Cognition and Mental Health in Patients With Multiple...
6
JULY/AUGUST 2018 PRACTICAL NEUROLOGY 57 MULTIPLE SCLEROSIS Cognition and Mental Health in Patients With Multiple Sclerosis Neuropsychologic evaluation and treatment can improve quality of life. Kathleen D. Tingus, PhD; Katelyn L. Steele, MA; and Alexander J. Steiner, PsyD Cognitive impairment and mood disorders are estimated to occur in >50% of patients with multiple sclerosis (MS) early in the disease course, making mental health both a diagnostic and a quality- of-life (QoL) issue that affects relationships, occupational/vocational status, and long-term health outcomes (Figure). 1 Early detection of cognitive impairment and psychiatric distress in this population is critical to allow for earlier treatment intervention, bet- ter patient education about treatment options and modifiable lifestyle factors, and engagement in counseling with patients and their families. After the identification of cognitive impair- ment, clinicians should strive to characterize cognitive dysfunc- tion and assess for the presence of comorbid or symptomatic mental health issues in patients with MS. Evaluation can be done objectively with neuropsychologic assessment of cogni- tion and psychiatric symptoms. Neuropsychological Evaluation Goals of Evaluation The goal of the neuropsychologic evaluation is to character- ize the pattern and severity of any cognitive dysfunction and determine whether it is consistent with symptoms of MS and neuroimaging findings or is an alternative or comorbid diagno- sis. Neuropsychologic assessment can also assess the relation- ship between mental health and any functional disabilities that may interfere with the ability to complete activities of daily living. Serial evaluations over time can determine if a neurocog- nitive disorder or other mental health disorder is present and monitor cognition and psychiatric symptom severity. A critical part of neuropsychologic assessment includes providing feedback and discussing the results with the patient to give information on cognitive strengths and weakness and educate the patient regarding how competing etiologic factors can exacerbate cognitive dysfunction and mental health con- ditions. It is vital that during this feedback session the impor- tance of treating the disease as a way of potentially improving cognitive and mental health symptoms is emphasized. Specific Tests Neuropsychologic evaluation. Tests should assess multiple cognitive domains to ensure all potential areas of cognitive dysfunction are evaluated. However, specific to the MS popu- lation, and particularly in the context of the high prevalence rates of fatigue/somnolence in patients with MS, the bat- tery should be brief (approximately 2-3 hours). Shorter and more efficient assessments are warranted, as performances for patients with MS deteriorate more rapidly compared to control Figure. Relationships between mental health and multiple sclerosis. [Reproduced from Penner IK. Evaluation of cognition and fatigue in multiple sclerosis: daily practice and future directions. Acta Neurol Scand. 2016;134(200):19-23 with permission] 1 PN0718_CF_Cognition.indd 57 7/18/18 9:30 AM
Transcript of Cognition and Mental Health in Patients With Multiple...

JULY/AUGUST 2018 PRACTICAL NEUROLOGY 57
M U LT I P L E S C L E R O S I S
Cognition and Mental Health in Patients With Multiple SclerosisNeuropsychologic evaluation and treatment can improve quality of life.
Kathleen D. Tingus, PhD; Katelyn L. Steele, MA; and Alexander J. Steiner, PsyD
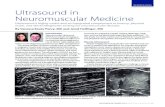
Cognitive impairment and mood disorders are estimated to occur in >50% of patients with multiple sclerosis (MS) early in the disease course, making mental health both a diagnostic and a quality-
of-life (QoL) issue that affects relationships, occupational/vocational status, and long-term health outcomes (Figure).1
Early detection of cognitive impairment and psychiatric distress in this population is critical to allow for earlier treatment intervention, bet-
ter patient education about treatment options and modifiable lifestyle factors, and engagement in counseling with patients and their families. After the identification of cognitive impair-ment, clinicians should strive to characterize cognitive dysfunc-tion and assess for the presence of comorbid or symptomatic mental health issues in patients with MS. Evaluation can be done objectively with neuropsychologic assessment of cogni-tion and psychiatric symptoms.
Neuropsychological EvaluationGoals of Evaluation
The goal of the neuropsychologic evaluation is to character-ize the pattern and severity of any cognitive dysfunction and determine whether it is consistent with symptoms of MS and neuroimaging findings or is an alternative or comorbid diagno-sis. Neuropsychologic assessment can also assess the relation-ship between mental health and any functional disabilities that may interfere with the ability to complete activities of daily living. Serial evaluations over time can determine if a neurocog-nitive disorder or other mental health disorder is present and monitor cognition and psychiatric symptom severity.
A critical part of neuropsychologic assessment includes providing feedback and discussing the results with the patient
to give information on cognitive strengths and weakness and educate the patient regarding how competing etiologic factors can exacerbate cognitive dysfunction and mental health con-ditions. It is vital that during this feedback session the impor-tance of treating the disease as a way of potentially improving cognitive and mental health symptoms is emphasized.
Specific TestsNeuropsychologic evaluation. Tests should assess multiple
cognitive domains to ensure all potential areas of cognitive dysfunction are evaluated. However, specific to the MS popu-lation, and particularly in the context of the high prevalence rates of fatigue/somnolence in patients with MS, the bat-tery should be brief (approximately 2-3 hours). Shorter and more efficient assessments are warranted, as performances for patients with MS deteriorate more rapidly compared to control
Figure. Relationships between mental health and multiple
sclerosis. [Reproduced from Penner IK. Evaluation of cognition and
fatigue in multiple sclerosis: daily practice and future directions.
Acta Neurol Scand. 2016;134(200):19-23 with permission]1
PN0718_CF_Cognition.indd 57 7/18/18 9:30 AM

58 PRACTICAL NEUROLOGY JULY/AUGUST 2018
M U LT I P L E S C L E R O S I S
subjects during a neuropsychologic evaluation.2 At the initial stages of assessing cognition in patients with MS, an extended screening evaluation may be appropriate to clarify if a more comprehensive evaluation is indicated. The Brief Repeatable Battery (BRB) takes 20 to 30 minutes to administer, includes measures most sensitive to the cognitive dysfunction associated with MS, and includes measures with available alternate forms, making repeat evaluation(s) over time possible. The BRB is avail-able through the National Multiple Sclerosis Society.3 Another widely accepted battery used in assessing cognition in patients with MS is the Minimal Assessment of Cognitive Function in MS (MACFIMS), which takes approximately 90 minutes to complete; a strength of the MACFIMS is that it was developed by a consensus of researchers and includes additional measures of emotional functioning and fatigue, relative to the BRB.4
Screening evaluation by neurology. As neurologists may have limited time to devote to cognitive testing, the Symbol Digit Modalities Test (SDMT) may help in deciding whether to refer for more extensive neuropsychologic testing. The SDMT is one of 7 subtests comprising the MACFIMS; it does not require extensive training and takes only 5 minutes to administer. The SDMT has emerged as the strongest brief screening instru-ment for cognitive impairment.5 In addition, neurologists who specialize in MS are encouraged to familiarize themselves with well-validated brief instruments that screen for cogni-tive impairment, such as the Montreal Cognitive Assessment (MoCA), which has been validated in persons with MS (Case Study).6,7 Self-report measures of subjective cognitive dif-ficulties, such as the Behavioral Rating Inventory of Executive
Function–Adult Version (BRIEF-A), may also be helpful in detecting early cognitive changes in patients.8 A guideline from the American Academy of Neurology is available that covers assessment of psychiatric disorders in individuals with MS.9
CognitionAssessment of Cognition
It is critical to assess for cognitive dysfunction, which occurs in >50% of patients with MS; multiple cognitive domains should be tested (Table).10 Some patients’ cognitive deficits are relatively mild, whereas others’ are severe enough to warrant diagnoses of neurocognitive disorders.
Although neurocognitive dysfunction may be present in all MS subtypes, diagnostic classification may be useful, as dif-ferent subtypes are associated with more severe and adverse cognitive outcomes.11 Patients with secondary progressive MS have greater impairments at the level of encoding of verbal material in memory processing/learning, processing speed, response inhibition, and set-shifting.12 More profound cogni-tive dysfunction has been reported in patients with progressive MS compared to those with relapsing MS; patients with pri-mary progressive MS may have more severe cognitive impair-ments than those with secondary progressive MS.13 Cognitive changes may also manifest during an acute relapse.
Neuropsychologic correlates of MS vary across the lifespan.10 Recent work suggests that although adult-onset MS has sev-eral features in common with pediatric-onset MS, the cohorts often differ in several regards.14 Although physical disability progression is reported to be slower among pediatric patients,
Mrs. Smith, age 44 is a right-handed, white women who lives alone and has had 12 years of formal education. She was diag-nosed with MS 2 years ago and, during a follow-up visit, states that she has become increasingly irritable, is having difficulties focusing and concentrating. and is experiencing significant sad-ness, anhedonia, apathy, fatigue, and loss of motivation; all of which are a change from her self-reported baseline.
In this example, the neurologist should screen for any cogni-tive impairment using a validated brief screening measure of gross cognitive functioning (eg, MoCA). The PHQ-2 would help screen for a possible mood disturbance, such as depression. These screening tools can aid the decision of whether to refer the patient for a comprehensive neuropsychological evaluation.
This highlights the possibility of genuine cognitive distur-bance related to central nervous system dysfunction in the context of MS and also addresses the potential role that mood disturbance can play in a patient’s self-appraisal of his or her cognitive symptoms. It is quite common for patients with MS to experience comorbid depression and objective cognitive
dysfunction. If the patient has a score of 30/30 on the MoCA, but endorses significant depression on the PHQ-2, it is plausible that the she or he is experiencing a depressive episode resulting in an overappraisal of cognitive dysfunction.
Conversely, if the patient has a score of 22/30 on the MoCA although denies depression on the PHQ-2, it is possible that the patient is experiencing genuine cognitive dysfunction related to MS. In that case, presentation of apathy, fatigue, and anhedonia may be connected to the disease process, rather than a mood disturbance, and the treating neurologist should then ask about the onset, duration, frequency, and intensity of the patient’s irritability, mood disturbance, and cognitive difficulties while considering any medical, situational, or psychosocial factors that could exacerbate those symptoms (eg, metabolic disturbance, social stressors). Regardless of findings during the neurologic examination, a referral for a comprehensive neuropsychologi-cal evaluation, in this example, is indicated, as results from a neuropsychologic examination will aid differential diagnosis and provide detailed and specific treatment recommendations.
Case Study
PN0718_CF_Cognition.indd 58 7/18/18 9:30 AM

JULY/AUGUST 2018 PRACTICAL NEUROLOGY 59
M U LT I P L E S C L E R O S I S
profound cognitive dysfunction can occur and more dramati-cally affects life trajectories in pediatric patients compared to adults. This is presumably related to demyelination and inflam-mation disrupting typical cognitive development.14 No longi-tudinal studies assessing MS across the lifespan are available.
MRI Lesion CorrelationsThe study of the correlation between lesion location, brain
networks, and their relation to objective cognitive function
among persons with MS is still in its infancy.15 Cognitive dys-function is typically relative to observed lesion load on T2 MRI sequences and associated with greater lesion load, location of white matter lesions, microstructural injury, gray matter lesions, cortical and subcortical gray matter volume loss, and abnormal activation during fMRI tasks.1,14,16-18 Despite these relationships, each patient can present with a distinct pattern of neuropsychological deficits. As a result of this diffuse pat-tern of cognitive deficits associated with lesion burden, cogni-
TABLE. DISPLAY OF COGNITIVE DOMAINS, SUBDOMAINS, AND CLINICAL OBSERVATIONS
COGNITIVE DOMAINSAND SUBDOMAINS
CLINICAL OBSERVATIONS OR SYMPTOMS
Attention and Processing Speed Simple attention,a divided attention,a sustained attention,a selective attention,a information pro-cessing speed,a and orientation
Daily tasks take longer to complete and work requires more double-checking. It is difficult to concentrate, sustain focus, or attend to sensory input. Disorientation and altered mental status may occur.
Frontal Systems “Executive” AbilitiesPlanning and organization,a inhibition and self-monitoring,a mental flexibility and set-shifting,a working memory,a initiation and vigilance,a con-ceptualization and problem solving, decision making,a and abstract reasoning
Multi-stage projects can be more difficult to complete. It can be more difficult to plan and organize tasks or find solutions to everyday problems. Shifting from one environ-mental stimuli to another or resuming an interrupted task may be challenging. Self-monitoring may be affected and persons may be more susceptible to financial scams. It is more difficult to remember new information (eg, phone numbers).
Language Expressive language (verbal fluency,a object naming, writing, calculations) and receptive language (auditory comprehension, ability to follow commands, loss of semantic knowledge)
Persons affected may have trouble finding words or names or have nonfluent, agrammatical, or halting speech, finding speaking more difficult. It may be difficult to track or understand conversation. There may be difficulty with writing, spelling, cal-culating or solving problems, or following directions, especially multi-step directions. Understanding new words, concepts, and semantic meaning of previously known information can occur, as can an inability to express thoughts.
Learning and Memory Encoding sensory input,a memory consolida-tion and storage, prospective memory, memory retention, memory retrieval,a and memory recognition
Encoding sensory input can be challenging and it may be difficult to recall details of recent events because the information was either never encoded or because informa-tion was not retained or requires cuing to aid retrieval. Patients may need or have compensatory strategies (eg, calendar, grocery lists, appointment reminders).
Visuospatial/Visuoperceptual/Visuoconstructive Abilities Visual scanning,a visuomotor construction,a visual integration, spatial orientation, proprio-ception, visual agnosia, and prosopagnosia
Patients may have difficulty distinguishing left and right, trouble finding items left in plain sight, get lost or disoriented, or feel out of place. Drawing, reading and recogniz-ing familiar faces or items may be difficult, either as a result of impaired visual integra-tion or insult to focal cortical regions (ie, fusiform gyrus).
Motor Fine manual dexterity,a motor speed,a motor apraxia, motor planning and sequencing
Dressing may be difficult due to fine manual dexterity issuses or motor sequencing and planning impairments. Executing simple or complex, meaningful or meaningless, skilled or purposeful movements, writing, and using utensils may be challenging.
aSubdomains that are most commonly associated with MS as a result of nonspecific white matter-lesion load..
PN0718_CF_Cognition.indd 59 7/18/18 9:30 AM

60 PRACTICAL NEUROLOGY JULY/AUGUST 2018
M U LT I P L E S C L E R O S I S
tive dysfunction that results from MS is often best character-ized as a subcortical dementia. The cardinal neurocognitive profile of a subcortical dementia is termed frontosubcortical, as the core deficits associated with a frontosubcortical pattern of dysfunction stem from disruption of white matter connectiv-ity between frontal cortical networks and subcortical regions. This often manifests in deficient frontal systems (executive abilities), deficient processing speed, and deficient fine manual dexterity/motor speed. Additionally, there is evidence that cognitive dysfunction in MS cannot be fully explained by white matter injury alone.19 White matter atrophy is most frequently associated with impairments in the domains of processing speed and working memory, whereas gray matter atrophy is often more associated with focal dysfunction and comorbid psychiatric symptoms including disinhibition or euphoria.20
Although the degree of cognitive dysfunction may vary, the frontosubcortical neurocognitive profile in patients with MS is rather stable. MS subtypes differently affect the degree of cognitive dysfunction observed, rather than domain-specific variability. Although the cognitive profile is often associated with lesion load and location (eg, periventricular, juxtacortical, infratentorial, or spinal cord regions), it is disruption of connec-tivity that largely attenuates processing speed, frontal systems, and motor functions. Nonetheless, periventricular and juxta-cortical lesions are more associated with cognitive processing deficits, whereas infratentorial or spinal cord lesions are more associated with motor and sensory-processing deficits.
Specific Cognitive ImpairmentsFindings from large-scale, controlled studies consistently
show that processing speed and episodic memory are the most commonly affected cognitive domains in persons with MS, although concurrent deficits in executive functions, verbal fluency, and visuospatial processing have also been seen.17 Patients with MS often experience increased difficulty in mem-ory processing, such as difficulty retrieving names, misplacing personal items, forgetfulness in daily life, or difficulties in plan-ning and organizing. Episodic memory deficits are commonly observed on formal neuropsychologic exam. However, one clear distinction between MS and other neurologic diseases (eg, Alzheimer’s disease) is that memory retention remains relatively intact. Instead, patients with MS often have deficient acquisition and learning of new material, particularly at the level of encoding, and this deficit is presumed to be attenu-ated by slowed processing speed and weak executive control. Although patients may have difficulty retrieving successfully encoded information (often the result of frontal dysfunction), they rarely present as densely amnestic. Patients with MS may also have deficits in aspects of social cognition including theory of mind (understanding and predicting the mental states of others), empathy, and social perception (ie, facial recognition,
understanding social or affective prosody), that can signifi-cantly affect interpersonal relationships, but the relationship between social cognitive deficits and MS remains unresolved.21
Impact of Comorbidities and DisabilitiesComorbid effects of extraneous factors often experienced by
patients with MS (ie, depression, fatigue, pain, physical immo-bility, or sleep disruption) should also be considered for their effects on cognition. Fatigue has been reported in up to 90% of individuals with MS.22 In addition, the point prevalence of pain in patients with MS is roughly 50%, while approximately 75% of patients with MS report having experienced pain within the past month.23 These complicating and overlapping fac-tors make a qualitative approach necessary to ensure accurate characterization of cognitive performance.
Objective cognitive performance can be associated with physical disability and disease duration. Evidence of cognitive dysfunction is often observed before physical disability status is documented or even occurs.17 There is a critical need for establishing the validity of neuropsychologic measures in the context of comorbidities and disabilities, as well as a more robust characterization of various cognitive phenotypes in patients with MS through prospective longitudinal design.17
Adequate sleep is critical for healthy brain function. Disrupted sleep or the presence of a superimposed sleep disor-der can negatively affect cognition and contribute to ongoing psychiatric symptoms. Within the MS population, underly-ing sleep disorders are common and often remain undiag-nosed.24,25 Objective sleep measures (eg, polysomnography, actigraphy) have been found to predict cognitive dysfunction in patients with MS; however, self-reported sleep disruption may not be predictive of objective cognitive dysfunction.26 (See Sleep Disorders in Patients With Multiple Sclerosis p. 47)
Mental Health and Neuropsychiatric ManifestationsEmotional well-being can affect every area of life. Patients
with MS often have significant stress from disease and treat-ment burden as do their family members, friends, and caregiv-ers.27 Although changes in emotional state can be related to the situational stressor of living with MS, there are additional neurologic and immunologic changes associated with mental health in MS.26-29 In particular, a higher incidence of major depressive disorder, anxiety, frequent mood swings, increased irritability/agitation, and pseudobulbar affect have all been reported in patients with MS.27-30 Intrathecal inflammation can induce mood alterations and several biomarkers of neuroin-flammation (ie, interleukin-2 CSF levels, TNF-a, interleukin-1b) have been identified to correlate with self-report measures of depression and anxiety in persons with MS.31 Additionally, psychiatric syndromes are invariably a possible side effect of corticosteroid therapy, which may be used in treating patients with MS, that should be monitored accordingly.
PN0718_CF_Cognition.indd 60 7/18/18 9:30 AM

JULY/AUGUST 2018 PRACTICAL NEUROLOGY 61
M U LT I P L E S C L E R O S I S
DepressionEstimated prevalence of depression in patients with MS
is 20%, with lifetime prevalence as high as 50%, substantially higher than in the general population.27-29 Depression in patients with MS negatively affects QoL, adaptive function, emotional well-being, and treatment adherence.27,32 Routine depression screening is strongly recommended.33,34 The 2-item Patient Health Questionnaire (PHQ-2) is the briefest avail-able screening measure for depression.35 The Beck Depression Inventory-Second edition (BDI-II) is another sound and robust measure for characterizing depressive symptom severity in patients with MS and takes only 5 to10 minutes to complete.36
Sexual DysfunctionSexual dysfunction is a common complication of MS, occur-
ring in 50% to 90% of men with MS and 40% to 80% of women with MS.37 Clinicians should assess for sexual dysfunction, as it can lead to increased interpersonal difficulties, increased rates of anxiety and depression, and decreased QoL.38
Anxiety DisordersHigher lifetime prevalence rates of anxiety have been observed
in patients with MS compared to the general population.28 Generalized anxiety disorder is most commonly reported in the MS literature, followed by panic disorder and obsessive-compul-sive disorder.28 Anxiety and fear of future progression of symp-toms in MS may be underappreciated and have been found to be associated with increased levels of depressive symptoms.28
Psychotic Spectrum DisordersBipolar disorder is the only severe mental illness that occurs
with significant frequency in patients with MS compared to the general population. Epidemiological studies have been lim-ited, however, by small sample sizes or weak research design. Few large-scale empirical studies have found a relationship between MS and other psychotic spectrum disorders.
TreatmentCognitive Rehabilitation
Ongoing research efforts are focused on cognitive rehabili-tation and intervention. Restoration of cognitive functioning and enhancement of compensatory strategies continue to be explored; however, which are the best cognitive rehabilitation treatment options for patients with MS are still a matter of debate.15 Cognitive rehabilitation therapy (CRT) is a promising nonpharmacological option that entails learning new cognitive strategies to compensate for cognitive problems; however, the effectiveness of CRT in patients with MS is as yet unproven due to contradictory findings of the methodologically limited studies completed.15,39 Mindfulness-based cognitive therapy (MBCT) is another nonpharmacological treatment combin-ing elements of mindfulness training and cognitive behavioral
therapy. Preliminary evidence supports that MBCT has a posi-tive effect on cognition in healthy individuals; findings may be generalizable to persons with MS.40 A systematic review and a meta-analysis on the efficacy of computer-based cognitive training in the neuropsychologic performance of patients with MS found that computer-based cognitive training significantly improved memory performance in patients with MS, relative to healthy controls.41 To date, however, most outcome studies have been limited to focusing exclusively on relapsing-remit-ting MS, and treatment efficacy remains speculative.42 As in the general population, the act of exercise in patients with MS has been demonstrated to have a positive impact on cognition, perhaps due to secondary improvements related to improved sleep, mood, and vascular health.43 In addition, neurologists are strongly encouraged to reaffirm the importance of a healthy diet, routine exercise regimen, and adequate sleep to their patients, to increase the likelihood of optimal cognitive and emotional functioning.
Treatment for Neuropsychiatric DisordersThere are a number of available psychotherapeutic treat-
ments to alleviate psychiatric distress in patients with MS. Cognitive behavioral therapy (CBT) is effective for treating depression in patients with MS.44,45 CBT focuses on the core principle that psychologic problems are based, in part, on faulty ways of thinking and learned patterns of unhelpful behavior and involves efforts to change distorted thinking pat-terns or alter maladaptive behavior patterns.45 In patients with MS, the psychologist may focus on a patient’s ability to main-tain social relationships or to reduce perceived disease burden and fears of disease progression. Mindfulness-based interven-tions also successfully treat psychologic symptoms in patients with MS.40 Mindfulness therapies involve bringing one’s attention to experiences occurring in the present, which can be developed through meditation and other stress-relaxation techniques or breathing exercises.
Several systematic reviews show promising findings related to the efficacy of CBT for reducing fatigue in patients with MS.22,46 In the context of ongoing sleep disruption, especially insomnia, CBT for insomnia (CBT-I) is recommended.47 Meta-analyses have shown that relaxation techniques and mindful-ness interventions decrease fatigue.46 Because pharmacological interventions are often useful in conjunction with psycho-therapeutic interventions, consultation with a psychiatrist to explore mood-stabilizing medications is also recommended. Neurologists are well positioned to refer patients for psycho-therapy (eg, CBT) to target mood stabilization.47
ConclusionsCognitive interventions for persons with MS optimally
involve adjunctive pharmacologic treatments in combination with behavioral approaches (eg, cognitive training, psycho-
PN0718_CF_Cognition.indd 61 7/18/18 9:30 AM

62 PRACTICAL NEUROLOGY JULY/AUGUST 2018
M U LT I P L E S C L E R O S I S
therapy, sleep hygiene, routine exercise) to optimize cogni-tion.19 Preventive efforts that increase the likelihood of optimal cognitive functioning and emotional well-being include physi-cal activity and exercise, regular engagement in cognitively stimulating activities, limiting alcohol intake, and smoking ces-sation. Sumowski and colleagues highlight the importance for treating clinicians to incorporate a holistic approach to clinical intervention, which includes considering the unique circum-stances of each patient’s life (eg, existing family/social support systems, available financial/health care/educational resources, and medical or psychiatric comorbidities).17 n
1. Penner IK. Evaluation of cognition and fatigue in multiple sclerosis: daily practice and future directions. Acta Neurol Scand. 2016;134(200):19-23.2. Krupp LB, Elkins LE. Fatigue and declines in cognitive functioning in multiple sclerosis. Neurology. 2000;55(7):934-939. 3. Rao SM. Manual for the Brief Repeatable Battery of Neuropsychological Tests in Multiple Sclerosis. New York, NY: National Multiple Sclerosis Society; 1990.4. Benedict RH, Fischer JS, Archibald CJ, et al. Minimal neuropsychological assessment of MS patients: a consensus approach. Clin Neuropsychol. 2002;16(3):381-397.5. Kim S, Zemon V, Rath JF, et al. Screening instruments for the early detection of cognitive impairment in patients with Multiple Sclerosis. Int J MS Care. 2017;19(1):1-10.6. Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695-699.7. Dagenais E, Rouleau I, Demers M, et al. Value of the MoCA test as a screening instrument in multiple sclerosis. Can J Neurol Sci. 2013;40(3):410-415. 8. Roth RM, Gioia GA. Behavior Rating Inventory of Executive Function-Adult. Psychological Assessment Resources Lutz, FL; 2005.9. Minden SL, Feinstein A, Kalb RC, et al. Evidence-based guideline: assessment and management of psychiatric disorders in individuals with MS report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2014;82(2):174-181. 10. MacAllister WS, Belman AL, Milazzo M, et al. Cognitive functioning in children and adolescents with multiple sclerosis. Neurology. 2005;64(8):1422-1425.11. Huijbregts SC, Kalkers NF, de Sonneville LM, de Groot V, Reuling IE, Polman CH. Differences in cognitive impairment of relapsing remitting, secondary, and primary progressive MS. Neurology. 2004;63(2):335-339. 12. Ntoskou K, Messinis L, Nasios G, et al. Cognitive and language deficits in multiple sclerosis: comparison of relapsing remit-ting and secondary progressive subtypes. Open Neurol J. 2018;12:19-30. 13. Rosti-Otajarvi E, Ruutiainen J, Huhtala H, Hamalainen P. Cognitive performance profile in different phenotypes of MS with cognitive complaints. Mult Scler Relat Disord. 2014;3(4):463-472.14. Nunan-Saah J, Paulraj SR, Waubant E, Krupp LB, Gomez RG. Neuropsychological correlates of multiple sclerosis across the lifespan. Mult Scler. 2015;21(11):1355-1364.15. Nauta IM, Speckens AEM, Kessels RPC, et al. Cognitive rehabilitation and mindfulness in multiple sclerosis (REMIND-MS): a study protocol for a randomised controlled trial. BMC Neurol. 2017;17(1):201.16. Bagert B, Camplair P, Bourdette D. Cognitive dysfunction in multiple sclerosis: natural history, pathophysiology and management. CNS Drugs. 2002;16(7):445-455.17. Sumowski JF, Benedict R, Enzinger C, et al. Cognition in multiple sclerosis: state of the field and priorities for the future. Neurology. 2018;90(6):278-288.18. Calabrese M, Agosta F, Rinaldi F, et al. Cortical lesions and atrophy associated with cognitive impairment in relapsing-remitting multiple sclerosis. Arch Neurol. 2009;66(9):1144-1150. 19. Benedict RHB, DeLuca J, Enzinger C, Geurts JJG, Krupp LB, Rao SM. Neuropsychology of multiple sclerosis: looking back and moving forward. J Int Neuropsychol Soc. 2017;23(9-10):832-842.20. Sanfilipo MP, Benedict RH, Weinstock-Guttman B, Bakshi R. Gray and white matter brain atrophy and neuropsychological impairment in multiple sclerosis. Neurology. 2006;66(5):685-692.21. Chalah MA, Ayache SS. Deficits in social cognition: an unveiled signature of multiple sclerosis. J Int Neuropsychol Soc. 2017;23(3):266-286. 22. Chalah MA, Ayache SS. Cognitive behavioral therapies and multiple sclerosis fatigue: a review of literature. J Clin Neurosci. 2018;52:1-4.23. O’Connor AB, Schwid SR, Herrmann DN, Markman JD, Dworkin RH. Pain associated with multiple sclerosis: systematic review and proposed classification. Pain. 2008;137(1):96-111.24. Bamer AM, Johnson KL, Amtmann D, Kraft GH. Prevalence of sleep problems in individuals with multiple sclerosis. Mult Scler. 2008;14(8):1127-1130.25. Hensen HA, Krishnan AV, Eckert DJ. Sleep-disordered breathing in people with multiple sclerosis: prevalence, pathophysi-ological mechanisms, and disease consequences. Front Neurol. 2017;8:740.26. Hughes AJ, Dunn KM, Chaffee T. Sleep disturbance and cognitive dysfunction in multiple sclerosis: a systematic review. Curr Neurol Neurosci Rep. 2018;18(1):2. 27. Pinkston JB, Alekseeva N. Neuropsychiatric manifestations of multiple sclerosis. Neurol Res. 2006;28(3):284-290.28. Chwastiak LA, Ehde DM. Psychiatric issues in multiple sclerosis. Psychiatr Clin North Am. 2007;30(4):803-817.
29. Arnett PA, Barwick FH, Beeney JE. Depression in multiple sclerosis: review and theoretical proposal. J Int Neuropsychol Soc. 2008;14(5):691-724.30. Siegert RJ, Abernethy DA. Depression in multiple sclerosis: a review. J Neurol Neurosurg Psychiatry. 2005;76(4):469-475.31. Rossi S, Studer V, Motta C, et al. Neuroinflammation drives anxiety and depression in relapsing-remitting multiple sclerosis. Neurology. 2017;89(13):1338-1347.32. Bruce JM, Hancock LM, Arnett P, Lynch S. Treatment adherence in multiple sclerosis: association with emotional status, personality, and cognition. J Behav Med. 2010;33(3):219-227. 33. IsHak W, Lopez E, Steiner A, et al. Evaluating the impact of depression screening in general hospitals: a pilot study of patient reported outcomes of quality of life, functioning, and psychiatric symptom severity. Int J Med. 2016;4(2):32-38.34. IsHak WW, Pan D, Steiner AJ, et al. Patient-reported outcomes of quality of life, functioning, and GI/psychiatric symptom severity in patients with inflammatory bowel disease (IBD). Inflamm Bowel Dis. 2017;23(5):798-803. 35. Kroenke K, Spitzer RL, Williams JB. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284-1292.36. Beck AT, Steer RA, Brown GK. Beck depression inventory-II. San Antonio. 1996.37. Pottgen J, Rose A, van de Vis W, et al. Sexual dysfunctions in MS in relation to neuropsychiatric aspects and its psychologi-cal treatment: a scoping review. PLoS One. 2018;13(2):e0193381. 38. Brotto L, Atallah S, Johnson-Agbakwu C, et al. Psychological and interpersonal dimensions of sexual function and dysfunc-tion. J Sex Med. 2016;13(4):538-571.39. Lovera J, Kovner B. Cognitive impairment in multiple sclerosis. Curr Neurol Neurosci Rep. 2012;12(5):618-627.40. Fox KC, Nijeboer S, Dixon ML, et al. Is meditation associated with altered brain structure? A systematic review and meta-analysis of morphometric neuroimaging in meditation practitioners. Neurosci Biobehav Rev. 2014;43:48-73.41. Dardiotis E, Nousia A, Siokas V, et al. Efficacy of computer-based cognitive training in neuropsychological performance of patients with multiple sclerosis: a systematic review and meta-analysis. Mult Scler Relat Disord. 2018;20:58-66. 42. Messinis L, Papathanasopoulos P, Kosmidis MH, Nasios G, Kambanaros M. Neuropsychological features of multiple sclerosis: impact and rehabilitation. Behav Neurol. 2018:4831647.43. Prakash RS, Snook EM, Motl RW, Kramer AF. Aerobic fitness is associated with gray matter volume and white matter integrity in multiple sclerosis. Brain Res. 2010;1341:41-51.44. Graziano F, Calandri E, Borghi M, Bonino S. The effects of a group-based cognitive behavioral therapy on people with multiple sclerosis: a randomized controlled trial. Clin Rehabil. 2014;28(3):264-274.45. Hind D, Cotter J, Thake A, et al. Cognitive behavioural therapy for the treatment of depression in people with multiple sclerosis: a systematic review and meta-analysis. BMC Psychiatry. 2014;14:5.46. Phyo AZZ, Demaneuf T, De Livera AM, et al. The efficacy of psychological interventions for managing fatigue in people with multiple sclerosis: a systematic review and meta-analysis. Front. Neurol. 2018;9:149.47. Smith MT, Huang MI, Manber R. Cognitive behavior therapy for chronic insomnia occurring within the context of medical and psychiatric disorders. Clin Psychol Rev. 2005;25(5):559-592.
Kathleen D. Tingus, PhDAssociate Professor of Psychiatry and NeurologyDepartment of Neurology and Department of Psychiatry and Biobehavioral SciencesUniversity of California, Los AngelesDavid Geffen School of Medicine at UCLALos Angeles, CA
Katelyn L. Steele, MANeuropsychology ExternDepartment of Psychiatry and Biobehavioral SciencesUniversity of California, Los AngelesDavid Geffen School of Medicine at UCLALos Angeles, CA
Alexander J. Steiner, PsyDPostdoctoral FellowDepartment of Psychiatry and Biobehavioral SciencesUniversity of California, Los AngelesDavid Geffen School of Medicine at UCLALos Angeles, CA
DisclosuresAll authors declare that there are no conflicts of interest or financial disclosures.
PN0718_CF_Cognition.indd 62 7/18/18 9:30 AM