
Closed chest permanent atrioventricular block in dogs
10
Closed chest permanent atrioventricular block in dogs Ten mongrel dogs underwent transcutaneous His bundle ablation by means of pulsed synchronized electrical shocks delivered between an electrode catheter adjacent to the His bundle and a metal plate behind the dog’s back. Detailed histologic studies were performed 3 months after induction of stable complete atrioventricular (AV) block in nine dogs. The ventricular response ranged from 35 to 51 beats/min (bpm). Graded increases in overdrive ventricular pacing resulted in graded increases in pacemaker suppression up to a paced cycle length of 450 msec. All dogs showed extensive damage to the approaches to the AV node, the AV node, and the penetrating portion of the common bundle. This technique resulted in complete AV block with typical features of an infranodal pacemaker and correlated with the histologic findings of severe damage to the AV junction. The minimal myocardial damage suggests that this technique may be applicable for control of drug refractory supraventricular arrhythmias in humans. (AM HEART J 105461, 1963.) Roland0 Gonzalez, M.D., Melvin Scheinman, M.D., Saroji Bharati, M.D., and Maurice Lev, M.D. San Francisco, Calif., and Chicago, Ill. Earlier, we described’ a technique for closed chest His bundle ablation in dogs. Stable complete atrio- ventricular (AV) block was documented and was associated with minimal gross damage to the atrium and ventricle. No evidence of change to the tricuspid valve or septal perforation was noted. The purpose of the current report is to describe the electrophysi- ologic characteristics of the emerging chronic pace- maker as well as the anatomic changes in the specialized cardiac conduction system. METHODS Technique. Our technique for closed chest His bundle ablation wasdescribed in detail previously.’ The catheter used in these experiments was a standard No. 6 French quadripolar electrode catheter in which two thirds of the circumference of the distal catheter was insulated with a high-voltage plastic coating. One third of the circumfer- ence was left uninsulated to record His bundle potentials and to deliver pulsed electrical energy. Our earlier experi- ence with standard electrode catheters revealed that AV block was transient after shock. The smaller electrode surface is thought to be necessary to maximize current density and enhancelocal tissue changes. From the Department of Medicine, University of California-San Francisco; and the Congenital Heart Disease Research and Training Center, Hektoen Institute. Supported in part by Grant HL 07605-19 from the National Heart, Lung and Blood Institute, National Institutes of Health. Received for publication Nov. 9, 1981; revision received Feb. 2, 1982; accepted March 3, 1982. Reprint requests: Melvin Scheinman, M.D., Room 573, Moffitt Hospital, University of California-San Francisco, San Francisco, CA 94143. ECG II BIPOLAR UNIPOLAR 1 UNIPOLAR 2 Fig. 1. Simultaneous recordings of lead II, bipolar, and unipolar His bundle recordings. The shock was delivered via the electrode showingthe largest unipolar His bundle deflection. Ten mongrel dogs were anesthetized with intravenous pentobarbital sodium(30 mg/kg). The dogs were artificial- ly ventilated and their upper back was shaved over a 4-inch squarearea.A metal plate coveredwith conducting jelly wasplaced over the shaved area. After 12-lead ECGs 461
-
Upload
rolando-gonzalez -
Category
Documents
-
view
213 -
download
0
Transcript of Closed chest permanent atrioventricular block in dogs
Closed chest permanent atrioventricular block in dogs
Ten mongrel dogs underwent transcutaneous His bundle ablation by means of pulsed synchronized electrical shocks delivered between an electrode catheter adjacent to the His bundle and a metal plate behind the dog’s back. Detailed histologic studies were performed 3 months after induction of stable complete atrioventricular (AV) block in nine dogs. The ventricular response ranged from 35 to 51 beats/min (bpm). Graded increases in overdrive ventricular pacing resulted in graded increases in pacemaker suppression up to a paced cycle length of 450 msec. All dogs showed extensive damage to the approaches to the AV node, the AV node, and the penetrating portion of the common bundle. This technique resulted in complete AV block with typical features of an infranodal pacemaker and correlated with the histologic findings of severe damage to the AV junction. The minimal myocardial damage suggests that this technique may be applicable for control of drug refractory supraventricular arrhythmias in humans. (AM HEART J 105461, 1963.)
Roland0 Gonzalez, M.D., Melvin Scheinman, M.D., Saroji Bharati, M.D., and Maurice Lev, M.D. San Francisco, Calif., and Chicago, Ill.
Earlier, we described’ a technique for closed chest His bundle ablation in dogs. Stable complete atrio- ventricular (AV) block was documented and was associated with minimal gross damage to the atrium and ventricle. No evidence of change to the tricuspid valve or septal perforation was noted. The purpose of the current report is to describe the electrophysi- ologic characteristics of the emerging chronic pace- maker as well as the anatomic changes in the specialized cardiac conduction system.
METHODS
Technique. Our technique for closed chest His bundle ablation was described in detail previously.’ The catheter used in these experiments was a standard No. 6 French quadripolar electrode catheter in which two thirds of the circumference of the distal catheter was insulated with a high-voltage plastic coating. One third of the circumfer- ence was left uninsulated to record His bundle potentials and to deliver pulsed electrical energy. Our earlier experi- ence with standard electrode catheters revealed that AV block was transient after shock. The smaller electrode surface is thought to be necessary to maximize current density and enhance local tissue changes.
From the Department of Medicine, University of California-San Francisco; and the Congenital Heart Disease Research and Training Center, Hektoen Institute.
Supported in part by Grant HL 07605-19 from the National Heart, Lung and Blood Institute, National Institutes of Health.
Received for publication Nov. 9, 1981; revision received Feb. 2, 1982; accepted March 3, 1982.
Reprint requests: Melvin Scheinman, M.D., Room 573, Moffitt Hospital, University of California-San Francisco, San Francisco, CA 94143.
ECG II
BIPOLAR
UNIPOLAR 1
UNIPOLAR 2
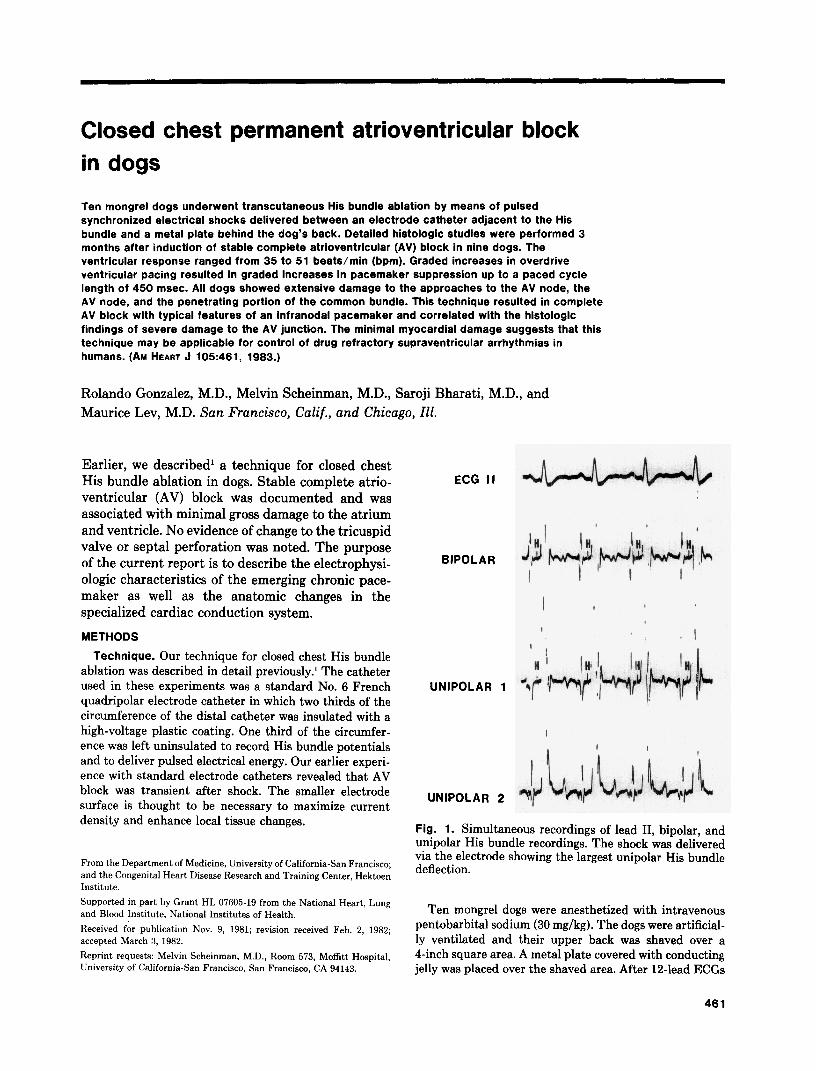
Fig. 1. Simultaneous recordings of lead II, bipolar, and unipolar His bundle recordings. The shock was delivered via the electrode showing the largest unipolar His bundle deflection.
Ten mongrel dogs were anesthetized with intravenous pentobarbital sodium (30 mg/kg). The dogs were artificial- ly ventilated and their upper back was shaved over a 4-inch square area. A metal plate covered with conducting jelly was placed over the shaved area. After 12-lead ECGs
461

462 Gonzalez et al. March, 1983
American Heart Journal
“6
Fig. 2. Twelve-lead ECG showing complete atrioventricular block and right bundle branch block pattern.
Table I. Methods of histologic study
Case no. SA node and approaches A V node and approaches,
bundle, and bundle branches No. of sections
Q 10-3 stains *“I Q 10.-g stains A”, Q 20 L
2 Q IO-3 stains AV Q IO-L2 stains “36 3 Q IO-3 stains AV, Q 10---X stains 418
AV, Q 20--~-2 stains 4 Q 10-3 stains AV, Q lo-- 3 stains :3 10
AV, Q 20.--2 stains 5 Q 10-3 stains AV, Q 10-Z stains 396
AV, Q 20---2 stains 6 Q 10-3 stains AV, Q 10--:X stains 342
AV, Q 26 2 st,ains 7 Q 10-3 stains AV, Q 10--t? stains 374
AV, Q 20-- 2 stains 8 Q 10-3 stains AV, Q lo--3 stains 354
AV, Q 20--Z stains 9 Q 10-3 stains AV, Q 10P~-Z stains ,370
AV, Q 20--2 stains __--- ---.-- -
Abbreviations: AV = atrioventricular; AV,.AV, = implies the atrioventricular nodal, bundle, and bundle branches were taken in two blocks; Q = every tenth section was studied; SA = sinoatrial; 2 stains = the two stains used were hematoxylin-eosin and Weigert-van Gieson; 3 stains = the three stains used were
hematoxylin-e&n, Weigert-van Gieson, and Gomori trichrome.
were obtained, the modified quadripolar electrode cathe- ter was inserted into one of the femoral veins and posi- tioned across the tricuspid valve for His bundle (HB) recording and delivery of pulsed electric energy. To select the electrode of the catheter from which the energy was delivered, both bipolar and unipolar HB recordings were
obtained (Fig. 1). The electrode that generated the largest unipolar HB potential was identified, and a single direct current pulse synchronized to the QRS was delivered between this electrode (cathode) and the metal plate positioned behind the back of the dog (anode)
Follow-up studies. One dog developed ventricular

Volume 105
Number 3 Closed chest permanent AV block in dogs 463
25 mm/s
Fig. 3. Twelve-lead ECG showing complete atrioventricular block and left bundle branch block pattern.
CONTROL POST BLOCK
100 m m / m 50 mm,scc
Fig. 4. Left panel, Simultaneous control surface lead II and His bundle electrogram (HBE). After induction of complete atrioventricular block, a discrete potential (arrows) was recorded from the right septal surface below the tricuspid valve.
fibrillation after shock due to faulty synchronization and was not defibrillated. The delivered electric pulse was 4 msec in duration. The static impedance of the circuit was 3000 Q and the effective delivered energy was 35 joules. After production of complete AV block, the dogs were followed for a period of 3 months. At the end of this period, repeat surface 12-lead ECGs were obtained. Stan- dard quadripolar electrode catheters were inserted into the right femoral vein and artery and were positioned in
the right and left ventricles in all nine dogs. The right AV junctional area as well as the inflow tract of the right ventricle and aortic valve area were extensively explored to detect His bundle or bundle branch potentials. The effects of right ventricular overdrive pacing on pacemaker automaticity was evaluated by analysis of 10 cycles after abrupt cessation of pacing. The right ventricle was paced for 2 minutes beginning at a paced cycle length of 700 msec. After a rest period of 3 minutes, pacing was resumed
464 Gonzalez et al.
Maximum CL/SCL
OL
March, 1983
American Heart Journal
I 0
I l , I I 2 4 6 8 IO
Post Pacing Cycle
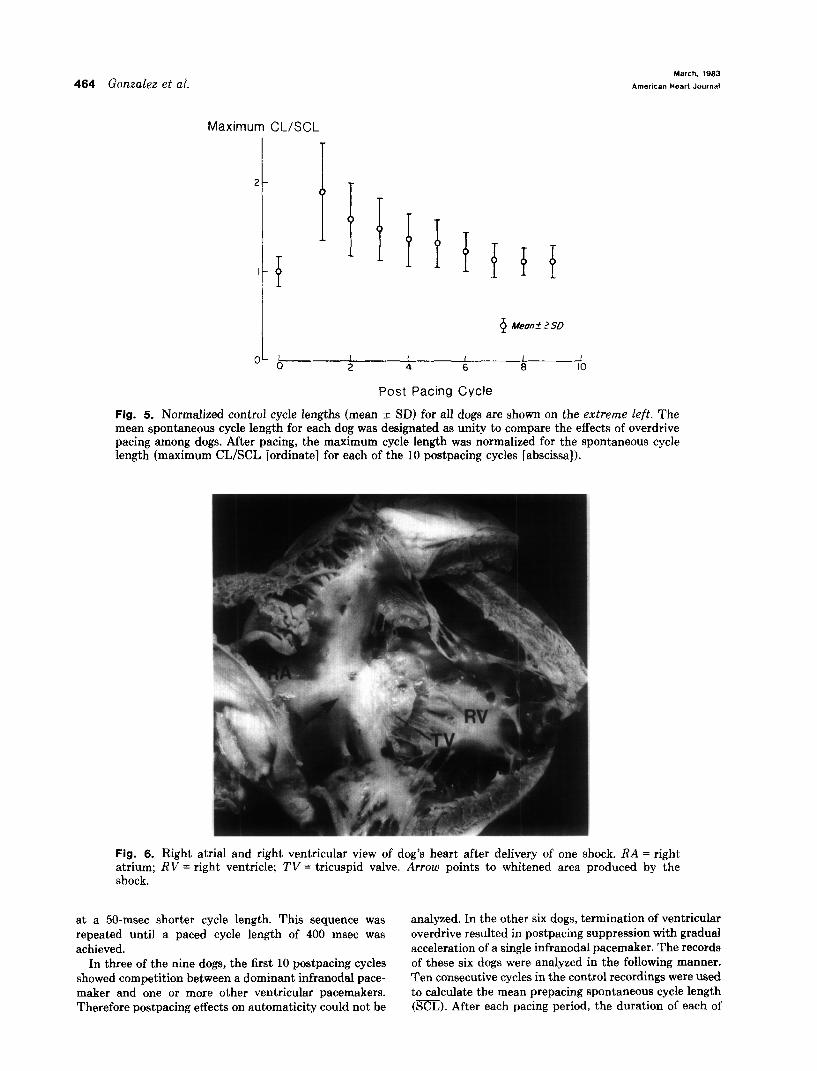
Fig. 5. Normalized control cycle lengths (mean + SD) for all dogs are shown on the extreme left. The mean spontaneous cycle length for each dog was designated as unity to compare the effects of overdrive pacing among dogs. After pacing, the maximum cycle length was normalized for the spontaneous cycle length (maximum CL/SCL [ordinate] for each of the 10 postpacing cycles [abscissa]).
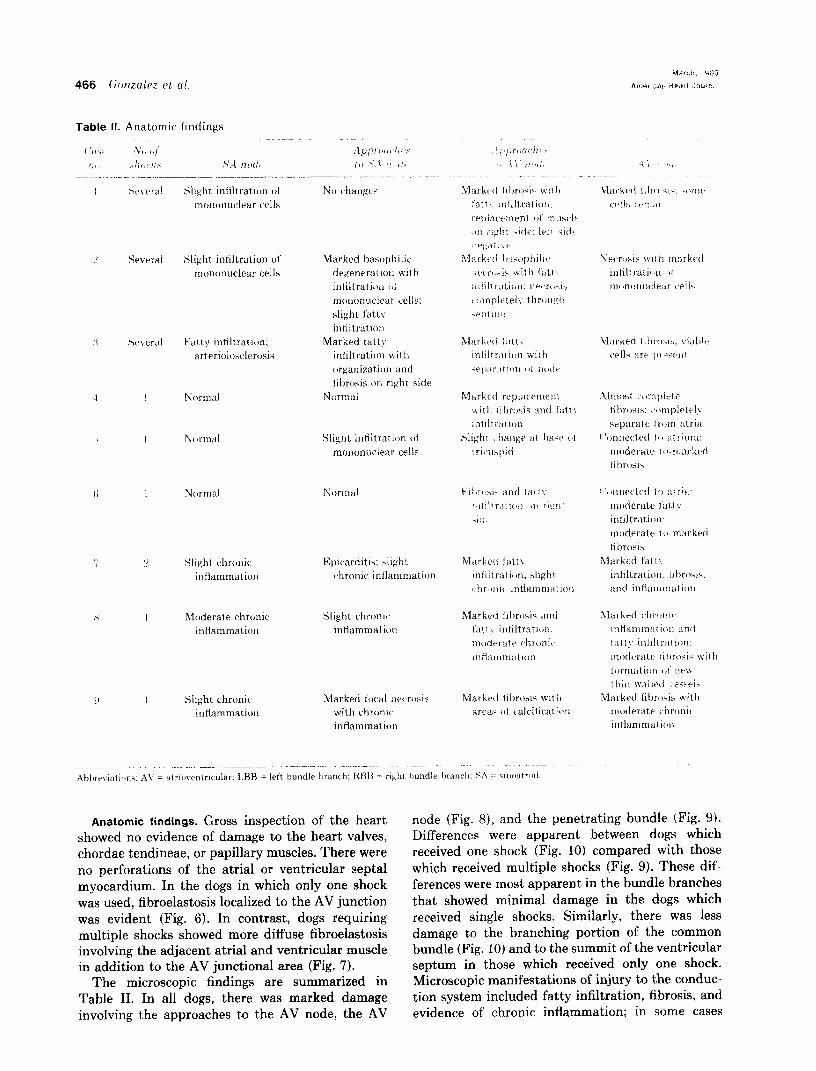
Fig. 6. Right atria1 and right ventricular view of dog’s heart after delivery of one shock. RA = right atrium; RV = right ventricle: TV = tricuspid valve. Arrow points to whitened area produced by the shock.
at a 50-msec shorter cycle length. This sequence was analyzed. In the other six dogs, termination of ventricular repeated until a paced cycle length of 400 msec was overdrive resulted in postpacing suppression with gradual achieved. acceleration of a single infranodal pacemaker. The records
In three of the nine dogs, the first 10 postpacing cycles of these six dogs were analyzed in the following manner. showed competition between a dominant infranodal pace- Ten consecutive cycles in the control recordings were used maker and one or more other ventricular pacemakers. to calculate the mean prepacing spontaneous cycle length Therefore postpacing effects on automaticity could not be (m). After each pacing period, the duration of each of

Volume 105
Number 3 Closed chest permanent AV block in dogs 465
Fig. 7. Right atria1 and right ventricular view of dog’s heart after delivery of multiple shocks. RA = right atrium: RV = right ventricle; TV = tricusnid valve. Arrows point to the whitened area produced by the multiple shocks:
the first 10 cycles was measured. The interval between the last ventricular paced cycle and the first spontaneous ventricular depolarization was defined as the first cycle, and subsequent cycles were sequentially numbered. Each cycle was normalized by dividing its duration by the SCL. The paced cycle length that resulted in the maximum normalized first cycle for each dog was identified. The next nine cycles were also normalized, and the mean ? standard deviation was calculated for each cycle in the
nine dogs. Pathologic examination (gross and microscopic). The
hearts were dissected and examined. The conduction system was studied in a manner reported previously.“,’ The tissue blocks included the approaches to the sinoatri- al (SA) node, SA node, approaches to the AV node, AV node, and in part the atrial preferential pathways and the AV bundle and the bundle branches up to the level of the moderator band. The methods of study including the staining procedures are summarized in Table I.
RESULTS
Induction of AV block and post-block heart rates. Stable complete AV block was induced immediately postshock in nine consecutive dogs. One shock was required to produce chronic complete AV block in five dogs, whereas four dogs required two to four shocks. Transient bursts of atrial or ventricular arrhythmias were usually recorded after each shock. Serial weekly ECG rhythm strips recorded over the 3-month follow-up period showed maintenance of
complete AV block with ventricular rates between 34 and 51 bpm. The slow rates were well tolerated, and none of the dogs required cardiac pacing. Three months after stable complete AV block, control mean atria1 and ventricular cycle lengths were 487 & 58 msec and 1441 -t 223 msec, respectively.
Post-block QRS patterns. The 12-lead ECG obtained at the end of the follow-up period revealed a broad QRS complex with either right (Fig. 2) or left bundle branch patterns (Fig. 3). In three dogs, at least two competing ventricular pacemakers (differ- ing rates and QRS morphology) were present. His bundle or bundle branch potentials could not be recorded from the electrode catheters used to explore the right or left AV conducting system in seven dogs, but probable right bundle branch poten- tials were recorded in two (Fig. 4). There was no correlation between specific bundle block patterns or presence or absence of recorded fascicular deflec- tions and anatomic changes.
Post-block overdrive pacing. The effects of right ventricular overdrive pacing are shown in Fig. 5. For all paced cycle lengths, maximal suppression occurred in the first postpacing cycle with gradual return to the spontaneous rate within 1 to 2 minutes. In addition, the degree of pacemaker suppression increased to a paced cycle length of 450 msec with a tendency to decrease at a paced cycle length of 400 msec.
466 (ionzale ~1, (11.
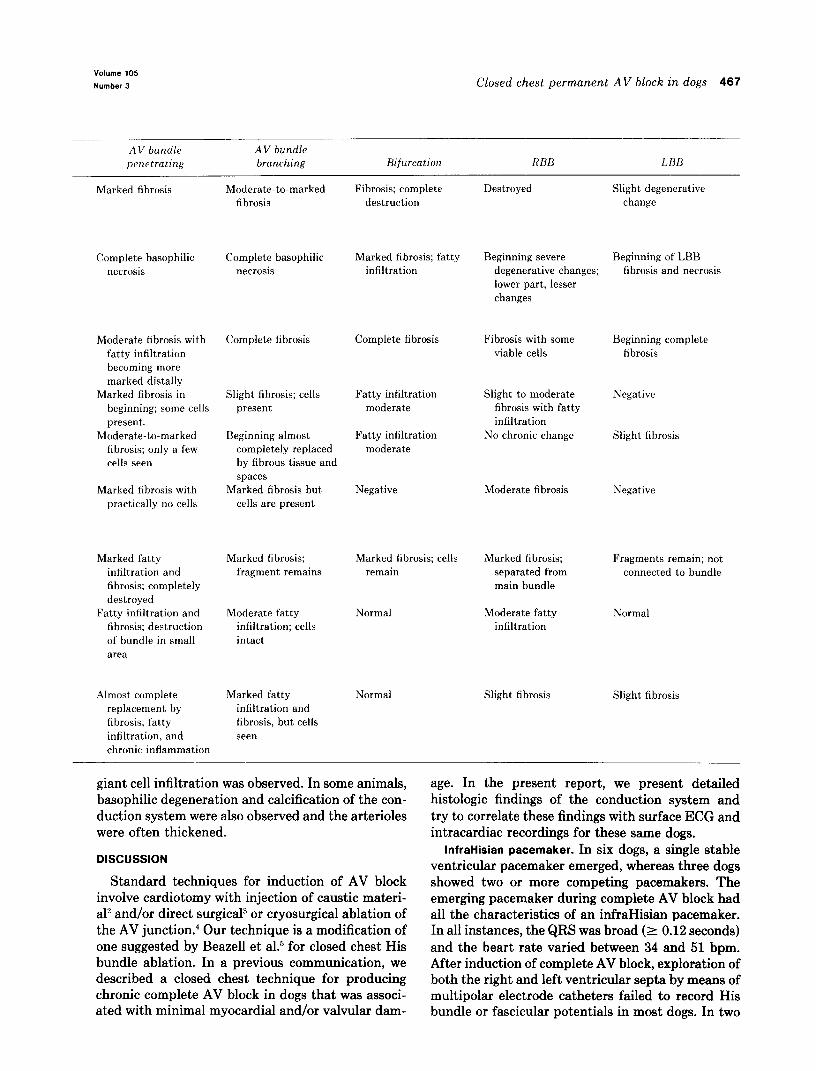
Table II. Anatomic findings
Slighl infiltration ot mononuclear cells
L! Several Slight infiltration oi’ mononuclear cells
Marked hasophilic degeneration with inliltrati<ln /I: mononuclear cells; slight f’at 1>- infiltration
Marked t’attx infiliratitrn with
organizatiorl and fibrosis on right side
Normal
Pal ty infiltration; arterioluscler~)sis
Slight intiltmti<)n (11 mononuclear cells
I Normal
I Nr,rmal Nlxmwl Ii
Rpic,arditis; sligh! chronic, intiammation
Slight chronic infiammation
Moderate chronic inflammation
Slight chrtmrc, infiamtnatirn:
Slight chronic inflammation
Marked t’ocal necrosis with chronic inflammation
node (Fig. 8), and the penetrating bundle (Fig. 9). Differences were apparent between dogs which received one shock (Fig. 10) compared with those which received multiple shocks (Fig. 9). These dif- ferences were most apparent in the bundle branches that showed minimal damage in the dogs which received single shocks. Similarly, there was less damage to the branching portion of the common bundle (Fig. 10) and to the summit of the ventricular septum in those which received only one shock. Microscopic manifestations of injury to the conduc- tion system included fatty infiltration, fibrosis, and evidence of chronic inflammation; in some cases
Anatomic findings. Gross inspection of the heart showed no evidence of damage to the heart valves, chordae tendineae, or papillary muscles. There were no perforations of the atria1 or ventricular septal myocardium. In the dogs in which only one shock was used, fibroelastosis localized to the AV junction was evident (Fig. 6). In contrast, dogs requiring multiple shocks showed more diffuse fibroelastosis involving the adjacent atria1 and ventricular muscle in addition to the AV junctional area (Fig. 7).
The microscopic findings are summarized in Table II. In all dogs, there was marked damage involving the approaches to the AV node, the AV
Volume 105
Number 3 Closed chest permanent AV block in dogs 467
AV bundle penetrating
AV bundle branching Bifurcation RBB LBB
Marked fibrosis Moderate-to-marked fibrosis
Fibrosis; complete destruction
Destroyed Slight degenerative change
Complete basophilic necrosis
Moderate fibrosis with fatty infiltration becoming more marked distally
Marked fibrosis in beginning; some cells present.
Moderate-to-marked fibrosis; only a few cells seen
Marked fibrosis with practically no cells
Marked fatty infiltration and fibrosis; completely destroyed
Fatty infiltration and fibrosis; destruction of bundle in small area
Almost complete replacement by fibrosis, fatty infiltration, and chronic inflammation
Complete basophilic necrosis
Complete fibrosis
Slight fibrosis; cells Fatty infiltration present moderate
Beginning almost completely replaced by fibrous tissue and spaces
Marked fibrosis but cells are present
Fatty infiltration moderate
Negative
Marked fibrosis; fragment remains
Moderate fatty infiltration; cells intact
Marked fibrosis; fatty infiltration
Complete fibrosis
Marked fibrosis; cells remain
Normal
Beginning severe Beginning of LBB degenerative changes; fibrosis and necrosis
lower part, lesser changes
Fibrosis with some viable cells
Beginning complete fibrosis
Slight-to-moderate fibrosis with fatty infiltration
No chronic change
Negative
Slight fibrosis
Moderate fibrosis
Marked fibrosis; separated from main bundle
Moderate fatty infiltration
Negative
Fragments remain; not connected to bundle
Normal
Marked fatty infiltration and fibrosis, but cells seen
Normal Slight fibrosis Slight fibrosis
giant cell infiltration was observed. In some animals, basophilic degeneration and calcification of the con- duction system were also observed and the arterioles were often thickened.
DISCUSSION
Standard techniques for induction of AV block involve cardiotomy with injection of caustic materi- al2 and/or direct surgical” or cryosurgical ablation of the AV junction.4 Our technique is a modification of one suggested by Beazell et a1.5 for closed chest His bundle ablation. In a previous communication, we described a closed chest technique for producing chronic complete AV block in dogs that was associ- ated with minimal myocardial and/or valvular dam-
age. In the present report, we present detailed histologic findings of the conduction system and try to correlate these findings with surface ECG and intracardiac recordings for these same dogs.
InfraHisian pacemaker. In six dogs, a single stable ventricular pacemaker emerged, whereas three dogs showed two or more competing pacemakers. The emerging pacemaker during complete AV block had all the characteristics of an infraHisian pacemaker. In all instances, the QRS was broad (L 0.12 seconds) and the heart rate varied between 34 and 51 bpm. After induction of complete AV block, exploration of both the right and left ventricular septa by means of multipolar electrode catheters failed to record His bundle or fascicular potentials in most dogs. In two

466 Gonzalez et al. March, 1983
hwrican Heart Journal
Fig. 6. Approaches to atrioventricular node and atrioventricular node after multiple shocks. (Weigert- van Gieson stain; original magnification x30.) Note replacement of the approaches by fat, and isolation of only a remnant of the atrioventricular node. AP = approaches to atrioventricular node; N = atrioventric- ular node; V = ventricular septum.
dogs, however, a potential was recorded 10 and 15 msec, respectively, before inscription of the QRS while the catheter was positioned in the right ventri- cle. The responses to overdrive right ventricular pacing and to administration of atropine and pro- pranolol’ were all compatible with an infranodal pacemaker.6
Electrophysiologic-histologic correlations. There was good correlation between the electrophysiologic and histologic findings. All dogs showed extensive damage to the approaches to the AV node, to the AV
node, and to the penetrating portion of the common bundle. One might therefore have predicted emer- gence of an infranodal pacemaker. We could not, however, find a clear-cut correlation between specif- ic bundle branch block patterns and any specific lesion in the conduction system. Two dogs with a presumed fascicular rhythm had a left bundle branch block pattern that was compatible with a pacemaker site in the right bundle branch. In addi- tion, lesions within the His bundle may have pro- duced either right or left bundle branch patterns.
“Olwlle 105
Number 3 Closed chest permanent AV block in dogs 469
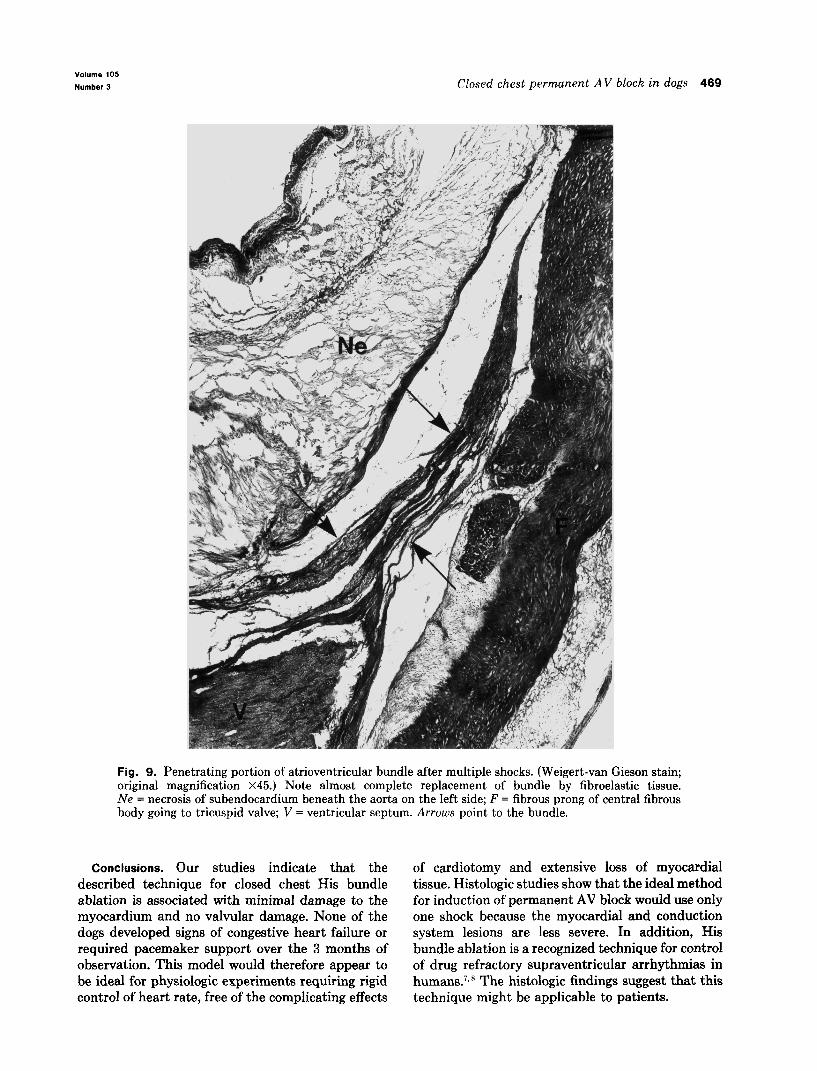
Fig. 9. Penetrating portion of atrioventricular bundle after multiple shocks. (Weigert-van Gieson stain; original magnification ~45.) Note almost complete replacement of bundle by fibroelastic tissue. Ne = necrosis of subendocardium beneath the aorta on the left side; F = fibrous prong of central fibrous body going to tricuspid valve; V = ventricular septum. Arrows point to the bundle.
Conclusions. Our studies indicate that the described technique for closed chest His bundle ablation is associated with minimal damage to the myocardium and no valvular damage. None of the dogs developed signs of congestive heart failure or required pacemaker support over the 3 months of observation. This model would therefore appear to be ideal for physiologic experiments requiring rigid control of heart rate, free of the complicating effects
of cardiotomy and extensive loss of myocardial tissue. Histologic studies show that the ideal method for induction of permanent AV block would use only one shock because the myocardial and conduction system lesions are less severe. In addition, His bundle ablation is a recognized technique for control of drug refractory supraventricular arrhythmias in humans.7x 8 The histologic findings suggest that this technique might be applicable to patients.

470 Gonzalez et al.
Fig. 10. Branching part of the atrioventricular bundle, intact after delivery of one shock. {Weigert-van Gieson stain; original magnification x45.) V = ventricular septum. .A~~~ccs point tc~ the atrioventricular bundle.
REFERENCES
1. Gonzalez R, Scheinman M, Margaretten W, Rubinstein M: Closed-chest electrode-catheter technique for His bundle ablation in dogs. Am J Physiol (Heart Circ Physiol) 241:H283, 1981.
2. Starzl TE, Gaertner RA, Baker RR: Acute complete heart block in dogs. Circulation 12:82, 1955.
3. Meakins J: Experimental heart block with atrioventricular rhythm. Heart 5:281, 1913.
4. Harrison L, Gallagher JJ, Kasell J, Anderson RH, Mikat E, Hackel DB, Wall&e AG: Cryosurgical ablation of the A-V node-His bundle. A new method for producing A-V block. .I Circulation 55:463, 1977.
5. Beazell JW, Tan KS, Fewkes JL, Furmanski M, Fisher DA:
Technique lor thta production ~JI permanent lesions m the intracardiac conduction system inbstr). Clin Res 25:141A, 1977.
6. Scherlag BJ. Lazzara R, Helfant RH: Differentiation of “A-V junctional rhythms.” Circulation 48:304, 1973.
7. Klein GJ, Scaly WC, Pritchett ELC. Harrison L, Hackel DB, Davis I). Kasell .I, Wallace AG, Gallagher JJ: Cryosurgical ahlation of’ the at rioventricular node-His bundle: Long-term follow-up and properties of the ,junctional pacemaker. Circu- lation 61:8. 1980.
8. Gonzalez R, Scheinman M, Thomas A, Desai d. Peters R, Dzindzio B: Electrophysiologic characterization of surgically induced His hundle rhythm in man. PACE 4:152. 1981.


















