COGNITIVE APPROACHES TO SUICIDE Center for Disease Control and Prevention February 6, 2004 Aaron T....
39
COGNITIVE APPROACHES TO SUICIDE Center for Disease Control and Prevention February 6, 2004 Aaron T. Beck, M.D. Gregory K. Brown, Ph.D. University of Pennsylvania
-
Upload
sheila-mccormick -
Category
Documents
-
view
213 -
download
0
Transcript of COGNITIVE APPROACHES TO SUICIDE Center for Disease Control and Prevention February 6, 2004 Aaron T....

COGNITIVE APPROACHES TO SUICIDE
Center for Disease Control and PreventionFebruary 6, 2004
Aaron T. Beck, M.D.
Gregory K. Brown, Ph.D.University of Pennsylvania

REVIEW OF STUDIES 1969-2004
I. CLASSIFICATION

NIMH TASK FORCE 1969
ATTEMPTED SUICIDE
1. Degree of Intent
2. Degree of Medical Lethality
SUICIDE IDEATION
1. Degree of Intent
2. Degree of Medical Lethality
COMPLETED SUICIDE
1. Degree of Intent

Definition of a Suicide Attempt
“a potentially self-injurious behavior with a nonfatal outcome, for which there is evidence (either explicit or implicit) that the person intended at some (nonzero) level to kill himself/herself.”
Source: O’Carroll, Berman, Maris, Moscicki, Tanney, & Silverman (1996)

Intentional Self-Injury Behavior
SuicideIntent
Definite
Uncertain/ Potential
None
Definite
DefiniteSuicideAttempt (1)
PossibleSuicideAttempt (2)
SuicideIdeation
Uncertain
PossibleSuicideAttempt (3)
PossibleSuicideAttempt (4)
MildSuicideIdeation
None
Intentional Self-Injury Behavior without Suicide Intent (5)
Possible/PotentialSelf-Injury Behavior without Suicide Intent (6)

II. ASSESSMENT

INSTRUMENT DEVELOPMENT
1. MEDICAL LETHALITY (BIOLOGICAL DAMAGE) SCALE
2. SUICIDE INTENT SCALE (FOR ATTEMPTERS)
• POST-SUICIDE SCALEa. Psychological Autopsy
4. SUICIDE IDEATION SCALE

5. HOPELESNESS SCALE
6. SUICIDE IDEATION AT WORST POINT
7. WISH TO LIVE – WISH TO DIE SCALE
8. BECK DEPRESSION INVENTORY – SUICIDE ITEM
CONSTRUCT VALIDITY
1. DEPRESSION SCALE, SUICIDE INTENT
SCALE, POST SUICIDE INTENT SCALE,
AND HOPELESSNESS SCALE
CORRELATE SIGNIFICANTLY WITH
MEDICAL LETHALITY

2. HOPELESSNESS CORRELATES MORE
STRONGLY THAN DOES DEPRESSION
WITH LETHALITY (INCLUDING DEATH).
a. Hopelessness-intent correlation is high when depression is partialed out, but not vice-versa.
b. Hopelessness correlation persists across all
demographic and diagnostic groups.
c. Hopelessness as a mediator between stressors and suicide.

III. PREDICTION OF SUICIDE

Risk Factors for Psychiatric Patients 1975-2000
• Sampled 6,891 psychiatric outpatients
• Conducted National Death Index search
• Identified 49 suicide cases
• All patients received structured interviews and standardized assessment measures
Source: Brown, Beck, Steer, & Grisham (2000)
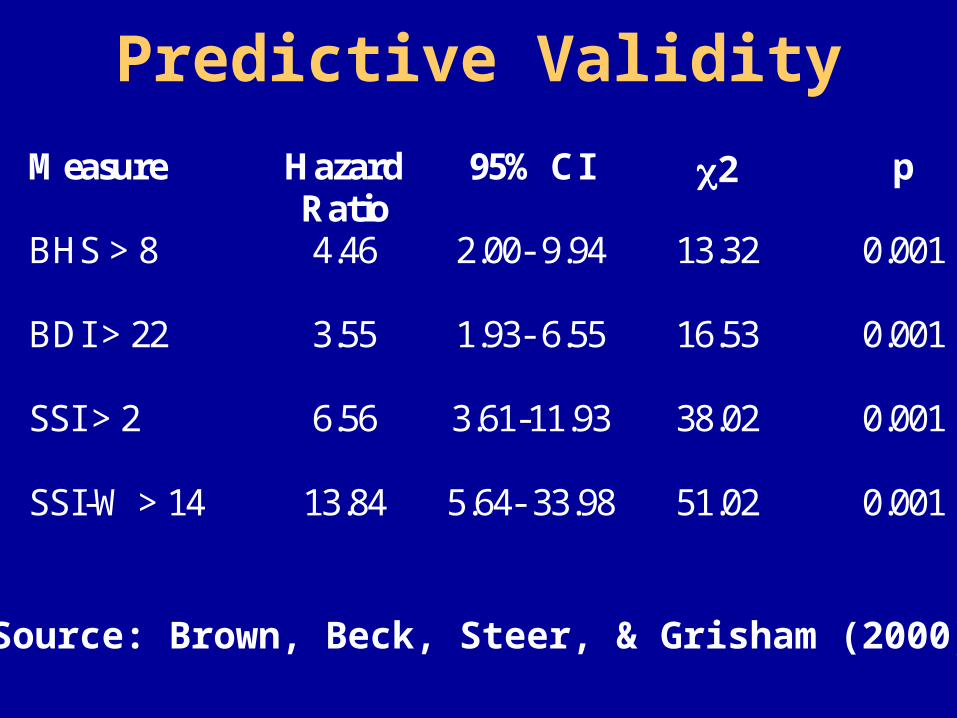
Predictive Validity
Measure Hazard Ratio
95% CI 2 p
BHS > 8 4.46 2.00- 9.94 13.32 0.001
BDI > 22 3.55 1.93- 6.55 16.53 0.001
SSI > 2 6.56 3.61-11.93 38.02 0.001
SSI-W > 14 13.84 5.64- 33.98 51.02 0.001
Source: Brown, Beck, Steer, & Grisham (2000)

Adjusted Hazard Ratios For Suicide with Psychiatric Outpatients
0
0.5
1
1.5
2
2.5
3
3.5
4
Hospi
taliz
atio
nSui
cide
Atte
mpts
Bipol
ar D
isord
erM
ajor
Dep
ress
ion
Suici
de Id
eatio
nUne
mpl
oyed
Age (Y
ears
)
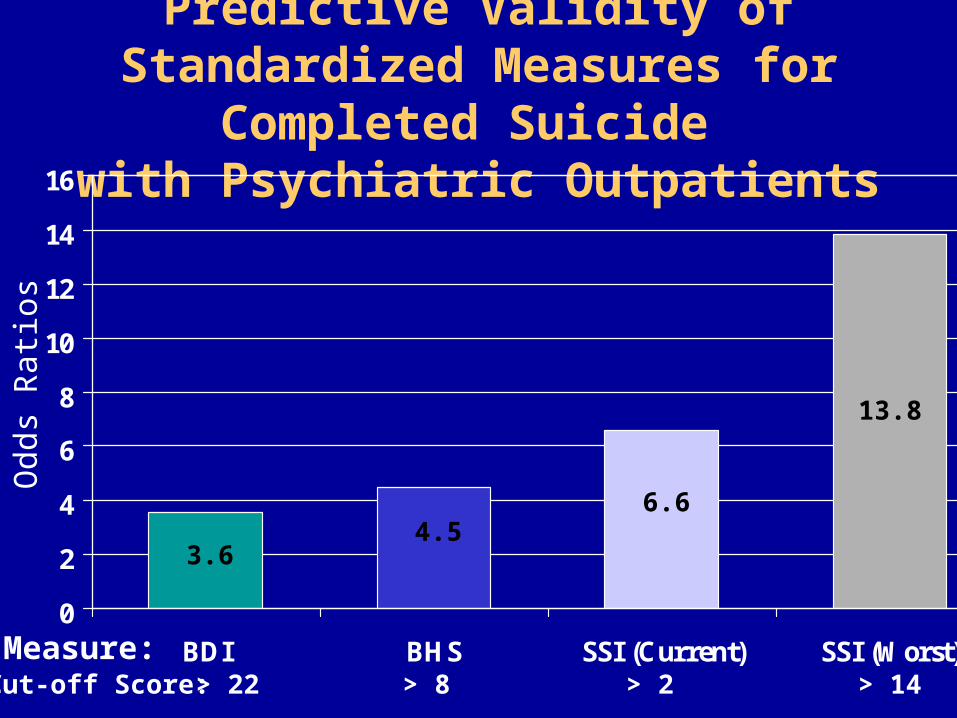
Predictive Validity of Standardized Measures for Completed Suicide
with Psychiatric Outpatients
0
2
4
6
8
10
12
14
16
BDI BHS SSI (Current) SSI (Worst)
Odd
s R
atio
s
Measure:Cut-off Score: > 22 > 8 > 2 > 14
3.64.5
6.6
13.8

Wish to Die vs. Wish to Live and Completed Suicide with Psychiatric Outpatients
0
0.5
1
1.5
2
2.5
3
3.5
Wish to Die = > Wish to Live Wish to Live > Wish to Die
Pe
rce
nt
Wh
o C
om
mit
ted
Su
icid
e
N = 21 of 637 N = 23 of 5131
3.2%
.4%
Odds Ratio = 7.4 (95% CI: 4.0-13.4), p < .001

SUICIDE ATTEMPTERS
1970-1975
2000-2001
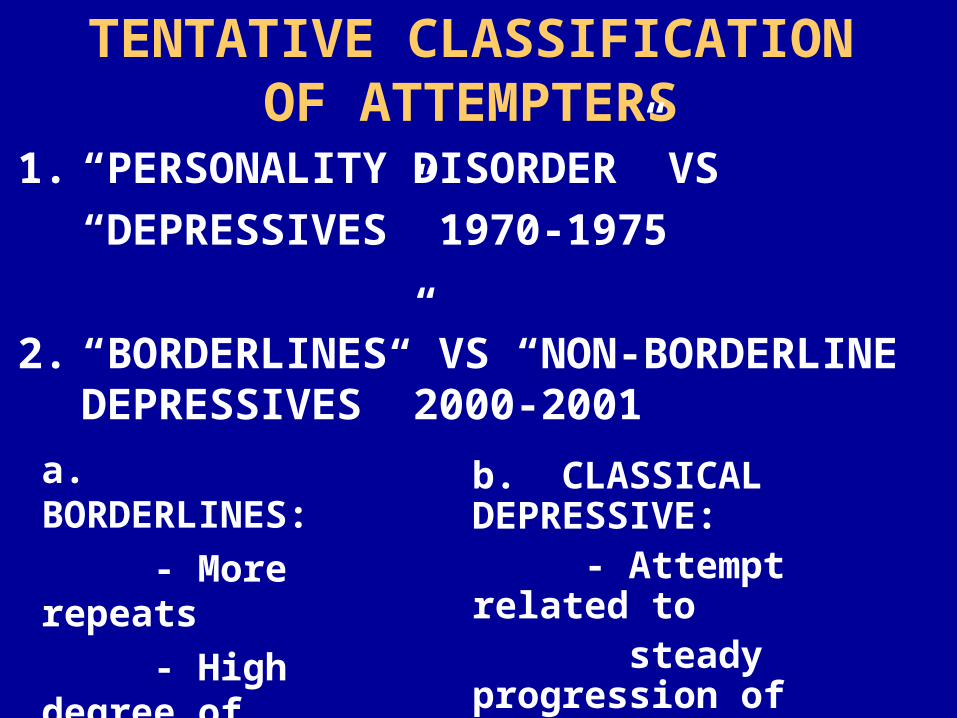
TENTATIVE CLASSIFICATION OF ATTEMPTERS
1. “PERSONALITY DISORDER” VS
“DEPRESSIVES” 1970-1975
2. “BORDERLINES” VS “NON-BORDERLINE DEPRESSIVES” 2000-2001
b. CLASSICAL DEPRESSIVE: - Attempt related to steady progression of depression
a. BORDERLINES:
- More repeats
- High degree of
reactivity
- Low control

CHARACTERISTICS OF ATTEMPTERS1970-1975
PERSONALITY DISORDERS ATTEMPT WHEN DISTRESSED
1. “Self-medicate” with drugs to relieve distress
2. Often feel shame, guilt, hopeless, after drug and then attempt
3. Low tolerance for frustration or distress
4. Poor problem solving
5. Defective self-control
6. More reality problems

DEPRESSIVE
(n = 109)
PERSONALITY DISORDER
(n = 182)
MALE 27.5% 53.3%
WHITE 53.2% 51.6%
AGE (YEARS) 30.7% 28.1%
MARRIED 24.8% 14.5%
SINGLE 34.9% 47.5%
WIDOWED 4.6% 2.8%
SEPARATED/
DIVORCED31.2% 27.9%
COHABITATING 4.6% 7.3%
SUICIDE AT 5 YR FOLLOW-UP 4.6% 8.2%

CHARACTERISTICS OF EPISODIC DEPRESSIVE ATTEMPTERS
ATTEMPT SUICIDE AT DEPTH OF
DEPRESSION (IF NOT RETARDED)
1. Profound hopelessness and generalized cognitive distortions
2. Suicide ideation only during episode
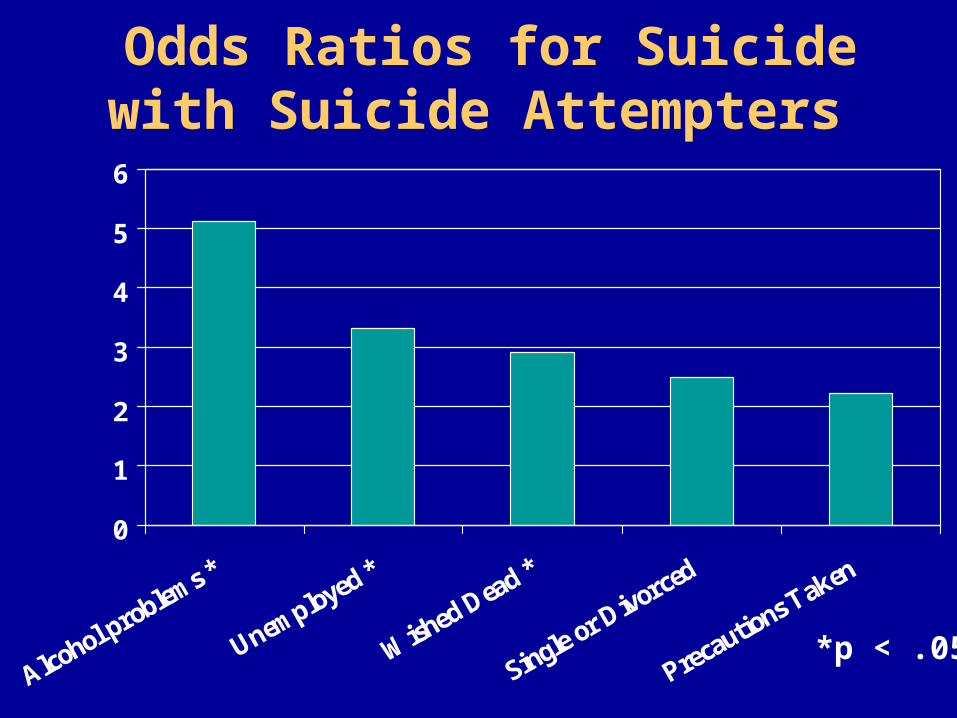
Odds Ratios for Suicide with Suicide Attempters
0
1
2
3
4
5
6
Alcohol problems *
Unemployed *
Wished Dead *
Single or Divorced
Precautions T
aken
*p < .05

Sensitivity of Reaction to Attempt for Completed Suicide
0
2
4
6
8
10
12
Glad Alive Ambivalent Wished Dead
Pe
rce
nt
Wh
o C
om
mit
ted
Su
icid
e
N = 9 of 176 N = 5 of 199 N = 10 of 101
5%2.5%
10%
Odds Ratio: 0.98 0.35 2.83

Wish to Die vs. Wish to Live and Completed Suicide with Psychiatric
Outpatients
0
0.5
1
1.5
2
2.5
3
3.5
Wish to Die = > Wish to Live Wish to Live > Wish to Die
Per
cent
Who
Com
mitt
ed S
uici
de
N = 21 of 637 N = 23 of 5131
3.2%
.4%
Odds Ratio = 7.4 (95% CI: 4.0-13.4), p < .001

IV: INTERVENTION

Cognitive Therapyfor Suicide Attempters
NIMH / CDC

Follow-upAssessm ents
1 ,3 ,6 ,12 ,18 ,24 m os
10 Sessionsof CT
Cognitive Therapy+ Enriched Care
Follow-upAssessm ents
1 ,3 ,6 ,12 ,18 ,24 m os
0 Sessionsof CT
Enriched Care
Random ization
Inform ed ConsentIntake Interview
Screened in EDor identified in PEEC logs by
study personnel
Study Design

Inclusion and Exclusion Criteria• Inclusion Criteria:
– Patient must be evaluated at the ED within 48 hours of attempting suicide
– Patient must complete a full baseline assessment within 3 weeks of making the attempt
– Age 16 or older – Patient must have at least two verifiable contacts with
telephone numbers– Must be able to provide informed consent
• Exclusion Criteria:– A severe incapacitating medical disorder that would
prevent participation in psychotherapy

Recruitment
538 Patients Referred186 were unable to be contacted
164 were excluded (not true attempters)
Of the 188 Eligible Patients Contacted68 (36%) refused
120 Baselines Completed
with 60 Patients assigned to CT+ECand 60 Patients assigned to EC

Sample Description

Age and Gender
Gender
43%
57%
Male Female
Mean Age
33.2 years
SD = 9.7

27.5
63.4
10.1
0
10
20
30
40
50
60
70
CaucasianAfrican AmericanOther
Ethnicity
%

Marital Status
64%11%
11%
7%7%
Single Divorced Married Separated Widowed
7%

0
10
20
30
40
50
60
<$8,000
$8-14,000
$14-20,000
>$20,000
Yearly Income66% Unemployed or Disabled

Method of Suicide Attempt
Overdose
58%Cut17%
Jump13%
Hang6%
Traffic3%
CO23%

Type of Drug Used in Overdose
52%
15%
13%
20%
Prescription
Over Counter
I llicit
Combination

Psychiatric Diagnoses
0
10
20
30
40
50
60
70
MDD Bipolar Substance Anxiety
• Mean Number of Axis I Diagnoses was 3• Most Patients had Major Depression with
Co-Morbid Substance Use Disorder
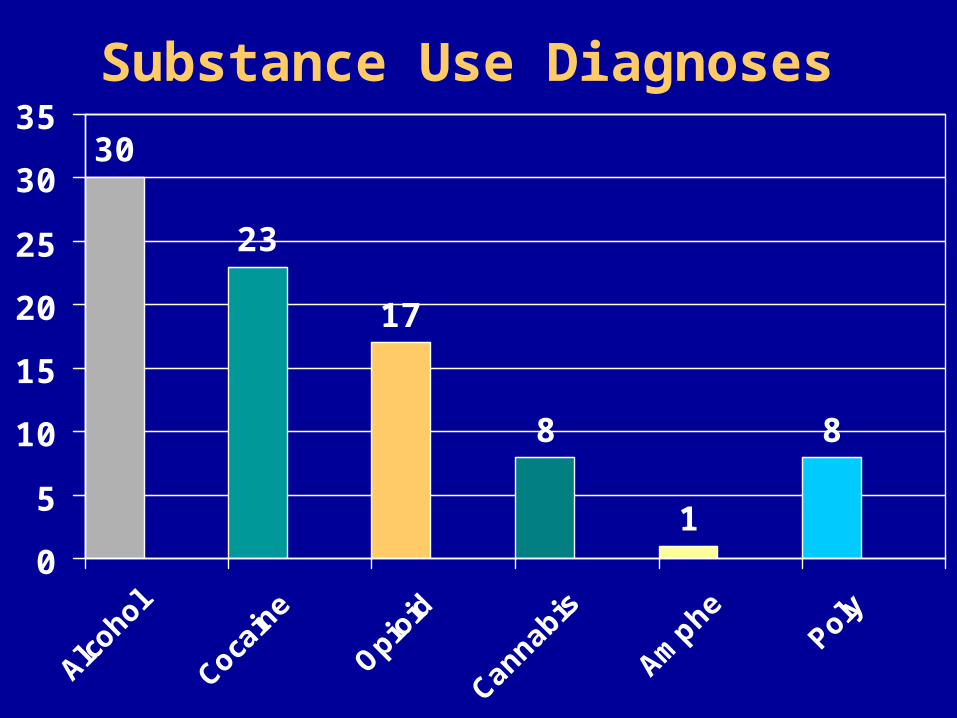
Substance Use Diagnoses
30
23
17
8
1
8
0
5
10
15
20
25
30
35
Alco
hol
Coca
ine
Opioid
Cann
abis
Amph
ePo
ly

Participation Bias
0.32, 3.64
1.0955 Other (n = 13)
0.22,0.68
0.396644 African American (n = 151)
1.49, 4.54
2.602951 Caucasian (n = 89)
CI (95%)ORYes % (n=180)
No % (n=112)
Ethnicity
Consent