06 surgical disease colon and rectum tutorial hajhamad m msu
American Joint Committee on Cancer • 2006 107
12
Colon and Rectum
(Sarcomas, lymphomas, and carcinoid tumors of the large intestine or appendix are not included.)
12
INTRODUCTION
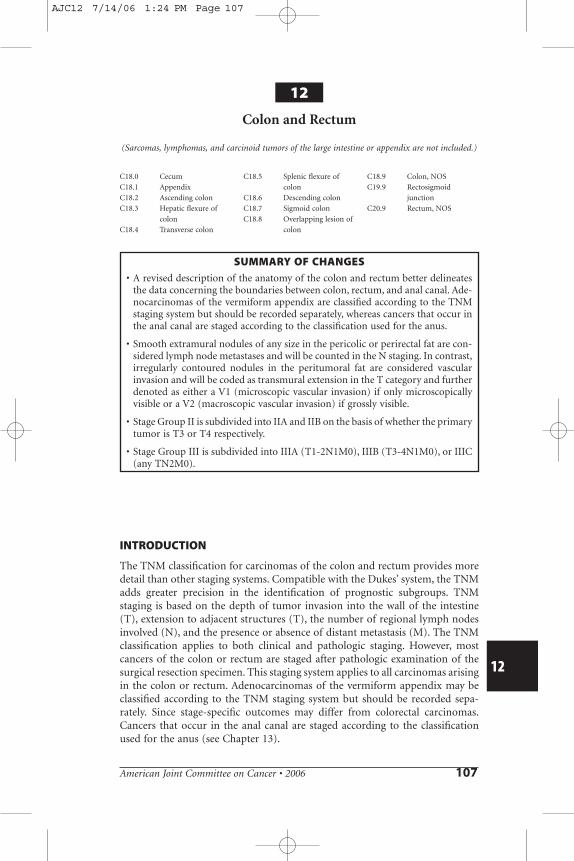
The TNM classification for carcinomas of the colon and rectum provides moredetail than other staging systems. Compatible with the Dukes’ system, the TNMadds greater precision in the identification of prognostic subgroups. TNMstaging is based on the depth of tumor invasion into the wall of the intestine(T), extension to adjacent structures (T), the number of regional lymph nodesinvolved (N), and the presence or absence of distant metastasis (M). The TNMclassification applies to both clinical and pathologic staging. However, mostcancers of the colon or rectum are staged after pathologic examination of thesurgical resection specimen. This staging system applies to all carcinomas arisingin the colon or rectum. Adenocarcinomas of the vermiform appendix may beclassified according to the TNM staging system but should be recorded sepa-rately. Since stage-specific outcomes may differ from colorectal carcinomas.Cancers that occur in the anal canal are staged according to the classificationused for the anus (see Chapter 13).
C18.0 Cecum
C18.1 Appendix
C18.2 Ascending colon
C18.3 Hepatic flexure of
colon
C18.4 Transverse colon
C18.5 Splenic flexure of
colon
C18.6 Descending colon
C18.7 Sigmoid colon
C18.8 Overlapping lesion of
colon
C18.9 Colon, NOS
C19.9 Rectosigmoid
junction
C20.9 Rectum, NOS
SUMMARY OF CHANGES
• A revised description of the anatomy of the colon and rectum better delineatesthe data concerning the boundaries between colon, rectum, and anal canal. Ade-nocarcinomas of the vermiform appendix are classified according to the TNMstaging system but should be recorded separately, whereas cancers that occur inthe anal canal are staged according to the classification used for the anus.
• Smooth extramural nodules of any size in the pericolic or perirectal fat are con-sidered lymph node metastases and will be counted in the N staging. In contrast,irregularly contoured nodules in the peritumoral fat are considered vascularinvasion and will be coded as transmural extension in the T category and furtherdenoted as either a V1 (microscopic vascular invasion) if only microscopicallyvisible or a V2 (macroscopic vascular invasion) if grossly visible.
• Stage Group II is subdivided into IIA and IIB on the basis of whether the primarytumor is T3 or T4 respectively.
• Stage Group III is subdivided into IIIA (T1-2N1M0), IIIB (T3-4N1M0), or IIIC(any TN2M0).
AJC12 7/14/06 1:24 PM Page 107
108 American Joint Committee on Cancer • 2006
ANATOMY
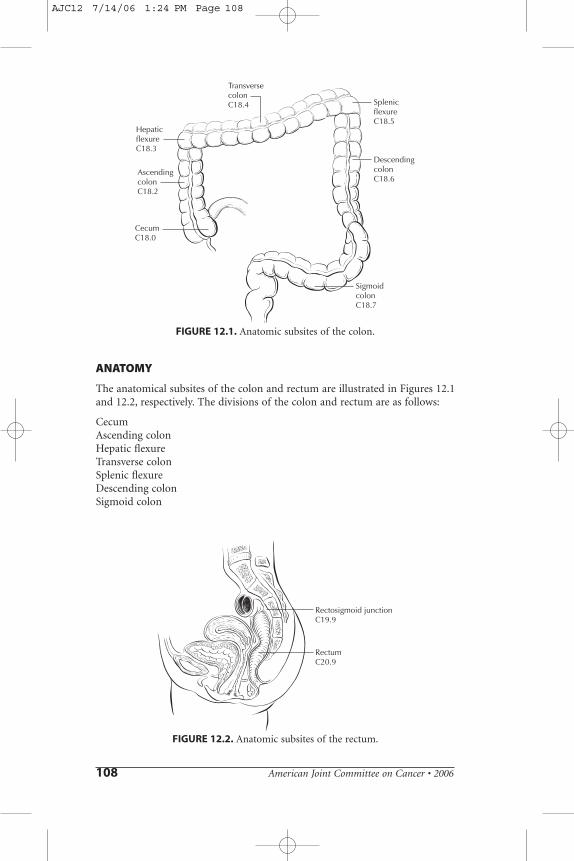
The anatomical subsites of the colon and rectum are illustrated in Figures 12.1and 12.2, respectively. The divisions of the colon and rectum are as follows:
CecumAscending colonHepatic flexureTransverse colonSplenic flexureDescending colonSigmoid colon
HepaticflexureC18.3
TransversecolonC18.4 Splenic
flexureC18.5
DescendingcolonC18.6
SigmoidcolonC18.7
AscendingcolonC18.2
CecumC18.0
FIGURE 12.1. Anatomic subsites of the colon.
Rectosigmoid junctionC19.9
RectumC20.9
FIGURE 12.2. Anatomic subsites of the rectum.
AJC12 7/14/06 1:24 PM Page 108

American Joint Committee on Cancer • 2006 109
Rectosigmoid colonRectum
Primary Site. The large intestine (colorectum) extends from the terminalileum to the anal canal. Excluding the rectum and vermiform appendix,the colon is divided into four parts: the right or ascending colon, the middle or transverse colon, the left or descending colon, and the sigmoid colon.The sigmoid is continuous with the rectum, which terminates at the anal canal.
The cecum is a large, blind pouch that arises from the proximal segment ofthe right colon. It measures 6 cm by 9 cm and is covered with peritoneum. Theascending colon measures 15–20 cm in length. The posterior surface of theascending (and descending) colon lacks peritoneum and thus is in direct contactwith the retroperitoneum. In contrast, the anterior and lateral surfaces of theascending (and descending) colon have serosa and are intraperitoneal. Thehepatic flexure connects the ascending colon with the transverse colon, passingjust inferior to the liver and anterior to the duodenum.
The transverse colon is entirely intraperitoneal, supported on a long mesentery that is attached to the pancreas. Anteriorly, its serosa is continuouswith the gastrocolic ligament. The splenic flexure connects the transverse colon to the descending colon, passing inferior to the spleen and anterior to thetail of the pancreas. As noted above, the posterior aspect of the descending colon lacks serosa and is in direct contact with the retroperitoneum, whereas the lateral and anterior surfaces have serosa and are intraperitoneal. Thedescending colon measures 10–15 cm in length. The colon becomes com-pletely intraperitoneal once again at the sigmoid colon, where the mesenterydevelops at the medial border of the left posterior major psoas muscle andextends to the rectum. The transition from sigmoid colon to rectum is markedby the fusion of the tenia of the sigmoid colon to form the circumferential longitudinal muscle of the rectum. This occurs roughly 12–15 cm from thedentate line.
Approximately 12 cm in length, the rectum extends proximally from thefusion of the tenia to the puborectalis ring distally. The rectum is covered byperitoneum in front and on both sides in its upper third and only on the ante-rior wall in its middle third. The peritoneum is reflected laterally from therectum to form the perirectal fossa and, anteriorly, the uterine or rectovesicalfold. There is no peritoneal covering in the lower third, which is often knownas the rectal ampulla. The anal canal, which measures 3–5 cm in length, extendsfrom the puborectalis sling to the anal verge.
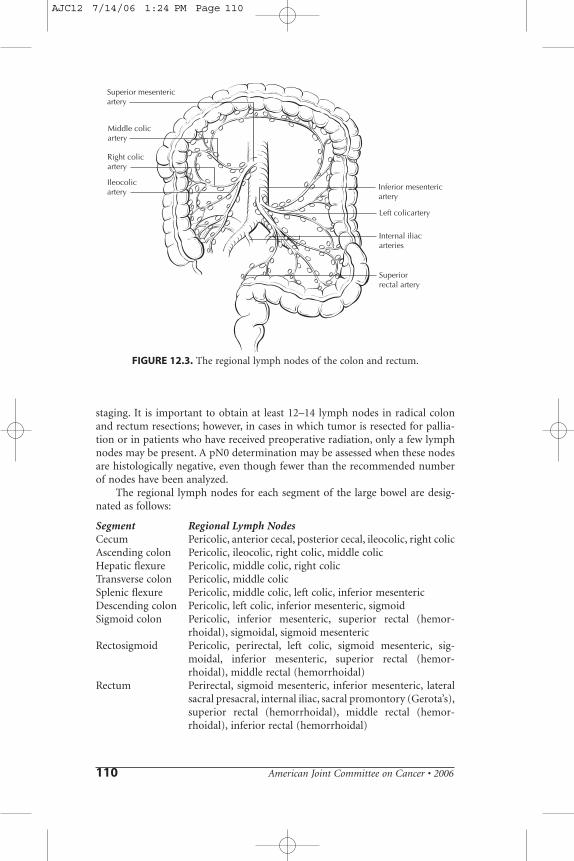
Regional Lymph Nodes. Regional nodes are located (1) along the course ofthe major vessels supplying the colon and rectum, (2) along the vascular arcadesof the marginal artery, and (3) adjacent to the colon—that is, located along themesocolic border of the colon. Specifically, the regional lymph nodes are thepericoloic and perirectal nodes and those found along the ileocolic, right colic,middle colic, left colic, inferior mesenteric artery, superior rectal (hemor-rhoidal), and internal iliac arteries (Figure 12.3).
For pN, the number of lymph nodes sampled should be recorded. Thenumber of nodes examined from an operative specimen has been reported tobe associated with improved survival, possibly because of increased accuracy in
12
AJC12 7/14/06 1:24 PM Page 109
110 American Joint Committee on Cancer • 2006
staging. It is important to obtain at least 12–14 lymph nodes in radical colonand rectum resections; however, in cases in which tumor is resected for pallia-tion or in patients who have received preoperative radiation, only a few lymphnodes may be present. A pN0 determination may be assessed when these nodesare histologically negative, even though fewer than the recommended numberof nodes have been analyzed.
The regional lymph nodes for each segment of the large bowel are desig-nated as follows:
Segment Regional Lymph NodesCecum Pericolic, anterior cecal, posterior cecal, ileocolic, right colicAscending colon Pericolic, ileocolic, right colic, middle colicHepatic flexure Pericolic, middle colic, right colicTransverse colon Pericolic, middle colicSplenic flexure Pericolic, middle colic, left colic, inferior mesentericDescending colon Pericolic, left colic, inferior mesenteric, sigmoidSigmoid colon Pericolic, inferior mesenteric, superior rectal (hemor-
rhoidal), sigmoidal, sigmoid mesentericRectosigmoid Pericolic, perirectal, left colic, sigmoid mesenteric, sig-
moidal, inferior mesenteric, superior rectal (hemor-rhoidal), middle rectal (hemorrhoidal)
Rectum Perirectal, sigmoid mesenteric, inferior mesenteric, lateralsacral presacral, internal iliac, sacral promontory (Gerota’s),superior rectal (hemorrhoidal), middle rectal (hemor-rhoidal), inferior rectal (hemorrhoidal)
Right colicartery
Ileocolicartery
Left colicartery
Superiorrectal artery
Internal iliacarteries
Inferior mesentericartery
Superior mesentericartery
Middle colicartery
FIGURE 12.3. The regional lymph nodes of the colon and rectum.
AJC12 7/14/06 1:24 PM Page 110
American Joint Committee on Cancer • 2006 111
Metastatic Sites. Although carcinomas of the colon and rectum can metastasize to almost any organ, the liver and lungs are the most common sites.Seeding of other segments of the colon, small intestine, or peritoneum can alsooccur.
DEFINITIONS
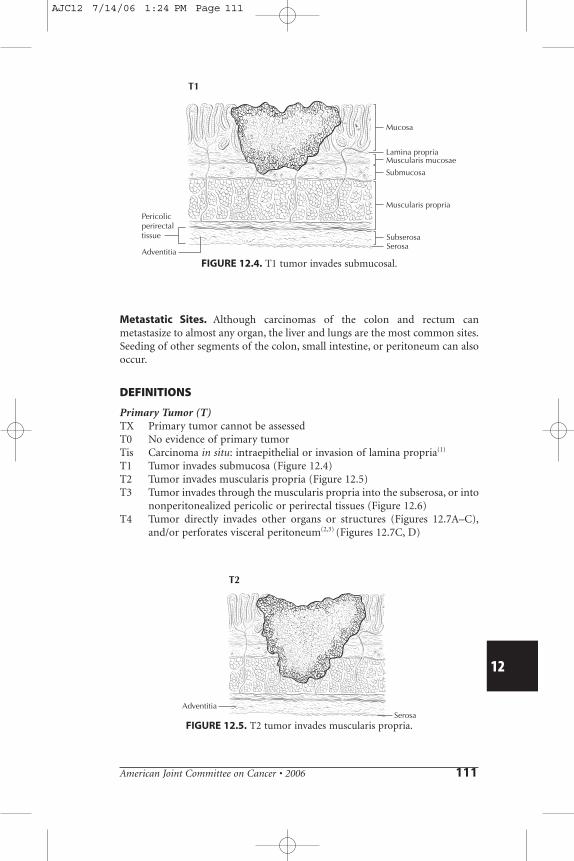
Primary Tumor (T)TX Primary tumor cannot be assessedT0 No evidence of primary tumorTis Carcinoma in situ: intraepithelial or invasion of lamina propria(1)
T1 Tumor invades submucosa (Figure 12.4)T2 Tumor invades muscularis propria (Figure 12.5)T3 Tumor invades through the muscularis propria into the subserosa, or into
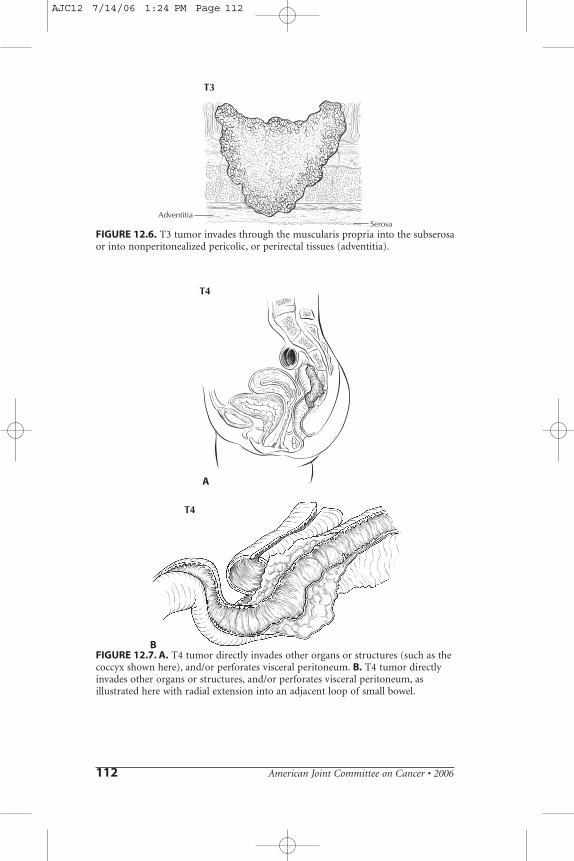
nonperitonealized pericolic or perirectal tissues (Figure 12.6)T4 Tumor directly invades other organs or structures (Figures 12.7A–C),
and/or perforates visceral peritoneum(2,3) (Figures 12.7C, D)
12
T1
Pericolicperirectaltissue
Mucosa
Lamina propria
Submucosa
Muscularis propria
Muscularis mucosae
SubserosaSerosa
Adventitia
FIGURE 12.4. T1 tumor invades submucosal.
T2
SerosaAdventitia
FIGURE 12.5. T2 tumor invades muscularis propria.
AJC12 7/14/06 1:24 PM Page 111
112 American Joint Committee on Cancer • 2006
T3
SerosaAdventitia
FIGURE 12.6. T3 tumor invades through the muscularis propria into the subserosaor into nonperitonealized pericolic, or perirectal tissues (adventitia).
T4
A
T4
BFIGURE 12.7. A. T4 tumor directly invades other organs or structures (such as thecoccyx shown here), and/or perforates visceral peritoneum. B. T4 tumor directlyinvades other organs or structures, and/or perforates visceral peritoneum, asillustrated here with radial extension into an adjacent loop of small bowel.
AJC12 7/14/06 1:24 PM Page 112
American Joint Committee on Cancer • 2006 113
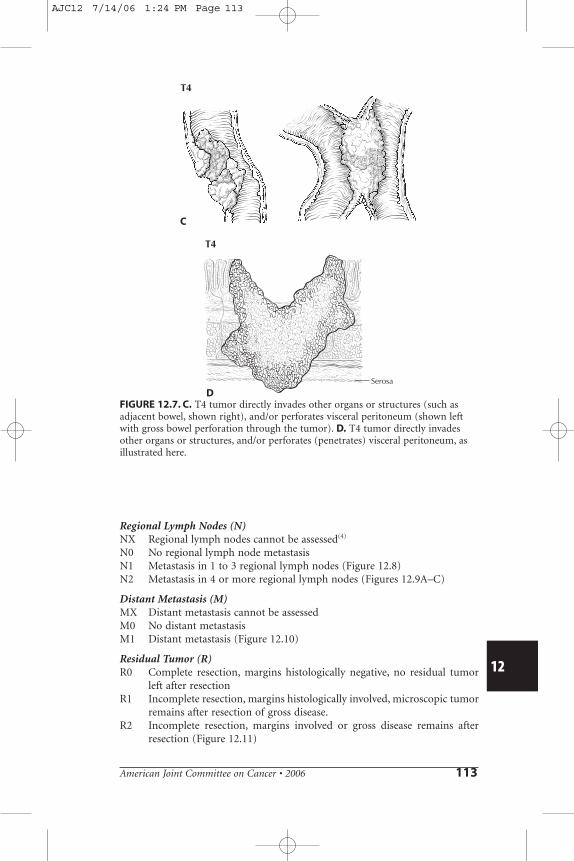
Regional Lymph Nodes (N)NX Regional lymph nodes cannot be assessed(4)
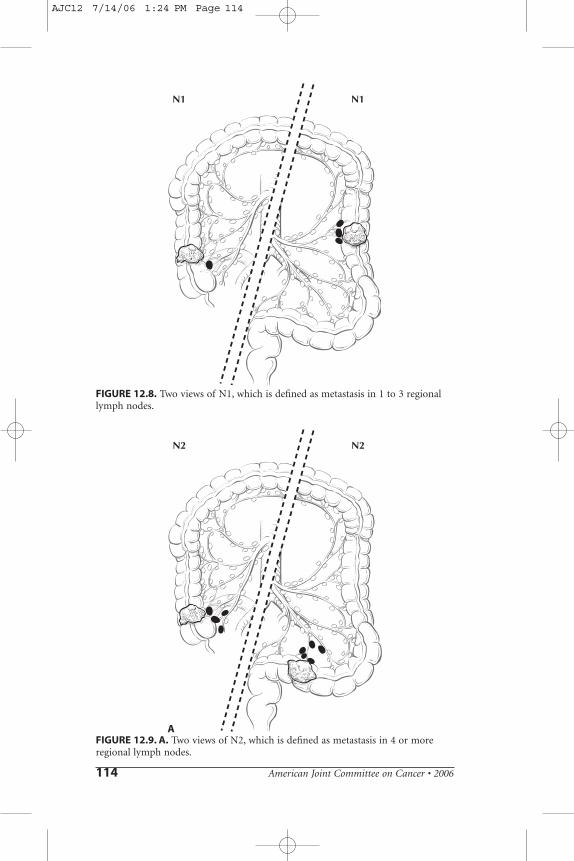
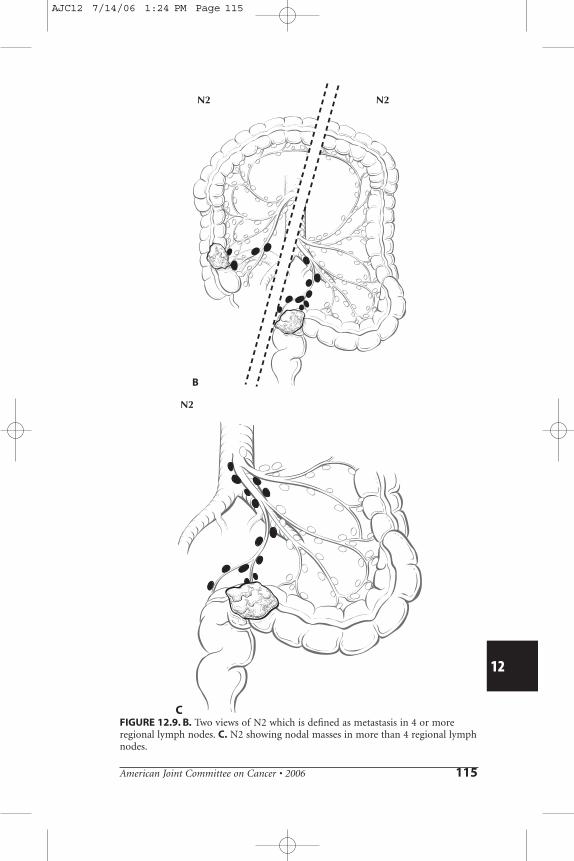
N0 No regional lymph node metastasisN1 Metastasis in 1 to 3 regional lymph nodes (Figure 12.8)N2 Metastasis in 4 or more regional lymph nodes (Figures 12.9A–C)
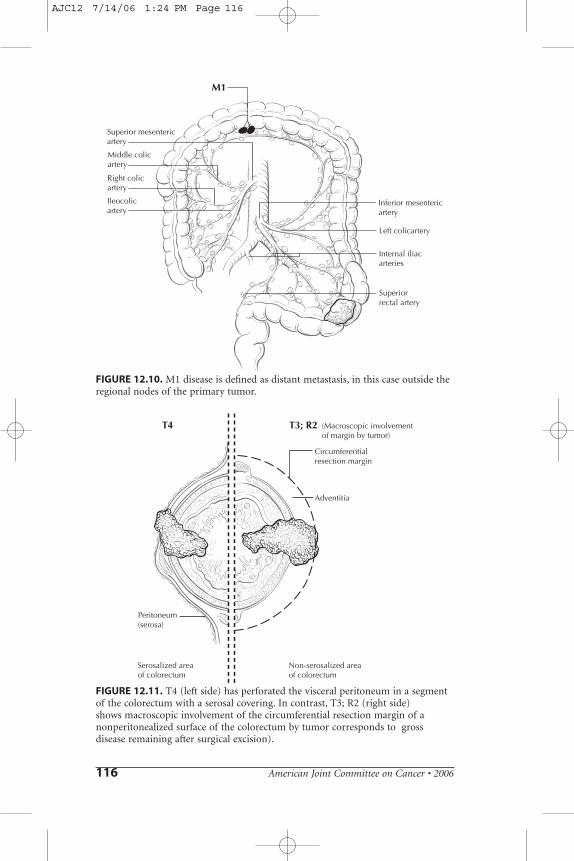
Distant Metastasis (M)MX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis (Figure 12.10)
Residual Tumor (R)R0 Complete resection, margins histologically negative, no residual tumor
left after resectionR1 Incomplete resection, margins histologically involved, microscopic tumor
remains after resection of gross disease.R2 Incomplete resection, margins involved or gross disease remains after
resection (Figure 12.11)
12
T4
C
T4
Serosa
DFIGURE 12.7. C. T4 tumor directly invades other organs or structures (such asadjacent bowel, shown right), and/or perforates visceral peritoneum (shown leftwith gross bowel perforation through the tumor). D. T4 tumor directly invadesother organs or structures, and/or perforates (penetrates) visceral peritoneum, asillustrated here.
AJC12 7/14/06 1:24 PM Page 113
114 American Joint Committee on Cancer • 2006
N1 N1
FIGURE 12.8. Two views of N1, which is defined as metastasis in 1 to 3 regionallymph nodes.
N2 N2
AFIGURE 12.9. A. Two views of N2, which is defined as metastasis in 4 or moreregional lymph nodes.
AJC12 7/14/06 1:24 PM Page 114
American Joint Committee on Cancer • 2006 115
12
N2 N2
B
N2
CFIGURE 12.9. B. Two views of N2 which is defined as metastasis in 4 or moreregional lymph nodes. C. N2 showing nodal masses in more than 4 regional lymphnodes.
AJC12 7/14/06 1:24 PM Page 115
116 American Joint Committee on Cancer • 2006
M1
Right colicartery
Ileocolicartery
Left colicartery
Superiorrectal artery
Internal iliacarteries
Inferior mesentericartery
Superior mesentericartery
Middle colicartery
FIGURE 12.10. M1 disease is defined as distant metastasis, in this case outside theregional nodes of the primary tumor.
T4 T3; R2
Circumferentialresection margin
Peritoneum(serosa)
Adventitia
(Macroscopic involvementof margin by tumor)
Serosalized areaof colorectum
Non-serosalized areaof colorectum
FIGURE 12.11. T4 (left side) has perforated the visceral peritoneum in a segmentof the colorectum with a serosal covering. In contrast, T3; R2 (right side) shows macroscopic involvement of the circumferential resection margin of anonperitonealized surface of the colorectum by tumor corresponds to grossdisease remaining after surgical excision).
AJC12 7/14/06 1:24 PM Page 116
American Joint Committee on Cancer • 2006 117
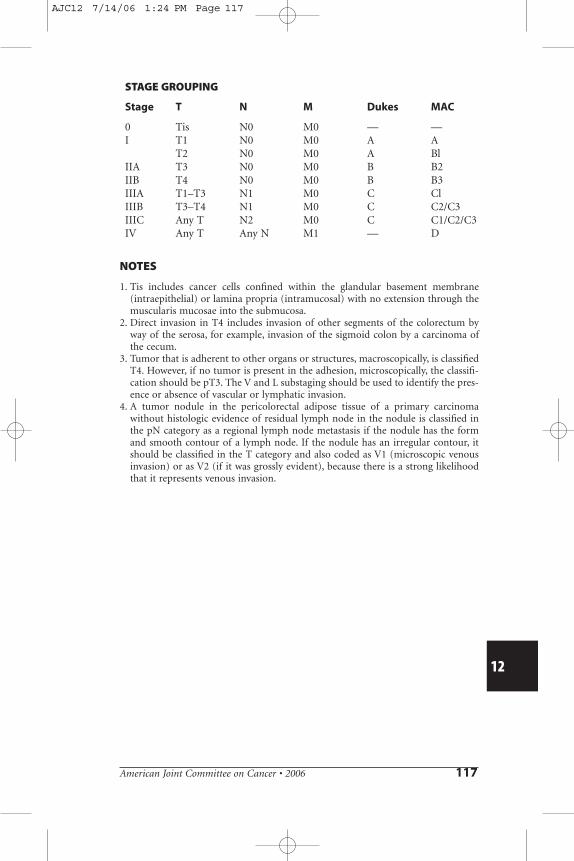
STAGE GROUPING
Stage T N M Dukes MAC
0 Tis N0 M0 — —I T1 N0 M0 A A
T2 N0 M0 A BlIIA T3 N0 M0 B B2IIB T4 N0 M0 B B3IIIA T1–T3 N1 M0 C ClIIIB T3–T4 N1 M0 C C2/C3IIIC Any T N2 M0 C C1/C2/C3IV Any T Any N M1 — D
NOTES
1. Tis includes cancer cells confined within the glandular basement membrane(intraepithelial) or lamina propria (intramucosal) with no extension through themuscularis mucosae into the submucosa.
2. Direct invasion in T4 includes invasion of other segments of the colorectum byway of the serosa, for example, invasion of the sigmoid colon by a carcinoma ofthe cecum.
3. Tumor that is adherent to other organs or structures, macroscopically, is classifiedT4. However, if no tumor is present in the adhesion, microscopically, the classifi-cation should be pT3. The V and L substaging should be used to identify the pres-ence or absence of vascular or lymphatic invasion.
4. A tumor nodule in the pericolorectal adipose tissue of a primary carcinomawithout histologic evidence of residual lymph node in the nodule is classified inthe pN category as a regional lymph node metastasis if the nodule has the formand smooth contour of a lymph node. If the nodule has an irregular contour, itshould be classified in the T category and also coded as V1 (microscopic venousinvasion) or as V2 (if it was grossly evident), because there is a strong likelihoodthat it represents venous invasion.
12
AJC12 7/14/06 1:24 PM Page 117

AJC12 7/14/06 1:24 PM Page 118