Cold pressor thallium-201 myocardial scintigraphy in the diagnosis of coronary artery disease
5
Cold PressorThallium-201 Myocardial Scintigraphyin the Diagnosis of Coronary Artery Disease MASOOD AHMAD, MD, FRCP(C), JERZY P. DUBIEL, MD, and HELMUT HAIBACH, MD Thallium-201 myocardial scintigraphy was per- formed during cold pressor stimulation in 36 patients aged 37 to 69 years. Thirty-one patients had coro- nary artery disease and 5 patients did not, as con- firmed by coronary cineangiography. Thallium-20 1 (1.5 to 2 mCi) was injected at 30 seconds of the cold pressor stimulation. The product of systolic pressure X heart rate increased from a baseline of 77.4 f 16 (standard deviation [SD]) to 103.6 f 17 at 30 sec- onds of the cold pressor test (p <0.0005). Transient perfusion deficits developed in 24 of 31 patients with coronary artery disease (sensitivity 77%), and all 5 patients without coronary artery disease had normal scintigrams. The sensitivity in detecting coronary artery disease was 40% in patients with 1 vessel disease, 91% in patients with 2 vessel disease, and 100% in patients with 3 vessel dis- ease. Exercise electrocardiograms (available in 29 Thallium-201 myocardial scintigraphy with exercise has proved a valuable noninvasive technique in the evalu- ation of myocardial perfusion in patients with coronary artery disease.’ Many sick and debilitated patients, however, are unable to perform the exercise needed for the test, and some have symptoms that are not related to exercise. The cold pressor test results in a rapid in- crease in blood pressure and induces abnormalities in left ventricular function in patients with coronary artery disease.“J In the present study, cold pressor stimulation was examined for the first time as an alternative to the standard exercise stress test in the scintigraphic eval- uation of myocardial perfusion. From the University of Missouri Health Science Center, Columbia, Missouri, and the University of Texas Medical Branch, Galveston, Texas. Manuscript received October 28, 1981; revised manuscript received June 22, 1982, accepted June 25. Address for reprints: Masood Ahmad, MD, Division of Cardiology, The University of Texas Medical Branch, Galveston, Texas 77550. of 36 patients) were positive for ischemia in 16 of 24 patients with coronary artery disease and in 1 of 5 patients without coronary artery disease (sensi- tivity 75% and specificity <60%). Exercise thal- lium-201 scintigrams, obtained in 16 patients, were positive in 11 patients with coronary artery disease and positive cold pressor thallium-201 scintigrams. Five patients without coronary artery disease and with normal cold pressor thallium-201 scintigrams had normal exercise thallium-201 scintigrams. Coronary cineangiography performed during cold pressor stimulation in 6 patients who had positive cold pressor and exercise thallium-201 scintigrams did not show coronary spasm. Our data indicate that cold pressor thallium-201 scintigraphy offers promise as a noninvasive test in the diagnosis of coronary artery disease and may be used in patients in whom exercise testing is not feasible. Methods Patient population: The study group consisted of 36 pa- tients (aged 37 to 69 years) whose coronary anatomy had been studied by coronary angiography. The patients were selected from a population being evaluated for chest pain syndromes and for possible coronary artery bypass surgery. Typical an- gina pectoris, brought on by exertion and relieved by rest and nitrates, was present in 30 patients. Six patients presented with chest pain that was atypical either in location or in its relation to exertion and nitrates. The duration of symptoms ranged from 1 to 11 years. Thirty-one patients were taking nitrates for relief of chest pain. Five patients were being treated with propranolol(40 to 180 mg daily) and 4 patients were taking digoxin (0.25 mg daily) and diuretics at the time of the study. Five patients had evidence of previous myocar- dial infarction, transmural in 2 patients and nontransmural in 3. Seven patients had ventricular arrhythmias (premature ventricular contractions) and nonspecific ST-T wave changes. There was evidence of cardiomegaly in 3 patients. All patients underwent standard left heart catheterization, and coronary December 1982 The American Journal of CARDIOLOGY Volume 50 1253
-
Upload
masood-ahmad -
Category
Documents
-
view
212 -
download
0
Transcript of Cold pressor thallium-201 myocardial scintigraphy in the diagnosis of coronary artery disease

Cold Pressor Thallium-201 Myocardial Scintigraphy in the Diagnosis of Coronary Artery Disease
MASOOD AHMAD, MD, FRCP(C), JERZY P. DUBIEL, MD, and HELMUT HAIBACH, MD
Thallium-201 myocardial scintigraphy was per- formed during cold pressor stimulation in 36 patients aged 37 to 69 years. Thirty-one patients had coro- nary artery disease and 5 patients did not, as con- firmed by coronary cineangiography. Thallium-20 1 (1.5 to 2 mCi) was injected at 30 seconds of the cold pressor stimulation. The product of systolic pressure X heart rate increased from a baseline of 77.4 f 16 (standard deviation [SD]) to 103.6 f 17 at 30 sec- onds of the cold pressor test (p <0.0005). Transient perfusion deficits developed in 24 of 31 patients with coronary artery disease (sensitivity 77%), and all 5 patients without coronary artery disease had normal scintigrams. The sensitivity in detecting coronary artery disease was 40% in patients with 1 vessel disease, 91% in patients with 2 vessel disease, and 100% in patients with 3 vessel dis- ease. Exercise electrocardiograms (available in 29
Thallium-201 myocardial scintigraphy with exercise has proved a valuable noninvasive technique in the evalu- ation of myocardial perfusion in patients with coronary artery disease.’ Many sick and debilitated patients, however, are unable to perform the exercise needed for the test, and some have symptoms that are not related to exercise. The cold pressor test results in a rapid in- crease in blood pressure and induces abnormalities in left ventricular function in patients with coronary artery disease.“J In the present study, cold pressor stimulation was examined for the first time as an alternative to the standard exercise stress test in the scintigraphic eval- uation of myocardial perfusion.
From the University of Missouri Health Science Center, Columbia, Missouri, and the University of Texas Medical Branch, Galveston, Texas. Manuscript received October 28, 1981; revised manuscript received June 22, 1982, accepted June 25.
Address for reprints: Masood Ahmad, MD, Division of Cardiology, The University of Texas Medical Branch, Galveston, Texas 77550.
of 36 patients) were positive for ischemia in 16 of 24 patients with coronary artery disease and in 1 of 5 patients without coronary artery disease (sensi- tivity 75% and specificity <60%). Exercise thal- lium-201 scintigrams, obtained in 16 patients, were positive in 11 patients with coronary artery disease and positive cold pressor thallium-201 scintigrams. Five patients without coronary artery disease and with normal cold pressor thallium-201 scintigrams had normal exercise thallium-201 scintigrams. Coronary cineangiography performed during cold pressor stimulation in 6 patients who had positive cold pressor and exercise thallium-201 scintigrams did not show coronary spasm. Our data indicate that cold pressor thallium-201 scintigraphy offers promise as a noninvasive test in the diagnosis of coronary artery disease and may be used in patients in whom exercise testing is not feasible.
Methods
Patient population: The study group consisted of 36 pa- tients (aged 37 to 69 years) whose coronary anatomy had been studied by coronary angiography. The patients were selected from a population being evaluated for chest pain syndromes and for possible coronary artery bypass surgery. Typical an- gina pectoris, brought on by exertion and relieved by rest and nitrates, was present in 30 patients. Six patients presented with chest pain that was atypical either in location or in its relation to exertion and nitrates. The duration of symptoms ranged from 1 to 11 years. Thirty-one patients were taking nitrates for relief of chest pain. Five patients were being treated with propranolol(40 to 180 mg daily) and 4 patients were taking digoxin (0.25 mg daily) and diuretics at the time of the study. Five patients had evidence of previous myocar- dial infarction, transmural in 2 patients and nontransmural in 3. Seven patients had ventricular arrhythmias (premature ventricular contractions) and nonspecific ST-T wave changes. There was evidence of cardiomegaly in 3 patients. All patients underwent standard left heart catheterization, and coronary
December 1982 The American Journal of CARDIOLOGY Volume 50 1253

COLD PRESSOR THALLIUM-201 SCINTIGRAPHY-AHMAD ET AL
cineangiograms were obtained in multiple projections. Left ventricular and coronary cineangiograms were interpreted by a single experienced observer. Coronary artery disease was diagnosed when 250% luminal diameter narrowing was ob- served in at least 1 major coronary artery. The interpretation of coronary angiograms was based on the observer’s visual estimate of the degree of luminal narrowing. Thirty-one pa- tients had significant coronary artery disease. Triple vessel coronary artery disease was present in 10 patients, double vessel disease in 11 patients, and single vessel disease in 10 patients. In the remaining 5 patients, coronary angiograms were read as normal based on no disease in 3 patients and <50% luminal diameter narrowing of 1 of the major vessels in 2 patients. Greater than 50% narrowing of the left main cor- onary artery was present in 2 patients with triple vessel dis- ease. Seven patients with triple vessel disease had areas of ventricular wall motion abnormality, and small discrete left ventricular aneurysms were present in 2 of these 7 patients. Two patients with double vessel disease also had areas of left ventricular wall motion abnormality. The left ventricular ejection fraction of 5 patients (4 with triple vessel and 1 with double vessel disease) was depressed and ranged from 35 to 45%. The resting left ventricular end-diastolic pressure in these 5 patients was abnormally elevated. In 5 patients, the left ventricular ejection fraction was mildly depressed, ranging from 45 to 55%, and the remaining 26 patients had a normal resting ejection fraction.
Twenty-nine patients (24 with and 5 without coronary ar- tery disease) were able to complete a symptom-limited max- imal exercise stress test using Bruce’s4 multistage treadmill protocol. The patient’s heart rate, blood pressure, and elec- trocardiogram (modified Vs electrode) were monitored throughout the exercise. In 13 patients, the exercise stress test was carried out at the time of hospitalization for cardiac catheterization. In the remaining 16 the test had been per- formed for the evaluation of chest pain within the 6 months before hospitalization. Seven patients did not have an exercise stress test, either because of an unstable clinical state (4 pa- tients) or because of severe peripheral vascular disease (3 patients). All exercise stress test electrocardiograms were interpreted by a single experienced observer without knowl- edge of the patients’ angiographic or scintigraphic data. Ex- ercise stress test was interpreted as positive when >l mm S-T segment depression was observed in the exercise electrocar- diogram.
Cold pressor thallium-201 scintigraphy: All patients underwent thallium-201 myocardial scintigraphy after the cold pressor test. After the baseline electrocardiogram and blood pressure were recorded, the patient’s one hand was suddenly immersed up to the level of the styloid process in a bucket of ice water (temperature 0 to 2’C) for 2 to 3 minutes. The electrocardiogram and blood pressure were monitored continuously. Thallium-201 (1 to 2 mCi) was injected intra- venously through a previously established intravenous line between 30 and 60 seconds of the cold pressor test. This time of injection was chosen because maximal changes in heart rate and blood pressure occurred at 30 seconds of cold exposure in all patients. In addition, this time of injection allowed the maximal uptake of thallium-201 by the myocardium to occur while the patient was still under cold pressor challenge. Imaging was begun within 5 to 10 minutes of the termination of the cold pressor test. An Ohio Nuclear Series 120 Gamma Camera and a high resolution collimator were used for imag- ing. Polaroid scintiphotographs with counts of 300,000 to 400,000 were obtained in the anterior, 45” left anterior oblique, and left lateral views. Data were also recorded on magnetic tape for subsequent analysis on a PDP-11 digital computer.
Follow-up thallium-201 scintigrams were obtained in the same projections 4 hours after the initial scintigrams. Image pro- cessing and interpretations were carried out as previously described.5 All interpretations were based on Polaroid scin- tiphotographs. Computer-processed images were used for further confirmation of the results. Briefly, thallium-201 scintigrams were interpreted as abnormal when a discrete area of decreased or absent activity was noted. Partial or complete resolution of the scintigraphic defect from early images to follow-up examination was required before the defect was labeled as related to stress.
According to the method of Richie et al,’ the anatomic lo- cation of the perfusion defect was determined from the left anterior oblique view in which the medial wedge represents the left anterior descending coronary distribution (an anterior defect); the posterolateral wedge, the circumflex coronary distribution (a posterior defect); and the inferior wedge, the posterior descending coronary distribution (an inferior de- fect). With the exception of the perfusion defects at the apex, image abnormalities were not considered defects unless they were visualized in the left anterior oblique view. Each set of early and follow-up scintigrams was read independently by 2 observers without knowledge of the clinical or cineangio- graphic data. The 2 independent observers agreed completely regarding the presence or absence of perfusion deficits in all but 8 instances. The disagreements in these 8 instances were resolved by adding a third observer and the final interpreta- tion was then based on a consensus of 2 of 3 observers.
Thallium-201 scintigraphy with exercise: Within 1 week of cold pressor thallium-201 scintigraphy, 16 patients were exercised on a treadmill to a symptom-limited maximum. Heart rate and blood pressure were monitored continuously. Thallium-201 (1.5 to 2 mCi) was injected 1 minute before termination of the exercise. Scintigrams were obtained im- mediately after the exercise and 4 to 6 hours later. Analysis and interpretation of the scintigrams were carried out as de- scribed in the preceding section. Thallium-201 scintigrams during exercise could not be obtained in 13 patients, because 7 urgently required coronary bypass surgery and 6 others were unwilling to participate in an additional exercise test.
Thallium-201 scintigraphy at rest: To exclude the pos- sibility that transient deficits of myocardial perfusion might have occurred independent of the stress intervention, we performed resting thallium-201 scintigraphy in 6 patients with triple vessel disease. All of these 6 patients had had transient perfusion deficits after the cold pressor and exercise tests. Thallium-201 scintigraphy was then performed at rest, without intervention, and repeated 4 hours later.
Coronary cineangiography during the cold pressor test: The mechanism of ischemia during the cold pressor test was examined in 6 patients and the possibility of coronary spasm as a cause was evaluated by performing coronary cineangiography before and during the cold pressor challenge. Coronary cineangiograms obtained before and during the cold pressor test were compared.
Results
A positive electrocardiographic exercise stress test was recorded in 18 of 24 patients with coronary artery disease and in 1 of 5 patients without coronary artery disease (a sensitivity of 75% and specificity of 80% for the whole group). Sensitivity was low (50%) in patients with single vessel disease. The patient with normal coronary angiograms and false-positive exercise stress test was not receiving digoxin or diuretics at the time of the test.
1254 December 1982 The American Journal of CARDIOLOGY Volume 50

COLD PRESSOR THALLIUM-201 SCINTIGRAPHY-AHMAD ET AL
TABLE I Thallium-201 Sclntigraphic and Exercise Electrocardiographic Data
Total Patients
(n)
Systolic Pressure X Heart Rate Patients (n) With (Mean f SD) Positive Changes/Total Patients
Thallium-201 1 Vessel 2 Vessel 3 Vessel No Baseline Injection’ CAD CAD CAD CAD Sensitivity+
Cold pressor thallium-201 scintigraphy
Exercise ECG Exercise
36 77.4 f 16 103.6 f 17.0+ 4110 lO/ll lO/lO O/5 77%
29 75.2 f 11.7 210.8 f 8.3+ 5710 516 818 l/5 75% 16 72.3 f 8.2 202.6 f 7.3% 212 313 676 o/5 100%
thallium-201 scintigraphy
Resting thallium-201 scintiaraohv
6 77.6 f 8.2 77.6 f 8.2 l/6
l Injections were performed at 30 to 60 seconds of the cold pressor test during cold pressor scintigraphy, at peak exercise during exercise scintigraphy, and at rest during restin
r!! scintigraphy. + Sensitivity figures are for total patients. f p <0.0005 compared with baseline.
CAD = coronary artery disease: E G = electrocardiogram.
The scintigraphic data are presented in Table I. After the cold pressor test, an increase in the systolic blood pressure X heart rate product (double product) was observed in all patients. The mean double product for the group was significantly higher at 30 seconds of the cold pressor test (p <0.0005) (t test for paired data). After the initial increase in the double product at 30 seconds, no further significant increase occurred at 2 minutes of the cold pressor test. Both heart rate and blood pressure returned to baseline values within 5 minutes of the termination of the test in all patients. In addition to the changes in the double product, angina developed in 4 patients during the test and a >l mm S-T segment depression in the electrocardiogram was observed in 3 of these 4 patients. In 5 patients, frequent unifocal premature ventricular contractions were ob- served during the test with complete resolution after the test. In none of the patients did sustained angina or new changes in the l%-lead electrocardiogram obtained 4 to 6 hours after the test develop.
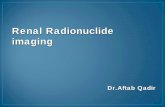
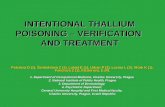
Transient perfusion deficits were observed in 24 of 31 patients with coronary artery disease (a sensitivity of 77%). The sensitivity for the detection of coronary artery disease was high in patients with double and triple vessel disease (Table I). The location of a perfu- sion defect generally corresponded to that of a stenotic vessel in all patients with single vessel disease. Transient perfusion deficits, however, did not generally distin- guish patients with single vessel disease from those with double and triple vessel disease. Only the most severely ischemic area among the several that may be present in patients with 2 and 3 vessel disease was identified. All 5 patients without coronary artery disease had normal scintigrams. Figure 1 shows representative scintigrams obtained early and late after the cold pressor test.
Thallium-201 scintigrams after symptom-limited maximal exercise stress test were obtained in 16 pa- tients. Eleven patients (6 with triple, 3 with double, and 2 with single vessel disease) had positive scintigrams after exercise. All of these 11 patients also had positive scintigrams after the cold pressor test. The 5 patients
with normal coronary cineangiograms had normal ex- ercise scintigrams. The sensitivity level of cold pressor thallium-201 scintigraphy in detecting coronary artery disease was not significantly different from the sensi- tivity levels obtained during exercise scintigraphy and exercise electrocardiography (chi-square test for inde-
1
2
3
FIGURE 1. Thallium-201 scintigrams (45“ left anterior oblique pro- jection), immediately after the cold pressor test (left) and 4 hours later (right). Normal scintigrams in a patient with normal coronary angiograms (panel l), abnormal scintigrams in patients with single vessel disease (circumflex vessel) (panel 2), double vessel disease (left anterior de- scending and right coronary vessels) (panel 3), and triple vessel disease (panel 4). Arrows point to the areas of transient perfusion deficits.
December 1982 The American Journal of CARDIOLOGY Volume 50 1255

COLD PRESSOR THALLIUM-201 SCINTIGRAPHY-AHMAD ET AL
pendence). The site of the transient perfusion deficits observed in the 45O left anterior oblique cold pressor thallium-201 scintigrams was identical to the site of the perfusion deficits observed in the 45” left anterior oblique exercise thallium-201 scintigram in 8 patients. Anterior perfusion deficits were observed in 6 patients with triple vessel disease, in 1 patient with double vessel disease (left anterior descending and right coronary artery), and in 1 patient with single vessel disease (iso- lated left anterior descending lesion). Cold pressor scintigraphy induced posterior perfusion deficits in 2 patients with double vessel disease (right coronary and circumflex vessels) whereas with exercise scintigraphy the perfusion deficits appeared in the inferior region. In 1 patient with an isolated high grade (>90%) proxi- mal lesion of a dominant circumflex coronary artery the perfusion deficit was high posterior during the cold pressor test and inferior during the exercise. Among the 6 patients who had thallium-201 scintigraphy per- formed at rest, only 1 patient showed a mild transient perfusion deficit in the early scintigram in the absence of angina or the electrocardiographic changes of ische- mia. The perfusion deficit was smaller than the one observed in the cold pressor thallium-201 scintigram and resolved completely in the follow-up scintigram. No transient deficits of perfusion were observed in the re- maining 5 patients. Permanent perfusion deficits were observed in 2 patients with a previous transmural myocardial infarction at rest as well as during the cold pressor scintigraphy. The 3 patients with a previous nontransmural myocardial infarction demonstrated no permanent perfusion abnormality.
The mean double product achieved at 30 seconds of the cold pressor test during coronary cineangiography in 6 patients with coronary artery disease was 101.3 f 10.24 and was not significantly different from that at- tained during cold pressor thallium-201 scintigraphy (99.7 f 9.3) (t test for paired data). Coronary spasm, either focal or generalized, was not detected in any of these 6 patients with positive cold pressor and exercise thallium-201 scintigrams.
Discussion
The cold pressor test is a simple and effective alpha-adrenergic stimulus. z~,c Because a rapid increase in blood pressure and heart rate occurs during cold pressor stimulation, a number of recent investigations have focused on its use as a stress test in patients with coronary artery disease.“,7,s Wainwright et al” evaluated left ventricular function in normal subjects and in pa- tients with coronary artery disease by performing ra- dionuclide angiography during the cold pressor test. An increase in the left ventricular ejection fraction was reported in normal subjects. In patients with coronary artery disease, reduction in ejection fraction and de- velopment of regional wall motion abnormalities were observed. In other studies, increased coronary vascular resistance7 and angiographic evidence of coronary artery spasms were observed during the cold pressor test. The simple technique of cold pressor stimulation, its effec- tiveness in challenging the circulatory system, and its
apparent innocuous nature led us to investigate its role in evaluating myocardial perfusion in patients with coronary artery disease.
Our preliminary results with cold pressor thallium- 201 myocardial scintigraphy were encouraging. Tran- sient perfusion deficits were observed in the thallium- 201 scintigrams, after the cold pressor test, in 24 of 31 patients with coronary artery disease, and all 5 patients with normal coronary angiograms had normal scinti- grams. As reported with exercise thallium-201 scintig- raphy,’ the detection of coronary artery disease with cold pressor thallium-201 scintigraphy was highest in patients with double and triple vessel disease. All pa- tients with coronary artery disease, who had exercise- induced ischemic changes in the electrocardiograms and in the thallium-201 scintigrams, also had positive cold pressor thallium-201 scintigrams. In 5 patients without coronary artery disease, both cold pressor and exercise thallium-201 scintigraphy were equally specific in ruling out the presence of coronary artery disease.
Of 5 patients with previous myocardial infarction, only 2 patients with a discrete left ventricular aneurysm demonstrated permanent perfusion deficits in addition to the adjacent transient perfusion deficits in the cold pressor thallium-201 scintigram. Ten patients (5 pa- tients with and 5 without previous myocardial infarc- tion) demonstrated depressed left ventricular ejection fractions or regional wall motion abnormality, or both, at the time of cardiac catheterization. Abnormal left ventricular function in patients without evidence of previous myocardial infarction may be related to the development of ischemia at the time of left ventricular angiography or may be due to the presence of an un- recognized previous myocardial necrosis in some of these patients.
Gewirtz et al’s reported that redistribution of thal- lium-201 in myocardial segments with initially low thallium-201 uptake may occur at rest, suggesting that transient perfusion abnormalities seen in some patients may be independent of stress intervention. The absence of transient perfusion deficits in the resting thallium- 201 scintigrams in 5 of our patients with positive cold pressor thallium-201 scintigrams, however, suggests that scintigraphic changes in these patients were due to the cold pressor test. In 1 patient with triple vessel disease and a mild degree of resting redistribution, the transient perfusion abnormalities were more pro- nounced during the cold pressor test. The similarity or adjacent nature of the site of the perfusion abnormality in 10 of 11 patients with positive cold pressor and ex- ercise thallium-201 scintigrams further validates the relation of the perfusion deficits to the stress inter- vention.
There are a few reports in the literature regarding the possible mechanisms involved in altered myocardial perfusion during the cold pressor challenge.2,gT11 Feld- man et a19 recently reported an increase in coronary vascular resistance in the angiographically defined potentially abnormal regions (>50% coronary artery narrowing) during the cold pressor test. Their study concluded that the increase in coronary resistance was
1256 December 1962 The American Journal of CARDIOLOGY Volume 50

COLD PRESSOR THALLIUM-201 SCINTIGRAPHY-AHMAD ET AL
not due to coronary spasm but possibly to a differential effect of an increased left ventricular end-diastolic pressure on regional blood flow. Thus, it appears that in patients with coronary artery disease, a heterogene- ous myocardial perfusion is possible during the cold pressor test, with only modest increases in the double product and without any angiographic evidence of coronary spasm. Mudge et a1,7 however, did not observe increased left ventricular diastolic pressure in some of their patients with increased coronary vascular resis- tance during cold pressor stimulation. In their study,; a decrease in coronary blood flow and an increase in coronary vascular resistance were thought to be due to coronary vascular constriction secondary to alpha- adrenergic stimulation during the cold pressor test. In our study, the double products achieved during cold pressor stimulation were significantly lower than those obtained during exercise, which indicates that an in- crease in myocardial oxygen demand was probably not the primary mechanism responsible for perfusion ab- normalities. The possibility that coronary spasm may have played a role in producing perfusion deficits cannot be excluded. No coronary spasm was detected, however, in 6 patients in whom coronary angiograms were ob- tained during the cold pressor test.
In summary, our data for the first time provide ob- jective evidence of altered myocardial perfusion during cold pressor stimulation in patients with coronary artery disease. Cold pressor thallium-201 scintigraphy offers promise in detecting abnormal myocardial perfusion and appears to be sensitive in identifying patients with severe coronary artery disease. The limitations of standard exercise thallium-201 scintigraphy became obvious to us during the course of this study in that we were not able to exercise all of our patients. In com- parison, the cold pressor challenge was performed with relative ease in all patients. Thus, the cold pressor test may find a diagnostic role in those patients in whom exercise stress test is not feasible. In our experience, cold pressor stimulation is safe and effective and can be
performed easily at the patient’s bedside. The exact physiologic mechanisms that become operational at the level of the coronary circulation during the cold expo- sure need further clarification. Our data indicate that further studies in a larger number of patients are war- ranted in order to define more clearly the sensitivity, specificity, and safety of cold pressor thallium-201 myocardial scintigraphy in patients with coronary ar- tery disease
Acknowledgment: We acknowledge the technical assis- tance of Scott Goldberg and the secretarial assistance of Mary Darden and Jeanne Arceneaux. We also thank J. Sanfellipo, MD, for his assistance in the cardiac catheterization labora- tory.
1.
2.
3.
4.
5.
6.
7.
6.
9.
10.
11.
References
Ritchie JL, Trobaugh GB, Hamilton GW, et al. Myocardial imaging with thallium-201 at rest and during exercise. Comparison with coronary arte- riography and resting and stress electrocardiography. Circulation 1977; 56:66-7 1. Boyer JT, Freaser JR, Doyle AE. The haemodynamic effects of cold im- mersion. Clin Sci 1960;19:539-550. Wainwright RJ, Brennand-Roper DA, Cueni TA, Sowton E, Hilson AJ, Maisey MN. Cold pressor test in detection of coronary heart-disease and cardiomyopathy using technetium-99m gated blood-pool imaging. Lancet 1979:2:320-323. Bruce RA, Kusumi F, Hosmer D. Maximal oxvaen intake and nomooraohic assessment of funciional aerobic impairmeni in cardiovascular drse&e. Am Heart J 1973:85:546-562. Ahmad M, Merry $L, Hafbach H. Evidence of impaired myocardial perfusion and abnormal left ventricular function during exercise in patients with iso- lated systolic narrowing of the left anterior descending coionary artery. Am J Cardiol 1981;48:832-836. Greene MA, Boftax AJ, Lustig GA, et al. Circulatory dynamics during the cold pressor test. Am J Cardiol 1965; 16:54-60. Mudge GH Jr, Gotdberg S, Gunther S, Mann T, Grossman W. Comparison of metabolic and vasoconstrictor stimuli on coronary vascular resistance in man. Circulation 1979;59:544-550. Raizner AE, Chahine RA, lshlmorl T, et al. Provocation of coronary artery spasm by the cold pressor test. Hemodynamic, arteriographic and quanti- tative angiographic observations. Circulation 1980;62:925-932. Feldman RL, Whittle JL, Pepina CJ, Conti RC. Effects of cold-pressor test on regional coronary hemodynamic and angiographic responses (abstr). Am J Cardiol 1981;47:450. Gewirtz H, Belier GA, Strauss HW, et al. Transient defects of resting thallium scans in patients with coronary artery disease. Circulation 1979; 59:707-713. Gunther S, Green L, Muller JE. Mudae GH Jr. Grossman W. lnaporooriate coronary vasoconstriction in patients with coronary artery disease: g role for nifedipine? Am J Cardiol 1979;44:793-797.
December 1982 The American Journal of CARDIOLOGY Volume 50 1257