
Cold Injury - Northwestern Universitysites.surgery.northwestern.edu/reading/Documents/curriculum/Box...
7
Cold Injury Injuries caused by cold exposure can be systemic (as seen in hypothermia), regional (as in frostbite), or combination. In this article, the authors discuss the degrees of hypothermia, the classifications of frostbite, and the treatment of both. ¯ Throughout history, cold weather has played a role in the outcome of wars and military actions, t It influenced military campaigns, such as those of Alexander of Macedon, and contributed to such notable defeats as Napoleon’s Army in Poland in 1812. World War II saw more than 90,000 U.S. troop casualties from the cold, 2 over 12,000 of these from frostbite. Perhaps the most dramatic cases of freezing oc- curred in B17 and B24 bombers making high-altitude bombing runs over Germa- ny. When attacked by fighters, the waist- port gunners opened their doors to fire and were exposed to very cold air rushing by-:at 200mph. During the winter of ’,: 1943, frostbite caused morecasualties in these bomber crews than all other sources combined. 3 Cold resulted in over 9,000 casualties during the Korean War, most of these occurring in the winter of 1952. 2 Civilian cold injury, seen with alcohol- ism and drug abuse, is more commonin the elderly. Hundreds of recreational boaters, merchant mariners, and commer- cial fishermen also are injured annually. 4 Cold injury can be systemic (as seen in hypothermia), regional (as in frostbite)-, or a combination. There are several mani- festations of regional cold injury that depend upon the temperature and huAaidi- ty( Chilblain is caused by temperatures abow’, freezing in the presence of high humidity. It is rarely a serious problem becauSe the lesions are limited, superfi- cial, and heal quickly. Trench foot or immersion foot occurs when wet feet are exposed to temperatures of 32 ° F to 50 ° F for long periods, usually greater than 12 hours. Frostbite results from tissue expo- sure to subfreezing temperatures. Hypothermia Hypothermia, or systemic cold injury, is a cllinical state of subnormal~entral or "core" temperature. Because some con- troversy exists as to the best technique for arriving at this "core" temperature, for purposes of this discussion, a rectal tem- perature below 35 ° C represents clinical hypot]hermia. 4 It should be noted that the usual clinical thermometer cannot register a temperature below 34.5 ° C. Conse- quently, a laboratory thermometer or an electrical thermistor should be used. When determining rectal temperatures, it is advisable to insert the probe at least 10 cm beyond the anal sphincter to. provide an accurate reading of the core. 5 The first level of hypothermia (mild) occurs; with core temperatures between 33 ° C and 35 ° C. Under these conditions, there is marked shivering unless hypogly- cemia suppresses this response. The body attempts to support the core temperature by peripheral vasoconstriction, tachycar- dia, and increased cardiac output. 5 Dehy- dration and an increase in hematocrit may follow an increase in urinary output know~ as cold diuresis. Individuals feet intense cold but remain conscious. They normally recover spontaneously due to the retained shivering response, and ther- F. Alan Barber, M.D. Clinical Associate Prof., Division of Orthopedic Surgery University of Texas Health Science Ctr.: Orthopedic Surgeon Piano Orthopedic & Sports Med. Center Purcell Smith III. M.D. Orthopedic Surgeon Piano Orthopedic & Sports Med. Center Bradley T. Britt., M.D. Orthopedic Surgeon Piano Orthopedic & Sports Med. Center Piano. Texas February1988 ¯ Surgical Rounds for Orthopaedics¯ 31
Transcript of Cold Injury - Northwestern Universitysites.surgery.northwestern.edu/reading/Documents/curriculum/Box...

Cold Injury
Injuries caused by cold exposure can besystemic (as seen in hypothermia),regional (as in frostbite), or combination. In this article, theauthors discuss the degrees ofhypothermia, the classifications offrostbite, and the treatment of both.
¯ Throughout history, cold weather has
played a role in the outcome of wars andmilitary actions, t It influenced militarycampaigns, such as those of Alexander ofMacedon, and contributed to such notabledefeats as Napoleon’s Army in Poland in1812. World War II saw more than 90,000U.S. troop casualties from the cold, 2 over12,000 of these from frostbite. Perhapsthe most dramatic cases of freezing oc-curred in B17 and B24 bombers makinghigh-altitude bombing runs over Germa-ny. When attacked by fighters, the waist-port gunners opened their doors to fireand were exposed to very cold air rushingby-:at 200mph. During the winter of
’,: 1943, frostbite caused morecasualties inthese bomber crews than all other sourcescombined.3 Cold resulted in over 9,000casualties during the Korean War, most ofthese occurring in the winter of 1952.2
Civilian cold injury, seen with alcohol-ism and drug abuse, is more common inthe elderly. Hundreds of recreational
boaters, merchant mariners, and commer-cial fishermen also are injured annually.4
Cold injury can be systemic (as seen inhypothermia), regional (as in frostbite)-,
or a combination. There are several mani-festations of regional cold injury thatdepend upon the temperature and huAaidi-
ty( Chilblain is caused by temperatures
abow’, freezing in the presence of highhumidity. It is rarely a serious problembecauSe the lesions are limited, superfi-cial, and heal quickly. Trench foot orimmersion foot occurs when wet feet areexposed to temperatures of 32° F to 50° Ffor long periods, usually greater than 12hours. Frostbite results from tissue expo-sure to subfreezing temperatures.
HypothermiaHypothermia, or systemic cold injury,
is a cllinical state of subnormal ~entral or"core" temperature. Because some con-troversy exists as to the best technique forarriving at this "core" temperature, forpurposes of this discussion, a rectal tem-perature below 35° C represents clinicalhypot]hermia.4 It should be noted that theusual clinical thermometer cannot registera temperature below 34.5 ° C. Conse-quently, a laboratory thermometer or an
electrical thermistor should be used.When determining rectal temperatures, itis advisable to insert the probe at least 10cm beyond the anal sphincter to. providean accurate reading of the core.5
The first level of hypothermia (mild)occurs; with core temperatures between33° C and 35° C. Under these conditions,there is marked shivering unless hypogly-
cemia suppresses this response. The bodyattempts to support the core temperature
by peripheral vasoconstriction, tachycar-dia, and increased cardiac output.5 Dehy-dration and an increase in hematocrit mayfollow an increase in urinary output
know~ as cold diuresis. Individuals feetintense cold but remain conscious. Theynormally recover spontaneously due tothe retained shivering response, and ther-
F. Alan Barber,M.D.Clinical AssociateProf., Division ofOrthopedic SurgeryUniversity of TexasHealth Science Ctr.:Orthopedic SurgeonPiano Orthopedic &Sports Med. Center
Purcell Smith III.M.D.Orthopedic SurgeonPiano Orthopedic &Sports Med. Center
Bradley T. Britt.,M.D.Orthopedic SurgeonPiano Orthopedic &Sports Med. CenterPiano. Texas
February 1988 ̄ Surgical Rounds for Orthopaedics ¯ 31

apeutic intervention for mild hypothermianeed not be aggressive.
Moderate hypothermia, with a coretemperature between 30° C and 33° C,suppresses the shivering reflex, resultingin muscle and joint stiffness. Centralnervous system depression and loss ofconsciousness can occur when the brainreaches a temperature between 32° C and30° C. Coordination and peripheral motorand sensory nerve function are impaired.The decreased heart rate, cardiacoutput,blood pressure, and diminished peripheralcirculation make these parameters difficultto measure. Decreased cell metabolismdiminishes the oxygen demand and con-tributes to respiratory slowing. The ECGbegins to show bradycardia, increased PQand QT intervals, broadened QRS cc,m-plexes, nodal rhythm, second-degreeatrioventricular block, and atrial fibrilla-tion. Bowel peristalsis decreases, withfrank ileus developing at about 28° C.
A wide gap of up to 20° C can e~:istbetween the core and skin temperatures.When the skin temperature reaches 12° C,vasodilatation occurs because of precapi!-lary sphincter paralysis. This further de-creases the core temperature, produces aflushing response, and probably is thecause of the "paradoxical undressing"that occurs in this state.6
Severe.hypothermia exists oncecore temperature drops below 30° C. Pro-nounced bradycardia .is accompanied byatrial fibrillation and premature ventricu-lar contractions. Respirations may reachone to two per minute. Hypothermia ofthis degree shifts the oxyhemoglobin dis-sociation curve to the left. However,because of the marked acidosis that alsodevelops, the net result is a right shift ofthe curve.7 The individual is comatose,and it is very difficult to determine wheth-er he is still alive. Blood pressure andpulses are impossible to detect by thestandard indirect methods. Pupils will notrespond to light; muscle and joint stiffnessmay resemble rigor morris. Because ofthese physi_cal findings, no patient should
be considered dead until rewarmingoccurred. ~
Treatment of HypothermiaTreatment of hypothermia is the resto-
ration of all lost heat without precipitatingadditional or fatal side effects. Some au-thors suggest that hypothermia by itselfneed not be fatal above a core temperatureof 25° C.~ Below 25° C, ventricular fibril-lation may appear spontaneously, al-though this may not be fatal. There isevidence in dogs that ventricular fibrilla-tion can be tolerated for periods greaterthan one hour if appropriate rewarmingand defibrillation is initiated.8
As rewarming occurs, there is a de-crease in peripheral vasoconstriction,which may convert compensated hypovo-lemia into hypovolemic shock. Acidosismay result due to the more efficient re-moval of acid metabolites from the pe-riphery. The riskof acidosis is increasedif heat is applied directly to the periphera!tissue. A return of the tissue temperatureto normal levels also increases the tissueoxygen requirements. If the cardiac mus-cle is cooler than the peripheral tissues, itmay be difficult to sustain an adequatecardiac output.
An interesting phenomenon may occurwhen the patient is removed from the coldenvironment: the core temperature maydecrease further..This ’,’after drop" resultsfrom the peripheral tissues continuing todrain heat from the core. The major dropwill occur in the first 15 to 20 minutes,and the core temperature will stabilize inabout 30 minutes.
Hypoxia, metabolic acidosis, and hy-potension should be treated with oxygen,intermittent positive pressure ventilation,sodium bicarbonate, and warm intrave-nous fluids. 9 Respiratory problems mayinclude aspiration pneumonitis, pulmo-nary edema, and thickened bronchial se-cretions. However, suciioning or intuba:tion~ should be done x, ery cautiously be-cause of the increased risk of cardiacarrhythmias. Cardiac monitoring should
¯ Surgical Rounds for Orthopaedics ¯ February 1988

be in place, before any manipulations areinitiated. The central venous pressure alsoshould be monitored, but care should betaken to avoid contact of the catheter tipand the myocardium. Because of the hy-povolemia, urinary output should bemonitored with a catheter. Laboratorytests should include electrolytes.
Prophylactic antibiotics should be con-sidered in view of the potential pulmonaryproblems as well as other injuries thatmay be present. The diagnosis of infectionis difficult in the acute stage of hypother-mia.
Active rewarming should continue untilthe core temperature reaches the 32° C to34° C range. At that point, because of therisks of hyperpyrexia, active effortsshould cease.1° In addition, because of thesignificant metabolic acidosis that can re-sult from shivering during rewarming,phenothiazines should be given,u
The actual rewarming techniques areeither active (rapid) or passive (slow). uniformity of opinion exists as to which isthe best method, although intermediaterates of rewarming should be avoided.12
Passive rewarming allows the patient torewarm himself with his own endogenousheat production alone, usually while atbed rest in a warm room. Rewarmingoccurs slowly with the core temperaturerising at about 10 C per hour.13.If shiver-ing develops, the rewarming rate maydouble) With ~severe hypothermia, it mayrequire 12 to 24 hours tO complete thepassive rewarming process; Slow re-warming techniques usually avoid re-warming hypotension and "after drop"problems as well as allow for the gradualcorrection of fluid balance.
Rapid active rewarming attempts tominimize the time the individual is in thehypothermic state, quickly revitalizes aweakened and irritable myocardium, andmitigates the "after drop" by overwhelm-ing the temperature gradients within thebody with the. application of heat.4 Activerewarming techniques are divided intosurface or core procedures. Surface re-
warn~ting includes the use of warm blan-kets, hot packs, or immersion of the bodyinto water between 40° C and 45° C,14’15
Core rewarming techniques include peri-toneal dialysis, warm-water enemas, ex-tracorporeal circulation, mediastinal la-vage, gastric lavage, diathermy, andbreathing warm air. 1°’16z6 Regardless ofthe techniques selected, resuscitationshould never¯ be terminated until completerewarming has been achieved.
FrostbiteThe basic mechanism by which cold
injures tissues can be divided into directeffects on the cells and extracellular fluidand indirect effects on the circulation andorga~,ized tissues.
Direct injury results when bare tissuecomes in contact with supercool liquid ormetal. This causes immediate freezing ofthe skin and, depending upon the lengthand intensity of the exposure, the underly-ing tissue. More gradual freezing allowsice crystals to develop in the extracellularfluid, which then attract water from thecells, creating a hyperosmolar.intracellu-lar environment with resulting cell dam-age. Intracellular ice crystal .formationand cold-induced shifts in the cell mem-brane: lipid and phospholipid proportionalso can result in the disruption of the cellmembrane.
Indirectly, tissue injury can result from¯ vascular stasis .and hypoxemia.i:Coid ex2.,
posure causes severe vasoconstriction anda decreased ..p~ripheral blood ~flow;capillaries and arterioles can plug andeventually lead to thrombus formation.This causes vascular occlusion, tissue hy-poxia, and ischemic necrosis. Structural-ly, the damage resembles a burn.
Frostbite ClassificationsTwo clinical classifications of frostbite
exist, but unless the patient is seen beforerewarming takes place, any classificationcan "be applied only retrospectively. -Washtburn’s division of frostbite .into su-perficial and deep categories has the bene-
February 1988 o.Surgical Rounds for Orthopaedics ? 33

fit of simplicity.~ Superficial frostbite ap-plies to a part that is white and frozen c,nthe surface but feels soft and resilientwhen the examiner presses the tissue gent-ly and firmly. Deep frostbite cannot bedepressed and feels hard and solid. Afterthe part has thawed, one cannot prognosti-cate.
The four-part classification can be ap-plied only as the clinical course begins ’tomanifest itself and cannot be used figrprognostication. It is difficult to placemost patients into a single category. First-degree cold injury consists of hyperemiaand edema. Edema develops in threehours and lasts five to ten days. Sloughingof the superficial skin layers begins afterabout one week and may last one month.
Second-degree cold injury is associatedwith edema and hyperemia as well asblisters developing on the first day. Theblisters eventually dry and form blackeschars within two to four weeks. Whenthe eschar sloughs, pink tender skin isleft.
Third-degree cold injury consists offull-’thickness skin injury with some ex-tension into the subcutaneous tissues.Blisters appear at the edges of the third-degree injury, in areas of second-degreeinjury. The skin becomes a hard, blackeschar, which takes two months to heal. If_eschars’ are circumferential, they oftenproduce a tourniquet effect. ~ ......
Fourth-degree Cold injury inVolves alltissues~ indluding bone, with total de-struction of the affected part. The partbecomes bla_ck and dry and shrivels withdemarcation in one to two months. Themummifiedpart usually autoamputa~cesafter two to three months (Figure 1).
The Clinical PictureResistance to cold varies with the type
of tissue. Although the skin, fascia, andconnective tissues are resistant, bone andtendon are the most resistant. Nerves and
numb. This often is followed by a pleas-ant feeling of warmth. First the skinbecomes red, then pale and waxy white.The initial stage of "frost nip" is revers-ible and treatment straightforward. Ifallowed to go unchecked, frostbite is in-evitable and adequate treatment in thefield impossible. The sudden blanching ofthe skin must be noticed promptly. Firm,steady pressure of a warm hand on thecold nose, cheek, or ear must continueuntil the color returns. Cold hands can beplaced in the warm axillae. Cold feet canbe placed against a warm abdomen orchest sheltered from the wind. Never rubor massage an extremity, and never applysnow.
Temperature, humidity, wind velocityat the initial exposure, and the timeelapsed before adequate rewarming alleffect the clinical result. The latter is theleast important in terms of overall prog-nosis. It is often advisable to allow thepatient to walk for hours on frozen feet ifit facilitates his evacuation from a remote.area. Once his toes or feet thaw, hebecomes a stretcher case, and refreezingseverely, c0.mpromises the injured tissues.
Emergency physicians rarely see thedead, white, hard, brittle stage of frostbitefrom which some prognostication can bemade. Wartime statistics indicate that lessthan 2% of cold injuries were seen by a
...... medical o~cer before rewarming.~Previous significant episodes of cold
...... whether affecting the. presentlyinvolved part or not, increage the risk offurther cold injury. Individuals who areundernourished, elderly, or have otherinjuries resulting in decreased tissue per-fusion (such as shock or peripheral vascu-lar disease) are at an increased risk forfrostbite.
The wind-chill factor accentuates oraccelerates the development of frostbite.Heat loss by convection greatly enhancessurfaCe cooling. A temperature of-30° F
striated muscles, in contrast, are higl!Iy with a wind speed of 25 mph has the same
sensitive. The individual affected by frc,st- cooling effect on exposed flesh as a tem-
bite feels uncomfortably cold and later perature of 0° F without wind.
34 ̄ Surgical Rounds for Orthopaedics ° February 1988

Figure 1--Frostbite injury to the toes.
Treatment of FrostbiteThe patient with frostbite must be re-
moved from the cold as soon as possible.Rapid rewarming is the treatment of
Upon arrival at an adequate facility, thepatient should be treated for both frostbiteand hypothermia. After all the clotheshave been removed from the extremity,
choice.3 It is better to wait to thaw a part the affected part should be rewarmed
than -to "do so ~:inc0mpletely oi:~:risk the :-.rapidlyby:placing it into a large volume
chance of refreezing, even if this delays of water maintained at 104°.F to 108° F
rewarming several hours. De6reiised cir-culation has a significant effect on frost-bite, and anything that can c~fribute todecreased circulation should be avoided,especially smoking. It is better to splintfractures in a well-padded device than toapply traction because the straps applyingthe force obstruct blood flow. Boots orshoes should be removed from any ex-tremity with a fracture and replaced withseveral layers Of blankets or other suitablematerial. Alcohol also should be avoidedbecause the increased surface bl0bdflowlowers the core temperature and contrib-utes to hypothermia.
(40° C to .42° .C), Once the feet or toesthaw., walking should not b~ permitted.
Rewarming can be very painful in thefirst few minutes and is worse in thosewith impaired circulation. Therefore, nar-c0tics may be required. Rewarming of anextremity should not take over 20 min-utes, and further immersion is of nobenefit. Never rub or massage a frozenextremity, even after thawing. Rubbingthe extrerriity with snow or exposing it toan ~pen fire or dry heat has no piaceinthetrea~ment of frostbitd find actually inCreas-es the damage.
Although accurate assessment of the
February 1988 ̄ Surgical Rounds for Orthopaedics ° 35
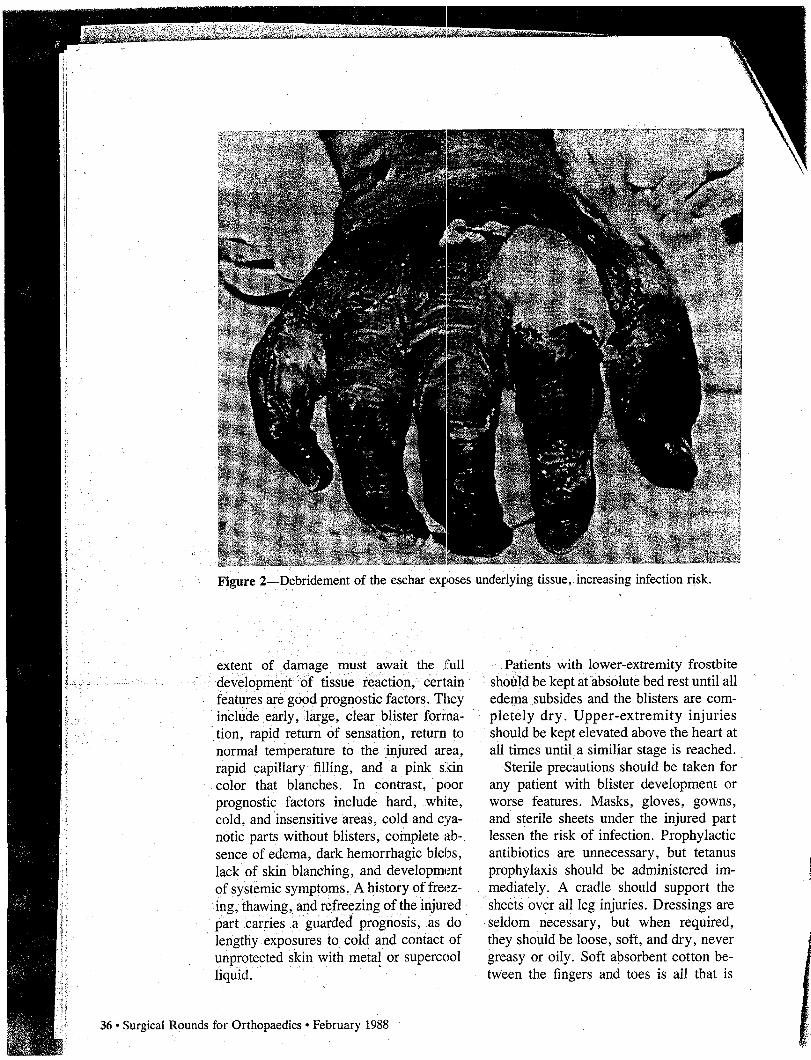
Figure 2 Debridement of the eschar exl?oses underlying tissue, increasing infection risk.
extent of damage must await the full¯ development ~0f tissue reaction,. Certainfeatures are good prognostic factors. Theyinclude early, ,large, clear blister forma-
tion, rapid return of sensation, return tonormal temperature to the injured area,rapid capillary filling, and a pink skincolor that blanches. In contrast, poorprognostic factors include hard, white,cold, and insensitive areas, cold and cya-notic parts without blisters, complete ab-sence of edema, dark hemorrhagic blebs,lack of skin blanching, and developmentof systemic symptoms. A history of freez-ing, thawing, and refreezing of the injuredpart carries a guarded prognosis, as dolengthy exposures to cold and contact ofunprotected skin with meta! or supercoolliquid.
Patients with lower-extremity frostbiteshould be kept at absolute bed rest until alledema subsides and the blisters are com-pletely dry. Upper-extremity injuriesshould be kept elevated above the heart atall times until a similiar stage is reached.
Sterile precautions should be taken forany patient with blister development orworse features. Masks, gloves, gowns,and sterile sheets under the injured partlessen the risk of infection. Prophylacticantibiotics are unnecessary, but tetanusprophylaxis should be administered im-mediately. A cradle should support thesheets over all leg injuries. Dressings areseldom necessary, but when required,they should be loose, soft, and dry, nevergreasy or oily. Soft absorbent cotton be-tween the fingers and toes is all that is
36 ̄ Surgical Rounds for Orthopaedics ¯ February 1988

needed. Dressings should be changedonly when they are very dirty. The roomshould be kept comfortably warm (72° Fto 78° F) in order to maintain bodywarmth during convalescence.
Physical therapy should provide twice-a-day active range of motion for 20 min-utes in a 37° C whirlpool solution ofhexachlorophene and water, but passivemanipulations should be avoided. Thesewhirlpool treatments provide all thewound debridement necessary. All opera-tive interventions should be avoided ex-cept for splitting circumferential escharsthat impede circulation. Intact blistersshould not be debrided, even if theydecompress spontaneously. Any de-bridement exposes sensitive underlyingtissue and increases the risk of infection(Figure 2). If infection develops, broad-spectrum antibiotics should be used untilspecific sensitivities are available. Smok-ing is prohibited Until healing is complete.
Patience in operative management isvery important. Even in cases of obviousdeep injury undoubtedly requiring ampu-tation, observation for one to two monthsfrequently shows a considerable reductionin the amount to be removed (Figure 3).The diet should be high in protein withmultivitamin supplements. Generally, theresults are improved by protection of theextremity during and after rewarming,prevention of infection, and gentle activerange-of-motion exercises in a whirlpoolbath to maintain function.
Long-term follow-up of Korean Warfrostbite victims showed that even after 13years, excessive sweating, pain, cold feet,numbness, abnormal color, and jointsymptoms were reported. These symp-toms were caused by cold exposure. Pa-tients had persistent tissue loss, scarring,toe and fingernail abnormalities, pigmentchanges, and radiographic bone and jointchanges. Other long-term complicationsof frostbite include destruction of theepiphyseal plates of the phalanges, stunt-ed growth and mild flexion deformities,and loss of fingernails.’~7 ̄ ~
Figure: 3--Amputation should be delayed at least one to two monthsto allow for further recovery.
References1. Barber FA: Cold injury in the military. Med Bulletin of the
U.S. Army Europe 37:22-27, 1980.2. Cold injury: Technca Bulletin 81. Department of the
Army, p~n 1-13, 1976.3. Washburn B: Frostbite. N Engl J Meal 266:974-982, 1962.4. Harnett RM, Pruitt JR, Sias FR: A review of the literature
concerning resuscitation from hypothermia. Part I: The problemand general approaches. Aviat Space Environ Med 54:425-434,1983.
5. Lonning PE, Skulberg A, Abyholm F: Accidental hypother-mia: A review of the literature. Acta Anaesthesiol Scand 30:601-613, 1986.
6. Wedin B. Vanguard L, Hiruonen J: ’Paradoxical undressinT’in fatal hypothermia. J Forensic Sci Soc 24:543-553, 1979.
7. Marcus P, Edwards R: Serum enzyme levels during experi-mental hypothermia in man. Q J Exp Physiol 63:371-381. 1978.
8. Hughes CW: Discussion in Physiology of Induced Hypo-thermia. Dripps RD (Ed). Pub. 451, Natl Acad Sci--Natl ResCouncil, Washington, 1956.
9. Ledingham IM. Mone JG: Accidental hypothermia. Lancet1:391, 1978.
I0. Truscott DG, Firor WB. Clein LJ: Accidental profoundhypothermia. Arch Surg 106:216-218, 1973.
1l. Henneman DH, Bunker JP, Brewster WR: Immediatemetabolic response to hypothermia in man. J Appl Physiol12:164-1,,58. 1958.
12. Hervey GR: Physiological changes encountered in hypo-thermia. Proc R Soc Med 66:1053-1058, I973.
t3. MilIer JV, Danzl DF, Thomas DM: Urban accidental
February 1988 ̄ Surgical Rounds for Orthopaedics; ° 37













![COLD INJURIES-1.ppt [Read-Only]ocw.usu.ac.id/.../emd166_slide_cold_injuries.pdf · compensate for cold that produces injury. • Duration of exposure, humidity, wind, altitude, clothing,](https://static.fdocuments.us/doc/165x107/5f41a4b40465033ce30ec818/cold-injuries-1ppt-read-onlyocwusuacidemd166slidecold-compensate.jpg)




