Clinical Study Quantitative Elastography for Cervical Stiffness...
10
Clinical Study Quantitative Elastography for Cervical Stiffness Assessment during Pregnancy A. Fruscalzo, 1,2 A. P. Londero, 3 C. Fröhlich, 1 U. Möllmann, 4 and R. Schmitz 4 1 Obstetrics and Gynecology, Mathias-Spital Rheine, Frankenburgstraße 31, 48431 Rheine, Germany 2 Obstetrics and Gynecology, St. Franziskus Hospital, Hohenzollernring 72, 48145 M¨ unster, Germany 3 Clinic of Obstetrics and Gynecology, University Hospital of Udine, University of Udine, P.le S. M. Della Misericordia 1, 35100 Udine, Italy 4 Clinic of Obstetrics and Gynecology, University of M¨ unster, Albert-Schweitzer Campus 1, 48149 M¨ unster, Germany Correspondence should be addressed to A. Fruscalzo; [email protected] Received 31 October 2013; Revised 27 December 2013; Accepted 30 December 2013; Published 5 March 2014 Academic Editor: Irma Virant-Klun Copyright © 2014 A. Fruscalzo et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Aim. Feasibility and reliability of tissue Doppler imaging-(TDI-) based elastography for cervical quantitative stiffness assessment during all three trimesters of pregnancy were evaluated. Materials and Methods. Prospective case-control study including seventy- four patients collected between the 12th and 42nd weeks of gestation. e tissue strain (TS) was measured by two independent operators as natural strain. Intra- and interoperator intraclass correlation coefficient (ICC) agreements were evaluated. Results. TS measurement was always feasible and exhibited a high performance in terms of reliability (intraoperator ICC-agreement = 0.93; interoperator ICC agreement = 0.89 and 0.93 for a single measurement and for the average of two measurements, resp.). Cervical TS showed also a significant correlation with gestational age, cervical length, and parity. Conclusions. TS measurement during pregnancy demonstrated high feasibility and reliability. Furthermore, TS significantly correlated with gestational age, cervical length, and parity. 1. Introduction e process of cervical ripening precedes the active labor by several weeks and is defined as increased soſtening, effacement, and early cervical dilatation during pregnancy. Digital cervical examination remains the standard method for evaluating cervical ripening modifications. e Bishop score is a 10-point scoring system for assessing cervical dilation, effacement, consistency, and position, as well as fetal station [1]. Nonetheless, this approach is subjective and only semi- quantitative, and its specificity in patients with low scores is unsatisfactory [2]. us, an objective estimation of these parameters, inclusive cervical stiffness assessment, could be very important for the estimation of preterm delivery risk and labor induction success. Elastography is a new imaging technique for the assess- ment of tissue stiffness by imaging the degree of tissue deformation (i.e., tissue strain, TS) [3, 4]. is tool could allow a quantitative and objective evaluation of the cervical stiffness and thus potentially replace the current subjective and semiquantitative evaluation by palpation [5]. Tissue Doppler imaging (TDI) is a Doppler-based tool for the imag- ing and estimation of tissue strain (TS) using ultrasound. TDI allows for the tracking of tissue movement, while the TDI- Q (Q-quantification) soſtware (Toshiba Medical Systems, Tokyo, Japan) facilitates an estimation of tissue stiffness based on the TS calculation [6]. Two previous preliminary studies have demonstrated the good reproducibility of the method and suggested its possible application for studying tissue elasticity during pregnancy. In these pilot studies, the standardization of the raw data acquisition techniques was addressed and demonstrated [7, 8]. Nonetheless, the feasibility and reliability of TS measurement in all three trimesters of pregnancy have not been investigated yet. e aim of our study was to evaluate the feasibility and reliability of tissue Doppler imaging- (TDI-) based elasto- graphy for cervical quantitative stiffness assessment across all three trimesters of pregnancy. Hindawi Publishing Corporation BioMed Research International Volume 2014, Article ID 826535, 9 pages http://dx.doi.org/10.1155/2014/826535
Transcript of Clinical Study Quantitative Elastography for Cervical Stiffness...

Clinical StudyQuantitative Elastography for Cervical Stiffness Assessmentduring Pregnancy
A Fruscalzo12 A P Londero3 C Froumlhlich1 U Moumlllmann4 and R Schmitz4
1 Obstetrics and Gynecology Mathias-Spital Rheine Frankenburgstraszlige 31 48431 Rheine Germany2Obstetrics and Gynecology St Franziskus Hospital Hohenzollernring 72 48145 Munster Germany3 Clinic of Obstetrics and Gynecology University Hospital of Udine University of UdinePle S M Della Misericordia 1 35100 Udine Italy
4Clinic of Obstetrics and Gynecology University of Munster Albert-Schweitzer Campus 1 48149 Munster Germany
Correspondence should be addressed to A Fruscalzo fruscalliberoit
Received 31 October 2013 Revised 27 December 2013 Accepted 30 December 2013 Published 5 March 2014
Academic Editor Irma Virant-Klun
Copyright copy 2014 A Fruscalzo et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Aim Feasibility and reliability of tissue Doppler imaging-(TDI-) based elastography for cervical quantitative stiffness assessmentduring all three trimesters of pregnancy were evaluatedMaterials and Methods Prospective case-control study including seventy-four patients collected between the 12th and 42nd weeks of gestation The tissue strain (TS) was measured by two independentoperators as natural strain Intra- and interoperator intraclass correlation coefficient (ICC) agreements were evaluated Results TSmeasurement was always feasible and exhibited a high performance in terms of reliability (intraoperator ICC-agreement = 093interoperator ICC agreement = 089 and 093 for a single measurement and for the average of two measurements resp) CervicalTS showed also a significant correlation with gestational age cervical length and parity Conclusions TS measurement duringpregnancy demonstrated high feasibility and reliability Furthermore TS significantly correlated with gestational age cervicallength and parity
1 Introduction
The process of cervical ripening precedes the active laborby several weeks and is defined as increased softeningeffacement and early cervical dilatation during pregnancyDigital cervical examination remains the standardmethod forevaluating cervical ripening modifications The Bishop scoreis a 10-point scoring system for assessing cervical dilationeffacement consistency and position as well as fetal station[1] Nonetheless this approach is subjective and only semi-quantitative and its specificity in patients with low scoresis unsatisfactory [2] Thus an objective estimation of theseparameters inclusive cervical stiffness assessment could bevery important for the estimation of pretermdelivery risk andlabor induction success
Elastography is a new imaging technique for the assess-ment of tissue stiffness by imaging the degree of tissuedeformation (ie tissue strain TS) [3 4] This tool couldallow a quantitative and objective evaluation of the cervical
stiffness and thus potentially replace the current subjectiveand semiquantitative evaluation by palpation [5] TissueDoppler imaging (TDI) is a Doppler-based tool for the imag-ing and estimation of tissue strain (TS) using ultrasound TDIallows for the tracking of tissue movement while the TDI-Q (Q-quantification) software (Toshiba Medical SystemsTokyo Japan) facilitates an estimation of tissue stiffnessbased on the TS calculation [6] Two previous preliminarystudies have demonstrated the good reproducibility of themethod and suggested its possible application for studyingtissue elasticity during pregnancy In these pilot studiesthe standardization of the raw data acquisition techniqueswas addressed and demonstrated [7 8] Nonetheless thefeasibility and reliability of TS measurement in all threetrimesters of pregnancy have not been investigated yet
The aim of our study was to evaluate the feasibility andreliability of tissue Doppler imaging- (TDI-) based elasto-graphy for cervical quantitative stiffness assessment across allthree trimesters of pregnancy
Hindawi Publishing CorporationBioMed Research InternationalVolume 2014 Article ID 826535 9 pageshttpdxdoiorg1011552014826535
2 BioMed Research International
Rela
xatio
n
Com
pres
sion
Relaxation phase
ROI
Probe
Compression phase
A
B
C
D
(a) (b)
1
2
Probe
Probe
ROI
ROI
12
1
2
12
1 2 1 2
2
1
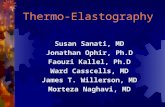
Figure 1 (a) Strainmeasurement process the sequence of drawings (A B C andD) shows one cycle of gentle compression and the subsequentrelaxation of the anterior lip of the cervix through the vaginal probe as previously described (b) The process of TS calculation is displayed(above a compression and under a relaxation phase) a circular region of interest (ROI) is placed covering the whole thickness of the anteriorcervical lip The strain is then calculated during a compression phase (above from a time of maximal relaxation 1 to a time of maximalcompression 2) as well as during a relaxation phase (under from a time of maximal compression 2 to the time of the subsequent maximalrelaxation 1) The strain values are indicated as a function of the time during the movement (yellow line on the right)
2 Materials and Methods
21 Patients and Setting The study was conducted prospec-tively It was designed according to the Declaration ofHelsinki and was approved by the local ethics boardInformed consent was obtained from all patients at thetime of enrolment The patients included 74 consecutiveunselected women ranging from the 12th to the 42nd weeksof pregnancy recruited at the University Hospital of RheineGermany The preexamination exclusion criteria includedpretermmembrane rupture or uterine contractions and a riskof preterm delivery A minimal functional cervical lengthof approximately 15mm (which conformed to the vaginalprobe dimensions) was required to provide a sufficientcervical surface for an optimal examination Indeed a cervixshorter than the vaginal probe would not permit adequatelycompressing the cervix
22 Strain Measurement The process of TS measurementwas subdivided into the following two steps the first stepconsisted of the acquisition of raw data (raw data set acqui-sition) and the second step consisted of the analysis of the
acquired raw data for the purpose of strainmeasurement (TScalculation) The process of strain measurement is describedin Figure 1
23 Raw Data Set Acquisition Elastography was performedby a total of 2 gynaecologists Each patient underwent atransvaginal real-time elastography by the first operator andtwo raw data sets were acquired (f1 and f2) Elastography wasclosely replicated by a second operator and one additionalraw data set was acquired (s1) Real-time elastography wasconducted using a 9MHz vaginal probe and an Aplio XGultrasound system (Toshiba Medical Systems Tokyo Japan)The procedure was executed as follows [7] one to two cyclesof the gentle compression-relaxation phases were exertedalong the longitudinal axis of the cervix avoiding the lateraland longitudinal dislocation of the tissues until a maxi-mal compression of its anterior portion was obtained (ieuntil no further shortening of the anteroposterior diametercould be observed and the posterior part of the cervicallip begins to be axially dislocated) In order to check thequality of themovements exerted the transducer movementscould be monitored in the real-time B-mode displayed on
BioMed Research International 3
the left panel of the screen while the real-time elastographyis contemporarily displayed on the right panel using the split-screen mode Then a five-second loop including the lastcycles of compression-relaxation was acquired and stored inthe machine as raw data The raw data were acquired usingTDI software (Toshiba Medical Systems Tokyo Japan)
24 Raw Data Set Analysis and TS Calculation The TScalculations were performed offline using TDI-Q softwareThe procedure was executed as follows the region of interest(ROI) tracking function was selected and the natural strainpreset was chosen with a derivative pitch value of 5mm Acircular ROI was placed covering the whole thickness of theanterior cervical lip during the frame of the maximal tissuerelaxation Furthermore the ROI should be placed along theaxis of the compressing vaginal probe in the middle partof the cervix The TS values were then calculated duringthe relaxation phase (from the frame of maximal compres-sion to the frame of the subsequent maximal relaxation)Strain values were measured considering the cycle with alarger compression-relaxation cervical tissue excursion Aftermanually selecting the cycle of interest with a cursor thesoftware automatically calculated the strain which occurredduring the selected movement of compression (Figure 1)The strain calculation was executed by the first operator (F)both on its own acquired raw data set (Ff1 and Ff2) forthe calculation of intraobserver variability and on the firstraw data set acquired by the second operator (Fs1) for thecalculation of interoperator reliability The TS calculationwas then performed by the second operator (S) on its ownacquired raw data set (Ss1) and on the first raw data setacquired by the first operator (Sf1) across the entire patientpopulation for the calculation of interoperator reliability
25 Statistical Analysis The data were analysed using R(version 2141) and a significance level of 119875 lt 005 wasconsidered to be significant The data are presented as themedian values and the interquartile ranges (IQR) the meanvalue and standard deviation with prevalence and absolutevalues or the reference values and 95 confidence intervalsFirst we performed an analysis for each protocol to test theintraobserver and interobserver reliability of the raw dataset acquisition and the TS calculation (per protocol) Thenwe conducted additional tests to better assess the reliabil-ity of TS measurement (other analysis) For the reliabilityanalysis of the raw data acquisition and TS calculation weused the following tests intraclass correlation coefficient(ICC) the mean of differences and the difference betweenTS valuesmean of TS values (percentage difference) Thepercentage difference is defined as the difference between twovalues divided by the average of the two values It is shown as apercentage and we used it to show the amount of differencesbetween two measurements Moreover we used the Bland-Altman plots of the average against the differences of thetwo measurements and the limits of agreement were set astwo standard deviations from the mean of the differencesWe also plotted the 95 confidence intervals of the meanof differences to assess if the no difference line was inside
Table 1 Population features
Gestational age at examination (weeks) 2908 (plusmn893)First quartile (12ndash20 weeksrsquo gestation) 257 (1974)Second quartile (21ndash29 weeksrsquo gestation) 230 (1774)Third quartile (30ndash37 weeksrsquo gestation) 257 (1974)Fourth quartile (38ndash42 weeksrsquo gestation) 257 (1974)
Gravidity 2 (1-2)Parity 1 (1-2)
Para = 0 243 (1874)Para ge 1 757 (5674)
Cervical length (mm) 369 (plusmn1017)Number of fetuses
One 973 (7274)Twins 27 (274)
Pregnancy outcomesMode of delivery
Ongoing pregnancy 41 (3074)Vaginal spontaneous delivery 38 (2874)Cesarean section 20 (1574)Operative delivery 1 (174)
Gestational age at birth (weeks) 388 (plusmn18)Birth weight (grams) 323841 (plusmn64105)Description of the studied population The values reported are mean(plusmn standard deviation) median (interquartile range) or prevalence
or outside of this range We also used the following tests forthe continuous variables one way ANOVA Kruskal-Wallistest t-test or Wilcoxon test For the categorical variables weused Chi-square or exact Fisher tests where appropriate Toassess the correlations we used locally weighted scatter-plotsmoothing least squares line linear regression and Pearsonrsquostest where appropriate Finally we used Levenersquos test for thehomogeneity of variances to assess the degree of variance ofdifferences among the average measurements
The STARD (Standards for Reporting of DiagnosticAccuracy) criteria for the accurate reporting of studies ofdiagnostic accuracy were considered [9]
3 Results
31 Population Description The mean gestational age at thetime of examination in the 74 women considered in theconfirmatory phase (including the 17 women of trial phase)was 2908 weeks (plusmn893) Of these 41 had an ongoingpregnancy at the time of the statistical analysis of the studyresults whereas 59 had already delivered all at term ofpregnancy and without pregnancy-associated complicationsThe characteristics of the study population are summarisedin Table 1
32 Reproducibility of Raw Data Set Acquisition and TSCalculation In Table 2 we show the reproducibility ofraw data acquisition and the TS calculation during thevalidation phase We note that the reproducibility of the
4 BioMed Research International
Table 2 Reliability of tissue strain measurement
ICC consistency ICC agreement MD SD DM of TSReliability of straincalculation
Intraobserver (Ff1Ff1) 097 (095098) 097 (095098) minus0005 (minus00150006) 0047 7 (5ndash8)Interobserver (Ff1Sf1) 098 (097099) 098 (097099) minus0007 (minus00170002) 0041 5 (4ndash6)Interobserver (Fs1Ss1) 099 (099100) 099 (099100) minus0001 (minus00070004) 0023 3 (3-4)Interobserver (Ff1Sf1and Fs1Ss1) 099 (098099) 099 (098099) minus0004 (minus00100001) 0033 4 (3ndash5)
Reliability of raw dataacquirement
Interobserver (Ff1Fs1) 089 (084093) 089 (082093) minus0029 (minus0050minus0007) 0092 12 (9ndash15)Interobserver (Sf1Ss1) 091 (086094) 091 (085094) minus0020 (minus00400000) 0084 10 (8ndash13)Interobserver (Ff1Fs1and Sf1Ss1) 090 (086093) 089 (085092) minus0024 (minus0038minus0009) 0089 11 (10ndash13)
Reliability of raw dataacquirement and straincalculation
Intraobserver (Ff1Ff2) 093 (089096) 093 (090096) 0002 (minus00150019) 0072 10 (8ndash13)Interobserver (Ff1Ss1) 090 (085094) 089 (082093) minus0029 (minus0050minus0008) 0088 12 (9ndash14)Interobserver(Ff1Ff2Ss1mdashaverage of 2raw data)
093 (089096) 093 (089096) 0001 (minus00160018) 0072 10 (8ndash13)
Reproducibility of tissue strain measurement including raw data acquirement and tissue strain (TS) calculation In brackets the 95 confidence interval isreportedMDmean of differences SD standard deviation ofMD DM of TS (= percentage difference) difference between TS valuesmean of TS values (meanvalue and CI95)
TS calculation was high with an ICC agreement rangingbetween 097 and 099 Even if we consider the Bland-Altman plots most of the differences were within the regionof agreement (plusmn two standard deviations) and the averagediscrepancy between measures (bias space between dottedzero line and mean of differences line) was inconsistent(Figures 2(a) 2(b) and 2(c) and Table 2) Therefore we hadobserved an intra- and interobserver reproducibility of the TScalculation as well as a high intraobserver reproducibility ofthe raw data acquisition and the TS calculation (Figure 2(d))Across all the Bland-Altman plots (Figure 2) there wereno significant trends to obtain larger or smaller differencesbetween measurements as the average increased (119875 gt 005)Moreover we tested the variability of the scatter around thebias line across the graph using Levenersquos test for homogeneityof variance and the only relevant values are shown in Figures2(f) and 2(b) (one measurement) and Figure 2(c) (meanof two raw data measurements) which showed significanceof 119875 = 0054 119875 lt 005 and 119875 = 0399 respectivelyFurthermore regarding the interobserver reproducibility ofthe raw data acquisition (Figures 2(e) 2(f) 2(b) and 2(c) andTable 2) we found the lowest ICC values (ranging between089 and 091) however these values were in the moderateto high agreement regions [10] If we look at the Bland-Altman plots we note the presence of a bias (indicated bythe white space between the dotted zero line and the meanof the differences line) in all the plots that consider theinterobserver variability of rawdata acquisition or acquisition
and TS calculation (Figures 2(e) 2(f) and 2(b)) Bland-Altman plots the distance between the black line (themean ofdifferences) and the horizontal middle dotted zero line andthis space is defined as bias (= systematic error) (see Figures2(e) and 2(f)) The presence of this bias raises the questionof whether this average discrepancy between operators (iethe bias) is of clinical importance (ie if the intra- andinteroperator variability ofmeasurements are greater than thevariability due to differences among gestational age groups)Unfortunately we lacked the data to provide such an answerbecause the clinical usage of this test in the evaluation ofcervix has not yet been assessed Regardless to evaluatethe possible clinical relevance of this average discrepancybetween the operators (ie the bias) we made some furtherconsiderations First in Figures 2(e) 2(f) and 2(b) thedotted zero line was out of the 95 confidence intervalrange of the mean of differences (gray band) while in theother plots this was not the case Moreover in Figure 2(i)considering the mean of the two raw data acquisitions andthe TS calculations of F for the comparison along with theone raw data acquisition and TS calculation of S the biaswas corrected for and Levenersquos test became nonsignificantSecond the mean cervical TS at 12ndash20 gestational weeks was035 (plusmn007) at 21ndash29 gestational weeks was 041 (plusmn015) at30ndash37 gestational weeks was 065 (plusmn012) and after 37 weekswas 073 (plusmn009 119875 lt 005) The difference between everytwo values of the above TS values in relation to the meanof every two considered values (percentage difference) had a
BioMed Research International 5
mean value of 4317 (plusmn2400) (CI95 2705ndash5929) whilethe percentage difference due to the interobserver variability(DM of TS mean and CI95) had values which rangedbetween 10 and 12 (Table 2)
33 Relevant Correlations of Cervical TSwithMain PopulationFeatures Finally we found a significant correlation of the TSwith gestational age and cervical length (Figure 3) As full-term pregnancy approached the TS values increased reflect-ing softer cervical tissue Moreover a shorter cervical lengthmore frequently correlated with a high TS (again indicatinga softer cervix) (Figure 3) Overall the pluripara womenexhibited shorter and softer cervical properties compared tothe nullipara women (119875 lt 005) Correlation between TSand cervical length and parity for each subcategory were notsignificant (except for TS in the 21st to 29th gestational age)probably due to the low number of patients considered ineach subgroup (Table 3)
4 Discussion
Developing a new imaging technique for an objective assess-ment of tissue stiffness is potentially an important topicin obstetrics This could be helpful for an objective andnoninvasive description of the physiologic modification ofthe cervical stiffness occurring during pregnancy and fora better estimation of preterm delivery risk and laborinduction success Other authors tried to address this topicTekesin et al proposed the quantitative ultrasonic tissuecharacterization (QUTC) tool a software-based automatedtissue gray-scale analysis process Nonetheless this tool isbased only on a static B-mode picture of the cervix andthe insufficient interobserver reliability limited its furtherdevelopment [11] Recently Swiatkowska-Freund and Preisdescribed a cervical elastography tool where the entity oftissue movements against the vaginal probe during pelvicarterial pulsation and breathingsmovementwere representedon a colour map Unfortunately this colour-based Doppleranalysis allows only semiquantitative evaluation of tissuemovements on a scale from 0 to 4 Furthermore clinicalrelevance of these findings has yet to be confirmed [12]Molina et al and Fruscalzo and Schmitz proposed a similarapproach to that proposed by our group demonstrating thereliability of quantitative elastography but failing to find theway to standardize the applied pressure needed for translatingthe tool to the clinical practice [13 14] Finally Hernandez-Andrade et al demonstrated how also in a manually gen-erated semiquantitative elastography cervical tissue strainwas related to the most important clinical characteristics ofa nonselected population of pregnant women (in particularparity and cervical length) They showed also how cervicaltissue strainwasmore strongly associatedwith cervical lengththan with gestational age This could be explained by the factthat cervical softening accompanied by cervical shorteningis not always even if usually directly related to the advancinggestation age [15] Similarly significant correlation betweenthe cervical length and cervical elasticitywas reported in theirpreliminary results by Fuchs et al [16]
In this study the natural strain was chosen to test fora universal setting for the TS measurement that could beapplied throughout the whole gestational period Indeed theLagrangian but not the natural strain failed to perform inthe 3rd trimester when the cervix is softer and the tissuedeformation increases [8] The strain can be calculated bothas Lagrangian and natural strain Whereas the Lagrangianstrain describes the deformation (120576) of an object with itslength 119871(119905) relative to its initial length 119871(1199050)(120576119871(119905) = [119871(119905) minus119871(1199050)]119871(1199050)) the natural strain is based on the temporalintegration of the instantaneous deformation (119889120576) of thetissue (119889120576119873(119905) = [119871(119905 + 119889119905) minus 119871(119905)]119871(119905)) [17] In practicefor Lagrangian strain we just need a start and an enddimension to calculate the strain while natural strain willbe calculated over several measurement points In generalLagrangian strain is thought to bemore accurate than naturalstrain when small deformations are measured while thenatural strain is thought to be more appropriate in the caseof heterogeneous tissues or large tissue deformations (gt10ndash15) Indeed the software is less accurate in the strain calcu-lation than Lagrangian strain when following the ROI duringlarge movements While using natural strain calculation themeasured values are less dependent on the definition of theinitial length 1198710 [6] As discussed in our previous studies[7 8] in order to standardize the raw data set acquirementprocess the compressing force was exerted until a maximalcompression of its anterior portion was obtained and thecervical lip begins to be dislocated without further compres-sion Furthermore in order to standardize the procedureof strain calculation the ROI chosen was placed on thefull thickness of the anterior cervical lip Positioning theROI on different levels of the target tissue (anterior andposterior cervical lip) introduces an important bias on thestrain measurement Indeed different portions of the cervixare subjected to different forces depending on the distancefrom the compressing probe (due to the absorption of theforce) Otherwise examining the proximal and distal part ofthe cervix will imply exerting the compression movementsnot more perpendicularly to the cervix and introducing ashear strain component that actually cannot be calculatedFurthermore the distal part of the cervix would slip awayduring the compression movements and its lack of stabilitywould compromise the principles of standardisation of theapplied force Finally a minimal cervical length was required(we proposed a value of 15mm fitting the dimension ofthe vaginal probe) because the compression force should beexerted perpendicular to the longitudinal axis of the cervixIndeed it is intuitive that a very short cervix (shorter thanthe vaginal probe) does not permit adequately compressingthe cervix by the probe [7 8]
The results obtained using the proposed setting (5mmDPduring a relaxation phase) showed excellent results A highreliability was shown when comparing two measurementsof the same raw data set both if they were calculated bythe same operator and if they were calculated by anotheroperator (indicating intra- and interobserver reliability forthe TS calculation) These findings indicate that the processof TS calculation using the TDI-Q software has been properlystandardised and appears to be stable
6 BioMed Research International
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Intraobserver variabilityFf1Ff1 (calculation)
(a)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFf1Sf1 (calculation)
(b)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFs1Ss1 (calculation)
(c)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Intraobserver variability(acquirement and calculation)Ff1-Ff2
(d)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 (acquirement)
(e)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Ss1 (acquirement and calculation)
(f)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Sf1 and Fs1Ss1
(calculation)
(g)
minus03minus02minus01
00010203
(acquirement)
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 and Sf1Ss1
(h)
minus03minus02minus01
00010203
(acquirement and calculation)
00 02 04 06 08 10
Interobserver variabilityaverage of 2 raw dataFf1-Ff2Ss1
(i)
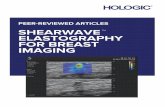
Figure 2 Reliability of tissue strain measurement Plots (a) (b) (c) (d) (e) and (f) (per protocol analysis) the Bland-Altman plotsdemonstrate the degree of concordance between the pairs of cervical TSs The region of agreement is included inside the two standarddeviations interval from the mean of differencesThe space included between the zero dotted lines and the mean of differences represents thebiasThe gray band where plotted represents the 95 confidence interval of themean of differences F and S refer to the operator undergoingthe TS calculation f and s refer to the operator undergoing the raw data acquirement where f1 and s1 and f2 and s2 refer respectively to the firstand second raw data sets (a)The intraobserver variability of the TS calculation of the same raw data (Ff1Ff1) is shown (b)The interobservervariability of the TS calculation of the same raw data by the two investigators (Ff1Sf1) is depicted (c) The interobserver variability of the TScalculation of the same raw data (Fs1Ss1) is shown (d) The intraobserver variability of the raw data acquisition and calculation (Ff1-Ff2) isshown (e) The interobserver variability of the raw data acquisition with two raw data sets acquired by different investigators (f and s) andcalculated by the same investigator is presented (Ff1Fs1) (f) The interobserver variability of the raw data acquisition and calculation by thetwo investigators is indicated (Ff1Ss1) Plots (g) (h) and (i) (other analysis) the Bland-Altman plots demonstrate the degree of concordancebetween the pairs of cervical TSs (g) The interobserver variability of the TS calculation in this plot we analyse all data from Figures 2(b)and 2(c) (ie Ff1Sf1 and Fs1Ss1) (h) The interobserver variability of the raw data acquirement the two raw data sets acquired by the twoinvestigators (F and S) aremeasured by the same investigator (Ff1Fs1 and Sf1Ss1) (i)The interobserver variability of the rawdata acquirementand calculation is shown (Ff1-Ff2Ss1 yielding an average of the 2 raw data f1 and f2) In this analysis we took into consideration the averageof the raw data measurements of investigator F versus the TS acquisition and measurement of one raw data set by investigator S
BioMed Research International 7
20 30 40Gestational age (weeks)
02
03
04
05
06
07
08
09
Cer
vica
l TS
rho 082 (CI95 073088)(P le 005)
(a)
20 30 40Gestational age (weeks)
20
30
40
50
60
Cer
vica
l len
gth
(mm
)
rho minus057 (CI95 minus071minus039)(P le 005)
(b)
20 30 40 50 600203040506070809
Cervical length (mm)
Cer
vica
l TS
rho minus059 (CI95 minus072minus042)(P le 005)
(c)
Figure 3 Tissue strain and patientsrsquo clinical features The correlation of TS (average of two raw data set measurements) with the gestationalage and cervical length (rho and 119875 value refer to Pearsonrsquos test)
Table 3 Strain values and parity
N Para = 0 (119899 = 18) N Para ge 1 (119899 = 56) PTS 18 037 (plusmn014) 56 059 (plusmn017) lt005
TS at 12ndash20 weeksrsquo gestation 8 035 (plusmn009) 11 035 (plusmn005) 0900TS at 21ndash29 weeksrsquo gestation 6 029 (plusmn005) 10 049 (plusmn014) lt005TS at 30ndash37 weeksrsquo gestation 3 058 (plusmn015) 16 066 (plusmn011) 0455TS at 38ndash42 weeksrsquo gestation 0 NA 19 073 (plusmn009) NA
Cervical length (mm) 18 4147 (plusmn992) 56 3537 (plusmn996) lt005Cervical length at 12ndash20 weeksrsquo gestation 8 4312 (plusmn1051) 11 4455 (plusmn726) 0748Cervical length at 21ndash29 weeksrsquo gestation 6 4267 (plusmn535) 10 398 (plusmn573) 0334Cervical length at 30ndash37 weeksrsquo gestation 3 3467 (plusmn1563) 16 3293 (plusmn919) 0868Cervical length at 38ndash42 weeksrsquo gestation 0 NA 19 2933 (plusmn902) NA
Tissue strain values related to parity and cervical length Mean (plusmn standard deviation)
Furthermore a high reliability was shown for the TSmea-surements when comparing the three different raw data sets(indicating intra- and interobserver reliability for the wholeprocess of TS measurement) The interobserver reliabilitywas less consistent due to the biases in raw data acquisitionbetween the two operators This difference could be over-come for example by repeating the measurement twice andcalculating the mean TS so that the eventual bias between
operators A and B will disappear These results confirm theimpression that the critical aspect of the TS measurementthat accounts for measurement reliability depends upon theprocess of raw data acquisition
Finally our results were correlated with the clinicalfeatures of the study population Specifically the cervicalTS seems to be related both to patientrsquos gestational ageand to her cervical length and parity Therefore unless the
8 BioMed Research International
relatively small number of patients used here does not allowfor generalisations these results indicate the potential clinicalapplicability of the TDI and TDI-Q tools for the quantitativemeasurement of TS
41 Limitations of the Study A major limitation of theproposed tool is the dependency of TS on the appliedforce during the movement of the cervical compression[14 18] However standardised conditions for the raw dataacquisition (maximal exertion of compression and care inavoiding the dislocation of the cervix) can optimise the TDI-based TS measurements to enhance feasibility and reliabilityTheproblems of themanual compression and unknown valueof the applied force implicate the impossibility to calculate theabsolute value of the elastic module of the cervix but allowedan estimation of the tissue stiffness Recently a manualmethod for cervical stiffness evaluation was proposed basedon the calculation of the anteroposterior cervical diameteranteroposterior 10 cervical diameter measured before (AP)and after (AP1015840) application of pressure on the cervix usingthe transvaginal probe The author describes an excellentintra- and interobserver correlation as well as a betterprediction of preterm delivery compared to the cervicallength measurement [19] Thus even if the technique ofParra measures the strain as Lagrangian strain while in ourprotocol the measure was made using the natural strain themechanism used for strain measurement remains the sameNonetheless comparison among different studies should bedone with caution Indeed for a small deformation thenatural and Lagrangian strains are similar as the Lagrangianand natural strains are interrelated by a fixed mathematicalformula (120576119873(119905) = ln(1 + 120576119871(119905)) but for a larger deformation(as induced in this study) the natural strain will always begreater [17]
The measurement of the stiffness in very short cer-vices can be limited due to the impossibility to direct thecompressing force perpendicularly to the cervical tissueHowever assessing the risk of preterm delivery in an asymp-tomatic patient will be probably more interesting than inpatients with a very ripened cervix which are already knownto be at great increased risk for preterm delivery
Furthermore in order to reduce the number of measure-ments to be performed the feasibility and reliability studywasfirst conducted testing some of these combinations amonga restricted group of patients by a single operator and thentested among thewhole study populationThus even if resultsdemonstrated the high reliability of this tool using the chosenpreset this does not exclude that other settings could workeven better than this Further studies considering this topiccomparing different settings and ROIs positioned in differentregions of the cervix are currently ongoing The clinicalusefulness of this diagnostic tool should be now tested inlarge prospective clinical settings even if preliminary resultsappear to be promising [20]
5 Conclusions
Under standardised conditions for the acquisition of rawdata and strain calculation the TDI-based cervical strain
measurements obtained during pregnancy are feasible andshow high intra- and interoperator reliability The strainmeasurements obtained during the relaxation frame using aDPof 5mmproved to be awell-performingTDI-Q setting forthe cervical TS measurement An objective and quantitativeestimation of cervical stiffness during pregnancy could bevery important for the estimation of preterm delivery riskand could improve assessment of cervical ripening at termto select patients for successful labor induction The clinicalusefulness of this diagnostic tool should be now tested in largeprospective clinical settings
Ethical Approval
The paper was approved by Ethics Committee of the localCollege of Surgeons and themedical Faculty at the Universityof Munster (Reference number 2010-256-f-S)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Authorsrsquo Contribution
A Fruscalzo contributed to conception planning perform-ing the experiments and writing the paper A P Londerocontributed to statistical analysis and cowriting the paperC Frohlich contributed to performing the experiments UMollmann contributed to performing the experiments andR Schmitz contributed to performing the experiments andcowriting the paper
Disclosure
The current address of A Fruscalzo is Obstetrics and Gyne-cology St Franziskus Hospital Hohenzollernring 72 48145Munster Germany
Acknowledgments
The authors thank Dr G Heywinkel (Chief Gynaecolo-gist Mathias-Spital Rheine Germany) Professor M Meyer-Wittkopf (Director of the Prenatal Diagnostic DepartmentMathias-Spital Rheine Germany) W Gorissen (ToshibaMedical Systems Europe Zoetermeer The Netherlands)Professor B Bijnens (ICREA-Universitat Pompeu FabraBarcelona Spain) and S Bertozzi (Clinic of Surgical Semei-otic AOU ldquoS M della Misericordiardquo of Udine Italy) for theirvaluable scientific advice as well as Dr A Dolle and Mr FHassel (Toshiba Medical Systems Neuss Germany) for theirlogistic and technical assistance
References
[1] E H Bishop ldquoPelvic scoring for elective inductionrdquo Obstetricsand Gynecology vol 24 pp 266ndash268 1964
BioMed Research International 9
[2] P Rozenberg ldquoThe secret cervixrdquo Ultrasound in Obstetrics andGynecology vol 32 no 2 pp 126ndash127 2008
[3] M L Palmeri and K R Nightingale ldquoWhat challenges must beovercome before ultrasound elasticity imaging is ready for theclinicrdquo Imaging in Medicine vol 3 no 4 pp 433ndash444 2011
[4] J Ophir I Cespedes H Ponnekanti Y Yazdi and X LildquoElastography a quantitative method for imaging the elasticityof biological tissuesrdquo Ultrasonic Imaging vol 13 no 2 pp 111ndash134 1991
[5] T M Eggeboslash I Oslashkland C Heien L K Gjessing P Romund-stad and K A Salvesen ldquoCan ultrasound measurementsreplace digitally assessed elements of the Bishop scorerdquo ActaObstetricia et Gynecologica Scandinavica vol 88 no 3 pp 325ndash331 2009
[6] G R Sutherland L Hatle P Claus J DrsquoHooge and BH Bijnens Doppler Myocardial Imaging A Textbook BSWKScientific Consulting and Publishing Hasselt Belgium 2006
[7] A Fruscalzo R Schmitz W Klockenbusch and J SteinhardldquoReliability of cervix elastography in late first and secondtrimester of pregnancyrdquo Ultraschall in der Medizin vol 33 no7 pp E101ndashE107 2012
[8] A Fruscalzo J Steinhard A P Londero et al ldquoReliabilityof quantitative elastography of the uterine cervix in at-termpregnanciesrdquo Journal of Perinatal Medicine vol 41 no 4 pp421ndash427 2013
[9] P M Bossuyt J B Reitsma D E Bruns et al ldquoTowards com-plete and accurate reporting of studies of diagnostic accuracythe STARD initiativerdquo Clinical Chemistry vol 49 no 1 pp 1ndash62003
[10] P E Shrout ldquoMeasurement reliability and agreement in psychi-atryrdquo Statistical Methods in Medical Research vol 7 no 3 pp301ndash317 1998
[11] I Tekesin L Hellmeyer G Heller A Romer M Kuhnert andS Schmidt ldquoEvaluation of quantitative ultrasound tissue char-acterization of the cervix and cervical length in the predictionof premature delivery for patients with spontaneous pretermlaborrdquo The American Journal of Obstetrics and Gynecology vol189 no 2 pp 532ndash539 2003
[12] M Swiatkowska-Freund and K Preis ldquoElastography of theuterine cervix implications for success of induction of laborrdquoUltrasound in Obstetrics and Gynecology vol 38 no 1 pp 52ndash56 2011
[13] F S Molina L F Gomez J Florido M C Padilla andK H Nicolaides ldquoQuantification of cervical elastography areproducibility studyrdquoUltrasound in Obstetrics and Gynecologyvol 39 no 6 pp 685ndash689 2012
[14] A Fruscalzo and R Schmitz ldquoQuantitative cervical elastogra-phy in pregnancyrdquoUltrasound inObstetrics andGynecology vol40 no 5 p 612 2012
[15] E Hernandez-Andrade S S Hassan H Ahn et al ldquoEvaluationof cervical stiffness during pregnancy using semiquantitativeultrasound elastographyrdquoUltrasound in Obstetrics and Gynecol-ogy vol 41 no 2 pp 152ndash161 2013
[16] T Fuchs R Woyton M Pomorski et al ldquoSonoelastography ofthe uterine cervix as a newdiagnostic tool of cervical assessmentin pregnant womenmdashpreliminary reportrdquo Ginekologia Polskavol 84 no 1 pp 12ndash16 2013
[17] J DrsquoHooge A Heimdal F Jamal et al ldquoRegional strain andstrain rate measurements by cardiac ultrasound principles
implementation and limitationsrdquo European Journal of Echocar-diography vol 1 no 3 pp 154ndash170 2000
[18] A Fruscalzo and R Schmitz ldquoReplyrdquo Ultrasound in Obstetricsand Gynecology vol 41 no 6 pp 712ndash714 2013
[19] M Parra-Saavedra L Gomez A Barrero G Parra F Vergaraand E Navarro ldquoPrediction of preterm birth using the cervicalconsistency indexrdquo Ultrasound in Obstetrics and Gynecologyvol 38 no 1 pp 44ndash51 2011
[20] A Fruscalzo A P Londero C Fr119894hlich M Meyer-Wittkopfand R Schmitz ldquoQuantitative elastography of cervix for pre-dicting labor induction successrdquo Ultraschall in der Medizin2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
Rela
xatio
n
Com
pres
sion
Relaxation phase
ROI
Probe
Compression phase
A
B
C
D
(a) (b)
1
2
Probe
Probe
ROI
ROI
12
1
2
12
1 2 1 2
2
1
Figure 1 (a) Strainmeasurement process the sequence of drawings (A B C andD) shows one cycle of gentle compression and the subsequentrelaxation of the anterior lip of the cervix through the vaginal probe as previously described (b) The process of TS calculation is displayed(above a compression and under a relaxation phase) a circular region of interest (ROI) is placed covering the whole thickness of the anteriorcervical lip The strain is then calculated during a compression phase (above from a time of maximal relaxation 1 to a time of maximalcompression 2) as well as during a relaxation phase (under from a time of maximal compression 2 to the time of the subsequent maximalrelaxation 1) The strain values are indicated as a function of the time during the movement (yellow line on the right)
2 Materials and Methods
21 Patients and Setting The study was conducted prospec-tively It was designed according to the Declaration ofHelsinki and was approved by the local ethics boardInformed consent was obtained from all patients at thetime of enrolment The patients included 74 consecutiveunselected women ranging from the 12th to the 42nd weeksof pregnancy recruited at the University Hospital of RheineGermany The preexamination exclusion criteria includedpretermmembrane rupture or uterine contractions and a riskof preterm delivery A minimal functional cervical lengthof approximately 15mm (which conformed to the vaginalprobe dimensions) was required to provide a sufficientcervical surface for an optimal examination Indeed a cervixshorter than the vaginal probe would not permit adequatelycompressing the cervix
22 Strain Measurement The process of TS measurementwas subdivided into the following two steps the first stepconsisted of the acquisition of raw data (raw data set acqui-sition) and the second step consisted of the analysis of the
acquired raw data for the purpose of strainmeasurement (TScalculation) The process of strain measurement is describedin Figure 1
23 Raw Data Set Acquisition Elastography was performedby a total of 2 gynaecologists Each patient underwent atransvaginal real-time elastography by the first operator andtwo raw data sets were acquired (f1 and f2) Elastography wasclosely replicated by a second operator and one additionalraw data set was acquired (s1) Real-time elastography wasconducted using a 9MHz vaginal probe and an Aplio XGultrasound system (Toshiba Medical Systems Tokyo Japan)The procedure was executed as follows [7] one to two cyclesof the gentle compression-relaxation phases were exertedalong the longitudinal axis of the cervix avoiding the lateraland longitudinal dislocation of the tissues until a maxi-mal compression of its anterior portion was obtained (ieuntil no further shortening of the anteroposterior diametercould be observed and the posterior part of the cervicallip begins to be axially dislocated) In order to check thequality of themovements exerted the transducer movementscould be monitored in the real-time B-mode displayed on
BioMed Research International 3
the left panel of the screen while the real-time elastographyis contemporarily displayed on the right panel using the split-screen mode Then a five-second loop including the lastcycles of compression-relaxation was acquired and stored inthe machine as raw data The raw data were acquired usingTDI software (Toshiba Medical Systems Tokyo Japan)
24 Raw Data Set Analysis and TS Calculation The TScalculations were performed offline using TDI-Q softwareThe procedure was executed as follows the region of interest(ROI) tracking function was selected and the natural strainpreset was chosen with a derivative pitch value of 5mm Acircular ROI was placed covering the whole thickness of theanterior cervical lip during the frame of the maximal tissuerelaxation Furthermore the ROI should be placed along theaxis of the compressing vaginal probe in the middle partof the cervix The TS values were then calculated duringthe relaxation phase (from the frame of maximal compres-sion to the frame of the subsequent maximal relaxation)Strain values were measured considering the cycle with alarger compression-relaxation cervical tissue excursion Aftermanually selecting the cycle of interest with a cursor thesoftware automatically calculated the strain which occurredduring the selected movement of compression (Figure 1)The strain calculation was executed by the first operator (F)both on its own acquired raw data set (Ff1 and Ff2) forthe calculation of intraobserver variability and on the firstraw data set acquired by the second operator (Fs1) for thecalculation of interoperator reliability The TS calculationwas then performed by the second operator (S) on its ownacquired raw data set (Ss1) and on the first raw data setacquired by the first operator (Sf1) across the entire patientpopulation for the calculation of interoperator reliability
25 Statistical Analysis The data were analysed using R(version 2141) and a significance level of 119875 lt 005 wasconsidered to be significant The data are presented as themedian values and the interquartile ranges (IQR) the meanvalue and standard deviation with prevalence and absolutevalues or the reference values and 95 confidence intervalsFirst we performed an analysis for each protocol to test theintraobserver and interobserver reliability of the raw dataset acquisition and the TS calculation (per protocol) Thenwe conducted additional tests to better assess the reliabil-ity of TS measurement (other analysis) For the reliabilityanalysis of the raw data acquisition and TS calculation weused the following tests intraclass correlation coefficient(ICC) the mean of differences and the difference betweenTS valuesmean of TS values (percentage difference) Thepercentage difference is defined as the difference between twovalues divided by the average of the two values It is shown as apercentage and we used it to show the amount of differencesbetween two measurements Moreover we used the Bland-Altman plots of the average against the differences of thetwo measurements and the limits of agreement were set astwo standard deviations from the mean of the differencesWe also plotted the 95 confidence intervals of the meanof differences to assess if the no difference line was inside
Table 1 Population features
Gestational age at examination (weeks) 2908 (plusmn893)First quartile (12ndash20 weeksrsquo gestation) 257 (1974)Second quartile (21ndash29 weeksrsquo gestation) 230 (1774)Third quartile (30ndash37 weeksrsquo gestation) 257 (1974)Fourth quartile (38ndash42 weeksrsquo gestation) 257 (1974)
Gravidity 2 (1-2)Parity 1 (1-2)
Para = 0 243 (1874)Para ge 1 757 (5674)
Cervical length (mm) 369 (plusmn1017)Number of fetuses
One 973 (7274)Twins 27 (274)
Pregnancy outcomesMode of delivery
Ongoing pregnancy 41 (3074)Vaginal spontaneous delivery 38 (2874)Cesarean section 20 (1574)Operative delivery 1 (174)
Gestational age at birth (weeks) 388 (plusmn18)Birth weight (grams) 323841 (plusmn64105)Description of the studied population The values reported are mean(plusmn standard deviation) median (interquartile range) or prevalence
or outside of this range We also used the following tests forthe continuous variables one way ANOVA Kruskal-Wallistest t-test or Wilcoxon test For the categorical variables weused Chi-square or exact Fisher tests where appropriate Toassess the correlations we used locally weighted scatter-plotsmoothing least squares line linear regression and Pearsonrsquostest where appropriate Finally we used Levenersquos test for thehomogeneity of variances to assess the degree of variance ofdifferences among the average measurements
The STARD (Standards for Reporting of DiagnosticAccuracy) criteria for the accurate reporting of studies ofdiagnostic accuracy were considered [9]
3 Results
31 Population Description The mean gestational age at thetime of examination in the 74 women considered in theconfirmatory phase (including the 17 women of trial phase)was 2908 weeks (plusmn893) Of these 41 had an ongoingpregnancy at the time of the statistical analysis of the studyresults whereas 59 had already delivered all at term ofpregnancy and without pregnancy-associated complicationsThe characteristics of the study population are summarisedin Table 1
32 Reproducibility of Raw Data Set Acquisition and TSCalculation In Table 2 we show the reproducibility ofraw data acquisition and the TS calculation during thevalidation phase We note that the reproducibility of the
4 BioMed Research International
Table 2 Reliability of tissue strain measurement
ICC consistency ICC agreement MD SD DM of TSReliability of straincalculation
Intraobserver (Ff1Ff1) 097 (095098) 097 (095098) minus0005 (minus00150006) 0047 7 (5ndash8)Interobserver (Ff1Sf1) 098 (097099) 098 (097099) minus0007 (minus00170002) 0041 5 (4ndash6)Interobserver (Fs1Ss1) 099 (099100) 099 (099100) minus0001 (minus00070004) 0023 3 (3-4)Interobserver (Ff1Sf1and Fs1Ss1) 099 (098099) 099 (098099) minus0004 (minus00100001) 0033 4 (3ndash5)
Reliability of raw dataacquirement
Interobserver (Ff1Fs1) 089 (084093) 089 (082093) minus0029 (minus0050minus0007) 0092 12 (9ndash15)Interobserver (Sf1Ss1) 091 (086094) 091 (085094) minus0020 (minus00400000) 0084 10 (8ndash13)Interobserver (Ff1Fs1and Sf1Ss1) 090 (086093) 089 (085092) minus0024 (minus0038minus0009) 0089 11 (10ndash13)
Reliability of raw dataacquirement and straincalculation
Intraobserver (Ff1Ff2) 093 (089096) 093 (090096) 0002 (minus00150019) 0072 10 (8ndash13)Interobserver (Ff1Ss1) 090 (085094) 089 (082093) minus0029 (minus0050minus0008) 0088 12 (9ndash14)Interobserver(Ff1Ff2Ss1mdashaverage of 2raw data)
093 (089096) 093 (089096) 0001 (minus00160018) 0072 10 (8ndash13)
Reproducibility of tissue strain measurement including raw data acquirement and tissue strain (TS) calculation In brackets the 95 confidence interval isreportedMDmean of differences SD standard deviation ofMD DM of TS (= percentage difference) difference between TS valuesmean of TS values (meanvalue and CI95)
TS calculation was high with an ICC agreement rangingbetween 097 and 099 Even if we consider the Bland-Altman plots most of the differences were within the regionof agreement (plusmn two standard deviations) and the averagediscrepancy between measures (bias space between dottedzero line and mean of differences line) was inconsistent(Figures 2(a) 2(b) and 2(c) and Table 2) Therefore we hadobserved an intra- and interobserver reproducibility of the TScalculation as well as a high intraobserver reproducibility ofthe raw data acquisition and the TS calculation (Figure 2(d))Across all the Bland-Altman plots (Figure 2) there wereno significant trends to obtain larger or smaller differencesbetween measurements as the average increased (119875 gt 005)Moreover we tested the variability of the scatter around thebias line across the graph using Levenersquos test for homogeneityof variance and the only relevant values are shown in Figures2(f) and 2(b) (one measurement) and Figure 2(c) (meanof two raw data measurements) which showed significanceof 119875 = 0054 119875 lt 005 and 119875 = 0399 respectivelyFurthermore regarding the interobserver reproducibility ofthe raw data acquisition (Figures 2(e) 2(f) 2(b) and 2(c) andTable 2) we found the lowest ICC values (ranging between089 and 091) however these values were in the moderateto high agreement regions [10] If we look at the Bland-Altman plots we note the presence of a bias (indicated bythe white space between the dotted zero line and the meanof the differences line) in all the plots that consider theinterobserver variability of rawdata acquisition or acquisition
and TS calculation (Figures 2(e) 2(f) and 2(b)) Bland-Altman plots the distance between the black line (themean ofdifferences) and the horizontal middle dotted zero line andthis space is defined as bias (= systematic error) (see Figures2(e) and 2(f)) The presence of this bias raises the questionof whether this average discrepancy between operators (iethe bias) is of clinical importance (ie if the intra- andinteroperator variability ofmeasurements are greater than thevariability due to differences among gestational age groups)Unfortunately we lacked the data to provide such an answerbecause the clinical usage of this test in the evaluation ofcervix has not yet been assessed Regardless to evaluatethe possible clinical relevance of this average discrepancybetween the operators (ie the bias) we made some furtherconsiderations First in Figures 2(e) 2(f) and 2(b) thedotted zero line was out of the 95 confidence intervalrange of the mean of differences (gray band) while in theother plots this was not the case Moreover in Figure 2(i)considering the mean of the two raw data acquisitions andthe TS calculations of F for the comparison along with theone raw data acquisition and TS calculation of S the biaswas corrected for and Levenersquos test became nonsignificantSecond the mean cervical TS at 12ndash20 gestational weeks was035 (plusmn007) at 21ndash29 gestational weeks was 041 (plusmn015) at30ndash37 gestational weeks was 065 (plusmn012) and after 37 weekswas 073 (plusmn009 119875 lt 005) The difference between everytwo values of the above TS values in relation to the meanof every two considered values (percentage difference) had a
BioMed Research International 5
mean value of 4317 (plusmn2400) (CI95 2705ndash5929) whilethe percentage difference due to the interobserver variability(DM of TS mean and CI95) had values which rangedbetween 10 and 12 (Table 2)
33 Relevant Correlations of Cervical TSwithMain PopulationFeatures Finally we found a significant correlation of the TSwith gestational age and cervical length (Figure 3) As full-term pregnancy approached the TS values increased reflect-ing softer cervical tissue Moreover a shorter cervical lengthmore frequently correlated with a high TS (again indicatinga softer cervix) (Figure 3) Overall the pluripara womenexhibited shorter and softer cervical properties compared tothe nullipara women (119875 lt 005) Correlation between TSand cervical length and parity for each subcategory were notsignificant (except for TS in the 21st to 29th gestational age)probably due to the low number of patients considered ineach subgroup (Table 3)
4 Discussion
Developing a new imaging technique for an objective assess-ment of tissue stiffness is potentially an important topicin obstetrics This could be helpful for an objective andnoninvasive description of the physiologic modification ofthe cervical stiffness occurring during pregnancy and fora better estimation of preterm delivery risk and laborinduction success Other authors tried to address this topicTekesin et al proposed the quantitative ultrasonic tissuecharacterization (QUTC) tool a software-based automatedtissue gray-scale analysis process Nonetheless this tool isbased only on a static B-mode picture of the cervix andthe insufficient interobserver reliability limited its furtherdevelopment [11] Recently Swiatkowska-Freund and Preisdescribed a cervical elastography tool where the entity oftissue movements against the vaginal probe during pelvicarterial pulsation and breathingsmovementwere representedon a colour map Unfortunately this colour-based Doppleranalysis allows only semiquantitative evaluation of tissuemovements on a scale from 0 to 4 Furthermore clinicalrelevance of these findings has yet to be confirmed [12]Molina et al and Fruscalzo and Schmitz proposed a similarapproach to that proposed by our group demonstrating thereliability of quantitative elastography but failing to find theway to standardize the applied pressure needed for translatingthe tool to the clinical practice [13 14] Finally Hernandez-Andrade et al demonstrated how also in a manually gen-erated semiquantitative elastography cervical tissue strainwas related to the most important clinical characteristics ofa nonselected population of pregnant women (in particularparity and cervical length) They showed also how cervicaltissue strainwasmore strongly associatedwith cervical lengththan with gestational age This could be explained by the factthat cervical softening accompanied by cervical shorteningis not always even if usually directly related to the advancinggestation age [15] Similarly significant correlation betweenthe cervical length and cervical elasticitywas reported in theirpreliminary results by Fuchs et al [16]
In this study the natural strain was chosen to test fora universal setting for the TS measurement that could beapplied throughout the whole gestational period Indeed theLagrangian but not the natural strain failed to perform inthe 3rd trimester when the cervix is softer and the tissuedeformation increases [8] The strain can be calculated bothas Lagrangian and natural strain Whereas the Lagrangianstrain describes the deformation (120576) of an object with itslength 119871(119905) relative to its initial length 119871(1199050)(120576119871(119905) = [119871(119905) minus119871(1199050)]119871(1199050)) the natural strain is based on the temporalintegration of the instantaneous deformation (119889120576) of thetissue (119889120576119873(119905) = [119871(119905 + 119889119905) minus 119871(119905)]119871(119905)) [17] In practicefor Lagrangian strain we just need a start and an enddimension to calculate the strain while natural strain willbe calculated over several measurement points In generalLagrangian strain is thought to bemore accurate than naturalstrain when small deformations are measured while thenatural strain is thought to be more appropriate in the caseof heterogeneous tissues or large tissue deformations (gt10ndash15) Indeed the software is less accurate in the strain calcu-lation than Lagrangian strain when following the ROI duringlarge movements While using natural strain calculation themeasured values are less dependent on the definition of theinitial length 1198710 [6] As discussed in our previous studies[7 8] in order to standardize the raw data set acquirementprocess the compressing force was exerted until a maximalcompression of its anterior portion was obtained and thecervical lip begins to be dislocated without further compres-sion Furthermore in order to standardize the procedureof strain calculation the ROI chosen was placed on thefull thickness of the anterior cervical lip Positioning theROI on different levels of the target tissue (anterior andposterior cervical lip) introduces an important bias on thestrain measurement Indeed different portions of the cervixare subjected to different forces depending on the distancefrom the compressing probe (due to the absorption of theforce) Otherwise examining the proximal and distal part ofthe cervix will imply exerting the compression movementsnot more perpendicularly to the cervix and introducing ashear strain component that actually cannot be calculatedFurthermore the distal part of the cervix would slip awayduring the compression movements and its lack of stabilitywould compromise the principles of standardisation of theapplied force Finally a minimal cervical length was required(we proposed a value of 15mm fitting the dimension ofthe vaginal probe) because the compression force should beexerted perpendicular to the longitudinal axis of the cervixIndeed it is intuitive that a very short cervix (shorter thanthe vaginal probe) does not permit adequately compressingthe cervix by the probe [7 8]
The results obtained using the proposed setting (5mmDPduring a relaxation phase) showed excellent results A highreliability was shown when comparing two measurementsof the same raw data set both if they were calculated bythe same operator and if they were calculated by anotheroperator (indicating intra- and interobserver reliability forthe TS calculation) These findings indicate that the processof TS calculation using the TDI-Q software has been properlystandardised and appears to be stable
6 BioMed Research International
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Intraobserver variabilityFf1Ff1 (calculation)
(a)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFf1Sf1 (calculation)
(b)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFs1Ss1 (calculation)
(c)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Intraobserver variability(acquirement and calculation)Ff1-Ff2
(d)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 (acquirement)
(e)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Ss1 (acquirement and calculation)
(f)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Sf1 and Fs1Ss1
(calculation)
(g)
minus03minus02minus01
00010203
(acquirement)
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 and Sf1Ss1
(h)
minus03minus02minus01
00010203
(acquirement and calculation)
00 02 04 06 08 10
Interobserver variabilityaverage of 2 raw dataFf1-Ff2Ss1
(i)
Figure 2 Reliability of tissue strain measurement Plots (a) (b) (c) (d) (e) and (f) (per protocol analysis) the Bland-Altman plotsdemonstrate the degree of concordance between the pairs of cervical TSs The region of agreement is included inside the two standarddeviations interval from the mean of differencesThe space included between the zero dotted lines and the mean of differences represents thebiasThe gray band where plotted represents the 95 confidence interval of themean of differences F and S refer to the operator undergoingthe TS calculation f and s refer to the operator undergoing the raw data acquirement where f1 and s1 and f2 and s2 refer respectively to the firstand second raw data sets (a)The intraobserver variability of the TS calculation of the same raw data (Ff1Ff1) is shown (b)The interobservervariability of the TS calculation of the same raw data by the two investigators (Ff1Sf1) is depicted (c) The interobserver variability of the TScalculation of the same raw data (Fs1Ss1) is shown (d) The intraobserver variability of the raw data acquisition and calculation (Ff1-Ff2) isshown (e) The interobserver variability of the raw data acquisition with two raw data sets acquired by different investigators (f and s) andcalculated by the same investigator is presented (Ff1Fs1) (f) The interobserver variability of the raw data acquisition and calculation by thetwo investigators is indicated (Ff1Ss1) Plots (g) (h) and (i) (other analysis) the Bland-Altman plots demonstrate the degree of concordancebetween the pairs of cervical TSs (g) The interobserver variability of the TS calculation in this plot we analyse all data from Figures 2(b)and 2(c) (ie Ff1Sf1 and Fs1Ss1) (h) The interobserver variability of the raw data acquirement the two raw data sets acquired by the twoinvestigators (F and S) aremeasured by the same investigator (Ff1Fs1 and Sf1Ss1) (i)The interobserver variability of the rawdata acquirementand calculation is shown (Ff1-Ff2Ss1 yielding an average of the 2 raw data f1 and f2) In this analysis we took into consideration the averageof the raw data measurements of investigator F versus the TS acquisition and measurement of one raw data set by investigator S
BioMed Research International 7
20 30 40Gestational age (weeks)
02
03
04
05
06
07
08
09
Cer
vica
l TS
rho 082 (CI95 073088)(P le 005)
(a)
20 30 40Gestational age (weeks)
20
30
40
50
60
Cer
vica
l len
gth
(mm
)
rho minus057 (CI95 minus071minus039)(P le 005)
(b)
20 30 40 50 600203040506070809
Cervical length (mm)
Cer
vica
l TS
rho minus059 (CI95 minus072minus042)(P le 005)
(c)
Figure 3 Tissue strain and patientsrsquo clinical features The correlation of TS (average of two raw data set measurements) with the gestationalage and cervical length (rho and 119875 value refer to Pearsonrsquos test)
Table 3 Strain values and parity
N Para = 0 (119899 = 18) N Para ge 1 (119899 = 56) PTS 18 037 (plusmn014) 56 059 (plusmn017) lt005
TS at 12ndash20 weeksrsquo gestation 8 035 (plusmn009) 11 035 (plusmn005) 0900TS at 21ndash29 weeksrsquo gestation 6 029 (plusmn005) 10 049 (plusmn014) lt005TS at 30ndash37 weeksrsquo gestation 3 058 (plusmn015) 16 066 (plusmn011) 0455TS at 38ndash42 weeksrsquo gestation 0 NA 19 073 (plusmn009) NA
Cervical length (mm) 18 4147 (plusmn992) 56 3537 (plusmn996) lt005Cervical length at 12ndash20 weeksrsquo gestation 8 4312 (plusmn1051) 11 4455 (plusmn726) 0748Cervical length at 21ndash29 weeksrsquo gestation 6 4267 (plusmn535) 10 398 (plusmn573) 0334Cervical length at 30ndash37 weeksrsquo gestation 3 3467 (plusmn1563) 16 3293 (plusmn919) 0868Cervical length at 38ndash42 weeksrsquo gestation 0 NA 19 2933 (plusmn902) NA
Tissue strain values related to parity and cervical length Mean (plusmn standard deviation)
Furthermore a high reliability was shown for the TSmea-surements when comparing the three different raw data sets(indicating intra- and interobserver reliability for the wholeprocess of TS measurement) The interobserver reliabilitywas less consistent due to the biases in raw data acquisitionbetween the two operators This difference could be over-come for example by repeating the measurement twice andcalculating the mean TS so that the eventual bias between
operators A and B will disappear These results confirm theimpression that the critical aspect of the TS measurementthat accounts for measurement reliability depends upon theprocess of raw data acquisition
Finally our results were correlated with the clinicalfeatures of the study population Specifically the cervicalTS seems to be related both to patientrsquos gestational ageand to her cervical length and parity Therefore unless the
8 BioMed Research International
relatively small number of patients used here does not allowfor generalisations these results indicate the potential clinicalapplicability of the TDI and TDI-Q tools for the quantitativemeasurement of TS
41 Limitations of the Study A major limitation of theproposed tool is the dependency of TS on the appliedforce during the movement of the cervical compression[14 18] However standardised conditions for the raw dataacquisition (maximal exertion of compression and care inavoiding the dislocation of the cervix) can optimise the TDI-based TS measurements to enhance feasibility and reliabilityTheproblems of themanual compression and unknown valueof the applied force implicate the impossibility to calculate theabsolute value of the elastic module of the cervix but allowedan estimation of the tissue stiffness Recently a manualmethod for cervical stiffness evaluation was proposed basedon the calculation of the anteroposterior cervical diameteranteroposterior 10 cervical diameter measured before (AP)and after (AP1015840) application of pressure on the cervix usingthe transvaginal probe The author describes an excellentintra- and interobserver correlation as well as a betterprediction of preterm delivery compared to the cervicallength measurement [19] Thus even if the technique ofParra measures the strain as Lagrangian strain while in ourprotocol the measure was made using the natural strain themechanism used for strain measurement remains the sameNonetheless comparison among different studies should bedone with caution Indeed for a small deformation thenatural and Lagrangian strains are similar as the Lagrangianand natural strains are interrelated by a fixed mathematicalformula (120576119873(119905) = ln(1 + 120576119871(119905)) but for a larger deformation(as induced in this study) the natural strain will always begreater [17]
The measurement of the stiffness in very short cer-vices can be limited due to the impossibility to direct thecompressing force perpendicularly to the cervical tissueHowever assessing the risk of preterm delivery in an asymp-tomatic patient will be probably more interesting than inpatients with a very ripened cervix which are already knownto be at great increased risk for preterm delivery
Furthermore in order to reduce the number of measure-ments to be performed the feasibility and reliability studywasfirst conducted testing some of these combinations amonga restricted group of patients by a single operator and thentested among thewhole study populationThus even if resultsdemonstrated the high reliability of this tool using the chosenpreset this does not exclude that other settings could workeven better than this Further studies considering this topiccomparing different settings and ROIs positioned in differentregions of the cervix are currently ongoing The clinicalusefulness of this diagnostic tool should be now tested inlarge prospective clinical settings even if preliminary resultsappear to be promising [20]
5 Conclusions
Under standardised conditions for the acquisition of rawdata and strain calculation the TDI-based cervical strain
measurements obtained during pregnancy are feasible andshow high intra- and interoperator reliability The strainmeasurements obtained during the relaxation frame using aDPof 5mmproved to be awell-performingTDI-Q setting forthe cervical TS measurement An objective and quantitativeestimation of cervical stiffness during pregnancy could bevery important for the estimation of preterm delivery riskand could improve assessment of cervical ripening at termto select patients for successful labor induction The clinicalusefulness of this diagnostic tool should be now tested in largeprospective clinical settings
Ethical Approval
The paper was approved by Ethics Committee of the localCollege of Surgeons and themedical Faculty at the Universityof Munster (Reference number 2010-256-f-S)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Authorsrsquo Contribution
A Fruscalzo contributed to conception planning perform-ing the experiments and writing the paper A P Londerocontributed to statistical analysis and cowriting the paperC Frohlich contributed to performing the experiments UMollmann contributed to performing the experiments andR Schmitz contributed to performing the experiments andcowriting the paper
Disclosure
The current address of A Fruscalzo is Obstetrics and Gyne-cology St Franziskus Hospital Hohenzollernring 72 48145Munster Germany
Acknowledgments
The authors thank Dr G Heywinkel (Chief Gynaecolo-gist Mathias-Spital Rheine Germany) Professor M Meyer-Wittkopf (Director of the Prenatal Diagnostic DepartmentMathias-Spital Rheine Germany) W Gorissen (ToshibaMedical Systems Europe Zoetermeer The Netherlands)Professor B Bijnens (ICREA-Universitat Pompeu FabraBarcelona Spain) and S Bertozzi (Clinic of Surgical Semei-otic AOU ldquoS M della Misericordiardquo of Udine Italy) for theirvaluable scientific advice as well as Dr A Dolle and Mr FHassel (Toshiba Medical Systems Neuss Germany) for theirlogistic and technical assistance
References
[1] E H Bishop ldquoPelvic scoring for elective inductionrdquo Obstetricsand Gynecology vol 24 pp 266ndash268 1964
BioMed Research International 9
[2] P Rozenberg ldquoThe secret cervixrdquo Ultrasound in Obstetrics andGynecology vol 32 no 2 pp 126ndash127 2008
[3] M L Palmeri and K R Nightingale ldquoWhat challenges must beovercome before ultrasound elasticity imaging is ready for theclinicrdquo Imaging in Medicine vol 3 no 4 pp 433ndash444 2011
[4] J Ophir I Cespedes H Ponnekanti Y Yazdi and X LildquoElastography a quantitative method for imaging the elasticityof biological tissuesrdquo Ultrasonic Imaging vol 13 no 2 pp 111ndash134 1991
[5] T M Eggeboslash I Oslashkland C Heien L K Gjessing P Romund-stad and K A Salvesen ldquoCan ultrasound measurementsreplace digitally assessed elements of the Bishop scorerdquo ActaObstetricia et Gynecologica Scandinavica vol 88 no 3 pp 325ndash331 2009
[6] G R Sutherland L Hatle P Claus J DrsquoHooge and BH Bijnens Doppler Myocardial Imaging A Textbook BSWKScientific Consulting and Publishing Hasselt Belgium 2006
[7] A Fruscalzo R Schmitz W Klockenbusch and J SteinhardldquoReliability of cervix elastography in late first and secondtrimester of pregnancyrdquo Ultraschall in der Medizin vol 33 no7 pp E101ndashE107 2012
[8] A Fruscalzo J Steinhard A P Londero et al ldquoReliabilityof quantitative elastography of the uterine cervix in at-termpregnanciesrdquo Journal of Perinatal Medicine vol 41 no 4 pp421ndash427 2013
[9] P M Bossuyt J B Reitsma D E Bruns et al ldquoTowards com-plete and accurate reporting of studies of diagnostic accuracythe STARD initiativerdquo Clinical Chemistry vol 49 no 1 pp 1ndash62003
[10] P E Shrout ldquoMeasurement reliability and agreement in psychi-atryrdquo Statistical Methods in Medical Research vol 7 no 3 pp301ndash317 1998
[11] I Tekesin L Hellmeyer G Heller A Romer M Kuhnert andS Schmidt ldquoEvaluation of quantitative ultrasound tissue char-acterization of the cervix and cervical length in the predictionof premature delivery for patients with spontaneous pretermlaborrdquo The American Journal of Obstetrics and Gynecology vol189 no 2 pp 532ndash539 2003
[12] M Swiatkowska-Freund and K Preis ldquoElastography of theuterine cervix implications for success of induction of laborrdquoUltrasound in Obstetrics and Gynecology vol 38 no 1 pp 52ndash56 2011
[13] F S Molina L F Gomez J Florido M C Padilla andK H Nicolaides ldquoQuantification of cervical elastography areproducibility studyrdquoUltrasound in Obstetrics and Gynecologyvol 39 no 6 pp 685ndash689 2012
[14] A Fruscalzo and R Schmitz ldquoQuantitative cervical elastogra-phy in pregnancyrdquoUltrasound inObstetrics andGynecology vol40 no 5 p 612 2012
[15] E Hernandez-Andrade S S Hassan H Ahn et al ldquoEvaluationof cervical stiffness during pregnancy using semiquantitativeultrasound elastographyrdquoUltrasound in Obstetrics and Gynecol-ogy vol 41 no 2 pp 152ndash161 2013
[16] T Fuchs R Woyton M Pomorski et al ldquoSonoelastography ofthe uterine cervix as a newdiagnostic tool of cervical assessmentin pregnant womenmdashpreliminary reportrdquo Ginekologia Polskavol 84 no 1 pp 12ndash16 2013
[17] J DrsquoHooge A Heimdal F Jamal et al ldquoRegional strain andstrain rate measurements by cardiac ultrasound principles
implementation and limitationsrdquo European Journal of Echocar-diography vol 1 no 3 pp 154ndash170 2000
[18] A Fruscalzo and R Schmitz ldquoReplyrdquo Ultrasound in Obstetricsand Gynecology vol 41 no 6 pp 712ndash714 2013
[19] M Parra-Saavedra L Gomez A Barrero G Parra F Vergaraand E Navarro ldquoPrediction of preterm birth using the cervicalconsistency indexrdquo Ultrasound in Obstetrics and Gynecologyvol 38 no 1 pp 44ndash51 2011
[20] A Fruscalzo A P Londero C Fr119894hlich M Meyer-Wittkopfand R Schmitz ldquoQuantitative elastography of cervix for pre-dicting labor induction successrdquo Ultraschall in der Medizin2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
the left panel of the screen while the real-time elastographyis contemporarily displayed on the right panel using the split-screen mode Then a five-second loop including the lastcycles of compression-relaxation was acquired and stored inthe machine as raw data The raw data were acquired usingTDI software (Toshiba Medical Systems Tokyo Japan)
24 Raw Data Set Analysis and TS Calculation The TScalculations were performed offline using TDI-Q softwareThe procedure was executed as follows the region of interest(ROI) tracking function was selected and the natural strainpreset was chosen with a derivative pitch value of 5mm Acircular ROI was placed covering the whole thickness of theanterior cervical lip during the frame of the maximal tissuerelaxation Furthermore the ROI should be placed along theaxis of the compressing vaginal probe in the middle partof the cervix The TS values were then calculated duringthe relaxation phase (from the frame of maximal compres-sion to the frame of the subsequent maximal relaxation)Strain values were measured considering the cycle with alarger compression-relaxation cervical tissue excursion Aftermanually selecting the cycle of interest with a cursor thesoftware automatically calculated the strain which occurredduring the selected movement of compression (Figure 1)The strain calculation was executed by the first operator (F)both on its own acquired raw data set (Ff1 and Ff2) forthe calculation of intraobserver variability and on the firstraw data set acquired by the second operator (Fs1) for thecalculation of interoperator reliability The TS calculationwas then performed by the second operator (S) on its ownacquired raw data set (Ss1) and on the first raw data setacquired by the first operator (Sf1) across the entire patientpopulation for the calculation of interoperator reliability
25 Statistical Analysis The data were analysed using R(version 2141) and a significance level of 119875 lt 005 wasconsidered to be significant The data are presented as themedian values and the interquartile ranges (IQR) the meanvalue and standard deviation with prevalence and absolutevalues or the reference values and 95 confidence intervalsFirst we performed an analysis for each protocol to test theintraobserver and interobserver reliability of the raw dataset acquisition and the TS calculation (per protocol) Thenwe conducted additional tests to better assess the reliabil-ity of TS measurement (other analysis) For the reliabilityanalysis of the raw data acquisition and TS calculation weused the following tests intraclass correlation coefficient(ICC) the mean of differences and the difference betweenTS valuesmean of TS values (percentage difference) Thepercentage difference is defined as the difference between twovalues divided by the average of the two values It is shown as apercentage and we used it to show the amount of differencesbetween two measurements Moreover we used the Bland-Altman plots of the average against the differences of thetwo measurements and the limits of agreement were set astwo standard deviations from the mean of the differencesWe also plotted the 95 confidence intervals of the meanof differences to assess if the no difference line was inside
Table 1 Population features
Gestational age at examination (weeks) 2908 (plusmn893)First quartile (12ndash20 weeksrsquo gestation) 257 (1974)Second quartile (21ndash29 weeksrsquo gestation) 230 (1774)Third quartile (30ndash37 weeksrsquo gestation) 257 (1974)Fourth quartile (38ndash42 weeksrsquo gestation) 257 (1974)
Gravidity 2 (1-2)Parity 1 (1-2)
Para = 0 243 (1874)Para ge 1 757 (5674)
Cervical length (mm) 369 (plusmn1017)Number of fetuses
One 973 (7274)Twins 27 (274)
Pregnancy outcomesMode of delivery
Ongoing pregnancy 41 (3074)Vaginal spontaneous delivery 38 (2874)Cesarean section 20 (1574)Operative delivery 1 (174)
Gestational age at birth (weeks) 388 (plusmn18)Birth weight (grams) 323841 (plusmn64105)Description of the studied population The values reported are mean(plusmn standard deviation) median (interquartile range) or prevalence
or outside of this range We also used the following tests forthe continuous variables one way ANOVA Kruskal-Wallistest t-test or Wilcoxon test For the categorical variables weused Chi-square or exact Fisher tests where appropriate Toassess the correlations we used locally weighted scatter-plotsmoothing least squares line linear regression and Pearsonrsquostest where appropriate Finally we used Levenersquos test for thehomogeneity of variances to assess the degree of variance ofdifferences among the average measurements
The STARD (Standards for Reporting of DiagnosticAccuracy) criteria for the accurate reporting of studies ofdiagnostic accuracy were considered [9]
3 Results
31 Population Description The mean gestational age at thetime of examination in the 74 women considered in theconfirmatory phase (including the 17 women of trial phase)was 2908 weeks (plusmn893) Of these 41 had an ongoingpregnancy at the time of the statistical analysis of the studyresults whereas 59 had already delivered all at term ofpregnancy and without pregnancy-associated complicationsThe characteristics of the study population are summarisedin Table 1
32 Reproducibility of Raw Data Set Acquisition and TSCalculation In Table 2 we show the reproducibility ofraw data acquisition and the TS calculation during thevalidation phase We note that the reproducibility of the
4 BioMed Research International
Table 2 Reliability of tissue strain measurement
ICC consistency ICC agreement MD SD DM of TSReliability of straincalculation
Intraobserver (Ff1Ff1) 097 (095098) 097 (095098) minus0005 (minus00150006) 0047 7 (5ndash8)Interobserver (Ff1Sf1) 098 (097099) 098 (097099) minus0007 (minus00170002) 0041 5 (4ndash6)Interobserver (Fs1Ss1) 099 (099100) 099 (099100) minus0001 (minus00070004) 0023 3 (3-4)Interobserver (Ff1Sf1and Fs1Ss1) 099 (098099) 099 (098099) minus0004 (minus00100001) 0033 4 (3ndash5)
Reliability of raw dataacquirement
Interobserver (Ff1Fs1) 089 (084093) 089 (082093) minus0029 (minus0050minus0007) 0092 12 (9ndash15)Interobserver (Sf1Ss1) 091 (086094) 091 (085094) minus0020 (minus00400000) 0084 10 (8ndash13)Interobserver (Ff1Fs1and Sf1Ss1) 090 (086093) 089 (085092) minus0024 (minus0038minus0009) 0089 11 (10ndash13)
Reliability of raw dataacquirement and straincalculation
Intraobserver (Ff1Ff2) 093 (089096) 093 (090096) 0002 (minus00150019) 0072 10 (8ndash13)Interobserver (Ff1Ss1) 090 (085094) 089 (082093) minus0029 (minus0050minus0008) 0088 12 (9ndash14)Interobserver(Ff1Ff2Ss1mdashaverage of 2raw data)
093 (089096) 093 (089096) 0001 (minus00160018) 0072 10 (8ndash13)
Reproducibility of tissue strain measurement including raw data acquirement and tissue strain (TS) calculation In brackets the 95 confidence interval isreportedMDmean of differences SD standard deviation ofMD DM of TS (= percentage difference) difference between TS valuesmean of TS values (meanvalue and CI95)
TS calculation was high with an ICC agreement rangingbetween 097 and 099 Even if we consider the Bland-Altman plots most of the differences were within the regionof agreement (plusmn two standard deviations) and the averagediscrepancy between measures (bias space between dottedzero line and mean of differences line) was inconsistent(Figures 2(a) 2(b) and 2(c) and Table 2) Therefore we hadobserved an intra- and interobserver reproducibility of the TScalculation as well as a high intraobserver reproducibility ofthe raw data acquisition and the TS calculation (Figure 2(d))Across all the Bland-Altman plots (Figure 2) there wereno significant trends to obtain larger or smaller differencesbetween measurements as the average increased (119875 gt 005)Moreover we tested the variability of the scatter around thebias line across the graph using Levenersquos test for homogeneityof variance and the only relevant values are shown in Figures2(f) and 2(b) (one measurement) and Figure 2(c) (meanof two raw data measurements) which showed significanceof 119875 = 0054 119875 lt 005 and 119875 = 0399 respectivelyFurthermore regarding the interobserver reproducibility ofthe raw data acquisition (Figures 2(e) 2(f) 2(b) and 2(c) andTable 2) we found the lowest ICC values (ranging between089 and 091) however these values were in the moderateto high agreement regions [10] If we look at the Bland-Altman plots we note the presence of a bias (indicated bythe white space between the dotted zero line and the meanof the differences line) in all the plots that consider theinterobserver variability of rawdata acquisition or acquisition
and TS calculation (Figures 2(e) 2(f) and 2(b)) Bland-Altman plots the distance between the black line (themean ofdifferences) and the horizontal middle dotted zero line andthis space is defined as bias (= systematic error) (see Figures2(e) and 2(f)) The presence of this bias raises the questionof whether this average discrepancy between operators (iethe bias) is of clinical importance (ie if the intra- andinteroperator variability ofmeasurements are greater than thevariability due to differences among gestational age groups)Unfortunately we lacked the data to provide such an answerbecause the clinical usage of this test in the evaluation ofcervix has not yet been assessed Regardless to evaluatethe possible clinical relevance of this average discrepancybetween the operators (ie the bias) we made some furtherconsiderations First in Figures 2(e) 2(f) and 2(b) thedotted zero line was out of the 95 confidence intervalrange of the mean of differences (gray band) while in theother plots this was not the case Moreover in Figure 2(i)considering the mean of the two raw data acquisitions andthe TS calculations of F for the comparison along with theone raw data acquisition and TS calculation of S the biaswas corrected for and Levenersquos test became nonsignificantSecond the mean cervical TS at 12ndash20 gestational weeks was035 (plusmn007) at 21ndash29 gestational weeks was 041 (plusmn015) at30ndash37 gestational weeks was 065 (plusmn012) and after 37 weekswas 073 (plusmn009 119875 lt 005) The difference between everytwo values of the above TS values in relation to the meanof every two considered values (percentage difference) had a
BioMed Research International 5
mean value of 4317 (plusmn2400) (CI95 2705ndash5929) whilethe percentage difference due to the interobserver variability(DM of TS mean and CI95) had values which rangedbetween 10 and 12 (Table 2)
33 Relevant Correlations of Cervical TSwithMain PopulationFeatures Finally we found a significant correlation of the TSwith gestational age and cervical length (Figure 3) As full-term pregnancy approached the TS values increased reflect-ing softer cervical tissue Moreover a shorter cervical lengthmore frequently correlated with a high TS (again indicatinga softer cervix) (Figure 3) Overall the pluripara womenexhibited shorter and softer cervical properties compared tothe nullipara women (119875 lt 005) Correlation between TSand cervical length and parity for each subcategory were notsignificant (except for TS in the 21st to 29th gestational age)probably due to the low number of patients considered ineach subgroup (Table 3)
4 Discussion
Developing a new imaging technique for an objective assess-ment of tissue stiffness is potentially an important topicin obstetrics This could be helpful for an objective andnoninvasive description of the physiologic modification ofthe cervical stiffness occurring during pregnancy and fora better estimation of preterm delivery risk and laborinduction success Other authors tried to address this topicTekesin et al proposed the quantitative ultrasonic tissuecharacterization (QUTC) tool a software-based automatedtissue gray-scale analysis process Nonetheless this tool isbased only on a static B-mode picture of the cervix andthe insufficient interobserver reliability limited its furtherdevelopment [11] Recently Swiatkowska-Freund and Preisdescribed a cervical elastography tool where the entity oftissue movements against the vaginal probe during pelvicarterial pulsation and breathingsmovementwere representedon a colour map Unfortunately this colour-based Doppleranalysis allows only semiquantitative evaluation of tissuemovements on a scale from 0 to 4 Furthermore clinicalrelevance of these findings has yet to be confirmed [12]Molina et al and Fruscalzo and Schmitz proposed a similarapproach to that proposed by our group demonstrating thereliability of quantitative elastography but failing to find theway to standardize the applied pressure needed for translatingthe tool to the clinical practice [13 14] Finally Hernandez-Andrade et al demonstrated how also in a manually gen-erated semiquantitative elastography cervical tissue strainwas related to the most important clinical characteristics ofa nonselected population of pregnant women (in particularparity and cervical length) They showed also how cervicaltissue strainwasmore strongly associatedwith cervical lengththan with gestational age This could be explained by the factthat cervical softening accompanied by cervical shorteningis not always even if usually directly related to the advancinggestation age [15] Similarly significant correlation betweenthe cervical length and cervical elasticitywas reported in theirpreliminary results by Fuchs et al [16]
In this study the natural strain was chosen to test fora universal setting for the TS measurement that could beapplied throughout the whole gestational period Indeed theLagrangian but not the natural strain failed to perform inthe 3rd trimester when the cervix is softer and the tissuedeformation increases [8] The strain can be calculated bothas Lagrangian and natural strain Whereas the Lagrangianstrain describes the deformation (120576) of an object with itslength 119871(119905) relative to its initial length 119871(1199050)(120576119871(119905) = [119871(119905) minus119871(1199050)]119871(1199050)) the natural strain is based on the temporalintegration of the instantaneous deformation (119889120576) of thetissue (119889120576119873(119905) = [119871(119905 + 119889119905) minus 119871(119905)]119871(119905)) [17] In practicefor Lagrangian strain we just need a start and an enddimension to calculate the strain while natural strain willbe calculated over several measurement points In generalLagrangian strain is thought to bemore accurate than naturalstrain when small deformations are measured while thenatural strain is thought to be more appropriate in the caseof heterogeneous tissues or large tissue deformations (gt10ndash15) Indeed the software is less accurate in the strain calcu-lation than Lagrangian strain when following the ROI duringlarge movements While using natural strain calculation themeasured values are less dependent on the definition of theinitial length 1198710 [6] As discussed in our previous studies[7 8] in order to standardize the raw data set acquirementprocess the compressing force was exerted until a maximalcompression of its anterior portion was obtained and thecervical lip begins to be dislocated without further compres-sion Furthermore in order to standardize the procedureof strain calculation the ROI chosen was placed on thefull thickness of the anterior cervical lip Positioning theROI on different levels of the target tissue (anterior andposterior cervical lip) introduces an important bias on thestrain measurement Indeed different portions of the cervixare subjected to different forces depending on the distancefrom the compressing probe (due to the absorption of theforce) Otherwise examining the proximal and distal part ofthe cervix will imply exerting the compression movementsnot more perpendicularly to the cervix and introducing ashear strain component that actually cannot be calculatedFurthermore the distal part of the cervix would slip awayduring the compression movements and its lack of stabilitywould compromise the principles of standardisation of theapplied force Finally a minimal cervical length was required(we proposed a value of 15mm fitting the dimension ofthe vaginal probe) because the compression force should beexerted perpendicular to the longitudinal axis of the cervixIndeed it is intuitive that a very short cervix (shorter thanthe vaginal probe) does not permit adequately compressingthe cervix by the probe [7 8]
The results obtained using the proposed setting (5mmDPduring a relaxation phase) showed excellent results A highreliability was shown when comparing two measurementsof the same raw data set both if they were calculated bythe same operator and if they were calculated by anotheroperator (indicating intra- and interobserver reliability forthe TS calculation) These findings indicate that the processof TS calculation using the TDI-Q software has been properlystandardised and appears to be stable
6 BioMed Research International
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Intraobserver variabilityFf1Ff1 (calculation)
(a)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFf1Sf1 (calculation)
(b)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFs1Ss1 (calculation)
(c)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Intraobserver variability(acquirement and calculation)Ff1-Ff2
(d)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 (acquirement)
(e)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Ss1 (acquirement and calculation)
(f)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Sf1 and Fs1Ss1
(calculation)
(g)
minus03minus02minus01
00010203
(acquirement)
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 and Sf1Ss1
(h)
minus03minus02minus01
00010203
(acquirement and calculation)
00 02 04 06 08 10
Interobserver variabilityaverage of 2 raw dataFf1-Ff2Ss1
(i)
Figure 2 Reliability of tissue strain measurement Plots (a) (b) (c) (d) (e) and (f) (per protocol analysis) the Bland-Altman plotsdemonstrate the degree of concordance between the pairs of cervical TSs The region of agreement is included inside the two standarddeviations interval from the mean of differencesThe space included between the zero dotted lines and the mean of differences represents thebiasThe gray band where plotted represents the 95 confidence interval of themean of differences F and S refer to the operator undergoingthe TS calculation f and s refer to the operator undergoing the raw data acquirement where f1 and s1 and f2 and s2 refer respectively to the firstand second raw data sets (a)The intraobserver variability of the TS calculation of the same raw data (Ff1Ff1) is shown (b)The interobservervariability of the TS calculation of the same raw data by the two investigators (Ff1Sf1) is depicted (c) The interobserver variability of the TScalculation of the same raw data (Fs1Ss1) is shown (d) The intraobserver variability of the raw data acquisition and calculation (Ff1-Ff2) isshown (e) The interobserver variability of the raw data acquisition with two raw data sets acquired by different investigators (f and s) andcalculated by the same investigator is presented (Ff1Fs1) (f) The interobserver variability of the raw data acquisition and calculation by thetwo investigators is indicated (Ff1Ss1) Plots (g) (h) and (i) (other analysis) the Bland-Altman plots demonstrate the degree of concordancebetween the pairs of cervical TSs (g) The interobserver variability of the TS calculation in this plot we analyse all data from Figures 2(b)and 2(c) (ie Ff1Sf1 and Fs1Ss1) (h) The interobserver variability of the raw data acquirement the two raw data sets acquired by the twoinvestigators (F and S) aremeasured by the same investigator (Ff1Fs1 and Sf1Ss1) (i)The interobserver variability of the rawdata acquirementand calculation is shown (Ff1-Ff2Ss1 yielding an average of the 2 raw data f1 and f2) In this analysis we took into consideration the averageof the raw data measurements of investigator F versus the TS acquisition and measurement of one raw data set by investigator S
BioMed Research International 7
20 30 40Gestational age (weeks)
02
03
04
05
06
07
08
09
Cer
vica
l TS
rho 082 (CI95 073088)(P le 005)
(a)
20 30 40Gestational age (weeks)
20
30
40
50
60
Cer
vica
l len
gth
(mm
)
rho minus057 (CI95 minus071minus039)(P le 005)
(b)
20 30 40 50 600203040506070809
Cervical length (mm)
Cer
vica
l TS
rho minus059 (CI95 minus072minus042)(P le 005)
(c)
Figure 3 Tissue strain and patientsrsquo clinical features The correlation of TS (average of two raw data set measurements) with the gestationalage and cervical length (rho and 119875 value refer to Pearsonrsquos test)
Table 3 Strain values and parity
N Para = 0 (119899 = 18) N Para ge 1 (119899 = 56) PTS 18 037 (plusmn014) 56 059 (plusmn017) lt005
TS at 12ndash20 weeksrsquo gestation 8 035 (plusmn009) 11 035 (plusmn005) 0900TS at 21ndash29 weeksrsquo gestation 6 029 (plusmn005) 10 049 (plusmn014) lt005TS at 30ndash37 weeksrsquo gestation 3 058 (plusmn015) 16 066 (plusmn011) 0455TS at 38ndash42 weeksrsquo gestation 0 NA 19 073 (plusmn009) NA
Cervical length (mm) 18 4147 (plusmn992) 56 3537 (plusmn996) lt005Cervical length at 12ndash20 weeksrsquo gestation 8 4312 (plusmn1051) 11 4455 (plusmn726) 0748Cervical length at 21ndash29 weeksrsquo gestation 6 4267 (plusmn535) 10 398 (plusmn573) 0334Cervical length at 30ndash37 weeksrsquo gestation 3 3467 (plusmn1563) 16 3293 (plusmn919) 0868Cervical length at 38ndash42 weeksrsquo gestation 0 NA 19 2933 (plusmn902) NA
Tissue strain values related to parity and cervical length Mean (plusmn standard deviation)
Furthermore a high reliability was shown for the TSmea-surements when comparing the three different raw data sets(indicating intra- and interobserver reliability for the wholeprocess of TS measurement) The interobserver reliabilitywas less consistent due to the biases in raw data acquisitionbetween the two operators This difference could be over-come for example by repeating the measurement twice andcalculating the mean TS so that the eventual bias between
operators A and B will disappear These results confirm theimpression that the critical aspect of the TS measurementthat accounts for measurement reliability depends upon theprocess of raw data acquisition
Finally our results were correlated with the clinicalfeatures of the study population Specifically the cervicalTS seems to be related both to patientrsquos gestational ageand to her cervical length and parity Therefore unless the
8 BioMed Research International
relatively small number of patients used here does not allowfor generalisations these results indicate the potential clinicalapplicability of the TDI and TDI-Q tools for the quantitativemeasurement of TS
41 Limitations of the Study A major limitation of theproposed tool is the dependency of TS on the appliedforce during the movement of the cervical compression[14 18] However standardised conditions for the raw dataacquisition (maximal exertion of compression and care inavoiding the dislocation of the cervix) can optimise the TDI-based TS measurements to enhance feasibility and reliabilityTheproblems of themanual compression and unknown valueof the applied force implicate the impossibility to calculate theabsolute value of the elastic module of the cervix but allowedan estimation of the tissue stiffness Recently a manualmethod for cervical stiffness evaluation was proposed basedon the calculation of the anteroposterior cervical diameteranteroposterior 10 cervical diameter measured before (AP)and after (AP1015840) application of pressure on the cervix usingthe transvaginal probe The author describes an excellentintra- and interobserver correlation as well as a betterprediction of preterm delivery compared to the cervicallength measurement [19] Thus even if the technique ofParra measures the strain as Lagrangian strain while in ourprotocol the measure was made using the natural strain themechanism used for strain measurement remains the sameNonetheless comparison among different studies should bedone with caution Indeed for a small deformation thenatural and Lagrangian strains are similar as the Lagrangianand natural strains are interrelated by a fixed mathematicalformula (120576119873(119905) = ln(1 + 120576119871(119905)) but for a larger deformation(as induced in this study) the natural strain will always begreater [17]
The measurement of the stiffness in very short cer-vices can be limited due to the impossibility to direct thecompressing force perpendicularly to the cervical tissueHowever assessing the risk of preterm delivery in an asymp-tomatic patient will be probably more interesting than inpatients with a very ripened cervix which are already knownto be at great increased risk for preterm delivery
Furthermore in order to reduce the number of measure-ments to be performed the feasibility and reliability studywasfirst conducted testing some of these combinations amonga restricted group of patients by a single operator and thentested among thewhole study populationThus even if resultsdemonstrated the high reliability of this tool using the chosenpreset this does not exclude that other settings could workeven better than this Further studies considering this topiccomparing different settings and ROIs positioned in differentregions of the cervix are currently ongoing The clinicalusefulness of this diagnostic tool should be now tested inlarge prospective clinical settings even if preliminary resultsappear to be promising [20]
5 Conclusions
Under standardised conditions for the acquisition of rawdata and strain calculation the TDI-based cervical strain
measurements obtained during pregnancy are feasible andshow high intra- and interoperator reliability The strainmeasurements obtained during the relaxation frame using aDPof 5mmproved to be awell-performingTDI-Q setting forthe cervical TS measurement An objective and quantitativeestimation of cervical stiffness during pregnancy could bevery important for the estimation of preterm delivery riskand could improve assessment of cervical ripening at termto select patients for successful labor induction The clinicalusefulness of this diagnostic tool should be now tested in largeprospective clinical settings
Ethical Approval
The paper was approved by Ethics Committee of the localCollege of Surgeons and themedical Faculty at the Universityof Munster (Reference number 2010-256-f-S)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Authorsrsquo Contribution
A Fruscalzo contributed to conception planning perform-ing the experiments and writing the paper A P Londerocontributed to statistical analysis and cowriting the paperC Frohlich contributed to performing the experiments UMollmann contributed to performing the experiments andR Schmitz contributed to performing the experiments andcowriting the paper
Disclosure
The current address of A Fruscalzo is Obstetrics and Gyne-cology St Franziskus Hospital Hohenzollernring 72 48145Munster Germany
Acknowledgments
The authors thank Dr G Heywinkel (Chief Gynaecolo-gist Mathias-Spital Rheine Germany) Professor M Meyer-Wittkopf (Director of the Prenatal Diagnostic DepartmentMathias-Spital Rheine Germany) W Gorissen (ToshibaMedical Systems Europe Zoetermeer The Netherlands)Professor B Bijnens (ICREA-Universitat Pompeu FabraBarcelona Spain) and S Bertozzi (Clinic of Surgical Semei-otic AOU ldquoS M della Misericordiardquo of Udine Italy) for theirvaluable scientific advice as well as Dr A Dolle and Mr FHassel (Toshiba Medical Systems Neuss Germany) for theirlogistic and technical assistance
References
[1] E H Bishop ldquoPelvic scoring for elective inductionrdquo Obstetricsand Gynecology vol 24 pp 266ndash268 1964
BioMed Research International 9
[2] P Rozenberg ldquoThe secret cervixrdquo Ultrasound in Obstetrics andGynecology vol 32 no 2 pp 126ndash127 2008
[3] M L Palmeri and K R Nightingale ldquoWhat challenges must beovercome before ultrasound elasticity imaging is ready for theclinicrdquo Imaging in Medicine vol 3 no 4 pp 433ndash444 2011
[4] J Ophir I Cespedes H Ponnekanti Y Yazdi and X LildquoElastography a quantitative method for imaging the elasticityof biological tissuesrdquo Ultrasonic Imaging vol 13 no 2 pp 111ndash134 1991
[5] T M Eggeboslash I Oslashkland C Heien L K Gjessing P Romund-stad and K A Salvesen ldquoCan ultrasound measurementsreplace digitally assessed elements of the Bishop scorerdquo ActaObstetricia et Gynecologica Scandinavica vol 88 no 3 pp 325ndash331 2009
[6] G R Sutherland L Hatle P Claus J DrsquoHooge and BH Bijnens Doppler Myocardial Imaging A Textbook BSWKScientific Consulting and Publishing Hasselt Belgium 2006
[7] A Fruscalzo R Schmitz W Klockenbusch and J SteinhardldquoReliability of cervix elastography in late first and secondtrimester of pregnancyrdquo Ultraschall in der Medizin vol 33 no7 pp E101ndashE107 2012
[8] A Fruscalzo J Steinhard A P Londero et al ldquoReliabilityof quantitative elastography of the uterine cervix in at-termpregnanciesrdquo Journal of Perinatal Medicine vol 41 no 4 pp421ndash427 2013
[9] P M Bossuyt J B Reitsma D E Bruns et al ldquoTowards com-plete and accurate reporting of studies of diagnostic accuracythe STARD initiativerdquo Clinical Chemistry vol 49 no 1 pp 1ndash62003
[10] P E Shrout ldquoMeasurement reliability and agreement in psychi-atryrdquo Statistical Methods in Medical Research vol 7 no 3 pp301ndash317 1998
[11] I Tekesin L Hellmeyer G Heller A Romer M Kuhnert andS Schmidt ldquoEvaluation of quantitative ultrasound tissue char-acterization of the cervix and cervical length in the predictionof premature delivery for patients with spontaneous pretermlaborrdquo The American Journal of Obstetrics and Gynecology vol189 no 2 pp 532ndash539 2003
[12] M Swiatkowska-Freund and K Preis ldquoElastography of theuterine cervix implications for success of induction of laborrdquoUltrasound in Obstetrics and Gynecology vol 38 no 1 pp 52ndash56 2011
[13] F S Molina L F Gomez J Florido M C Padilla andK H Nicolaides ldquoQuantification of cervical elastography areproducibility studyrdquoUltrasound in Obstetrics and Gynecologyvol 39 no 6 pp 685ndash689 2012
[14] A Fruscalzo and R Schmitz ldquoQuantitative cervical elastogra-phy in pregnancyrdquoUltrasound inObstetrics andGynecology vol40 no 5 p 612 2012
[15] E Hernandez-Andrade S S Hassan H Ahn et al ldquoEvaluationof cervical stiffness during pregnancy using semiquantitativeultrasound elastographyrdquoUltrasound in Obstetrics and Gynecol-ogy vol 41 no 2 pp 152ndash161 2013
[16] T Fuchs R Woyton M Pomorski et al ldquoSonoelastography ofthe uterine cervix as a newdiagnostic tool of cervical assessmentin pregnant womenmdashpreliminary reportrdquo Ginekologia Polskavol 84 no 1 pp 12ndash16 2013
[17] J DrsquoHooge A Heimdal F Jamal et al ldquoRegional strain andstrain rate measurements by cardiac ultrasound principles
implementation and limitationsrdquo European Journal of Echocar-diography vol 1 no 3 pp 154ndash170 2000
[18] A Fruscalzo and R Schmitz ldquoReplyrdquo Ultrasound in Obstetricsand Gynecology vol 41 no 6 pp 712ndash714 2013
[19] M Parra-Saavedra L Gomez A Barrero G Parra F Vergaraand E Navarro ldquoPrediction of preterm birth using the cervicalconsistency indexrdquo Ultrasound in Obstetrics and Gynecologyvol 38 no 1 pp 44ndash51 2011
[20] A Fruscalzo A P Londero C Fr119894hlich M Meyer-Wittkopfand R Schmitz ldquoQuantitative elastography of cervix for pre-dicting labor induction successrdquo Ultraschall in der Medizin2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
Table 2 Reliability of tissue strain measurement
ICC consistency ICC agreement MD SD DM of TSReliability of straincalculation
Intraobserver (Ff1Ff1) 097 (095098) 097 (095098) minus0005 (minus00150006) 0047 7 (5ndash8)Interobserver (Ff1Sf1) 098 (097099) 098 (097099) minus0007 (minus00170002) 0041 5 (4ndash6)Interobserver (Fs1Ss1) 099 (099100) 099 (099100) minus0001 (minus00070004) 0023 3 (3-4)Interobserver (Ff1Sf1and Fs1Ss1) 099 (098099) 099 (098099) minus0004 (minus00100001) 0033 4 (3ndash5)
Reliability of raw dataacquirement
Interobserver (Ff1Fs1) 089 (084093) 089 (082093) minus0029 (minus0050minus0007) 0092 12 (9ndash15)Interobserver (Sf1Ss1) 091 (086094) 091 (085094) minus0020 (minus00400000) 0084 10 (8ndash13)Interobserver (Ff1Fs1and Sf1Ss1) 090 (086093) 089 (085092) minus0024 (minus0038minus0009) 0089 11 (10ndash13)
Reliability of raw dataacquirement and straincalculation
Intraobserver (Ff1Ff2) 093 (089096) 093 (090096) 0002 (minus00150019) 0072 10 (8ndash13)Interobserver (Ff1Ss1) 090 (085094) 089 (082093) minus0029 (minus0050minus0008) 0088 12 (9ndash14)Interobserver(Ff1Ff2Ss1mdashaverage of 2raw data)
093 (089096) 093 (089096) 0001 (minus00160018) 0072 10 (8ndash13)
Reproducibility of tissue strain measurement including raw data acquirement and tissue strain (TS) calculation In brackets the 95 confidence interval isreportedMDmean of differences SD standard deviation ofMD DM of TS (= percentage difference) difference between TS valuesmean of TS values (meanvalue and CI95)
TS calculation was high with an ICC agreement rangingbetween 097 and 099 Even if we consider the Bland-Altman plots most of the differences were within the regionof agreement (plusmn two standard deviations) and the averagediscrepancy between measures (bias space between dottedzero line and mean of differences line) was inconsistent(Figures 2(a) 2(b) and 2(c) and Table 2) Therefore we hadobserved an intra- and interobserver reproducibility of the TScalculation as well as a high intraobserver reproducibility ofthe raw data acquisition and the TS calculation (Figure 2(d))Across all the Bland-Altman plots (Figure 2) there wereno significant trends to obtain larger or smaller differencesbetween measurements as the average increased (119875 gt 005)Moreover we tested the variability of the scatter around thebias line across the graph using Levenersquos test for homogeneityof variance and the only relevant values are shown in Figures2(f) and 2(b) (one measurement) and Figure 2(c) (meanof two raw data measurements) which showed significanceof 119875 = 0054 119875 lt 005 and 119875 = 0399 respectivelyFurthermore regarding the interobserver reproducibility ofthe raw data acquisition (Figures 2(e) 2(f) 2(b) and 2(c) andTable 2) we found the lowest ICC values (ranging between089 and 091) however these values were in the moderateto high agreement regions [10] If we look at the Bland-Altman plots we note the presence of a bias (indicated bythe white space between the dotted zero line and the meanof the differences line) in all the plots that consider theinterobserver variability of rawdata acquisition or acquisition
and TS calculation (Figures 2(e) 2(f) and 2(b)) Bland-Altman plots the distance between the black line (themean ofdifferences) and the horizontal middle dotted zero line andthis space is defined as bias (= systematic error) (see Figures2(e) and 2(f)) The presence of this bias raises the questionof whether this average discrepancy between operators (iethe bias) is of clinical importance (ie if the intra- andinteroperator variability ofmeasurements are greater than thevariability due to differences among gestational age groups)Unfortunately we lacked the data to provide such an answerbecause the clinical usage of this test in the evaluation ofcervix has not yet been assessed Regardless to evaluatethe possible clinical relevance of this average discrepancybetween the operators (ie the bias) we made some furtherconsiderations First in Figures 2(e) 2(f) and 2(b) thedotted zero line was out of the 95 confidence intervalrange of the mean of differences (gray band) while in theother plots this was not the case Moreover in Figure 2(i)considering the mean of the two raw data acquisitions andthe TS calculations of F for the comparison along with theone raw data acquisition and TS calculation of S the biaswas corrected for and Levenersquos test became nonsignificantSecond the mean cervical TS at 12ndash20 gestational weeks was035 (plusmn007) at 21ndash29 gestational weeks was 041 (plusmn015) at30ndash37 gestational weeks was 065 (plusmn012) and after 37 weekswas 073 (plusmn009 119875 lt 005) The difference between everytwo values of the above TS values in relation to the meanof every two considered values (percentage difference) had a
BioMed Research International 5
mean value of 4317 (plusmn2400) (CI95 2705ndash5929) whilethe percentage difference due to the interobserver variability(DM of TS mean and CI95) had values which rangedbetween 10 and 12 (Table 2)
33 Relevant Correlations of Cervical TSwithMain PopulationFeatures Finally we found a significant correlation of the TSwith gestational age and cervical length (Figure 3) As full-term pregnancy approached the TS values increased reflect-ing softer cervical tissue Moreover a shorter cervical lengthmore frequently correlated with a high TS (again indicatinga softer cervix) (Figure 3) Overall the pluripara womenexhibited shorter and softer cervical properties compared tothe nullipara women (119875 lt 005) Correlation between TSand cervical length and parity for each subcategory were notsignificant (except for TS in the 21st to 29th gestational age)probably due to the low number of patients considered ineach subgroup (Table 3)
4 Discussion
Developing a new imaging technique for an objective assess-ment of tissue stiffness is potentially an important topicin obstetrics This could be helpful for an objective andnoninvasive description of the physiologic modification ofthe cervical stiffness occurring during pregnancy and fora better estimation of preterm delivery risk and laborinduction success Other authors tried to address this topicTekesin et al proposed the quantitative ultrasonic tissuecharacterization (QUTC) tool a software-based automatedtissue gray-scale analysis process Nonetheless this tool isbased only on a static B-mode picture of the cervix andthe insufficient interobserver reliability limited its furtherdevelopment [11] Recently Swiatkowska-Freund and Preisdescribed a cervical elastography tool where the entity oftissue movements against the vaginal probe during pelvicarterial pulsation and breathingsmovementwere representedon a colour map Unfortunately this colour-based Doppleranalysis allows only semiquantitative evaluation of tissuemovements on a scale from 0 to 4 Furthermore clinicalrelevance of these findings has yet to be confirmed [12]Molina et al and Fruscalzo and Schmitz proposed a similarapproach to that proposed by our group demonstrating thereliability of quantitative elastography but failing to find theway to standardize the applied pressure needed for translatingthe tool to the clinical practice [13 14] Finally Hernandez-Andrade et al demonstrated how also in a manually gen-erated semiquantitative elastography cervical tissue strainwas related to the most important clinical characteristics ofa nonselected population of pregnant women (in particularparity and cervical length) They showed also how cervicaltissue strainwasmore strongly associatedwith cervical lengththan with gestational age This could be explained by the factthat cervical softening accompanied by cervical shorteningis not always even if usually directly related to the advancinggestation age [15] Similarly significant correlation betweenthe cervical length and cervical elasticitywas reported in theirpreliminary results by Fuchs et al [16]
In this study the natural strain was chosen to test fora universal setting for the TS measurement that could beapplied throughout the whole gestational period Indeed theLagrangian but not the natural strain failed to perform inthe 3rd trimester when the cervix is softer and the tissuedeformation increases [8] The strain can be calculated bothas Lagrangian and natural strain Whereas the Lagrangianstrain describes the deformation (120576) of an object with itslength 119871(119905) relative to its initial length 119871(1199050)(120576119871(119905) = [119871(119905) minus119871(1199050)]119871(1199050)) the natural strain is based on the temporalintegration of the instantaneous deformation (119889120576) of thetissue (119889120576119873(119905) = [119871(119905 + 119889119905) minus 119871(119905)]119871(119905)) [17] In practicefor Lagrangian strain we just need a start and an enddimension to calculate the strain while natural strain willbe calculated over several measurement points In generalLagrangian strain is thought to bemore accurate than naturalstrain when small deformations are measured while thenatural strain is thought to be more appropriate in the caseof heterogeneous tissues or large tissue deformations (gt10ndash15) Indeed the software is less accurate in the strain calcu-lation than Lagrangian strain when following the ROI duringlarge movements While using natural strain calculation themeasured values are less dependent on the definition of theinitial length 1198710 [6] As discussed in our previous studies[7 8] in order to standardize the raw data set acquirementprocess the compressing force was exerted until a maximalcompression of its anterior portion was obtained and thecervical lip begins to be dislocated without further compres-sion Furthermore in order to standardize the procedureof strain calculation the ROI chosen was placed on thefull thickness of the anterior cervical lip Positioning theROI on different levels of the target tissue (anterior andposterior cervical lip) introduces an important bias on thestrain measurement Indeed different portions of the cervixare subjected to different forces depending on the distancefrom the compressing probe (due to the absorption of theforce) Otherwise examining the proximal and distal part ofthe cervix will imply exerting the compression movementsnot more perpendicularly to the cervix and introducing ashear strain component that actually cannot be calculatedFurthermore the distal part of the cervix would slip awayduring the compression movements and its lack of stabilitywould compromise the principles of standardisation of theapplied force Finally a minimal cervical length was required(we proposed a value of 15mm fitting the dimension ofthe vaginal probe) because the compression force should beexerted perpendicular to the longitudinal axis of the cervixIndeed it is intuitive that a very short cervix (shorter thanthe vaginal probe) does not permit adequately compressingthe cervix by the probe [7 8]
The results obtained using the proposed setting (5mmDPduring a relaxation phase) showed excellent results A highreliability was shown when comparing two measurementsof the same raw data set both if they were calculated bythe same operator and if they were calculated by anotheroperator (indicating intra- and interobserver reliability forthe TS calculation) These findings indicate that the processof TS calculation using the TDI-Q software has been properlystandardised and appears to be stable
6 BioMed Research International
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Intraobserver variabilityFf1Ff1 (calculation)
(a)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFf1Sf1 (calculation)
(b)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFs1Ss1 (calculation)
(c)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Intraobserver variability(acquirement and calculation)Ff1-Ff2
(d)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 (acquirement)
(e)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Ss1 (acquirement and calculation)
(f)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Sf1 and Fs1Ss1
(calculation)
(g)
minus03minus02minus01
00010203
(acquirement)
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 and Sf1Ss1
(h)
minus03minus02minus01
00010203
(acquirement and calculation)
00 02 04 06 08 10
Interobserver variabilityaverage of 2 raw dataFf1-Ff2Ss1
(i)
Figure 2 Reliability of tissue strain measurement Plots (a) (b) (c) (d) (e) and (f) (per protocol analysis) the Bland-Altman plotsdemonstrate the degree of concordance between the pairs of cervical TSs The region of agreement is included inside the two standarddeviations interval from the mean of differencesThe space included between the zero dotted lines and the mean of differences represents thebiasThe gray band where plotted represents the 95 confidence interval of themean of differences F and S refer to the operator undergoingthe TS calculation f and s refer to the operator undergoing the raw data acquirement where f1 and s1 and f2 and s2 refer respectively to the firstand second raw data sets (a)The intraobserver variability of the TS calculation of the same raw data (Ff1Ff1) is shown (b)The interobservervariability of the TS calculation of the same raw data by the two investigators (Ff1Sf1) is depicted (c) The interobserver variability of the TScalculation of the same raw data (Fs1Ss1) is shown (d) The intraobserver variability of the raw data acquisition and calculation (Ff1-Ff2) isshown (e) The interobserver variability of the raw data acquisition with two raw data sets acquired by different investigators (f and s) andcalculated by the same investigator is presented (Ff1Fs1) (f) The interobserver variability of the raw data acquisition and calculation by thetwo investigators is indicated (Ff1Ss1) Plots (g) (h) and (i) (other analysis) the Bland-Altman plots demonstrate the degree of concordancebetween the pairs of cervical TSs (g) The interobserver variability of the TS calculation in this plot we analyse all data from Figures 2(b)and 2(c) (ie Ff1Sf1 and Fs1Ss1) (h) The interobserver variability of the raw data acquirement the two raw data sets acquired by the twoinvestigators (F and S) aremeasured by the same investigator (Ff1Fs1 and Sf1Ss1) (i)The interobserver variability of the rawdata acquirementand calculation is shown (Ff1-Ff2Ss1 yielding an average of the 2 raw data f1 and f2) In this analysis we took into consideration the averageof the raw data measurements of investigator F versus the TS acquisition and measurement of one raw data set by investigator S
BioMed Research International 7
20 30 40Gestational age (weeks)
02
03
04
05
06
07
08
09
Cer
vica
l TS
rho 082 (CI95 073088)(P le 005)
(a)
20 30 40Gestational age (weeks)
20
30
40
50
60
Cer
vica
l len
gth
(mm
)
rho minus057 (CI95 minus071minus039)(P le 005)
(b)
20 30 40 50 600203040506070809
Cervical length (mm)
Cer
vica
l TS
rho minus059 (CI95 minus072minus042)(P le 005)
(c)
Figure 3 Tissue strain and patientsrsquo clinical features The correlation of TS (average of two raw data set measurements) with the gestationalage and cervical length (rho and 119875 value refer to Pearsonrsquos test)
Table 3 Strain values and parity
N Para = 0 (119899 = 18) N Para ge 1 (119899 = 56) PTS 18 037 (plusmn014) 56 059 (plusmn017) lt005
TS at 12ndash20 weeksrsquo gestation 8 035 (plusmn009) 11 035 (plusmn005) 0900TS at 21ndash29 weeksrsquo gestation 6 029 (plusmn005) 10 049 (plusmn014) lt005TS at 30ndash37 weeksrsquo gestation 3 058 (plusmn015) 16 066 (plusmn011) 0455TS at 38ndash42 weeksrsquo gestation 0 NA 19 073 (plusmn009) NA
Cervical length (mm) 18 4147 (plusmn992) 56 3537 (plusmn996) lt005Cervical length at 12ndash20 weeksrsquo gestation 8 4312 (plusmn1051) 11 4455 (plusmn726) 0748Cervical length at 21ndash29 weeksrsquo gestation 6 4267 (plusmn535) 10 398 (plusmn573) 0334Cervical length at 30ndash37 weeksrsquo gestation 3 3467 (plusmn1563) 16 3293 (plusmn919) 0868Cervical length at 38ndash42 weeksrsquo gestation 0 NA 19 2933 (plusmn902) NA
Tissue strain values related to parity and cervical length Mean (plusmn standard deviation)
Furthermore a high reliability was shown for the TSmea-surements when comparing the three different raw data sets(indicating intra- and interobserver reliability for the wholeprocess of TS measurement) The interobserver reliabilitywas less consistent due to the biases in raw data acquisitionbetween the two operators This difference could be over-come for example by repeating the measurement twice andcalculating the mean TS so that the eventual bias between
operators A and B will disappear These results confirm theimpression that the critical aspect of the TS measurementthat accounts for measurement reliability depends upon theprocess of raw data acquisition
Finally our results were correlated with the clinicalfeatures of the study population Specifically the cervicalTS seems to be related both to patientrsquos gestational ageand to her cervical length and parity Therefore unless the
8 BioMed Research International
relatively small number of patients used here does not allowfor generalisations these results indicate the potential clinicalapplicability of the TDI and TDI-Q tools for the quantitativemeasurement of TS
41 Limitations of the Study A major limitation of theproposed tool is the dependency of TS on the appliedforce during the movement of the cervical compression[14 18] However standardised conditions for the raw dataacquisition (maximal exertion of compression and care inavoiding the dislocation of the cervix) can optimise the TDI-based TS measurements to enhance feasibility and reliabilityTheproblems of themanual compression and unknown valueof the applied force implicate the impossibility to calculate theabsolute value of the elastic module of the cervix but allowedan estimation of the tissue stiffness Recently a manualmethod for cervical stiffness evaluation was proposed basedon the calculation of the anteroposterior cervical diameteranteroposterior 10 cervical diameter measured before (AP)and after (AP1015840) application of pressure on the cervix usingthe transvaginal probe The author describes an excellentintra- and interobserver correlation as well as a betterprediction of preterm delivery compared to the cervicallength measurement [19] Thus even if the technique ofParra measures the strain as Lagrangian strain while in ourprotocol the measure was made using the natural strain themechanism used for strain measurement remains the sameNonetheless comparison among different studies should bedone with caution Indeed for a small deformation thenatural and Lagrangian strains are similar as the Lagrangianand natural strains are interrelated by a fixed mathematicalformula (120576119873(119905) = ln(1 + 120576119871(119905)) but for a larger deformation(as induced in this study) the natural strain will always begreater [17]
The measurement of the stiffness in very short cer-vices can be limited due to the impossibility to direct thecompressing force perpendicularly to the cervical tissueHowever assessing the risk of preterm delivery in an asymp-tomatic patient will be probably more interesting than inpatients with a very ripened cervix which are already knownto be at great increased risk for preterm delivery
Furthermore in order to reduce the number of measure-ments to be performed the feasibility and reliability studywasfirst conducted testing some of these combinations amonga restricted group of patients by a single operator and thentested among thewhole study populationThus even if resultsdemonstrated the high reliability of this tool using the chosenpreset this does not exclude that other settings could workeven better than this Further studies considering this topiccomparing different settings and ROIs positioned in differentregions of the cervix are currently ongoing The clinicalusefulness of this diagnostic tool should be now tested inlarge prospective clinical settings even if preliminary resultsappear to be promising [20]
5 Conclusions
Under standardised conditions for the acquisition of rawdata and strain calculation the TDI-based cervical strain
measurements obtained during pregnancy are feasible andshow high intra- and interoperator reliability The strainmeasurements obtained during the relaxation frame using aDPof 5mmproved to be awell-performingTDI-Q setting forthe cervical TS measurement An objective and quantitativeestimation of cervical stiffness during pregnancy could bevery important for the estimation of preterm delivery riskand could improve assessment of cervical ripening at termto select patients for successful labor induction The clinicalusefulness of this diagnostic tool should be now tested in largeprospective clinical settings
Ethical Approval
The paper was approved by Ethics Committee of the localCollege of Surgeons and themedical Faculty at the Universityof Munster (Reference number 2010-256-f-S)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Authorsrsquo Contribution
A Fruscalzo contributed to conception planning perform-ing the experiments and writing the paper A P Londerocontributed to statistical analysis and cowriting the paperC Frohlich contributed to performing the experiments UMollmann contributed to performing the experiments andR Schmitz contributed to performing the experiments andcowriting the paper
Disclosure
The current address of A Fruscalzo is Obstetrics and Gyne-cology St Franziskus Hospital Hohenzollernring 72 48145Munster Germany
Acknowledgments
The authors thank Dr G Heywinkel (Chief Gynaecolo-gist Mathias-Spital Rheine Germany) Professor M Meyer-Wittkopf (Director of the Prenatal Diagnostic DepartmentMathias-Spital Rheine Germany) W Gorissen (ToshibaMedical Systems Europe Zoetermeer The Netherlands)Professor B Bijnens (ICREA-Universitat Pompeu FabraBarcelona Spain) and S Bertozzi (Clinic of Surgical Semei-otic AOU ldquoS M della Misericordiardquo of Udine Italy) for theirvaluable scientific advice as well as Dr A Dolle and Mr FHassel (Toshiba Medical Systems Neuss Germany) for theirlogistic and technical assistance
References
[1] E H Bishop ldquoPelvic scoring for elective inductionrdquo Obstetricsand Gynecology vol 24 pp 266ndash268 1964
BioMed Research International 9
[2] P Rozenberg ldquoThe secret cervixrdquo Ultrasound in Obstetrics andGynecology vol 32 no 2 pp 126ndash127 2008
[3] M L Palmeri and K R Nightingale ldquoWhat challenges must beovercome before ultrasound elasticity imaging is ready for theclinicrdquo Imaging in Medicine vol 3 no 4 pp 433ndash444 2011
[4] J Ophir I Cespedes H Ponnekanti Y Yazdi and X LildquoElastography a quantitative method for imaging the elasticityof biological tissuesrdquo Ultrasonic Imaging vol 13 no 2 pp 111ndash134 1991
[5] T M Eggeboslash I Oslashkland C Heien L K Gjessing P Romund-stad and K A Salvesen ldquoCan ultrasound measurementsreplace digitally assessed elements of the Bishop scorerdquo ActaObstetricia et Gynecologica Scandinavica vol 88 no 3 pp 325ndash331 2009
[6] G R Sutherland L Hatle P Claus J DrsquoHooge and BH Bijnens Doppler Myocardial Imaging A Textbook BSWKScientific Consulting and Publishing Hasselt Belgium 2006
[7] A Fruscalzo R Schmitz W Klockenbusch and J SteinhardldquoReliability of cervix elastography in late first and secondtrimester of pregnancyrdquo Ultraschall in der Medizin vol 33 no7 pp E101ndashE107 2012
[8] A Fruscalzo J Steinhard A P Londero et al ldquoReliabilityof quantitative elastography of the uterine cervix in at-termpregnanciesrdquo Journal of Perinatal Medicine vol 41 no 4 pp421ndash427 2013
[9] P M Bossuyt J B Reitsma D E Bruns et al ldquoTowards com-plete and accurate reporting of studies of diagnostic accuracythe STARD initiativerdquo Clinical Chemistry vol 49 no 1 pp 1ndash62003
[10] P E Shrout ldquoMeasurement reliability and agreement in psychi-atryrdquo Statistical Methods in Medical Research vol 7 no 3 pp301ndash317 1998
[11] I Tekesin L Hellmeyer G Heller A Romer M Kuhnert andS Schmidt ldquoEvaluation of quantitative ultrasound tissue char-acterization of the cervix and cervical length in the predictionof premature delivery for patients with spontaneous pretermlaborrdquo The American Journal of Obstetrics and Gynecology vol189 no 2 pp 532ndash539 2003
[12] M Swiatkowska-Freund and K Preis ldquoElastography of theuterine cervix implications for success of induction of laborrdquoUltrasound in Obstetrics and Gynecology vol 38 no 1 pp 52ndash56 2011
[13] F S Molina L F Gomez J Florido M C Padilla andK H Nicolaides ldquoQuantification of cervical elastography areproducibility studyrdquoUltrasound in Obstetrics and Gynecologyvol 39 no 6 pp 685ndash689 2012
[14] A Fruscalzo and R Schmitz ldquoQuantitative cervical elastogra-phy in pregnancyrdquoUltrasound inObstetrics andGynecology vol40 no 5 p 612 2012
[15] E Hernandez-Andrade S S Hassan H Ahn et al ldquoEvaluationof cervical stiffness during pregnancy using semiquantitativeultrasound elastographyrdquoUltrasound in Obstetrics and Gynecol-ogy vol 41 no 2 pp 152ndash161 2013
[16] T Fuchs R Woyton M Pomorski et al ldquoSonoelastography ofthe uterine cervix as a newdiagnostic tool of cervical assessmentin pregnant womenmdashpreliminary reportrdquo Ginekologia Polskavol 84 no 1 pp 12ndash16 2013
[17] J DrsquoHooge A Heimdal F Jamal et al ldquoRegional strain andstrain rate measurements by cardiac ultrasound principles
implementation and limitationsrdquo European Journal of Echocar-diography vol 1 no 3 pp 154ndash170 2000
[18] A Fruscalzo and R Schmitz ldquoReplyrdquo Ultrasound in Obstetricsand Gynecology vol 41 no 6 pp 712ndash714 2013
[19] M Parra-Saavedra L Gomez A Barrero G Parra F Vergaraand E Navarro ldquoPrediction of preterm birth using the cervicalconsistency indexrdquo Ultrasound in Obstetrics and Gynecologyvol 38 no 1 pp 44ndash51 2011
[20] A Fruscalzo A P Londero C Fr119894hlich M Meyer-Wittkopfand R Schmitz ldquoQuantitative elastography of cervix for pre-dicting labor induction successrdquo Ultraschall in der Medizin2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
mean value of 4317 (plusmn2400) (CI95 2705ndash5929) whilethe percentage difference due to the interobserver variability(DM of TS mean and CI95) had values which rangedbetween 10 and 12 (Table 2)
33 Relevant Correlations of Cervical TSwithMain PopulationFeatures Finally we found a significant correlation of the TSwith gestational age and cervical length (Figure 3) As full-term pregnancy approached the TS values increased reflect-ing softer cervical tissue Moreover a shorter cervical lengthmore frequently correlated with a high TS (again indicatinga softer cervix) (Figure 3) Overall the pluripara womenexhibited shorter and softer cervical properties compared tothe nullipara women (119875 lt 005) Correlation between TSand cervical length and parity for each subcategory were notsignificant (except for TS in the 21st to 29th gestational age)probably due to the low number of patients considered ineach subgroup (Table 3)
4 Discussion
Developing a new imaging technique for an objective assess-ment of tissue stiffness is potentially an important topicin obstetrics This could be helpful for an objective andnoninvasive description of the physiologic modification ofthe cervical stiffness occurring during pregnancy and fora better estimation of preterm delivery risk and laborinduction success Other authors tried to address this topicTekesin et al proposed the quantitative ultrasonic tissuecharacterization (QUTC) tool a software-based automatedtissue gray-scale analysis process Nonetheless this tool isbased only on a static B-mode picture of the cervix andthe insufficient interobserver reliability limited its furtherdevelopment [11] Recently Swiatkowska-Freund and Preisdescribed a cervical elastography tool where the entity oftissue movements against the vaginal probe during pelvicarterial pulsation and breathingsmovementwere representedon a colour map Unfortunately this colour-based Doppleranalysis allows only semiquantitative evaluation of tissuemovements on a scale from 0 to 4 Furthermore clinicalrelevance of these findings has yet to be confirmed [12]Molina et al and Fruscalzo and Schmitz proposed a similarapproach to that proposed by our group demonstrating thereliability of quantitative elastography but failing to find theway to standardize the applied pressure needed for translatingthe tool to the clinical practice [13 14] Finally Hernandez-Andrade et al demonstrated how also in a manually gen-erated semiquantitative elastography cervical tissue strainwas related to the most important clinical characteristics ofa nonselected population of pregnant women (in particularparity and cervical length) They showed also how cervicaltissue strainwasmore strongly associatedwith cervical lengththan with gestational age This could be explained by the factthat cervical softening accompanied by cervical shorteningis not always even if usually directly related to the advancinggestation age [15] Similarly significant correlation betweenthe cervical length and cervical elasticitywas reported in theirpreliminary results by Fuchs et al [16]
In this study the natural strain was chosen to test fora universal setting for the TS measurement that could beapplied throughout the whole gestational period Indeed theLagrangian but not the natural strain failed to perform inthe 3rd trimester when the cervix is softer and the tissuedeformation increases [8] The strain can be calculated bothas Lagrangian and natural strain Whereas the Lagrangianstrain describes the deformation (120576) of an object with itslength 119871(119905) relative to its initial length 119871(1199050)(120576119871(119905) = [119871(119905) minus119871(1199050)]119871(1199050)) the natural strain is based on the temporalintegration of the instantaneous deformation (119889120576) of thetissue (119889120576119873(119905) = [119871(119905 + 119889119905) minus 119871(119905)]119871(119905)) [17] In practicefor Lagrangian strain we just need a start and an enddimension to calculate the strain while natural strain willbe calculated over several measurement points In generalLagrangian strain is thought to bemore accurate than naturalstrain when small deformations are measured while thenatural strain is thought to be more appropriate in the caseof heterogeneous tissues or large tissue deformations (gt10ndash15) Indeed the software is less accurate in the strain calcu-lation than Lagrangian strain when following the ROI duringlarge movements While using natural strain calculation themeasured values are less dependent on the definition of theinitial length 1198710 [6] As discussed in our previous studies[7 8] in order to standardize the raw data set acquirementprocess the compressing force was exerted until a maximalcompression of its anterior portion was obtained and thecervical lip begins to be dislocated without further compres-sion Furthermore in order to standardize the procedureof strain calculation the ROI chosen was placed on thefull thickness of the anterior cervical lip Positioning theROI on different levels of the target tissue (anterior andposterior cervical lip) introduces an important bias on thestrain measurement Indeed different portions of the cervixare subjected to different forces depending on the distancefrom the compressing probe (due to the absorption of theforce) Otherwise examining the proximal and distal part ofthe cervix will imply exerting the compression movementsnot more perpendicularly to the cervix and introducing ashear strain component that actually cannot be calculatedFurthermore the distal part of the cervix would slip awayduring the compression movements and its lack of stabilitywould compromise the principles of standardisation of theapplied force Finally a minimal cervical length was required(we proposed a value of 15mm fitting the dimension ofthe vaginal probe) because the compression force should beexerted perpendicular to the longitudinal axis of the cervixIndeed it is intuitive that a very short cervix (shorter thanthe vaginal probe) does not permit adequately compressingthe cervix by the probe [7 8]
The results obtained using the proposed setting (5mmDPduring a relaxation phase) showed excellent results A highreliability was shown when comparing two measurementsof the same raw data set both if they were calculated bythe same operator and if they were calculated by anotheroperator (indicating intra- and interobserver reliability forthe TS calculation) These findings indicate that the processof TS calculation using the TDI-Q software has been properlystandardised and appears to be stable
6 BioMed Research International
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Intraobserver variabilityFf1Ff1 (calculation)
(a)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFf1Sf1 (calculation)
(b)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFs1Ss1 (calculation)
(c)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Intraobserver variability(acquirement and calculation)Ff1-Ff2
(d)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 (acquirement)
(e)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Ss1 (acquirement and calculation)
(f)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Sf1 and Fs1Ss1
(calculation)
(g)
minus03minus02minus01
00010203
(acquirement)
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 and Sf1Ss1
(h)
minus03minus02minus01
00010203
(acquirement and calculation)
00 02 04 06 08 10
Interobserver variabilityaverage of 2 raw dataFf1-Ff2Ss1
(i)
Figure 2 Reliability of tissue strain measurement Plots (a) (b) (c) (d) (e) and (f) (per protocol analysis) the Bland-Altman plotsdemonstrate the degree of concordance between the pairs of cervical TSs The region of agreement is included inside the two standarddeviations interval from the mean of differencesThe space included between the zero dotted lines and the mean of differences represents thebiasThe gray band where plotted represents the 95 confidence interval of themean of differences F and S refer to the operator undergoingthe TS calculation f and s refer to the operator undergoing the raw data acquirement where f1 and s1 and f2 and s2 refer respectively to the firstand second raw data sets (a)The intraobserver variability of the TS calculation of the same raw data (Ff1Ff1) is shown (b)The interobservervariability of the TS calculation of the same raw data by the two investigators (Ff1Sf1) is depicted (c) The interobserver variability of the TScalculation of the same raw data (Fs1Ss1) is shown (d) The intraobserver variability of the raw data acquisition and calculation (Ff1-Ff2) isshown (e) The interobserver variability of the raw data acquisition with two raw data sets acquired by different investigators (f and s) andcalculated by the same investigator is presented (Ff1Fs1) (f) The interobserver variability of the raw data acquisition and calculation by thetwo investigators is indicated (Ff1Ss1) Plots (g) (h) and (i) (other analysis) the Bland-Altman plots demonstrate the degree of concordancebetween the pairs of cervical TSs (g) The interobserver variability of the TS calculation in this plot we analyse all data from Figures 2(b)and 2(c) (ie Ff1Sf1 and Fs1Ss1) (h) The interobserver variability of the raw data acquirement the two raw data sets acquired by the twoinvestigators (F and S) aremeasured by the same investigator (Ff1Fs1 and Sf1Ss1) (i)The interobserver variability of the rawdata acquirementand calculation is shown (Ff1-Ff2Ss1 yielding an average of the 2 raw data f1 and f2) In this analysis we took into consideration the averageof the raw data measurements of investigator F versus the TS acquisition and measurement of one raw data set by investigator S
BioMed Research International 7
20 30 40Gestational age (weeks)
02
03
04
05
06
07
08
09
Cer
vica
l TS
rho 082 (CI95 073088)(P le 005)
(a)
20 30 40Gestational age (weeks)
20
30
40
50
60
Cer
vica
l len
gth
(mm
)
rho minus057 (CI95 minus071minus039)(P le 005)
(b)
20 30 40 50 600203040506070809
Cervical length (mm)
Cer
vica
l TS
rho minus059 (CI95 minus072minus042)(P le 005)
(c)
Figure 3 Tissue strain and patientsrsquo clinical features The correlation of TS (average of two raw data set measurements) with the gestationalage and cervical length (rho and 119875 value refer to Pearsonrsquos test)
Table 3 Strain values and parity
N Para = 0 (119899 = 18) N Para ge 1 (119899 = 56) PTS 18 037 (plusmn014) 56 059 (plusmn017) lt005
TS at 12ndash20 weeksrsquo gestation 8 035 (plusmn009) 11 035 (plusmn005) 0900TS at 21ndash29 weeksrsquo gestation 6 029 (plusmn005) 10 049 (plusmn014) lt005TS at 30ndash37 weeksrsquo gestation 3 058 (plusmn015) 16 066 (plusmn011) 0455TS at 38ndash42 weeksrsquo gestation 0 NA 19 073 (plusmn009) NA
Cervical length (mm) 18 4147 (plusmn992) 56 3537 (plusmn996) lt005Cervical length at 12ndash20 weeksrsquo gestation 8 4312 (plusmn1051) 11 4455 (plusmn726) 0748Cervical length at 21ndash29 weeksrsquo gestation 6 4267 (plusmn535) 10 398 (plusmn573) 0334Cervical length at 30ndash37 weeksrsquo gestation 3 3467 (plusmn1563) 16 3293 (plusmn919) 0868Cervical length at 38ndash42 weeksrsquo gestation 0 NA 19 2933 (plusmn902) NA
Tissue strain values related to parity and cervical length Mean (plusmn standard deviation)
Furthermore a high reliability was shown for the TSmea-surements when comparing the three different raw data sets(indicating intra- and interobserver reliability for the wholeprocess of TS measurement) The interobserver reliabilitywas less consistent due to the biases in raw data acquisitionbetween the two operators This difference could be over-come for example by repeating the measurement twice andcalculating the mean TS so that the eventual bias between
operators A and B will disappear These results confirm theimpression that the critical aspect of the TS measurementthat accounts for measurement reliability depends upon theprocess of raw data acquisition
Finally our results were correlated with the clinicalfeatures of the study population Specifically the cervicalTS seems to be related both to patientrsquos gestational ageand to her cervical length and parity Therefore unless the
8 BioMed Research International
relatively small number of patients used here does not allowfor generalisations these results indicate the potential clinicalapplicability of the TDI and TDI-Q tools for the quantitativemeasurement of TS
41 Limitations of the Study A major limitation of theproposed tool is the dependency of TS on the appliedforce during the movement of the cervical compression[14 18] However standardised conditions for the raw dataacquisition (maximal exertion of compression and care inavoiding the dislocation of the cervix) can optimise the TDI-based TS measurements to enhance feasibility and reliabilityTheproblems of themanual compression and unknown valueof the applied force implicate the impossibility to calculate theabsolute value of the elastic module of the cervix but allowedan estimation of the tissue stiffness Recently a manualmethod for cervical stiffness evaluation was proposed basedon the calculation of the anteroposterior cervical diameteranteroposterior 10 cervical diameter measured before (AP)and after (AP1015840) application of pressure on the cervix usingthe transvaginal probe The author describes an excellentintra- and interobserver correlation as well as a betterprediction of preterm delivery compared to the cervicallength measurement [19] Thus even if the technique ofParra measures the strain as Lagrangian strain while in ourprotocol the measure was made using the natural strain themechanism used for strain measurement remains the sameNonetheless comparison among different studies should bedone with caution Indeed for a small deformation thenatural and Lagrangian strains are similar as the Lagrangianand natural strains are interrelated by a fixed mathematicalformula (120576119873(119905) = ln(1 + 120576119871(119905)) but for a larger deformation(as induced in this study) the natural strain will always begreater [17]
The measurement of the stiffness in very short cer-vices can be limited due to the impossibility to direct thecompressing force perpendicularly to the cervical tissueHowever assessing the risk of preterm delivery in an asymp-tomatic patient will be probably more interesting than inpatients with a very ripened cervix which are already knownto be at great increased risk for preterm delivery
Furthermore in order to reduce the number of measure-ments to be performed the feasibility and reliability studywasfirst conducted testing some of these combinations amonga restricted group of patients by a single operator and thentested among thewhole study populationThus even if resultsdemonstrated the high reliability of this tool using the chosenpreset this does not exclude that other settings could workeven better than this Further studies considering this topiccomparing different settings and ROIs positioned in differentregions of the cervix are currently ongoing The clinicalusefulness of this diagnostic tool should be now tested inlarge prospective clinical settings even if preliminary resultsappear to be promising [20]
5 Conclusions
Under standardised conditions for the acquisition of rawdata and strain calculation the TDI-based cervical strain
measurements obtained during pregnancy are feasible andshow high intra- and interoperator reliability The strainmeasurements obtained during the relaxation frame using aDPof 5mmproved to be awell-performingTDI-Q setting forthe cervical TS measurement An objective and quantitativeestimation of cervical stiffness during pregnancy could bevery important for the estimation of preterm delivery riskand could improve assessment of cervical ripening at termto select patients for successful labor induction The clinicalusefulness of this diagnostic tool should be now tested in largeprospective clinical settings
Ethical Approval
The paper was approved by Ethics Committee of the localCollege of Surgeons and themedical Faculty at the Universityof Munster (Reference number 2010-256-f-S)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Authorsrsquo Contribution
A Fruscalzo contributed to conception planning perform-ing the experiments and writing the paper A P Londerocontributed to statistical analysis and cowriting the paperC Frohlich contributed to performing the experiments UMollmann contributed to performing the experiments andR Schmitz contributed to performing the experiments andcowriting the paper
Disclosure
The current address of A Fruscalzo is Obstetrics and Gyne-cology St Franziskus Hospital Hohenzollernring 72 48145Munster Germany
Acknowledgments
The authors thank Dr G Heywinkel (Chief Gynaecolo-gist Mathias-Spital Rheine Germany) Professor M Meyer-Wittkopf (Director of the Prenatal Diagnostic DepartmentMathias-Spital Rheine Germany) W Gorissen (ToshibaMedical Systems Europe Zoetermeer The Netherlands)Professor B Bijnens (ICREA-Universitat Pompeu FabraBarcelona Spain) and S Bertozzi (Clinic of Surgical Semei-otic AOU ldquoS M della Misericordiardquo of Udine Italy) for theirvaluable scientific advice as well as Dr A Dolle and Mr FHassel (Toshiba Medical Systems Neuss Germany) for theirlogistic and technical assistance
References
[1] E H Bishop ldquoPelvic scoring for elective inductionrdquo Obstetricsand Gynecology vol 24 pp 266ndash268 1964
BioMed Research International 9
[2] P Rozenberg ldquoThe secret cervixrdquo Ultrasound in Obstetrics andGynecology vol 32 no 2 pp 126ndash127 2008
[3] M L Palmeri and K R Nightingale ldquoWhat challenges must beovercome before ultrasound elasticity imaging is ready for theclinicrdquo Imaging in Medicine vol 3 no 4 pp 433ndash444 2011
[4] J Ophir I Cespedes H Ponnekanti Y Yazdi and X LildquoElastography a quantitative method for imaging the elasticityof biological tissuesrdquo Ultrasonic Imaging vol 13 no 2 pp 111ndash134 1991
[5] T M Eggeboslash I Oslashkland C Heien L K Gjessing P Romund-stad and K A Salvesen ldquoCan ultrasound measurementsreplace digitally assessed elements of the Bishop scorerdquo ActaObstetricia et Gynecologica Scandinavica vol 88 no 3 pp 325ndash331 2009
[6] G R Sutherland L Hatle P Claus J DrsquoHooge and BH Bijnens Doppler Myocardial Imaging A Textbook BSWKScientific Consulting and Publishing Hasselt Belgium 2006
[7] A Fruscalzo R Schmitz W Klockenbusch and J SteinhardldquoReliability of cervix elastography in late first and secondtrimester of pregnancyrdquo Ultraschall in der Medizin vol 33 no7 pp E101ndashE107 2012
[8] A Fruscalzo J Steinhard A P Londero et al ldquoReliabilityof quantitative elastography of the uterine cervix in at-termpregnanciesrdquo Journal of Perinatal Medicine vol 41 no 4 pp421ndash427 2013
[9] P M Bossuyt J B Reitsma D E Bruns et al ldquoTowards com-plete and accurate reporting of studies of diagnostic accuracythe STARD initiativerdquo Clinical Chemistry vol 49 no 1 pp 1ndash62003
[10] P E Shrout ldquoMeasurement reliability and agreement in psychi-atryrdquo Statistical Methods in Medical Research vol 7 no 3 pp301ndash317 1998
[11] I Tekesin L Hellmeyer G Heller A Romer M Kuhnert andS Schmidt ldquoEvaluation of quantitative ultrasound tissue char-acterization of the cervix and cervical length in the predictionof premature delivery for patients with spontaneous pretermlaborrdquo The American Journal of Obstetrics and Gynecology vol189 no 2 pp 532ndash539 2003
[12] M Swiatkowska-Freund and K Preis ldquoElastography of theuterine cervix implications for success of induction of laborrdquoUltrasound in Obstetrics and Gynecology vol 38 no 1 pp 52ndash56 2011
[13] F S Molina L F Gomez J Florido M C Padilla andK H Nicolaides ldquoQuantification of cervical elastography areproducibility studyrdquoUltrasound in Obstetrics and Gynecologyvol 39 no 6 pp 685ndash689 2012
[14] A Fruscalzo and R Schmitz ldquoQuantitative cervical elastogra-phy in pregnancyrdquoUltrasound inObstetrics andGynecology vol40 no 5 p 612 2012
[15] E Hernandez-Andrade S S Hassan H Ahn et al ldquoEvaluationof cervical stiffness during pregnancy using semiquantitativeultrasound elastographyrdquoUltrasound in Obstetrics and Gynecol-ogy vol 41 no 2 pp 152ndash161 2013
[16] T Fuchs R Woyton M Pomorski et al ldquoSonoelastography ofthe uterine cervix as a newdiagnostic tool of cervical assessmentin pregnant womenmdashpreliminary reportrdquo Ginekologia Polskavol 84 no 1 pp 12ndash16 2013
[17] J DrsquoHooge A Heimdal F Jamal et al ldquoRegional strain andstrain rate measurements by cardiac ultrasound principles
implementation and limitationsrdquo European Journal of Echocar-diography vol 1 no 3 pp 154ndash170 2000
[18] A Fruscalzo and R Schmitz ldquoReplyrdquo Ultrasound in Obstetricsand Gynecology vol 41 no 6 pp 712ndash714 2013
[19] M Parra-Saavedra L Gomez A Barrero G Parra F Vergaraand E Navarro ldquoPrediction of preterm birth using the cervicalconsistency indexrdquo Ultrasound in Obstetrics and Gynecologyvol 38 no 1 pp 44ndash51 2011
[20] A Fruscalzo A P Londero C Fr119894hlich M Meyer-Wittkopfand R Schmitz ldquoQuantitative elastography of cervix for pre-dicting labor induction successrdquo Ultraschall in der Medizin2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 BioMed Research International
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Intraobserver variabilityFf1Ff1 (calculation)
(a)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFf1Sf1 (calculation)
(b)
00 02 04 06 08 10
minus03
minus02
minus01
00
01
02
03
Interobserver variabilityFs1Ss1 (calculation)
(c)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Intraobserver variability(acquirement and calculation)Ff1-Ff2
(d)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 (acquirement)
(e)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Ss1 (acquirement and calculation)
(f)
minus03
minus02
minus01
00
01
02
03
00 02 04 06 08 10
Interobserver variabilityFf1Sf1 and Fs1Ss1
(calculation)
(g)
minus03minus02minus01
00010203
(acquirement)
00 02 04 06 08 10
Interobserver variabilityFf1Fs1 and Sf1Ss1
(h)
minus03minus02minus01
00010203
(acquirement and calculation)
00 02 04 06 08 10
Interobserver variabilityaverage of 2 raw dataFf1-Ff2Ss1
(i)
Figure 2 Reliability of tissue strain measurement Plots (a) (b) (c) (d) (e) and (f) (per protocol analysis) the Bland-Altman plotsdemonstrate the degree of concordance between the pairs of cervical TSs The region of agreement is included inside the two standarddeviations interval from the mean of differencesThe space included between the zero dotted lines and the mean of differences represents thebiasThe gray band where plotted represents the 95 confidence interval of themean of differences F and S refer to the operator undergoingthe TS calculation f and s refer to the operator undergoing the raw data acquirement where f1 and s1 and f2 and s2 refer respectively to the firstand second raw data sets (a)The intraobserver variability of the TS calculation of the same raw data (Ff1Ff1) is shown (b)The interobservervariability of the TS calculation of the same raw data by the two investigators (Ff1Sf1) is depicted (c) The interobserver variability of the TScalculation of the same raw data (Fs1Ss1) is shown (d) The intraobserver variability of the raw data acquisition and calculation (Ff1-Ff2) isshown (e) The interobserver variability of the raw data acquisition with two raw data sets acquired by different investigators (f and s) andcalculated by the same investigator is presented (Ff1Fs1) (f) The interobserver variability of the raw data acquisition and calculation by thetwo investigators is indicated (Ff1Ss1) Plots (g) (h) and (i) (other analysis) the Bland-Altman plots demonstrate the degree of concordancebetween the pairs of cervical TSs (g) The interobserver variability of the TS calculation in this plot we analyse all data from Figures 2(b)and 2(c) (ie Ff1Sf1 and Fs1Ss1) (h) The interobserver variability of the raw data acquirement the two raw data sets acquired by the twoinvestigators (F and S) aremeasured by the same investigator (Ff1Fs1 and Sf1Ss1) (i)The interobserver variability of the rawdata acquirementand calculation is shown (Ff1-Ff2Ss1 yielding an average of the 2 raw data f1 and f2) In this analysis we took into consideration the averageof the raw data measurements of investigator F versus the TS acquisition and measurement of one raw data set by investigator S
BioMed Research International 7
20 30 40Gestational age (weeks)
02
03
04
05
06
07
08
09
Cer
vica
l TS
rho 082 (CI95 073088)(P le 005)
(a)
20 30 40Gestational age (weeks)
20
30
40
50
60
Cer
vica
l len
gth
(mm
)
rho minus057 (CI95 minus071minus039)(P le 005)
(b)
20 30 40 50 600203040506070809
Cervical length (mm)
Cer
vica
l TS
rho minus059 (CI95 minus072minus042)(P le 005)
(c)
Figure 3 Tissue strain and patientsrsquo clinical features The correlation of TS (average of two raw data set measurements) with the gestationalage and cervical length (rho and 119875 value refer to Pearsonrsquos test)
Table 3 Strain values and parity
N Para = 0 (119899 = 18) N Para ge 1 (119899 = 56) PTS 18 037 (plusmn014) 56 059 (plusmn017) lt005
TS at 12ndash20 weeksrsquo gestation 8 035 (plusmn009) 11 035 (plusmn005) 0900TS at 21ndash29 weeksrsquo gestation 6 029 (plusmn005) 10 049 (plusmn014) lt005TS at 30ndash37 weeksrsquo gestation 3 058 (plusmn015) 16 066 (plusmn011) 0455TS at 38ndash42 weeksrsquo gestation 0 NA 19 073 (plusmn009) NA
Cervical length (mm) 18 4147 (plusmn992) 56 3537 (plusmn996) lt005Cervical length at 12ndash20 weeksrsquo gestation 8 4312 (plusmn1051) 11 4455 (plusmn726) 0748Cervical length at 21ndash29 weeksrsquo gestation 6 4267 (plusmn535) 10 398 (plusmn573) 0334Cervical length at 30ndash37 weeksrsquo gestation 3 3467 (plusmn1563) 16 3293 (plusmn919) 0868Cervical length at 38ndash42 weeksrsquo gestation 0 NA 19 2933 (plusmn902) NA
Tissue strain values related to parity and cervical length Mean (plusmn standard deviation)
Furthermore a high reliability was shown for the TSmea-surements when comparing the three different raw data sets(indicating intra- and interobserver reliability for the wholeprocess of TS measurement) The interobserver reliabilitywas less consistent due to the biases in raw data acquisitionbetween the two operators This difference could be over-come for example by repeating the measurement twice andcalculating the mean TS so that the eventual bias between
operators A and B will disappear These results confirm theimpression that the critical aspect of the TS measurementthat accounts for measurement reliability depends upon theprocess of raw data acquisition
Finally our results were correlated with the clinicalfeatures of the study population Specifically the cervicalTS seems to be related both to patientrsquos gestational ageand to her cervical length and parity Therefore unless the
8 BioMed Research International
relatively small number of patients used here does not allowfor generalisations these results indicate the potential clinicalapplicability of the TDI and TDI-Q tools for the quantitativemeasurement of TS
41 Limitations of the Study A major limitation of theproposed tool is the dependency of TS on the appliedforce during the movement of the cervical compression[14 18] However standardised conditions for the raw dataacquisition (maximal exertion of compression and care inavoiding the dislocation of the cervix) can optimise the TDI-based TS measurements to enhance feasibility and reliabilityTheproblems of themanual compression and unknown valueof the applied force implicate the impossibility to calculate theabsolute value of the elastic module of the cervix but allowedan estimation of the tissue stiffness Recently a manualmethod for cervical stiffness evaluation was proposed basedon the calculation of the anteroposterior cervical diameteranteroposterior 10 cervical diameter measured before (AP)and after (AP1015840) application of pressure on the cervix usingthe transvaginal probe The author describes an excellentintra- and interobserver correlation as well as a betterprediction of preterm delivery compared to the cervicallength measurement [19] Thus even if the technique ofParra measures the strain as Lagrangian strain while in ourprotocol the measure was made using the natural strain themechanism used for strain measurement remains the sameNonetheless comparison among different studies should bedone with caution Indeed for a small deformation thenatural and Lagrangian strains are similar as the Lagrangianand natural strains are interrelated by a fixed mathematicalformula (120576119873(119905) = ln(1 + 120576119871(119905)) but for a larger deformation(as induced in this study) the natural strain will always begreater [17]
The measurement of the stiffness in very short cer-vices can be limited due to the impossibility to direct thecompressing force perpendicularly to the cervical tissueHowever assessing the risk of preterm delivery in an asymp-tomatic patient will be probably more interesting than inpatients with a very ripened cervix which are already knownto be at great increased risk for preterm delivery
Furthermore in order to reduce the number of measure-ments to be performed the feasibility and reliability studywasfirst conducted testing some of these combinations amonga restricted group of patients by a single operator and thentested among thewhole study populationThus even if resultsdemonstrated the high reliability of this tool using the chosenpreset this does not exclude that other settings could workeven better than this Further studies considering this topiccomparing different settings and ROIs positioned in differentregions of the cervix are currently ongoing The clinicalusefulness of this diagnostic tool should be now tested inlarge prospective clinical settings even if preliminary resultsappear to be promising [20]
5 Conclusions
Under standardised conditions for the acquisition of rawdata and strain calculation the TDI-based cervical strain
measurements obtained during pregnancy are feasible andshow high intra- and interoperator reliability The strainmeasurements obtained during the relaxation frame using aDPof 5mmproved to be awell-performingTDI-Q setting forthe cervical TS measurement An objective and quantitativeestimation of cervical stiffness during pregnancy could bevery important for the estimation of preterm delivery riskand could improve assessment of cervical ripening at termto select patients for successful labor induction The clinicalusefulness of this diagnostic tool should be now tested in largeprospective clinical settings
Ethical Approval
The paper was approved by Ethics Committee of the localCollege of Surgeons and themedical Faculty at the Universityof Munster (Reference number 2010-256-f-S)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Authorsrsquo Contribution
A Fruscalzo contributed to conception planning perform-ing the experiments and writing the paper A P Londerocontributed to statistical analysis and cowriting the paperC Frohlich contributed to performing the experiments UMollmann contributed to performing the experiments andR Schmitz contributed to performing the experiments andcowriting the paper
Disclosure
The current address of A Fruscalzo is Obstetrics and Gyne-cology St Franziskus Hospital Hohenzollernring 72 48145Munster Germany
Acknowledgments
The authors thank Dr G Heywinkel (Chief Gynaecolo-gist Mathias-Spital Rheine Germany) Professor M Meyer-Wittkopf (Director of the Prenatal Diagnostic DepartmentMathias-Spital Rheine Germany) W Gorissen (ToshibaMedical Systems Europe Zoetermeer The Netherlands)Professor B Bijnens (ICREA-Universitat Pompeu FabraBarcelona Spain) and S Bertozzi (Clinic of Surgical Semei-otic AOU ldquoS M della Misericordiardquo of Udine Italy) for theirvaluable scientific advice as well as Dr A Dolle and Mr FHassel (Toshiba Medical Systems Neuss Germany) for theirlogistic and technical assistance
References
[1] E H Bishop ldquoPelvic scoring for elective inductionrdquo Obstetricsand Gynecology vol 24 pp 266ndash268 1964
BioMed Research International 9
[2] P Rozenberg ldquoThe secret cervixrdquo Ultrasound in Obstetrics andGynecology vol 32 no 2 pp 126ndash127 2008
[3] M L Palmeri and K R Nightingale ldquoWhat challenges must beovercome before ultrasound elasticity imaging is ready for theclinicrdquo Imaging in Medicine vol 3 no 4 pp 433ndash444 2011
[4] J Ophir I Cespedes H Ponnekanti Y Yazdi and X LildquoElastography a quantitative method for imaging the elasticityof biological tissuesrdquo Ultrasonic Imaging vol 13 no 2 pp 111ndash134 1991
[5] T M Eggeboslash I Oslashkland C Heien L K Gjessing P Romund-stad and K A Salvesen ldquoCan ultrasound measurementsreplace digitally assessed elements of the Bishop scorerdquo ActaObstetricia et Gynecologica Scandinavica vol 88 no 3 pp 325ndash331 2009
[6] G R Sutherland L Hatle P Claus J DrsquoHooge and BH Bijnens Doppler Myocardial Imaging A Textbook BSWKScientific Consulting and Publishing Hasselt Belgium 2006
[7] A Fruscalzo R Schmitz W Klockenbusch and J SteinhardldquoReliability of cervix elastography in late first and secondtrimester of pregnancyrdquo Ultraschall in der Medizin vol 33 no7 pp E101ndashE107 2012
[8] A Fruscalzo J Steinhard A P Londero et al ldquoReliabilityof quantitative elastography of the uterine cervix in at-termpregnanciesrdquo Journal of Perinatal Medicine vol 41 no 4 pp421ndash427 2013
[9] P M Bossuyt J B Reitsma D E Bruns et al ldquoTowards com-plete and accurate reporting of studies of diagnostic accuracythe STARD initiativerdquo Clinical Chemistry vol 49 no 1 pp 1ndash62003
[10] P E Shrout ldquoMeasurement reliability and agreement in psychi-atryrdquo Statistical Methods in Medical Research vol 7 no 3 pp301ndash317 1998
[11] I Tekesin L Hellmeyer G Heller A Romer M Kuhnert andS Schmidt ldquoEvaluation of quantitative ultrasound tissue char-acterization of the cervix and cervical length in the predictionof premature delivery for patients with spontaneous pretermlaborrdquo The American Journal of Obstetrics and Gynecology vol189 no 2 pp 532ndash539 2003
[12] M Swiatkowska-Freund and K Preis ldquoElastography of theuterine cervix implications for success of induction of laborrdquoUltrasound in Obstetrics and Gynecology vol 38 no 1 pp 52ndash56 2011
[13] F S Molina L F Gomez J Florido M C Padilla andK H Nicolaides ldquoQuantification of cervical elastography areproducibility studyrdquoUltrasound in Obstetrics and Gynecologyvol 39 no 6 pp 685ndash689 2012
[14] A Fruscalzo and R Schmitz ldquoQuantitative cervical elastogra-phy in pregnancyrdquoUltrasound inObstetrics andGynecology vol40 no 5 p 612 2012
[15] E Hernandez-Andrade S S Hassan H Ahn et al ldquoEvaluationof cervical stiffness during pregnancy using semiquantitativeultrasound elastographyrdquoUltrasound in Obstetrics and Gynecol-ogy vol 41 no 2 pp 152ndash161 2013
[16] T Fuchs R Woyton M Pomorski et al ldquoSonoelastography ofthe uterine cervix as a newdiagnostic tool of cervical assessmentin pregnant womenmdashpreliminary reportrdquo Ginekologia Polskavol 84 no 1 pp 12ndash16 2013
[17] J DrsquoHooge A Heimdal F Jamal et al ldquoRegional strain andstrain rate measurements by cardiac ultrasound principles
implementation and limitationsrdquo European Journal of Echocar-diography vol 1 no 3 pp 154ndash170 2000
[18] A Fruscalzo and R Schmitz ldquoReplyrdquo Ultrasound in Obstetricsand Gynecology vol 41 no 6 pp 712ndash714 2013
[19] M Parra-Saavedra L Gomez A Barrero G Parra F Vergaraand E Navarro ldquoPrediction of preterm birth using the cervicalconsistency indexrdquo Ultrasound in Obstetrics and Gynecologyvol 38 no 1 pp 44ndash51 2011
[20] A Fruscalzo A P Londero C Fr119894hlich M Meyer-Wittkopfand R Schmitz ldquoQuantitative elastography of cervix for pre-dicting labor induction successrdquo Ultraschall in der Medizin2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 7
20 30 40Gestational age (weeks)
02
03
04
05
06
07
08
09
Cer
vica
l TS
rho 082 (CI95 073088)(P le 005)
(a)
20 30 40Gestational age (weeks)
20
30
40
50
60
Cer
vica
l len
gth
(mm
)
rho minus057 (CI95 minus071minus039)(P le 005)
(b)
20 30 40 50 600203040506070809
Cervical length (mm)
Cer
vica
l TS
rho minus059 (CI95 minus072minus042)(P le 005)
(c)
Figure 3 Tissue strain and patientsrsquo clinical features The correlation of TS (average of two raw data set measurements) with the gestationalage and cervical length (rho and 119875 value refer to Pearsonrsquos test)
Table 3 Strain values and parity
N Para = 0 (119899 = 18) N Para ge 1 (119899 = 56) PTS 18 037 (plusmn014) 56 059 (plusmn017) lt005
TS at 12ndash20 weeksrsquo gestation 8 035 (plusmn009) 11 035 (plusmn005) 0900TS at 21ndash29 weeksrsquo gestation 6 029 (plusmn005) 10 049 (plusmn014) lt005TS at 30ndash37 weeksrsquo gestation 3 058 (plusmn015) 16 066 (plusmn011) 0455TS at 38ndash42 weeksrsquo gestation 0 NA 19 073 (plusmn009) NA
Cervical length (mm) 18 4147 (plusmn992) 56 3537 (plusmn996) lt005Cervical length at 12ndash20 weeksrsquo gestation 8 4312 (plusmn1051) 11 4455 (plusmn726) 0748Cervical length at 21ndash29 weeksrsquo gestation 6 4267 (plusmn535) 10 398 (plusmn573) 0334Cervical length at 30ndash37 weeksrsquo gestation 3 3467 (plusmn1563) 16 3293 (plusmn919) 0868Cervical length at 38ndash42 weeksrsquo gestation 0 NA 19 2933 (plusmn902) NA
Tissue strain values related to parity and cervical length Mean (plusmn standard deviation)
Furthermore a high reliability was shown for the TSmea-surements when comparing the three different raw data sets(indicating intra- and interobserver reliability for the wholeprocess of TS measurement) The interobserver reliabilitywas less consistent due to the biases in raw data acquisitionbetween the two operators This difference could be over-come for example by repeating the measurement twice andcalculating the mean TS so that the eventual bias between
operators A and B will disappear These results confirm theimpression that the critical aspect of the TS measurementthat accounts for measurement reliability depends upon theprocess of raw data acquisition
Finally our results were correlated with the clinicalfeatures of the study population Specifically the cervicalTS seems to be related both to patientrsquos gestational ageand to her cervical length and parity Therefore unless the
8 BioMed Research International
relatively small number of patients used here does not allowfor generalisations these results indicate the potential clinicalapplicability of the TDI and TDI-Q tools for the quantitativemeasurement of TS
41 Limitations of the Study A major limitation of theproposed tool is the dependency of TS on the appliedforce during the movement of the cervical compression[14 18] However standardised conditions for the raw dataacquisition (maximal exertion of compression and care inavoiding the dislocation of the cervix) can optimise the TDI-based TS measurements to enhance feasibility and reliabilityTheproblems of themanual compression and unknown valueof the applied force implicate the impossibility to calculate theabsolute value of the elastic module of the cervix but allowedan estimation of the tissue stiffness Recently a manualmethod for cervical stiffness evaluation was proposed basedon the calculation of the anteroposterior cervical diameteranteroposterior 10 cervical diameter measured before (AP)and after (AP1015840) application of pressure on the cervix usingthe transvaginal probe The author describes an excellentintra- and interobserver correlation as well as a betterprediction of preterm delivery compared to the cervicallength measurement [19] Thus even if the technique ofParra measures the strain as Lagrangian strain while in ourprotocol the measure was made using the natural strain themechanism used for strain measurement remains the sameNonetheless comparison among different studies should bedone with caution Indeed for a small deformation thenatural and Lagrangian strains are similar as the Lagrangianand natural strains are interrelated by a fixed mathematicalformula (120576119873(119905) = ln(1 + 120576119871(119905)) but for a larger deformation(as induced in this study) the natural strain will always begreater [17]
The measurement of the stiffness in very short cer-vices can be limited due to the impossibility to direct thecompressing force perpendicularly to the cervical tissueHowever assessing the risk of preterm delivery in an asymp-tomatic patient will be probably more interesting than inpatients with a very ripened cervix which are already knownto be at great increased risk for preterm delivery
Furthermore in order to reduce the number of measure-ments to be performed the feasibility and reliability studywasfirst conducted testing some of these combinations amonga restricted group of patients by a single operator and thentested among thewhole study populationThus even if resultsdemonstrated the high reliability of this tool using the chosenpreset this does not exclude that other settings could workeven better than this Further studies considering this topiccomparing different settings and ROIs positioned in differentregions of the cervix are currently ongoing The clinicalusefulness of this diagnostic tool should be now tested inlarge prospective clinical settings even if preliminary resultsappear to be promising [20]
5 Conclusions
Under standardised conditions for the acquisition of rawdata and strain calculation the TDI-based cervical strain
measurements obtained during pregnancy are feasible andshow high intra- and interoperator reliability The strainmeasurements obtained during the relaxation frame using aDPof 5mmproved to be awell-performingTDI-Q setting forthe cervical TS measurement An objective and quantitativeestimation of cervical stiffness during pregnancy could bevery important for the estimation of preterm delivery riskand could improve assessment of cervical ripening at termto select patients for successful labor induction The clinicalusefulness of this diagnostic tool should be now tested in largeprospective clinical settings
Ethical Approval
The paper was approved by Ethics Committee of the localCollege of Surgeons and themedical Faculty at the Universityof Munster (Reference number 2010-256-f-S)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Authorsrsquo Contribution
A Fruscalzo contributed to conception planning perform-ing the experiments and writing the paper A P Londerocontributed to statistical analysis and cowriting the paperC Frohlich contributed to performing the experiments UMollmann contributed to performing the experiments andR Schmitz contributed to performing the experiments andcowriting the paper
Disclosure
The current address of A Fruscalzo is Obstetrics and Gyne-cology St Franziskus Hospital Hohenzollernring 72 48145Munster Germany
Acknowledgments
The authors thank Dr G Heywinkel (Chief Gynaecolo-gist Mathias-Spital Rheine Germany) Professor M Meyer-Wittkopf (Director of the Prenatal Diagnostic DepartmentMathias-Spital Rheine Germany) W Gorissen (ToshibaMedical Systems Europe Zoetermeer The Netherlands)Professor B Bijnens (ICREA-Universitat Pompeu FabraBarcelona Spain) and S Bertozzi (Clinic of Surgical Semei-otic AOU ldquoS M della Misericordiardquo of Udine Italy) for theirvaluable scientific advice as well as Dr A Dolle and Mr FHassel (Toshiba Medical Systems Neuss Germany) for theirlogistic and technical assistance
References
[1] E H Bishop ldquoPelvic scoring for elective inductionrdquo Obstetricsand Gynecology vol 24 pp 266ndash268 1964
BioMed Research International 9
[2] P Rozenberg ldquoThe secret cervixrdquo Ultrasound in Obstetrics andGynecology vol 32 no 2 pp 126ndash127 2008
[3] M L Palmeri and K R Nightingale ldquoWhat challenges must beovercome before ultrasound elasticity imaging is ready for theclinicrdquo Imaging in Medicine vol 3 no 4 pp 433ndash444 2011
[4] J Ophir I Cespedes H Ponnekanti Y Yazdi and X LildquoElastography a quantitative method for imaging the elasticityof biological tissuesrdquo Ultrasonic Imaging vol 13 no 2 pp 111ndash134 1991
[5] T M Eggeboslash I Oslashkland C Heien L K Gjessing P Romund-stad and K A Salvesen ldquoCan ultrasound measurementsreplace digitally assessed elements of the Bishop scorerdquo ActaObstetricia et Gynecologica Scandinavica vol 88 no 3 pp 325ndash331 2009
[6] G R Sutherland L Hatle P Claus J DrsquoHooge and BH Bijnens Doppler Myocardial Imaging A Textbook BSWKScientific Consulting and Publishing Hasselt Belgium 2006
[7] A Fruscalzo R Schmitz W Klockenbusch and J SteinhardldquoReliability of cervix elastography in late first and secondtrimester of pregnancyrdquo Ultraschall in der Medizin vol 33 no7 pp E101ndashE107 2012
[8] A Fruscalzo J Steinhard A P Londero et al ldquoReliabilityof quantitative elastography of the uterine cervix in at-termpregnanciesrdquo Journal of Perinatal Medicine vol 41 no 4 pp421ndash427 2013
[9] P M Bossuyt J B Reitsma D E Bruns et al ldquoTowards com-plete and accurate reporting of studies of diagnostic accuracythe STARD initiativerdquo Clinical Chemistry vol 49 no 1 pp 1ndash62003
[10] P E Shrout ldquoMeasurement reliability and agreement in psychi-atryrdquo Statistical Methods in Medical Research vol 7 no 3 pp301ndash317 1998
[11] I Tekesin L Hellmeyer G Heller A Romer M Kuhnert andS Schmidt ldquoEvaluation of quantitative ultrasound tissue char-acterization of the cervix and cervical length in the predictionof premature delivery for patients with spontaneous pretermlaborrdquo The American Journal of Obstetrics and Gynecology vol189 no 2 pp 532ndash539 2003
[12] M Swiatkowska-Freund and K Preis ldquoElastography of theuterine cervix implications for success of induction of laborrdquoUltrasound in Obstetrics and Gynecology vol 38 no 1 pp 52ndash56 2011
[13] F S Molina L F Gomez J Florido M C Padilla andK H Nicolaides ldquoQuantification of cervical elastography areproducibility studyrdquoUltrasound in Obstetrics and Gynecologyvol 39 no 6 pp 685ndash689 2012
[14] A Fruscalzo and R Schmitz ldquoQuantitative cervical elastogra-phy in pregnancyrdquoUltrasound inObstetrics andGynecology vol40 no 5 p 612 2012
[15] E Hernandez-Andrade S S Hassan H Ahn et al ldquoEvaluationof cervical stiffness during pregnancy using semiquantitativeultrasound elastographyrdquoUltrasound in Obstetrics and Gynecol-ogy vol 41 no 2 pp 152ndash161 2013
[16] T Fuchs R Woyton M Pomorski et al ldquoSonoelastography ofthe uterine cervix as a newdiagnostic tool of cervical assessmentin pregnant womenmdashpreliminary reportrdquo Ginekologia Polskavol 84 no 1 pp 12ndash16 2013
[17] J DrsquoHooge A Heimdal F Jamal et al ldquoRegional strain andstrain rate measurements by cardiac ultrasound principles
implementation and limitationsrdquo European Journal of Echocar-diography vol 1 no 3 pp 154ndash170 2000
[18] A Fruscalzo and R Schmitz ldquoReplyrdquo Ultrasound in Obstetricsand Gynecology vol 41 no 6 pp 712ndash714 2013
[19] M Parra-Saavedra L Gomez A Barrero G Parra F Vergaraand E Navarro ldquoPrediction of preterm birth using the cervicalconsistency indexrdquo Ultrasound in Obstetrics and Gynecologyvol 38 no 1 pp 44ndash51 2011
[20] A Fruscalzo A P Londero C Fr119894hlich M Meyer-Wittkopfand R Schmitz ldquoQuantitative elastography of cervix for pre-dicting labor induction successrdquo Ultraschall in der Medizin2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 BioMed Research International
relatively small number of patients used here does not allowfor generalisations these results indicate the potential clinicalapplicability of the TDI and TDI-Q tools for the quantitativemeasurement of TS
41 Limitations of the Study A major limitation of theproposed tool is the dependency of TS on the appliedforce during the movement of the cervical compression[14 18] However standardised conditions for the raw dataacquisition (maximal exertion of compression and care inavoiding the dislocation of the cervix) can optimise the TDI-based TS measurements to enhance feasibility and reliabilityTheproblems of themanual compression and unknown valueof the applied force implicate the impossibility to calculate theabsolute value of the elastic module of the cervix but allowedan estimation of the tissue stiffness Recently a manualmethod for cervical stiffness evaluation was proposed basedon the calculation of the anteroposterior cervical diameteranteroposterior 10 cervical diameter measured before (AP)and after (AP1015840) application of pressure on the cervix usingthe transvaginal probe The author describes an excellentintra- and interobserver correlation as well as a betterprediction of preterm delivery compared to the cervicallength measurement [19] Thus even if the technique ofParra measures the strain as Lagrangian strain while in ourprotocol the measure was made using the natural strain themechanism used for strain measurement remains the sameNonetheless comparison among different studies should bedone with caution Indeed for a small deformation thenatural and Lagrangian strains are similar as the Lagrangianand natural strains are interrelated by a fixed mathematicalformula (120576119873(119905) = ln(1 + 120576119871(119905)) but for a larger deformation(as induced in this study) the natural strain will always begreater [17]
The measurement of the stiffness in very short cer-vices can be limited due to the impossibility to direct thecompressing force perpendicularly to the cervical tissueHowever assessing the risk of preterm delivery in an asymp-tomatic patient will be probably more interesting than inpatients with a very ripened cervix which are already knownto be at great increased risk for preterm delivery
Furthermore in order to reduce the number of measure-ments to be performed the feasibility and reliability studywasfirst conducted testing some of these combinations amonga restricted group of patients by a single operator and thentested among thewhole study populationThus even if resultsdemonstrated the high reliability of this tool using the chosenpreset this does not exclude that other settings could workeven better than this Further studies considering this topiccomparing different settings and ROIs positioned in differentregions of the cervix are currently ongoing The clinicalusefulness of this diagnostic tool should be now tested inlarge prospective clinical settings even if preliminary resultsappear to be promising [20]
5 Conclusions
Under standardised conditions for the acquisition of rawdata and strain calculation the TDI-based cervical strain
measurements obtained during pregnancy are feasible andshow high intra- and interoperator reliability The strainmeasurements obtained during the relaxation frame using aDPof 5mmproved to be awell-performingTDI-Q setting forthe cervical TS measurement An objective and quantitativeestimation of cervical stiffness during pregnancy could bevery important for the estimation of preterm delivery riskand could improve assessment of cervical ripening at termto select patients for successful labor induction The clinicalusefulness of this diagnostic tool should be now tested in largeprospective clinical settings
Ethical Approval
The paper was approved by Ethics Committee of the localCollege of Surgeons and themedical Faculty at the Universityof Munster (Reference number 2010-256-f-S)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Authorsrsquo Contribution
A Fruscalzo contributed to conception planning perform-ing the experiments and writing the paper A P Londerocontributed to statistical analysis and cowriting the paperC Frohlich contributed to performing the experiments UMollmann contributed to performing the experiments andR Schmitz contributed to performing the experiments andcowriting the paper
Disclosure
The current address of A Fruscalzo is Obstetrics and Gyne-cology St Franziskus Hospital Hohenzollernring 72 48145Munster Germany
Acknowledgments
The authors thank Dr G Heywinkel (Chief Gynaecolo-gist Mathias-Spital Rheine Germany) Professor M Meyer-Wittkopf (Director of the Prenatal Diagnostic DepartmentMathias-Spital Rheine Germany) W Gorissen (ToshibaMedical Systems Europe Zoetermeer The Netherlands)Professor B Bijnens (ICREA-Universitat Pompeu FabraBarcelona Spain) and S Bertozzi (Clinic of Surgical Semei-otic AOU ldquoS M della Misericordiardquo of Udine Italy) for theirvaluable scientific advice as well as Dr A Dolle and Mr FHassel (Toshiba Medical Systems Neuss Germany) for theirlogistic and technical assistance
References
[1] E H Bishop ldquoPelvic scoring for elective inductionrdquo Obstetricsand Gynecology vol 24 pp 266ndash268 1964
BioMed Research International 9
[2] P Rozenberg ldquoThe secret cervixrdquo Ultrasound in Obstetrics andGynecology vol 32 no 2 pp 126ndash127 2008
[3] M L Palmeri and K R Nightingale ldquoWhat challenges must beovercome before ultrasound elasticity imaging is ready for theclinicrdquo Imaging in Medicine vol 3 no 4 pp 433ndash444 2011
[4] J Ophir I Cespedes H Ponnekanti Y Yazdi and X LildquoElastography a quantitative method for imaging the elasticityof biological tissuesrdquo Ultrasonic Imaging vol 13 no 2 pp 111ndash134 1991
[5] T M Eggeboslash I Oslashkland C Heien L K Gjessing P Romund-stad and K A Salvesen ldquoCan ultrasound measurementsreplace digitally assessed elements of the Bishop scorerdquo ActaObstetricia et Gynecologica Scandinavica vol 88 no 3 pp 325ndash331 2009
[6] G R Sutherland L Hatle P Claus J DrsquoHooge and BH Bijnens Doppler Myocardial Imaging A Textbook BSWKScientific Consulting and Publishing Hasselt Belgium 2006
[7] A Fruscalzo R Schmitz W Klockenbusch and J SteinhardldquoReliability of cervix elastography in late first and secondtrimester of pregnancyrdquo Ultraschall in der Medizin vol 33 no7 pp E101ndashE107 2012
[8] A Fruscalzo J Steinhard A P Londero et al ldquoReliabilityof quantitative elastography of the uterine cervix in at-termpregnanciesrdquo Journal of Perinatal Medicine vol 41 no 4 pp421ndash427 2013
[9] P M Bossuyt J B Reitsma D E Bruns et al ldquoTowards com-plete and accurate reporting of studies of diagnostic accuracythe STARD initiativerdquo Clinical Chemistry vol 49 no 1 pp 1ndash62003
[10] P E Shrout ldquoMeasurement reliability and agreement in psychi-atryrdquo Statistical Methods in Medical Research vol 7 no 3 pp301ndash317 1998
[11] I Tekesin L Hellmeyer G Heller A Romer M Kuhnert andS Schmidt ldquoEvaluation of quantitative ultrasound tissue char-acterization of the cervix and cervical length in the predictionof premature delivery for patients with spontaneous pretermlaborrdquo The American Journal of Obstetrics and Gynecology vol189 no 2 pp 532ndash539 2003
[12] M Swiatkowska-Freund and K Preis ldquoElastography of theuterine cervix implications for success of induction of laborrdquoUltrasound in Obstetrics and Gynecology vol 38 no 1 pp 52ndash56 2011
[13] F S Molina L F Gomez J Florido M C Padilla andK H Nicolaides ldquoQuantification of cervical elastography areproducibility studyrdquoUltrasound in Obstetrics and Gynecologyvol 39 no 6 pp 685ndash689 2012
[14] A Fruscalzo and R Schmitz ldquoQuantitative cervical elastogra-phy in pregnancyrdquoUltrasound inObstetrics andGynecology vol40 no 5 p 612 2012
[15] E Hernandez-Andrade S S Hassan H Ahn et al ldquoEvaluationof cervical stiffness during pregnancy using semiquantitativeultrasound elastographyrdquoUltrasound in Obstetrics and Gynecol-ogy vol 41 no 2 pp 152ndash161 2013
[16] T Fuchs R Woyton M Pomorski et al ldquoSonoelastography ofthe uterine cervix as a newdiagnostic tool of cervical assessmentin pregnant womenmdashpreliminary reportrdquo Ginekologia Polskavol 84 no 1 pp 12ndash16 2013
[17] J DrsquoHooge A Heimdal F Jamal et al ldquoRegional strain andstrain rate measurements by cardiac ultrasound principles
implementation and limitationsrdquo European Journal of Echocar-diography vol 1 no 3 pp 154ndash170 2000
[18] A Fruscalzo and R Schmitz ldquoReplyrdquo Ultrasound in Obstetricsand Gynecology vol 41 no 6 pp 712ndash714 2013
[19] M Parra-Saavedra L Gomez A Barrero G Parra F Vergaraand E Navarro ldquoPrediction of preterm birth using the cervicalconsistency indexrdquo Ultrasound in Obstetrics and Gynecologyvol 38 no 1 pp 44ndash51 2011
[20] A Fruscalzo A P Londero C Fr119894hlich M Meyer-Wittkopfand R Schmitz ldquoQuantitative elastography of cervix for pre-dicting labor induction successrdquo Ultraschall in der Medizin2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 9
[2] P Rozenberg ldquoThe secret cervixrdquo Ultrasound in Obstetrics andGynecology vol 32 no 2 pp 126ndash127 2008
[3] M L Palmeri and K R Nightingale ldquoWhat challenges must beovercome before ultrasound elasticity imaging is ready for theclinicrdquo Imaging in Medicine vol 3 no 4 pp 433ndash444 2011
[4] J Ophir I Cespedes H Ponnekanti Y Yazdi and X LildquoElastography a quantitative method for imaging the elasticityof biological tissuesrdquo Ultrasonic Imaging vol 13 no 2 pp 111ndash134 1991
[5] T M Eggeboslash I Oslashkland C Heien L K Gjessing P Romund-stad and K A Salvesen ldquoCan ultrasound measurementsreplace digitally assessed elements of the Bishop scorerdquo ActaObstetricia et Gynecologica Scandinavica vol 88 no 3 pp 325ndash331 2009
[6] G R Sutherland L Hatle P Claus J DrsquoHooge and BH Bijnens Doppler Myocardial Imaging A Textbook BSWKScientific Consulting and Publishing Hasselt Belgium 2006
[7] A Fruscalzo R Schmitz W Klockenbusch and J SteinhardldquoReliability of cervix elastography in late first and secondtrimester of pregnancyrdquo Ultraschall in der Medizin vol 33 no7 pp E101ndashE107 2012
[8] A Fruscalzo J Steinhard A P Londero et al ldquoReliabilityof quantitative elastography of the uterine cervix in at-termpregnanciesrdquo Journal of Perinatal Medicine vol 41 no 4 pp421ndash427 2013
[9] P M Bossuyt J B Reitsma D E Bruns et al ldquoTowards com-plete and accurate reporting of studies of diagnostic accuracythe STARD initiativerdquo Clinical Chemistry vol 49 no 1 pp 1ndash62003
[10] P E Shrout ldquoMeasurement reliability and agreement in psychi-atryrdquo Statistical Methods in Medical Research vol 7 no 3 pp301ndash317 1998
[11] I Tekesin L Hellmeyer G Heller A Romer M Kuhnert andS Schmidt ldquoEvaluation of quantitative ultrasound tissue char-acterization of the cervix and cervical length in the predictionof premature delivery for patients with spontaneous pretermlaborrdquo The American Journal of Obstetrics and Gynecology vol189 no 2 pp 532ndash539 2003
[12] M Swiatkowska-Freund and K Preis ldquoElastography of theuterine cervix implications for success of induction of laborrdquoUltrasound in Obstetrics and Gynecology vol 38 no 1 pp 52ndash56 2011
[13] F S Molina L F Gomez J Florido M C Padilla andK H Nicolaides ldquoQuantification of cervical elastography areproducibility studyrdquoUltrasound in Obstetrics and Gynecologyvol 39 no 6 pp 685ndash689 2012
[14] A Fruscalzo and R Schmitz ldquoQuantitative cervical elastogra-phy in pregnancyrdquoUltrasound inObstetrics andGynecology vol40 no 5 p 612 2012
[15] E Hernandez-Andrade S S Hassan H Ahn et al ldquoEvaluationof cervical stiffness during pregnancy using semiquantitativeultrasound elastographyrdquoUltrasound in Obstetrics and Gynecol-ogy vol 41 no 2 pp 152ndash161 2013
[16] T Fuchs R Woyton M Pomorski et al ldquoSonoelastography ofthe uterine cervix as a newdiagnostic tool of cervical assessmentin pregnant womenmdashpreliminary reportrdquo Ginekologia Polskavol 84 no 1 pp 12ndash16 2013
[17] J DrsquoHooge A Heimdal F Jamal et al ldquoRegional strain andstrain rate measurements by cardiac ultrasound principles
implementation and limitationsrdquo European Journal of Echocar-diography vol 1 no 3 pp 154ndash170 2000
[18] A Fruscalzo and R Schmitz ldquoReplyrdquo Ultrasound in Obstetricsand Gynecology vol 41 no 6 pp 712ndash714 2013
[19] M Parra-Saavedra L Gomez A Barrero G Parra F Vergaraand E Navarro ldquoPrediction of preterm birth using the cervicalconsistency indexrdquo Ultrasound in Obstetrics and Gynecologyvol 38 no 1 pp 44ndash51 2011
[20] A Fruscalzo A P Londero C Fr119894hlich M Meyer-Wittkopfand R Schmitz ldquoQuantitative elastography of cervix for pre-dicting labor induction successrdquo Ultraschall in der Medizin2014
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom


![Research Associate (Part-Time) [Fixed Term]measure tissue perfusion and MR elastography (to measure tissue stiffness). The aim of advancing imaging technologies and applications draws](https://static.fdocuments.us/doc/165x107/5f8c41ab2fd7220f220cda34/research-associate-part-time-fixed-term-measure-tissue-perfusion-and-mr-elastography.jpg)

![Regional Quantification of Myocardial Stiffness Using MR ... · Regional Quantification of Myocardial Stiffness Using MR Elastography ... the infarcts were allowed to fibrose [4]](https://static.fdocuments.us/doc/165x107/5be6eed209d3f247448dd51f/regional-quantification-of-myocardial-stiffness-using-mr-regional-quantification.jpg)