
Colorectal Cancer (CRC) 1)Epidemiology, Risk Factors 2)Symptoms, Stages, Therapy 3) Molecular...
51
Colorectal Cancer (CRC) 1) Epidemiology, Risk Factors 2) Symptoms, Stages, Therapy 3) Molecular Biology & Pathology 4)Screening
-
Upload
arthur-brown -
Category
Documents
-
view
221 -
download
1
Transcript of Colorectal Cancer (CRC) 1)Epidemiology, Risk Factors 2)Symptoms, Stages, Therapy 3) Molecular...
Colorectal Cancer (CRC)
1) Epidemiology, Risk Factors
2) Symptoms, Stages, Therapy
3) Molecular Biology & Pathology
4) Screening

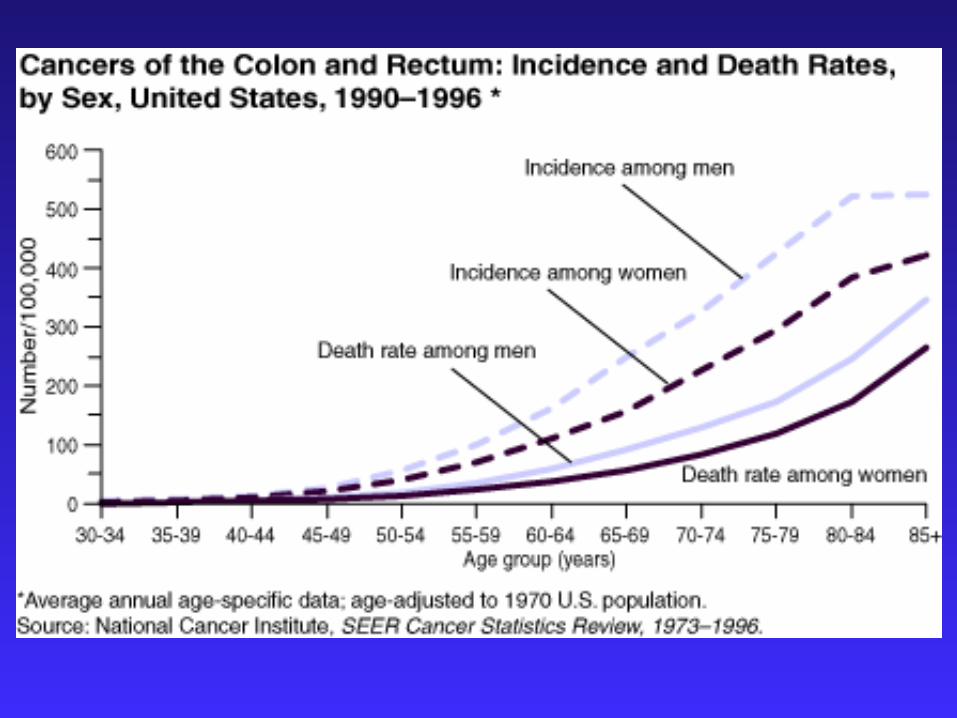
EPIDEMIOLOGY
one of the most common cancers in the world
US: 4th most common cancer (after lung, prostate, and breast cancers)
2nd most common cause of cancer death(after lung cancer)
2001: 130,000 new cases of CRC 56,500 deaths caused by CRC
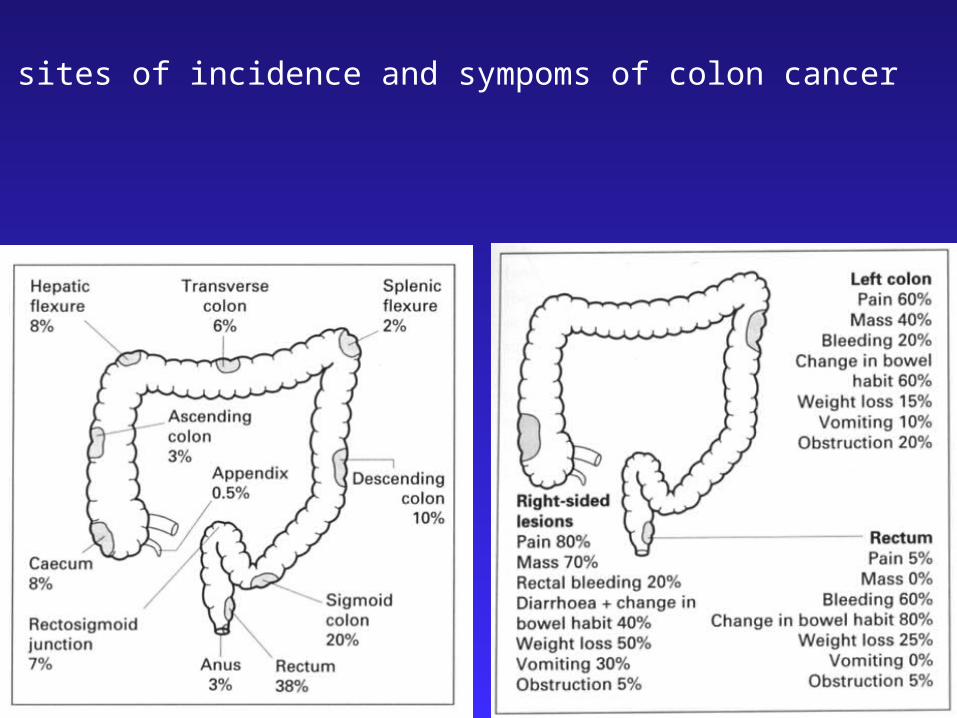
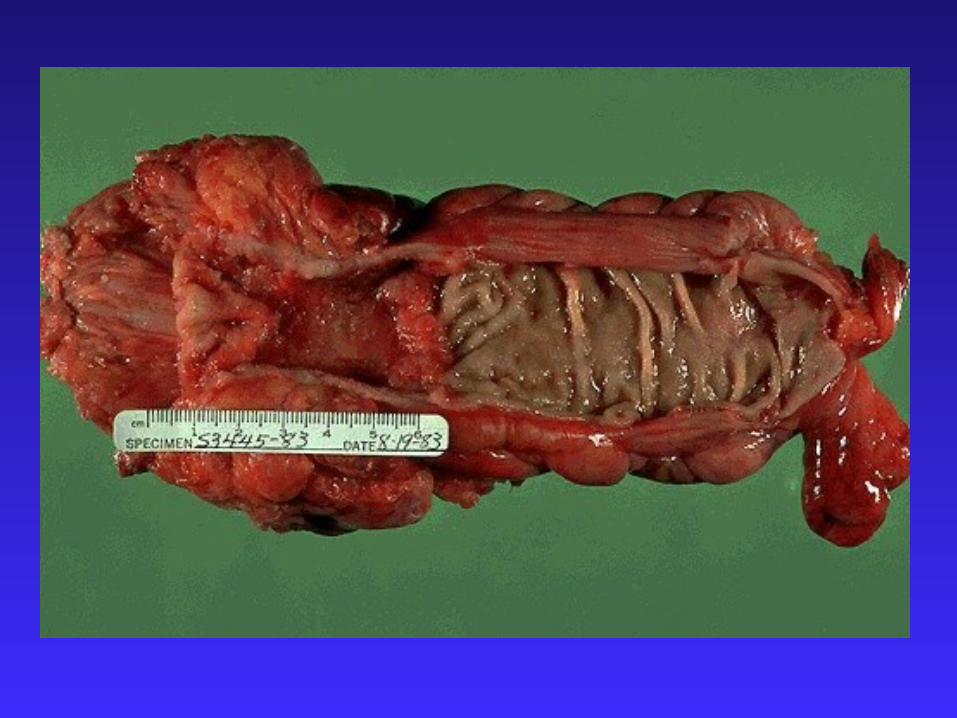
Typical sites of incidence and sympoms of colon cancer


Risk factors for CRC
Age
Adenomas, Polyps
Sedentary lifestyle, Diet, Obesity
Family History of CRC
Inflammatory Bowel Disease (IBD)
Hereditary Syndromes(familial adenomatous polyposis (FAP))

result of interplay between environmental and genetic factors
Central environmental factors:
diet and lifestyle
35% of all cancers are attributable to diet
50%-75% of CRC in the US may be preventable through dietary modifications
Development of CRC
consumption of red meat
animal and saturated fat
refined carbohydrates
alcohol
increased risk
Dietary factors implicated in colorectal carcinogenesis

dietary fiber
vegetables
fruits
antioxidant vitamins
calcium
folate (B Vitamin)
decreased risk
Dietary factors implicated in colorectal carcinogenesis










Symptoms associated with CRC
weight loss
loss of appetite
night sweats
fever
rectal bleeding
change in bowel habits
obstruction
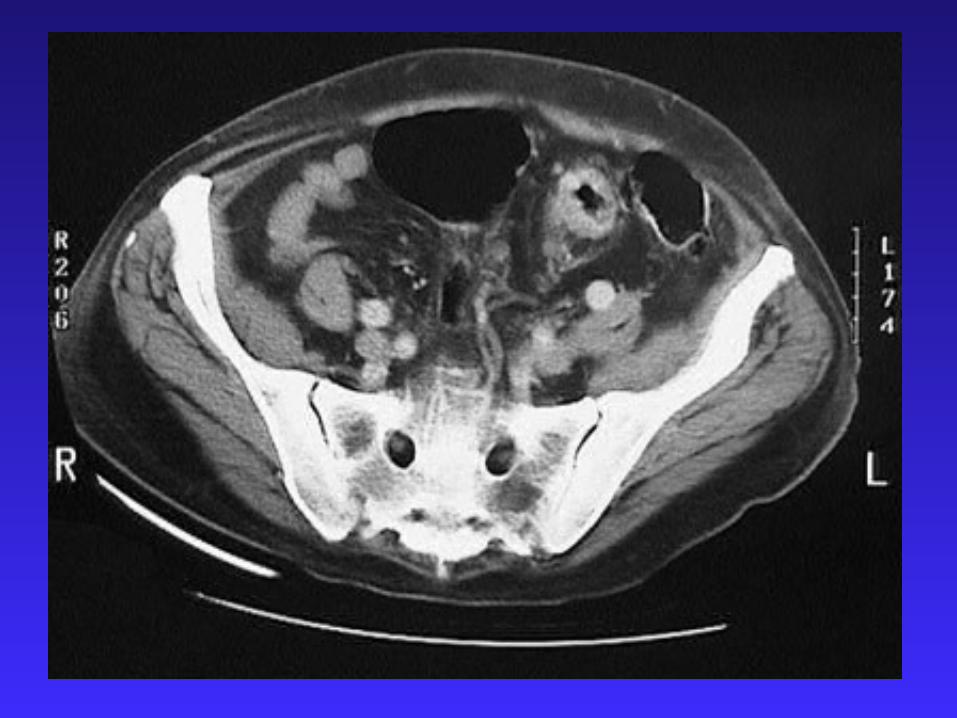
abdominal pain & mass
iron-deficiency anemia

TNM system
Primary tumor (T)
Regional lymph nodes (N)
Distant metastasis (M)
Staging of CRC
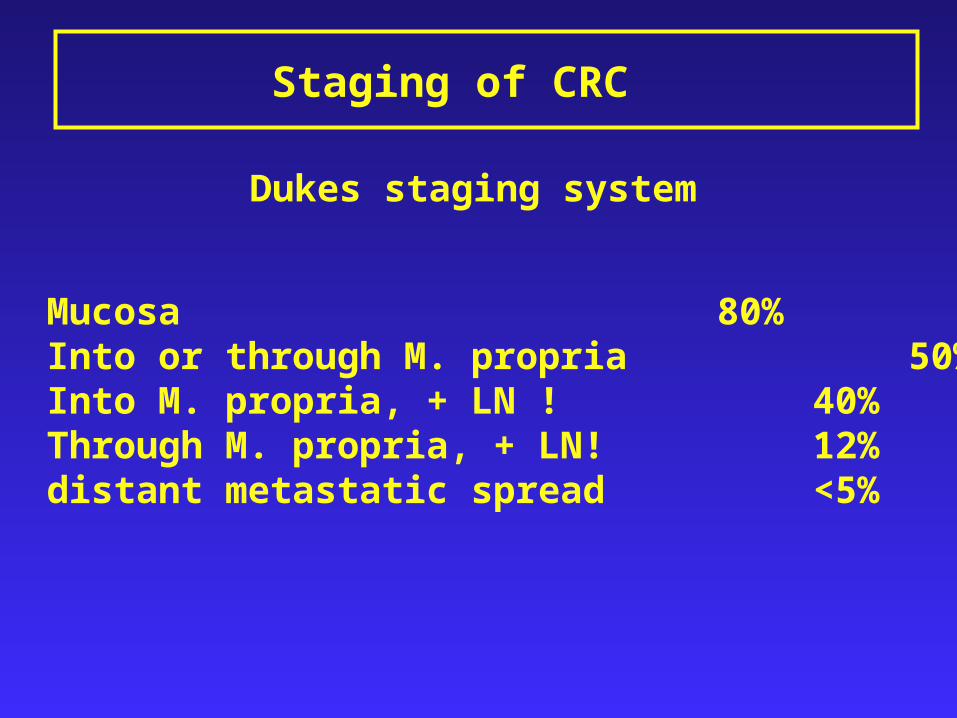
Staging of CRC
A Mucosa 80%B Into or through M. propria 50%C1 Into M. propria, + LN ! 40%C2 Through M. propria, + LN! 12%D distant metastatic spread <5%
Dukes staging system

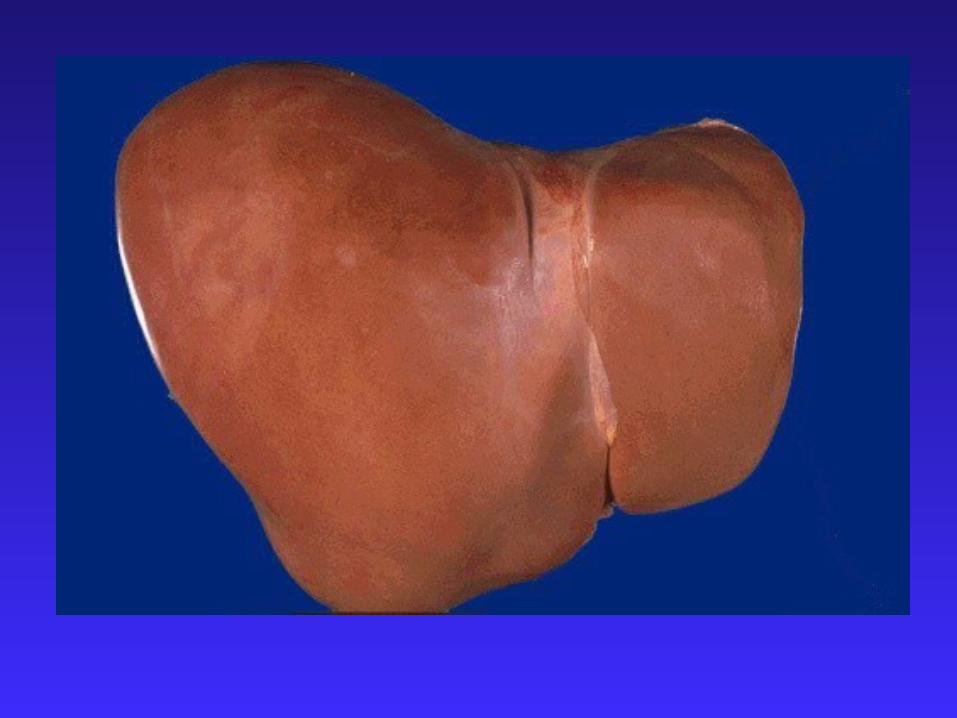
Sites of metastasis
Liver
Lung
Brain
Bones
Via blood
Lymph nodesAbdominal wall
Nerves
Vessels
Via lymphaticsPer continuitatem



Therapy
Surgical resection the only curative treatment
Likelihood of cure is greater when disease isdetected at early stage
Early detection and screening is of pivotalimportance

Screening
What is screening?
a public health service in which members of a defined population are examined to identify those individuals who would benefit from treatment
to benefit: to reduce the risk of a disease or itscomplications
fecal occult blood test (FOBT)chemical test for blood in a stool sample. annual screening by FOBT reduces colorectal cancer deaths by 33%
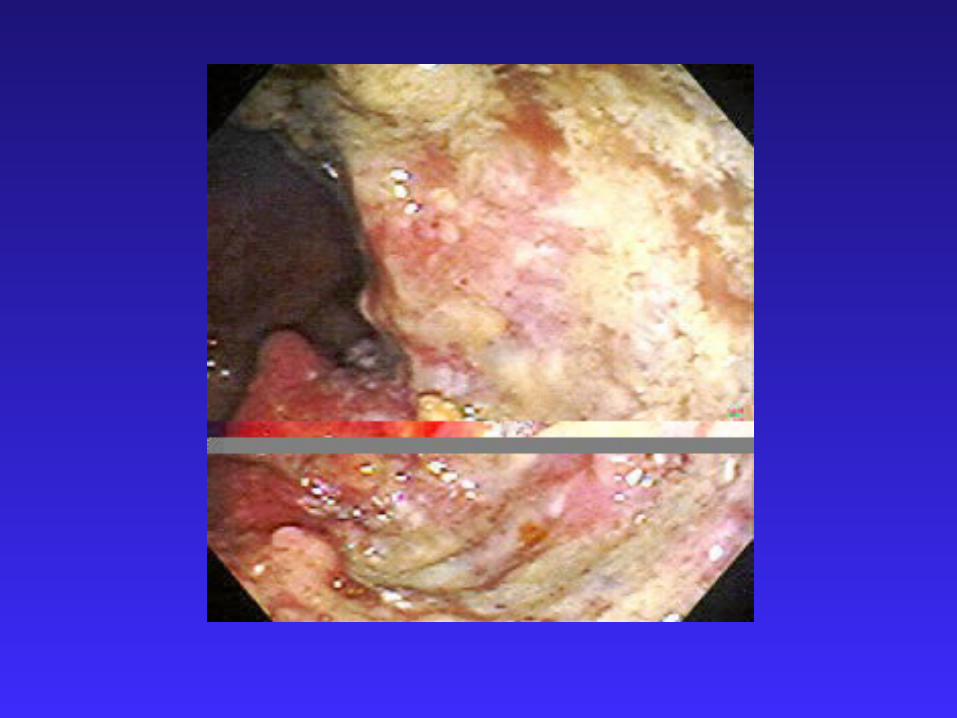
Flexible sigmoidoscopy can detect about 65%–75% of polyps and 40%–65% of colorectal cancers. rectum and sigmoid colon are visually inspected
Types of Screening
regular screening for all adults aged 50 years or older is recommended
FOBT every year
flexible sigmoidoscopy every 5 years
total colon examination by colonoscopy every 10 years or by barium enema every 5–10 years
Current Screening Guidelines

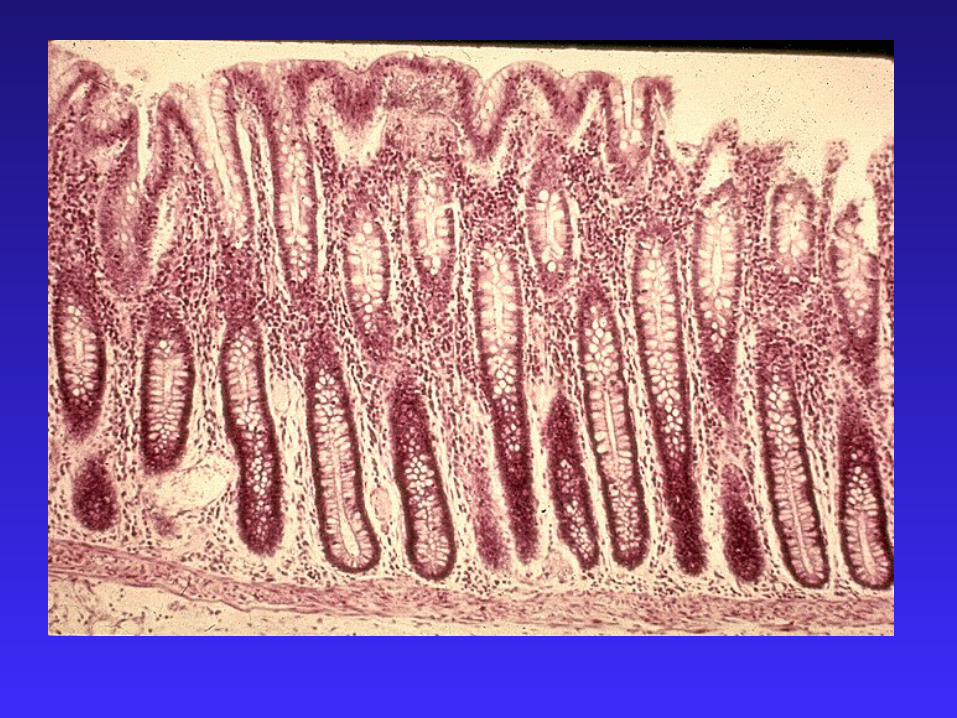
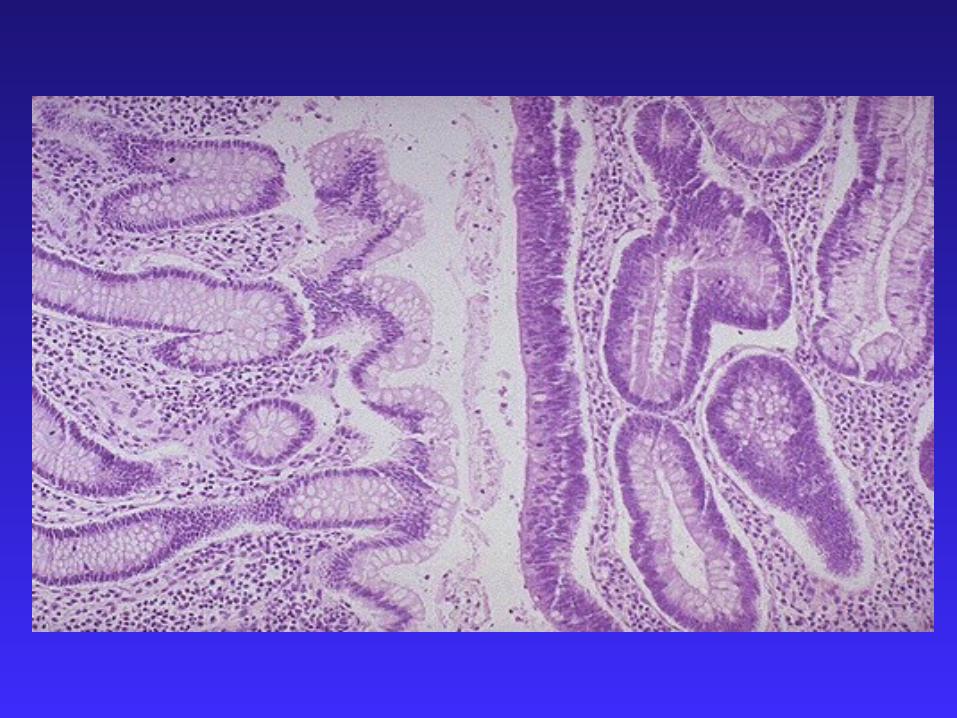
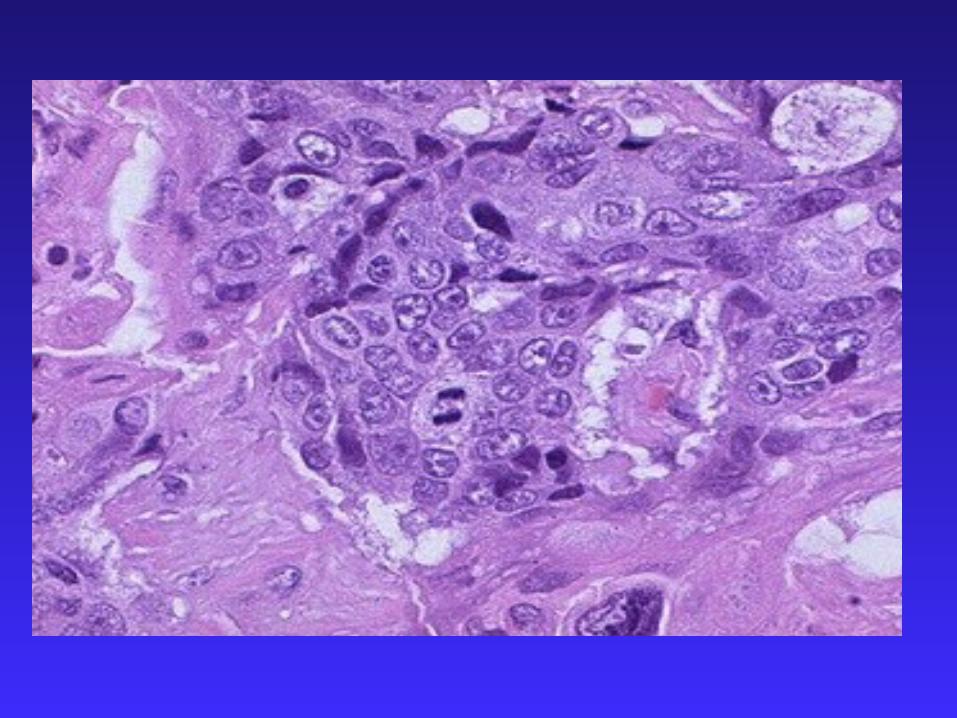

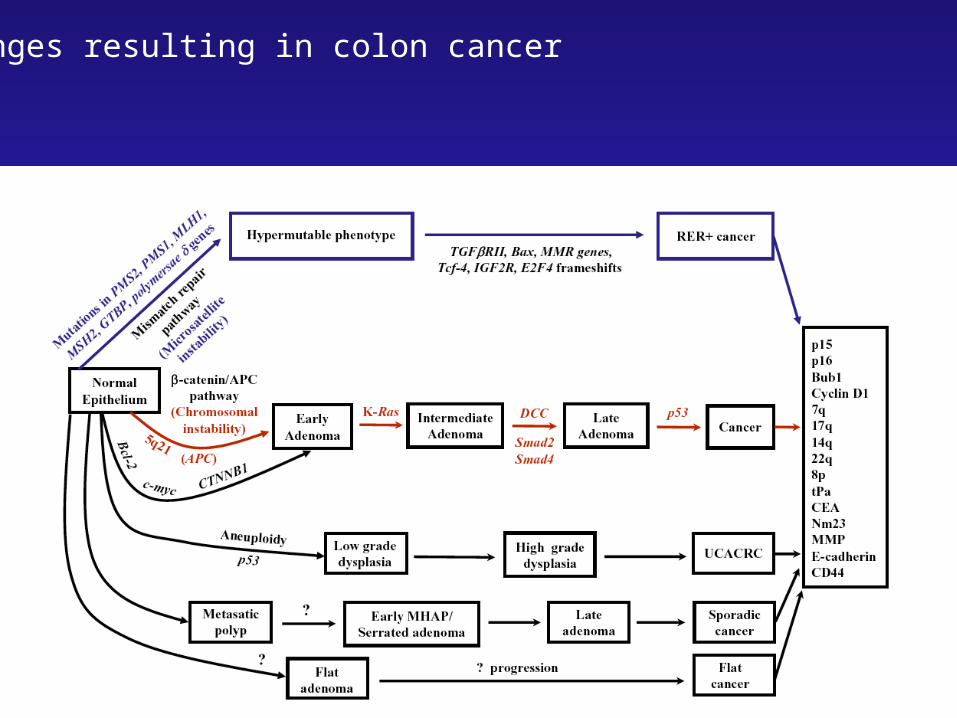
Changes resulting in colon cancer

Molecular Biology & Pathology
CRCs arise from a series of histopathological and molecular changes that transform normal epithelial cells
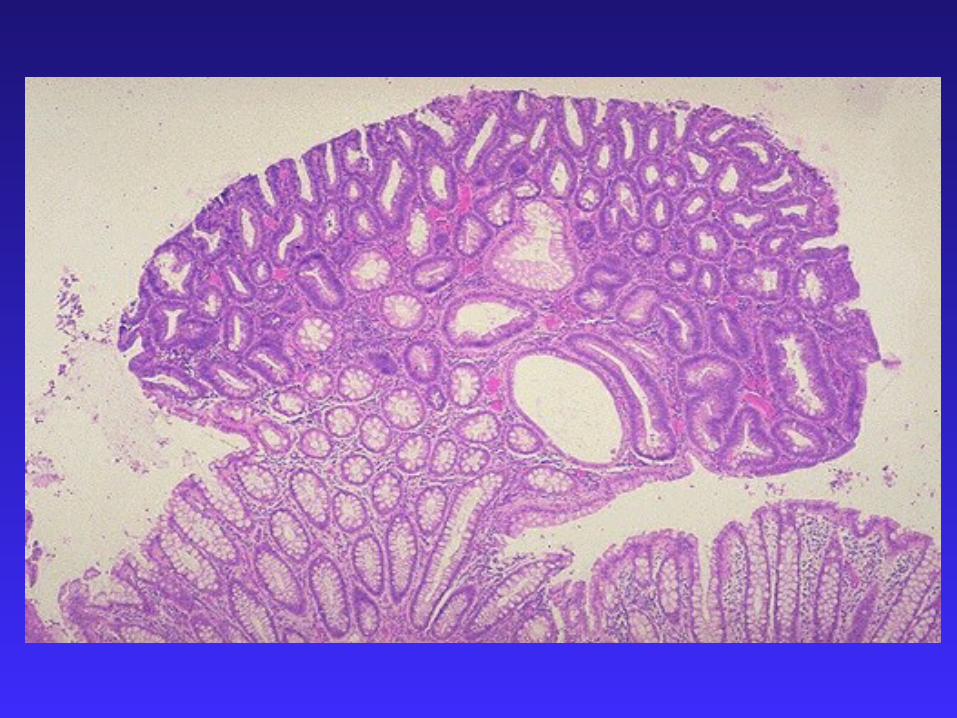
Intermediate step is the adenomatous polyp
Adenoma-Carcinoma-Sequence (Vogelstein & Kinzler)
Polyps occur universally in FAP, but FAP accounts for only 1% of CRCs
Adenomatous Polyps in general population:33% at age 5070% at age 70

Mutations in the APC pathway cause increased proliferation

MMR defects give rise to TGF-beta RII mutations, which preventcell cycle inhibitor (p15) and protease inhibitor (PAI-1) expression
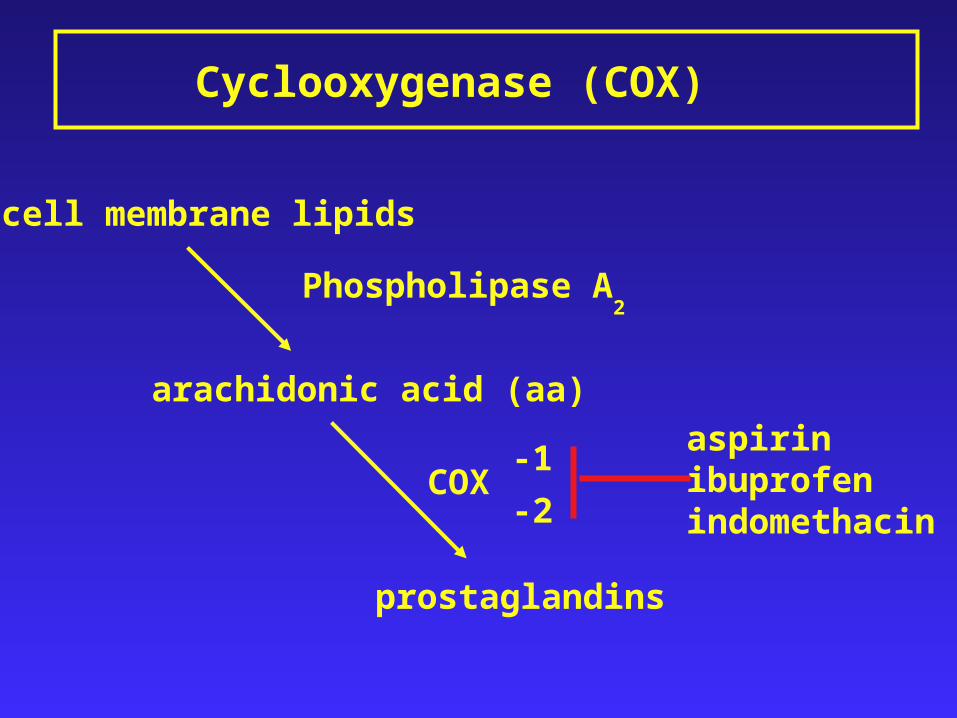
Cyclooxygenase (COX)
cell membrane lipids
arachidonic acid (aa)
prostaglandins
Phospholipase A2
COX-1
-2
aspirinibuprofenindomethacin

COX and CRC
COX-2 not detectable in normal colon but in 90% of CRCs and 40% of adenomas
Animal models: COX-inhibition results in 50% reduction of carcinomas and >90% reduction of adenomas
Epidemiological studies: patients regularly taking aspirin showed 40-50% reduced risk of CRC
But: minimal effective dose and duration of treatmenthave not yet been determined
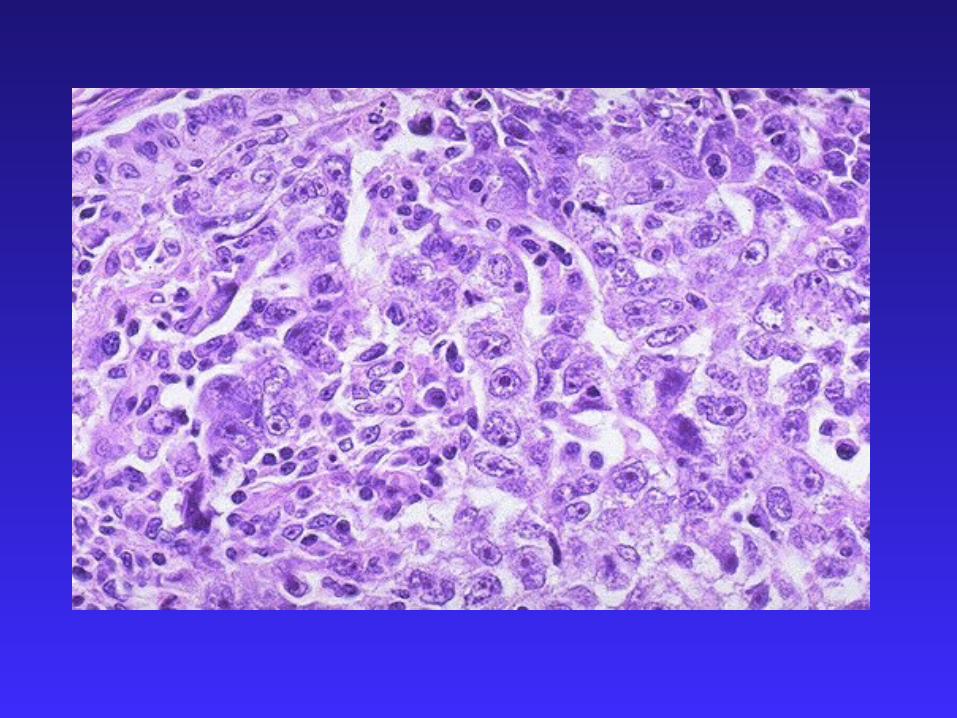
Microenvironment
Control mechanisms of mitosis & apotosis lost
High metabolic rates, glycolysis (Warburg),high lactic acid output
Result: hostile microenvironmental conditions(Hypoxia, low pH, low glucose, free oxygen radicals)

Hypoxia
Central factor for tumor growth and spread
Correlated to tumor hypoxia:Therapy outcome & probablility of metastasis
Hypoxia exerts selective pressuregenetic instability results in survival of cellsbetter adapted to lack of oxygen
Evolution of highly aggressive tumor cells


“Sign up to receive an e-mail message reminding you to have your colon screened at www.wewantthebestforyou.com”
CRC and the Internet

CRC is a leading cause of death
Early stages are detectable
Screening can prevent CRC
Katie Couric: http://www.nccra.com/about/videos.htm
Summary
















![CRC Screening Colorectal Cancer Screening. “Colorectal cancer commands the attention of [us all] because it is one of the most lethal diseases that we.](https://static.fdocuments.us/doc/165x107/56649d765503460f94a57f36/crc-screening-colorectal-cancer-screening-colorectal-cancer-commands-the.jpg)

