
Cohabitation and US Adult Mortality - Wiley Online Library
18
HUI LIU Michigan State University CORINNE RECZEK University of Cincinnati* Cohabitation and U.S. Adult Mortality: An Examination by Gender and Race This study is the first to explore the relationship between cohabitation and U.S. adult mortal- ity using a nationally representative sample. Using data from the National Health Interview Survey-Longitudinal Mortality Follow-up files 1997 – 2004 (N = 193,851), the authors found that divorced, widowed, and never-married White men had higher mortality rates than cohabiting White men, and never-married Black men had higher mortality rates than cohabit- ing Black men. In contrast, the mortality rates of nonmarried White and Black women were not different from those of their cohabiting counterparts. The results also revealed that mor- tality rates of married White men and women were lower than their cohabiting counterparts and that these mortality differences tended to decrease with age. The authors found no signif- icant mortality differences when they compared married Black men or women to their cohabiting counterparts. The identified mortality differ- ences were partially—but not fully—explained by income, psychological, or health behavior differences across groups. Department of Sociology, Michigan State University, 316 Berkey Hall, East Lansing, MI 48824-1111 ([email protected]). *Department of Sociology, University of Cincinnati, 1018 Crosley Tower, Cincinnati, OH 45221-0378. Key Words: age, cohabitation, gender, marriage, mortal- ity, race. The prevalence of nonmarital cohabitation in the United States has steadily increased, from 0.4 million cohabiters in 1960 to 7.6 million in 2011 (U.S. Census Bureau, 2011). Given a sub- stantial literature showing that participation in marriage may protect health and longevity (for a review, see Carr & Springer, 2010), one cen- tral concern related to this rising rate is that cohabiters may not receive the same health and longevity benefits as married individuals. In gen- eral, research suggests that married people are healthier and live longer than nonmarried people (Waite & Gallagher, 2000), yet studies tend to analyze nonmarried individuals as one homo- geneous group that includes cohabiting, never- married, divorced, and widowed people. Thus, very little is known about how the mortality of cohabiters differs from other union status groups (Carr & Springer). At least on some dimen- sions, recent research suggests that cohabitation is similar to marriage: Intimate partners in both married and cohabiting unions share a home; engage in emotional and sexual intimacy; and act as a potential confidant, caregiver, and financial supporter (Musick & Bumpass, 2012). There- fore, cohabitation and marriage may promote health and longevity in analogous ways. Alterna- tively, some research suggests that cohabitation is dissimilar to marriage: Compared to married individuals, cohabiters are more likely to engage in risky health behaviors (Horwitz & White, 1998), report strain in their relationships (Skin- ner, Bahr, Crane, & Call, 2002), experience more 794 Journal of Marriage and Family 74 (August 2012): 794 – 811 DOI:10.1111/j.1741-3737.2012.00983.x
Transcript of Cohabitation and US Adult Mortality - Wiley Online Library
HUI LIU Michigan State University
CORINNE RECZEK University of Cincinnati*
Cohabitation and U.S. Adult Mortality: An
Examination by Gender and Race
This study is the first to explore the relationshipbetween cohabitation and U.S. adult mortal-ity using a nationally representative sample.Using data from the National Health InterviewSurvey-Longitudinal Mortality Follow-up files1997 – 2004 (N = 193,851), the authors foundthat divorced, widowed, and never-marriedWhite men had higher mortality rates thancohabiting White men, and never-married Blackmen had higher mortality rates than cohabit-ing Black men. In contrast, the mortality ratesof nonmarried White and Black women werenot different from those of their cohabitingcounterparts. The results also revealed that mor-tality rates of married White men and womenwere lower than their cohabiting counterpartsand that these mortality differences tended todecrease with age. The authors found no signif-icant mortality differences when they comparedmarried Black men or women to their cohabitingcounterparts. The identified mortality differ-ences were partially—but not fully—explainedby income, psychological, or health behaviordifferences across groups.
Department of Sociology, Michigan State University, 316Berkey Hall, East Lansing, MI 48824-1111([email protected]).
*Department of Sociology, University of Cincinnati, 1018Crosley Tower, Cincinnati, OH 45221-0378.
Key Words: age, cohabitation, gender, marriage, mortal-ity, race.
The prevalence of nonmarital cohabitation inthe United States has steadily increased, from0.4 million cohabiters in 1960 to 7.6 million in2011 (U.S. Census Bureau, 2011). Given a sub-stantial literature showing that participation inmarriage may protect health and longevity (fora review, see Carr & Springer, 2010), one cen-tral concern related to this rising rate is thatcohabiters may not receive the same health andlongevity benefits as married individuals. In gen-eral, research suggests that married people arehealthier and live longer than nonmarried people(Waite & Gallagher, 2000), yet studies tend toanalyze nonmarried individuals as one homo-geneous group that includes cohabiting, never-married, divorced, and widowed people. Thus,very little is known about how the mortality ofcohabiters differs from other union status groups(Carr & Springer). At least on some dimen-sions, recent research suggests that cohabitationis similar to marriage: Intimate partners in bothmarried and cohabiting unions share a home;engage in emotional and sexual intimacy; and actas a potential confidant, caregiver, and financialsupporter (Musick & Bumpass, 2012). There-fore, cohabitation and marriage may promotehealth and longevity in analogous ways. Alterna-tively, some research suggests that cohabitationis dissimilar to marriage: Compared to marriedindividuals, cohabiters are more likely to engagein risky health behaviors (Horwitz & White,1998), report strain in their relationships (Skin-ner, Bahr, Crane, & Call, 2002), experience more
794 Journal of Marriage and Family 74 (August 2012): 794 – 811DOI:10.1111/j.1741-3737.2012.00983.x

Cohabitation and U.S. Adult Mortality 795
psychological distress (Brown, 2000), and haveshorter relationship durations (Heaton, 2002).Thus, cohabiting partners may not receive thesame longevity benefits as married spouses.
The present study is the first to explorethe relationship between cohabitation and adultmortality in the United States using a nation-ally representative sample. We compared themortality rates of cohabiters to the mortalityrates of married, unpartnered never-married,divorced/separated, and widowed individuals.We further examined whether family income,psychological distress, and health behavior—themost frequently documented mechanisms link-ing union status and health (Waite & Gallagher,2000)—explain union status differences in mor-tality. Given the long-standing observationsabout gender and racial differences in familyand mortality processes (Brown, Van Hook, &Glick, 2008) we, for the first time, pay specialattention to the intersections of gender and racialdifferences in the link between cohabitation andmortality.
BACKGROUND
Cohabitation and Mortality: EmpiricalEvidence
Empirical evidence on the link between cohabi-tation and mortality is sparse and based on datafrom European populations. European studiessuggest that individuals who cohabit with oth-ers face a higher mortality risk than marriedpeople but a lower mortality risk than thosewho live alone (e.g., Koskinen, Joutsenniemi,Martelin, & Martikainen, 2007). In their studyof a Danish population, Lund and colleagues(2002) found that the lower mortality rate ofthose who live with someone in comparison tothose who live alone cannot be explained bydifferences in health behaviors such as smok-ing, diet, or physical activity. Researchers haveexplored the link between cohabitation and othermeasures of well-being in the United States andCanada, but this literature provides inconsistentevidence. For example, some studies have foundthat cohabiters report higher levels of psycho-logical distress and lower levels of self-ratedhealth than married individual but report betterhealth than unpartnered single people (Brown,2000; Wu, Penning, Pollard, & Hart, 2003).In contrast, Fuller (2010) found that, comparedto both married and unpartnered single people,
cohabiters tend to have poorer self-rated healthand higher levels of psychological distress andspend a longer time recovering from a healthproblem. Still other studies have found no sig-nificant difference between married individualsand cohabiters on a range of health outcomes(Musick & Bumpass, 2012; Wu & Hart, 2002).Overall, these studies provide little consistentinsight into how mortality rates may be simi-lar or different for U.S. cohabiters versus otherunion status groups.
Cohabitation and Mortality: TheoreticalPredictions
Despite a paucity of empirical evidence onthe link between cohabitation and mortality,a long-standing literature linking marital rela-tionships with health offers theoretical insightinto this research area. Some studies suggestthat people who marry are the healthiest of thepopulation—leaving unhealthy people selectedoutside the bounds of marriage into other uniontypes, such as cohabitation (Horwitz & White,1998; Kenney & McLanahan, 2006). Additionalresearch, however, suggests processes beyondselection, wherein involvement in a maritalrelationship is related to unique economic, psy-chological, and social resources, which in turnpromote longevity, are at play (Ross, Mirowsky,& Goldsteen, 1990; Waite & Gallagher, 2000).Whether these resources are present, however—and, if so, to what degree—in cohabiting rela-tionships is unclear. To build our hypotheses onthe relationship between cohabitation and mor-tality, we focused on three primary resources thatare believed to accrue in marriage : (a) economicresources, (b) psychological well-being, and (c)the social control of health behavior.
Economic resources. Economic resources are akey reason hypothesized to account for the bet-ter health and lower mortality rates of marriedpeople (Waite & Gallagher, 2000). A substan-tial literature suggests that marriage leads to anincrease in economic resources through special-ization in the division of labor, economies ofscale, and the pooling of wealth (Becker, 1981;Waite & Gallagher). These economic resourcesmay promote longevity by, for example, enhanc-ing one’s financial capability to buy fruits andvegetables and thus improving nutrition, pro-viding or easing access to health insurance,and increasing the probability of access to

796 Journal of Marriage and Family
professional care in the event of illness or injury(Ross et al., 1990). Cohabiters share living spacewith a partner and may, to some degree, benefitfrom economies of scale in ways similar to mar-ried people, yet, cohabiters are less likely thanmarried individuals to pool their income (Brines& Joyner, 1999) or to specialize between house-hold and paid work (Gupta, 1999), which mayresult in diminished economic returns (Becker,1981). Moreover, some research suggests thatmarriage becomes a financial ‘‘capstone’’ (Cher-lin, 2004), whereby cohabiters delay marriagein order to obtain the financial stability theybelieve is necessary to achieve before marriage(Edin & Kefalas, 2005). In this sense, cohabitersmay not accrue the financial benefits of mar-riage—or may benefit only incrementally—andin turn have higher mortality rates than marriedpeople, although lower rates than unpartneredsingle people.
Psychological well-being. The marital relation-ship also provides access to psychologicalresources, such as social support (i.e., providinglove, advice, and care) and social integration(i.e., feeling connected to others), which in turnpromote psychological and physical well-being(Ross et al., 1990). Cohabiting partners provideat least some emotional and social support forone another and therefore may promote healthin ways similar to married spouses (Musick &Bumpass, 2012). In contrast, however, cohabita-tion is often a short-term state; most cohabiterseither break up or marry within 5 years, althoughthe duration of cohabitation has increased inrecent years (Kennedy & Bumpass, 2008).Moreover, cohabiters are less likely to receivesupport from friends or relatives (Eggebeen,2005) and are more likely to report relationshipstrain (Horwitz & White, 1998), express con-cern about their relationship dissolving (Brown,2000), and have higher levels of psychologi-cal distress (Brown; Wu et al., 2003) than theirmarried counterparts—all factors that have beenshown to contribute to higher mortality rates(Tower, Kasl, & Darefsky, 2002). Because ofthese differences, cohabitation may not providethe same psychological benefits as marriage(Bumpass & Lu, 2000; Waite & Gallagher,2000). We expect that, if this is the case, thencohabiters would have higher mortality ratesthan married people, although lower rates thanunpartnered never-married, divorced, and wid-owed individuals.
Social control of health behavior. One of thesignificant social resources spouses accrue inmarriage is the social control of health behav-iors. Social control processes shape health habitsindirectly through the internalization and self-enforcement of appropriate health habit norms.For example, entrance into the role of hus-band brings a set of health-related norms (e.g.,decreased alcohol use) that become internal-ized. Social control also operates directly whenspouses attempt to regulate their partners’ healthbehaviors (Umberson, 1992). The social controlof health behaviors promotes healthier habits,such as exercise, eating more fruits and vegeta-bles, and drinking and smoking cessation, whichin turn shape mortality (Umberson). Becauseof varying levels of social control, cohabitersare more likely to engage in risky behaviorcompared to married people (Horwitz & White,1998) but less likely to engage in risky behav-ior compared to single individuals (Kenney &McLanahan, 2006). We expected that cohabiterswould have higher mortality rates than marriedindividuals but lower mortality rates than singleindividuals because of different levels of socialcontrol regarding health behavior.
Gender, Cohabitation, and Mortality
Empirical evidence on gender differences inthe link between cohabitation and mortality isinconsistent and mostly based on data gatheredoutside the United States, yet this body of worksuggests that important gender dynamics maybe at play. A 10-year follow-up study of a 65-to 84-year-old Italian population found that themortality rate of cohabiting men was lower thanthe rate of men who lived alone but that women’ssurvival was not related to cohabitation status(Scafato et al., 2008). In contrast, a mortalitystudy of a Danish elderly population age 75 andabove found that continuously living alone was astronger predictor of the mortality of women thanof men (Lund, Modvig, Due, & Holstein, 2000).Still other European studies have reported nosignificant gender difference in the relationshipbetween cohabitation status and mortality (e.g.,Lund et al., 2002). Significantly more researchhas examined gender differences in the linkbetween marriage and mortality. This body ofwork suggests that the economic, social, andpsychological aspects of marriage differentiallybenefit men’s and women’s health and longevityand that, overall, men’s health benefits more

Cohabitation and U.S. Adult Mortality 797
from marriage than women’s (Ross et al., 1990;Umberson, 1992). Married men receive higherlevels of social control of health behaviors andgreater psychological benefits (e.g., emotionalsupport) than married women (Umberson). Incontrast, married women tend to benefit fromincreased economic resources as a result of mar-riage to a typically higher earning spouse; thisincome boost has been highlighted as the keymechanism linking marriage and mortality forwomen (Lillard & Waite, 1995).
In line with the research on gender, health,and marriage, Duncan, Wilkerson, and England(2006) found that young men who transition tocohabitation are more likely than young womento reduce their marijuana use and binge drinking,perhaps because of women’s greater social con-trol efforts. Similarly, cohabiting men—just likemarried men—earn more than their female part-ners (Brines & Joyner, 1999). This research sug-gests that cohabiting relationships are, to someextent, gendered in similar ways as the maritaltie, wherein cohabiting men may receive higherlevels of social and psychological resources fromtheir female partners and cohabiting women mayreceive greater economic resources from theirmale partners. Such dynamics may in turn shapemortality rates for cohabiting men and women insimilar ways as marriage, yet cohabiting partnersare more egalitarian than married couples, andthey are less likely to pool their income (Brines& Joyner). Thus, cohabiting women may notgain the same economic benefits that marriedwomen do (Waite & Gallagher, 2000). In addi-tion, research suggests that there are overallfewer social and psychological resources foundin cohabiting unions compared to marriages(Bumpass & Lu, 2000). Therefore, althoughcohabiting men may receive similar types ofsocial and psychological resources comparedto married men, they may not receive theseresources to the same degree (Waite & Gal-lagher), effectively leveling the gender gap inmortality for cohabiting men and women.
Race, Cohabitation, and Mortality
In the United States, cohabitation is more preva-lent among Blacks than Whites (U.S. CensusBureau, 2011). Mortality rates are also higherfor Blacks than Whites until around age 80,when the mortality rates of Blacks becomelower than Whites; this crossover pattern ispossibly due to selection processes (Rogers,
Hummer, & Nam, 2000). Despite researchsuggesting that both cohabitation and mortal-ity vary across race, we know of no studiesthat have examined how cohabitation shapesmortality differently across racial groups. Theprevalence rates of cohabitation across racialgroups suggest that cohabitation may have dif-ferent meanings and dynamics—and thereforeprovide different social, psychological, and eco-nomic resources—for Blacks and Whites. Suchresources may in turn differentially shape mor-tality across racial groups. For example, Whitesare more likely to marry their cohabiting part-ner than Blacks are (Brown et al., 2008), andtherefore cohabitation for Whites may be moreof a trial marriage (Thornton, Axinn, & Xie,2007). In contrast, cohabitation tends to be analternative to marriage, or ‘‘marriage-like,’’ forBlacks (Brown et al., 2008; Thornton et al.). Atrial marriage may have dynamics similar tothose of dating couples—including lower levelsof shared social, psychological, and economicresources—whereas marriage-like cohabitationmay have dynamics more similar to married cou-ples (Heuveline & Timberlake, 2004), includinghigher levels of these shared resources. This sug-gests that cohabitation may mirror the dynam-ics of marriage in ways that shape mortalitymore for Blacks than for Whites. Alternatively,researchers contend that married Black men andwomen benefit less from marriage than do theirWhite counterparts because of Black men andwomen’s higher levels of marital strain (Liu &Umberson, 2008). Moreover, the economic con-sequences of marriage and cohabitation differbetween Blacks and Whites. The earning pre-mium of married men relative to unmarried menis greater for Whites than for Blacks (Cohen,1999), and Black women are less likely thanWhite women to increase their financial capi-tal from relationship unions (Edin & Kefalas,2005). This body of work suggests that cohabi-tation, like marriage, may bring fewer economicbenefits and have a smaller protective effect onmortality for Blacks than for Whites in compar-ison to being single.
Additional Sociodemographic Covariates
Theoretical and empirical evidence suggests thatboth union status and mortality are associatedwith other sociodemographic characteristics.Mortality rates certainly vary by age: Youngerindividuals are more likely to be never married

798 Journal of Marriage and Family
and view cohabitation as a precursor to mar-riage, whereas older individuals are more likelyto be previously married and view cohabitationas an alternative to marriage (King & Scott,2005). Both cohabitation and mortality rates arehigher among groups with lower levels of edu-cation than those with higher levels of education(Bumpass & Lu, 2000; Rogers et al., 2000).Cohabitation is less prevalent, and mortality ishigher, in less economically developed regions(e.g., the South) in comparison to more econom-ically developed regions (e.g., the Northeast;Rogers et al.). Individuals in poorer health, astrong predictor for mortality, are less likelyto get married than enter into cohabitation orremain single (Horwitz & White, 1998).
METHOD
Data and Sample
We used data from the public use version ofthe National Health Interview Survey—Longi-tudinal Mortality Follow-Up (NHIS-LMF). TheNational Health Interview Survey (NHIS) isa cross-sectional household interview surveyconducted annually by the National Center forHealth Statistics (NCHS). The NHIS samplingfollows a multistage probability design and isrepresentative of the civilian noninstitutional-ized population of the United States (NCHS,2004). Through statistical matching techniques,all NHIS survey respondents age 18 and overwith sufficient identifying information who wereinterviewed between 1986 and 2004 are eligi-ble for mortality follow-up and linked to deathrecords in the National Death Index (NDI)through the end of 2006 (NCHS). The NDI is anational file of deaths that occur each year in theUnited States. In this study, we used the pooledNHIS-LMF files from 1997 to 2004, because theNHIS did not collect information on cohabita-tion status prior to 1997. We excluded 11,782respondents (i.e., 5.72%) who had insufficientidentifying information and were thus ineligiblefor mortality follow-up. Those ineligible respon-dents were more likely to be nonmarried and tohave a lower socioeconomic status, and thusmore likely to die. Therefore, our estimates ofmortality rates are likely to be conservative. TheNHIS collected sociodemographic and healthinformation for all individuals in the house-hold. One sample adult was randomly selectedfrom each NHIS family in order to collect more
detailed health information (e.g., health behav-iors, psychological distress). The present studyis restricted to the Sample Adult Core files: thosedata that include measures of health behaviorsand psychological distress. The NHIS-LMF pro-vides a unique opportunity to investigate thecohabitation – mortality link because it includesa large number of deaths among cohabitersacross gender and racial subgroups. These dataalso provide high-quality measures for the keyvariables (e.g., socioeconomic status, psycho-logical distress, health behaviors) that are centralto the present study.
Only sample adults age 18 and above whowere identified as non-Hispanic White (here-after White) and non-Hispanic Black (here-after Black) were included in the analysis. Weexcluded 48,070 (20%) individuals from otherracial/ethnic groups because they are highly het-erogeneous, and the focus of our study was com-paring Whites and Blacks. We further excluded476 (i.e., 0.24%) observations with missing val-ues on cohabitation and marital status when thesurveys were conducted. In the final analysis, weincluded 193,851 respondents who were inter-viewed in the NHIS from 1997 to 2004; 7,113of these individuals died within 3 years after thesurvey was conducted. All analyses presentedare weighted to adjust for the complex samplingdesign, and we used robust standard errors fortests of significance.
Measures
Mortality. We estimated the mortality rate fromthe date when the survey was conducted tothe subsequent 3-year follow-up (i.e., thoseinterviewed in 1997 were followed up until2000, those interviewed in 1998 were followedup until 2001, etc.). We truncated the mortalityfollow-up to a 3-year period, rather than usingthe full mortality follow-up data (i.e., until theend of 2006), because NHIS did not follow upthe union status of the respondents, and the 3-year mortality follow-up reduces the exposure ofunion transitions. Our additional analyses (notshown but available on request) with 1-, 2-, or5-year mortality follow-up reveal results similarto those with the 3-year mortality follow-up.
Union status was the primary independentvariable used to predict the mortality risk ofparticipants up to 3 years after the respondentwas interviewed. Because NHIS-LMF dataprovide no information on union status at death,

Cohabitation and U.S. Adult Mortality 799
we used union status information collected at thebaseline NHIS survey. Union status was dividedinto five categories: (a) currently married,(b) cohabiting (i.e., nonmarried and living witha partner), (c) nonpartnered never married,(d) divorced/separated, and (e) widowed. Weused cohabiting as the reference group inthe analysis to better understand mortalitydifferences between cohabiters and other unionstatus groups. Transitions into and out of maritaland cohabiting unions were not identifiable inthe data because NHIS did not follow the unionstatus of the respondents.
Family income. We followed previous studies(e.g., Liu & Umberson, 2008) to measure familyincome and used the midpoint of each incomecategory, converted into 2004 U.S. dollars basedon the consumer price index. We used the log-arithmic transformation of family income toaddress the skewed distribution, which is furthercentered at the mean value. About 5% of respon-dents (n = 9,814) had missing reports on familyincome in the total analyzed sample. We imputedthose missing data using a single-imputationmethod based on age, gender, race, geographicregion, education, marital status, health status,and survey year. Although a multiple-imputationmethod is more methodologically sophisticated,researchers contend that single imputation isa reasonable approach when the proportion ofmissing data is small (Allison, 2001). We alsoexamined an additional measure of economicresources by using the ratio of family incometo poverty threshold, which considers the sizeof family. The results (not shown but availableon request) revealed patterns similar to thosereported when the family income measure wasused.
Psychological distress. We used the Kessler-6 scale (K6; Kessler et al., 2002) to mea-sure psychological distress. The K6 scale hasdemonstrated internal consistency and reliability(Cronbach’s α = .86) in measuring psycholog-ical distress. It is widely used to screen formental illness in large-scale surveys by askingabout the presence of six mental health symp-toms: ‘‘During the past 30 days, how often didyou feel: (a) So sad that nothing could cheer youup (factor loading = .7365), (b) Nervous (fac-tor loading = .6850), (c) Restless or fidgety?(factor loading = .6819), (d) Hopeless (factorloading = .7914), (e) That everything was an
effort (factor loading = .7155), or (f) Worthless(factor loading = .7440).’’ The responses rangefrom None of the time (coded 0) to All of thetime (coded 4). About 1.5% of respondents(n = 2, 837) had missing responses to theseitems. We used the single-imputation approachto impute those missing values based on age,gender, race, geographic region, education, fam-ily income, marital status, health status andsurvey year. The psychological distress scorewas constructed as a latent variable, with highervalues indicating higher levels of distress.
Health behaviors. We included three measuresof health behaviors: (a) smoking, (b) drinking,and (c) vigorous exercise. Smoking was mea-sured as a categorical variable: never smoked(the reference), current smoker, former smoker,and unknown smoking status. Drinking alsowas measured as a categorical variable: life-time abstainer (the reference), current drinker,former drinker, and unknown drinking status.Exercise was measured on the basis of the surveyquestion that asked about frequency of vigorousactivities longer than 10 min every week. Werecoded the response into six categories: (a) noexercise (the reference), (b) less than once aweek, (c) once a week, (d) two or three timesa week, (e) more than three times a week, and(f) unknown exercise status.
Other covariates included age at the baselinesurvey (in years), age at the baseline surveysquared, education (no high school diploma,high school graduate, some college, and col-lege graduate, with college graduate as thereference), and geographic region (Northeast,Midwest, South, and West, with Northeast as thereference). We also controlled for survey year(centered at 1997) to take into account the pooledmultiple years of NHIS. To control for the possi-bility that people in poorer health are more likelyto be selected into cohabitation rather than mar-riage, we included a measure of self-rated healthwith five categories: (a) excellent, (b) very good,(c) good, (d) fair, and (e) poor (the reference).In addition, previous research suggests that themeaning of the term cohabitation varies by age(Chevan, 1996; King & Scott, 2005). To controlfor the potential age variations in the mortal-ity links with cohabitation, we further includedinteraction terms of Union status × Age in themodels. Because the NHIS is a cross-sectionalsurvey, all analyzed variables were drawn fromthe baseline survey conducted between 1997 and

800 Journal of Marriage and Family
2004 except mortality data, which were takenfrom the mortality follow-up files.
Statistical Methods
Because the meanings and processes of cohabi-tation are fundamentally different across genderand racial groups (Thornton et al., 2007), weconducted analyses separately for White men,White women, Black men, and Black women.Within each gender and racial subgroup, we esti-mated a set of Cox proportional hazards models.In the first model, we examined the generalrelationship between cohabitation and mortal-ity, controlling for only the basic sociodemo-graphic covariates (i.e., age at baseline survey,age at baseline survey squared, age interac-tions with union status, survey year, education,and geographic region). We then added fam-ily income, psychological distress, and healthbehaviors separately as additional covariates toexamine whether such factors explain mortal-ity differences by union status. A reductionin the significance level and/or magnitude ofthe effect of union status across models wouldsuggest that the potential mechanism variablesexplain the association between cohabitation andmortality.
We used age at death as the analysis timescale to best control for the effect of age onmortality rates (see Singer & Willett, 2003).Age at death is measured in 1/4-year units—thesmallest unit available in the public versionsof the NHIS-LMF data. The mortality hazardfunction in our models reflects the mortality rateacross age. Cox models assume that the hazardfunction has a constant shape for all individuals,although there is no assumption about the exactshape of the shared hazard function. Results (notshown but available on request) from the chi-square test based on scaled Schoenfeld residualsrevealed little variation of this proportional haz-ards assumption. The Cox model we estimatedcan be specified as follows:
loghi(t)
h0(t)=
∑βjMj +
∑πkXk, (1)
where t represents the analytic time metric—theparticipants’ age; hi(t) is the resultant death haz-ard of the ith individual at age t ; h0(t) is thebaseline hazard at age t ; Mj represents the set ofunion status dummy variables; and βj representsthe corresponding coefficients (cohabiting is the
reference group); Xk stands for the other covari-ates included in the model; and πk represents thecorresponding coefficients. The βj values areof greatest interest for this study because theyreflect mortality differences between cohabitersand other union status groups.
RESULTS
We first report, in Table 1, descriptive statis-tics of all analyzed variables for White men,White women, Black men, and Black women.The results in Table 1 suggest that Black menhad the highest proportion of deaths and weremore likely to cohabit than other gender andracial subgroups. Black men and women wereless likely to be married and more likely to livein the South than White men and women. Whitemen were the most likely to be college gradu-ates, followed by White women, Black women,and Black men. White men and women wereolder, were less likely to report poor health, andhad higher levels of family income than Blackmen and women. In comparison to their femalecounterparts, White men and Black men weremore likely to be current smokers and drinkers,more likely to exercise, and tended to reportlower levels of psychological distress.
General Relationship Between Cohabitationand Mortality Across Gender and Race
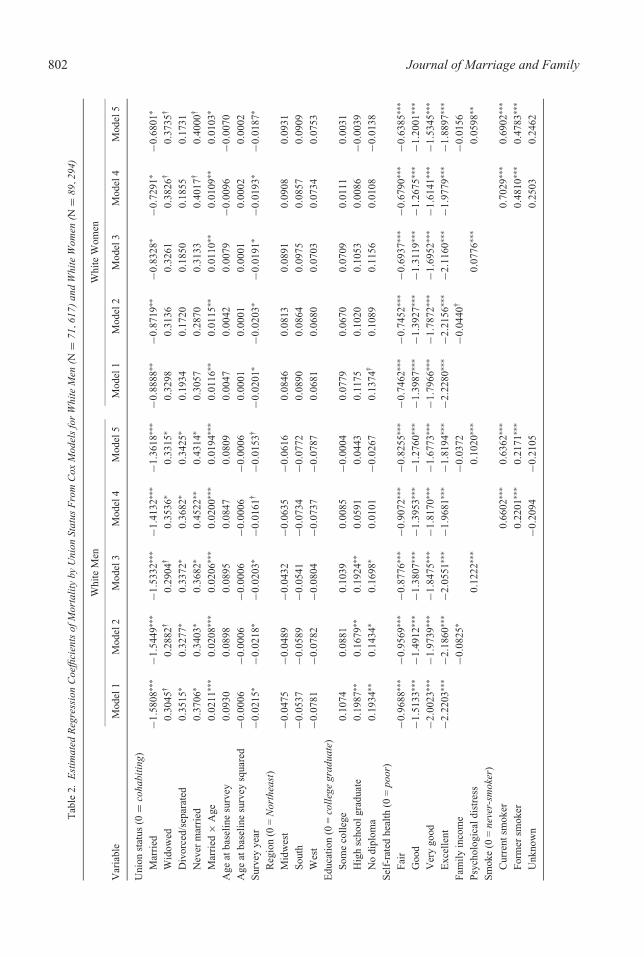
We now turn to the results from the Cox regres-sion models. The results in Tables 2 and 3show the estimated regression coefficients formortality by union status from five Cox mod-els for White men, White women, Black men,and Black women separately. We first discussthe results from Model 1 of Tables 2 and 3that controlled for the basic sociodemographiccovariates. The results from Model 1 in Table 2suggest that married White men and Whitewomen had lower mortality than their cohab-iting counterparts; specifically, the mortalityhazard was 79.42% (i.e., [1 − e1.5808] × 100)and 58.89% (i.e., [1 − e−0.8888] × 100) lower formarried White men and married White women,respectively, in comparison to their cohabitingcounterparts. For both White men and women,the significant age interaction effects with mar-ried individuals suggest that the mortality dif-ferences between married people and cohabiterstended to decrease with age. The gap convergedaround age 75 (i.e., 1.5808/0.0211) for White

Cohabitation and U.S. Adult Mortality 801
Table 1. Weighted Descriptive Statistics
Variable White Men White Women Black Men Black Women
Total no. observations 71,617 89,294 12,503 20,437Total no. deaths 2,903 3,023 558 629% of deaths 4.05 3.39 4.46 3.08Union status (%)
Cohabiting 5.49 5.21 8.13 5.21Married 62.88 58.83 42.87 29.89Widowed 2.81 11.14 3.05 10.68Divorced/separated 9.43 11.5 14.43 20.22Never married 19.38 13.32 31.52 34.00
Region (%)Northeast 19.95 20.75 15.42 17.05Midwest 29.18 28.73 18.20 19.37South 34.32 34.04 58.44 56.97West 16.55 16.47 7.94 6.61
Education (%)College graduate 27.79 23.98 13.23 14.49Some college 29.12 31.17 30.64 31.53High school graduate 29.88 31.73 32.53 30.18No diploma 13.21 13.12 23.60 23.80
Self-rated health (%)Poor 2.69 2.93 4.06 4.55Fair 7.65 8.52 11.96 14.30Good 22.89 24.81 25.80 29.72Very good 32.87 33.27 28.80 28.38Excellent 33.90 30.47 29.38 23.05
Smoking (%)Never smoked 44.58 55.29 54.01 67.78Current smoker 25.66 22.51 27.62 19.83Former smoker 29.25 21.77 17.5 11.79Unknown 0.50 0.44 0.87 0.61
Drinking (%)Lifetime abstainer 12.50 22.86 23.74 41.10Current drinker 70.68 60.91 56.72 41.44Former drinker 15.36 15.05 17.36 16.06Unknown 1.46 1.18 2.18 1.40
Exercise (%)No exercise 53.30 64.71 57.87 74.71Less than once a week 3.44 2.39 2.59 2.12Once a week 6.98 4.72 6.21 3.49Two or three times a week 16.31 14.11 15.81 10.66More than three times a week 18.82 13.17 16.43 8.23Unknown 1.15 0.92 1.08 0.78
Mean age at the baseline survey 45.67 47.38 41.45 42.64Median family income 46,355.83 41,065.22 34,015.61 30,798.91Mean of psychological distress −0.10 0.03 −0.10 0.08
Note: Total numbers of observations and deaths are unweighted. All other statistics are weighted.
men and 77 (i.e., 0.8888/0.0116) for Whitewomen. Age interactions with other union statuswere not significant and thus are not included inthe final reported models.
The results from Model 1 in Table 2 fur-ther suggest that, in comparison to cohab-iting White men, the mortality hazard was42.12% (i.e., [e0.3515 − 1] × 100) higher for
802 Journal of Marriage and FamilyT
able
2.E
stim
ated
Reg
ress
ion
Coe
ffici
ents
ofM
orta
lity
byU
nion
Stat
usF
rom
Cox
Mod
els
for
Whi
teM
en(N
=71
,61
7)an
dW
hite
Wom
en(N
=89
,29
4)
Whi
teM
enW
hite
Wom
en
Var
iabl
eM
odel
1M
odel
2M
odel
3M
odel
4M
odel
5M
odel
1M
odel
2M
odel
3M
odel
4M
odel
5
Uni
onst
atus
(0=
coha
bitin
g)M
arri
ed−1
.580
8∗∗∗
−1.5
449∗
∗∗−1
.533
2∗∗∗
−1.4
132∗
∗∗−1
.361
8∗∗∗
−0.8
888∗
∗−0
.871
9∗∗
−0.8
328∗
−0.7
291∗
−0.6
801∗
Wid
owed
0.30
45†
0.28
82†
0.29
04†
0.35
36∗
0.33
15∗
0.32
980.
3136
0.32
610.
3826
†0.
3735
†
Div
orce
d/se
para
ted
0.35
15∗
0.32
77∗
0.33
72∗
0.36
82∗
0.34
25∗
0.19
340.
1720
0.18
500.
1855
0.17
31N
ever
mar
ried
0.37
06∗
0.34
03∗
0.36
82∗
0.45
22∗∗
0.43
14∗
0.30
570.
2870
0.31
330.
4017
†0.
4000
†
Mar
ried
×A
ge0.
0211
∗∗∗
0.02
08∗∗
∗0.
0206
∗∗∗
0.02
00∗∗
∗0.
0194
∗∗∗
0.01
16∗∗
0.01
15∗∗
0.01
10∗∗
0.01
09∗∗
0.01
03∗
Age
atba
selin
esu
rvey
0.09
300.
0898
0.08
950.
0847
0.08
090.
0047
0.00
420.
0079
−0.0
096
−0.0
070
Age
atba
selin
esu
rvey
squa
red
−0.0
006
−0.0
006
−0.0
006
−0.0
006
−0.0
006
0.00
010.
0001
0.00
010.
0002
0.00
02Su
rvey
year
−0.0
215∗
−0.0
218∗
−0.0
203∗
−0.0
161†
−0.0
153†
−0.0
201∗
−0.0
203∗
−0.0
191∗
−0.0
193∗
−0.0
187∗
Reg
ion
(0=
Nor
thea
st)
Mid
wes
t−0
.047
5−0
.048
9−0
.043
2−0
.063
5−0
.061
60.
0846
0.08
130.
0891
0.09
080.
0931
Sout
h−0
.053
7−0
.058
9−0
.054
1−0
.073
4−0
.077
20.
0890
0.08
640.
0975
0.08
570.
0909
Wes
t−0
.078
1−0
.078
2−0
.080
4−0
.073
7−0
.078
70.
0681
0.06
800.
0703
0.07
340.
0753
Edu
catio
n(0
=co
llege
grad
uate
)So
me
colle
ge0.
1074
0.08
810.
1039
0.00
85−0
.000
40.
0779
0.06
700.
0709
0.01
110.
0031
Hig
hsc
hool
grad
uate
0.19
87∗∗
0.16
79∗∗
0.19
24∗∗
0.05
910.
0443
0.11
750.
1020
0.10
530.
0086
−0.0
039
No
dipl
oma
0.19
34∗∗
0.14
34∗
0.16
98∗
0.01
01−0
.026
70.
1374
†0.
1089
0.11
560.
0108
−0.0
138
Self
-rat
edhe
alth
(0=
poor
)Fa
ir−0
.968
8∗∗∗
−0.9
569∗
∗∗−0
.877
6∗∗∗
−0.9
072∗
∗∗−0
.825
5∗∗∗
−0.7
462∗
∗∗−0
.745
2∗∗∗
−0.6
937∗
∗∗−0
.679
0∗∗∗
−0.6
385∗
∗∗
Goo
d−1
.513
3∗∗∗
−1.4
912∗
∗∗−1
.380
7∗∗∗
−1.3
953∗
∗∗−1
.276
0∗∗∗
−1.3
987∗
∗∗−1
.392
7∗∗∗
−1.3
119∗
∗∗−1
.267
5∗∗∗
−1.2
001∗
∗∗
Ver
ygo
od−2
.002
3∗∗∗
−1.9
739∗
∗∗−1
.847
5∗∗∗
−1.8
170∗
∗∗−1
.677
3∗∗∗
−1.7
966∗
∗∗−1
.787
2∗∗∗
−1.6
952∗
∗∗−1
.614
1∗∗∗
−1.5
345∗
∗∗
Exc
elle
nt−2
.220
3∗∗∗
−2.1
860∗
∗∗−2
.055
1∗∗∗
−1.9
681∗
∗∗−1
.819
4∗∗∗
−2.2
280∗
∗∗−2
.215
6∗∗∗
−2.1
160∗
∗∗−1
.977
9∗∗∗
−1.8
897∗
∗∗
Fam
ilyin
com
e−0
.082
5∗−0
.037
2−0
.044
0†−0
.015
6Ps
ycho
logi
cald
istr
ess
0.12
22∗∗
∗0.
1020
∗∗∗
0.07
76∗∗
∗0.
0598
∗∗
Smok
e(0
=ne
ver-
smok
er)
Cur
rent
smok
er0.
6602
∗∗∗
0.63
62∗∗
∗0.
7029
∗∗∗
0.69
02∗∗
∗
Form
ersm
oker
0.22
01∗∗
∗0.
2171
∗∗∗
0.48
10∗∗
∗0.
4783
∗∗∗
Unk
now
n−0
.209
4−0
.210
50.
2503
0.24
62
Cohabitation and U.S. Adult Mortality 803T
able
2.C
ontin
ued
Whi
teM
enW
hite
Wom
en
Var
iabl
eM
odel
1M
odel
2M
odel
3M
odel
4M
odel
5M
odel
1M
odel
2M
odel
3M
odel
4M
odel
5
Dri
nk(0
=lif
etim
eab
stai
ner)
Cur
rent
drin
ker
−0.0
388
−0.0
364
−0.2
783∗
∗∗−0
.276
9∗∗∗
Form
erdr
inke
r0.
1681
∗∗0.
1662
∗0.
0335
0.02
87U
nkno
wn
0.20
440.
1908
0.02
380.
0178
Exe
rcis
e(0
=no
exer
cise
)L
ess
than
once
aw
eek
−0.0
621
−0.0
506
−0.2
824
−0.2
815
Onc
ea
wee
k−0
.666
4∗∗∗
−0.6
507∗
∗∗−0
.522
7∗−0
.518
5∗
Tw
oor
thre
etim
esa
wee
k−0
.606
5∗∗∗
−0.5
959∗
∗∗−0
.485
0∗∗∗
−0.4
793∗
∗∗
Mor
eth
anth
ree
times
aw
eek
−0.4
682∗
∗∗−0
.460
5∗∗∗
−0.4
561∗
∗∗−0
.452
3∗∗∗
Unk
now
n−0
.311
9−0
.330
0−0
.479
8−0
.475
3
Not
e:A
gein
tera
ctio
nsw
ithot
her
unio
nst
atus
wer
eno
tsig
nific
anti
nth
epr
elim
inar
yan
alys
isan
dth
usno
tinc
lude
din
the
final
repo
rted
mod
els.
†p
<.1
0.∗ p
<.0
5.∗∗
p<
.01.
∗∗∗ p
<.0
01.
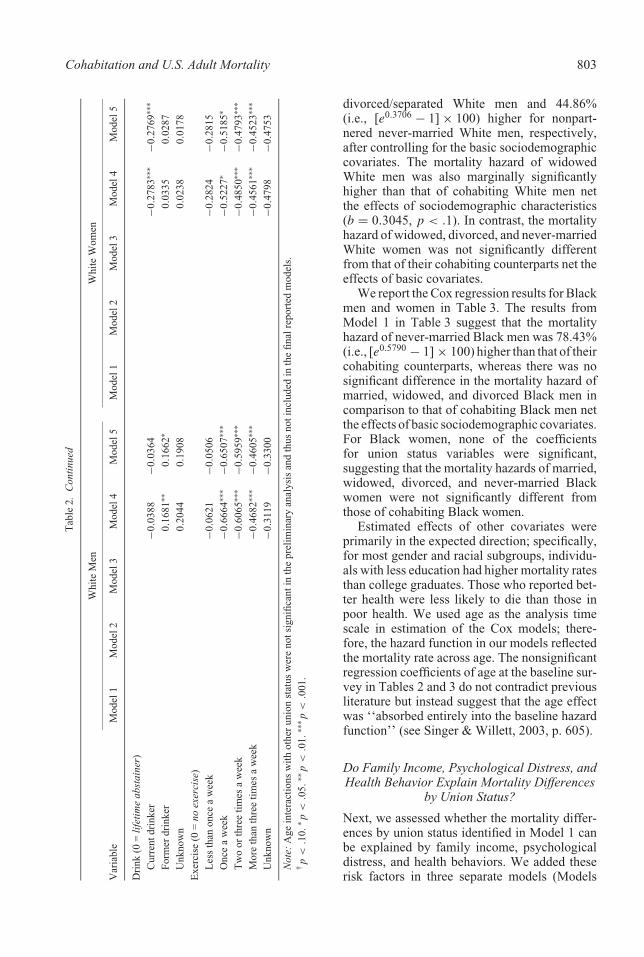
divorced/separated White men and 44.86%(i.e., [e0.3706 − 1] × 100) higher for nonpart-nered never-married White men, respectively,after controlling for the basic sociodemographiccovariates. The mortality hazard of widowedWhite men was also marginally significantlyhigher than that of cohabiting White men netthe effects of sociodemographic characteristics(b = 0.3045, p < .1). In contrast, the mortalityhazard of widowed, divorced, and never-marriedWhite women was not significantly differentfrom that of their cohabiting counterparts net theeffects of basic covariates.
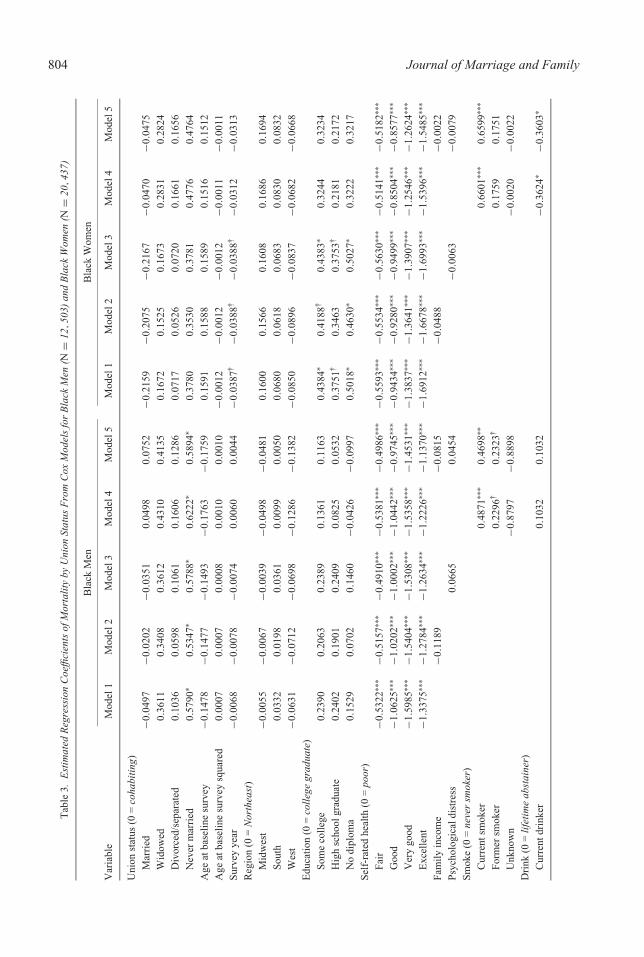
We report the Cox regression results for Blackmen and women in Table 3. The results fromModel 1 in Table 3 suggest that the mortalityhazard of never-married Black men was 78.43%(i.e., [e0.5790 − 1] × 100) higher than that of theircohabiting counterparts, whereas there was nosignificant difference in the mortality hazard ofmarried, widowed, and divorced Black men incomparison to that of cohabiting Black men netthe effects of basic sociodemographic covariates.For Black women, none of the coefficientsfor union status variables were significant,suggesting that the mortality hazards of married,widowed, divorced, and never-married Blackwomen were not significantly different fromthose of cohabiting Black women.
Estimated effects of other covariates wereprimarily in the expected direction; specifically,for most gender and racial subgroups, individu-als with less education had higher mortality ratesthan college graduates. Those who reported bet-ter health were less likely to die than those inpoor health. We used age as the analysis timescale in estimation of the Cox models; there-fore, the hazard function in our models reflectedthe mortality rate across age. The nonsignificantregression coefficients of age at the baseline sur-vey in Tables 2 and 3 do not contradict previousliterature but instead suggest that the age effectwas ‘‘absorbed entirely into the baseline hazardfunction’’ (see Singer & Willett, 2003, p. 605).
Do Family Income, Psychological Distress, andHealth Behavior Explain Mortality Differences
by Union Status?
Next, we assessed whether the mortality differ-ences by union status identified in Model 1 canbe explained by family income, psychologicaldistress, and health behaviors. We added theserisk factors in three separate models (Models
804 Journal of Marriage and FamilyT
able
3.E
stim
ated
Reg
ress
ion
Coe
ffici
ents
ofM
orta
lity
byU
nion
Stat
usF
rom
Cox
Mod
els
for
Bla
ckM
en(N
=12
,50
3)an
dB
lack
Wom
en(N
=20
,43
7)
Bla
ckM
enB
lack
Wom
en
Var
iabl
eM
odel
1M
odel
2M
odel
3M
odel
4M
odel
5M
odel
1M
odel
2M
odel
3M
odel
4M
odel
5
Uni
onst
atus
(0=
coha
bitin
g)M
arri
ed−0
.049
7−0
.020
2−0
.035
10.
0498
0.07
52−0
.215
9−0
.207
5−0
.216
7−0
.047
0−0
.047
5W
idow
ed0.
3611
0.34
080.
3612
0.43
100.
4135
0.16
720.
1525
0.16
730.
2831
0.28
24D
ivor
ced/
sepa
rate
d0.
1036
0.05
980.
1061
0.16
060.
1286
0.07
170.
0526
0.07
200.
1661
0.16
56N
ever
mar
ried
0.57
90∗
0.53
47∗
0.57
88∗
0.62
22∗
0.58
94∗
0.37
800.
3530
0.37
810.
4776
0.47
64A
geat
base
line
surv
ey−0
.147
8−0
.147
7−0
.149
3−0
.176
3−0
.175
90.
1591
0.15
880.
1589
0.15
160.
1512
Age
atba
selin
esu
rvey
squa
red
0.00
070.
0007
0.00
080.
0010
0.00
10−0
.001
2−0
.001
2−0
.001
2−0
.001
1−0
.001
1Su
rvey
year
−0.0
068
−0.0
078
−0.0
074
0.00
600.
0044
−0.0
387†
−0.0
388†
−0.0
388†
−0.0
312
−0.0
313
Reg
ion
(0=
Nor
thea
st)
Mid
wes
t−0
.005
5−0
.006
7−0
.003
9−0
.049
8−0
.048
10.
1600
0.15
660.
1608
0.16
860.
1694
Sout
h0.
0332
0.01
980.
0361
0.00
990.
0050
0.06
800.
0618
0.06
830.
0830
0.08
32W
est
−0.0
631
−0.0
712
−0.0
698
−0.1
286
−0.1
382
−0.0
850
−0.0
896
−0.0
837
−0.0
682
−0.0
668
Edu
catio
n(0
=co
llege
grad
uate
)So
me
colle
ge0.
2390
0.20
630.
2389
0.13
610.
1163
0.43
84∗
0.41
88†
0.43
83∗
0.32
440.
3234
Hig
hsc
hool
grad
uate
0.24
020.
1901
0.24
090.
0825
0.05
320.
3751
†0.
3463
0.37
53†
0.21
810.
2172
No
dipl
oma
0.15
290.
0702
0.14
60−0
.042
6−0
.099
70.
5018
∗0.
4630
∗0.
5027
∗0.
3222
0.32
17Se
lf-r
ated
heal
th(0
=po
or)
Fair
−0.5
322∗
∗∗−0
.515
7∗∗∗
−0.4
910∗
∗∗−0
.538
1∗∗∗
−0.4
986∗
∗∗−0
.559
3∗∗∗
−0.5
534∗
∗∗−0
.563
0∗∗∗
−0.5
141∗
∗∗−0
.518
2∗∗∗
Goo
d−1
.062
5∗∗∗
−1.0
202∗
∗∗−1
.000
2∗∗∗
−1.0
442∗
∗∗−0
.974
5∗∗∗
−0.9
434∗
∗∗−0
.928
0∗∗∗
−0.9
499∗
∗∗−0
.850
4∗∗∗
−0.8
577∗
∗∗
Ver
ygo
od−1
.598
5∗∗∗
−1.5
404∗
∗∗−1
.530
8∗∗∗
−1.5
358∗
∗∗−1
.453
1∗∗∗
−1.3
837∗
∗∗−1
.364
1∗∗∗
−1.3
907∗
∗∗−1
.254
6∗∗∗
−1.2
624∗
∗∗
Exc
elle
nt−1
.337
5∗∗∗
−1.2
784∗
∗∗−1
.263
4∗∗∗
−1.2
226∗
∗∗−1
.137
0∗∗∗
−1.6
912∗
∗∗−1
.667
8∗∗∗
−1.6
993∗
∗∗−1
.539
6∗∗∗
−1.5
485∗
∗∗
Fam
ilyin
com
e−0
.118
9−0
.081
5−0
.048
8−0
.002
2Ps
ycho
logi
cald
istr
ess
0.06
650.
0454
−0.0
063
−0.0
079
Smok
e(0
=ne
ver
smok
er)
Cur
rent
smok
er0.
4871
∗∗∗
0.46
98∗∗
0.66
01∗∗
∗0.
6599
∗∗∗
Form
ersm
oker
0.22
96†
0.23
23†
0.17
590.
1751
Unk
now
n−0
.879
7−0
.889
8−0
.002
0−0
.002
2D
rink
(0=
lifet
ime
abst
aine
r)C
urre
ntdr
inke
r0.
1032
0.10
32−0
.362
4∗−0
.360
3∗

Cohabitation and U.S. Adult Mortality 805T
able
3.C
ontin
ued
Bla
ckM
enB
lack
Wom
en
Var
iabl
eM
odel
1M
odel
2M
odel
3M
odel
4M
odel
5M
odel
1M
odel
2M
odel
3M
odel
4M
odel
5
Form
erdr
inke
r0.
0152
0.00
460.
0190
0.02
07U
nkno
wn
−0.2
167
−0.2
054
0.41
250.
4127
Exe
rcis
e(0
=no
exer
cise
)L
ess
than
once
aw
eek
0.51
150.
5209
−1.3
231
−1.3
243
Onc
ea
wee
k−0
.712
4−0
.707
2−1
.406
9∗−1
.406
9∗T
wo
orth
ree
times
aw
eek
−0.5
407†
−0.5
256†
−1.2
912∗
∗∗−1
.290
6∗∗∗
Mor
eth
anth
ree
times
aw
eek
−0.5
128†
−0.5
002
−0.2
887
−0.2
889
Unk
now
n−0
.858
6−0
.860
4−0
.493
4−0
.492
8
Not
e:A
gein
tera
ctio
nsw
ithun
ion
stat
uses
wer
eno
tsig
nific
anti
nth
epr
elim
inar
yan
alys
is,a
ndth
usno
tinc
lude
din
the
final
repo
rted
mod
els.
†p
<.1
0.∗ p
<.0
5.∗∗
p<
.01.
∗∗∗ p
<.0
01.
2 – 4) as additional covariates in Tables 2 and3 for each gender and racial subgroup. Theseresults suggest that, for both White men andwomen, family income was negatively relatedto mortality (Model 2) and psychological dis-tress was positively related to mortality (Model3). For all gender and racial subgroups, thosewho exercised more often tended to have lowermortality; and both current and former smokershad higher mortality than never-smokers (Model4). Former drinkers had higher mortality thanlifetime abstainers among White men, whereascurrent drinkers had lower mortality than life-time abstainers among White women and Blackwomen (Model 4).
All of the union status differences in mortal-ity identified in Model 1 remained statisticallysignificant after these potential mechanism vari-ables were controlled for separately in Models 2through 4. This suggests that family income, psy-chological distress, and health behavior did notfully explain the identified mortality differences,yet we did find some partial reductions in the sig-nificance of these differences once we controlledfor these factors. We controlled for all covariates(including sociodemographic, family income,psychological distress, and health behavior vari-ables) in our final model, Model 5, in Tables 2and 3. These results suggest that after all covari-ates were controlled for, the mortality hazardsof widowed, divorced, and never-married Whitemen and of never-married Black men were sig-nificantly higher than that of their cohabitingcounterparts; the mortality hazards of marriedWhite men and White women were significantlylower than that of their cohabiting counterparts.
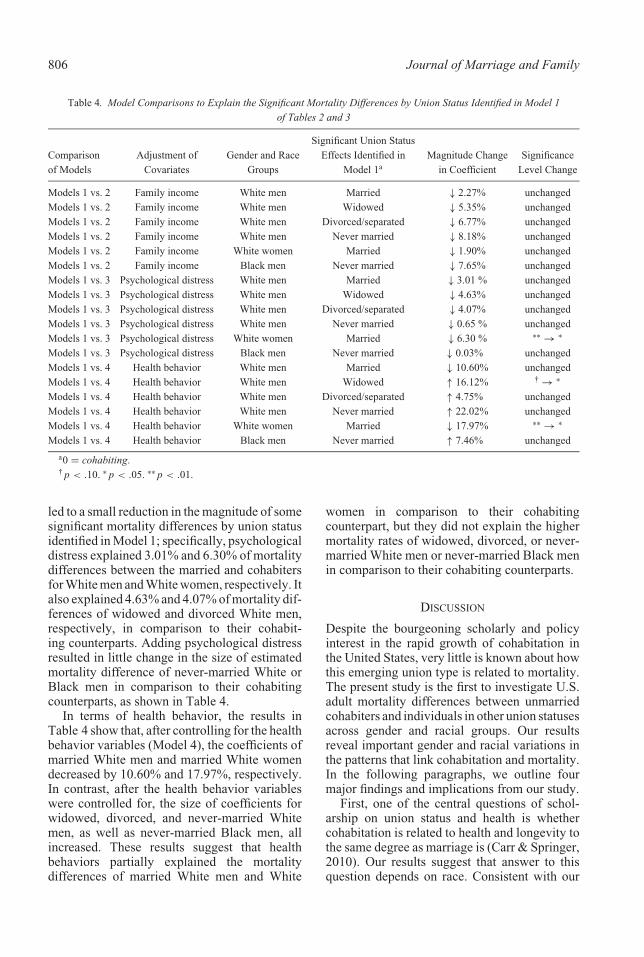
Table 4 summarizes results for comparisonsof union status effects on mortality from Models2 through 4 versus Model 1. As summarizedin Table 4, after family income was added(Model 2), the coefficient for married indi-viduals decreased by 2.27% (i.e., [1.5808 −1.5449]/1.5808) for White men and 1.90% forWhite women in comparison to their cohabitingcounterparts. Moreover, after family income wasadded (Model 2), the coefficients for widowed,divorced, and never-married White men, aswell for never-married Black men, decreased by5.35%, 6.77%, 8.18%, and 7.65%, respectively.These results suggest that cohabiters had differ-ent mortality rates in comparison to other unionstatus groups in some part because they haddifferent levels of family income. Similarly, theaddition of psychological distress (Model 3) also
806 Journal of Marriage and Family
Table 4. Model Comparisons to Explain the Significant Mortality Differences by Union Status Identified in Model 1of Tables 2 and 3
Comparisonof Models
Adjustment ofCovariates
Gender and RaceGroups
Significant Union StatusEffects Identified in
Model 1aMagnitude Change
in CoefficientSignificance
Level Change
Models 1 vs. 2 Family income White men Married ↓ 2.27% unchangedModels 1 vs. 2 Family income White men Widowed ↓ 5.35% unchangedModels 1 vs. 2 Family income White men Divorced/separated ↓ 6.77% unchangedModels 1 vs. 2 Family income White men Never married ↓ 8.18% unchangedModels 1 vs. 2 Family income White women Married ↓ 1.90% unchangedModels 1 vs. 2 Family income Black men Never married ↓ 7.65% unchangedModels 1 vs. 3 Psychological distress White men Married ↓ 3.01 % unchangedModels 1 vs. 3 Psychological distress White men Widowed ↓ 4.63% unchangedModels 1 vs. 3 Psychological distress White men Divorced/separated ↓ 4.07% unchangedModels 1 vs. 3 Psychological distress White men Never married ↓ 0.65 % unchangedModels 1 vs. 3 Psychological distress White women Married ↓ 6.30 % ∗∗ → ∗
Models 1 vs. 3 Psychological distress Black men Never married ↓ 0.03% unchangedModels 1 vs. 4 Health behavior White men Married ↓ 10.60% unchangedModels 1 vs. 4 Health behavior White men Widowed ↑ 16.12% † → ∗
Models 1 vs. 4 Health behavior White men Divorced/separated ↑ 4.75% unchangedModels 1 vs. 4 Health behavior White men Never married ↑ 22.02% unchangedModels 1 vs. 4 Health behavior White women Married ↓ 17.97% ∗∗ → ∗
Models 1 vs. 4 Health behavior Black men Never married ↑ 7.46% unchanged
a0 = cohabiting.†p < .10. ∗p < .05. ∗∗p < .01.
led to a small reduction in the magnitude of somesignificant mortality differences by union statusidentified in Model 1; specifically, psychologicaldistress explained 3.01% and 6.30% of mortalitydifferences between the married and cohabitersfor White men and White women, respectively. Italso explained 4.63% and 4.07% of mortality dif-ferences of widowed and divorced White men,respectively, in comparison to their cohabit-ing counterparts. Adding psychological distressresulted in little change in the size of estimatedmortality difference of never-married White orBlack men in comparison to their cohabitingcounterparts, as shown in Table 4.
In terms of health behavior, the results inTable 4 show that, after controlling for the healthbehavior variables (Model 4), the coefficients ofmarried White men and married White womendecreased by 10.60% and 17.97%, respectively.In contrast, after the health behavior variableswere controlled for, the size of coefficients forwidowed, divorced, and never-married Whitemen, as well as never-married Black men, allincreased. These results suggest that healthbehaviors partially explained the mortalitydifferences of married White men and White
women in comparison to their cohabitingcounterpart, but they did not explain the highermortality rates of widowed, divorced, or never-married White men or never-married Black menin comparison to their cohabiting counterparts.
DISCUSSION
Despite the bourgeoning scholarly and policyinterest in the rapid growth of cohabitation inthe United States, very little is known about howthis emerging union type is related to mortality.The present study is the first to investigate U.S.adult mortality differences between unmarriedcohabiters and individuals in other union statusesacross gender and racial groups. Our resultsreveal important gender and racial variations inthe patterns that link cohabitation and mortality.In the following paragraphs, we outline fourmajor findings and implications from our study.
First, one of the central questions of schol-arship on union status and health is whethercohabitation is related to health and longevity tothe same degree as marriage is (Carr & Springer,2010). Our results suggest that answer to thisquestion depends on race. Consistent with our

Cohabitation and U.S. Adult Mortality 807
hypothesis regarding race differences, we foundthat the mortality of married White men andwomen was lower than that of their cohab-iting White counterparts, but there were nosignificant mortality differences between mar-ried Black men and women in comparison totheir cohabiting Black counterparts. This find-ing is consistent with research suggesting thatcohabitation and marriage have very differentmeanings for Whites and Blacks, whereby mar-riage confers different social, economic, andpsychological experiences across racial groups(Brown et al., 2008; Thornton et al. 2007).Whites are more likely to see cohabitation asa trial marriage (Brown et al., 2008; Thorntonet al.), which may mean lower levels of sharedsocial, psychological, and economic resources.In contrast, cohabitation is more prevalent andis perceived as an alternative to marriage forBlacks (Brown et al., 2008; Thornton et al.);thus, cohabitation may mirror the dynamics ofmarriage and promote health in capacities simi-lar to marriage. It is also likely that, because oflower levels of earnings for both Black men andBlack women compared to their White counter-parts, marriage may not confer the same degreeof social and economic benefits for Blacks asfor Whites (Edin & Kefalas, 2005). Therefore,Black cohabiting men and women may moreeasily match their married counterparts on thesesocial and economic components that promotehealth. Alternatively, because cohabitation ismore common among Blacks, it is possible thatthe selection of people in poorer health intocohabitation, rather than marriage, is less rele-vant for Blacks compared to Whites.
Second, we found that the mortality advantageof married White men and women in comparisonto their cohabiting counterparts decreased withage. This finding is consistent with previousresearch suggesting that marital status is astronger predictor of mortality at younger ages,when marital roles are more central (Gove, 1973;Mineau, Smith, & Bean, 2002). Researchershave suggested that the meaning, context,and motivations for cohabitation vary by age(Chevan, 1996; King & Scott, 2005). Oldercohabiters (i.e., age 50+) report higher levels ofstability and relationship quality and are morelikely to have been previously married thanyounger cohabiters (Brown, Lee, & Bulanda,2006; Bumpass & Lu, 2000; King & Scott).This suggests that having been previouslymarried changes the expectations for intimate
relationships; older individuals who do not wishto remarry after an earlier divorce may viewcohabitation as a marriage-like union (King &Scott) and thus receive a marriage-like boostin mortality. In contrast, younger couples aremore likely to see their cohabiting unions as aprecursor to marriage (King & Scott), suggestingthat the processes of cohabitation will be lesslikely to promote health and longevity. Thedecreasing mortality difference between themarried and cohabiters may also, however,reflect selection processes. Cohabiters facehigher mortality rates than married individuals,and this process of mortality selection wouldleave a more robust cohabiting subpopulation atolder ages.
Third, although cohabitation was related tohigher mortality in comparison to marriageamong Whites, our results suggest that Whiteand Black cohabiting men tended to have lowermortality compared to their unpartnered coun-terparts. Previous studies on health and familystatus typically combine cohabiters within otherunion status groups—such as the never-married,divorced, or widowed—without distinguishingcohabiting and unpartnered individuals (Liu &Umberson, 2008), yet there is reason to believethat there are important differences among thesegroups and that these differences shape mortalityrisk (Carr & Springer, 2010). In line with a grow-ing body of research highlighting the diversity ofthe unmarried category (Liu, 2009), our resultsrevealed higher mortality for White and Blacksingle men—but, notably, not White and Blacksingle women—in comparison to their cohabit-ing counterparts. This finding is consistent withprevious research that suggests any union—cohabiting or married—is more important formen’s mortality than women’s (Gove, 1973;Liu). Our results suggest that cohabitation maypromote longevity for men in similar ways asmarriage, albeit to a lesser degree. These resultsalso call for family researchers to seriouslyconsider the heterogeneity of the nonmarriedgroup across race and gender in their futureresearch.
Fourth and finally, our results provide pre-viously unexplored evidence on the role ofkey psychological, social, and economic mech-anisms through which cohabitation is linked tomortality. Past research suggests that cohab-iters tend to live less healthy lifestyles (Fuller,2010; Horwitz & White, 1998), enjoy fewereconomic benefits (Brines & Joyner, 1999), and

808 Journal of Marriage and Family
experience more relationship strain and psy-chological distress (Brown, 2000)—all factorsthat may lead to higher mortality—than mar-ried individuals. Our results suggest that, in ourstudy, these economic, social, and psychologicalfactors operated together to explain part of themortality differentials across gender and race,yet these factors failed to fully explain any of thesignificant mortality differences between cohab-iters and other union status groups. We expectedeconomic resources to explain the mortality dif-ferentials by union status for White women morethan for White men or Black men because ofdifferential earnings across racial and gendergroups (Cohen, 1999; Edin & Kefalas, 2005),yet we found that family income explained apart, but not all, of mortality differences byunion status in similar ways for White women,White men, and Black men. With an increasein women’s labor force participation, it is possi-ble that women’s roles in contributing to familyincome—and, in turn, mortality—have becomemore important over time (Oppenheimer, 1997).This suggests that women’s socioeconomicstatus may become more important to theirspouses’ health and mortality now than inthe past.
Given previous research indicating that mar-riage confers important psychological resourcesto men, but not to women (Ross et al., 1990),we expected that social psychological factorswould be one major variable that would explainthe relationship between union status and mor-tality for both White and Black men but not forwomen. We found that psychological distressexplained only a small portion of the mortal-ity differences for White married, divorced,and widowed men compared to their cohabit-ing counterparts but explained virtually none ofthe effect for White or Black never-married mencompared to their cohabiting counterparts. Sur-prisingly, we found that psychological distressexplained a portion of the mortality differencebetween White cohabiting and married women.This finding may reflect the fact that womenare more likely to report depressive symptomsthan men (Rosenfield, 1999). It may also bethe case that cohabiting White women wish tomarry but do not have access to a willing partner,causing strain and psychological distress; suchstrain may in turn affect their mortality (Edin &Kefalas, 2005). It may also be that women withlower levels of psychological distress, and thuslower mortality risk, are more likely to select
into marriage. Future research should explorethese possibilities.
In line with previous research indicating thatmen’s health behavior is more strongly shapedby union status, we expected that health behav-iors would explain another major part of therelationship between cohabitation and mortal-ity for men, but not women (Umberson, 1992).We found this to be the case for married Whitemen in comparison to their cohabiting coun-terparts, yet health behaviors did not explainthe mortality differences of White widowed,divorced, and never-married men in compari-son to their White cohabiting counterparts, orthe differences of Black never-married menin comparison to their Black cohabiting coun-terparts. Moreover, we surprisingly found thathealth behaviors explained a significant portion(about 18%) of mortality differences betweenmarried and cohabiting White women. Withrapid changes in gender ideology and socialnorms, women now tend to partake in riskyhealth behaviors to a greater extent than in thepast (Preston & Wang, 2006). It is possible thatwith the increase in women’s risky behaviors,marriage has become a more important source ofsocial control to regulate women’s health behav-iors in ways that have been historically found formen. Future research should explore the poten-tial changes in social control of health behaviorsprovided by marriage for men and women.
Taken together, our results suggest that noneof the examined economic, social, and psycho-logical factors can fully explain the identifiedmortality differences by union status across gen-der and racial groups. Various social, biological,psychological, and behavioral mechanisms worktogether to forge links between cohabitationand mortality. Future studies should examineother social psychological factors, such as socialand emotional support, relationship quality, andrelationship duration to assess the relative impor-tance of other potential explanations for thecohabitation links with mortality.
Limitations and Conclusions
This study has several limitations. First, wewere unable to identify union status transitionsusing data from the NHIS-LMF. The truncationof a mortality follow-up to a 3-year period(or 1 or 2 years in our unreported additionalanalysis) should lower the chance of unionstatus transitions; however, we cannot exclude

Cohabitation and U.S. Adult Mortality 809
the possibility that some respondents may nothave stayed in the same union status withinthe mortality follow-up period. Second, theNHIS-LMF links eligible adults in the NHISsurvey through probabilistic record linkage tothe NDI to obtain follow-up data on mortality.Issues such as incorrect matches may haveintroduced bias into the data. The effect of falsematches increases with the length of the follow-up period (Ingram, Lochner, & Cox, 2008).Nevertheless, the NHIS-LMF provides a uniqueopportunity to study how the link betweencohabitation and mortality differs by socialgroups. In general, the mortality estimationfrom the NHIS-LMF is quite consistent withthat of the U.S. population (Ingram et al.). Athird limitation is that, although we attempted totease out some selectivity effects of cohabitationon mortality by controlling for baseline healthand socioeconomic status, we were not fullyable to deal with selection issues with theNHIS data because these data are basedon cross-sectional surveys. To fully explorehow different selection and causal processescontribute to mortality differences by unionstatus, future studies should use longitudinaldata with adequate measures of potentialselection factors. In addition, the NHIS islimited by a lack of information on cohabitationexperiences prior to the survey, which may affectmortality. Although we grouped all cohabitersinto one category, family scholars shouldconsider the heterogeneity among cohabiters infuture research (Heuveline & Timberlake, 2004).For example, never-married cohabiters versuspreviously married cohabiters, or short- versuslong-term cohabiters, may live in different socialcontexts that influence mortality. Future studiesshould consider the duration and histories ofunion status in examining cohabitation andmortality by using alternative data sets.
Despite these limitations, this study makesan important contribution to the literature onunion status and mortality. This is the first studyto document U.S. adult mortality differencesbetween cohabiters and other union status groupsacross gender and racial groups. With the rapidgrowth of cohabitation in the United States,policymakers and scholars continue to questionwhether cohabitation and marriage promotewell-being in equivalent ways. Although someresearchers emphasize the similarity betweencohabitation and marriage (e.g., Musick &Bumpass, 2012), others view the rising trend
of cohabitation as a threat to population health(e.g., Waite & Gallagher, 2000). Our results onmortality differences by union status add to themixed evidence on these debates. Cohabitationmay not be as protective as marriage forlongevity, but it may provide some degreeof benefit in comparison to being single. Thecomplexity of this issue is further highlighted byour findings across gender and racial subgroups,suggesting that involvement in any intimateunion—in comparison to singlehood—is moreimportant for men’s mortality than women’s.Moreover, we emphasize that the type of union(e.g., marriage vs. cohabitation) may be moreimportant in affecting health and longevityfor Whites than for Blacks as well as moreimportant for younger individuals than for olderindividuals.
NOTE
We thank Debra Umberson and R. Kelly Raley for theirhelpful comments and advice on early drafts of this article.An earlier version of this article was presented at the 2011annual meeting of the Population Association of America,Washington, DC.
REFERENCES
Allison, P. (2001). Missing data. Thousand Oaks, CA:Sage.
Becker, G. S. (1981). A treatise on the family. Oxford,UK: Oxford University Press.
Brines, J., & Joyner, K. (1999). The ties thatbind: Principles of cohesion in cohabitation andmarriage. American Sociological Review, 64,333 – 355. doi:10.2307/2657490
Brown, S. L. (2000). The effect of union type on psy-chological well-being: Depression among cohab-iters versus marrieds. Journal of Health and SocialBehavior, 41, 241 – 255. doi:10.2307/2676319
Brown, S. L., Lee, G. R., & Bulanda, J. R. (2006).Cohabitation among older adults: A nationalportrait. Journals of Gerontology: Series B:Psychological Sciences and Social Sciences, 61,S71 – S79. doi:10.1093/geronb/61.2.S71
Brown, S. L., Van Hook, J., & Glick, J. E. (2008).Generational differences in cohabitation andmarriage in the U.S. Population Research andPolicy Review, 27, 531 – 550. doi:10.1007/s11113-008-9088-3
Bumpass, L., & Lu, H. (2000). Trends in cohabitationand implications for children’s family contexts inthe United States. Population Studies, 54, 29 – 41.doi:10.1080/713779060
Carr, D., & Springer, K. W. (2010). Advances infamilies and health research in the 21st century.
810 Journal of Marriage and Family
Journal of Marriage and Family, 72, 743 – 761.doi:10.1111/j.1741 – 3737.2010.00728.x
Cherlin, A. (2004). The deinstitutionalization ofAmerican marriage. Journal of Marriage and Fam-ily, 66, 848 – 861. doi:10.1111/j.0022-2445.2004.00058.x
Chevan, A. (1996). As cheaply as one: Cohabitationin the older population. Journal of Marriage andthe Family, 58, 656 – 667. doi:10.2307/353726
Cohen, P. N. (1999). Racial-ethnic and gender dif-ferences in returns to cohabitation and marriage:Evidence from the current population survey. Pop-ulation Division Working Paper No. 35, U.S.Census Bureau, Washington, DC.
Duncan, G. J., Wilkerson, B., & England, P. (2006).Cleaning up their act: The effects of marriage andcohabitation on licit and illicit drug use. Demog-raphy, 43, 691 – 710. doi:0.1353/dem.2006.0032
Edin, K., & Kefalas, M. (2005). Promises I can keep:Why poor women put motherhood before marriage.Berkeley: University of California Press.
Eggebeen, D. J. (2005). Cohabitation and exchangesof support. Social Forces, 83, 1097 – 1110.doi:10.1353/sof.2005.0027
Fuller, T. (2010). Relationship status, health, andhealth behavior: An examination of cohabitersand commuters. Sociological Perspectives, 53,221 – 245. doi:10.1525/sop.2010.53.2.221
Gove, W. R. (1973). Sex, marital status, and mortal-ity. American Journal of Sociology, 79, 45 – 67.doi:10.1086/225505
Gupta, S. (1999). The effects of transitions inmarital status transitions on men’s performance ofhousework. Journal of Marriage and the Family,61, 700 – 711. doi:10.2307/353571
Heaton, T. B. (2002). Factors contributing to increas-ing marital stability in the United States.Journal of Family Issues, 23, 392 – 409.doi:10.1177/0192513X02023003004
Heuveline, P., & Timberlake, J. M. (2004). Therole of cohabitation in family formation: TheUnited States in comparative perspective. Jour-nal of Marriage and Family, 66, 1214 – 1230.doi:10.1111/j.0022 – 2445.2004.00088.x
Horwitz, A. V., & White, H. R. (1998). The relation-ship of cohabitation and mental health: A study ofa young adult cohort. Journal of Marriage and theFamily, 60, 505 – 514. doi:10.2307/353865
Ingram, D. D., Lochner, K. A., & Cox, C. S. (2008).Mortality experience of the 1986 – 2000 NationalHealth Interview Survey Linked Mortality Filesparticipants. Hyattsville, MD: National Center forHealth Statistics.
Kennedy, S., & Bumpass, L. (2008). Cohabitationand children’s living arrangements: New estimatesfrom the United States. Demographic Research,19, 1663 – 1692. doi:0.4054/DemRes.2008.19.47
Kenney, C., & McLanahan, S. (2006). Why are cohab-iting relationships more violent than marriages?
Demography, 43, 127 – 140. doi:10.1353/dem.2006.0007
Kessler, R. C., Andrews, G., Colpe, L. J., Hiripi, E.,Mroczek, D. K., Normand, S-L. T., Walters, E. E.,& Zaslavsky, A. M. (2002). Short screening scalesto monitor population prevalences and trends innon-specific psychological distress. PsychologicalMedicine, 32, 959 – 976. doi:10.1017/S0033291702006074
King, V., & Scott, M. E. (2005). A comparisonof cohabiting relationships among older andyounger adults. Journal of Marriage and Family,67, 271 – 285. doi:10.1111/j.0022 – 2445.2005.00115.x
Koskinen, S., Joutsenniemi, K., Martelin, T., & Mar-tikainen, P. (2007). Mortality differences accord-ing to living arrangements. International Journalof Epidemiology, 36, 1255 – 1264. doi:10.1093/ije/dym212
Lillard, L. A., & Waite, L. J. (1995). Til deathdo us part: Marital disruption and mortality.American Journal of Sociology, 100, 1131 – 1156.doi:10.1086/230634
Liu, H. (2009). Till death do us part: Marital status andmortality trends, 1986 – 2000. Journal of Marriageand Family, 71, 1158 – 1173. doi:10.1111/j.1741-3737.2009.00661.x
Liu, H., & Umberson, D. (2008). The times theyare a changin’: Marital status and health dif-ferentials from 1972 to 2003. Journal ofHealth and Social Behavior, 49, 239 – 253.doi:0.1177/002214650804900301
Lund, R., Due, P., Modvig, J., Holstein, B. E., Dams-gaard, M. T., & Andersen, P. K. (2002). Cohabita-tion and marital status as predictors of mortality:An eight year follow-up study. Social Science& Medicine, 55, 673 – 679. doi:10.1016/S0277-9536(01)00219 – 2
Lund, R., Modvig, J., Due, P., & Holstein, B. E.(2000). Stability and change in structural socialrelations as predictor of mortality among elderlywomen and men. European Journal of Epidemi-ology, 16, 1087 – 1097. doi:10.1023/A:1010897810514
Mineau, G. P., Smith, K. R., & Bean, L. L. (2002).Historical trends of survival among widowsand widowers. Social Science & Medicine, 54,245 – 254. doi:10.1016/S0277-9536(01)00024 – 7
Musick, K., & Bumpass, L. (2012). Reexamining thecase for marriage: Union formation and changes inwell-being. Journal of Marriage and Family, 74,1 – 18. doi:0.1111/j.1741-3737.2011.00873.x
National Center for Health Statistics. (2004). NationalHealth Interview Survey—Multiple Cause of DeathPublic Use Data File: 1986 – 2000 survey years.Hyattsville, MD: National Center for HealthStatistics.
Oppenheimer, V. K. (1997). Women’s employmentand the gain to marriage: The specialization and

Cohabitation and U.S. Adult Mortality 811
trading model. Annual Review of Sociology, 23,431 – 453. doi:10.1146/annurev.soc.23.1.431
Preston, S. H., & Wang, H. (2006). Sex mortalitydifferentials in the United States: The role of cohortsmoking patterns. Demography, 43, 631 – 646.doi:10.1353/dem.2006.0037
Rogers, R. G., Hummer, R., & Nam, C. (2000).Living and dying in the USA: Behavioral, healthand social differentials of adult mortality. SanDiego, CA: Academic Press.
Rosenfield, S. (1999). Splitting the difference: Gen-der, the self, and mental health. In C. Aneshensel& J. Phelan (Eds.), Handbook of the sociology ofmental health (pp. 209 – 224). New York: PlenumPress.
Ross, C. E., Mirowsky, J., & Goldsteen, K. (1990).The impact of family on health: The decade inreview. Journal of Marriage and the Family, 52,1059 – 1078. doi:10.2307/353319
Scafato, E., Galluzzo, L., Gandin, C., Ghirini,S., Baldereschi, M., Capurso, A., Maggi, S.,& Farchi, G. (2008). Marital and cohabita-tion status as predictors of mortality: A 10-year follow-up of an Italian elderly cohort.Social Science & Medicine, 67, 1456 – 1464.doi:10.1016/j.socscimed.2008.06.026
Singer, J., & Willett, J. (2003). Applied longitudinaldata analysis: Modeling change and eventoccurrence. New York: Oxford University Press.
Skinner, K. B., Bahr, S. J., Crane, D. R., &Call, V. R. A. (2002). Cohabitation, marriage, and
remarriage: A comparison of relationship qualityover time. Journal of Family Issues, 23, 74 – 90.doi:10.1177/0192513X02023001004
Thornton, A., Axinn, W., & Xie, Y. (2007). Marriageand cohabitation. Chicago: University of ChicagoPress.
Tower, R. B., Kasl, S. V., & Darefsky, A. S. (2002).Types of marital closeness and mortality riskin older couples. Psychosomatic Medicine, 64,644 – 659.
Umberson, D. (1992). Gender, marital status, and thesocial control of health behavior. Social Science& Medicine, 34, 907 – 917. doi:10.1016/0277-9536(92)90259-S
U.S. Census Bureau. (2011). Current population sur-vey, 2011 annual social and economic supplement.Retrieved from http://www.census.gov/apsd/techdoc/cps/cpsmar11.pdf
Waite, L. J., & Gallagher, M. (2000). The case formarriage: Why married people are happier,healthier, and better off financially. New York:Doubleday.
Wu, Z., & Hart, R. (2002). The effects of mari-tal and nonmarital union transition on health.Journal of Marriage and Family, 64, 420 – 432.doi:10.1111/j.1741 – 3737.2002.00420.x
Wu, Z., Penning, M. J., Pollard, M. S., & Hart, R.(2003). In sickness and in health: Does cohabita-tion count? Journal of Family Issues, 24, 811 – 838.doi:10.1177/0192513X03254519













![Cohabitation Rights Bill [HL]](https://static.fdocuments.us/doc/165x107/58a1a2ef1a28ab90398b940f/cohabitation-rights-bill-hl.jpg)




