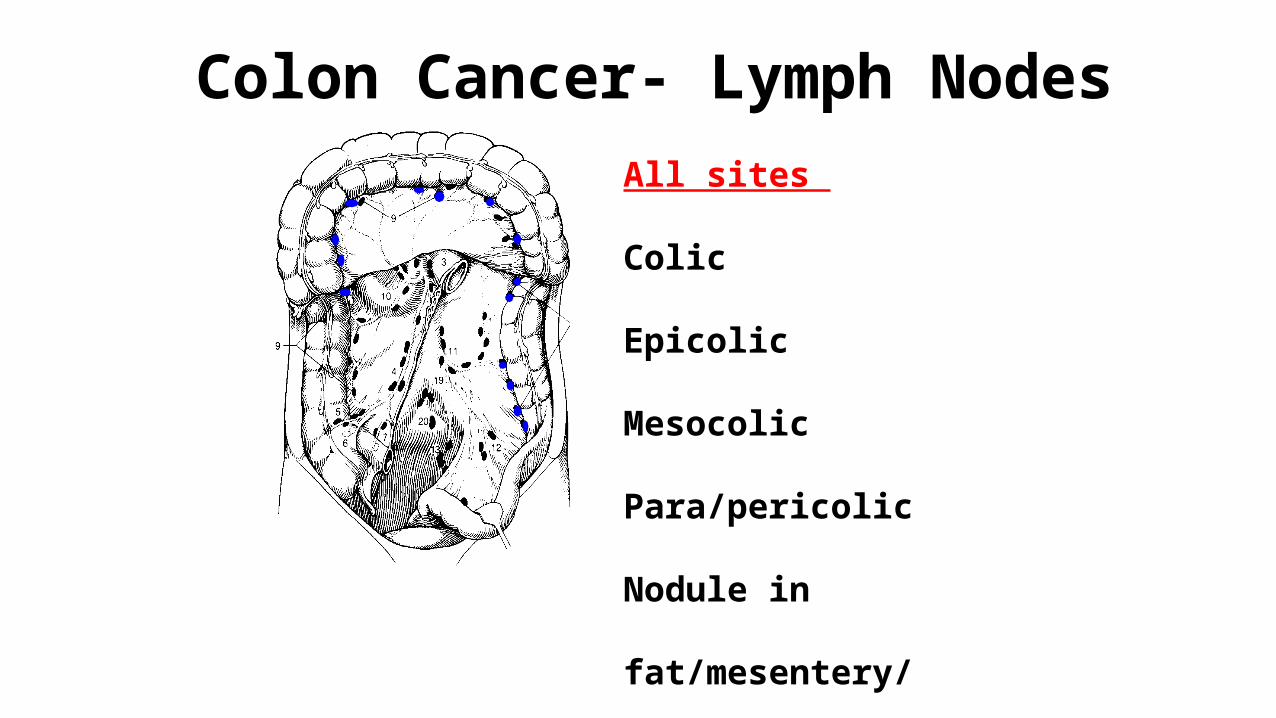
Colon Cancer- Lymph NodesAll sites
Colic
Epicolic
Mesocolic
Para/pericolic
Nodule in fat/mesentery/
mesocolic fat
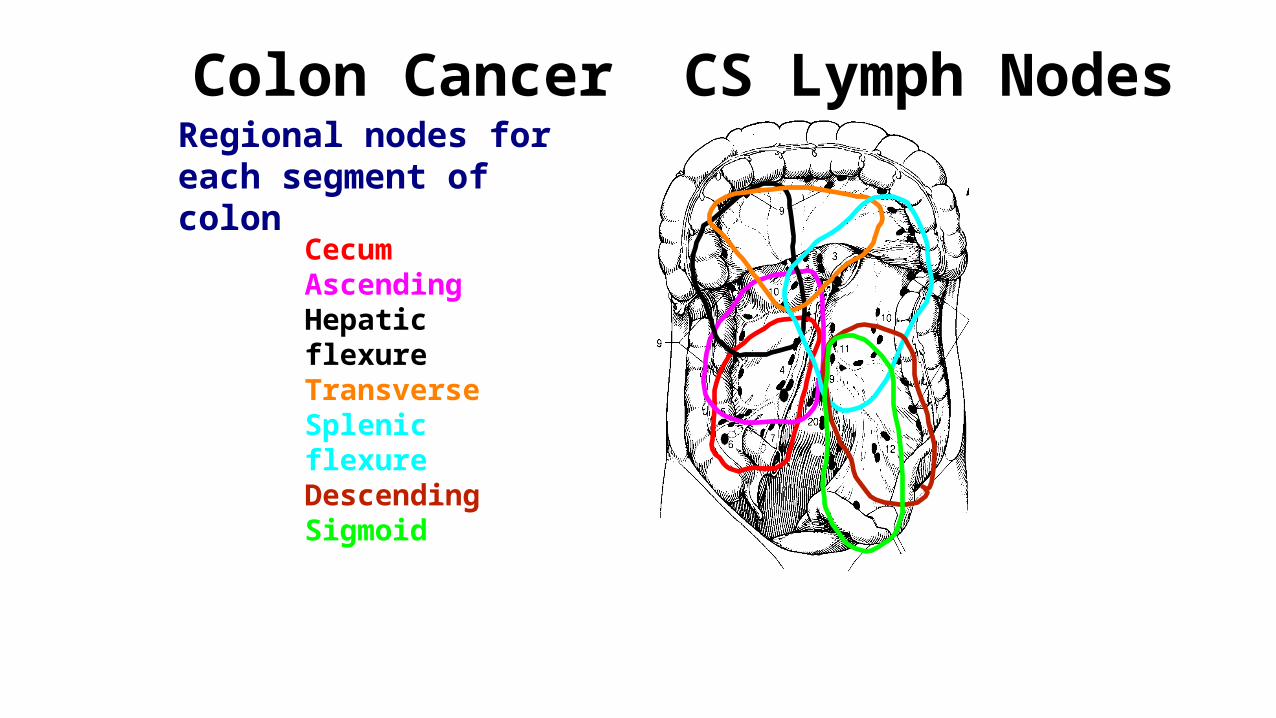
Regional nodes for each segment of colon
Colon Cancer CS Lymph Nodes
CecumAscendingHepatic flexureTransverseSplenic flexureDescendingSigmoid
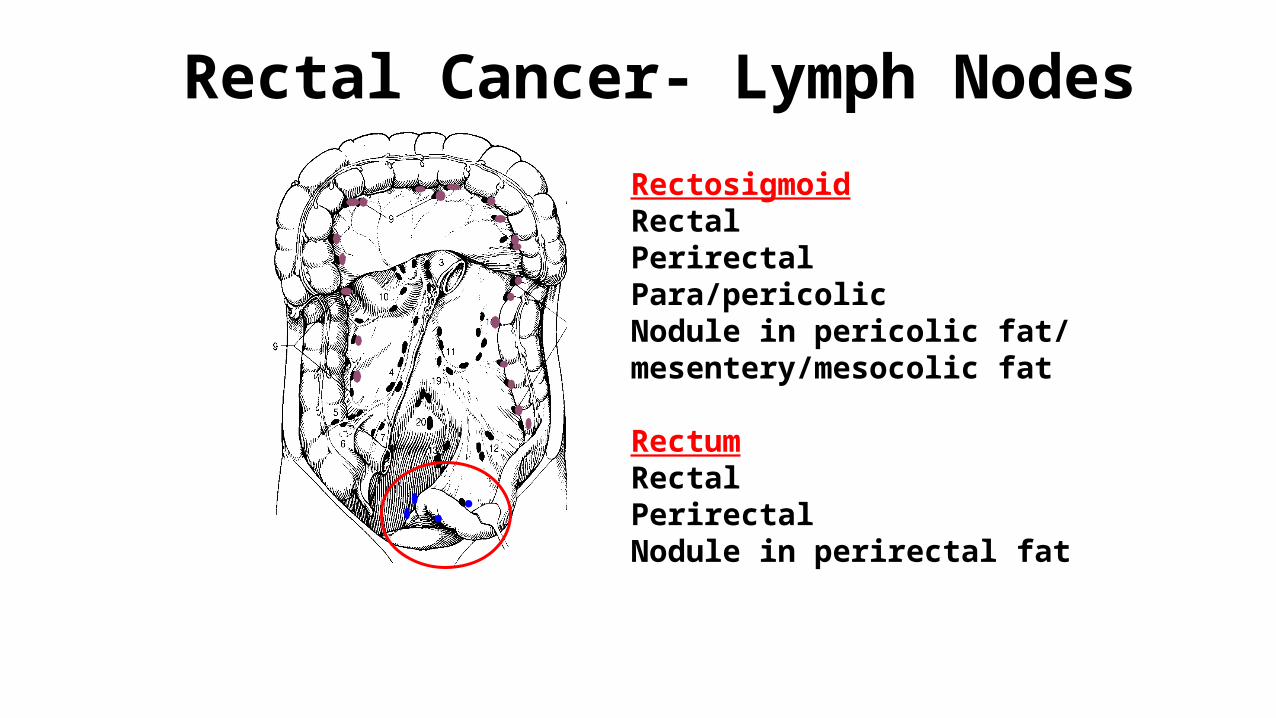
Rectal Cancer- Lymph NodesRectosigmoidRectalPerirectalPara/pericolicNodule in pericolic fat/ mesentery/mesocolic fat
RectumRectalPerirectalNodule in perirectal fat
Rectum• Rectum -12 to 15 cm in length
• Valves of Houston - three distinct submucosal folds
• Posteriorly -presacral fascia,
• Anteriorly - Denonvilliers' fascia
• Lateral ligaments support the lower rectum
• The rectum is classically divided into three parts: the upper third, the middle third, and the lower third. Each part is practically assumed to be 5 cm in length.
Rectum Arterial Supply• Superior rectal artery <- inferior mesenteric artery (upper rectum) • Middle rectal artery <- internal iliac• Inferior rectal artery <- internal pudendal <- internal iliac artery. • Rich collaterals
Veins and LymphaticsVenous• Superior rectal vein -> inferior mesenteric -> portal system • Middle rectal vein -> internal iliac vein • Inferior rectal vein -> internal pudendal vein -> internal iliac vein• Submucosal plexus deep to the columns of Morgagni forms the hemorrhoidal
plexus and drains into all three veins.
Rectum Lymphatic Drainage• Parallels the vascular supply• Upper and middle rectum -> inferior mesenteric nodes • Lower rectum -> inferior mesenteric and internal iliac nodes Anal canal • Proximal to the dentate line -> inferior mesenteric and internal iliac nodes • Distal -> inguinal nodes, inferior mesenteric and internal iliac nodes

Rectum Nerve Supply• Sympathetic - L1–L3 -> preaortic plexus -> hypogastric plexus combine with ->• Parasympathetic (nervi erigentes) S2–S4 to form the pelvic plexus. • Sympathetic and parasympathetic fibers then supply the anorectum and adjacent
urogenital organs.

EPIDEMIOLOGY
MALE FEMALE

BOTH
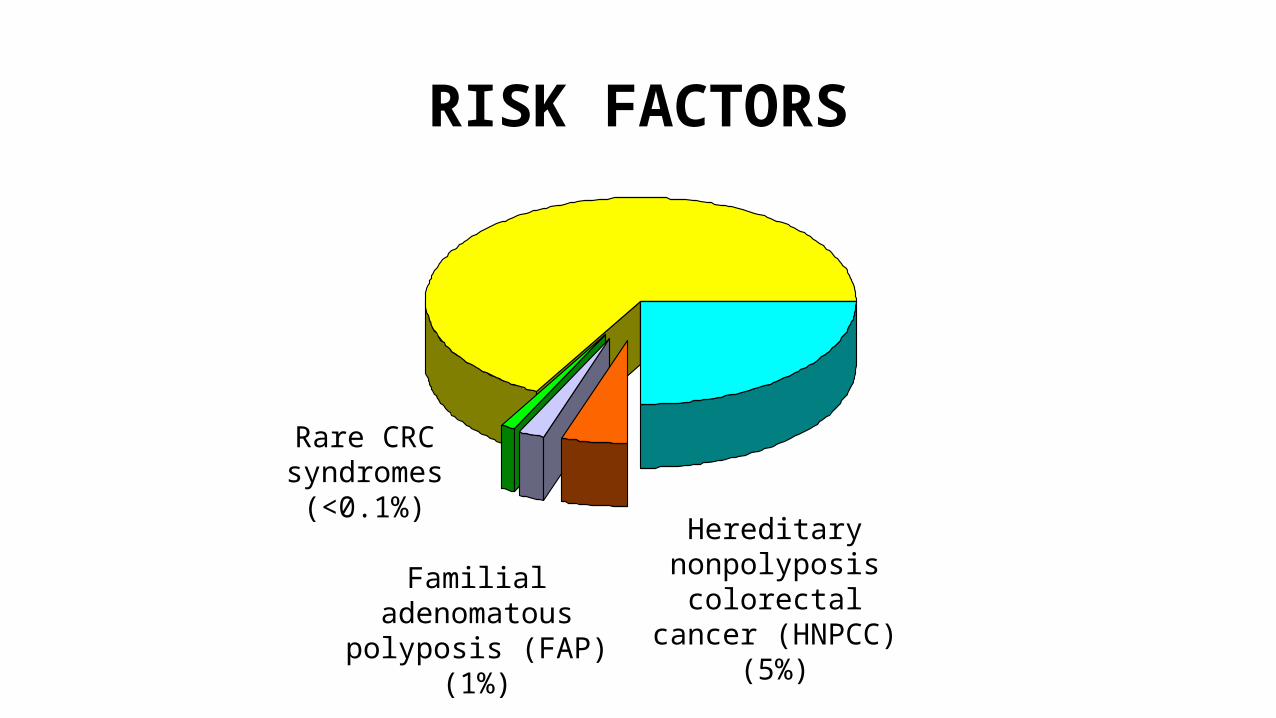
RISK FACTORS
Sporadic (65%–85%)
Familial (10%–30%)
Hereditary nonpolyposis colorectal
cancer (HNPCC) (5%)Familial adenomatous polyposis (FAP) (1%)
Rare CRC syndromes
(<0.1%)

Familial Risk
Approximatelifetime CRC risk
(%)
Affected family members
0
20
40
60
80
100
None One 1° One 1° and two
2°
One 1° age <45
Two 1° HNPCC mutation
2% 6% 8% 10%17%
70%
Aarnio M et al. Int J Cancer 64:430, 1995 Houlston RS et al. Br Med J 301:366, 1990 St John DJ et al. Ann Intern Med 118:785, 1993
20
100
80
60
40
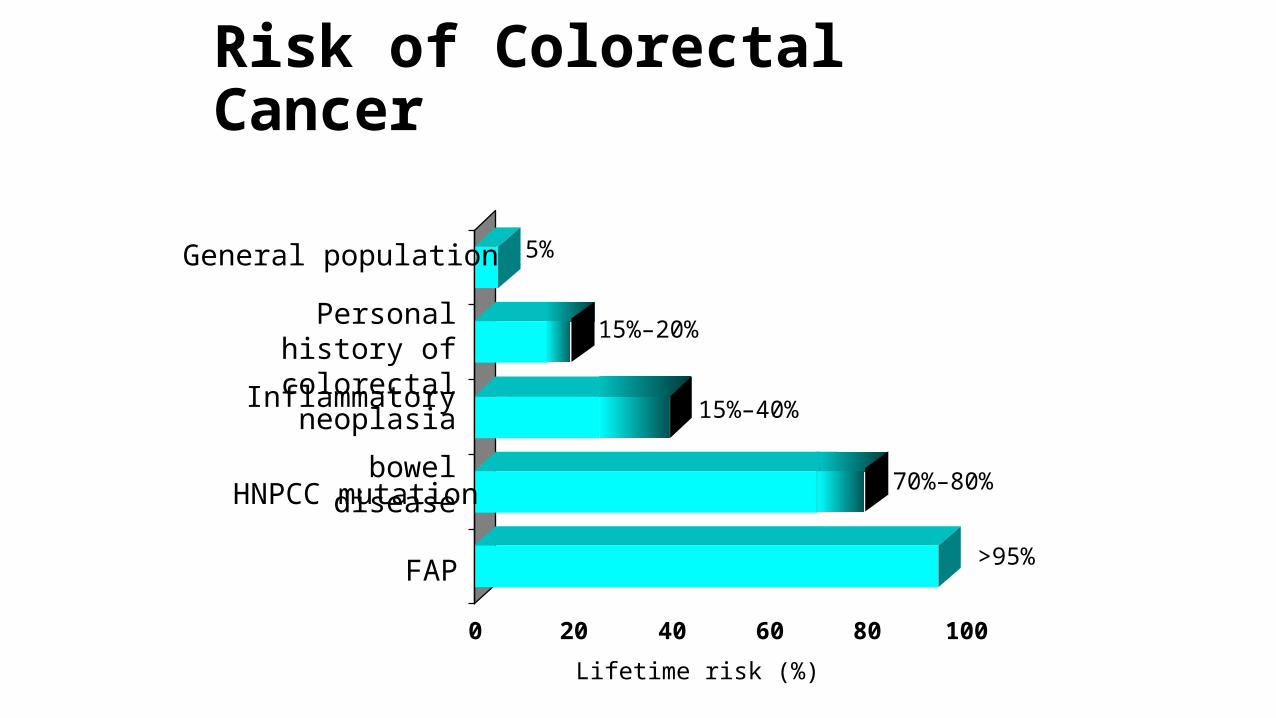
Risk of Colorectal Cancer
0 20 40 60 80 100
General population
Personal history of colorectal neoplasia
Inflammatory bowel disease
HNPCC mutation
FAP
5%
15%–20%
15%–40%
70%–80%
>95%
Lifetime risk (%)
GeneticsAPC gene • Present in 80% of sporadic cases • Tumor-suppressor gene• Ad
K-RAS• Proto-oncogene • Only one allele • G protein involved in intracellular gtp signal transduction.

MYH gene • Base excision repair gene• AR
DCC• Tumor-suppressor • Present in more than 70% of colorectal carcinomas
P53• Tumor-suppressor gene • Crucial for initiating apoptosis• 75% of colorectal cancers
• Race and Ethnicity• Higher rates and mortalities among blacks than whites
• Socioeconomic status• Possible association between low SES and colorectal cancer mortality
• Alcohol• Somewhat controversial, but appears that high alcohol intake increases risk
• Tobacco• Most studies indicate excess risk in smokers
Other Factors

• Fruit, Vegetables, and Fiber
• Association between higher intake of vegetables and lower cancer risk
• Folate
• Higher intake of folate associated with lower colon cancer risk
• Calcium
• Avoidance of low intakes of calcium may minimize risk of colon cancer
• Fat, Carbohydrates, and Proteins
• Excess energy intake leading to obesity increases the risk of colon cancer
• Possible association of red meat with increased risk

• Higher BMI is associated with an increased risk of colon cancer
• Approximately twofold higher risk in individuals who are overweight or obese
• Individuals who are more physically active have a decreased risk of colon cancer
Lifestyle Factors- BMI & Physical Activity
Adenomatous polyps • Seen in 25% of the population older than 50 years• The risk of carcinoma in a polyp larger than 2 cm is 35 to 50%.
Familial juvenile polyposis • Autosomal dominant • May degenerate into adenomas and, eventually, carcinoma.
Familial Adenomatous Polyposis • Autosomal dominant • Mutation in the APC gene, located on chromosome 5q. • Lifetime risk approaches 100% by age 50 years.• FAP may be associated with congenital hypertrophy of the retinal pigmented epithelium,
desmoid tumors, epidermoid cysts, mandibular osteomas (Gardner's syndrome), and central nervous system tumors (Turcot's syndrome).
PRE INVASIVE LESIONS
Attenuated FAP• AFAP is a recently recognized variant of FAP associated with mutations at
the 3' or 5' end of the APC gene. • Carcinoma develops in more than 50% of these patients
Hereditary Nonpolyposis Colon Cancer (Lynch Syndrome)• Extremely rare (1 to 3%). • Autosomal dominant • Average age: 40 to 45 years• 70% of affected individuals will develop colorectal cancer. • Risk of synchronous or metachronous colorectal carcinoma is 40%. • Associated with extracolonic malignancies, including endometrial, which is
most common, ovarian, pancreas, stomach, small bowel, biliary, and urinary tract carcinomas.
• Diagnosis of HNPCC is made based upon family history.

CLINICAL FEATURES

SCREENING• Neoplastic polyps, including tubular adenomas, villous adenomas, and
tubulovillous adenomas, are precursors of colon cancers.• Most CRC arise from pre-existing polyps. • The cumulative lifetime risk of developing CRC in the United States is
about 6%.• The goal of screening is to detect preinvasive polyps or early invasive
cancer.
• The American Cancer Society (ACS) and the United States Preventative Services Task Force recommend screening in average-risk individuals starting at age 50.
• The ACS advocates for tests that detect adenomatous polyps and cancer as follows:
• 1. Flexible sigmoidoscopy every 5 years.• 2. Double contrast barium enema every 5 years.• 3. Computed tomography (CT) colonography every 5 years.• 4. Colonoscopy every 10 years.• 5. Guaiac-based fecal occult blood, fecal immunohistochemical, and stool DNA
tests may be performed for CRC, but not polyp, detection.

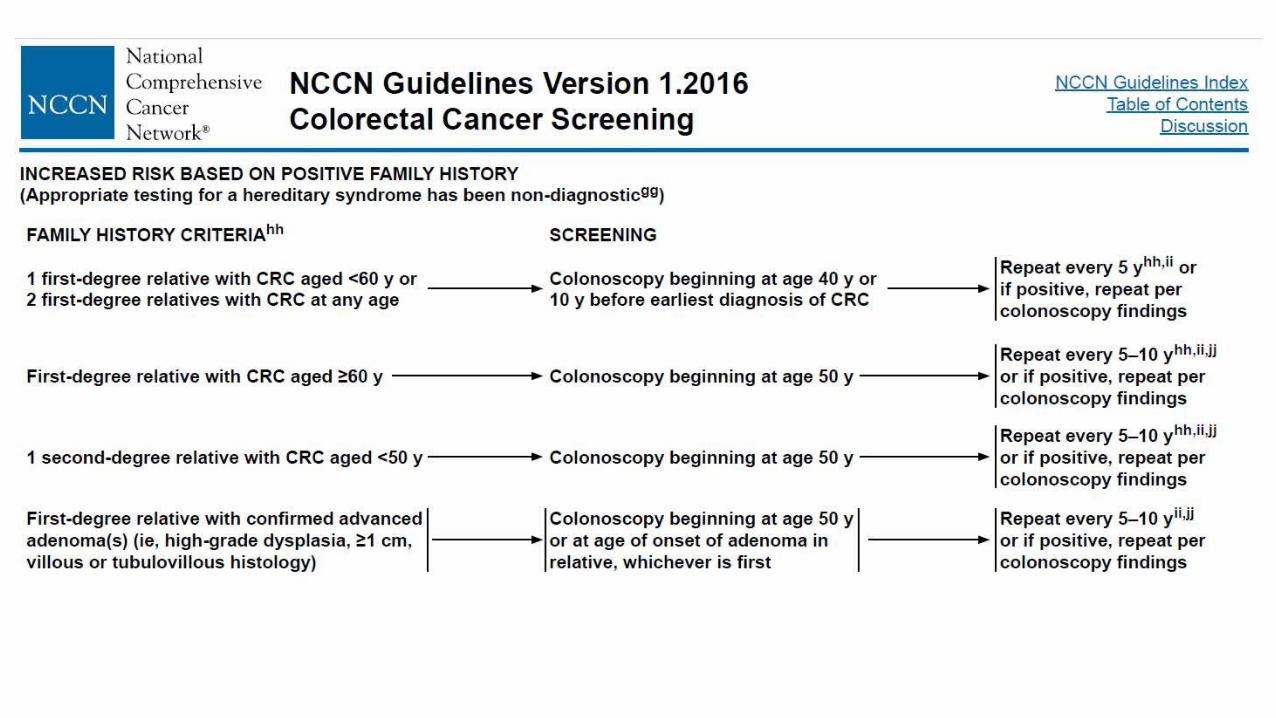
• In high-risk patients (patients with adenomatous polyps, history of CRC, first-degree relative diagnosed with CRC or adenomas, inflammatory bowel disease, or high risk due to family history or genetic testing), more-intensive surveillance is recommended.
• Individuals with FAP initiate annual sigmoidoscopy or colonoscopy beginning at age 10 to 12 years until age 35 to 40 years if negative.
• Patients with HNPCC initiate annual screening at age 20 to 25 years or 10 years prior to earliest familial CRC diagnosis.
• Patients with inflammatory bowel disease should initiate screening with colonoscopy 8 to 10 years after initial diagnosis.
PATHWAY OF SPREAD
• Local• Multidirectional growth progression• Intramural- bowel wall penetration• Invasion into adjacent organs/ structures• Perineural invasion ~10 cm from primary lesion
• Lymphomatous• Tumor grade• LVI
• Normal lymphatic flow along major arteries to three echelons of LN• Pericolic/ Intermediate /Principal LN
• Hematogenous• Liver- primary site – 40%• Lung- 2nd most common site• 10-15% have episode of distant metastasis at diagnosis
• Peritoneal seeding/ implantation• Intraluminal/ serosal sheding/ by surgical manipulation

PATHOLOGY• I. Epithelial
• Benign• Malignant
• Adeno ca >95%• Mucinous adenoca 17%• Signet ring cell ca 2-4%• SCC• Adenosquamous• Undiff/ Unclassified
II. Neuroendocrinal – carcinoidIII. Nonepithelial
Leiomyoma/ lipoma/hemangiomaLeiomyosarcomaIV. Hematopoietic/ lymphoid(DLBCL)V. UnclassifiedVI. SecondariesVII. Tumor like lesionsVIII. Epithelial atypia in Ulcerative colitis
Microscopic Anatomy of Large Intestine• Villi are absent • Contains numerous goblet cells• Intestinal crypts – simple tubular glands• Lined with simple columnar epithelial tissue
• Epithelium changes at anal canal• Becomes stratified squamous epithelium
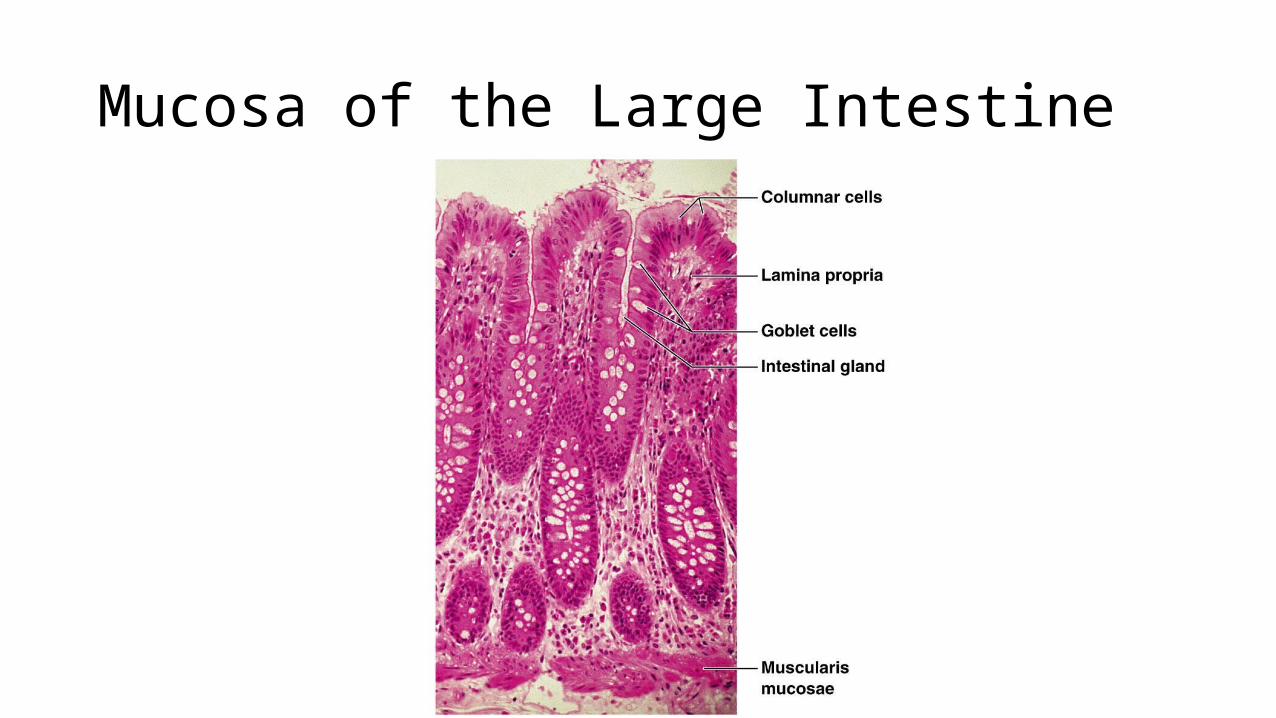
Mucosa of the Large Intestine
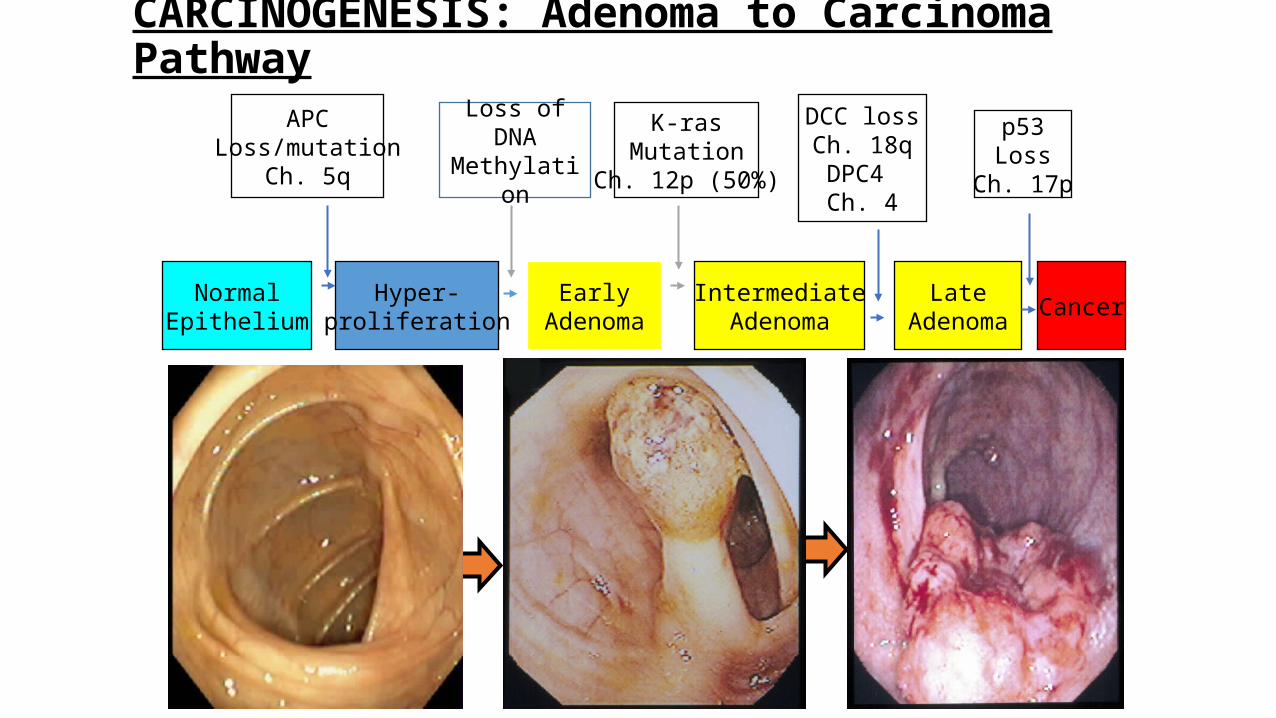
CARCINOGENESIS: Adenoma to Carcinoma Pathway
APCLoss/mutation
Ch. 5q
NormalEpithelium
EarlyAdenoma CancerHyper-
proliferationIntermediate
AdenomaLate
Adenoma
K-rasMutation
Ch. 12p (50%)
DCC lossCh. 18qDPC4 Ch. 4
p53Loss
Ch. 17p
Loss of DNA Methylation
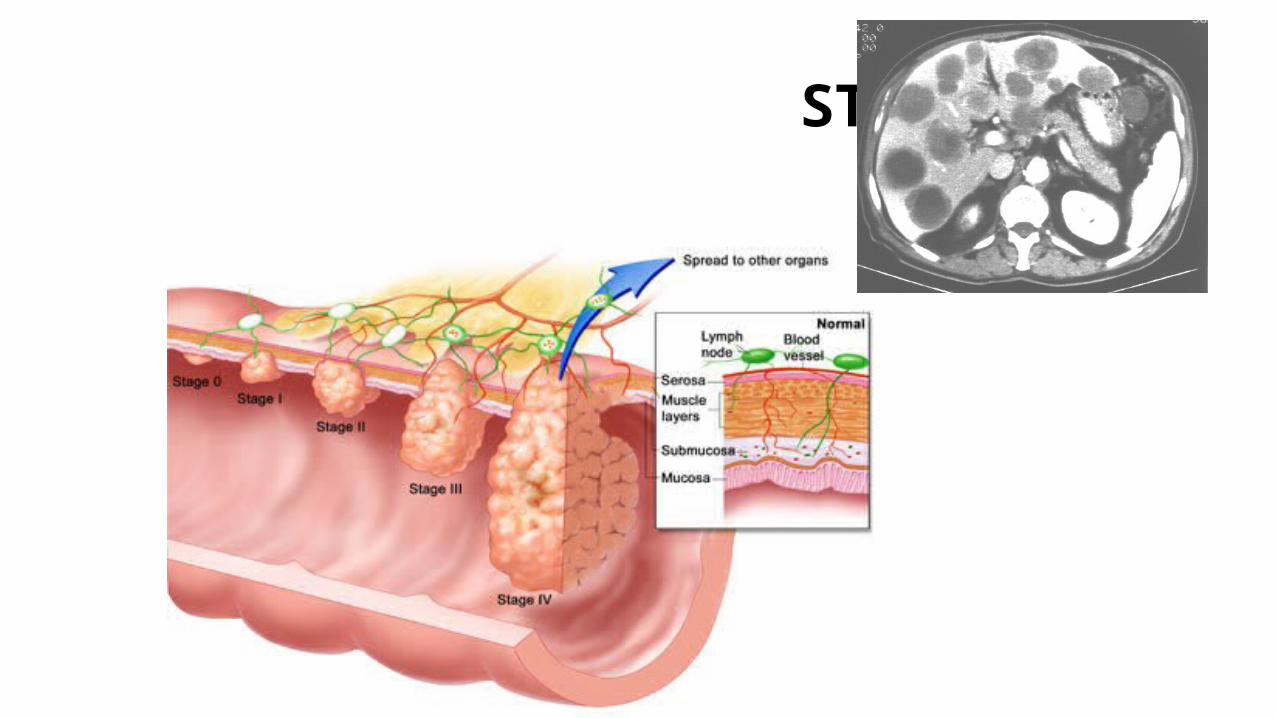
STAGING

Stage 0 Colorectal Cancer• Known as “cancer in situ,” meaning
the cancer is located in the mucosa (moist tissue lining the colon or rectum)
• Removal of the polyp (polypectomy) is the usual treatment
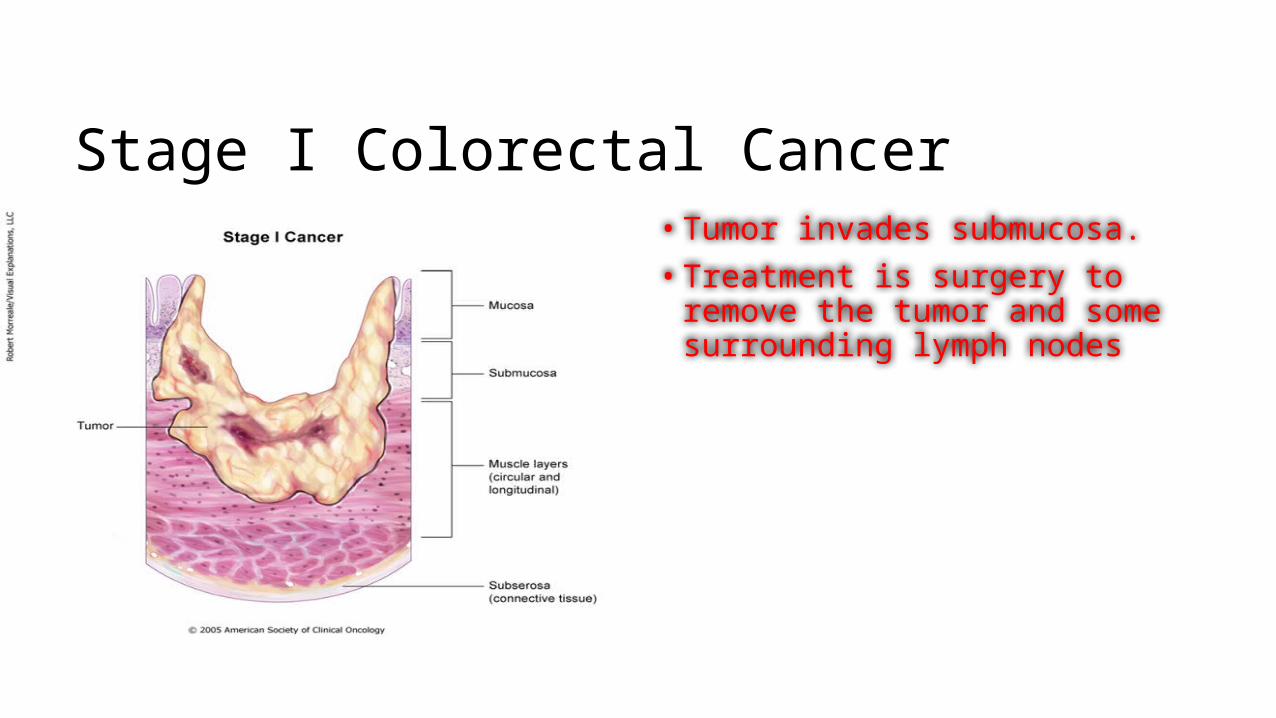
Stage I Colorectal Cancer• Tumor invades submucosa. • Treatment is surgery to remove the
tumor and some surrounding lymph nodes
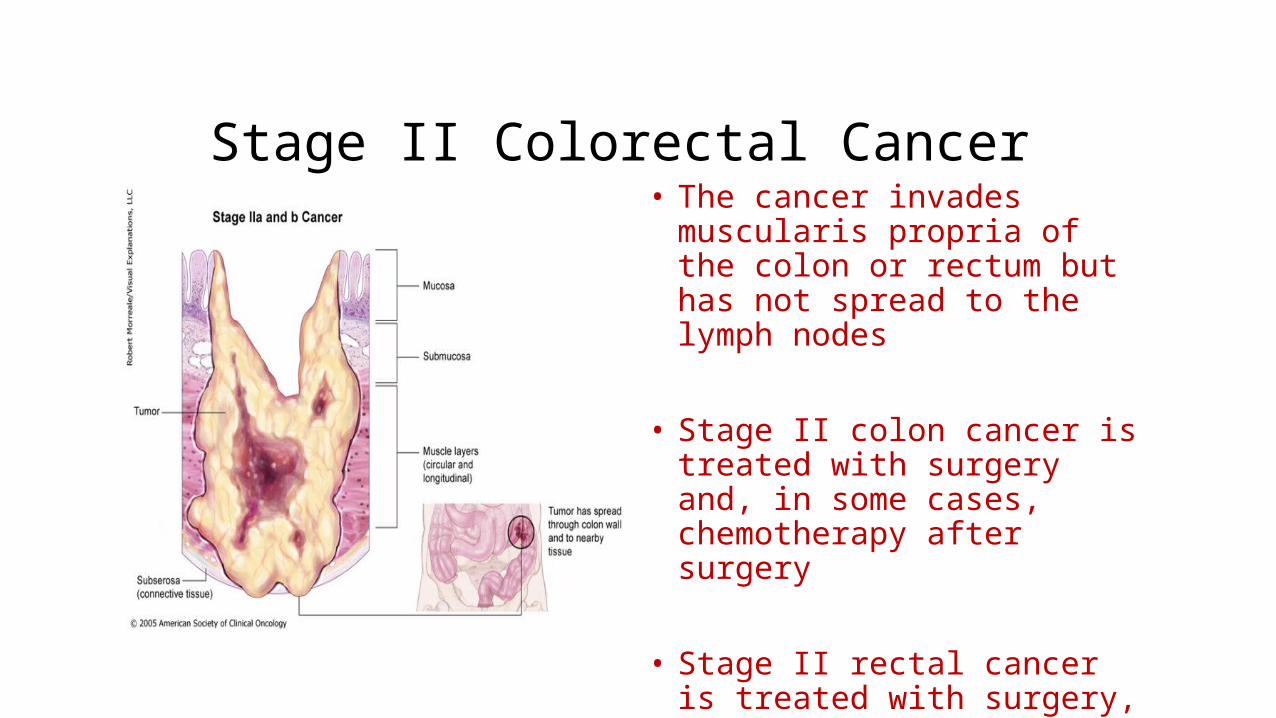
Stage II Colorectal Cancer• The cancer invades muscularis
propria of the colon or rectum but has not spread to the lymph nodes
• Stage II colon cancer is treated with surgery and, in some cases, chemotherapy after surgery
• Stage II rectal cancer is treated with surgery, radiation therapy, and chemotherapy
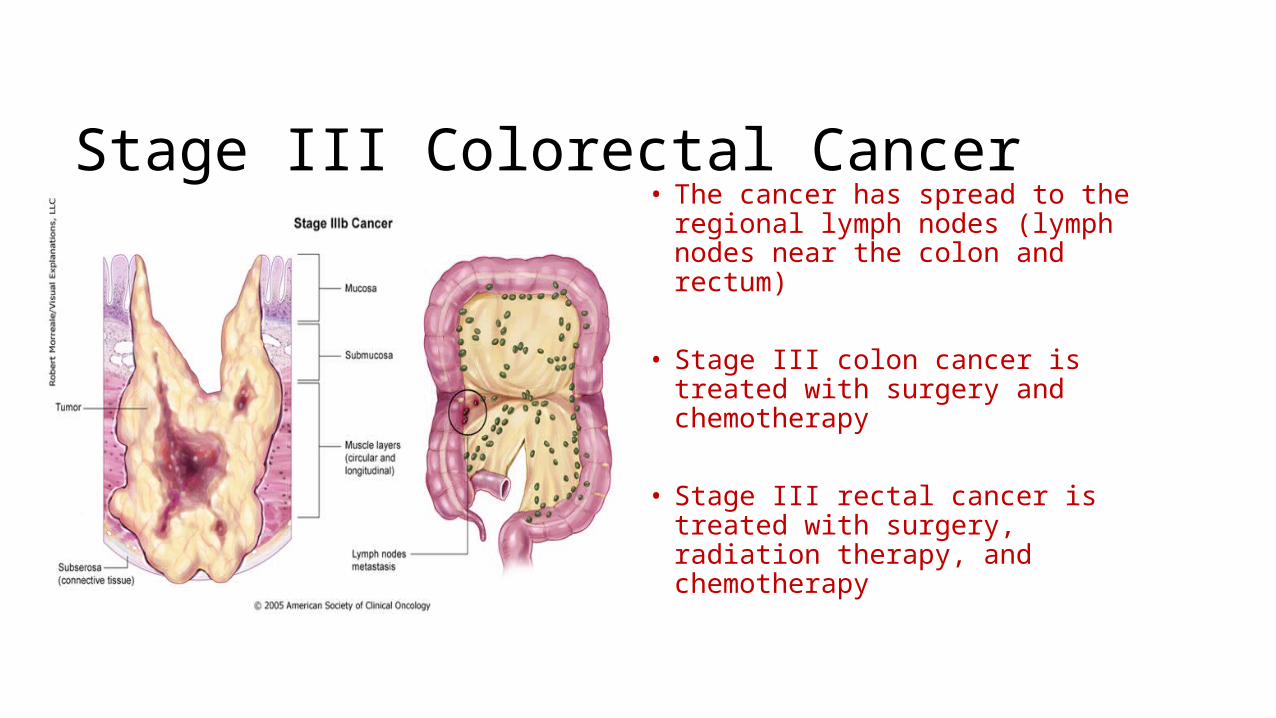
Stage III Colorectal Cancer• The cancer has spread to the
regional lymph nodes (lymph nodes near the colon and rectum)
• Stage III colon cancer is treated with surgery and chemotherapy
• Stage III rectal cancer is treated with surgery, radiation therapy, and chemotherapy
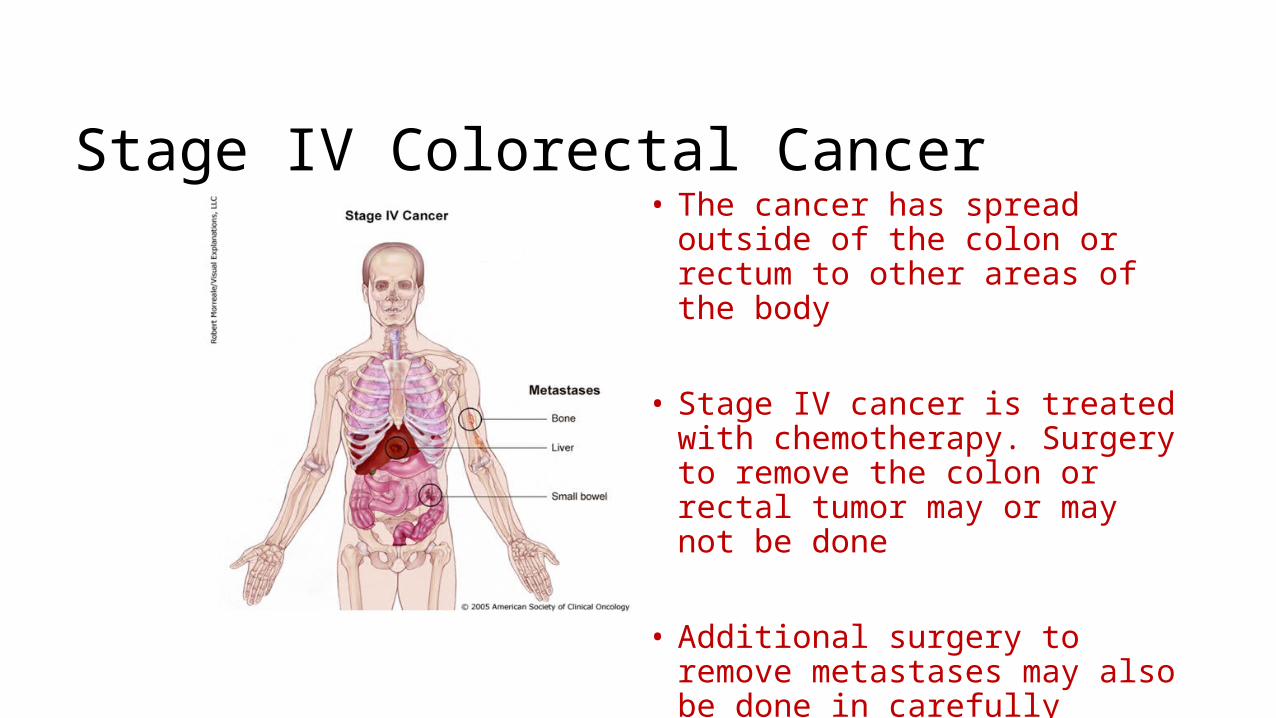
Stage IV Colorectal Cancer• The cancer has spread outside of
the colon or rectum to other areas of the body
• Stage IV cancer is treated with chemotherapy. Surgery to remove the colon or rectal tumor may or may not be done
• Additional surgery to remove metastases may also be done in carefully selected patients

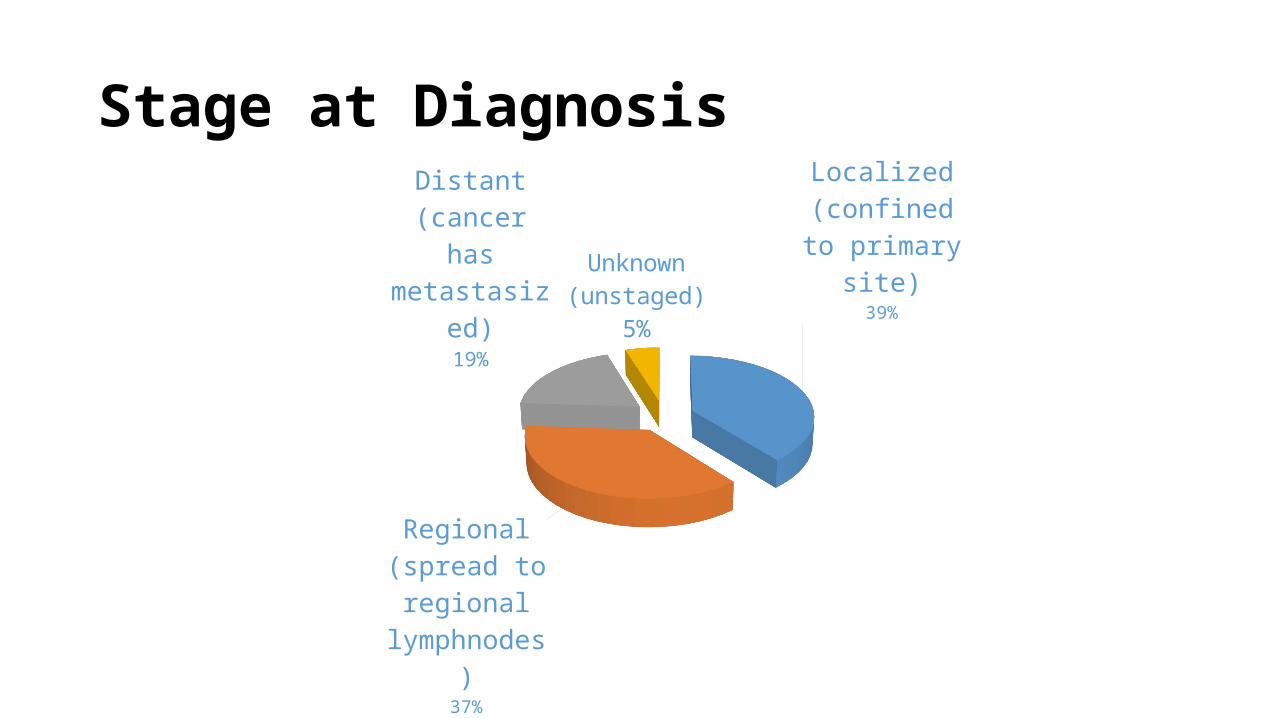
Stage at DiagnosisLocalized (confined to primary
site)39%
Regional (spread to regional lymph-nodes)
37%
Distant (cancer has metastas-
ized)19%
Unknown (unstaged)5%
Sites of Metastasis
• Liver
• Lung
• Brain
• Bone
DIAGNOSTIC WORK UP• Complete history
• Physical examination /DRE-size, location, distance from the verge, mobile versus fixed, and sphincter function.
• Pelvic exam should be performed in women.
• Routine investigations-CBC/LFT/KFT
• Confirmatory- Biopsy
• Gold standard- Colonoscopy+ Biopsy
• Staging workup
• CXR or Chest CT
• Barium enema
• Colonoscopy- To evaluate extent of tumour
• USG Whole Abdomen
• CECT abdomen- pelvis-The sensitivity of CT scan is 50% to 80% accurate, with a 30% to 80% specificity .
65% to 75% accurate for tumor staging and 55% to 65% accurate in mesorectal lymph node staging.
• The ability of CT scans for detecting distant metastasis, including pelvic and para-aortic lymph nodes, is higher than for detecting perirectal nodal involvement (75% to 87% vs. 45%).
• MRI-Liver MRI is considered the test of choice in assessment of hepatic metastases in patients with CRC.
• PET-CT Scan has emerging role.

• For rectal malignancies• Endoscopic Ultrasound (EUS)• Transrectal EUS techniques have been more helpful in efforts to clinically
stage rectal cancers. • EUS is 80% to 95% accurate in tumor staging and 70% to 75% accurate in
mesorectal lymph node staging.
• MRI• MRI techniques have high accuracy in defining the extent of rectal cancer
extension into the mesorectum and in determining the location and stage of tumor.
• Another advantage of MRI is that it can detect involved lymph nodes on the basis of characteristics other than size.

• Others• Stool cytology • CEA• IHC markers- keratin• Molecular markers- Oncogenes• DNA flow cytometry • Immunoscintigraphy
• Screening investigations
PROGNOSITC FACTORS
• ADVERSE C/F• Younger age < 40 yr• Long symptomatology• Obstruction/ perforation• Ulcerative lesion• BT
• ADVERSE PATHOLOGY• High grade• Colloid/ Signet ring cell• LVI +• Perineural invasion +• Aneuploidy• ↑↑ CEA/ collagen• Cell surface antigens CA-
19.9• Local immune response
Most important guide to prognosis is STAGE of the disease i.e. depth of penetration and number of LNs involved
TREATMENT OPTIONS
SURGERY RADIOTHERAPY
CHEMOTHERAPY TARGETED
• SURGRY is the GOLD STANDARD and principle therapy of primary and non metastatic CA Colon
• Curative
• Palliative
• Accurate disease staging
• Guides adjuvant treatment
SURGERY

• PRINCIPLE: Standard treatment•WIDE RESECTION of the involved segment including the lymphatic drainage areas+ mesocolon+ enblock resection of the neighbouring involved organs.
•AIM•To excise the primary lesion with adequate margin ~5 cm of normal bowel proximal and distal to the tumor•To reconstitute bowel continuity •To avoid complications•To inspect the other viscera for mets
• TYPES OF SURGICAL RESECTION• Right Hemicolectomy• Extended Right Hemicolectomy• Left Hemicolectomy• Segmental resection• Total Abdominal Colectomy: UC, FAP Syndrome/ FH
• Sx approach dictated by the lesion size and location.• Location determines what region of bowel is removed, and the extent of its
resection is dictated by its vascular and lymphatic supply.• Minimum of 12-15 LNs should be removed.
CHEMOTHERAPY• Adjuvant: Aim is to destroy microscopic metastatic disease and preventing
death from metastasis as substantially no. of patients treated surgically with curative intent eventually died of metastatic disease
• Metastatic setting/Palliative
• Adjuvant Chemotherapy• The benefit of adjuvant chemotherapy has been clearly demonstrated in stage
III patients, whereas benefit in stage II patients is more controversial. Prospective randomized trials have shown that the addition of 5-flourouracil (5-FU) and leucovorin (LV) improves survival for resected stage III patients.
RADIOTHERAPY• Indications of RT
• Incomplete excision/ Residual disease• Positive resection margins• B2, B3, C2 tumors arising in the immobolized bowel with close CRM(<1
cm)• Fixed tumors i.e. caecal and sigmoidal ca • Tumor a/w perforation/ obstruction/fistula/abscess
Techniques of Irradiation• Generally, an initial dose of 45 Gy in 25 fractions at 1.8 Gy per fraction is
delivered through larger fields to the primary tumor and at-risk tissues. Reduced fields may be treated to 50 Gy if only a small portion of small bowel is included.
• Critical normal (dose limiting) tissues• Small intestine: max 45 Gy (30 Gy by WART)• Liver : 2/3rd of liver should not get >30 Gy• Kidneys: 2/3rd of one kidney should not get >20 Gy • Spinal cord: max dose to spinal cord< 45 Gy

NEWER RT Techniques
IORT- Radiation boosting for dose intensification•T4 tumors with uncertain margins/ invading adjacent structures•Preop EBRT + 5-FU based CCT followed by resection with or without IORT and Post Op systemic therapy.
•Advantage•Visual contrast of target volume•Homogenous treatment of controlled thickness of tissue with tumor•Protection of mobile uninvolved normal tissue
•Disadvantage•Increase incidence of late normal tissue complications
•Dose- With 9-15 Mev electron, 10-20 Gy normalized at 90%
Adjuvant Therapy for Colon Ca• Stage I Colon: Surgery alone
• Stage II Colon: Adjuvant chemotherapy use is controversial. Indicated beyond stage IIA. Considered for the following:
• Obstructed or perforated colon cancer• High-risk histology-LVI +/ extramural spread or PD histo.• Involvement of adjacent organs (T4 lesion)• Inadequate LN sampling (<13 LNs retrieved)• Elevated preop CEA• High S-phase fraction• Tumor not having high level of MSI• 18q deletion
• Stage III Colon• FOLFOX (5-FU + leucovorin + oxaliplatin)• Improved both overall survival and disease-free survival (MOSAIC
Trial)• Adjuvant Chemo-RT is reserved for selected T4 lesions that involve
penetration to fixed structures• Unresectable disease- generally incurable
•Goal: Palliation- symptom control/ control of tumor growth/ lengthen PFS and OS•Palliative chemotherapy: indication if following guidelines are met•Favorable performance status•Acceptable BM / renal / hepatic function•Reasonable nutritional status•Well motivated patients
TREATMENT ALGORITHM RECTUM• Stage I• Lower one-third rectal cancers → APR• Upper/middle one-third rectal cancers → low anterior resection (LAR)• Highly-selected T1 tumors with good prognostic factors: local excision
alone• Good prognostic factors: tumor size <3 cm, circumferential resection line
<1/3, maximum distance from anal verge <8 cm, well-differentiated, surgical margin >3 mm, LVSI (−), PNI (−)
• T1 tumors with good prognostic factors (+), surveillance after surgery
• Stage II–III (resectable)- Preoperative 5-FU/RT + transabdominal surgery + adjuvant CT
• Stage III (unresectable and T4)- 5-FU/RT (then surgery if possible) + CT
• Stage IV- CT or surgery or RT or combinations of them

SURGERY

Surgical Procedure of Primary Site: Rectosigmoid
• Wedge or segmental resection, partial proctosigmoidectomy• Partial proctosigmoidectomy plus resection of contiguous organs• Pull through with sphincter preservation• Total proctectomy• Total colectomy• Total colectomy with ileostomy• Ileorectal reconstruction• Total colectomy with other pouch

Surgical Procedure of Primary Site: Rectum
• Wedge or segmental resection, partial proctectomy• Pull through with sphincter preservation• Total proctectomy• Total proctocolectomy, NOS• Proctectomy or proctocolectomy with resection in continuity with
other organs; pelvic exenteration• LAR• APR

RT PLANNING- Localization, Immobilization, and SimulationImmobilization and patient position• Prone with arms above the head.• Consider belly board to displace small bowel.• Simulate and treat with full bladder to displace small bowel.
Contrast agents and markers• Oral contrast to delineate the small bowel.• Barium enema to delineate the tumor (caution with respect to tumor
displacement).• IV contrast to delineate the tumor and LN.• Anal marker to delineate the anus.
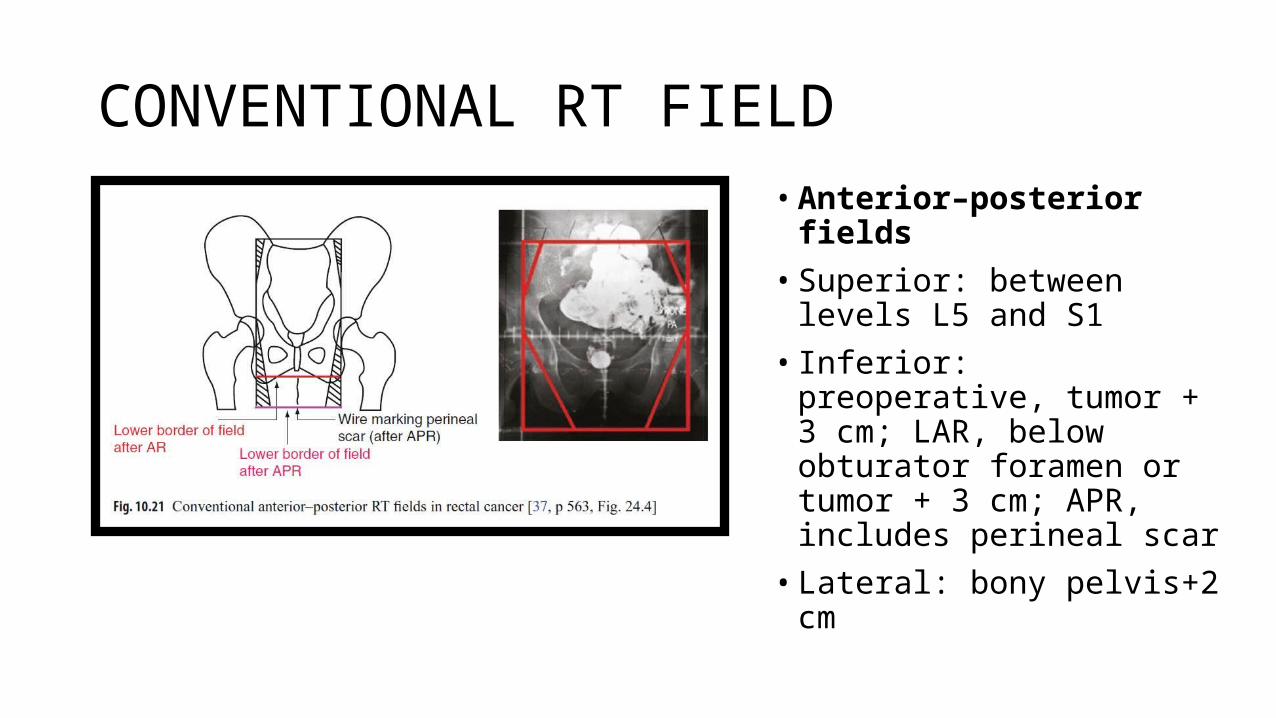
CONVENTIONAL RT FIELD• Anterior–posterior fields• Superior: between levels L5
and S1• Inferior: preoperative, tumor +
3 cm; LAR, below obturator foramen or tumor + 3 cm; APR, includes perineal scar
• Lateral: bony pelvis+2 cm
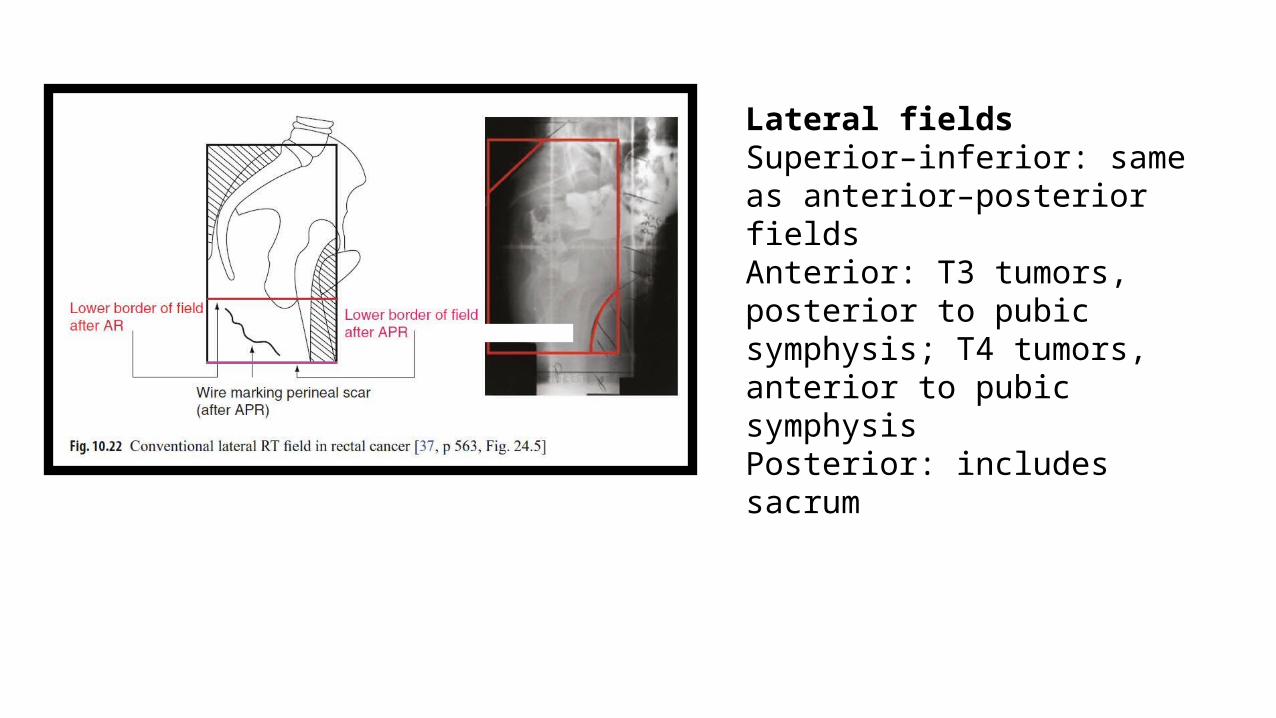
Lateral fieldsSuperior–inferior: same as anterior–posterior fieldsAnterior: T3 tumors, posterior to pubic symphysis; T4 tumors, anterior to pubic symphysisPosterior: includes sacrum

• Boost field → tumor/tumor bed + 2–3 cm. Sacral concavity should be included in lateral fields.
• Dose• 1.8 Gy/day, total dose: 45 Gy four field-box technique, 5.4 Gy boost may
be given.
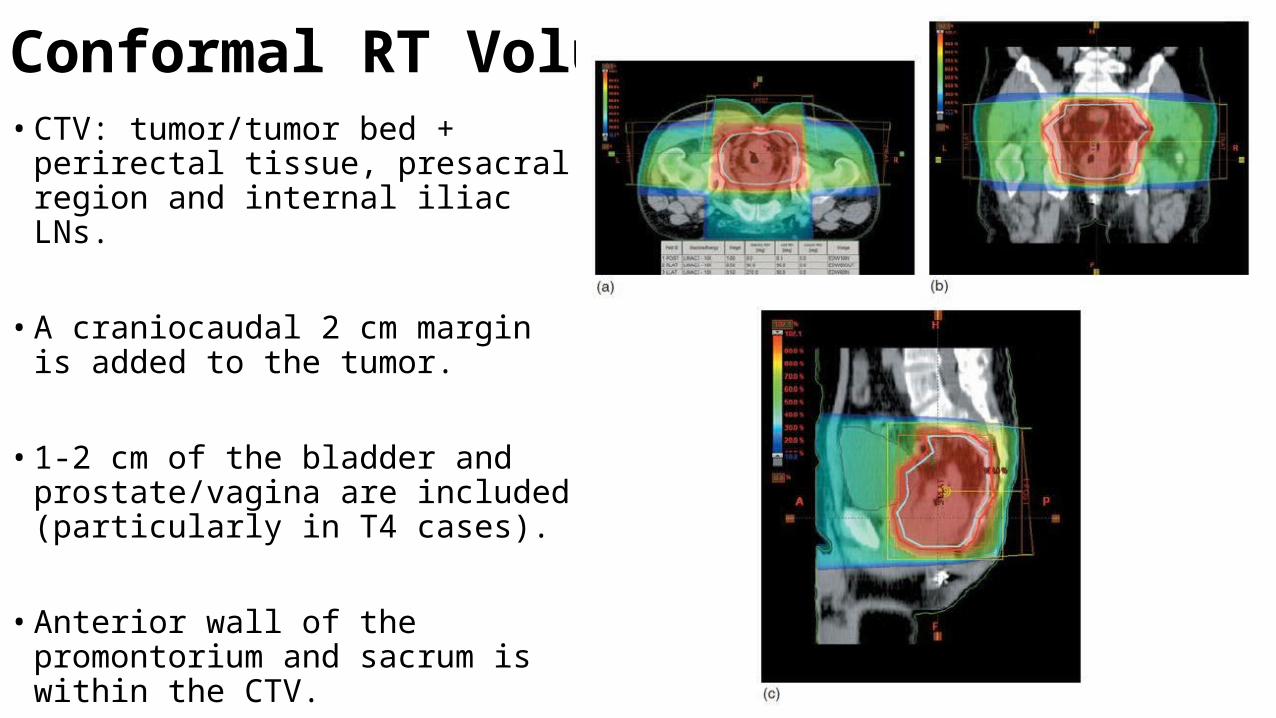
Conformal RT Volumes• CTV: tumor/tumor bed + perirectal tissue,
presacral region and internal iliac LNs.
• A craniocaudal 2 cm margin is added to the tumor.
• 1-2 cm of the bladder and prostate/vagina are included (particularly in T4 cases).
• Anterior wall of the promontorium and sacrum is within the CTV.
• PTV: CTV + 1–1.5 cm

Beam weighing typically 2:1:1 for PA and laterals• High energy for PA field• 6 MV photons used.• IORT: consider for close/+ microscopic margins, especially for T4 or
recurrent CA.• Brachytherapy: consider for macroscopic residual after pre-op
chemoRT and resection.

RT IN RECTUM• Preoperative RT• Advantages:• Large and advanced tumors may be
downsized during radiation and the chances of resection may also increase.
• Tumor cells that may be implanted into the surgical region are eradicated.
• Tumor cells that may enter circulation are eradicated and distant metastatic risk decreases.
• Tumor cells are more oxic before surgery and sensitive to radiation.
• Disadvantages:• Overtreatment of early or metastatic tumors• Delayed surgery and risk of stage
advancement• Postoperative perineal complications may
increase
• Postoperative RT• Advantages:• There is no overtreatment with radiation
due to pathological confirmation of exact stage.
• RT field is accurately designed since tumoral extension is known.
• Disadvantages:• RT efficacy may decrease due to hypoxic
medium after surgery.• Postoperative adhesions may increase
intestinal side effects of RT.• Field size increases after APR due to the
inclusion of the perineal scar in the RT portal.
Neoadjuvant Radiotherapy• It has emerged as the standard of care.• It is associated with-1. Tumour downstaging2. Improved Resectability and Tolerance3. Sphincter Preservation in Distal Rectum tumour4. Improvement in Locoregional control & Overall survival
• Swedish Rectal Cancer Trial (Pahlman et al. 1997; Folkesson et al. 2005): • 1,168 patients with resectable rectal CA randomized to• Pre-op RT (25 Gy/5 fx) and surgery vs surgery alone (non-TME surgery). • Pre-op RT improved 5-year Local Recurrence (11% vs. 27%) and 5-year
OS (58% vs. 48%). • Thirteen-year OS was 38% vs 30% & LR 9% vs 26%.• A higher rate of small bowel obstruction was seen in Pre Op RT arm.

• French Trial, Lyon 90-01• RT was given as 39Gy @ 3Gy/#• Arm I- RT followed by Sx within 2 weeks.• Arm II- RT followed by Sx within 6-8 weeks.• LC and OS was same of 33 months.• Pathologic downstaging in Arm I vs Arm II was 10% vs 26% favouring
longer interval before surgery.
• Two meta analysis of 12,000 patients of 14 trials each-• They reported that Neoadjuvant Radiation Treatment was associated with-• Significantly fewer local recurrences• Improved specific survival• OS benefit• Death from rectal cancer

Neoadjuvant Chemoradiation
• French FFCD 9203 (Gerard 2006): 733 patients with T3-4N0 resectable AdenoCa rectum randomized to pre-op RT (1.8/45 Gy) vs. pre-op concurrent Chemo RT + bolus 5FU(350mg/m2) and LV d1-5 weeks 1 and 5.
• All patients had adjuvant 4 cycles of 5FU-LV chemo.• No difference in 5 year OS.• Pre-op chemoRT increased pCR (3.6 →11.4%) ,Local Relapse decreased (8.1% vs
16.5%), but also grade 3–4 toxicity increased (2.7% → 14.6%). • No difference in sphincter saving surgery (52%), EFS, or OS (67%).

• EORTC 22921 (Bosset et al. 2006; JCO 2007): 1,011 patients with resectable rectal CA randomized to -
Pre-op RT, Pre-op chemoRT, Pre-op RT + post-op chemo, or Pre-op chemoRT + post-op chemo. • RT consisted of 45 Gy and chemo consisted of 5-FU and LV (pre-op
chemo × 2 cycles, post-op chemo × 4cycles). • Increased tumor down staging (14% vs. 5.3%; p = .0001) and lower rates
of LR (9% vs. 17%) but no difference in 5-year OS (65% in both arms). • This information suggests that although there are lower rates of
recurrence, there is no evidence that combined treatment offers a survival benefit compared to radiation alone in the neoadjuvant setting.
• There is, however, a higher incidence of acute toxicity associated with ChemoRT.
Pre Op vs Post Op Chemo RT
• German Rectal Cancer Study Group (Sauer et al. 2004): 823 patients with T3/4 or N+ rectal CA randomized to pre-op vs. post-op chemoRT. Both arms had 50.4 Gy with concurrent 5-FU; post-op arm had additional 5.4 Gy boost.
• Increased rate of sphincter saving procedures (39% vs. 19%); and decreased grade 3–4 acute and late toxicity and late anastomotic strictures.
• Overall, no difference in overall survival between pre- and post-operative chemoRT (76% vs 74%, p = 0.80) but local relapse rates were 6% in the pre-op chemoRT arm vs 13% in the post-op arm, p = 0.01
Oxaliplatin + 5-Fluorouracil + Leucovorin (mFOLFOX7)Oxaliplatin: 100 mg/m2 IV on day 15-Fluorouracil: 3000 mg/m2 IV continuous infusion on days 1 and 2 for 46 hoursLeucovorin: 400 mg/m2 IV on day 1 as a 2-hour infusion before 5-fluorouracilRepeat cycle every 2 weeks
Irinotecan + 5-Fluorouracil + Leucovorin (FOLFIRI Regimen)Irinotecan: 180 mg/m2 IV on day 15-Fluorouracil: 400 mg/m2 IV bolus on day 1, followed by 2400 mg/m2 IV
continuous infusion for 46 hoursLeucovorin: 200 mg/m2 IV on day 1 as a 2-hour infusion prior to 5-fluorouracil
on days 1 – 5 administered before 5 - Fluorouracil Repeat cycle every 2 weeks
CapecitabineCapecitabine: 1250 mg/m2 PO bid on days 1 – 14Repeat cycle every 21 days for a total of 8 cycles. Dose may be decreased to 850-1000 mg/m2 PO bid on days 1-14 to reduce the risk of toxicity without compromising clinical efficacy
Chemotherapy as adjuvant in CRC
Capecitabine + Oxaliplatin (XELOX)Capecitabine: 1000 mg/m2 PO bid on days 1 - 14Oxaliplatin: 130 mg/m2 IV on day 1Repeat cycle every 21 days. May decrease dose of capecitabine to 850 mg/m2 PO bid and dose of oxalioplatin to 100 mg/m2 IV to reduce the risk of toxicity without compromising clinical efficacy
Capecitabine + Irinotecan (XELIRI)Capecitabine: 1000 mg/m2 PO bid on days 1 - 14Irinotecan: 250 mg/m2 IV on day 1 Repeat cycle every 21 days. May decrease dose of capecitabine to 850 mg/m2 PO bid and dose of irinotecan to 200 mg/m2 IV to reduce the risk of toxicity without compromising clinical efficacy
Chemotherapy as adjuvant in CRC

Investigational adjuvant approaches
• Portal vein infusion (↑DFS by 10%)• Intraperitoneal chemotherapy- stage III- 43% ↓mortality• Edrecolomab- not used• Vaccine- Canarypox virus encoded gene induce CEA specific T-cell
response in patients with advanced adenoca • ASI

Targeted therapy in advanced colon cancer
Targeting the angiogenesis process• Tumor growth and metastasis is strongly linked with angiogenesis process.
• The vascular network in the tumor growth involves different complex pathways.
• VEGF is the most potent and specific angiogenic factor and its expression in CRC is correlated with recurrence and prognosis.
• Two different strategies devised to target VEGF are:1. Developing MCA directed against VEGF2. Developing intervention to VEGF pathway involving small different molecules with
tyrosine kinase inhibition activity directed towards the VEGF receptors
Anti – VEGF monoclonal antibody
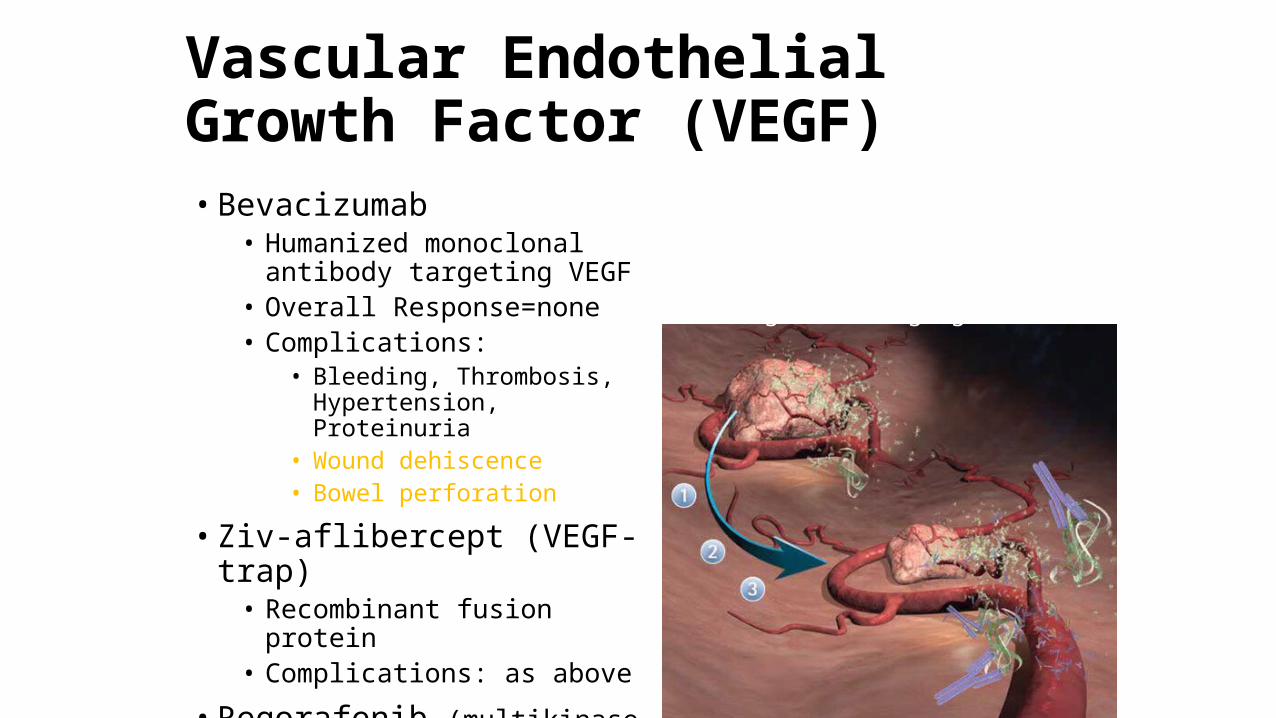
Vascular Endothelial Growth Factor (VEGF)• Bevacizumab
• Humanized monoclonal antibody targeting VEGF
• Overall Response=none• Complications:
• Bleeding, Thrombosis, Hypertension, Proteinuria
• Wound dehiscence• Bowel perforation
• Ziv-aflibercept (VEGF-trap)• Recombinant fusion protein• Complications: as above
• Regorafenib (multikinase inhibitor) VEGFR/Raf/Kit/PDGFR
Agents bind or trap VEGF, reducing tumor angiogenesis
Bevacizumab Approved for use in metastatic CRC in combination with IV 5FU as first-
line Dose: 5 mg/kg IV over 90 mins every 2 weeks
• Toxicities: 1. GI Perforation2. Wound Dehiscence3. Hemorrhage4. Risk of Arteriel TE Events (MI, Stoke)5. Hypertension6. Infusion-related Toxicity7. Proteinuria8. Nehprotic Syndrome
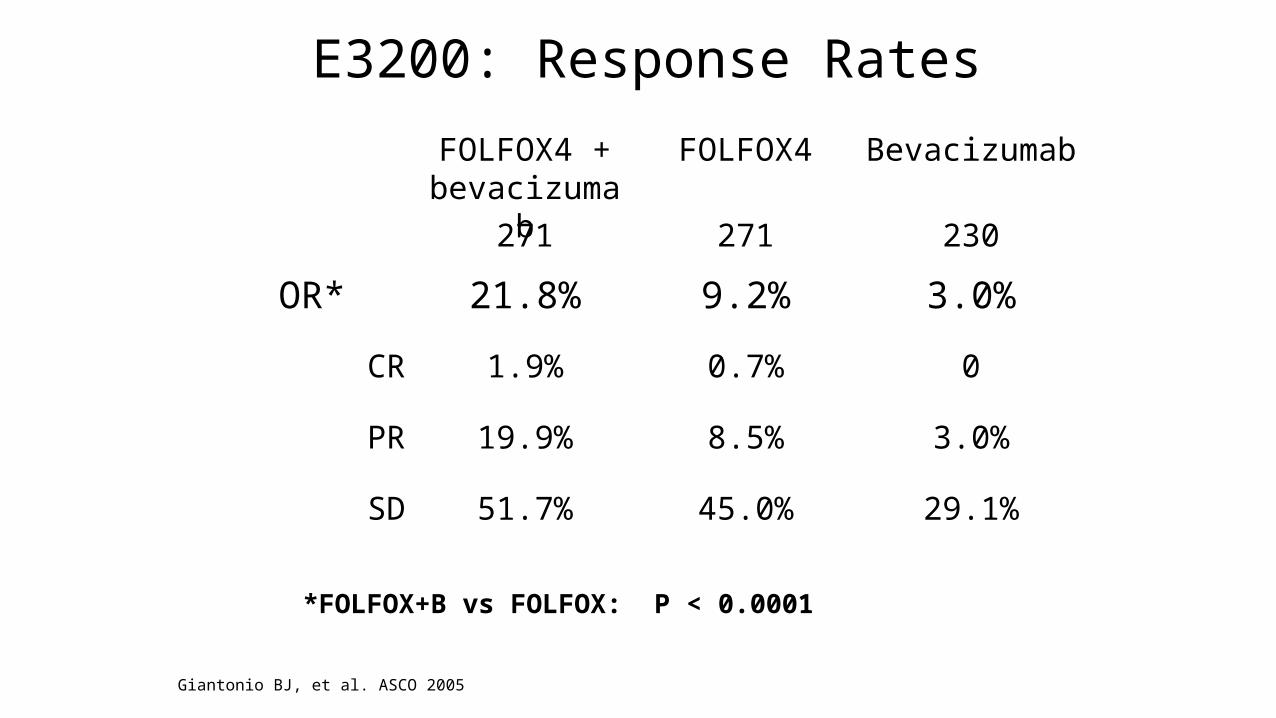
E3200: Response Rates
0.7%
3.0%9.2%21.8%OR*
01.9%CR
29.1%
3.0%
230
Bevacizumab
45.0%51.7%SD
8.5%19.9%PR
271271
FOLFOX4FOLFOX4 + bevacizumab
Giantonio BJ, et al. ASCO 2005
*FOLFOX+B vs FOLFOX: P < 0.0001

The importance of EGFR in metastatic colorectal cancer
EGFR is involved in the progression of mCRCPatients with EGFR-expressing tumors have a shorter
survival
EGFR is expressed in 75 – 89% of mCRC
Siddiqui and Piperdi. Ann Surg Oncol. 17:1168 2010
Cetuximab Chimeric MCA to EGFR Binds with high affinity to transmembrane domain of EGFR and
blocks binding of natural ligands (EGF, TGF) Inhibits EGFR function and downstream signal transduction
pathways, promoting apoptosis Synergistic inhibition with chemotherapy and radiation
Approved for use in EGFR expressing metastatic CRC in combination with Irinotecam in patients refractory to irinotecam or as mono therapy in pts intolerant to irinotecam
Dose: Loading dose of 400 mg/m2., then 250 mg/m2 IV weekly Infusion-related toxicity (40-50%), rash, ILD, asthenia & fatigue,
paronychia

Cetuximab in EGFR expressing metastatic CRC: first line trials
Hoehler T. et al.Proc ESMO 2004
Van Cutsem E. et al.Proc ESMO 2004
Reference
21% resection oflivermetastases
remarks
21 %2%PD
24 %17%SD
55 %81% (74% conf.)(61-88)
CR + PR(95% CI)
3843Total patients
FUFOX +cetuximab
FOLFOX +cetuximab

FOLFIRI5-FU bolus 400 mg/m2, infusion 2400 mg/m2 + Irinotecan 180 mg/m2 +Leucovorin 400 mg/m2
every 2 wks(n = 609)
Patients with previously untreated EGFR-expressing metastatic colorectal cancer, stratified by geographical region, ECOG PS (N = 1217)
FOLFIRI + Cetuximab5-FU bolus 400 mg/m2, infusion 2400 mg/m2 + Irinotecan 180 mg/m2 +Leucovorin 400 mg/m2 every 2 wksCetuximab 400 mg/m2 initial dose, then 250 mg/m2 wkly(n = 608)Van Cutsem E, et al. ASCO 2007. Abstract 4000.
CRYSTAL Trial FOLFIRI ± Cetuximab
EGFR Monoclonal Antibodies• Cetuximab
• Overall Response = 10%• Complications:
• Diarrhea• Skin toxicity• Infusion reactions• Hypomagnesemia• Interstitial lung disease
KRAS-wild type patients only!
Panitumumab– Overall Response =
10%– Complications:
Diarrhea Skin toxicity Hypomagnesemia
FOLLOW UP
• CEA every 3 month x 1st 3 yrs, than 6 monthly up to 5 yrs (CEA detects 80% recurrence) and
• Complete physical examination on each Follow Up
• CECT whole abdomen yearly x 1st 3 yrs
• Colonoscopy every 3 to 5 yrs
• FDG-PET- rising CEA in two consecutive tests in absence of imageable disease by CT

RISING CEA
COLONOSCOPY
FDG-PET
NORMAL
CXR CECT
TAKE HOME MESSAGE
• Incidence and death rates are declining• Eat right, exercise and avoid smoking• Highest risk observed in persons who are both physically inactive and
have high BMIs• Screening saves lives• Most people get screened because their doctor told them to• Advances in treatment have led to improved survival• Advances in molecular profiling of cancers has led to personalized
treatments

THANK YOU