Clinical Trials: Why, What, Wherefore? Guy de Bruyn Perinatal HIV Research Unit University of the...
37
Clinical Trials: Why, What, Wherefore? Guy de Bruyn Perinatal HIV Research Unit University of the Witwatersrand Chris Hani Baragwanath Hospital Johannesburg, South Africa
-
Upload
melissa-bryant -
Category
Documents
-
view
219 -
download
2
Transcript of Clinical Trials: Why, What, Wherefore? Guy de Bruyn Perinatal HIV Research Unit University of the...

Clinical Trials: Why, What, Wherefore?
Guy de Bruyn
Perinatal HIV Research UnitUniversity of the Witwatersrand
Chris Hani Baragwanath HospitalJohannesburg, South Africa
Why we need clinical trials
• Health care challenge: addressing the need for interventions providing greater efficacy and reduced toxicity– Improved benefit/risk– Broader access– Less costly
• Scientific challenge: evaluating efficacy and side effects of promising interventions in a manner that is– Timely– Efficient– Reliable
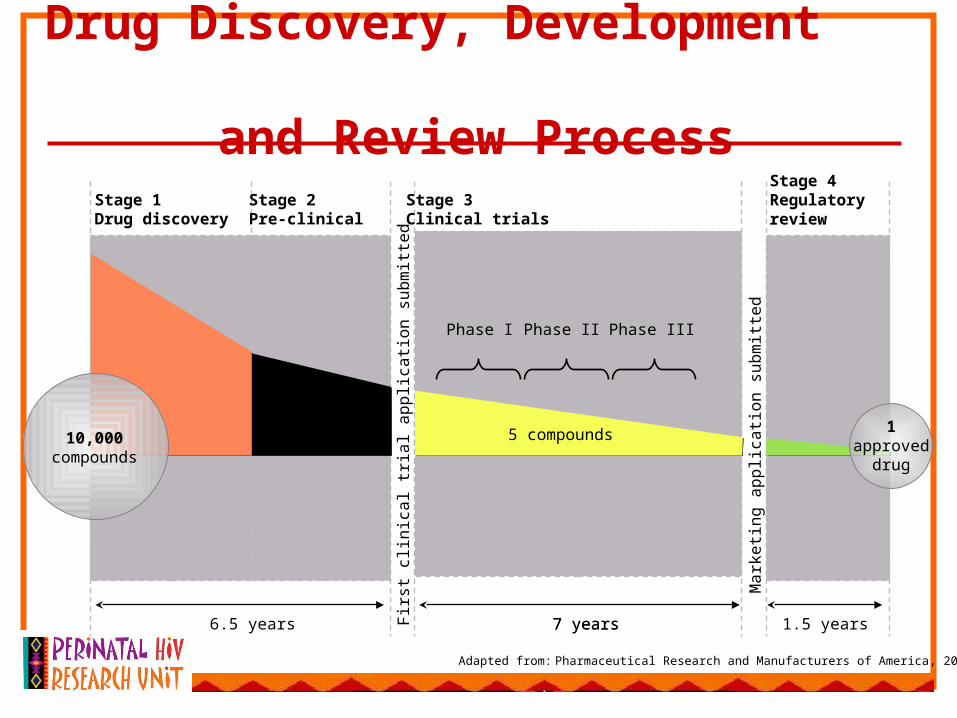
Drug Discovery, Development and Review Process
Adapted from: Pharmaceutical Research and Manufacturers of America, 2006
Phase I Phase IIIPhase II
Stage 1Drug discovery
Stage 2Pre-clinical
Stage 3Clinical trials
Stage 4Regulatory review
7 years7 years6.5 years 1.5 years
5 compounds250 compounds
1approved
drug
10,000compounds
Firs
t cl
inic
al t
rial a
pp
lica
tion
su
bm
itte
d
Ma
rke
ting
ap
plic
atio
n s
ub
mitt
ed

Types of Clinical Studies
• Four Phases of Clinical Experimentation– 0 – preclinical– 1 – Dose seeking/PK– 2 – Biologic activity– 3 – Clinical Efficacy, Safety– 4 – Post-marketing, extended evaluation

What is involved in doing a clinical trial
• Steps in Experimentation:– 1. Formulating the Problem (Designing the
Study)• Formulating specific hypotheses
– Choice of populations (eligibility criteria)– Choice of treatments– Choice of endpoints– Defining degree of precision required (sample size)
• Developing a written study protocol– Operations Manual– Scientific Design

2. Conduct of the trial
• Recruitment
• Adherence
• Retention
• Data collection and processing
• Data monitoring committees
Trial Procedures
• Recruitment• Screening / determination of eligibility• Vaccination• Safety assessments
– Reactogenicity (local and systemic)– Clinical evaluation– Laboratory measures
• HIV prevention• Immunological endpoints / Correlates• Trial endpoints

Access to care - modified from Grady
• Care which is part of the scientific design
• Care needed to safely complete the trial
• Care for injuries and adverse events
• Post trial access
• Ancillary care– Care that some participants will
predictably need

Protocol mandates
• Avoiding pregnancy during the vaccination period
• Assessing symptoms of illness
• Ensuring adequate standard of care to control participants– Counselling – pre/post-test, risk reduction,
safer sex– Providing condoms
Care needed to safely complete the trial
• Resuscitation equipment
• Laboratory monitoring of haematologic parameters and other clinical laboratory values of potential interest– Anaemia– Leukopaenia– Alteration of hepatic enzyme tests

Ancillary care – some examples
• Hypertension– May be diagnosed incidentally during the conduct
of trial procedures– Treatment is lifelong– Management is multi-modal, i.e. requires attention
to weight, nutrition, exercise, in addition to possible pharmacotherapy
• Facilitating access to services– TOP– Psychosocial support – rape/trauma/DV– Mental illness
• Dental care
What about additional HIV prevention technologies?
• Male circumcision
• STI treatment – Diagnostics– Directed versus syndromic therapy
• Post-exposure prophylaxis
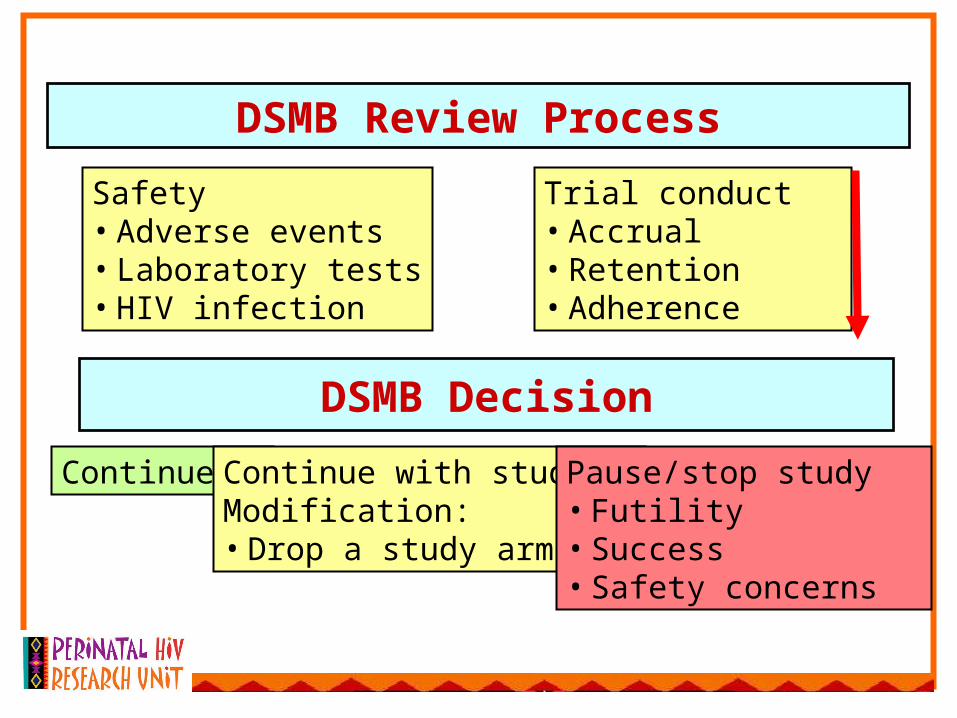
DSMB Review Process
Safety• Adverse events• Laboratory tests• HIV infection
Trial conduct• Accrual• Retention• Adherence
DSMB Decision
Continue Continue with studyModification:• Drop a study arm
Pause/stop study• Futility• Success• Safety concerns

• 3. Data Analysis– Interim/final analyses– Definitive/exploratory analyses
• 4. Reporting Results
1990
1995 2000 2005 2010
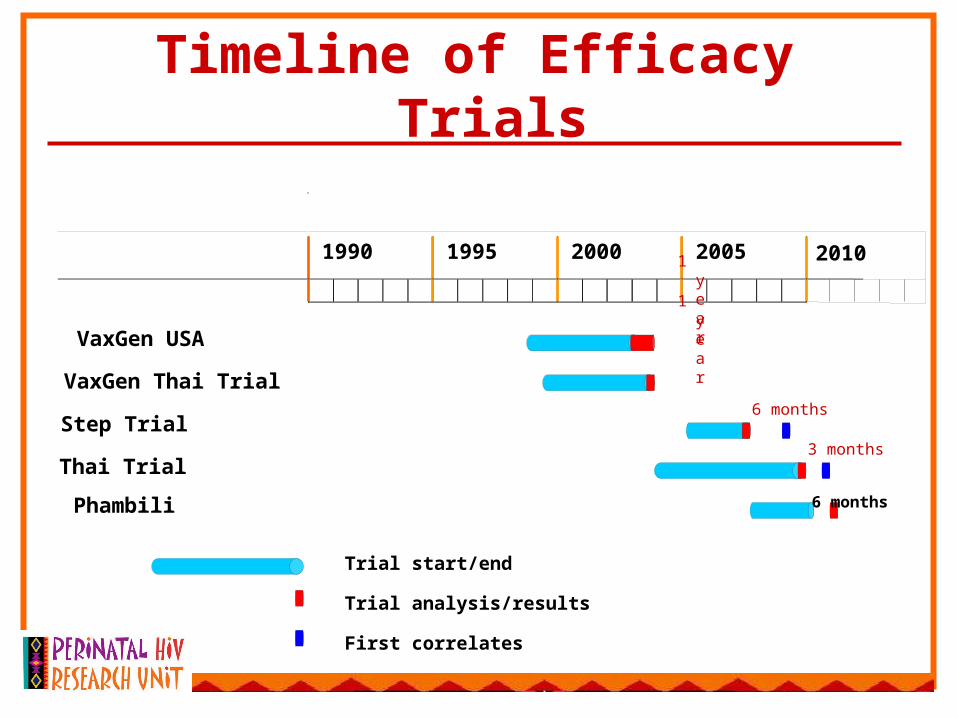
VaxGen USA
VaxGen Thai Trial
Step Trial
Thai Trial
Trial start/end
Trial analysis/results
First correlates
Timeline of Efficacy Trials
1 year
1 year
6 months
3 months
Phambili 6 months
Need for more efficient approaches
Current trial designs have numerous inefficiencies
Enhance/accelerate the vaccine development process by requiring fewer participants and a reduced time to meet study endpoints
Adaptive designs offer an alternative to the current approach
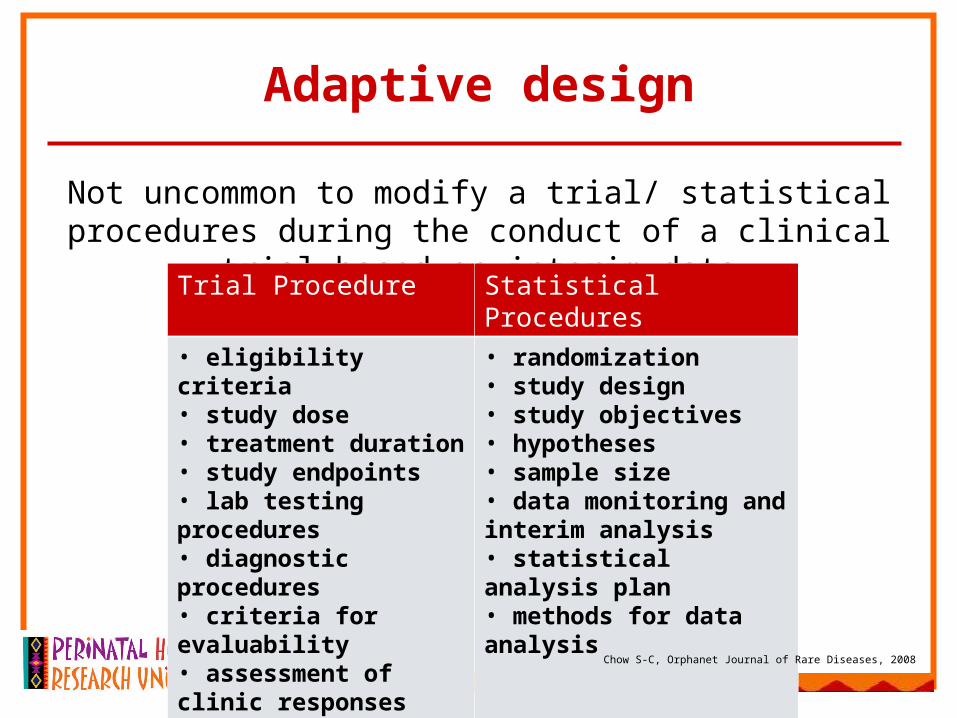
Adaptive design
Not uncommon to modify a trial/ statistical procedures during the conduct of a clinical trial based on interim data
Trial Procedure Statistical Procedures
• eligibility criteria• study dose• treatment duration• study endpoints• lab testing procedures• diagnostic procedures• criteria for evaluability• assessment of clinic responses
• randomization• study design• study objectives• hypotheses• sample size• data monitoring and interim analysis • statistical analysis plan• methods for data analysis
Chow S-C, Orphanet Journal of Rare Diseases, 2008

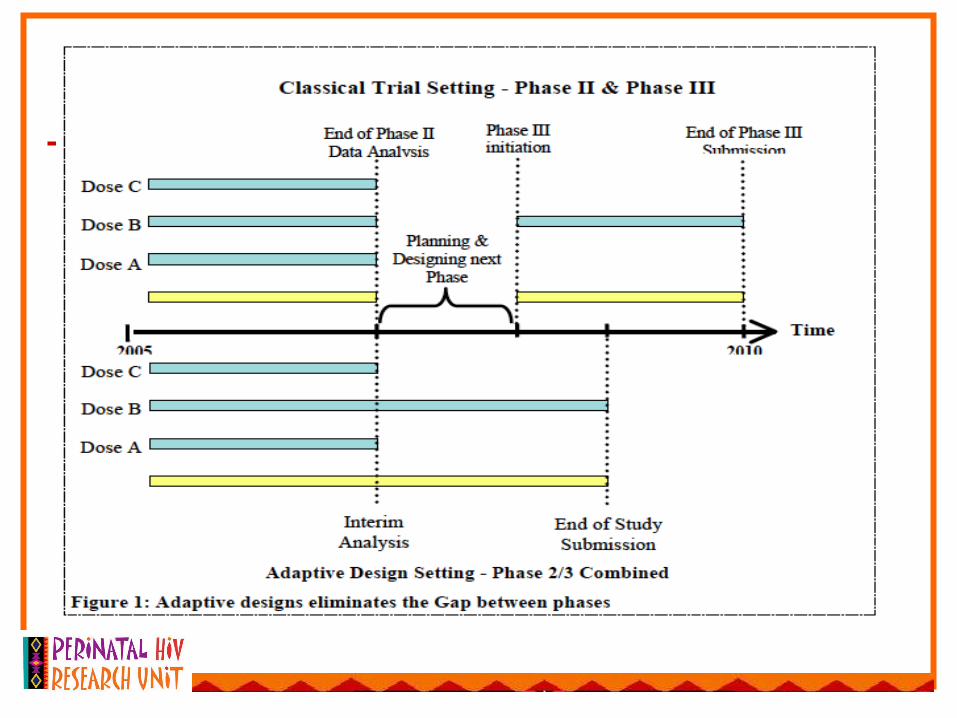
Phase II/III seamless trial design

Interpreting Results
• "It ain't so much the things we don't know that get us into trouble. It's the things we do know that just ain't so." — Artemus Ward
Interpretation of a p-value
• Which of these interpretations of p = 0.04 is correct?– (a) There is a 4% chance that the positive
result was a fluke– (b) If the trial were repeated 100 times in the
same population, under identical conditions, and in reality the vaccine is worthless, then only 4 of the trials on average would produce p-values ≤ 0.04
Main threats to achieving a reliable evaluation
• Variability: if same experiment is done several times, the results will be different each time– Variability depends on:
• How similar the participants are• How consistently treatment is administered• Sample size
– Methods to limit variability:• Eligibility criteria• Careful protocol specifications for treatment• Adequate sample size
Main threats to achieving a reliable evaluation
• Bias: tendency of a statistical estimate to deviate in one direction from a true value– Example: high risk patients may receive
more intensive intervention– Methods to control bias:
• Randomization• Adherence to interventions• Intention to treat analyses• High levels of retention / follow-up
Ethical considerations
• Principles of Research Ethics
Foundational Documents
• Nuremberg Code
• Declaration of Helsinki
• Belmont Report
• CIOMS

How Are Patients’ Rights Protected?
• Informed consent
• Scientific review
• Institutional review boards (IRBs)
• Data safety and monitoring boards

Case Studies…
• Vaxgen
• Thai
• SAPIT
• Caprisa 004
ARV-Based Microbicides
Tenofovir
UC-781
MIV
TMC120 (Dapivirine)
1% Tenofovir Vaginal Gel
• Active ingredient is tenofovir, an antiretroviral
• Has specific action against HIV and proven safety and activity as a therapeutic agent
• Provided in pre-filled applicators• Low levels of drug in the blood• Low frequency of side effects
Coital Dosing in CAPRISA 004
Participants advised to use gel which is in single-Participants advised to use gel which is in single-use, pre-filled applicators, as follows:use, pre-filled applicators, as follows:
• Coitally dependent use - 2 doses of gel per sex act
• Participants asked to apply the first dose of the assigned gel within 12 hours prior to coitus and to apply a second dose as soon as possible, within 12 hours, after coitus.
• Not more than two doses of gel in a 24-hour period.
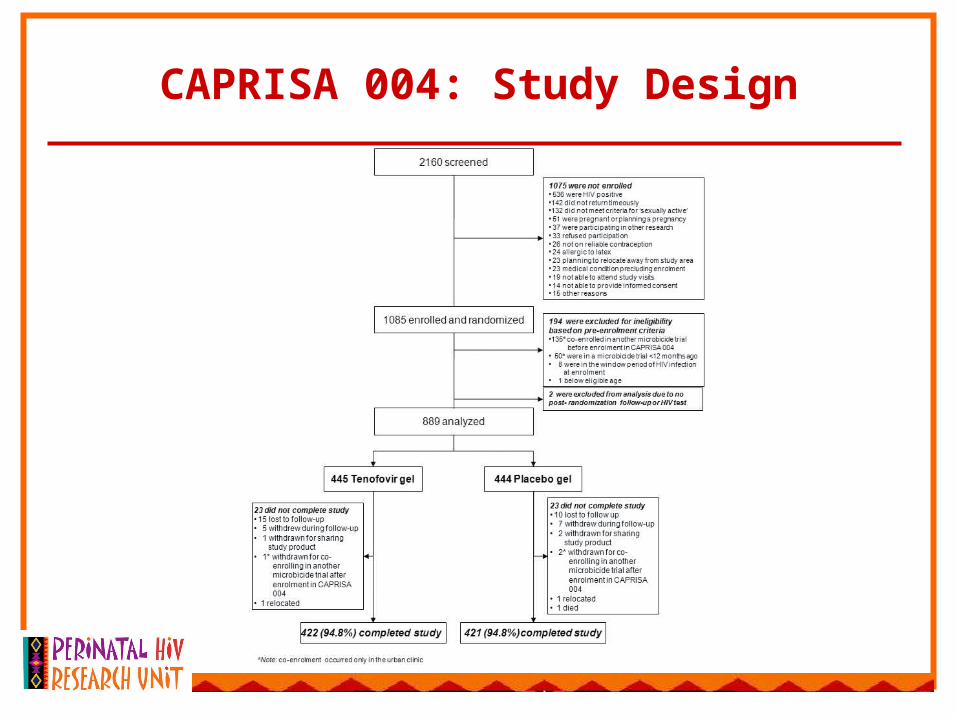
CAPRISA 004: Study Design

0.000.020.040.060.080.100.120.140.160.180.20
Pro
bab
ility
of
Infe
ctio
n
HIV Infections Over Time1
CAPRISA 004: Results
TDF prevents incident HSV infections2
• HSV infection rate: 29/202 vs. 48/224; • IRR 0.49 P=0.003
Safety• No TDF resistance• No evidence for renal or bone toxicity• Increased rate of mild diarrhea in TDF group
(17% vs. 11%)• No adverse outcomes with pregnancies
Placebo
Tenofovir
P=0.017
CVF Concentrations were Lower, and Detected Less Frequently in HIV+ Women3
109
108
107
106
103
102
101
100
104
105
TF
V C
once
ntra
tion
(ng/
mL)
Proportion withDetectable Concentrations
45% 96% 7%
4.5 (1-24) 4.5 (2-28) 6 (1-34)Time post reportedgel use (days)
1 (0-290,734) 520 (0-1,338,079) 0 (0-4,4)
HIV+ HIV- Placebo
Tenofovir Gel Placebo
Months of Follow-up
6 12 18 24 30
Effectiveness(P-value)
47%(0.069)
50%(0.007)
43%(0.004)
40%(0.013)
39%(0.017)
1. Abdool Karim Q, et al. 18th IAC; Vienna, July 18-23, 2010; Abst TUSS0502; 2. Kashuba A, et al. ibid. Abst. TUSS0503; 3. Sokal D, et al. ibid. Abst. TUSS0504.
Abdool Karim SS. N Engl J Med 2010;362:697-706.
The SAPIT trial
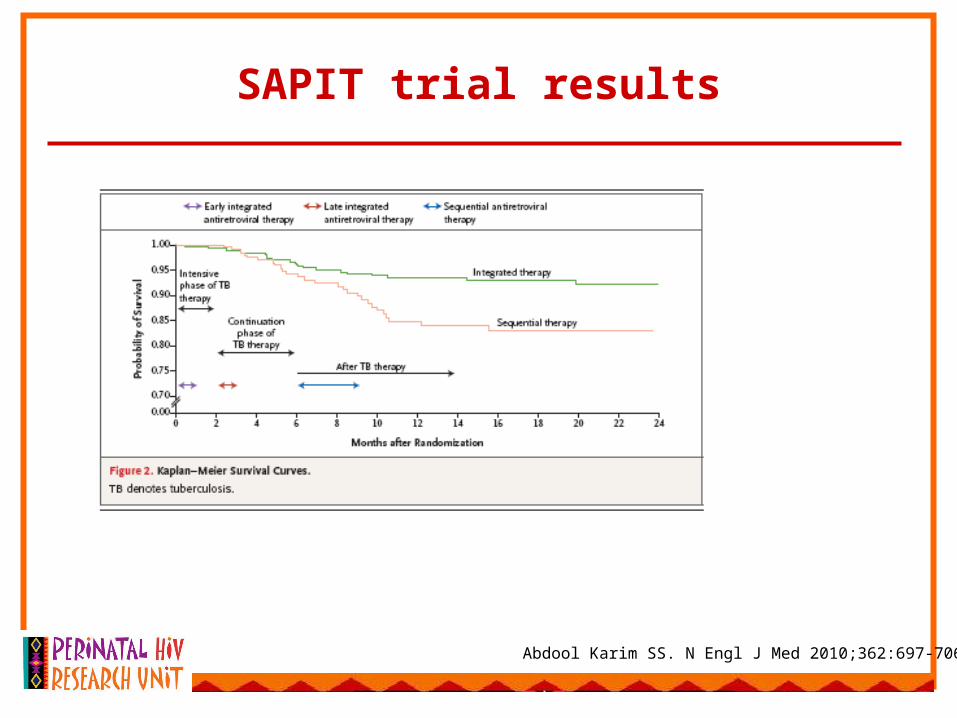
SAPIT trial results
Abdool Karim SS. N Engl J Med 2010;362:697-706.

Decisions made at the design stage met with disapproval by in-country experts
Boulle A. SAMJ 2010, Vol. 100, No. 9
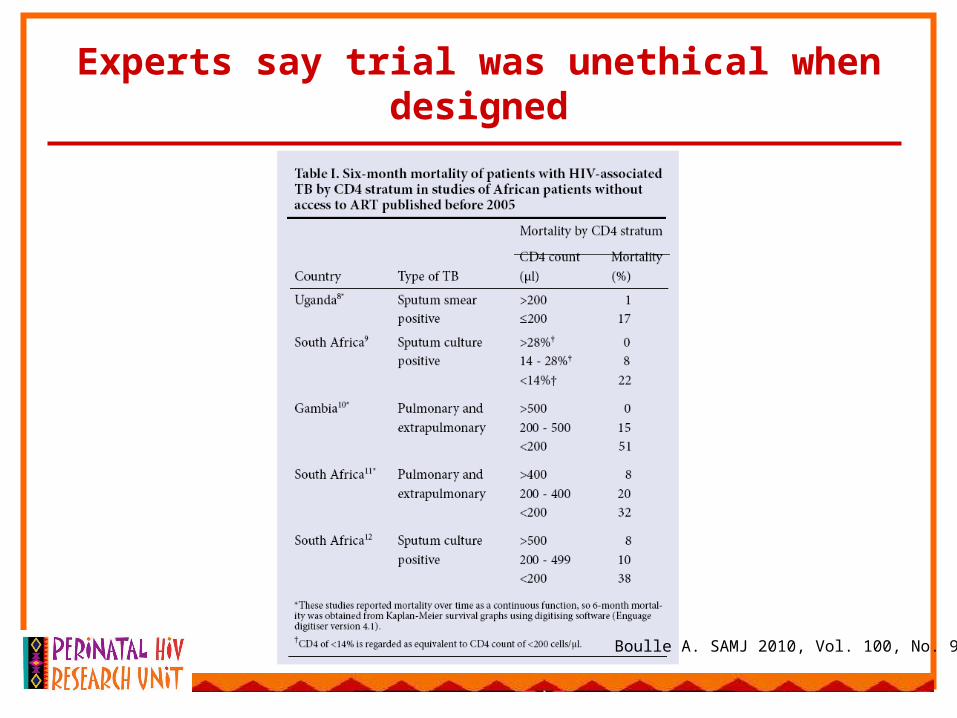
Experts say trial was unethical when designed
Boulle A. SAMJ 2010, Vol. 100, No. 9
Summary
• Why we need clinical trials
• What is involved in designing and implementing a clinical trial
• Ethical considerations
• Some examples