
Colette Rogers (Public Health Agency NI) & Fenton Howell (Department of Health, Ireland)
17
Tobacco Control and Harm Reduction? Dr Fenton Howell, Department of Health, Ireland Colette Rogers, Public Health Agency NI 1
-
Upload
institute-of-public-health-in-ireland -
Category
Healthcare
-
view
23 -
download
0
Transcript of Colette Rogers (Public Health Agency NI) & Fenton Howell (Department of Health, Ireland)

Tobacco Control and Harm Reduction?
Dr Fenton Howell, Department of Health, Ireland
Colette Rogers, Public Health Agency NI
1

Workshop
• Current Practice • Brief outline of issues around harm reduction and
public health interventions• Group work
– Do harm reduction strategies have a place in tobacco control?
– If yes, what form should it take, what are the benefits/risks?
– If no, what are the benefits/risks? what other alternatives are there to support current supply and demand reduction strategies in tobacco control?
2

3
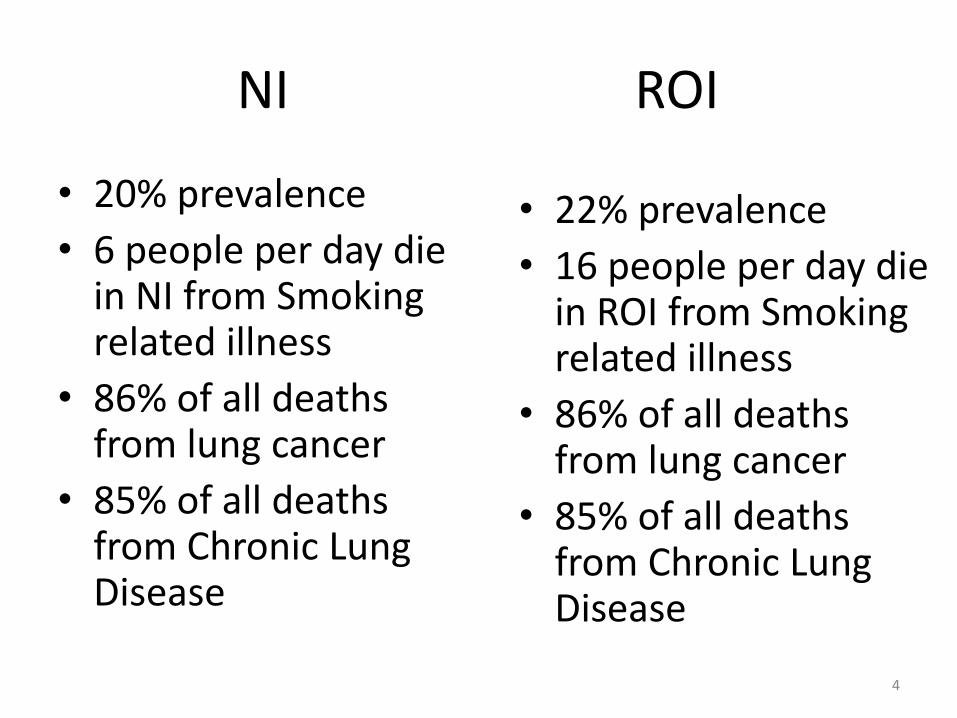
NI ROI
• 20% prevalence
• 6 people per day die in NI from Smoking related illness
• 86% of all deaths from lung cancer
• 85% of all deaths from Chronic Lung Disease
• 22% prevalence
• 16 people per day die in ROI from Smoking related illness
• 86% of all deaths from lung cancer
• 85% of all deaths from Chronic Lung Disease
4

What is harm reduction?
• Harm reduction is a pragmatic approach (public health policies, interventions or programs) designed to reduce the harmful consequences associated with substance use and high-risk activities.
• Harm reduction cuts across the spectrum from safer use to managed use to abstinence.
• Primary goal of most harm reduction strategies is to meet individuals “where they are at”
5

Examples of harm reduction
• Illicit drugs: – Needle syringe programmes
– Opiod substitution – e.g. Methadone
– Safe injecting facilities
– Overdose –prevention programmes- naloxone
• New national strategy: Reducing Harm, Supporting Recovery – a health-led response to drug and alcohol use in Ireland 2017-2025
6

Examples of harm reduction
• HIV/AIDS/STI:– Condoms– Safe sex
• Unwanted Pregnancy: – Contraception– Emergency contraception
• Road traffic accidents– Seatbelts, airbags, crumple zones etc
• Safe participation in sport:– Helmets- cycling, hurling, cricket, hockey etc– Life vests – water based activities
7

Why harm reduction and tobacco control and why now?
• WHO Framework Convention on Tobacco Control (WHO FCTC) defines tobacco control as: a range of supply, demand and harm reduction strategies that aim to improve the health of the population by eliminating or reducing their consumption of tobacco products and exposure to tobacco smoke
8

Why harm reduction and tobacco control and why now?
• Magnitude of the risk
– One in every two smokers will die from a tobacco related disease
• Worldwide
– 1 Billion smokers
– Spend $700 billion annually on cigs
– 6 million dying annually
– Expected to get worse
9

Why harm reduction and tobacco control and why now?
• Tobacco Free Ireland Page 51:There is a requirement for alternative, less harmful forms of nicotine. Whilst there are smokers who are able to quit abruptly, either alone or by using current support mechanisms, there are others who are unable to. These people need an alternative measure of support to reduce the harm they experience from tobacco use. This can involve the use of alternative safer sources of nicotine while they reduce their tobacco consumption in preparation to quit.
10

Why harm reduction and tobacco control and why now?
Ten Year Tobacco Control Strategy for NI (pg.44)
Levels of tobacco addiction vary and some smokers, in spite of frequent and determined efforts to quit smoking, find it impossible to completely break the addiction. In such cases, harm reduction schemes can reduce the risks to health through the regular substitution with NRT products… The Department of Health will continue to keep this subject under review.
11

Why harm reduction and tobacco control and why now?
NICE Guideline – Stop Smoking Interventions and Services - Draft for Consultation Sept 17 (pg6)
Those who advise people on how to quit smoking should…
• Encourage them to seek help to quit smoking completely in the future
• Ask them to think about adopting a harm reduction approach (see NICE guideline on smoking: harm reduction)
12

Why harm reduction and tobacco control and why now?
• Changed landscape: newer and less harmful modes of nicotine now available;
• For years – combustible products only- dirty delivery systems: cigarettes, pipes etc
• Now there are safer alternatives (not safe):– Medicinal nicotine therapy– Oral smokeless tobacco (SNUS – Sweden)– Aerosolized nicotine delivery – without tobacco– Heat -not-burn tobacco products; aerosolised
nicotine.– Technological disruptions suggest more alternatives to
come. 13

Harm reduction and tobacco control
• Its controversial, not only in tobacco control
• Harm reduction v zero tolerance
• People on both sides are finding evidence that supports what they want to believe
• Previous “harm reduction” efforts were unsuccessful – light/low tar cigs
• Nicotine addicts:
– nothing about me, without me
14

Public health objectives
• Control/regulation should be proportionate to the real risks
• Manage those products with different risk profiles differently
• Avoid unintentional consequences: protecting the most harmful at the expense of the least harmful
15

Public health intervention ladderWhat policy choices will leads to fewer funerals in years to come?
Eliminate choice: ban completely
Restrict choice: remove unhealthy ingredients from food
Guide choice through disincentives: tax on sugary soft drinks
Guide choice through incentives: fiscal – Bike to work scheme
Guide choice by changing the default policy: Chips as the standard or , veg as the standard with chips as the option
Enable choice: build cycle lanes, offer help to quit, provide free fruit at schools
Provide information: inform and educate the public e.g 5 a day, 10,000 steps
Do nothing
16

Workshop
• Group work
– Do harm reduction strategies have a place in tobacco control?
– If yes, what form should it take, what are the benefits/risks?
– If no, what are the benefits/risks? what other alternatives are there to support current supply and demand reduction strategies in tobacco control?
17







![Chéri; roman [par] Colette (Colette Willy) · 2018-07-10 · loaeaiiion colette chÉri tioman paris ahthÈmt:favaiujk'ïc-,Éditeurs ih20,rijkdusaint-gotharu](https://static.fdocuments.us/doc/165x107/5e5445d984d0055bf466a4b1/chri-roman-par-colette-colette-willy-2018-07-10-loaeaiiion-colette-chri.jpg)










