Colon

of 10
-
Upload
saadah-munawaroh-hd -
Category
Documents
-
view
215 -
download
0
description
Colon
Transcript of Colon
-
Th e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;8 nejm.org february 23, 2012 697
original article
Colonoscopy versus Fecal Immunochemical Testing in Colorectal-Cancer Screening
Enrique Quintero, M.D., Ph.D., Antoni Castells, M.D., Ph.D., Luis Bujanda, M.D., Ph.D., Joaqun Cubiella, M.D., Ph.D., Dolores Salas, M.D.,
ngel Lanas, M.D., Ph.D., Montserrat Andreu, M.D., Ph.D., Fernando Carballo, M.D., Ph.D., Juan Diego Morillas, M.D., Ph.D.,
Cristina Hernndez, B.Sc., Rodrigo Jover, M.D., Ph.D., Isabel Montalvo, M.D., Ph.D., Juan Arenas, M.D., Ph.D., Eva Laredo, R.N., Vicent Hernndez, M.D., Ph.D.,
Felipe Iglesias, R.N., Estela Cid, R.N., Raquel Zubizarreta, M.D., Teresa Sala, M.D., Marta Ponce, M.D., Mercedes Andrs, M.D., Gloria Teruel, M.D., Antonio Peris, M.D.,
Mara-Pilar Roncales, R.N., Mnica Polo-Toms, M.D., Ph.D., Xavier Bessa, M.D., Ph.D., Olga Ferrer-Armengou, R.N., Jaume Grau, M.D.,
Anna Serradesanferm, R.N., Akiko Ono, M.D., Jos Cruzado, M.D., Francisco Prez-Riquelme, M.D., Inmaculada Alonso-Abreu, M.D., Mariola de la Vega-Prieto, M.D., Juana Maria Reyes-Melian, M.D.,
Guillermo Cacho, M.D., Jos Daz-Tasende, M.D., Alberto Herreros-de-Tejada, M.D., Carmen Poves, M.D., Cecilio Santander, M.D., and Andrs Gonzlez-Navarro, M.D.,
for the COLONPREV Study Investigators*
The authors affiliations are listed in the Appendix. Address reprint requests to Dr. Castells at the Department of Gastroen-terology, Hospital Clnic, Villarroel 170, 08036 Barcelona, Spain, or at [email protected]; or to Dr. Quintero at the De-partment of Gastroenterology, Hospital Universitario de Canarias, Ctra. Ofra S/N Cuesta, 38320 La Laguna, Tenerife, Spain, or at [email protected].
Drs. Quintero and Castells contributed equally to this article.
*The investigators in the COLONPREV study are listed in the Supplementary Appendix, available at NEJM.org.
N Engl J Med 2012;366:697-706.Copyright 2012 Massachusetts Medical Society.
A bs tr ac t
BackgroundColonoscopy and fecal immunochemical testing (FIT) are accepted strategies for colorectal-cancer screening in the average-risk population.
MethodsIn this randomized, controlled trial involving asymptomatic adults 50 to 69 years of age, we compared one-time colonoscopy in 26,703 subjects with FIT every 2 years in 26,599 subjects. The primary outcome was the rate of death from colorectal cancer at 10 years. This interim report describes rates of participation, diagnostic findings, and occurrence of major complications at completion of the baseline screening. Study outcomes were analyzed in both intention-to-screen and as-screened populations.
ResultsThe rate of participation was higher in the FIT group than in the colonoscopy group (34.2% vs. 24.6%, P
-
Th e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;8 nejm.org february 23, 2012698
Colorectal cancer is the third most common cancer worldwide and the second leading cause of cancer-related deaths.1 Several studies have shown that colorectal-cancer screening is effective2-5 and cost-effective6 in the average-risk population.
Recommended strategies for colorectal-cancer screening fall into two broad categories: stool tests (occult blood and exfoliated DNA tests) and struc-tural examinations (flexible sigmoidoscopy, colo-noscopy, and computed tomographic colonogra-phy). Stool tests primarily detect cancer, and structural examinations detect both cancer and premalignant lesions.2 Stool tests for occult blood (guaiac testing and fecal immunochemical test-ing [FIT]) are predominantly used in Europe and Australia, whereas colonoscopy is the predomi-nant screening method in the United States.
Colonoscopy is considered the most accurate test for early detection and prevention of colorectal cancer. Although data from randomized studies evaluating the effect of colonoscopy on the rate of death from colorectal cancer are lacking, the pro-cedure is recommended as a first-line screening test on the basis of indirect data and observational studies. Population-based casecontrol studies have suggested that colonoscopy markedly reduces the risk of colorectal cancer7,8 and death.9 Recent evidence suggests that patients with no abnor-malities on a previous colonoscopy have a mark-edly reduced risk of colorectal cancer.8,10,11 In a cohort of average-risk subjects, the use of screen-ing colonoscopy was associated with a reduction in the incidence of colorectal cancer of 67% and a reduction in the rate of death of 65%.12 Cohort studies involving patients with adenomas have sug-gested that polypectomy can prevent approximate-ly 80% of colorectal cancers.13,14
Comparative studies have shown that the semi-quantitative FIT is more accurate than the guaiac test for the detection of colorectal cancer and ad-vanced adenomas,15-19 and this new test is now recommended as the first-choice fecal occult blood test in colorectal-cancer screening. Although FIT is less effective for neoplastic detection than colo-noscopy or sigmoidoscopy, evidence suggests that it may be better accepted,20,21 and higher accep-tance may counteract its lower detection capacity. It has been suggested that FIT may be more effec-tive and less costly than other screening strate-gies. We conducted a randomized, controlled trial to compare semiquantitative FIT with colonos-
copy. We hypothesized that FIT screening every 2 years would be noninferior to one-time colonosco-py with respect to a reduction in mortality related to colorectal cancer among average-risk subjects. This interim report describes rates of participation, diagnostic findings, and the occurrence of major complications at the completion of the baseline screening.
Me thods
Study DesignWe conducted this randomized, controlled, nonin-feriority trial in eight Spanish regions (Aragn, Basque Country, Canarias, Catalonia, Galicia, Ma-drid, Murcia, and Valencia) with the participation of 15 tertiary care hospitals. The study was designed to assess the efficacy of one-time colonoscopy and biennial FIT for reducing the rate of death from colorectal cancer at 10 years (primary trial out-come). The study started in November 2008 with an informative nationwide campaign.22 The recruit-ment period was initiated in June 2009, and the first round finished in June 2011. Ten-year follow-up will be completed in 2021.
The study protocol (available with the full text of this article at NEJM.org) was approved by the ethics committee at each hospital, and all subjects provided written informed consent.
Study PopulationAsymptomatic men and women between the ages of 50 and 69 years were eligible for enrollment. Exclusion criteria, which were ascertained after randomization by means of a questionnaire at the local screening office, included a personal history of colorectal cancer, adenoma, or inflammatory bowel disease; a family history of hereditary or familial colorectal cancer (i.e., 2 first-degree rel-atives with colorectal cancer or 1 in whom the dis-ease was diagnosed before the age of 60 years)23,24; a severe coexisting illness; and previous colecto-my. Subjects were also temporarily excluded if they had undergone fecal occult blood testing in the previous 2 years or sigmoidoscopy or colo-noscopy within the previous 5 years or if they had symptoms requiring additional workup. The subjects with previous screening tests became eligible when sufficient time had elapsed since the tests,2 and those with symptoms became eli-gible if the results of the clinical workup were negative.
The New England Journal of Medicine Downloaded from nejm.org at INSERM DISC DOC on November 2, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
-
Colonoscopy vs. Fecal Immunochemical Testing
n engl j med 366;8 nejm.org february 23, 2012 699
Randomization
Subjects were identified through each Community Health Registry, sorted according to household, and stratified according to age (in 5-year age groups) and sex. Households were randomly assigned in a 1:1 ratio to undergo either one-time colonoscopy or biennial FIT. Randomization was performed be-fore invitation with the use of a computer-generated allocation algorithm on the basis of a randomized-blocks method. Subjects were sent a preinvitation letter containing information on colorectal-cancer screening and the rationale for the study. Two weeks later, an invitation letter was sent indicating the subjects study-group assignment. Two addi-tional, reminder letters were mailed 3 and 6 months after the invitation to subjects who did not respond to the first mailed invitation. Subjects who agreed to participate in the study received an appointment at the local screening office, where they completed the questionnaire. The study design allowed for crossover between the two study groups.
Study InterventionsAmong patients undergoing colonoscopy, bowel cleansing and sedation were performed as de-scribed previously.25 All colonoscopies were per-formed by experienced endoscopists (those who had performed >200 colonoscopies per year).26 Pol-yps were categorized as non-neoplastic or neoplas-tic. Adenomas measuring 10 mm or more in diam-eter, with villous architecture, high-grade dysplasia, or intramucosal carcinoma, were classified as ad-vanced adenomas. Invasive cancer was considered to be present when malignant cells were observed beyond the muscularis mucosae. Advanced neo-plasm was defined as advanced adenoma or inva-sive cancer. Tumor staging, performed according to the classification system of the American Joint Committee on Cancer,27 was based on the most advanced lesion.
The FIT strategy consisted of analysis of a single stool sample with the use of the automated semi-quantitative OC-Sensor (Eiken Chemical) without specific restrictions on diet or medication use. Samples were processed as described previously28 at each regional hospital. Subjects who were found to have a hemoglobin level of 75 ng per milliliter or more were invited to undergo colonoscopy.
Details regarding quality indicators for colonos-copy are provided in the study protocol and in Ta-ble 1 in the Supplementary Appendix, available at NEJM.org.
Study Oversight
Palex Medical and Biogen Diagnstica donated sup-plies and automated fecal occult-blood analyzers used for FIT but provided no other support for the study. The companies were not involved in the de-sign of the study, in the analysis or interpretation of the data, or in the preparation of the manuscript.
Statistical AnalysisThis study was based on the assumption that screening average-risk subjects by means of bien-nial FIT would not be inferior to one-time colonos-copy with respect to the rate of death from colorec-tal cancer at 10 years. The calculations were based on an overall compliance rate of 30% and a crude 10-year rate of death from colorectal cancer of 6.96%.29 Therefore, assuming a crude 10-year rate of death from colorectal cancer of 1.74% among subjects undergoing colonoscopy (a 75% reduction) and of 3.41% among those screened by means of FIT (a 51% reduction) and accepting a noninferi-ority condition if the absolute difference was below 1.6 percentage points, we determined that a sample of 55,498 subjects (27,749 in each study group) would provide a power of 80%. A P value of less than 0.025 was considered to indicate statistical significance with the use of a one-sided test of proportions.30
We assessed study outcomes in both intention-to-screen and as-screened analyses. In the latter analysis, the detection rate was calculated as the number of subjects with true positive results di-vided by the number of subjects who actually un-derwent testing. The diagnostic yield was the number of subjects with true positive results divided by the number of eligible subjects in the intention-to-screen analysis. Subjects were exclud-ed from the intention-to-screen analysis if they at-tended the screening office visit and met one or more exclusion criteria. Subjects who did not at-tend the screening office visit and thus did not provide information about exclusion criteria were classified as eligible and were included in the intention-to-screen analysis. Definitions of other outcomes are provided in the study protocol. Be-tween-group differences in rates of participation, diagnostic yield, detection, and complications were established by logistic-regression analysis, with adjustment for age, sex, and participating center, and are reported as odds ratios with 95% confi-dence intervals. All analyses were performed with the use of SPSS statistical software, version 15.0.
The New England Journal of Medicine Downloaded from nejm.org at INSERM DISC DOC on November 2, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
-
Th e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;8 nejm.org february 23, 2012700
R esult s
Study PopulationOverall, 57,404 subjects were randomly assigned to undergo either colonoscopy or FIT. Of these sub-jects, 1970 could not be contacted and 2132 were excluded either permanently (1.7% in the colonos-copy group and 1.3% in the FIT group, P = 0.20) or temporarily (2.2% in the colonoscopy group and 2.2% in the FIT group, P = 0.11) (Fig. 1). The eligible population consisted of 26,703 subjects in the colo-noscopy group and 26,599 in the FIT group. The two groups were almost identical regarding both mean (SD) age (59.25.5 years in the colonoscopy group and 59.35.6 years in the FIT group, P = 0.35) and the proportion of subjects who were women (53.5% in the colonoscopy group and 54.3% in the FIT group, P = 0.25).
ParticipationAmong subjects who were assigned to undergo colonoscopy, 5649 subjects accepted the pro-posed strategy, whereas 1706 requested to be screened by means of FIT (Fig. 1). Of the 5649 subjects who agreed to undergo colonoscopy, 4953 actually did so, and 1628 underwent FIT, for a participation rate of 24.6%, according to the intention-to-screen analysis (average age, 59.15.5 years; proportion of subjects who were women, 53.4%). Among subjects who were assigned to undergo FIT, 9353 subjects accepted the pro-posed strategy, whereas 117 asked to be screened by colonoscopy. A total of 8983 subjects under-went FIT, and 106 underwent colonoscopy, for an overall participation rate of 34.2% (average age, 59.35.6 years; proportion of subjects who were women, 54.4%). Therefore, there were differenc-es between study groups regarding both the rate of participation (odds ratio in the colonoscopy group, 0.63; 95% confidence interval [CI], 0.60 to 0.65; P
-
Colonoscopy vs. Fecal Immunochemical Testing
n engl j med 366;8 nejm.org february 23, 2012 701
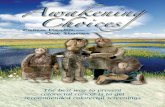
57,404 Patients underwent randomization
28,708 Were assignedto colonoscopy 28,696 Were assigned to FIT
916 Were not contacted 1054 Were not contacted
7368 Attended screening office 9512 Attended screening office
5649 Accepted colonoscopy
4953 Completed colonoscopy
92 Had positive results on FIT
76 Completed colonoscopy
675 Had positive results on FIT
587 Completed colonoscopy
Results:4 CRC
32 Advanced adenomas9 Nonadvanced adenomas
Results:26 CRC
482 Advanced adenomas1100 Nonadvanced adenomas
Results:32 CRC
220 Advanced adenomas103 Nonadvanced adenomas
Results:1 CRC
11 Advanced adenomas16 Nonadvanced adenomas
27,792 Were invited to undergocolonoscopy
27,642 Were invited to undergoFIT
472 Were permanently excluded206 Had previous CRC or adenoma56 Had inflammatory bowel disease
147 Had family history of CRC or polyposis63 Had severe coexisting illness
617 Were temporarily excluded60 Had colorectal symptoms
557 Had previous screening test
431 Were permanently excluded170 Had previous CRC or adenoma60 Had inflammatory bowel disease
177 Had family history of CRC or polyposis24 Had severe coexisting illness
612 Were temporarily excluded61 Had colorectal symptoms
551 Had previous screening test
26,703 Were eligiblefor colonoscopy 26,599 Were eligible for FIT
117 Requested colonoscopy
106 Completed colonoscopy
1706 Requested FIT
1628 Completed FIT
9353 Accepted FIT
8983 Completed FIT
Figure 1. Enrollment and Outcomes.
A total of 1970 subjects were not contacted after being randomly assigned to undergo either colonoscopy or fecal immunochemical test-ing (FIT) because they had died or had an inaccurate mailing address, which resulted in the return of the invitation letters. Criteria for permanent exclusion were a personal history of inflammatory bowel disease, colorectal polyps, or colorectal cancer (CRC) and a family history of CRC or polyposis syndromes. Temporary exclusion criteria were the presence of symptoms suggestive of colorectal disease and occult blood testing within the previous 2 years or sigmoidoscopy or colonoscopy within the previous 5 years. The subjects with pre-vious screening tests became eligible when sufficient time had elapsed since the tests, and those with symptoms became eligible if the results of the clinical workup were negative.
The New England Journal of Medicine Downloaded from nejm.org at INSERM DISC DOC on November 2, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
-
Th e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;8 nejm.org february 23, 2012702
the numbers of subjects who needed to undergo colonoscopy to find one colorectal cancer were 191 in the colonoscopy group and 18 in the FIT group; to find any advanced neoplasm, the num-bers were 10 and 2, respectively (Table 3 in the Supplementary Appendix).
ComplicationsMajor complications occurred in 24 subjects (0.5%) in the colonoscopy group (12 subjects with bleed-ing, 10 subjects with hypotension or bradycardia, 1 subject with perforation, and 1 subject with de-saturation) and in 10 subjects (0.1%) in the FIT group (8 subjects with bleeding and 2 subjects with hypotension or bradycardia, all of whom required colonoscopy because of a positive result on FIT). Accordingly, the complication rate was higher in the colonoscopy group than in the FIT group (odds ratio, 4.81; 95% CI, 2.26 to 10.20; P
-
Colonoscopy vs. Fecal Immunochemical Testing
n engl j med 366;8 nejm.org february 23, 2012 703
is that one-time screening with FIT was very simi-lar to one-time colonoscopy with respect to the rate of detection of colorectal cancer, and there was no significant difference in the stage of tumors de-tected by the two strategies. Additional cases of colorectal cancer might be detected during ongo-ing biennial FIT screening, and this could lead to an increased rate of cancer detection and a de-creased rate of death in this group. On the other hand, more tumors might have been prevented in the colonoscopy group owing to the larger number of adenomas detected and removed, in comparison with the FIT group.
The higher detection rate and diagnostic yield of colonoscopy with respect to premalignant le-sions also warrant comment. First, since advanced adenomas are usually considered a surrogate marker for colorectal cancer,32,33 the superiority of colonoscopy for detecting such lesions should be
considered a potential advantage of this strategy in terms of reducing not only the rate of death from colorectal cancer but also the incidence of dis-ease.34 However, this effect was diminished in our study by the lower participation rate in the colo-noscopy group than in the FIT group. Moreover, the first round of FIT screening detected about half the number of advanced adenomas that were de-tected by colonoscopy. The lower participation rate in the colonoscopy group and the recurrent nature of FIT screening may reduce the apparent advan-tage of colonoscopy. On the other hand, the re-markably high detection rate with colonoscopy for patients with nonadvanced adenomas is more dif-ficult to interpret. Most of these lesions correspond to low-risk adenomas, with a natural history that is more unpredictable but unquestionably less prone to progression to colorectal cancer than the natural history of advanced adenoma.34,35 Indeed,
Table 2. Diagnostic Yield of Colonoscopy and Fecal Immunochemical Testing (FIT), According to the Intention-to-Screen Analysis and the Location of the Colorectal Lesion.*
Colorectal LesionColonoscopy(N = 26,703)
FIT(N = 26,599)
Odds Ratio(95% CI) P Value
Subjects Rate Subjects Rate
no. % no. %
Cancer
Proximal 6
-
Th e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;8 nejm.org february 23, 2012704
recent European guidelines for quality assurance in colorectal-cancer screening consider patients with only one or two small adenomas (
-
Colonoscopy vs. Fecal Immunochemical Testing
n engl j med 366;8 nejm.org february 23, 2012 705
AppendixThe authors affiliations are as follows: the Department of Gastroenterology, Hospital Universitario de Canarias, Tenerife (E.Q., I.A.-A.); the Department of Gastroenterology, Hospital Clnic, Centro de Investigacin Biomdica en Red de Enfermedades Hepticas y Digestivas (CIBERehd), Institut dIvestigacions Biomediques August Pi i Sunyer (A.C.), the Department of Gastroenterology, Parc de Salut Mar, Institut Municipal dInvestigaci Mdica (IMIM), Pompeu Fabra University (M. Andreu, X.B., O.F.-A.), the Department of Epidemiology and Evaluation, Parc de Salut Mar, IMIM (C.H.), and Unitat dAvaluaci, Suport i Preventiva, Hospital Clnic (J.G., A.S.) all in Barcelona; the Department of Gastroenterology, Donostia Hospital, CIBERehd, University of Basque Country (L.B.), the Department of Gastroen-terology, Instituto Oncolgico, Obra Social Kutxa (I.M.), and the Department of Gastroenterology, Policlinica Gipuzkoa, CIBERehd (J.A.) all in San Sebastin; the Department of Gastroenterology, Complexo Hospitalario Universitario de Ourense, Ourense (J.C., E.C.); the Colorectal Cancer Screening Program, Direccin General de Salud Pblica, Conselleria de Sanitat (D.S., T.S., M. Andres, G.T.), and the Department of Gastroenterology, Hospital Universitario La Fe (M.P.) both in Valencia; the Department of Gastroen-terology, University of Zaragoza, IIS Aragn, CIBERehd, Zaragoza (A.L., M.-P.R., M.P.-T.); Unidad de Gestin Clnica de Digestivo, Hospital Universitario Virgen de la Arrixaca (F.C., A.O.), the Colorectal Cancer Prevention Program of the Regin de Murcia, Servicio Murciano de Salud (J.C.), and the Colorectal Cancer Prevention Program of the Regin de Murcia, Direccin General de Salud Pblica, Consejera de Sanidad y Poltica Social (F.P.-R.) all in Murcia; the Department of Gastroenterology, Hospital Clnico San Carlos (J.D.M., C.P.), the Department of Gastroenterology, Hospital Fundacin Alcorcn (G.C.), the Department of Gastroenterology, Hospital 12 de Octubre (J.D.-T.), the Department of Gastroenterology, Hospital de la Princesa, Instituto de Investigacin Sanitaria Princesa (IP), and CIBERehd (C.S.), and the Regional Office for Oncology Coordination, Consejera de Sanidad (A.G.-N.) all in Madrid; the Gas-troenterology Unit, Hospital General Universitario de Alicante, Alicante (R.J.); the Department of Gastroenterology, Lasarte-Oria Health Center, Osakidetza-Basque Health Service, Guipzcoa (E.L.); the Department of Gastroenterology, Complexo Hospitalario Universitario de Vigo, Vigo (V.H., F.I.); Direccin Xeral de Innovacin e Xestin da Sade Pblica, Conselleria de Sanidade, Xunta de Galicia (R.Z.); the Department of Gastroenterology, Consorcio Hospitalario de Castelln, Castelln (A.P.); the Colorectal Cancer Screening Program of the Comunidad de Canarias, Servicio Canario de la Salud (M.V.-P., J.M.R.-M.); and the Department of Gastroenterology, Hospital Puerta de Hierro, Majadahonda (A.H.-T.) all in Spain.
References1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of world-wide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010;127:2893-917.2. Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guide-line from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radi-ology. Gastroenterology 2008;134:1570-95.3. Mandel JS, Church TR, Bond JH, et al. The effect of fecal occult-blood screening on the incidence of colorectal cancer. N Engl J Med 2000;343:1603-7.4. Hewitson P, Glasziou P, Watson E, Towler B, Irwig L. Cochrane systematic review of colorectal cancer screening us-ing the fecal occult blood test (Hemoc-cult): an update. Am J Gastroenterol 2008; 103:1541-9.5. Atkin WS, Edwards R, Kralj-Hans I, et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal can-cer: a multicentre randomised controlled trial. Lancet 2010;375:1624-33.6. Heitman SJ, Hilsden RJ, Au F, Dowden S, Manns BJ. Colorectal cancer screening for average-risk North Americans: an eco-nomic evaluation. PLoS Med 2010;7(11): 1000370.7. Brenner H, Chang-Claude J, Seiler CM, Rickert A, Hoffmeister M. Protection from colorectal cancer after colonoscopy: a population-based, case-control study. Ann Intern Med 2011;154:22-30.8. Brenner H, Haug U, Arndt V, Stegma-ier C, Altenhofen L, Hoffmeister M. Low risk of colorectal cancer and advanced ad-
enomas more than 10 years after negative colonoscopy. Gastroenterology 2010;138: 870-6.9. Baxter NN, Goldwasser MA, Paszat LF, Saskin R, Urbach DR, Rabeneck L. As-sociation of colonoscopy and death from colorectal cancer. Ann Intern Med 2009; 150:1-8.10. Brenner H, Chang-Claude J, Seiler CM, Hoffmeister M. Long-term risk of colorectal cancer after negative colonos-copy. J Clin Oncol 2011;29:3761-7.11. Imperiale TF, Glowinski EA, Lin-Cooper C, Larkin GN, Rogge JD, Ransohoff DF. Five-year risk of colorectal neoplasia after negative screening colonoscopy. N Engl J Med 2008;359:1218-24. [Erratum, N Engl J Med 2009;361:2004.]12. Kahi CJ, Imperiale TF, Juliar BE, Rex DK. Effect of screening colonoscopy on colorectal cancer incidence and mortality. Clin Gastroenterol Hepatol 2009;7:770-5, quiz 711.13. Citarda F, Tomaselli G, Capocaccia R, Barcherini S, Crespi M. Efficacy in stan-dard clinical practice of colonoscopic pol-ypectomy in reducing colorectal cancer incidence. Gut 2001;48:812-5.14. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colono-scopic polypectomy. N Engl J Med 1993; 329:1977-81.15. Dancourt V, Lejeune C, Lepage C, Gailliard MC, Meny B, Faivre J. Immuno-chemical faecal occult blood tests are su-perior to guaiac-based tests for the detec-tion of colorectal neoplasms. Eur J Cancer 2008;44:2254-8.16. Hol L, Wilschut JA, van Ballegooijen M, et al. Screening for colorectal cancer:
random comparison of guaiac and immu-nochemical faecal occult blood testing at different cut-off levels. Br J Cancer 2009; 100:1103-10.17. Parra-Blanco A, Gimeno-Garca AZ, Quintero E, et al. Diagnostic accuracy of immunochemical versus guaiac faecal oc-cult blood tests for colorectal cancer screening. J Gastroenterol 2010;45:703-12.18. van Rossum LG, van Rijn AF, Laheij RJ, et al. Random comparison of guaiac and immunochemical fecal occult blood tests for colorectal cancer in a screening population. Gastroenterology 2008;135: 82-90.19. Levi Z, Birkenfeld S, Vilkin A, et al. A higher detection rate for colorectal cancer and advanced adenomatous polyp for screening with immunochemical fecal occult blood test than guaiac fecal occult blood test, despite lower compliance rate: a prospective, controlled, feasibility study. Int J Cancer 2011;128:2415-24.20. Hol L, van Leerdam ME, van Balle-gooijen M, et al. Screening for colorectal cancer: randomised trial comparing guaiac-based and immunochemical faecal occult blood testing and flexible sigmoidoscopy. Gut 2010;59:62-8.21. Segnan N, Senore C, Andreoni B, et al. Comparing attendance and detection rate of colonoscopy with sigmoidoscopy and FIT for colorectal cancer screening. Gastroenterology 2007;132:2304-12.22. Andreu Garca M, Marzo M, Mascort J, et al. Prevention of colorectal cancer. Gastroenterol Hepatol 2009;32:137-9. (In Spanish.)23. Castells A, Castellv-Bel S, Balaguer F. Concepts in familial colorectal cancer:
The New England Journal of Medicine Downloaded from nejm.org at INSERM DISC DOC on November 2, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.
-
n engl j med 366;8 nejm.org february 23, 2012706
Colonoscopy vs. Fecal Immunochemical Testing
where do we stand and what is the future? Gastroenterology 2009;137:404-9.24. Piol V, Castells A, Andreu M, et al. Accuracy of revised Bethesda guidelines, microsatellite instability, and immuno-histochemistry for the identification of patients with hereditary nonpolyposis colorectal cancer. JAMA 2005;293:1986-94.25. Parra-Blanco A, Nicolas-Perez D, Gi-meno-Garcia A, et al. The timing of bowel preparation before colonoscopy deter-mines the quality of cleansing, and is a significant factor contributing to the de-tection of flat lesions: a randomized study. World J Gastroenterol 2006;12:6161-6.26. Gua de prctica clnica de calidad en la colonoscopia de cribado del cncer color-rectal. Asociacin Espaola de Gastroen-terologa y Sociedad Espaola de Endo-scopia Digestiva, 2011 (http://www.aegastro .es/docs/cribado_colon.pdf).27. OConnell JB, Maggard MA, Ko CY. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J Natl Cancer Inst 2004;96:1420-5.
28. Vilkin A, Rozen P, Levi Z, et al. Perfor-mance characteristics and evaluation of an automated-developed and quantitative, immunochemical, fecal occult blood screening test. Am J Gastroenterol 2005; 100:2519-25.29. Scholefield JH, Moss SM. Faecal oc-cult blood screening for colorectal cancer. J Med Screen 2002;9:54-5.30. Hollis S, Campbell F. What is meant by intention to treat analysis? Survey of published randomised controlled trials. BMJ 1999;319:670-4.31. Lieberman D. A call to action mea-suring the quality of colonoscopy. N Engl J Med 2006;355:2588-9.32. Arber N, Eagle CJ, Spicak J, et al. Cele-coxib for the prevention of colorectal ad-enomatous polyps. N Engl J Med 2006; 355:885-95.33. Baron JA, Cole BF, Sandler RS, et al. A randomized trial of aspirin to prevent colorectal adenomas. N Engl J Med 2003; 348:891-9.34. Lieberman DA, Weiss DG, Bond JH, Ahnen DJ, Garewal H, Chejfec G. Use of
colonoscopy to screen asymptomatic adults for colorectal cancer. N Engl J Med 2000; 343:162-8. [Erratum, N Engl J Med 2000; 343:1204.]35. Lieberman DA, Weiss DG, Harford WV, et al. Five-year colon surveillance after screening colonoscopy. Gastroenterology 2007;133:1077-85.36. European guidelines for quality as-surance in colorectal cancer screening and diagnosis. Brussels: European Commis-sion, 2011 (http://bookshop.europa.eu/ is-bin/INTERSHOP.enfinity/WFS/ EU-Bookshop-Site/en_GB/-/EUR/ ViewPublication-Start?PublicationKey=ND3210390).37. Lieberman D. Colon cancer screening and surveillance controversies. Curr Opin Gastroenterol 2009;25:422-7.38. Haug U, Kuntz KM, Knudsen AB, Hundt S, Brenner H. Sensitivity of immu-nochemical faecal occult blood testing for detecting left- vs right-sided colorectal neoplasia. Br J Cancer 2011;104:1779-85.Copyright 2012 Massachusetts Medical Society.
AN NEJM APP FOR iPHONEThe NEJM Image Challenge app brings a popular online feature to the smartphone. Optimized for viewing on the iPhone and iPod Touch, the Image Challenge app lets
you test your diagnostic skills anytime, anywhere. The Image Challenge app randomly selects from 300 challenging clinical photos published in NEJM, with a new image added each week. View an image, choose your answer,
get immediate feedback, and see how others answered. The Image Challenge app is available at the iTunes App Store.
The New England Journal of Medicine Downloaded from nejm.org at INSERM DISC DOC on November 2, 2012. For personal use only. No other uses without permission.
Copyright 2012 Massachusetts Medical Society. All rights reserved.