Colon Screening Program - BC Cancer · Tubular Adenomas Carry the least risk for malignant...
2
Adenomatous polyps are benign neoplasms that may develop into carcinomas over time. Because this transformation typically occurs over many years, they can be identified and removed before they become malignant. All adenomas require complete removal. After removal, patients are at elevated risk of future adenomas and cancer. Ongoing colonoscopic surveillance is indicated in these individuals. Some histologic types of adenoma and multiple adenoma are known to carry a higher cancer risk and patients who have had these polyps removed require more frequent surveillance: Colon Screening Program Colorectal Polyp Information Sheet for Health Care Providers high-risk polyps Patients with these polyps require more frequent surveillance. Repeat colonoscopy in three years: • Villous and tubulovillous adenoma • Traditional serrated adenoma • Sessile serrated adenoma ≥ 10 mm or with dysplasia • Polyps containing high‑grade dysplasia or carcinoma • Tubular adenomas ≥ 10 mm • Three or more separate adenomas of any size Adenomatous polyp There are different types of polyps that may be identified and removed during a colonoscopy. The two types most commonly found are adenomatous and hyperplastic. type of adenoma description surveillance interval* Tubular Adenomas Sessile Serrated Adenoma with no dysplasia Carry the least risk for malignant transformation. Histologically they are composed of gland‑like structures. Repeat colonoscopy in 5‑10 years (unless adenoma features present as noted below) Villous Adenomas Tubulovillous Adenomas Carry a greater risk of malignant transformation. Histologically, they consist of finger‑like mucosal projections. Tubulo‑villous adenomas are a histologically mixed type with an intermediate prognosis. Repeat colonoscopy in 3 years. Traditional Serrated Adenoma Sessile Serrated Adenoma with dysplasia These adenomas are uncommon. Histologically they are a hybrid between a hyperplastic polyp and a tubular adenoma. Serrated adenomas have only recently been identified as a separate entity so their natural history is not completely understood. Patients should be followed up as for high‑risk adenomas. Repeat colonoscopy in 3 years. other adenoma features that affect cancer risk Degree of Dysplasia The grade of an adenoma is a reflection of the degree of histologic differentiation. The term “adenocarcinoma in situ” is replaced by high‑grade dysplasia. An adenoma with high‑grade dysplasia is high risk. Repeat colonoscopy in 3 years. Size of Adenoma Adenomas ≥ 10 mm in size are high risk. Repeat colonoscopy in 3 years. Number of Adenomas Present The more adenomas that are present, the greater the risk of future adenomas and cancer. If 3 or more identified, repeat colonoscopy in 3 years. If 10 or more identified, refer to the Hereditary Cancer Program. * BC Cancer Agency will recall patients for ongoing surveillance colonoscopies provided that they are within the target age range of 50‑74.
Transcript of Colon Screening Program - BC Cancer · Tubular Adenomas Carry the least risk for malignant...

Adenomatous polyps are benign neoplasms that may develop into carcinomas over time. Because this transformation typically occurs over many years, they can be identified and removed before they become malignant.
All adenomas require complete removal. After removal, patients are at elevated risk of future adenomas and cancer. Ongoing colonoscopic surveillance is indicated in these individuals. Some histologic types of adenoma and multiple adenoma are known to carry a higher cancer risk and patients who have had these polyps removed require more frequent surveillance:
Colon Screening ProgramColorectal Polyp Information Sheet for Health Care Providers
high-risk polypsPatients with these polyps require more frequent surveillance. Repeat colonoscopy in three years:
• Villous and tubulovillous adenoma
• Traditional serrated adenoma
• Sessile serrated adenoma ≥ 10 mm or with dysplasia
• Polyps containing high‑grade dysplasia or carcinoma
• Tubular adenomas ≥ 10 mm
• Three or more separate adenomas of any size
Adenomatous polyp
There are different types of polyps that may be identified and removed during a colonoscopy. The two types most commonly found are adenomatous and hyperplastic.
type of adenoma description surveillance interval*
Tubular Adenomas Sessile Serrated Adenoma with no dysplasia
Carry the least risk for malignant transformation. Histologically they are composed of gland‑like structures.
Repeat colonoscopy in 5‑10 years (unless adenoma features present as noted below)
Villous Adenomas Tubulovillous Adenomas
Carry a greater risk of malignant transformation. Histologically, they consist of finger‑like mucosal projections. Tubulo‑villous adenomas are a histologically mixed type with an intermediate prognosis.
Repeat colonoscopy in 3 years.
Traditional Serrated Adenoma Sessile Serrated Adenoma with dysplasia
These adenomas are uncommon. Histologically they are a hybrid between a hyperplastic polyp and a tubular adenoma. Serrated adenomas have only recently been identified as a separate entity so their natural history is not completely understood. Patients should be followed up as for high‑risk adenomas.
Repeat colonoscopy in 3 years.
other adenoma features that affect cancer risk
Degree of Dysplasia The grade of an adenoma is a reflection of the degree of histologic differentiation. The term “adenocarcinoma in situ” is replaced by high‑grade dysplasia. An adenoma with high‑grade dysplasia is high risk.
Repeat colonoscopy in 3 years.
Size of Adenoma Adenomas ≥ 10 mm in size are high risk. Repeat colonoscopy in 3 years.
Number of Adenomas Present The more adenomas that are present, the greater the risk of future adenomas and cancer.
If 3 or more identified, repeat colonoscopy in 3 years.
If 10 or more identified, refer to the Hereditary Cancer Program.
* BC Cancer Agency will recall patients for ongoing surveillance colonoscopies provided that they are within the target age range of 50‑74.

references
Other polypsThese include inflammatory polyps, mucosal prolapse polyps, prominent mucosal folds and polyps composed of lymphoid follicles. These do not require followup.
Occasionally, hamartomatous polyps may be encountered. Patients with this type of polyp may need additional investigations to determine whether any syndrome (e.g. Peutz‑Jeghers) is present.
AdenocarcinomaPatients who are diagnosed with adenocarcinoma will have appropriate work up and management arranged by their specialist or health care provider.
The individual surveillance needs of patients with a history of colon cancer cannot be met with the Colon Screening Program. These patients should continue to obtain care through their specialist or health care provider.
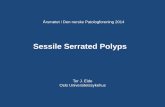
A hyperplastic polyp has no malignant potential and requires no followup.
hyperplastic polyp
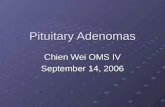
Tubular Adenoma Benign tumor composed of gland-like structures with intervening stroma.
Villous Adenoma Benign tumor consisting of finger-like projections.
Hyperplastic polyps
Adenocarcinoma This tumor has a glandular pattern, but the glands are not separated by stroma and are growing in a “back to back” fashion.
contact usColon Screening Program 801–686 West Broadway Vancouver, BC V5Z1G1
ph: 1‑877‑70‑colon (26566) [email protected] www.screeningbc.ca/colon
1. Lieberman et al. Guidelines for Colonoscopy after Surveillance after screening and polypectomy : A Concensus update by the US multi‑society Task Force on Colorectal Cancer. Gastroenterology 2012;143:844.
2. Ledin D, Enns R et al. Canadian Association of Gastroenterology on screening patients at average risk for developing colon cancer 2010. Can J Gastroenterology 2010;24(12):7050714.
3. Leddin D, Enns R, Hilsden R, Fallone CA, Rabeneck L, Sadowski DC, Singh H. Colorectal cancer surveillance after index colonoscopy: Guidance from the Canadian Association of Gastroenterology. Can J Gastroenterol 2013;27(4):224‑228.
Colon Screening ProgramColorectal Polyp Information Sheet for Health Care Providers
Version: November 2013