CMV: An Update - Academy · CMV: An Update Jay A. Fishman, M.D. Professor of Medicine, Harvard...
60
CMV: An Update Jay A. Fishman, M.D. Professor of Medicine, Harvard Medical School Director, Transplant Infectious Disease and Compromised Host Program, Massachusetts General Hospital Associate Director, MGH Transplant Center, Boston, MA, USA
Transcript of CMV: An Update - Academy · CMV: An Update Jay A. Fishman, M.D. Professor of Medicine, Harvard...

CMV:AnUpdate
JayA.Fishman,M.D.Professor ofMedicine,HarvardMedicalSchool
Director,TransplantInfectiousDiseaseandCompromised HostProgram,MassachusettsGeneralHospital
AssociateDirector,MGHTransplantCenter,Boston,MA,USA

Virusesmaybedangerous....

Cytomegalovirus
• Betaherpesvirinae subfamilyoftheHerpesviridae• Thestructure:
– Nucleuscontainingtheviralgenome(lineardouble-strandedDNA)– Icosahedral proteincapsid– >200geneswithsignificantvariation– Thetegumentproteinmatrix(e.g.,pp65):
• Proteinswithstructuralroles• Proteinswhichmodulatestheimmunehostcellresponse
– Anouterenvelopederivedfromthehostcellnuclearmembrane.• GlycoproteingB - involved incellattachmentandpenetration• GlycoproteingH- involved inthefusionoftheviralenvelopewiththehostcellmembrane
Pérez-Sola,M.J.etal.EIMC2008;26(1):38-47
CroughTetal.ClinMicrobRev,Jan2009,76-98

PathogenicConsiderations
• Longerreplicationcyclethanotherherpesviruses• Reactivation ofviralreplicationisrelatedtohostimmunityand
inflammation• “CMVInfection”isnotuniform
– ManygeneticvariantstrainsofCMVwithmultipletargetcells:Monocytes,macrophages,endothelialcells,epithelialcells,parenchymalcells,immaturedendriticcells,lymphocytes,CD34+cells
– “Latency”inmultiplecelltypes– Biologicaleffectsvarybyviralstrain:
• Cellulartropism,penetrationandtransfertothecellnucleus
• Viralgeneexpressioniscelltype-specific• Replicationandspreadtoothercells(virulence)• Immuneresponsestoinfectionbycelltype

DisseminatedCMV
Liver
LungKidney
Colon

RiskfactorsforCMVdiseaseinsolid-organtransplantpatients
§ Primaryinfection(D+/R−)§ Transplantedorgans,cells§ Bloodproducts
§ FactorsfavoringCMVreactivation§ Inflammation/Fever (cytokines)§ Surgery/Trauma§ Intraoperative hypothermia§ Sepsisorseverebacterial
infections§ T-celldepletion§ Co-infectionswithotherviruses
§ Herpesvirus6or7(HHV6or7)
Factorsfavoringprogressiontoinvasivedisease• Immunosuppression
• T-celldepletion• Mycophenolate,azathioprine• Methylprednisoloneboluses• Alemtuzumab• Highviralload
• Immunomodulation• Herpesvirus6(HHV6)orHHV7
• Geneticfactors• MutationsinTLR2andTLR4genes• Deficiencyofmannose-binding lectin orgenotypeassociatedwithlowproduction ofMBL
ModifiedfromGESITRA-SEIMC/REIPIrecommendationsforthemanagementofCMVinfectioninsolid-organ transplantpatients,Enferm InfeccMicrobiol Clin.2011

CMVreplicationandrelease
PathwaysforCMVreactivation
ReinkePetal.TransplantInfectDis 1999;1:157-64.
TNF-α
NF-κBStress
catechols
Pro-inflammatoryprostaglandins
cAMP
EICMV
Anti-T-cellantibodies

InmunecontrolofHCMVbyinnateandadaptativeimmunity
TaniaCrough.ClinMicrobRev.,Jan.2009,p.76–98
Replicationinmucosalepithelium
Limitedimmunerecognitionbyeffectorcells;latentreservoir
Reactivationfromlatency
ProcessingbyAPC;presentationtoAg-
specificcellsDC/MQà cytokines/chemokinesàactivateinnateimmunecells
B-cellsactivatedbyAPCsà AbsCMV-infectedMѲ à stimulateAg-specificT/NKcellsà IFNs,
TNF,cytolysis

1. CMVinhibitsdifferentiationofmyeloidantigen-presentingcellsfrommonocyticprecursors(transientblockinthecytokine-induceddifferentiationofmonocytesintofunctionallyactiveCD1a-positivedendritic cells)
2. CMValterstheimmunostimulatory propertiesofdifferent subsetsofmonocytesandDC,rendering themlesscapableofdeveloping intoprofessionalAPCs.
3. VirallyencodedIL-10(cmvIL-10)blunts theantiviralpropertiesofAPCs.4. HCMVhampersantigen-presentingcelltraffickingandphagocytic capacity.
– DecreasedAPCmigrationtositesofinflammationandtodraining lymphnodesinresponsetochemotactic stimuli(RANTES,MIP-1,andMIP-3)
• HCMV-infectedPlasmacytoid DCshavereducedsecretionofcytokinesincluding IFN-γ,reducedallostimulation,decreasedCD4andCD8T-cells
5. Transitorybutsubstantialimmunosuppressionthatinhibits theimmuneresponseagainstthevirusandunrelatedpathogens,mainlyinsubjectswithprimaryinfection
• Reactivationofotherviralinfectionsduring acuteHCMVinfection• Enhancespre-existingimmunosuppression insolid-organ transplantand
alloSCT recipients, increasingtheirriskforinvasivebacterialandfungalinfections
CMVaffectsmanyfunctionsofantigen-presentingcells

CMVRetinitis:LungTransplantRecipient

CMVcecalulcerationinpatientwithnegativeantigenemiaandPCRassaysforCMV

DirectEffects:InvasiveInfectionbyCMVInvasiveColitisAfterLiverTransplant

EffectsofViralInfectioninTransplantation
• “DIRECTEFFECTS”-- CAUSATIONOFINFECTIOUSDISEASESYNDROMES– Feverandneutropenia,hepatitis– Colitis,Retinitis,Nephritis,Pancreatitis
• “INDIRECT”orIMMUNOMODULATORYEFFECTS– SystemicImmuneSuppressionà OI’s– GraftRejection,GVHD– AbrogationOfTolerance
• Oncogenesis/CellularProliferation– HepatitisB:hepatocellular carcinoma– EpsteinBarrVirus:B-celllymphoma(PTLD)– HepatitisC:splenic lymphoma(villouslymphocytes)– Papillomavirus:Squamous cell&anogenital cancer– HHV8(KSHV):Kaposi’ssarcoma,effusionlymphoma– Acceleratedatherogenesis,BK-uretericobstruction

CMVSyndromeFever
WeaknessMyalgiaArthralgia
Myelosuppression
EndOrganDiseaseNephritisHepatitisCarditisColitis
PneumonitisRetinitis
Encephalitis
CMVdisease
LatentCMVinfection
ActiveCMVinfection(viremiaandintissue)
ALG,Fever,TNFα,Sepsis,Suppression
AtherosclerosisBronchiolitisobliterans
Vanishingbileductsyndrome
Opportunisticinfection
Systemicimmunesuppression
Acute Chronic Acute
Cellulareffects:antigenandcytokine
expression
EBV-associatedPTLD
Allograftinjury1
Allograftrejection1
FishmanJA&RubinRHNEngl JMed.1998;338:1741
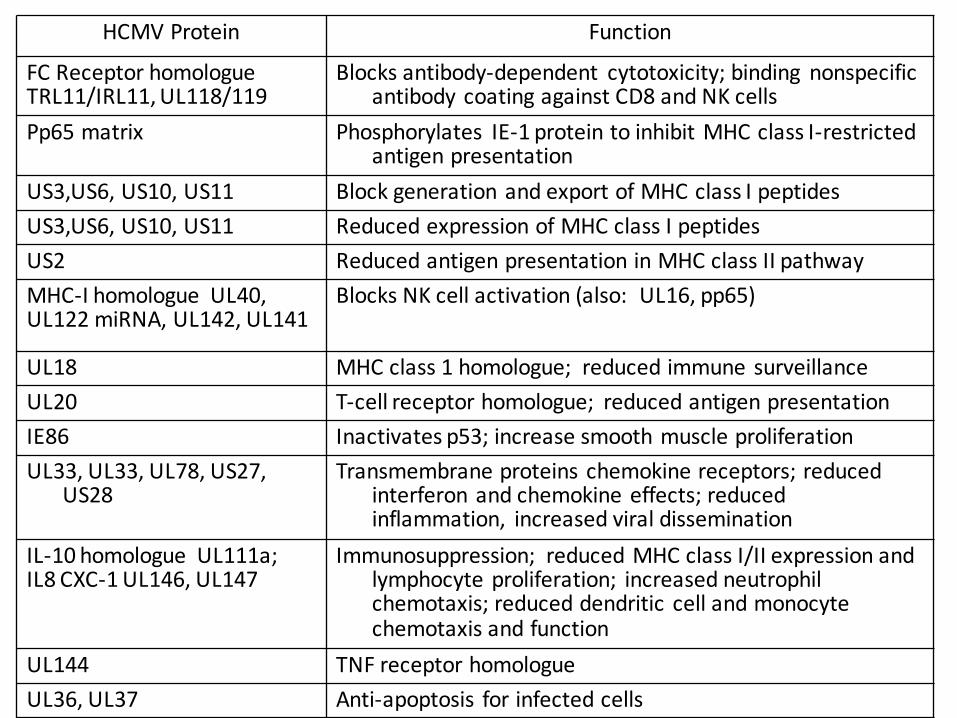
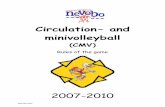
HCMVProtein Function
FCReceptorhomologueTRL11/IRL11,UL118/119
Blocksantibody-dependent cytotoxicity;binding nonspecificantibodycoatingagainstCD8andNKcells
Pp65matrix Phosphorylates IE-1proteintoinhibitMHCclassI-restrictedantigenpresentation
US3,US6,US10,US11 BlockgenerationandexportofMHCclassIpeptidesUS3,US6,US10,US11 ReducedexpressionofMHCclassIpeptidesUS2 ReducedantigenpresentationinMHCclassIIpathwayMHC-Ihomologue UL40,UL122miRNA,UL142,UL141
BlocksNKcellactivation(also:UL16,pp65)
UL18 MHCclass1homologue; reducedimmunesurveillanceUL20 T-cellreceptorhomologue; reducedantigenpresentationIE86 Inactivatesp53;increasesmoothmuscleproliferationUL33,UL33,UL78,US27,
US28Transmembraneproteinschemokinereceptors;reduced
interferonandchemokineeffects;reducedinflammation, increasedviraldissemination
IL-10homologue UL111a;IL8CXC-1UL146,UL147
Immunosuppression; reducedMHCclassI/IIexpressionandlymphocyteproliferation; increasedneutrophilchemotaxis;reduceddendritic cellandmonocytechemotaxisandfunction
UL144 TNFreceptorhomologueUL36,UL37 Anti-apoptosis forinfectedcells

CMVinterfaceswithinnateandadaptiveimmunesystems
CroughandKhanna,ClinMicrobiol Rev2009
Areasofinvestigation:
- Migrationandchemotaxis
- Cellulardifferentiation- Cellsurvivaland
apoptosis- Determinantsof
reactivationandlatency
- Pathogenrecognition- Globaltranscriptional
andfunctionalchanges

CMV“IndirectEffects”:PossibleMechanisms• UpregulationofMHCclassIIantigensandhomologybetweenCMVIEantigen
andMHCclass-I(HLA-DRβ)1-2
• BlockofCD8+(MHCclassI)recognition• BlocksCMVantigenprocessinganddisplay(immediateearlyAgmodification,
poorCTLresponse)• IncreasedICAM-1,VCAM,cellularmyc&fos(adhesion)• InversionofCD4/CD8ratio3-4
• Increasedcytokines:IL-1β,TNFα,IFNγ,IL-10,IL-4,IL-8,IL-2/IL-2R,C-X-Cchemokines,andIL-85-6
• IncreasedcytotoxicIgM7
• Stimulationofalloimmuneresponsebyviralproteins1-2
• IncreasedPDGF,TGFβ;autoantibodies• IncreasedgranzymeBCD8+T-cells,γδ-T-cells
ICAM-1=Intercellularadhesionmolecule-1PDGF=Platelet-derivedgrowthfactorVCAM=Vascularcelladhesionmolecule
1.Fujinami RS,etal.JVirol. 1988;62:100-105.2.BeckS.Nature. 1988;331:269-272.3.SchooleyRT,etal.NEnglJMed.1983;308:307-313.4.Fishman JA,etal.DiagnImmunol.1983;1:261-265.5.KernF,etal.JAmSocNephrol.1996;7:2476-2482.6.TongCY,etal.JMedVirol.2001;64:29-34.7.BaldwinWM3rd,etal.BrMed(ClinResEd).1983;287:1332-1334.

Mechanisms– ShortVersion– ⇑ Adhesionmolecules(VCAM,ICAM,LFA-1,VLA-4)
– ⇑ Pro-inflammatorycytokines– ⇑ HLA-DRandMHCClassImimic– ⇑ Anti-endothelialAbs?– ⇓ Antigenpresentation(dendriticcellmaturation)
– ⇓ Leukocytemobilization

OpportunisticInfectionsPromotedbyCMVInfectioninTransplantPatients
• Pneumocystiscarinii• Fungalinfections(esp.intra-abdominaltransplants):• Candidemia andintra-abdominal infection inOLTx;patientswithinitialpoorgraftfunction
• Aspergillusspp.RoleofCMVinpromotingfulminant HCVhepatitisratherthandirecteffect
• Bacteremia:Listeria monocytogenes• Epstein-Barrvirusinfection(RCWalkeretal,CID,1995,20:1346-55),HHV6,HHV8/KSHV?
• HCV:riskforcirrhosis,retransplantation,mortality

IndirectEffectsofCMV:Organ-specific• Renal:Decreasedearlygraftfunctionandsomechronicdysfunction(increased
byHHV6andHHV7)– AcutebutpossiblynotchronicallograftrejectionisreducedbyCMV
prophylaxis
• Liver:CMVassociatedwithcirrhosis,graftfailure,needforretransplantation&death– MoreaggressiveHCVrecurrenceandfibrosisafterOLTx (partially
attributedtoHHV6)– CMVdiseaseispreventable
• Heart:cardiacallograftvasculopathy– Reducedbyganciclovir +/- CMVIg
• Lungs:CMVandD+/R- associatedwithBronchiolitisObliteransSyndrome,infection,death– Reducedbyivganciclovir +/- CMVIg
• Pancreas:Notstudied(noCMVyetinislets)

CMVandHSCTOpportunisticInfections
MarretalBlood2002 Nichols etalJID2002

Therapeutics- Terminology• Whatareyoumeasuring?
– Antigenemia– measuringCMVspecificantigeninPBMCs,forexamplepp65assay
– Viremia– culture-basedonly(requiresreplicatingvirus)– DNAemia – measuringCMVDNAbyQNAT (wholebloodor
plasma)QNATcalibratedtotheWHOstandardispreferredfordiagnosis,decisionsregardingpreemptiveantiviraltreatment,andmonitoringresponsetotherapy.
– TissueorBAL– mustbenormalizedtohousekeepinggene,urea,unitvolume,unitmass.
– Viralassaysandcultureofblood,urine,ororalsecretionsarediscouragedinadultsfordiagnosisofactiveinfectionordisease.
• Serology– PositiveIgGisamarkerofpreviousexposure(positive
serologydoesnotdefine“activeinfection”)

Recommendations:Diagnostics• EitherplasmaorwholebloodisanacceptablespecimenforQNAT.Specimentypeorassayshouldnotbechangedwhenmonitoringpatients.
• DespitereportinginIU/ml,viralloadvaluescannotbedirectlycomparedacrosscentersand/orlaboratoriesunlessidenticaltestingreagentsandprocedurescanbeassured.
• Changesinviralloadexceeding0.5log10IU/ml(3-fold)areconsideredtorepresentclinicallysignificantdifferencesinDNAemia

Terminology2
• Surveillance – patientisatrisk,butnoevidenceofanevent(infection)orbiomarker(NAT)
• Monitoring – Patienthaseventorbiomarker(previouslyknownpositiveassay)
• Hybridapproach– universalprophylaxisfollowedbypreemptivetherapy(surveillanceafterprophylaxis)

DoweknowhowtoPreventCMVInfection?
Universalvs.Pre-emptivetherapy

Prophylaxisvs PreemptiveTherapy
• ProphylaxismaybepreferredinD+/R-,withD+orR+&antilymphocyte therapy,potentimmunosuppression including desensitization (plasmapheresis orimmunoadsorption) andABOincompatibleprotocols,orwithrituximab,bortezomib,eculizumab.Rolewithbelatacept hasnotbeenstudied.
• Treatmentofacuterejectionwithantilymphocyte antibodies inat-riskrecipientsshould resultinreinitiation ofprophylaxisorpreemptivetherapyfor1to3months
• CMVDNAemia iscommonaftercessationofprophylaxis,notablyinhighriskpatients
Prophylaxis PreEmptiveTherapy
EarlyCMVDNAemia Rare CommonPreventionofCMVdisease Goodefficacy Goodefficacy*
(*less optimalinhighriskpopulations)
LateCMV(infection/disease) Common RareResistance Uncommon UncommonEaseofimplementation Relativelyeasy MoredifficultOtherherpesviruses PreventsHSV,VZV DoesnotpreventOtherOpportunisticinfections Mayprevent UnknownCost Drugcosts Monitoringcosts
Safety Drugsideeffects Lessdrugtoxicity
Preventionofrejection Mayprevent Unknown
Graftsurvival Mayimprove Mayimprove

Time(days)
DoublingTime=ln2/a
y=y0eax
AverageDT=1-2days
Log 1
0ViralLoa
d
detectionthreshold
Preemptive inD+/R-
LisboaLF,etal.Abstractpresentedat:AmericanTransplantCongress;May30-June 3,2009;Boston,Massachusetts.Abstract388. DT=Doublingtime

CMVdiseaseinD+/R- renalrecipients:Meta-analysis(allagents)
• UniversalandPre-emptiveprophylaxissignificantlyreducetheriskofCMVdisease
-81%
-64%
-100%
-80%
-60%
-40%
-20%
0%Universal Pre-emptive
CM
V di
seas
e ris
k re
duct
ion
(%)
p=ns
Kalil AC et al. Ann Intern Med 2005; 143: 870

Anti-CMVProphylaxisIsAssociatedWithIncreasedRenalGraftSurvivalat4Years(P=0.0425)
1009080706050
0
Oralganciclovirprophylaxis
IVpreemptivetherapy
Freedo
mfrom
graftlo
ss;
uncensored
ford
eath(%
)
1 2 3 4Timeaftertransplantation(years)
KliemV,etal.AmJTransplant. 2008;8:975-983. (B)Khoury JA,etal.AmJTransplant.2006;6:2134-2143. (VGCV)(B)ReischigT,etal.AmJTransplant. 2008;8:69-77. (VACV)(B)
Pvalue(Logranktest)=0.0425
ProphylaxisreducedCMVinfectionby65%(P<0.0001)

Effectofanti-CMVprophylaxisonconcomitantinfections
0.31
0.65
0.27
0.0
0.2
0.4
0.6
0.8
1.0
Placebo/notreatment
Herp. Simplex,Varic. Zoster
Bacterialinfections
Protozoalinfections
Rela
tive
risk
-73% -69%-35%
Hodson EM et al. Lancet 2005; 365: 2105
FungalInfections

l Statisticallysignificantriskreductionofmortalitywithuniversalprophylaxis(Kaliletal)andallcausemortality(Hodsonetal).
Mortality:universalprophylaxisvs.pre-emptivetherapy
-38%
-6%
-60%
-50%
-40%
-30%
-20%
-10%
0%Prophylaxis Pre-emptive
Mor
talit
y: ri
sk re
duct
ion
(%)
Kalil AC et al. Ann Intern Med 2005; 143: 870Hodson EM et al. Lancet 2005; 365: 2105
p=0.032
p=ns

àD+/R+recipientsonpreemptivetherapyhadhighestrateofCMVdisease(19.2%vs.4.4%,P0.003).àNochgGFR,rejection,graftloss(5yrf/u)
11%
39%

D+R−onPre-emptiveTherapy:DirecteffectsofCMVandanti-CMVtreatment
Prophylactic(n=32)
Preemptive(n=80)
PValue
CMVinfection 11(34%) 40(60%) 0.02CMVdisease 5(16%) 21(26%) 0.3Late-onsetinfection 9(28%) 6(8%) 0.003Peakviralload(mean,log10copies/mL)
4.2±1.1 5.0±1.0 0.06
Anti-CMVdrugresistance 1(3%) 13(16%) 0.05RecurrentCMV 3(9%) 18(23%) 0.1
Couzietal,High IncidenceofAnticytomegalovirusDrugResistanceAmongD+R−KidneyTransplantRecipientsReceivingPreemptiveTherapy,AJT,2011

Prophylaxis,Pre-emptiveTherapy,andHybridCare
1 32 765Transplant Months
Pre-emptivemonitoringperiod(onceweeklyfor12-16weeks);ifCMVdetected(viralloadorpp65Ag),treatuntilcleared
indicatesCMVsurveillancebyviralload(orpp65Ag)
AmericanSocietyofTransplantation.AmJTransplant2004;4:51–8
Prophylaxisperiod(commonly90–100days)
HYBRID:Prophylaxis+Monitoring

Long-TermOutcomesofPreemptiveValganciclovirComparedwithValacyclovirProphylaxisforPreventionofCMVinRenal
Transplantation
JournaloftheAmericanSocietyofNephrologybyAmericanSocietyofNephrologyReproducedwithpermissionofAMERICANSOCIETYOFNEPHROLOGYintheformatRepublishincontinuingeducationmaterialsviaCopyrightClearanceCenter. 35


Cooking upahybridstrategybyDavide Abate

Hybrid Approaches Vary
• Inpre-emptivetherapy:• Surveillanceonceweeklyfor3- 4months• NAT-DNAemia atpositivethresholdà treatmentdose+/- reductionin
immunuosuppression forminimumof2weeksoftreatment.• Afterresolution,discontinueantiviralandcontinueweeklysurveillance.• SpecificthresholdsfordefiningoptimalPEThavenotyetbeendefined
• Useofsurveillanceafterprophylaxismaybeconsideredinpatientsconsideredatincreasedriskforpost-prophylaxisCMVdisease(e.g.,weeklyfor~8-12weeks).
• Specialgroups:• D+/R- patientsafterliver,heart,andpancreas3-6monthsdependingonthedegreeof
immunosuppression, includingantilymphocyte antibodiesforinduction.• D+/R- lungtransplantrecipients:6-12months.R+lungtransplantrecipients6months
prophylaxiswhileD+/R+areathigherriskfordevelopingCMVdisease.
• Limitedreportsdonotsupporttheroutineuseofsecondaryprophylaxis.

• ProspectivecohortstudyofconsecutiveCMV+SOTpatientsundergoingkidney,liver,liver–kidney)andhearttransplantation
• Lowrisk,R+,noanti-lymphocytedepletiontherapy• Testedevery2weeks(first100days)&every4weeks(day100-
180),~10-11testseach• Aviralloadof3983IU/ml*(2600copies/ml)wasestablishedas
theoptimalcut-off;99.6%NPV,sensitivity90%,specificity89%• AmajorityofpatientswillnotdevelopCMVdiseasewithout
specificantiviraltherapy(18of393incohort;15beforeday100)
• Limitations:can’tapplyifhigherrisk,ATGuse,differentISregimen 39

SpecialCases• Transplantrecipientsonmammaliantargetofrapamycin
(mTOR)inhibitorssuchassirolimus andeverolimusmayhavelowerratesofCMV;whetherthisshouldaltertheirpreventionstrategyisunknown.Effectisdose-dependent.
• TherearelimiteddatatosupporttheuseofCMVimmunoglobulin(CMVIg)forprophylaxiswhenappropriateantivirals aregiven.

Molecularmechanismsofanti-CMVeffectsofmTORinhibitors

• CMVeventsaftersolidorgantransplantationoccurredsignificantlymoreoftenunderCNIs(RR=2.27)thanwithrapamycin.
• mTOR-I+CNIvs.CNIalonein15trialsofkidney,heart,andlivertransplantationàhigherCMVincidencewhenpatientsreceivedanmTOR-Ifreeimmunosuppression(RR=2.45).

AllCMVIgG+@transplant;switched@6mos
prednisolone/MMFprednisolone/everolimus
prednisolone/CyA

mTOR Effectisdosedependent
AJT,11:2453–2462,November2011

CookingTreatmentRecommendations
TherapeuticMastersforCMV

Agent Route Target Toxicity Availability
Ganciclovir(GCV)
IV>>PO UL54,DNApolymerase
Marrow Yes
Valganciclovir(VGCV)
PO UL54,DNApolymerase
Marrow Yes
Foscarnet IV UL54,DNApolymerase
Renal,metabolic
Yes
Cidofovir(CDV)
IV UL54,DNApolymerase
Renal Yes
Brincidofovir(CMX001)
PO UL54,DNApolymerase
Less renalthanCDV
NotforCMV
Letermovir(AIC246)
PO/IV UL56, DNApackaging
Limited Experimental
Maribavir(MBV)
PO UL97, egress Limited Experimental
Anti-CMVAgents
NEWAGENTSWILLNOTCOVERHSV-VZVASWELLAS
VALGANCICLOVIR.

Therapy• WiththeuseofhighlysensitiveQNAT(LLOQ<200IU/ml),considerdiscontinuingtherapyafteroneresultislessthantheLLOQ.Confirmatorytestingshouldbedoneoneweekafterdiscontinuingtherapy.
• Iftheassayisnothighlysensitivethen2consecutiveundetectable(negative)resultsareneededtodiscontinuetherapy
• Drugresistanceshouldbesuspectedinpatientswithclinicaltreatmentfailuredespitegreaterthantwoweeksofantiviraltreatment

UL97Mutations
FoldchangeinganciclovirEC50a
Genotypefrequency
5-15x 2-5x <2x
Mostcommon M460V/I,H520Q,A594V,L595S,C603W
C592G
Lesscommonatcodons460,590-
607
M460T,A594G,595delb,L595F/W,E596Y,597del2b,
599del,K599T,600del,601del,601del2,C603R,C607Y,del(≥3)c
A591V,A594E/T,E596G,C603S,596delb,600del2,C607F
E596D,N597D,K599E/R,L600I,T601M,D605Ed
Atypicalloci F342Se,K355Me,V356Ge,V466Ge,C480Re,C518Y,P521Le
L405P,I610T,A613V M615V,Y617H,A619V,L634Q,E655K,A674T
(a)Moderateresistance(5-15x),low-graderesistance(2-5x),orinsignificantresistance(<2x)
(b)=inframedeletionofcodon
(c)Inframedeletionof≥3codons inthe590-607rangecanbeassumedtoconfermoderateganciclovirresistance(8- to15-fold).Deletionoflessthan3codonsmayconfervaryingdegreesofganciclovirresistance(4- to10-fold).
(d)D605E isabaselinesequencepolymorphismcommonineastAsia,unrelatedtodrugresistance
(e)Maribavircross-resistancedocumented,allexceptF342Saremarkedlygrowth-inhibited

AlgorithmforSuspectedCMVResistance
Kotton CN et al. UpdatedInternational Consensus Guidelines ontheManagementofCytomegalovirusinSolid-OrganTransplantation.Transplantation. 2013;96(4):333-360.
Genomesequence ofUL54andUL97
Caveats• Notallgenesaresequenced• Notallmutationsareknown• Notallmutationsareequal• Somemutationsassociatedwithdecreasedviralfitness• Polyclonalinfectionsarecommon
Kotton 2013

CMVUL54DNAPolymeraseMutations
Exo andregionVmutationsconferGCV-CDVcross-resistanceFOS-Rmutationsmayconferlow-gradeGCV±CDVcross-resistance
CrossResistance

Lurain NS,Chou S.Antiviraldrugresistanceofhuman cytomegalovirus.Clin Microbiol Rev.2010;23(4):689-712.
Ratio=IC50 ofmutant/IC50 ofwildtype
“IfatypicalUL97mutationthatconfersa5- to10-foldincreaseinGCVresistanceisdetected,aswitchtoFOSisindicated,especiallyinthepresenceofongoing diseaseorhighandincreasingviralloads.”

Immunology• Serostatus isusefulbutreflectshighlyvariablepopulations
intermsofpredictionofriskforCMVinfection.• IgG hypogammaglobulinemia isassociatedwithanincreased
riskofCMVdiseaseaftertransplantation.Measurementoftotalimmunoglobulins issuggestedinsituationswhereCMVisdifficulttocontrol.
• CMV-specificcellularimmunemonitoringhasbeenshowntopredictCMVinfectioninthepre-transplantandpost-transplantsettingsinprospectiveobservational,multi-centerstudies.InterventionalstudiestodeterminepreciseclinicalutilityofCMIareongoing.
• CMVvaccinesareinpreclinical,phaseIandphaseIItrials.TheprimarygoalofaCMVvaccineshouldbetopreventormodulateCMVreplicationand/orCMVdisease.
• T-celltherapiesshouldbefurtherevaluatedforresistant/refractoryCMV.

PredictiveMarkers?• Serostatus basedriskstratification(i.e.D+ /R−,D+ /R+,D−/R+,andD−/R−)hidesasubstantialheterogeneityoftheindividualrisksforCMVreplicationandprogressiontoCMVdisease.• TheriskofCMVdiseaseamongD+ /R−patientsinthefirstyearposttransplant rangefrom6.4to58.3%whentheorganrecipientswereregroupedaccordingtoCMV-specificcell-mediatedimmunitytestingresultsattheendofantiviralprophylaxis.• Testsandmarkerscapableofindividualizing theriskofCMVreplicationmaysignificantlyimproveCMVpreventative strategies.

Cell-mediatedimmunitytopredictcytomegalovirusdiseaseinhigh-risksolidorgantransplantrecipients:LateonsetCMV.
• UtilityoftestingCD8+T-cellresponseagainstCMVasapredictoroflate-onsetCMVdiseaseafterastandardcourseofantiviralprophylaxis.108evaluablepatients(D+/R+n=39;D-/R+n=34;D+/R- n=35)ofwhom18(16.7%)developedsymptomaticCMVdisease.
• TestingusingtheQuantiFERON-CMVassayatbaseline,1,2and3monthsposttransplant (21-peptidepool).
• CMIwasdetectablein38/108(35.2%)patients(cutoff0.1IU/mLinterferon-gamma).
• CMVdiseaseoccurredin2/38(5.3%)patientswithadetectableinterferon-gammaresponseversus16/70(22.9%)patientswithanegativeresponse;p=0.038.
• InthesubgroupofD+/R- patients,CMVdiseaseoccurredin1/10(10.0%)patientswithadetectableinterferon-gammaresponse(cutoff0.1IU/mL)versus10/25(40.0%)patientswithanegativeCMI,p=0.12.
• MonitoringofCMImaybeusefulforpredictinglate-onsetCMVdisease KumarDetal.AmJTransplant.2009May;9(5):1214-22.

IFN-γ andCMVDisease
P=0.02
DetectableIFN-γ CD8+response
NoDetectableIFN-γ CD8+response
KumarD,etal.AmJTransplant. 2009;9:1214-1222.(B)
0 10 20 30 40 50 60 70 80 90 10050
60
70
80
90
100
Timeafterstoppingprophylaxis(days)
Free
domfrom
CMVdisease(%
)

Chemokines andImmuneControlofCytomegalovirusinOrganTransplantRecipients.
• CMVviremic organtransplantrecipients,chemokineexpression—specificallythechemokineCCL8(AUC0.84995%CI0.721–0.978;p = 0.003)andtheinterferon-γ inducedchemokineCXCL10(AUC0.841,95%CI0.707–0.974;p = 0.004)—wereassociatedwithcontrolofviralreplication.
• HomozygousTTpolymorphismintheCCL8promoter(SNPrs3138035)ofD+/R- transplantrecipientsconferredanincreasedriskofviralreplicationafterdiscontinuationofantiviralprophylaxis(hazardratio3.6;95%CI2.077–51.88).
• TheprimarycelltypeproducingCCL8inresponsetoCMVpeptidestimulationwasthemonocyte fractionwhereCCL8productionisassociatedwithspontaneousviralclearanceinpatientswithCMVviremia. Thereisdose-dependentreductioninCCL8productionwithimmunosuppression.Lisboa,L.F.etal.(2015),AmericanJournalofTransplantation.doi: 10.1111/ajt.13207

Virus-SpecificTcellAdoptiveTransfer
Ridell etalScience1992

Leen etalBlood2013Papadopoulou etal.Sci TransMed2014
• PBMCsfromHLAhomozygous,seropositivedonors• Generatedtrivalent(CMV,EBV,AdV)CD8Tcells• CreatingabankofreadytousevirusspecificCTLs
• Identified50patientswithrefractoryviralinfectionsafterSCT
• MatchedHLAofvirusspecificTcellswithpatients• AdoptivetransferofvirusspecificTcellsweekly• Subsequently havedevelopedpentavalent Tcells(CMV,
EBV,HHV6,AdV,BKV)

Valganciclovir
Valganciclovir ->Ganciclovir
HighdoseGanciclovir+Foscarnet
HighdoseFoscarnet
CMVTcells
UL54K513N
UL54A834P
CMVdiseaseafterSCT

MajorChanges• Biology:MechanismofCMVeffectonmacrophagefunctionappearstobeviainhibitionofinflammatorypathways.
• QNAT:increasedsensitivityà positiveinGIdiseaseandsinglenegativeassaymaybesufficientforstoppingtherapy
• Prophylaxisroutinein:– AllD+R-– D+orR+heartandlungs.
• Multiplenewdrugsà soon?• UseofCMV-specificT-celltherapymightaddressresistance.