
Cns ii,mbbs
39
1
-
Upload
drbabai-halder -
Category
Health & Medicine
-
view
34 -
download
0
Transcript of Cns ii,mbbs

1
The principle cells of the CNS :
1. Neurons- functional units of the CNS, about 10¹¹ in human brain.
2. Glial cells-
- Astrocytes
- Oligodendrocytes
- Ependymal cells
- Choroid plexus epithelium
- Microglia.
3. Cells that compose of meninges.
4. Blood vessel elements.
2


10% of all tumors.
Commonest solid cancers in children.(2nd to Leuk for all malignancies)
Age: double peak 1st & 6th decade
Adults - 70% supra-tentorial
Children - 70% infra-tentorial
No/very rare extraneural spread.
Metastasis most common.
4

I. TUMOURS OF NEUROGLIA (GLIOMAS)1. Astrocytoma2. Oligodendroglioma3. Ependymoma4. Choroid plexus papilloma II. TUMOURS OF NEURONS1. Neuroblastoma2. Ganglioneuroblastoma3. Ganglioneuroma III. TUMOURS OF NEURONS AND NEUROGLIAGanglioglioma IV. POORLY-DIFFERENTIATED AND EMBRYONAL TUMOURS1. Medulloblastoma2. Neuroblastoma3. PNET V. TUMOURS OF MENINGES1. Meningioma2. Meningeal sarcoma
5

VI. NERVE SHEATH TUMOURS1. Schwannoma (neurilemmoma)2. Neurofibroma3. Malignant nerve sheath tumour VII. OTHER PRIMARY INTRAPARENCHYMAL TUMOURS1. Haemangioblastoma2. Primary CNS lymphoma3. Germ cell tumours VIII. MISCELLANEOUS TUMOURS1. Malignant melanoma2. Craniopharyngioma3. Pineal cell tumours4. Pituitary tumours IX. TUMOUR-LIKE LESIONS(epidermal cyst, dermoid cyst, colloid cyst) X. METASTATIC TUMOURS
carcinomas of the lung, breast,skin (malignant melanoma), kidney and the gastrointestinal tract and choriocarcinoma.
6

Adults:
Astrocytoma & Glioblastoma.
Meningioma
Metastasis.
Children:
Astrocytoma
Medulloblastoma
7

1. Neuron: Gangliocytoma, gangliogliomamedulloblastoma
2. Astrocyte: Astrocytoma, glioblastoma3. Oligodendrocyte: Oligodendroglioma4. Ependymal cell: Ependymoma5. Microglial cell: Tumors derived from microglial
cells have not been described.6. Meningeal cell: Meningiomas are derived from
arachnoidal cells and are usually dural-based.

◦Glioma Astrocytoma
Oligodendroglioma
Ependymoma
◦Neuronal lineage
◦Meningioma
◦Nerve Sheath Tumors

2 major divisions
a) Diffusely infiltrating astrocytoma
i.Diffuse astrocytoma(WHO Grade-II)
Ii. Anaplastic astrocytoma (WHO Grade-III)
Iii. Glioblastoma (WHO Grade-IV)
b) Circumscribed astrocytoma
i. Pilocytic astrocytoma (WHO Grade-I)
Ii.Pleomorphic xantho astrocytoma
Iii.Subependymal giant cell astrocytoma
10

10-15% of astrocytic tumors, peak incidence at ages 30 & 40.
Involves any region of CNS. Frontal and temporal lobes.
Slow growing tumor.
p53 mutation is seen in >60% of patients.
Variants-
Fibrillary astrocytoma
Gemistocytic astrocytoma
Protoplasmic astrocytoma.
11

12
Gross
Enlargement and distortion of involved area with blurring of gross anatomical boundaries.
Cystic areas and focal calcifications are common.

Most frequent variant.
Diagnostic criterion is nuclear atypia- enlarged, cigar shaped, irregular and hyperchromatic with coarse chromatin.
Cytoplasm is scanty.
Dyscohesive growth pattern.
Fibrillary matrix, microcysts containing mucinousfluid are seen.
Mitotic activity, necrosis and microvascular proliferation are absent.
IHC: GFAP, vimentin, S100.
13

14
GFAP
FRIBRILLARY ASTROCYTOMA

Gemistocytic neoplastic astrocytes comprises > 20% of all the tumor cells.
Individual cells having plump, glassy, eosinophilic, slightly angulated cytoplasm.
Nuclei are usually eccentric with distinct nucleoli and densely clumped chromatin.
Tumor cells project stout, randomly oriented processes, forming a coarse fibrillar network.
Perivascular lymphocytes cuffing seen.
IHC: GFAP, p53 and bcl 2.
Prognosis: Prone to progress to anaplasticastrocytoma and glioblastoma.
15

16
GEMISTOCYTIC ASTROCYTOMA
p53
GFAP

17
Rare variant
Composed of homogenous cell population of astrocytes.
Round to oval nuclei, short and delicate cytoplasmic processes in an abundant eosinophilicmatrix.
Mucoid degeneration and microcyst formation are common.
Mitotic activity absent.
IHC: Low immunoreactivity for GFAP.

Diffusely infiltrating malignant astrocytoma.
Mean age at dx 45yrs.
May arise de-novo or from diffuse astrocytoma.
Tendency to progress to glioblastoma, mean time interval 2 yrs.
Histo:
Increased cellularity, nuclear atypia and mitotic activity.
Multinucleated tumor cells and abnormal mitosis may be present.
Microvascular proliferation and necrosis are absent.
18

19

Most frequent and most malignant primary brain tumor.
Most common between 45 and 75 years.
Subcortical white matter of cerebral hemispheres is the most common site.
May arise de novo or through progression from diffuse astrocytoma or anaplastic astrocytoma.
May spread to the contralateral hemisphere (butterfly glioma) or may metastasize via CSF.
20
21
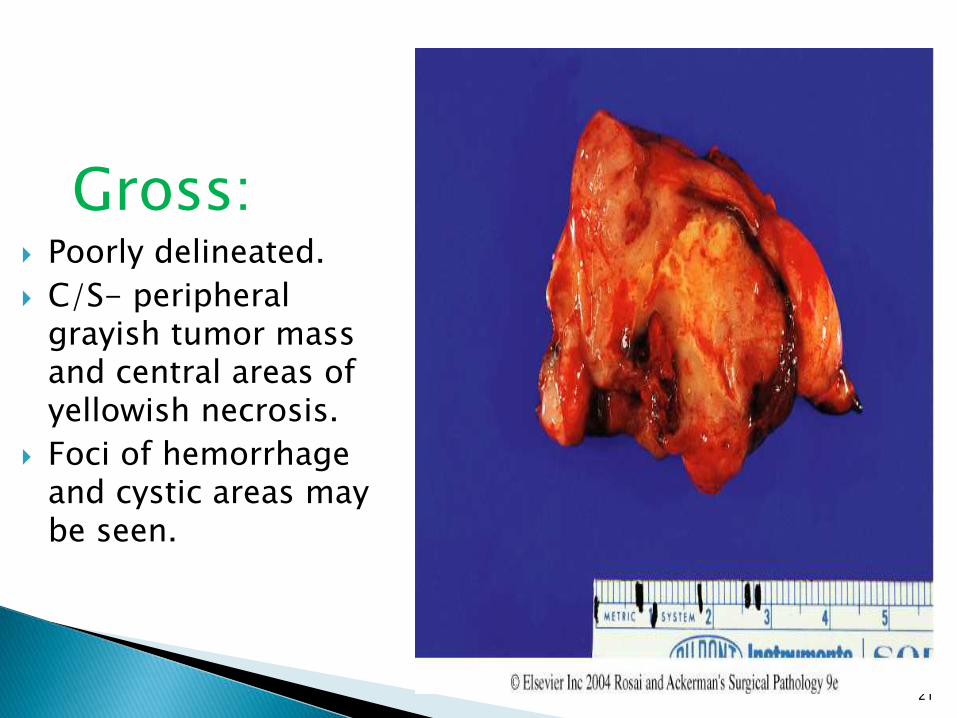
Gross: Poorly delineated.
C/S- peripheral grayish tumor mass and central areas of yellowish necrosis.
Foci of hemorrhage and cystic areas may be seen.

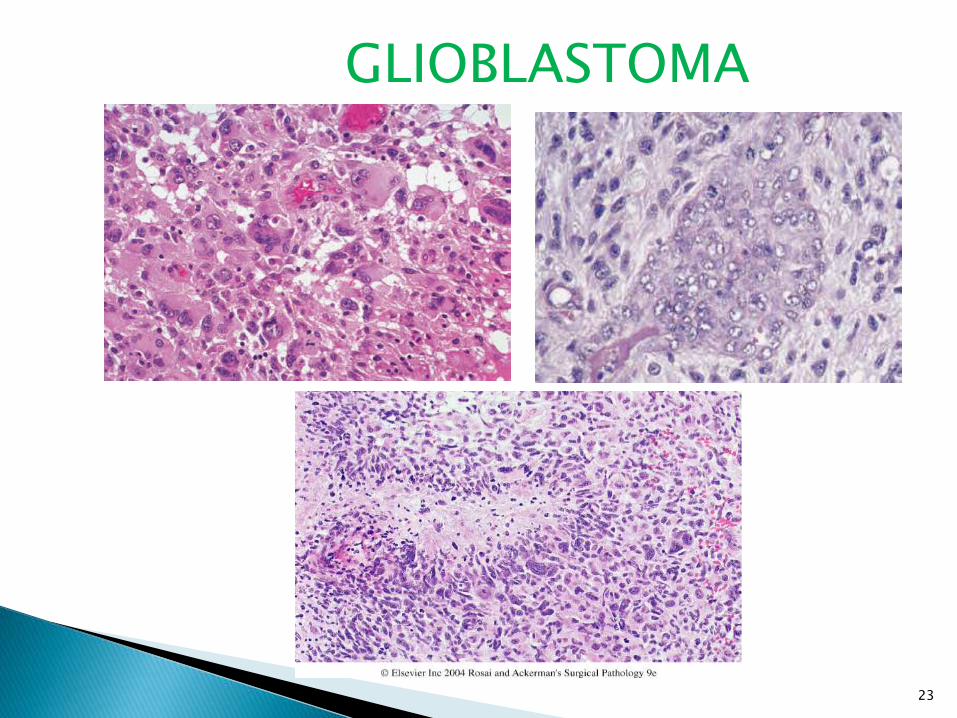
Histo:
Poorly differentiated, pleomorphic astrocytic tumor cells with marked atypia.
Prominent microvascular proliferation with glomeruloid tufts like appearance.
Pseudopalisading pattern of necrosis.
Tumor cells accumulating around neurons, blood vessels and subpial region of cortex.
Mitotic activity.
Multinucleated tumor giant cells.
Large cells with granular, PAS + cytoplasm may be scattered.
Adenoid and squamous metaplasia may be seen .
Perivascular lymphocytic cuffing may be seen.
22
23
GLIOBLASTOMA

5-6% of all gliomas.
Most common glioma in children.
First two decades of life.
Most common sites: Cerebellum, 3rd ventricular/ hypothalamic region, anterior optic pathway.
24

25
Macros: Soft, grey, discrete
mass.
Intra or paratumoralcyst formation is common

Histo:
Low to moderate cellularity with biphasic pattern-
Compacted bipolar cells with Rosenthal fibers.
Elongated, cytologically bland nuclei with long hair like processes.
High content of refractile eosinophilic fibrils, strong positivity for GFAP.
Loose textured multipolar cells with microcysts and granular bodies/ hyaline droplets.
Round to oval, cytologically bland nuclei.
Small cell body and short, cobweb-like precesses.
Fibril poor and weak GFAP +ve.
26

Mitoses are rare.
Hyalinized and glomeruloid vascular proliferation common.
Infarct-like and non-palisading necrosis seen.
Perivascular lymphocytic infiltration.
27

28
PYLOCYTIC ASTROCYTOMA
BIPHASIC PATTERN GFAP

29

Usually Benign slow-growing tumors of adults, F/M 3:2
Originate from meningothelial cells of the arachnoid.
Usually solitary ( multiple meningiomas NF2 ) Morphology:◦ Firm rounded masses, adherent to the dura and
compressing the underlying brain (no infiltration).◦ Histologic variants include:
Syncytial, fibroblastic, transitional, Psammomatous & papillary.
Malignant Meningioma is very rare◦ Infiltrates the underlying brain, shows marked nuclear
atypia, mitoses, & foci of necrosis. Other rare sarcomas of meninges include: ◦ Hemangiopericytoma, malignant fibrous histiocytoma &
Fibrosarcoma.

31

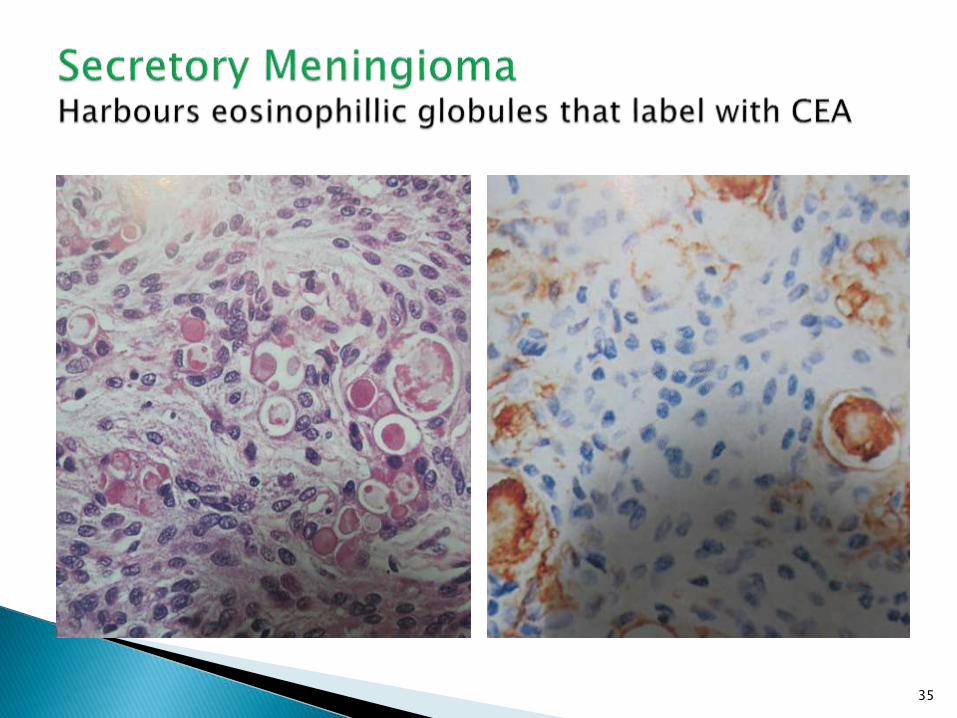
Syncytial (Meningotheliomatous) meningiomai. Lobular microarchitectureii. Cells having delicate round/oval nuclei, inconspicuous nucleoli,lightly eosinophilliccytoplasm and indistinct cytoplasmic borderiii. Tumor cells arranged in tight whorlsiv. Nuclear clearing and pale nuclear
pseudoinclusion containing invaginatedcytoplasm.v. Psammoma bodies
32

33

34
35

36

Mixed(transitional) M
Psammomatous M
Angiomatous M
Microcystic M
Lymphoplasmacyte-rich M
Metaplastic M
Choroid M
Clear cell M
Rhabdoid M
Atypical M
Anaplastic M
37

3 tiers of increasing biologic potential Meningioma WHO Gr-I Atypical Meningioma WHO Gr-II Anaplastic Meningioma WHO Gr –III
Atypical Meningioma define as A)4/more MF/10 HPFB)At least 3 of i)Hypercellurarity
ii)Paternless sheet like growthiii) Macronucleoliiv) Small cell with high N/C ratiov) Necrosis
Anaplastic Meningiomai) 20 or more MF/10HPF orii) Exibiting loss of differentiated features resulting
in CA, Melanoma,Sarcoma like appearance
38

39










![Pharmacology – II [PHL 322] CNS Depressants Dr. Mohd Nazam Ansari.](https://static.fdocuments.us/doc/165x107/56649d1f5503460f949f3aa4/pharmacology-ii-phl-322-cns-depressants-dr-mohd-nazam-ansari.jpg)




