Clostridium difficile two-step algorithmic testing
28
1 Clostridium difficile two-step algorithmic testing Adam Caulfield, PhD Spectrum Health Regional Laboratory SCACM September 29, 2017
Transcript of Clostridium difficile two-step algorithmic testing
1
Clostridium difficile two-step
algorithmic testing
Adam Caulfield, PhD
Spectrum Health Regional
Laboratory
SCACM
September 29, 2017
Outline
• C. difficile epidemiology
• Clinical criteria for testing
• Lab criteria for testing
• Test methods
• Standalone nucleic acid amplification tests (NAAT)
• Algorithm: enzyme immunoassay (EIA) + NAAT
• Comparison data
2
Clostridium difficile epidemiology
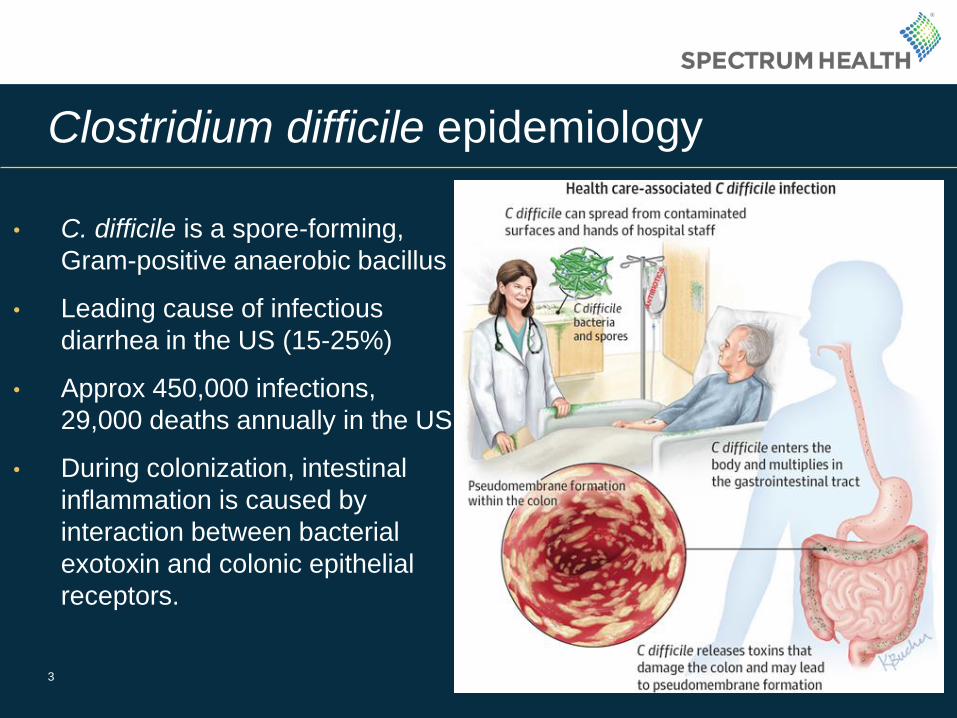
• C. difficile is a spore-forming,
Gram-positive anaerobic bacillus
• Leading cause of infectious
diarrhea in the US (15-25%)
• Approx 450,000 infections,
29,000 deaths annually in the US
• During colonization, intestinal
inflammation is caused by
interaction between bacterial
exotoxin and colonic epithelial
receptors.
3

Clostridium difficile epidemiology
• 30-50% of antibiotics prescribed
in hospitals are unnecessary or
incorrect.
• C. difficile accounts for 15-25%
of antibiotic associated diarrhea.
• $9,000-13,000 per case
• US annual cost: $500 million –
$1.5 billion (Seo et al, 2016, J
Clin Lab Anal).
4
Guidelines
• IDSA/SHEA: Cohen S.H. et al., Clinical practice guidelines for Clostridium difficile infection in adults: 2010
update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society
of America (IDSA). Infect Control Hosp Epidemiol, 2010. 31(5): p431-55.
• ACG: Surawicz C.M. et al., Guidelines for diagnosis, treatment, and prevention of Clostridium difficile
infections. Am J Gastroenterol, 2013. 108(4): p478-98.
• ESCMID: European Guidelines: Crobach et al, European Society of Clinical Microbiology and Infectious
Diseases: update of the diagnostic guidance document for Clostridium difficile infection. Clin Microbiol
Infection. 2016. 22: S63-S81
• ASM: Spring 2018?
• 1.) Only patients with significant diarrheal stool are tested (3+ in 24 hr).
• 2.) Do not test for cure.
• 3.) Do not perform repeat testing. Within 7 days is generally considered to be
unnecessary (positive results can persist after effective treatment).
• 4.) Asymptomatic patients should not be tested as a positive result represents
colonization and should not be treated.
• 5.) Method: either NAAT or two-step (EIA composed of GDH/toxin plus NAAT)
5
Clinical diagnosis
• C. difficile infection (CDI) –
no formal clinical
definition.
• Limit testing in low risk
populations (influences
predictive value of testing).
• Avoid testing of patients
with other explanations for
diarrhea: laxatives, IBD,
recent abdominal surgery,
viral illness, etc. 6
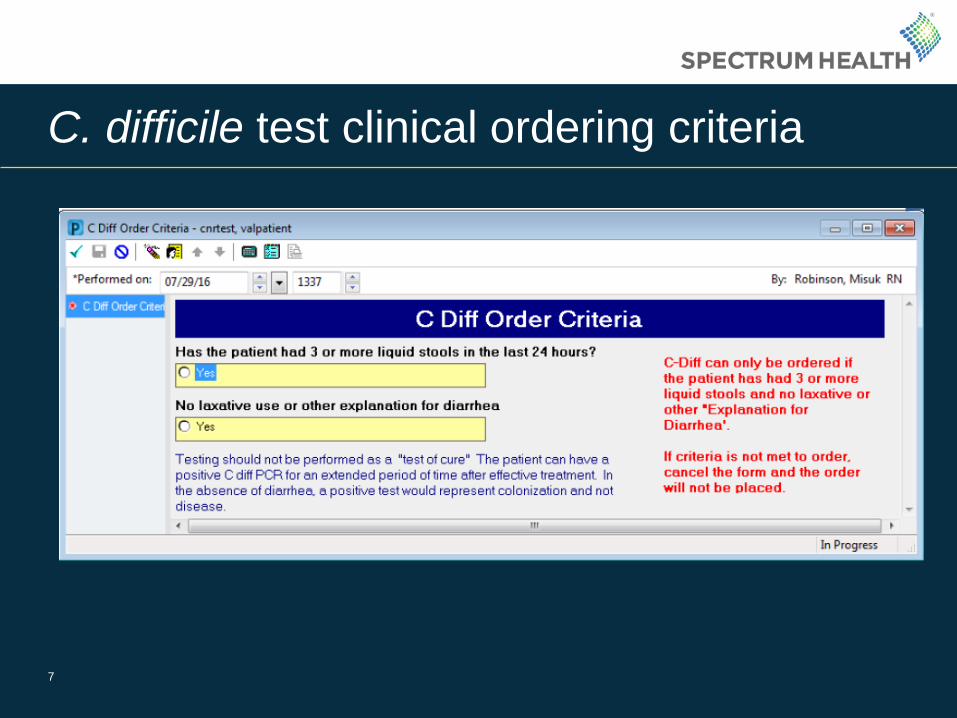
C. difficile test clinical ordering criteria
7
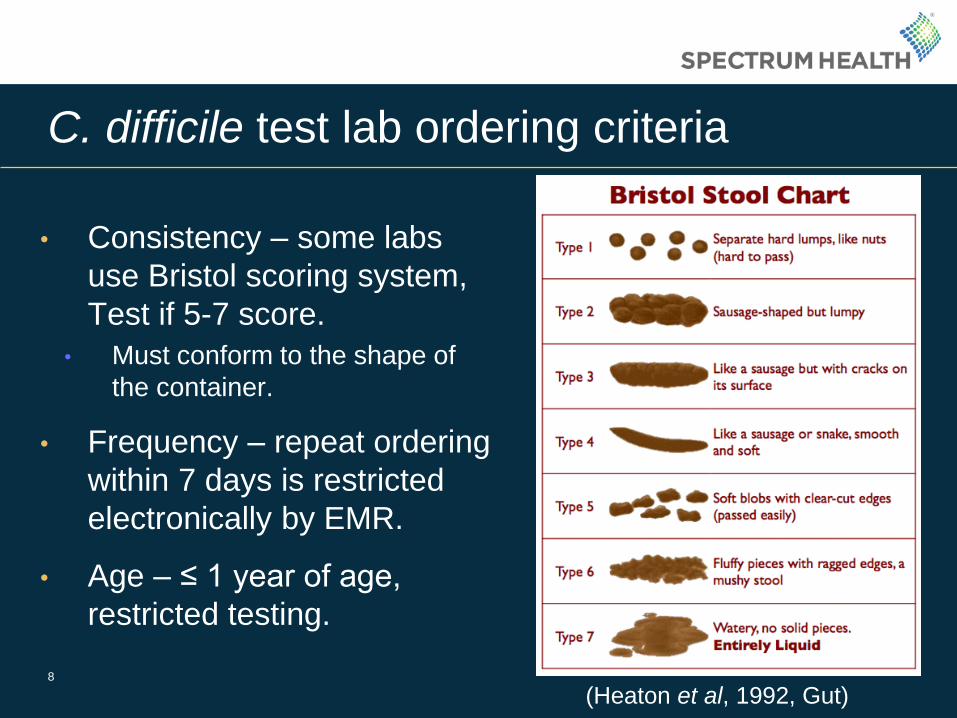
C. difficile test lab ordering criteria
8
• Consistency – some labs
use Bristol scoring system,
Test if 5-7 score.
• Must conform to the shape of
the container.
• Frequency – repeat ordering
within 7 days is restricted
electronically by EMR.
• Age – ≤ 1 year of age,
restricted testing.
(Heaton et al, 1992, Gut)

A role for stewardship teams – reduce fluoroquinolone usage
9
Clindamycin, cephalosporins, and fluoroquinolones are associated
with the highest risk of CDI (Dingle et al, 2017, Lancet Infect Dis).
• The incidence of C. difficile incidence in England declined by 80% after 2006, following the
implementation of national control policies.
• Hypotheses for role of stewardship in CDI reduction:
• (1) If C. difficile infection declines were driven by reductions in use of particular antibiotics, then
incidence of C. difficile infections caused by resistant isolates should decline faster than that caused
by susceptible isolates across multiple genotypes.
• (2) If C. difficile infection declines were driven by improvements in hospital infection control, then
transmitted (secondary) cases should decline regardless of susceptibility.
WGS of 4,000+ isolates for fluoroquinolone resistance.

Quinolone usage – High Risk for C. difficile
10
“Restricting fluoroquinolone prescribing appears to explain the decline in
incidence of C. difficile infections, above other measures” (Dingle et al, 2017,
Lancet Infect Dis).

Healthcare-onset C. difficile rates
11
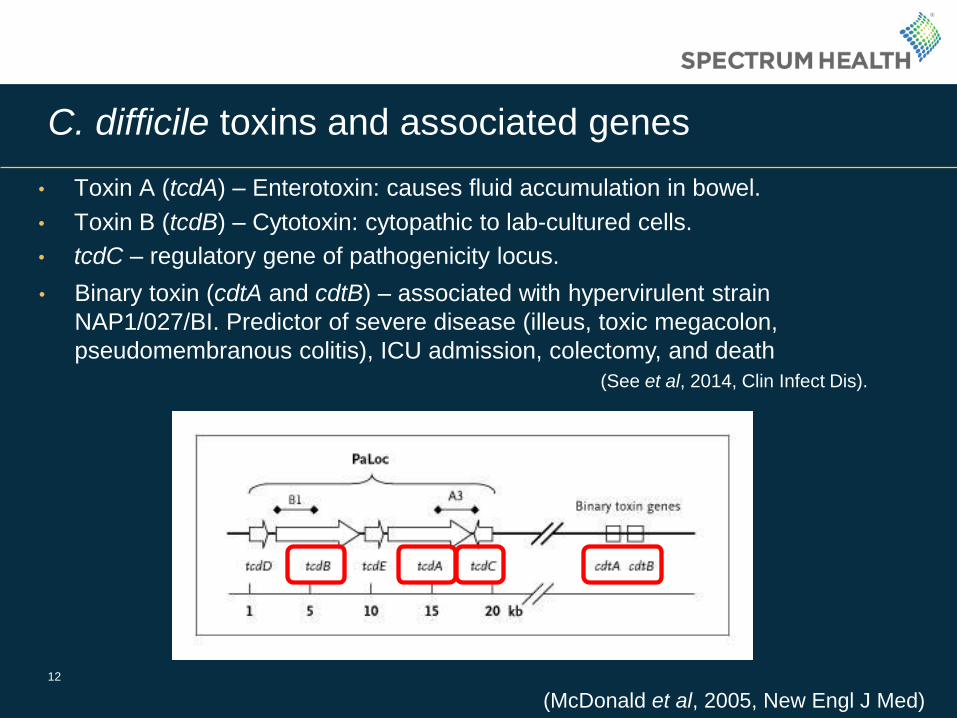
C. difficile toxins and associated genes
• Toxin A (tcdA) – Enterotoxin: causes fluid accumulation in bowel.
12
(McDonald et al, 2005, New Engl J Med)
• Toxin B (tcdB) – Cytotoxin: cytopathic to lab-cultured cells.
• tcdC – regulatory gene of pathogenicity locus.
• Binary toxin (cdtA and cdtB) – associated with hypervirulent strain
NAP1/027/BI. Predictor of severe disease (illeus, toxic megacolon,
pseudomembranous colitis), ICU admission, colectomy, and death
(See et al, 2014, Clin Infect Dis).
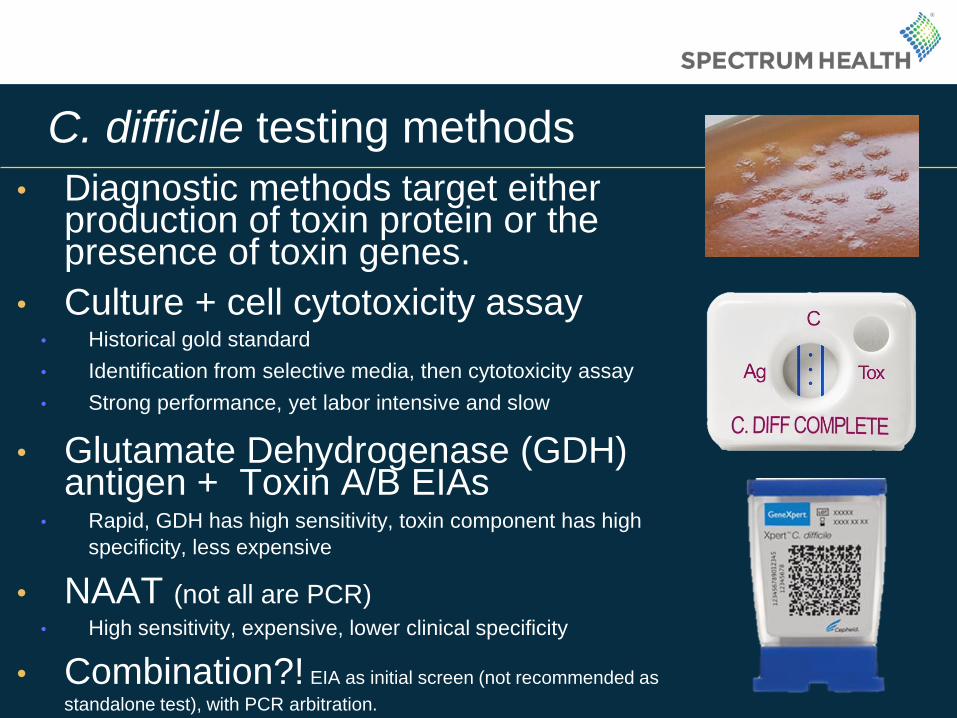
C. difficile testing methods
• Diagnostic methods target either production of toxin protein or the presence of toxin genes.
• Culture + cell cytotoxicity assay • Historical gold standard
• Identification from selective media, then cytotoxicity assay
• Strong performance, yet labor intensive and slow
• Glutamate Dehydrogenase (GDH) antigen + Toxin A/B EIAs
• Rapid, GDH has high sensitivity, toxin component has high
specificity, less expensive
• NAAT (not all are PCR)
• High sensitivity, expensive, lower clinical specificity
• Combination?! EIA as initial screen (not recommended as
standalone test), with PCR arbitration.
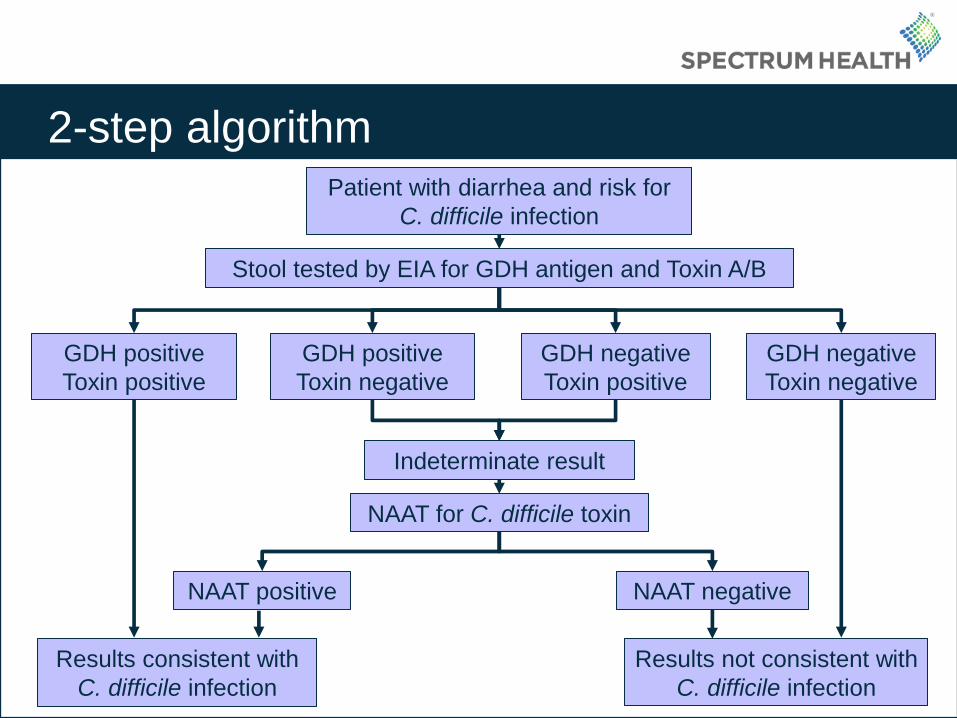
2-step algorithm
14
Patient with diarrhea and risk for
C. difficile infection
Stool tested by EIA for GDH antigen and Toxin A/B
GDH positive
Toxin negative
GDH negative
Toxin positive
Indeterminate result
NAAT for C. difficile toxin
GDH positive
Toxin positive
Results consistent with
C. difficile infection
GDH negative
Toxin negative
Results not consistent with
C. difficile infection
NAAT positive NAAT negative

Mayo Clinic study
• 268 beds, 6000 staff
• 500 prospective stool
specimens submitted
for C. difficile testing
• GDH/toxin EIA
• NAAT (x4)
• EIANAAT
15
Phoenix, AZ
Methods
• Specimens tested by methods individually and as part of
2-step algorithm
• Tested 4 different NAAT methods; all detect one or
multiple toxin-associated genes.
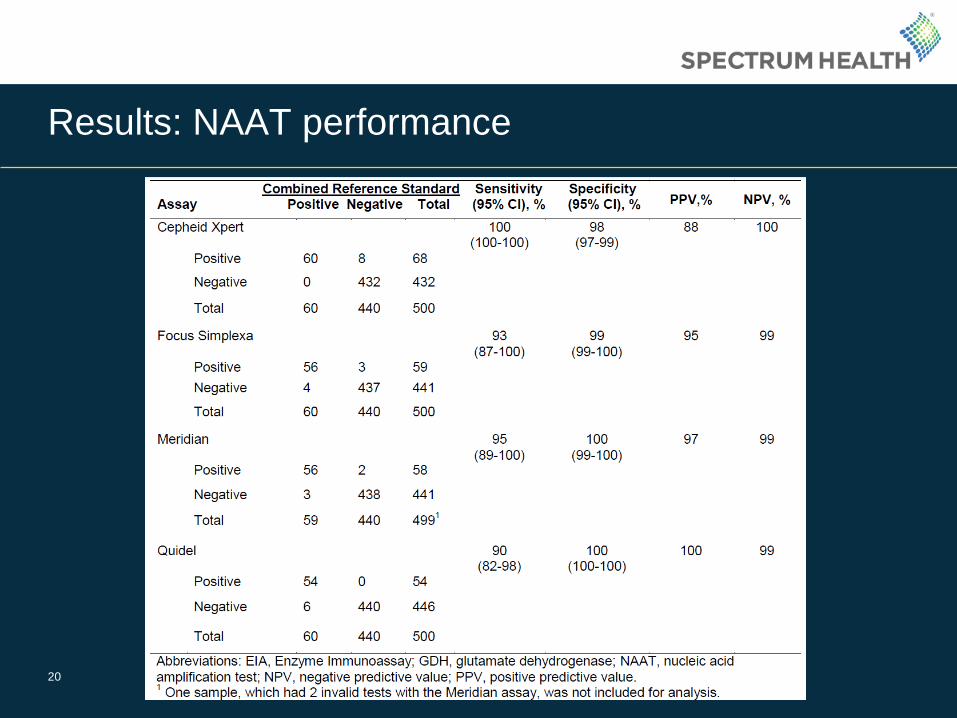
• Combined Reference Standard: for comparison, a
specimen was considered positive if all 4 molecular tests
were positive, and negative if all 4 negative. • If a discrepancy (only 1-3 molecular tests positive), toxigenic
culture was performed as definitive gold standard method.
• 18/500 = 3.6% discrepancy rate. 7/18 = 39% positive by toxigenic
culture.
16

Molecular platforms used for testing
Cepheid Xpert (PCR) tcdB, the binary toxin gene
(CDT), and tcdCΔ117
Focus Simplexa (PCR) tcdB
Meridian illumigene (LAMP) tcdA
Quidel AmpliVue (HDA) tcdA
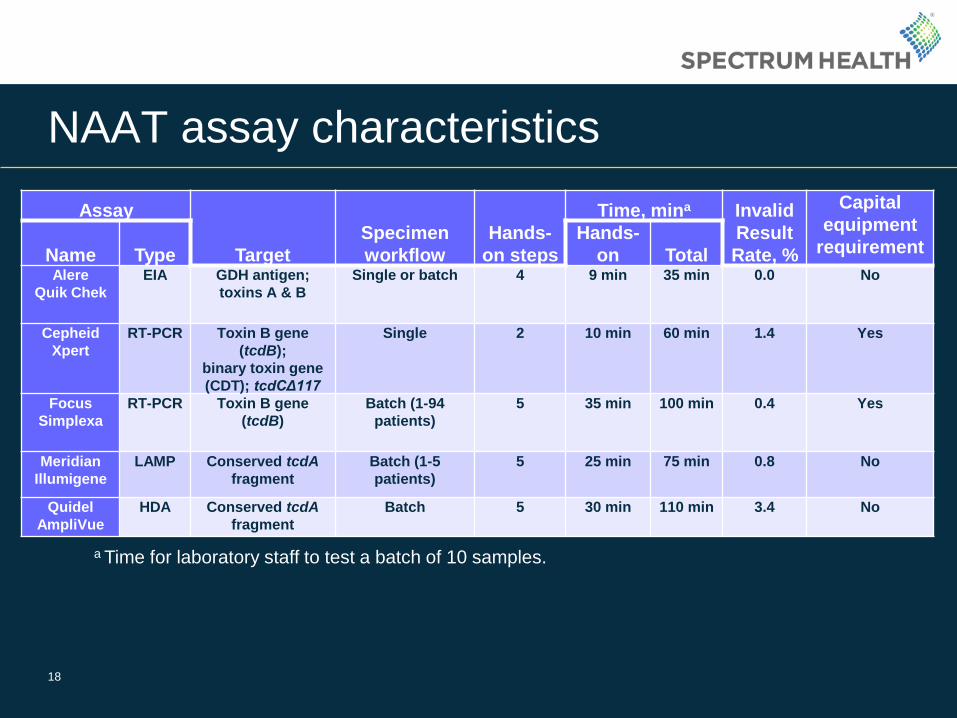
NAAT assay characteristics
Assay
Target
Specimen
workflow
Hands-
on steps
Time, mina Invalid
Result
Rate, %
Capital
equipment
requirement Name Type
Hands-
on Total Alere
Quik Chek
EIA GDH antigen;
toxins A & B
Single or batch 4 9 min 35 min 0.0 No
Cepheid
Xpert
RT-PCR Toxin B gene
(tcdB);
binary toxin gene
(CDT); tcdCΔ117
Single 2 10 min 60 min 1.4 Yes
Focus
Simplexa
RT-PCR Toxin B gene
(tcdB)
Batch (1-94
patients)
5 35 min 100 min 0.4 Yes
Meridian
Illumigene
LAMP Conserved tcdA
fragment
Batch (1-5
patients)
5 25 min 75 min 0.8 No
Quidel
AmpliVue
HDA Conserved tcdA
fragment
Batch 5 30 min 110 min 3.4 No
18
a Time for laboratory staff to test a batch of 10 samples.
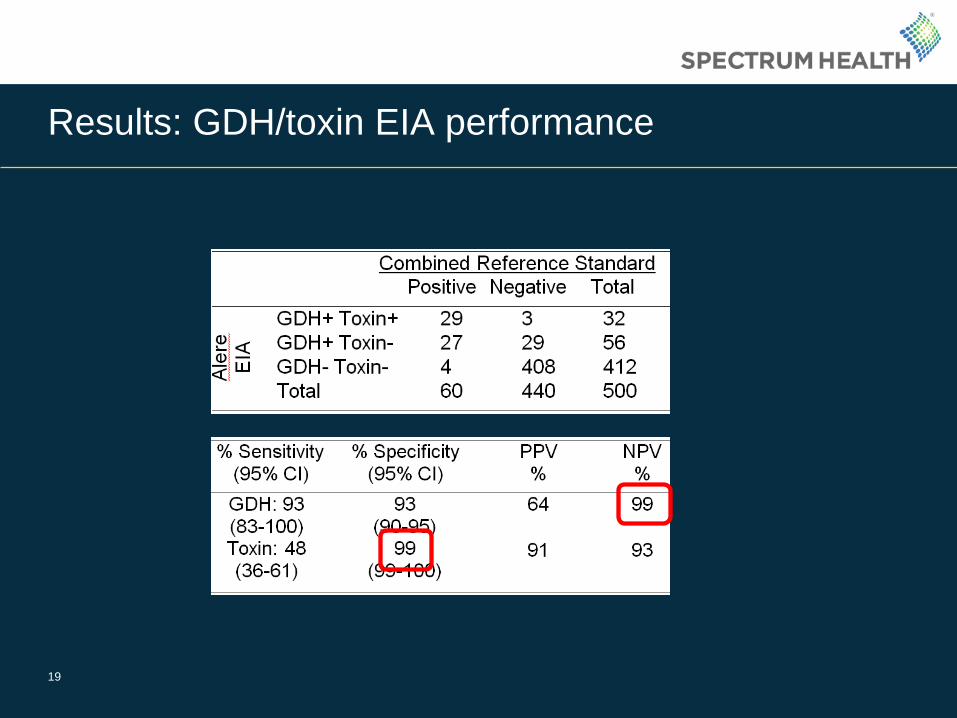
Results: GDH/toxin EIA performance
19
20
Results: NAAT performance

Results: performance of 2-step algorithm
• 88.8% of specimens
covered by EIA
21

Spectrum Health data
Cepheid PCR
Positive Negative Total
Ale
re E
IA
GDH+ Toxin+ 11 2 13
GDH+ Toxin- 12 6 18
GDH- Toxin- 3 91 94 Total 26 99 125
22
• Limitations:
• Smaller sample set (125)
• Not comparing to toxigenic culture as gold standard method.
Sensitivity Specificity PPV NPV
GDH 88.5% 91.9% 74.2% 96.8%
Toxin 42.3% 98.0% 84.6% 86.6%
What do positive/negative results really mean?
• Outcomes of 6500+ patients with diarrheal disease. (Planche et al., 2013, Lancet Infect Dis)
• Group 1: Toxin EIA (+), PCR (+)
• Group 2: Toxin EIA (-), PCR (+)
• Group 3: Toxin EIA (-), PCR (-)
• European Society of Clinical Microbiology and Infectious Disease
(ESCMID) guidelines recommend that NAAT methods are not to be used
as stand-alone tests, but rather as part of an algorithm including toxin EIA
testing. (Crobach et al., Clin Microbiol Infect, 2016)
• Due to low sensitivity of toxin EIA, it may miss some patients with CDI, so 2
step algorithm is a compromise using NAAT to detect toxin gene in patients
with high enough bacterial burden to be GDH positive.
23
More severe disease, longer duration of
diarrhea, more infection-related complications,
increased mortality.
No statistical difference
Impact of 2-step algorithm
• Clinical: • Avoid overdiagnosis/overtreatment of C. difficile carriers or at least
those with less severe disease.
• Financial: • Cheaper for lab, cheaper for patients
• With 90% of patients covered by the cheaper assay and only 10%
of patients requiring both tests, the average test charge per patient
would drop from $119 to $45. (SHGR does ~5,000 tests/yr)
• Reduced CMS penalty?
• Lab workflow • Slightly more complicated, batched testing required
24
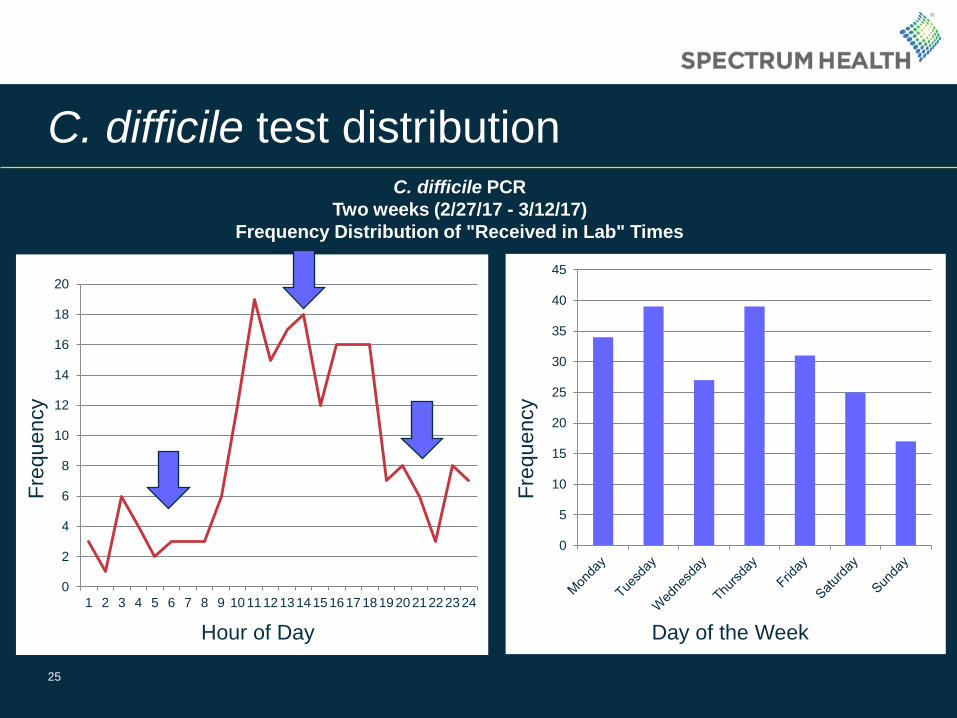
C. difficile test distribution
25
0
5
10
15
20
25
30
35
40
45
Day of the Week
Fre
quency
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4 5 6 7 8 9 101112131415161718192021222324
Fre
quency
Hour of Day
C. difficile PCR
Two weeks (2/27/17 - 3/12/17)
Frequency Distribution of "Received in Lab" Times
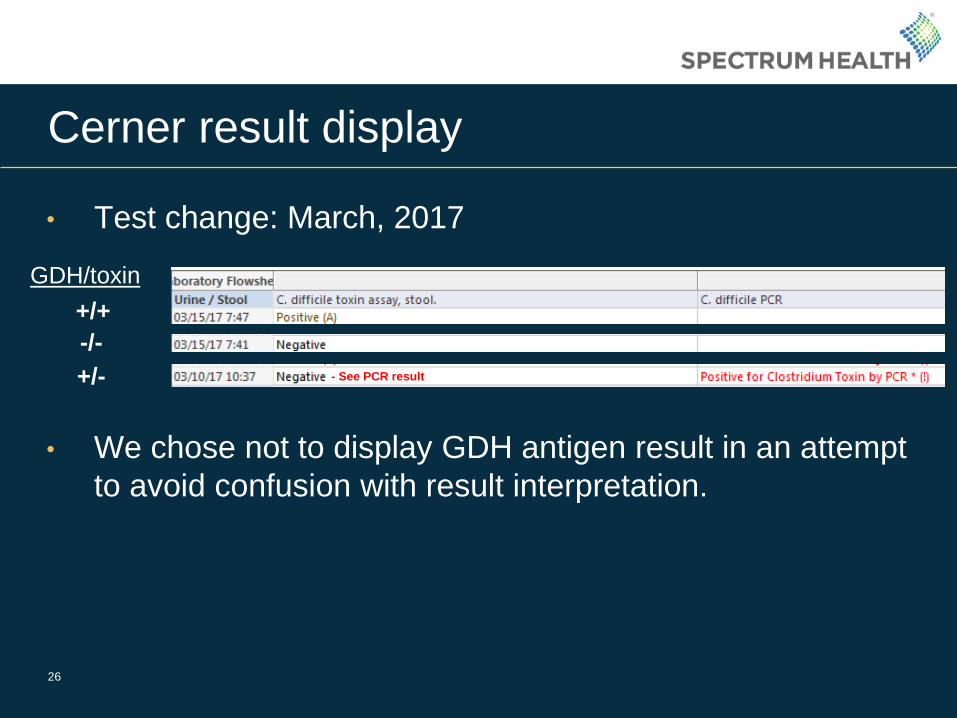
Cerner result display
• Test change: March, 2017
• We chose not to display GDH antigen result in an attempt
to avoid confusion with result interpretation.
26
GDH/toxin
+/+
-/-
+/- - See PCR result
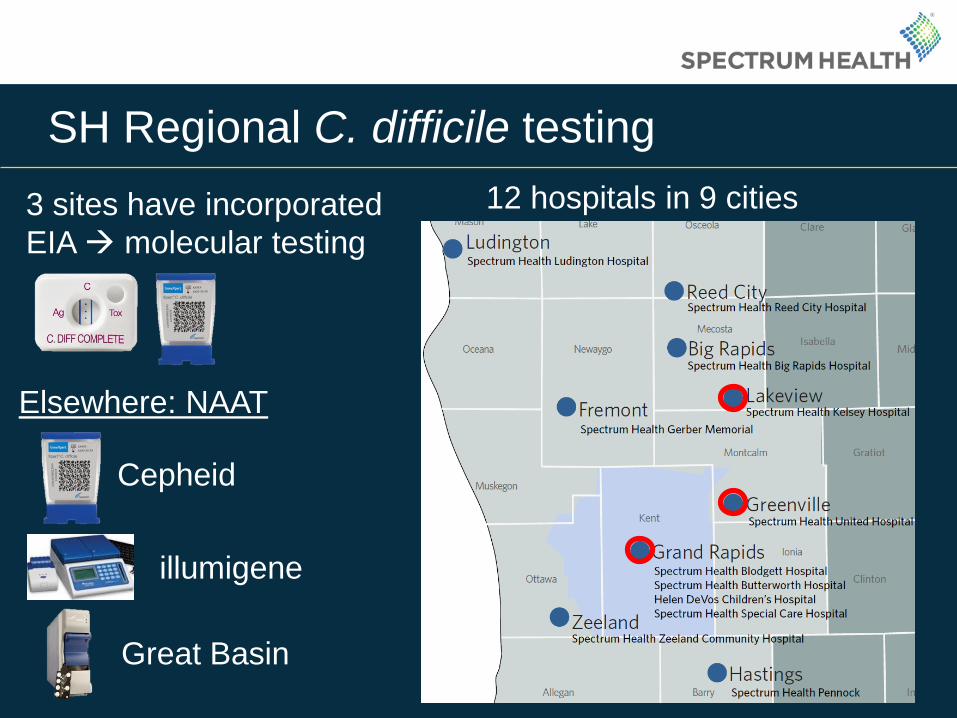
SH Regional C. difficile testing
27
Elsewhere: NAAT
Cepheid
illumigene
Great Basin
3 sites have incorporated
EIA molecular testing
12 hospitals in 9 cities
Conclusions
• CDI is a clinical diagnosis, aided by lab results.
• “Treat the patient, not the test.”
• Pre-analytical patient selection is more important than test method.
• Study: GDH performed well as a screening target (high NPV) and the
high specificity of toxin EIA obviates need for molecular confirmatory
testing. However, labs must maintain NAAT assay for specimens
with discrepant EIA results.
• Algorithm adds complexity, reduces overall cost.
• The decision to use either standalone NAAT or 2-step algorithm must
be made at the institutional level. Both approaches have pros/cons
and are supported by current guidelines.
28