Clinical Study Growth Arrest Specific Gene 6 Protein...
8
Hindawi Publishing Corporation Mediators of Inflammation Volume 2013, Article ID 406483, 7 pages http://dx.doi.org/10.1155/2013/406483 Clinical Study Growth Arrest Specific Gene 6 Protein Concentration in Cerebrospinal Fluid Correlates with Relapse Severity in Multiple Sclerosis P. P. Sainaghi, 1,2 L. Collimedaglia, 3 F. Alciato, 3 R. Molinari, 3 D. Sola, 3 E. Ranza, 3 P. Naldi, 3 F. Monaco, 2,3 M. Leone, 1,3 M. Pirisi, 2,3 and G. C. Avanzi 2,3 1 AOU “Maggiore della Carit` a,” 28100 Novara, Italy 2 (Interdisciplinary Research Center of Autoimmune Diseases) IRCAD, Via Solaroli 17, 28100 Novara, Italy 3 Department of Translational Medicine, “A. Avogadro” University, 28100 Novara, Italy Correspondence should be addressed to P. P. Sainaghi; [email protected] Received 29 January 2013; Revised 8 April 2013; Accepted 22 April 2013 Academic Editor: Carmen Guaza Copyright © 2013 P. P. Sainaghi et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. Growth arrest specific gene 6 (Gas6) protein enhances survival of oligodendrocytes and neurons, and it is involved in autoimmunity. erefore, we aimed to verify whether cerebrospinal-fluid (CSF) Gas6 concentration may represent a biomarker of disease activity in multiple sclerosis. Methods. Sixty-five patients who underwent a spinal tap during relapse of relapsing/remitting multiple sclerosis (RR-MS)(McDonald-criteria) were studied. Forty patients affected by noninflammatory/nonautoimmune neurological diseases served as controls. Relapse was defined according to Schumacher criteria. Symptoms were grouped according to Kurtzke-Functional System (FS). Clinical characteristics of the relapse, duration, Expanded-Disability-Status Scale (EDSS) change, number of FS involved, completeness of recovery, age, steroid therapy, were categorised. Patients were followed at 6-month intervals to assess relapse rate and EDSS progression. Gas6 was measured (CSF, plasma) by in-house-enzyme-linked immunoassay (ELISA). Results. Higher CSF Gas6 concentrations were observed in relapses lasting ≤60 days (8.7 ± 3.9 ng/mL) versus >60 days (6.5 ± 2.6) or controls (6.5 ± 2.4; = 0.05), with ≤2 FS involved (8.5 ± 3.8) versus >2 FS (5.6 ± 2.5) ( < 0.05) and EDSS change ≤2.5 points (8.8 ± 3.7) versus >2.5 (6.5 ± 3.5) ( = 0.04). Conversely, CSF Gas6 was not predictive of the completeness of recovery. Plasma and CSF concentrations were not related ( 2 = 0.0003), and neither were predictive of relapse rate or EDSS progression aſter first relapse. Conclusions. CSF concentration of Gas6 is inversely correlated with the severity of relapse in RR-MS patients but does not predict the subsequent course of the disease. 1. Introduction Multiple sclerosis (MS) is an immune-mediated disor- der of the central nervous system (CNS) determined by an inflammatory aggression to the myelin of neuronal fibers. e pathogenesis of MS involves complex interac- tions between many cell types, including both the adap- tive and innate immune systems. In this context, activated macrophages and microglial cells mediate myelin degrada- tion and oligodendrocyte damage by producing proinflam- matory cytokines such as tumor necrosis factor- (TNF-) alpha and interferon-gamma [1]. For this reason, molecules involved in dampening of macrophages activation could be involved in MS pathogenesis. Gas6 (growth arrest specific 6), a multimodular secreted protein, binds and activates receptors belonging to the Tyro- 3 tyrosine kinase receptor family (Tyro-3, Axl, and Mer) also known as TAM receptors [2–5]. Gas6/TAM interaction is involved in several physiological processes, including cell migration, adhesion, cell growth, and survival [6]. Recently, it has been claimed that Gas6/TAM system may be involved in the pathogenesis of autoimmune diseases [7]. is hypoth- esis is based on the observation that knock-out mice for TAM receptors display aberrant proliferation of T and B
Transcript of Clinical Study Growth Arrest Specific Gene 6 Protein...
Hindawi Publishing CorporationMediators of InflammationVolume 2013 Article ID 406483 7 pageshttpdxdoiorg1011552013406483
Clinical StudyGrowth Arrest Specific Gene 6 Protein Concentration inCerebrospinal Fluid Correlates with Relapse Severity inMultiple Sclerosis
P P Sainaghi12 L Collimedaglia3 F Alciato3 R Molinari3 D Sola3 E Ranza3 P Naldi3
F Monaco23 M Leone13 M Pirisi23 and G C Avanzi23
1 AOU ldquoMaggiore della Caritardquo 28100 Novara Italy2 (Interdisciplinary Research Center of Autoimmune Diseases) IRCAD Via Solaroli 17 28100 Novara Italy3 Department of Translational Medicine ldquoA Avogadrordquo University 28100 Novara Italy
Correspondence should be addressed to P P Sainaghi sainaghimedunipmnit
Received 29 January 2013 Revised 8 April 2013 Accepted 22 April 2013
Academic Editor Carmen Guaza
Copyright copy 2013 P P Sainaghi et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Background Growth arrest specific gene 6 (Gas6) protein enhances survival of oligodendrocytes and neurons and it is involved inautoimmunity Therefore we aimed to verify whether cerebrospinal-fluid (CSF) Gas6 concentration may represent a biomarker ofdisease activity in multiple sclerosisMethods Sixty-five patients who underwent a spinal tap during relapse of relapsingremittingmultiple sclerosis (RR-MS)(McDonald-criteria) were studied Forty patients affected by noninflammatorynonautoimmuneneurological diseases served as controls Relapse was defined according to Schumacher criteria Symptoms were grouped accordingto Kurtzke-Functional System (FS) Clinical characteristics of the relapse duration Expanded-Disability-Status Scale (EDSS)change number of FS involved completeness of recovery age steroid therapy were categorised Patients were followed at 6-monthintervals to assess relapse rate and EDSS progression Gas6 was measured (CSF plasma) by in-house-enzyme-linked immunoassay(ELISA) Results Higher CSF Gas6 concentrations were observed in relapses lasting le60 days (87 plusmn 39 ngmL) versus gt60 days(65 plusmn 26) or controls (65 plusmn 24 119875 = 005) with le2 FS involved (85 plusmn 38) versus gt2 FS (56 plusmn 25) (119875 lt 005) and EDSS changele25 points (88 plusmn 37) versus gt25 (65 plusmn 35) (119875 = 004) Conversely CSF Gas6 was not predictive of the completeness of recoveryPlasma and CSF concentrations were not related (1198772 = 00003) and neither were predictive of relapse rate or EDSS progressionafter first relapse Conclusions CSF concentration of Gas6 is inversely correlated with the severity of relapse in RR-MS patients butdoes not predict the subsequent course of the disease
1 Introduction
Multiple sclerosis (MS) is an immune-mediated disor-der of the central nervous system (CNS) determined byan inflammatory aggression to the myelin of neuronalfibers The pathogenesis of MS involves complex interac-tions between many cell types including both the adap-tive and innate immune systems In this context activatedmacrophages and microglial cells mediate myelin degrada-tion and oligodendrocyte damage by producing proinflam-matory cytokines such as tumor necrosis factor- (TNF-)alpha and interferon-gamma [1] For this reason molecules
involved in dampening of macrophages activation could beinvolved in MS pathogenesis
Gas6 (growth arrest specific 6) a multimodular secretedprotein binds and activates receptors belonging to the Tyro-3 tyrosine kinase receptor family (Tyro-3 Axl and Mer)also known as TAM receptors [2ndash5] Gas6TAM interactionis involved in several physiological processes including cellmigration adhesion cell growth and survival [6] Recentlyit has been claimed that Gas6TAM system may be involvedin the pathogenesis of autoimmune diseases [7]This hypoth-esis is based on the observation that knock-out mice forTAM receptors display aberrant proliferation of T and B
2 Mediators of Inflammation
lymphocytes with diffuse tissue infiltration and autoimmunemanifestations including vasculitis lupus-like lesions andautoantibodies This phenotype is likely the consequence ofmonocytes-macrophages hyperactivity [8] The importanceof Gas6 in controlling the immune response is supportedby the finding that Gas6 inhibits macrophage activation andcytokine production reducing interleukin (IL)-6 and TNF-alpha secretion through the activation of Mer receptors [9]
Direct evidences link Gas6 to autoimmune processeswithin the central nervous system (CNS) Gas6 and its TAMreceptors are expressed in the brain of embryonic and adultrats proportionally to synaptogenesis of cerebral tissues [10ndash12] In addition Gas6 promotes proliferative and antiapop-totic effects on several CNS cell types as hippocampal andcortical neurons [11 13] Schwann cells [14] and in particularoligodendrocytes which are protected from apoptosis troughAxlPI3-KAkt activation [15 16] Binder and colleagues havealso shown that the absence of Gas6 affects the efficiency ofremyelination following a demyelinating insult induced bycuprizone and that defect of remyelination is accompaniedto reduction in the number of mature oligodendrocytes [17]moreover the administration of recombinant human Gas6to the corpus callosum enhanced the myelin repair in thesame mouse model [18] These observations suggest that theGas6TAM system may be involved both in the regulationof the survival of neuronal and glial cells in particularof those involved in myelination and the control of theinnate immune response two paramount processes in MSpathogenesis Based on these premises in the present studywe measured CSF and plasma Gas6 protein during a relapseof multiple sclerosis in relation to relapse clinical features andseverity scores as Kurtzke-Functional-System (FS) to verifytheir usefulness as a biomarker of disease course
2 Methods
21 Patients Sixty-five consecutive patients admitted to anacademic referral centre from 2001 to 2005 with a diagnosisof clinically isolated syndrome (CIS) or Relapsing-Remitting(RR) MS were studied CIS was defined as the occurrenceof an acute or subacute event of the CNS affecting the opticnerves brainstem or spinal cord of presumed inflammatorydemyelinating origin in a patient with no history suggestiveof an earlier demyelinating episode [19] McDonald criteria[20]were used to diagnoseMS Inclusion criteriawere agege18years first visit to theMSCentre diagnostic lumbar punctureduring the relapse no treatment with corticosteroids priorto the lumbar puncture and no prior treatment with anyimmunomodulant drug Patients with primary progressiveMS were excluded The majority of patients (119899 = 45) weresampled during their first relapse the others were observedand sampled at their second (119899 = 16) or third relapse (119899 = 4)moreover at sampling 22 were CIS and 43 RR-MS After thefirst visit 55 patients (10 patients were lost to follow-up) wereprospectively followed and visited thereafter every 6 monthsthe follow-up ended on July 31 2009 (Table 1) Follow-upduration ranged from 25 to 11 years (mean 59 years SD 18)At the end of this follow-up period the diagnosis was CIS in
Table 1 Features of the population studied
Population studied Number of patientsFirst relapsesecondthird relapse 45164CISRR-MS 2243Patients with follow-up ge25 years 55CIS clinically isolated syndrome RR-MS relapsing remitting multiplesclerosis
9 cases and RR-MS in 42 while 4 patients had already enteredsecondary progression
The study was approved by a local Ethical Committeeand conducted in strict accordance with principles of theDeclaration of Helsinki Each patient gave a written informedconsent before the lumbar puncture to the use of hisher CSFfor experimental evaluation and to maintain data in the data-base
22 Relapse Definition and Evaluation Relapse was definedas ldquoacute or subacute occurrence recurrence or worseningof symptoms of neurologic dysfunction attributable to MSlasting more than 24 hours after a period of at least 30 daysof improvement or stabilityrdquo [21] Neurological deteriorationof preexisting symptoms accompanied by fever was notconsidered a relapse Paroxysmal episodes were consideredas relapse when multiple and occurring over not less than 24hours Symptoms occurring within a month after the initialsymptoms of relapse were considered to be part of the sameepisode Patients data were collected at the first visit at thecentre during the relapse and also at 3 7 and 30 days after therelapse onset For each relapse type of symptoms signs anddates of occurrence were collected as previously described[22] Briefly symptoms and signs were grouped to fit in withthe Kurtzke Functional System (FS) [23] The score for eachFS and the total EDSS score were calculated at onset atmaximum worsening (zenith) and at the first examinationafter the day of maximum improvement of the relapse Wecorrelated the following factors with Gas6 concentrationrelapse duration and severity recovery gender age at theonset of the relapse number of affected FSs Link index(le070gt070) annualized relapse rate and annualized EDSSprogression The relapse duration was calculated as the timebetween the date of onset of the first symptom and the dateof maximum improvement of the last symptomThe severityof the relapse was calculated as the difference between theEDSS score at the day of maximum worsening and the EDSSscore before the onset of the relapse the lowest ΔEDSS was05 (10 for the first relapse) Recovery was evaluated at thedate of maximum improvement and classified as complete(EDSS= 0) or incomplete (EDSSge 1) Annualized relapse ratewas calculated as the number of relapses during the follow-up divided by the months of the follow-up Annualized EDSSprogression was calculated as the difference between theEDSS score of the last follow-up visit available and the EDSSscore after the first relapse divided by the years of follow-up
23 CSF and Plasma Sampling and Gas6 Measurement CSFsamples of MS patients were drawn within 90 days from
Mediators of Inflammation 3
CSF
[Gas
6] (n
gm
L)
lowast
0
5
10
15
20
25
CISRR-MS Controls
(a)
CISRR-MS Controls
Plas
ma [
Gas
6] (n
gm
L)
ns
0
10
20
30
40
(b)
Figure 1 Gas6 concentration in CSF of patients with MS (a) The scatter plot displays CSF Gas6 concentrations of patients with MS (blackcircles) with respect to controls (white triangles) lowastindicates 119875 lt 005 in statistical comparison of the means (Studentrsquos t test) the horizontalbar indicated the mean value (b) The scatter plot displays plasma Gas6 concentrations of patients with MS (black circles) with respect tocontrols (white triangles) The horizontal bar indicated the mean value
the symptoms onset and before complete resolution of therelapse 29 patients underwent also a blood draw in thesame day of the spinal puncture CSF and plasma sampleswere obtained from a biobank including patients affectedby a noninflammatorynonautoimmune neurological dis-eases (NINAD) such as ischemic stroke amyotrophic lateralsclerosis headache and psychiatric conditions simulatingneurological diseases or otologic dizziness CSF and plasmasamples of cases and controls were stored at minus30∘C Gas6was measured by a sandwich ELISA developed and validatedin our laboratory for human plasma samples [24 25] andwith the same method modified for CSF assay as previouslydescribed [26] Samples from MS patients had been col-lected between 2001 and 2005 appropriately aliquoted andstored at minus80∘C to be tested for Gas6 concentration between2009 and 2010 Samples from NINAD controls were alsocollected along the years from 2001 and 2005 processed andstored similarly and used for Gas6 testing in 2007 theselatter data had already been published [26] Briefly a 96-well plate (NUNC ImmunoPlates MaxiSorp F96 NUNCHereford UK) is coated overnight with anti-human-Gas6primary antibody (goat polyclonal affinity purified IgG RampDSystems Minneapolis MN USA) The antigen is detected bya secondary biotin conjugated antibody (Biotinylated anti-human Gas6 antibody RampD Systems Minneapolis MNUSA) a streptavidin-peroxidase conjugate (Sigma St LouisMO USA) and TMB (331015840551015840-tetramethylbenzidine SigmaSt Louis MO USA) The reaction is blocked with sul-phuric acid 18 and absorbance detected at 450 nm with areference wavelength set at 570 nm Optical density is fittedversus nominal concentration by applying a four-parameterlogistic regression to the calibration curve prepared in Gas6depleted plasma or in BSA (Bovine serum albumin furtherpurified fraction V ge98 Sigma St Louis MO USA)The method has been validated according to the Food andDrug Administration guidelines for inter- and intra-assay coefficient of variation (CV) for Gas6 measurement in
human plasma and CSF (all CVs were within 15 withnegligible matrix effect) There was no cross-reactivity withhuman protein S (MP Biomedicals Solon OH USA) Thelowest quantification limit was 026 ngmL [24ndash26]
24 Statistical Analysis Data were collected and stored inan electronic database to be analyzed with the Statisticastatistical software program release 10 (StatSoft Tulsa OKUnited States) The Shapiro-Wilk test was performed toassess normality for any continuous variable analyzed Themeasures of central tendency anddispersion used throughoutthe paper weremeans and standard deviations for continuousvariables with normal distribution Accordingly normallydistributed variables were compared among groups bymeansof the Studentrsquos t-test ANOVA and post hoc comparisonsof the means (Tukeyrsquos post hoc test for nonhomogeneoussamplestest of Spjotvoll-Stoline) Categorical variables wereanalyzed with Pearson chi-square test and stepwise logisticregression to identify independent predictive factors of CSFGas6 variations A level of 005 (two-sided) was chosen toindicate statistical significance
3 Results
Mean CSF Gas6 concentration was nearly equal in CIS withrespect to RR-MS patients (78 plusmn 32 ngmL versus 79 plusmn 38Studentrsquos t-test 119875 = ns) but significantly higher in CISRR-MS (119899 = 65 37 females) patients with respect to controls(119899 = 40 22 females) (79 plusmn 37 ngmL versus 65 plusmn 24 ngmLresp 119875 lt 003) while plasma Gas6 concentration was notsignificantly different between groups (Studentrsquos t test 119875 =ns) (Figure 1)
Figure 2 shows mean CSF Gas6 concentration inrelationship to the duration of relapse CSF Gas6 concen-tration was significantly higher in shorter relapses (relapseslasting le60 days 87 plusmn 39 ngmL versus gt60 days
4 Mediators of Inflammation
Relapse duration
0
2
4
6
8
10
12
le60 days gt60 days Controls
lowast
lowast
CSF
[Gas
6] (n
gm
L)
(a)
0
2
4
6
8
10
12
le2 FS ge3 FS Controls
lowast
lowast
Number of FS involved
CSF
[Gas
6] (n
gm
L)
(b)
Relapse severity
0
2
4
6
8
10
12
ΔEDSS le 25 ΔEDSS ge 3 Controls
lowast
lowast
CSF
[Gas
6] (n
gm
L)
(c)
Figure 2 Gas6 concentration in CSF of patients withMS in relationto relapse features The graph shows means and standard deviationsof CSF Gas6 concentrations in relation to relapse duration le60days (dots) gt60 days (vertical lines) and controls (gray) (panel a)number of FS involved during the relapse le2 (dots) ge3 (verticallines) and controls (gray) (panel b) and EDSS score variationat maximum worsening (severity) le25 (dots) ge3 (vertical lines)and controls (gray) (panel c) lowastindicates 119875 le 005 in statisticalcomparison of the means (Tukeyrsquos post hoc test)
0
5
10
15
0 5 10 15 20 25 30 35 40plasma [Gas6] (ngmL)
CSF
[Gas
6] (n
gm
L)
Figure 3 Dissociation between CSF and plasma Gas6 concentra-tion The figure displays the absence of correlation between CSFand plasma Gas6 concentration measured simultaneously duringthe first relapse in MS patients The line indicates the regressionequation CSF Gas6 = 0007 sdot plasma Gas6 + 71 1199032 = 00003 119875 = ns
65 plusmn 26 ngmL and controls 65 plusmn 24 ngmL ANOVA119865 = 58 119875 lt 0004 Tukey post hoc test 119875 = 005) in relapseswith fewer FS involved (le2 FS 85 plusmn 38 ngmL versus ge3 FS56 plusmn 25 ngmL versus controls ANOVA 119865 = 67 119875 lt 0002Tukey post hoc test 119875 lt 005) and in relapses with lowerseverity (ΔEDSS le 25 88 plusmn 37 ngmL versus ge3 65 plusmn35 ngmL versus controls ANOVA 119865 = 66 119875 lt 0002Tukey post hoc test 119875 lt 0 04) In particular CSF Gas6concentration was inversely proportional to the EDSS scoreof the relapse (1198772 = 011 119875 lt 001) especially in pyramidalor cerebellar ones (1198772 = 0 25 119875 lt 0 003) On the otherhand CSF Gas6 concentration did not change accordingto completeness of recovery being similar in patients withor without complete recovery (82 plusmn 40 ngmL versus 76 plusmn35 versus controls ANOVA 119875 = ns) Alternatively CSFGas6 did not vary according to age therapy Link index(119875 = ns) Conversely plasma Gas6 concentration was notrelated to any of the clinical variables listed above (ANOVA119875 = ns) Indeed there was no relation between CSF andplasma Gas6 concentration (1198772 = 00003 119875 = ns) as shownin Figure 3 In stepwise logistic regression relapse durationand number of FS involved were significantly associatedwith Gas6 concentration (119865 133 and 65 resp 119875 lt 002)Treatment allocation according to relapse features is shownin Table 2
Follow-up data for a minimum of 25 years were availablefor 55 out of 65 patients and are presented in Table 3 Gas6concentration did not differ according to annualized relapserate either in CSF (Studentrsquos t test ge025year 84 plusmn 46 versuslt025year 80 plusmn 32 ngmL 119875 = ns) or in plasma (215 plusmn64 versus 213 plusmn 124 119875 = ns) and according to annualizedEDSS progression either in CSF (ge02 EDSS pointsyear 79 plusmn31 versus lt02 81 plusmn 48 119875 = ns) or in plasma (218 plusmn 88versus 234 plusmn 76 ngmL 119875 = ns) Moreover neither CSF norplasma Gas6 concentration correlated to annualized relapse
Mediators of Inflammation 5
Table 2 Treatment allocation according to relapse features
Relapse features Type of treatment1205942 analysis
No Oral PDNlowast IVMPlowastlowast
Duration le60gt60 days 2210 75 165 115 119875 = nsNumber of FS involved (le2gt2) 267 84 164 088 119875 = nsSeverity ΔEDSS (le25gt25) 2211 75 119 078 119875 = nsPDN prednisone IVMP intravenous methylprednisone FS functional system and ΔEDSS variation from baseline of Expanded-Disability-Status ScalelowastOral prednisone was administered at 50mgday for the first 5 days then 25mgday for the following 5 days and 125mgday for further 5 days and thendiscontinuedlowastlowastIntra venous methylprednisone was administered at 1000mgday iv infusion for 5 consecutive days
Table 3 Follow-up cohort features
M plusmn SD MedianFollow-up duration (years) 59 plusmn 18 52Annualized relapse rate (relapseyear) 032 plusmn 025 025Annualized relapse progression (ΔEDSSyear) 16 plusmn 10 10
rate or EDSS progression in linear regression analysis (datanot shown 119875 = ns)
4 Discussion
The present paper shows that CSF Gas6 concentration isslightly higher in patients suffering a first relapse of MS thanin control patients Interestingly a significant and substantialincrease in CSF was observed in patients suffering fromshorter less severe and less FS involved relapses Converselypatients who suffered from more severe relapse did notshow any variations of CSF Gas6 concentration with respectto control subjects This apparent paradox is reconciliatedby considering Gas6 as a protective protein able to limitinflammatory demyelination This hypothesis is sustained byseveral in vitro and in vivo studies that indicate forGas6 a roleas inhibitor of macrophages activation [7 9] and as a survivalfactor for neurons and oligodendrocytes [11 15 16] IndeedGas6 knock-out mice challenged with cuprizone displayincreased demyelination damage with greater lesions anda higher number of apoptotic oligodendrocytes infiltratingmacrophages and microglial cells [6] In absence of Gas6there is a delay in remyelination of the lesions induced bycuprizone [17] Moreover Gas6 concentration is raised in theCSF of patients suffering from CIDP a chronic autoimmunedemyelinating disease of the peripheral nerves which sharessome similarities with MS [26] In summary our results fitwell the data in the literature suggesting that MS patientswith higher CSF Gas6 might be able to limit the extentof inflammatory demyelination On the other hand Gas6elevation in CSF seems to be related to relapse features ratherthan to the presence of MS itself Additionally since analtered Gas6TAM ratio has been evidenced in establishedMS lesions [27] an impaired expression of TAM-receptor inabsence of alteration of Gas6 concentration may concurr toinfluence the disease course Further studies are needed toaddress this hypothesis
Themechanisms by which Gas6 might exert this putativeprotection by the effects of inflammatory demyelinationremain speculative Gas6 could act on macrophages andorglial cells this hypothesis is supported by the observationsindicating that Gas6 downregulates the production of proin-flammatory cytokines such as IL-6 and TNF-alpha andenhances the phagocytosis of cellular debris and apoptoticbodies through Mer receptor by activated macrophagesdendritic and microglial cells [7 9 28ndash30] Thus Gas6 maybe able to limit the activation of the innate immune responseand consequently the aggression to myelin fibers favoringcell debris and apoptotic bodies clearance which are in turninflammatory triggers Since mononuclear activation withcytokine production is crucial in the amplification of theautoimmune aggression to myelin and the failure to clearapoptotic cells iswidely considered a trigger of autoimmunityGas6 may have an important role in this context Alterna-tively Gas6TAM interaction could be relevant in processesof recovery after inflammatory demyelination since it is welldemonstrated that it enhances the survival of oligodendro-cytes and neurons [11 15] as happening for other cell lines[31] and mice lacking Gas6 have demyelinating lesions witha higher proportion of apoptotic oligodendrocytes duringcuprizone-induced demyelination [6] Consequently Gas6may participate actively in oligodendrocyte survival aftermyelin damage favoring a prompt repair It is conceivable thatpatients who suffer frommore severe relapse and who do notpresent an increase in CSF Gas6 concentration may have adefect in Gas6 expression and consequently present a defectin mechanisms of self-limitation to immune aggression toCNS or in myelin damage repair It must be pointed outhowever that we were unable to identify a relation betweenGas6 concentration in CSF and lack of complete recoveryafter the relapse which could be considered the clinicalcorrelate of an efficient recovery system
The putative role of Gas6 in the control of immuneaggression in the nervous system is strengthened by the find-ing that plasma and CSF Gas6 concentration are unrelatedin MS patients therefore the increase of Gas6 in the CSFwas not dependent on an increased plasma concentrationandor the breakdown of the blood-brain barrier but likelyon production by inflammatory cells within the CNS Theseresults are in line with previous results from our group con-cerning autoimmune polyneuropathies [26 32] Moreoverthe relation between CSF Gas6 and EDSS score was stricterin pyramidal and cerebellar relapses possibly because EDSS
6 Mediators of Inflammation
is more sensitive to the damage extension in pyramidal andcerebellar relapses with respect to other symptoms that aremainly subjective and less easy to score
Although the sample size was small and only a fewpatients had an active disease with a significant number ofrelapses or severe disability progression our data suggest thatmeasuring Gas6 concentration in CSF of MS patients canonly be useful to predict the evolution of a first relapse but notthe subsequent disease course Thus Gas6 may be importantin limiting the acute inflammatory demyelination during arelapse but less than so in the pathogenic mechanisms thatdetermine relapse recurrences and cumulative disability
In conclusion CSF Gas6 protein concentration is signifi-cantly increased inmilderMS relapses suggesting an involve-ment of this protein in limiting autoimmune demyelinatingprocesses or in favouring myelin repair after damage Gas6measurement in CSF during a relapse can be useful to predicthow a relapse will evolve but not the disease course in thelong term Further studies are warranted to clarify the Gas6and TAM receptors role in the pathogenesis of MS-relapsesand its clinical applications
Conflict of Interests
The authors declare no conflict of interest
Acknowledgments
This work was supported by (Fondazione Italiana SclerosiMultiplaItalian Multiple Sclerosis Foundation) FISM 2010research Grant During the paper preparation ProfessorFrancescoMonaco prematurely died All investigatorswish todedicate this paper to his memory honouring his dedicationto clinical research in neurological diseases
References
[1] D A Hafler J M Slavik D E Anderson K C OrsquoConnor P DeJager and C Baecher-Allan ldquoMultiple sclerosisrdquo ImmunologicalReviews vol 204 pp 208ndash231 2005
[2] GManfioletti C Brancolini G Avanzi and C Schneider ldquoTheprotein encoded by a growth arrest-specific gene (gas6) is a newmember of the vitamin K-dependent proteins related to proteinS a negative coregulator in the blood coagulation cascaderdquoMolecular and Cellular Biology vol 13 no 8 pp 4976ndash49851993
[3] P J Godowski M R Mark J Chen M D Sadick H Raaband R G Hammonds ldquoReevaluation of the roles of protein Sand Gas6 as ligands for the receptor tyrosine kinase RseTyro3rdquo Cell vol 82 no 3 pp 355ndash358 1995
[4] B C Varnum C Young G Elliot et al ldquoAxl receptor tyrosinekinase stimulated by the vitamin K-dependent protein encodedby growth-arrest-specific gene 6rdquo Nature vol 373 no 6515 pp623ndash626 1995
[5] D R Joseph ldquoSequence and functional relationships betweenandrogen-binding proteinsex hormone-binding globulin andits homologs protein S Gas6 laminin and agrinrdquo Steroids vol62 no 8-9 pp 578ndash588 1997
[6] M D Binder and T J Kilpatrick ldquoTAM receptor signalling anddemyelinationrdquo NeuroSignals vol 17 no 4 pp 277ndash287 2009
[7] G Lemke and Q Lu ldquoMacrophage regulation by Tyro 3 familyreceptorsrdquoCurrent Opinion in Immunology vol 15 no 1 pp 31ndash36 2003
[8] Q Lu and G Lemke ldquoHomeostatic regulation of the immunesystem by receptor tyrosine kinases of the Tyro 3 familyrdquoScience vol 293 no 5528 pp 306ndash311 2001
[9] F Alciato P P Sainaghi D Sola L Castello and G C AvanzildquoTNF-120572 IL-6 and IL-1 expression is inhibited by GAS6 inmonocytesmacrophagesrdquo Journal of Leukocyte Biology vol 87no 5 pp 869ndash875 2010
[10] A L Prieto J LWeber S TracyM J Heeb and C Lai ldquoGas6 aligand for the receptor protein-tyrosine kinase Tyro-3 is widelyexpressed in the central nervous systemrdquo Brain Research vol816 no 2 pp 646ndash661 1999
[11] H Funakoshi T Yonemasu T Nakano K Matumoto and TNakamura ldquoIdentification of Gas6 a putative ligand for Sky andAxl receptor tyrosine kinases as a novel neurotrophic factor forhippocampal neuronsrdquo Journal of Neuroscience Research vol68 no 2 pp 150ndash160 2002
[12] A L Prieto S OrsquoDell B Varnum and C Lai ldquoLocalizationand signaling of the receptor protein tyrosine kinase Tyro3 incortical and hippocampal neuronsrdquo Neuroscience vol 150 no2 pp 319ndash334 2007
[13] T Yagami K Ueda K Asakura et al ldquoGas6 rescues corticalneurons from amyloid 120573 protein-induced apoptosisrdquo Neu-ropharmacology vol 43 no 8 pp 1289ndash1296 2002
[14] R H Li J Chen G Hammonds et al ldquoIdentification ofGas6 as a growth factor for human Schwann cellsrdquo Journal ofNeuroscience vol 16 no 6 pp 2012ndash2019 1996
[15] S L Shankar K OrsquoGuin M Cammer et al ldquoThe growtharrest-specific gene product Gas6 promotes the survival ofhuman oligodendrocytes via a phosphatidylinositol 3-kinase-dependent pathwayrdquo Journal of Neuroscience vol 23 no 10 pp4208ndash4218 2003
[16] S L Shankar K OrsquoGuin M Kim et al ldquoGas6Axl signalingactivates the phosphatidylinositol 3-kinaseAkt1 survival path-way to protect oligodendrocytes from tumor necrosis factor120572-induced apoptosisrdquo Journal of Neuroscience vol 26 no 21 pp5638ndash5648 2006
[17] M D Binder J Xiao D Kemper G Z M Ma S S Murrayand T J Kilpatrick ldquoGas6 increases myelination by oligoden-drocytes and its deficiency delays recovery following cuprizone-induced demyelinationrdquo PLoS ONE vol 6 no 3 article e177272011
[18] V Tsiperson X Li G J Schwartz C S Raine and B Shafit-Zagardo ldquoGAS6 enhances repair following cuprizone-induceddemyelinationrdquo PLoS ONE vol 5 no 12 article e15748 2010
[19] D Miller F Barkhof X Montalban A Thompson and MFilippi ldquoClinically isolated syndromes suggestive of multiplesclerosis part I natural history pathogenesis diagnosis andprognosisrdquo Lancet Neurology vol 4 no 5 pp 281ndash288 2005
[20] W I McDonald A Compston G Edan et al ldquoRecommendeddiagnostic criteria for multiple sclerosis Guidelines from theInternational Panel on the Diagnosis of Multiple SclerosisrdquoAnnals of Neurology vol 50 no 1 pp 121ndash127 2001
[21] G A Schumacker G Beebe R F Kibler et al ldquoProblems ofexperimental trials of therapy in multiple sclerosis report bythe panel on the evaluation of experimental trials of therapy inmultiple sclerosisrdquo Annals of the New York Academy of Sciencesvol 122 pp 552ndash568 1965
[22] M A Leone S Bonissoni L Collimedaglia et al ldquoFactors pre-dicting incomplete recovery from relapses in multiple sclerosis
Mediators of Inflammation 7
A Prospective Studyrdquo Multiple Sclerosis vol 14 no 4 pp 485ndash493 2008
[23] J F Kurtzke ldquoRating neurologic impairment in multiple sclero-sis an expanded disability status scale (EDSS)rdquo Neurology vol33 no 11 pp 1444ndash1452 1983
[24] F Alciato P P Sainaghi L Castello L Bergamasco SCarnieletto and G C Avanzi ldquoDevelopment and validation ofan ELISA method for detection of Growth Arrest Specific 6(GAS6) protein in human plasmardquo Journal of Immunoassay andImmunochemistry vol 29 no 2 pp 167ndash180 2008
[25] P P Sainaghi F Alciato S Carnieletto et al ldquoGas6 evaluationin patients with acute dyspnea due to suspected pulmonaryembolismrdquo Respiratory Medicine vol 103 no 4 pp 589ndash5942009
[26] P P Sainaghi L Collimedaglia F Alciato et al ldquoEleva-tion of Gas6 protein concentration in cerebrospinal fluid ofpatients with chronic inflammatory demyelinating polyneu-ropathy (CIDP)rdquo Journal of the Neurological Sciences vol 269no 1-2 pp 138ndash142 2008
[27] J G Weinger K M Omari K Marsden C S Raine and BShafit-Zagardo ldquoUp-regulation of soluble Axl andMer receptortyrosine kinases negatively correlates with Gas6 in establishedmultiple sclerosis lesionsrdquo American Journal of Pathology vol175 no 1 pp 283ndash293 2009
[28] WH Shao Y Zhen R A Eisenberg and P L Cohen ldquoTheMerreceptor tyrosine kinase is expressed on discrete macrophagesubpopulations and mainly uses Gas6 as its ligand for uptake ofapoptotic cellsrdquoClinical Immunology vol 133 no 1 pp 138ndash1442009
[29] C Grommes C Y D Lee B L Wilkinson et al ldquoRegulation ofmicroglial phagocytosis and inflammatory gene expression byGas6 acting on the AxlMer family of tyrosine kinasesrdquo Journalof NeuroImmune Pharmacology vol 3 no 2 pp 130ndash140 2008
[30] P Sen M A Wallet Z Yi et al ldquoApoptotic cells induce Mertyrosine kinase-dependent blockade of NF-120581B activation indendritic cellsrdquo Blood vol 109 no 2 pp 653ndash660 2007
[31] P P Sainaghi L Castello L BergamascoMGalletti P Bellostaand G C Avanzi ldquoGas6 induces proliferation in prostatecarcinoma cell lines expressing the Axl receptorrdquo Journal ofCellular Physiology vol 204 no 1 pp 36ndash44 2005
[32] P P Sainaghi L Collimedaglia F Alciato et al ldquoThe expressionpattern of inflammatorymediators in cerebrospinal fluid differ-entiates Guillain-Barre syndrome from chronic inflammatorydemyelinating polyneuropathyrdquoCytokine vol 51 no 2 pp 138ndash143 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Mediators of Inflammation
lymphocytes with diffuse tissue infiltration and autoimmunemanifestations including vasculitis lupus-like lesions andautoantibodies This phenotype is likely the consequence ofmonocytes-macrophages hyperactivity [8] The importanceof Gas6 in controlling the immune response is supportedby the finding that Gas6 inhibits macrophage activation andcytokine production reducing interleukin (IL)-6 and TNF-alpha secretion through the activation of Mer receptors [9]
Direct evidences link Gas6 to autoimmune processeswithin the central nervous system (CNS) Gas6 and its TAMreceptors are expressed in the brain of embryonic and adultrats proportionally to synaptogenesis of cerebral tissues [10ndash12] In addition Gas6 promotes proliferative and antiapop-totic effects on several CNS cell types as hippocampal andcortical neurons [11 13] Schwann cells [14] and in particularoligodendrocytes which are protected from apoptosis troughAxlPI3-KAkt activation [15 16] Binder and colleagues havealso shown that the absence of Gas6 affects the efficiency ofremyelination following a demyelinating insult induced bycuprizone and that defect of remyelination is accompaniedto reduction in the number of mature oligodendrocytes [17]moreover the administration of recombinant human Gas6to the corpus callosum enhanced the myelin repair in thesame mouse model [18] These observations suggest that theGas6TAM system may be involved both in the regulationof the survival of neuronal and glial cells in particularof those involved in myelination and the control of theinnate immune response two paramount processes in MSpathogenesis Based on these premises in the present studywe measured CSF and plasma Gas6 protein during a relapseof multiple sclerosis in relation to relapse clinical features andseverity scores as Kurtzke-Functional-System (FS) to verifytheir usefulness as a biomarker of disease course
2 Methods
21 Patients Sixty-five consecutive patients admitted to anacademic referral centre from 2001 to 2005 with a diagnosisof clinically isolated syndrome (CIS) or Relapsing-Remitting(RR) MS were studied CIS was defined as the occurrenceof an acute or subacute event of the CNS affecting the opticnerves brainstem or spinal cord of presumed inflammatorydemyelinating origin in a patient with no history suggestiveof an earlier demyelinating episode [19] McDonald criteria[20]were used to diagnoseMS Inclusion criteriawere agege18years first visit to theMSCentre diagnostic lumbar punctureduring the relapse no treatment with corticosteroids priorto the lumbar puncture and no prior treatment with anyimmunomodulant drug Patients with primary progressiveMS were excluded The majority of patients (119899 = 45) weresampled during their first relapse the others were observedand sampled at their second (119899 = 16) or third relapse (119899 = 4)moreover at sampling 22 were CIS and 43 RR-MS After thefirst visit 55 patients (10 patients were lost to follow-up) wereprospectively followed and visited thereafter every 6 monthsthe follow-up ended on July 31 2009 (Table 1) Follow-upduration ranged from 25 to 11 years (mean 59 years SD 18)At the end of this follow-up period the diagnosis was CIS in
Table 1 Features of the population studied
Population studied Number of patientsFirst relapsesecondthird relapse 45164CISRR-MS 2243Patients with follow-up ge25 years 55CIS clinically isolated syndrome RR-MS relapsing remitting multiplesclerosis
9 cases and RR-MS in 42 while 4 patients had already enteredsecondary progression
The study was approved by a local Ethical Committeeand conducted in strict accordance with principles of theDeclaration of Helsinki Each patient gave a written informedconsent before the lumbar puncture to the use of hisher CSFfor experimental evaluation and to maintain data in the data-base
22 Relapse Definition and Evaluation Relapse was definedas ldquoacute or subacute occurrence recurrence or worseningof symptoms of neurologic dysfunction attributable to MSlasting more than 24 hours after a period of at least 30 daysof improvement or stabilityrdquo [21] Neurological deteriorationof preexisting symptoms accompanied by fever was notconsidered a relapse Paroxysmal episodes were consideredas relapse when multiple and occurring over not less than 24hours Symptoms occurring within a month after the initialsymptoms of relapse were considered to be part of the sameepisode Patients data were collected at the first visit at thecentre during the relapse and also at 3 7 and 30 days after therelapse onset For each relapse type of symptoms signs anddates of occurrence were collected as previously described[22] Briefly symptoms and signs were grouped to fit in withthe Kurtzke Functional System (FS) [23] The score for eachFS and the total EDSS score were calculated at onset atmaximum worsening (zenith) and at the first examinationafter the day of maximum improvement of the relapse Wecorrelated the following factors with Gas6 concentrationrelapse duration and severity recovery gender age at theonset of the relapse number of affected FSs Link index(le070gt070) annualized relapse rate and annualized EDSSprogression The relapse duration was calculated as the timebetween the date of onset of the first symptom and the dateof maximum improvement of the last symptomThe severityof the relapse was calculated as the difference between theEDSS score at the day of maximum worsening and the EDSSscore before the onset of the relapse the lowest ΔEDSS was05 (10 for the first relapse) Recovery was evaluated at thedate of maximum improvement and classified as complete(EDSS= 0) or incomplete (EDSSge 1) Annualized relapse ratewas calculated as the number of relapses during the follow-up divided by the months of the follow-up Annualized EDSSprogression was calculated as the difference between theEDSS score of the last follow-up visit available and the EDSSscore after the first relapse divided by the years of follow-up
23 CSF and Plasma Sampling and Gas6 Measurement CSFsamples of MS patients were drawn within 90 days from
Mediators of Inflammation 3
CSF
[Gas
6] (n
gm
L)
lowast
0
5
10
15
20
25
CISRR-MS Controls
(a)
CISRR-MS Controls
Plas
ma [
Gas
6] (n
gm
L)
ns
0
10
20
30
40
(b)
Figure 1 Gas6 concentration in CSF of patients with MS (a) The scatter plot displays CSF Gas6 concentrations of patients with MS (blackcircles) with respect to controls (white triangles) lowastindicates 119875 lt 005 in statistical comparison of the means (Studentrsquos t test) the horizontalbar indicated the mean value (b) The scatter plot displays plasma Gas6 concentrations of patients with MS (black circles) with respect tocontrols (white triangles) The horizontal bar indicated the mean value
the symptoms onset and before complete resolution of therelapse 29 patients underwent also a blood draw in thesame day of the spinal puncture CSF and plasma sampleswere obtained from a biobank including patients affectedby a noninflammatorynonautoimmune neurological dis-eases (NINAD) such as ischemic stroke amyotrophic lateralsclerosis headache and psychiatric conditions simulatingneurological diseases or otologic dizziness CSF and plasmasamples of cases and controls were stored at minus30∘C Gas6was measured by a sandwich ELISA developed and validatedin our laboratory for human plasma samples [24 25] andwith the same method modified for CSF assay as previouslydescribed [26] Samples from MS patients had been col-lected between 2001 and 2005 appropriately aliquoted andstored at minus80∘C to be tested for Gas6 concentration between2009 and 2010 Samples from NINAD controls were alsocollected along the years from 2001 and 2005 processed andstored similarly and used for Gas6 testing in 2007 theselatter data had already been published [26] Briefly a 96-well plate (NUNC ImmunoPlates MaxiSorp F96 NUNCHereford UK) is coated overnight with anti-human-Gas6primary antibody (goat polyclonal affinity purified IgG RampDSystems Minneapolis MN USA) The antigen is detected bya secondary biotin conjugated antibody (Biotinylated anti-human Gas6 antibody RampD Systems Minneapolis MNUSA) a streptavidin-peroxidase conjugate (Sigma St LouisMO USA) and TMB (331015840551015840-tetramethylbenzidine SigmaSt Louis MO USA) The reaction is blocked with sul-phuric acid 18 and absorbance detected at 450 nm with areference wavelength set at 570 nm Optical density is fittedversus nominal concentration by applying a four-parameterlogistic regression to the calibration curve prepared in Gas6depleted plasma or in BSA (Bovine serum albumin furtherpurified fraction V ge98 Sigma St Louis MO USA)The method has been validated according to the Food andDrug Administration guidelines for inter- and intra-assay coefficient of variation (CV) for Gas6 measurement in
human plasma and CSF (all CVs were within 15 withnegligible matrix effect) There was no cross-reactivity withhuman protein S (MP Biomedicals Solon OH USA) Thelowest quantification limit was 026 ngmL [24ndash26]
24 Statistical Analysis Data were collected and stored inan electronic database to be analyzed with the Statisticastatistical software program release 10 (StatSoft Tulsa OKUnited States) The Shapiro-Wilk test was performed toassess normality for any continuous variable analyzed Themeasures of central tendency anddispersion used throughoutthe paper weremeans and standard deviations for continuousvariables with normal distribution Accordingly normallydistributed variables were compared among groups bymeansof the Studentrsquos t-test ANOVA and post hoc comparisonsof the means (Tukeyrsquos post hoc test for nonhomogeneoussamplestest of Spjotvoll-Stoline) Categorical variables wereanalyzed with Pearson chi-square test and stepwise logisticregression to identify independent predictive factors of CSFGas6 variations A level of 005 (two-sided) was chosen toindicate statistical significance
3 Results
Mean CSF Gas6 concentration was nearly equal in CIS withrespect to RR-MS patients (78 plusmn 32 ngmL versus 79 plusmn 38Studentrsquos t-test 119875 = ns) but significantly higher in CISRR-MS (119899 = 65 37 females) patients with respect to controls(119899 = 40 22 females) (79 plusmn 37 ngmL versus 65 plusmn 24 ngmLresp 119875 lt 003) while plasma Gas6 concentration was notsignificantly different between groups (Studentrsquos t test 119875 =ns) (Figure 1)
Figure 2 shows mean CSF Gas6 concentration inrelationship to the duration of relapse CSF Gas6 concen-tration was significantly higher in shorter relapses (relapseslasting le60 days 87 plusmn 39 ngmL versus gt60 days
4 Mediators of Inflammation
Relapse duration
0
2
4
6
8
10
12
le60 days gt60 days Controls
lowast
lowast
CSF
[Gas
6] (n
gm
L)
(a)
0
2
4
6
8
10
12
le2 FS ge3 FS Controls
lowast
lowast
Number of FS involved
CSF
[Gas
6] (n
gm
L)
(b)
Relapse severity
0
2
4
6
8
10
12
ΔEDSS le 25 ΔEDSS ge 3 Controls
lowast
lowast
CSF
[Gas
6] (n
gm
L)
(c)
Figure 2 Gas6 concentration in CSF of patients withMS in relationto relapse features The graph shows means and standard deviationsof CSF Gas6 concentrations in relation to relapse duration le60days (dots) gt60 days (vertical lines) and controls (gray) (panel a)number of FS involved during the relapse le2 (dots) ge3 (verticallines) and controls (gray) (panel b) and EDSS score variationat maximum worsening (severity) le25 (dots) ge3 (vertical lines)and controls (gray) (panel c) lowastindicates 119875 le 005 in statisticalcomparison of the means (Tukeyrsquos post hoc test)
0
5
10
15
0 5 10 15 20 25 30 35 40plasma [Gas6] (ngmL)
CSF
[Gas
6] (n
gm
L)
Figure 3 Dissociation between CSF and plasma Gas6 concentra-tion The figure displays the absence of correlation between CSFand plasma Gas6 concentration measured simultaneously duringthe first relapse in MS patients The line indicates the regressionequation CSF Gas6 = 0007 sdot plasma Gas6 + 71 1199032 = 00003 119875 = ns
65 plusmn 26 ngmL and controls 65 plusmn 24 ngmL ANOVA119865 = 58 119875 lt 0004 Tukey post hoc test 119875 = 005) in relapseswith fewer FS involved (le2 FS 85 plusmn 38 ngmL versus ge3 FS56 plusmn 25 ngmL versus controls ANOVA 119865 = 67 119875 lt 0002Tukey post hoc test 119875 lt 005) and in relapses with lowerseverity (ΔEDSS le 25 88 plusmn 37 ngmL versus ge3 65 plusmn35 ngmL versus controls ANOVA 119865 = 66 119875 lt 0002Tukey post hoc test 119875 lt 0 04) In particular CSF Gas6concentration was inversely proportional to the EDSS scoreof the relapse (1198772 = 011 119875 lt 001) especially in pyramidalor cerebellar ones (1198772 = 0 25 119875 lt 0 003) On the otherhand CSF Gas6 concentration did not change accordingto completeness of recovery being similar in patients withor without complete recovery (82 plusmn 40 ngmL versus 76 plusmn35 versus controls ANOVA 119875 = ns) Alternatively CSFGas6 did not vary according to age therapy Link index(119875 = ns) Conversely plasma Gas6 concentration was notrelated to any of the clinical variables listed above (ANOVA119875 = ns) Indeed there was no relation between CSF andplasma Gas6 concentration (1198772 = 00003 119875 = ns) as shownin Figure 3 In stepwise logistic regression relapse durationand number of FS involved were significantly associatedwith Gas6 concentration (119865 133 and 65 resp 119875 lt 002)Treatment allocation according to relapse features is shownin Table 2
Follow-up data for a minimum of 25 years were availablefor 55 out of 65 patients and are presented in Table 3 Gas6concentration did not differ according to annualized relapserate either in CSF (Studentrsquos t test ge025year 84 plusmn 46 versuslt025year 80 plusmn 32 ngmL 119875 = ns) or in plasma (215 plusmn64 versus 213 plusmn 124 119875 = ns) and according to annualizedEDSS progression either in CSF (ge02 EDSS pointsyear 79 plusmn31 versus lt02 81 plusmn 48 119875 = ns) or in plasma (218 plusmn 88versus 234 plusmn 76 ngmL 119875 = ns) Moreover neither CSF norplasma Gas6 concentration correlated to annualized relapse
Mediators of Inflammation 5
Table 2 Treatment allocation according to relapse features
Relapse features Type of treatment1205942 analysis
No Oral PDNlowast IVMPlowastlowast
Duration le60gt60 days 2210 75 165 115 119875 = nsNumber of FS involved (le2gt2) 267 84 164 088 119875 = nsSeverity ΔEDSS (le25gt25) 2211 75 119 078 119875 = nsPDN prednisone IVMP intravenous methylprednisone FS functional system and ΔEDSS variation from baseline of Expanded-Disability-Status ScalelowastOral prednisone was administered at 50mgday for the first 5 days then 25mgday for the following 5 days and 125mgday for further 5 days and thendiscontinuedlowastlowastIntra venous methylprednisone was administered at 1000mgday iv infusion for 5 consecutive days
Table 3 Follow-up cohort features
M plusmn SD MedianFollow-up duration (years) 59 plusmn 18 52Annualized relapse rate (relapseyear) 032 plusmn 025 025Annualized relapse progression (ΔEDSSyear) 16 plusmn 10 10
rate or EDSS progression in linear regression analysis (datanot shown 119875 = ns)
4 Discussion
The present paper shows that CSF Gas6 concentration isslightly higher in patients suffering a first relapse of MS thanin control patients Interestingly a significant and substantialincrease in CSF was observed in patients suffering fromshorter less severe and less FS involved relapses Converselypatients who suffered from more severe relapse did notshow any variations of CSF Gas6 concentration with respectto control subjects This apparent paradox is reconciliatedby considering Gas6 as a protective protein able to limitinflammatory demyelination This hypothesis is sustained byseveral in vitro and in vivo studies that indicate forGas6 a roleas inhibitor of macrophages activation [7 9] and as a survivalfactor for neurons and oligodendrocytes [11 15 16] IndeedGas6 knock-out mice challenged with cuprizone displayincreased demyelination damage with greater lesions anda higher number of apoptotic oligodendrocytes infiltratingmacrophages and microglial cells [6] In absence of Gas6there is a delay in remyelination of the lesions induced bycuprizone [17] Moreover Gas6 concentration is raised in theCSF of patients suffering from CIDP a chronic autoimmunedemyelinating disease of the peripheral nerves which sharessome similarities with MS [26] In summary our results fitwell the data in the literature suggesting that MS patientswith higher CSF Gas6 might be able to limit the extentof inflammatory demyelination On the other hand Gas6elevation in CSF seems to be related to relapse features ratherthan to the presence of MS itself Additionally since analtered Gas6TAM ratio has been evidenced in establishedMS lesions [27] an impaired expression of TAM-receptor inabsence of alteration of Gas6 concentration may concurr toinfluence the disease course Further studies are needed toaddress this hypothesis
Themechanisms by which Gas6 might exert this putativeprotection by the effects of inflammatory demyelinationremain speculative Gas6 could act on macrophages andorglial cells this hypothesis is supported by the observationsindicating that Gas6 downregulates the production of proin-flammatory cytokines such as IL-6 and TNF-alpha andenhances the phagocytosis of cellular debris and apoptoticbodies through Mer receptor by activated macrophagesdendritic and microglial cells [7 9 28ndash30] Thus Gas6 maybe able to limit the activation of the innate immune responseand consequently the aggression to myelin fibers favoringcell debris and apoptotic bodies clearance which are in turninflammatory triggers Since mononuclear activation withcytokine production is crucial in the amplification of theautoimmune aggression to myelin and the failure to clearapoptotic cells iswidely considered a trigger of autoimmunityGas6 may have an important role in this context Alterna-tively Gas6TAM interaction could be relevant in processesof recovery after inflammatory demyelination since it is welldemonstrated that it enhances the survival of oligodendro-cytes and neurons [11 15] as happening for other cell lines[31] and mice lacking Gas6 have demyelinating lesions witha higher proportion of apoptotic oligodendrocytes duringcuprizone-induced demyelination [6] Consequently Gas6may participate actively in oligodendrocyte survival aftermyelin damage favoring a prompt repair It is conceivable thatpatients who suffer frommore severe relapse and who do notpresent an increase in CSF Gas6 concentration may have adefect in Gas6 expression and consequently present a defectin mechanisms of self-limitation to immune aggression toCNS or in myelin damage repair It must be pointed outhowever that we were unable to identify a relation betweenGas6 concentration in CSF and lack of complete recoveryafter the relapse which could be considered the clinicalcorrelate of an efficient recovery system
The putative role of Gas6 in the control of immuneaggression in the nervous system is strengthened by the find-ing that plasma and CSF Gas6 concentration are unrelatedin MS patients therefore the increase of Gas6 in the CSFwas not dependent on an increased plasma concentrationandor the breakdown of the blood-brain barrier but likelyon production by inflammatory cells within the CNS Theseresults are in line with previous results from our group con-cerning autoimmune polyneuropathies [26 32] Moreoverthe relation between CSF Gas6 and EDSS score was stricterin pyramidal and cerebellar relapses possibly because EDSS
6 Mediators of Inflammation
is more sensitive to the damage extension in pyramidal andcerebellar relapses with respect to other symptoms that aremainly subjective and less easy to score
Although the sample size was small and only a fewpatients had an active disease with a significant number ofrelapses or severe disability progression our data suggest thatmeasuring Gas6 concentration in CSF of MS patients canonly be useful to predict the evolution of a first relapse but notthe subsequent disease course Thus Gas6 may be importantin limiting the acute inflammatory demyelination during arelapse but less than so in the pathogenic mechanisms thatdetermine relapse recurrences and cumulative disability
In conclusion CSF Gas6 protein concentration is signifi-cantly increased inmilderMS relapses suggesting an involve-ment of this protein in limiting autoimmune demyelinatingprocesses or in favouring myelin repair after damage Gas6measurement in CSF during a relapse can be useful to predicthow a relapse will evolve but not the disease course in thelong term Further studies are warranted to clarify the Gas6and TAM receptors role in the pathogenesis of MS-relapsesand its clinical applications
Conflict of Interests
The authors declare no conflict of interest
Acknowledgments
This work was supported by (Fondazione Italiana SclerosiMultiplaItalian Multiple Sclerosis Foundation) FISM 2010research Grant During the paper preparation ProfessorFrancescoMonaco prematurely died All investigatorswish todedicate this paper to his memory honouring his dedicationto clinical research in neurological diseases
References
[1] D A Hafler J M Slavik D E Anderson K C OrsquoConnor P DeJager and C Baecher-Allan ldquoMultiple sclerosisrdquo ImmunologicalReviews vol 204 pp 208ndash231 2005
[2] GManfioletti C Brancolini G Avanzi and C Schneider ldquoTheprotein encoded by a growth arrest-specific gene (gas6) is a newmember of the vitamin K-dependent proteins related to proteinS a negative coregulator in the blood coagulation cascaderdquoMolecular and Cellular Biology vol 13 no 8 pp 4976ndash49851993
[3] P J Godowski M R Mark J Chen M D Sadick H Raaband R G Hammonds ldquoReevaluation of the roles of protein Sand Gas6 as ligands for the receptor tyrosine kinase RseTyro3rdquo Cell vol 82 no 3 pp 355ndash358 1995
[4] B C Varnum C Young G Elliot et al ldquoAxl receptor tyrosinekinase stimulated by the vitamin K-dependent protein encodedby growth-arrest-specific gene 6rdquo Nature vol 373 no 6515 pp623ndash626 1995
[5] D R Joseph ldquoSequence and functional relationships betweenandrogen-binding proteinsex hormone-binding globulin andits homologs protein S Gas6 laminin and agrinrdquo Steroids vol62 no 8-9 pp 578ndash588 1997
[6] M D Binder and T J Kilpatrick ldquoTAM receptor signalling anddemyelinationrdquo NeuroSignals vol 17 no 4 pp 277ndash287 2009
[7] G Lemke and Q Lu ldquoMacrophage regulation by Tyro 3 familyreceptorsrdquoCurrent Opinion in Immunology vol 15 no 1 pp 31ndash36 2003
[8] Q Lu and G Lemke ldquoHomeostatic regulation of the immunesystem by receptor tyrosine kinases of the Tyro 3 familyrdquoScience vol 293 no 5528 pp 306ndash311 2001
[9] F Alciato P P Sainaghi D Sola L Castello and G C AvanzildquoTNF-120572 IL-6 and IL-1 expression is inhibited by GAS6 inmonocytesmacrophagesrdquo Journal of Leukocyte Biology vol 87no 5 pp 869ndash875 2010
[10] A L Prieto J LWeber S TracyM J Heeb and C Lai ldquoGas6 aligand for the receptor protein-tyrosine kinase Tyro-3 is widelyexpressed in the central nervous systemrdquo Brain Research vol816 no 2 pp 646ndash661 1999
[11] H Funakoshi T Yonemasu T Nakano K Matumoto and TNakamura ldquoIdentification of Gas6 a putative ligand for Sky andAxl receptor tyrosine kinases as a novel neurotrophic factor forhippocampal neuronsrdquo Journal of Neuroscience Research vol68 no 2 pp 150ndash160 2002
[12] A L Prieto S OrsquoDell B Varnum and C Lai ldquoLocalizationand signaling of the receptor protein tyrosine kinase Tyro3 incortical and hippocampal neuronsrdquo Neuroscience vol 150 no2 pp 319ndash334 2007
[13] T Yagami K Ueda K Asakura et al ldquoGas6 rescues corticalneurons from amyloid 120573 protein-induced apoptosisrdquo Neu-ropharmacology vol 43 no 8 pp 1289ndash1296 2002
[14] R H Li J Chen G Hammonds et al ldquoIdentification ofGas6 as a growth factor for human Schwann cellsrdquo Journal ofNeuroscience vol 16 no 6 pp 2012ndash2019 1996
[15] S L Shankar K OrsquoGuin M Cammer et al ldquoThe growtharrest-specific gene product Gas6 promotes the survival ofhuman oligodendrocytes via a phosphatidylinositol 3-kinase-dependent pathwayrdquo Journal of Neuroscience vol 23 no 10 pp4208ndash4218 2003
[16] S L Shankar K OrsquoGuin M Kim et al ldquoGas6Axl signalingactivates the phosphatidylinositol 3-kinaseAkt1 survival path-way to protect oligodendrocytes from tumor necrosis factor120572-induced apoptosisrdquo Journal of Neuroscience vol 26 no 21 pp5638ndash5648 2006
[17] M D Binder J Xiao D Kemper G Z M Ma S S Murrayand T J Kilpatrick ldquoGas6 increases myelination by oligoden-drocytes and its deficiency delays recovery following cuprizone-induced demyelinationrdquo PLoS ONE vol 6 no 3 article e177272011
[18] V Tsiperson X Li G J Schwartz C S Raine and B Shafit-Zagardo ldquoGAS6 enhances repair following cuprizone-induceddemyelinationrdquo PLoS ONE vol 5 no 12 article e15748 2010
[19] D Miller F Barkhof X Montalban A Thompson and MFilippi ldquoClinically isolated syndromes suggestive of multiplesclerosis part I natural history pathogenesis diagnosis andprognosisrdquo Lancet Neurology vol 4 no 5 pp 281ndash288 2005
[20] W I McDonald A Compston G Edan et al ldquoRecommendeddiagnostic criteria for multiple sclerosis Guidelines from theInternational Panel on the Diagnosis of Multiple SclerosisrdquoAnnals of Neurology vol 50 no 1 pp 121ndash127 2001
[21] G A Schumacker G Beebe R F Kibler et al ldquoProblems ofexperimental trials of therapy in multiple sclerosis report bythe panel on the evaluation of experimental trials of therapy inmultiple sclerosisrdquo Annals of the New York Academy of Sciencesvol 122 pp 552ndash568 1965
[22] M A Leone S Bonissoni L Collimedaglia et al ldquoFactors pre-dicting incomplete recovery from relapses in multiple sclerosis
Mediators of Inflammation 7
A Prospective Studyrdquo Multiple Sclerosis vol 14 no 4 pp 485ndash493 2008
[23] J F Kurtzke ldquoRating neurologic impairment in multiple sclero-sis an expanded disability status scale (EDSS)rdquo Neurology vol33 no 11 pp 1444ndash1452 1983
[24] F Alciato P P Sainaghi L Castello L Bergamasco SCarnieletto and G C Avanzi ldquoDevelopment and validation ofan ELISA method for detection of Growth Arrest Specific 6(GAS6) protein in human plasmardquo Journal of Immunoassay andImmunochemistry vol 29 no 2 pp 167ndash180 2008
[25] P P Sainaghi F Alciato S Carnieletto et al ldquoGas6 evaluationin patients with acute dyspnea due to suspected pulmonaryembolismrdquo Respiratory Medicine vol 103 no 4 pp 589ndash5942009
[26] P P Sainaghi L Collimedaglia F Alciato et al ldquoEleva-tion of Gas6 protein concentration in cerebrospinal fluid ofpatients with chronic inflammatory demyelinating polyneu-ropathy (CIDP)rdquo Journal of the Neurological Sciences vol 269no 1-2 pp 138ndash142 2008
[27] J G Weinger K M Omari K Marsden C S Raine and BShafit-Zagardo ldquoUp-regulation of soluble Axl andMer receptortyrosine kinases negatively correlates with Gas6 in establishedmultiple sclerosis lesionsrdquo American Journal of Pathology vol175 no 1 pp 283ndash293 2009
[28] WH Shao Y Zhen R A Eisenberg and P L Cohen ldquoTheMerreceptor tyrosine kinase is expressed on discrete macrophagesubpopulations and mainly uses Gas6 as its ligand for uptake ofapoptotic cellsrdquoClinical Immunology vol 133 no 1 pp 138ndash1442009
[29] C Grommes C Y D Lee B L Wilkinson et al ldquoRegulation ofmicroglial phagocytosis and inflammatory gene expression byGas6 acting on the AxlMer family of tyrosine kinasesrdquo Journalof NeuroImmune Pharmacology vol 3 no 2 pp 130ndash140 2008
[30] P Sen M A Wallet Z Yi et al ldquoApoptotic cells induce Mertyrosine kinase-dependent blockade of NF-120581B activation indendritic cellsrdquo Blood vol 109 no 2 pp 653ndash660 2007
[31] P P Sainaghi L Castello L BergamascoMGalletti P Bellostaand G C Avanzi ldquoGas6 induces proliferation in prostatecarcinoma cell lines expressing the Axl receptorrdquo Journal ofCellular Physiology vol 204 no 1 pp 36ndash44 2005
[32] P P Sainaghi L Collimedaglia F Alciato et al ldquoThe expressionpattern of inflammatorymediators in cerebrospinal fluid differ-entiates Guillain-Barre syndrome from chronic inflammatorydemyelinating polyneuropathyrdquoCytokine vol 51 no 2 pp 138ndash143 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Mediators of Inflammation 3
CSF
[Gas
6] (n
gm
L)
lowast
0
5
10
15
20
25
CISRR-MS Controls
(a)
CISRR-MS Controls
Plas
ma [
Gas
6] (n
gm
L)
ns
0
10
20
30
40
(b)
Figure 1 Gas6 concentration in CSF of patients with MS (a) The scatter plot displays CSF Gas6 concentrations of patients with MS (blackcircles) with respect to controls (white triangles) lowastindicates 119875 lt 005 in statistical comparison of the means (Studentrsquos t test) the horizontalbar indicated the mean value (b) The scatter plot displays plasma Gas6 concentrations of patients with MS (black circles) with respect tocontrols (white triangles) The horizontal bar indicated the mean value
the symptoms onset and before complete resolution of therelapse 29 patients underwent also a blood draw in thesame day of the spinal puncture CSF and plasma sampleswere obtained from a biobank including patients affectedby a noninflammatorynonautoimmune neurological dis-eases (NINAD) such as ischemic stroke amyotrophic lateralsclerosis headache and psychiatric conditions simulatingneurological diseases or otologic dizziness CSF and plasmasamples of cases and controls were stored at minus30∘C Gas6was measured by a sandwich ELISA developed and validatedin our laboratory for human plasma samples [24 25] andwith the same method modified for CSF assay as previouslydescribed [26] Samples from MS patients had been col-lected between 2001 and 2005 appropriately aliquoted andstored at minus80∘C to be tested for Gas6 concentration between2009 and 2010 Samples from NINAD controls were alsocollected along the years from 2001 and 2005 processed andstored similarly and used for Gas6 testing in 2007 theselatter data had already been published [26] Briefly a 96-well plate (NUNC ImmunoPlates MaxiSorp F96 NUNCHereford UK) is coated overnight with anti-human-Gas6primary antibody (goat polyclonal affinity purified IgG RampDSystems Minneapolis MN USA) The antigen is detected bya secondary biotin conjugated antibody (Biotinylated anti-human Gas6 antibody RampD Systems Minneapolis MNUSA) a streptavidin-peroxidase conjugate (Sigma St LouisMO USA) and TMB (331015840551015840-tetramethylbenzidine SigmaSt Louis MO USA) The reaction is blocked with sul-phuric acid 18 and absorbance detected at 450 nm with areference wavelength set at 570 nm Optical density is fittedversus nominal concentration by applying a four-parameterlogistic regression to the calibration curve prepared in Gas6depleted plasma or in BSA (Bovine serum albumin furtherpurified fraction V ge98 Sigma St Louis MO USA)The method has been validated according to the Food andDrug Administration guidelines for inter- and intra-assay coefficient of variation (CV) for Gas6 measurement in
human plasma and CSF (all CVs were within 15 withnegligible matrix effect) There was no cross-reactivity withhuman protein S (MP Biomedicals Solon OH USA) Thelowest quantification limit was 026 ngmL [24ndash26]
24 Statistical Analysis Data were collected and stored inan electronic database to be analyzed with the Statisticastatistical software program release 10 (StatSoft Tulsa OKUnited States) The Shapiro-Wilk test was performed toassess normality for any continuous variable analyzed Themeasures of central tendency anddispersion used throughoutthe paper weremeans and standard deviations for continuousvariables with normal distribution Accordingly normallydistributed variables were compared among groups bymeansof the Studentrsquos t-test ANOVA and post hoc comparisonsof the means (Tukeyrsquos post hoc test for nonhomogeneoussamplestest of Spjotvoll-Stoline) Categorical variables wereanalyzed with Pearson chi-square test and stepwise logisticregression to identify independent predictive factors of CSFGas6 variations A level of 005 (two-sided) was chosen toindicate statistical significance
3 Results
Mean CSF Gas6 concentration was nearly equal in CIS withrespect to RR-MS patients (78 plusmn 32 ngmL versus 79 plusmn 38Studentrsquos t-test 119875 = ns) but significantly higher in CISRR-MS (119899 = 65 37 females) patients with respect to controls(119899 = 40 22 females) (79 plusmn 37 ngmL versus 65 plusmn 24 ngmLresp 119875 lt 003) while plasma Gas6 concentration was notsignificantly different between groups (Studentrsquos t test 119875 =ns) (Figure 1)
Figure 2 shows mean CSF Gas6 concentration inrelationship to the duration of relapse CSF Gas6 concen-tration was significantly higher in shorter relapses (relapseslasting le60 days 87 plusmn 39 ngmL versus gt60 days
4 Mediators of Inflammation
Relapse duration
0
2
4
6
8
10
12
le60 days gt60 days Controls
lowast
lowast
CSF
[Gas
6] (n
gm
L)
(a)
0
2
4
6
8
10
12
le2 FS ge3 FS Controls
lowast
lowast
Number of FS involved
CSF
[Gas
6] (n
gm
L)
(b)
Relapse severity
0
2
4
6
8
10
12
ΔEDSS le 25 ΔEDSS ge 3 Controls
lowast
lowast
CSF
[Gas
6] (n
gm
L)
(c)
Figure 2 Gas6 concentration in CSF of patients withMS in relationto relapse features The graph shows means and standard deviationsof CSF Gas6 concentrations in relation to relapse duration le60days (dots) gt60 days (vertical lines) and controls (gray) (panel a)number of FS involved during the relapse le2 (dots) ge3 (verticallines) and controls (gray) (panel b) and EDSS score variationat maximum worsening (severity) le25 (dots) ge3 (vertical lines)and controls (gray) (panel c) lowastindicates 119875 le 005 in statisticalcomparison of the means (Tukeyrsquos post hoc test)
0
5
10
15
0 5 10 15 20 25 30 35 40plasma [Gas6] (ngmL)
CSF
[Gas
6] (n
gm
L)
Figure 3 Dissociation between CSF and plasma Gas6 concentra-tion The figure displays the absence of correlation between CSFand plasma Gas6 concentration measured simultaneously duringthe first relapse in MS patients The line indicates the regressionequation CSF Gas6 = 0007 sdot plasma Gas6 + 71 1199032 = 00003 119875 = ns
65 plusmn 26 ngmL and controls 65 plusmn 24 ngmL ANOVA119865 = 58 119875 lt 0004 Tukey post hoc test 119875 = 005) in relapseswith fewer FS involved (le2 FS 85 plusmn 38 ngmL versus ge3 FS56 plusmn 25 ngmL versus controls ANOVA 119865 = 67 119875 lt 0002Tukey post hoc test 119875 lt 005) and in relapses with lowerseverity (ΔEDSS le 25 88 plusmn 37 ngmL versus ge3 65 plusmn35 ngmL versus controls ANOVA 119865 = 66 119875 lt 0002Tukey post hoc test 119875 lt 0 04) In particular CSF Gas6concentration was inversely proportional to the EDSS scoreof the relapse (1198772 = 011 119875 lt 001) especially in pyramidalor cerebellar ones (1198772 = 0 25 119875 lt 0 003) On the otherhand CSF Gas6 concentration did not change accordingto completeness of recovery being similar in patients withor without complete recovery (82 plusmn 40 ngmL versus 76 plusmn35 versus controls ANOVA 119875 = ns) Alternatively CSFGas6 did not vary according to age therapy Link index(119875 = ns) Conversely plasma Gas6 concentration was notrelated to any of the clinical variables listed above (ANOVA119875 = ns) Indeed there was no relation between CSF andplasma Gas6 concentration (1198772 = 00003 119875 = ns) as shownin Figure 3 In stepwise logistic regression relapse durationand number of FS involved were significantly associatedwith Gas6 concentration (119865 133 and 65 resp 119875 lt 002)Treatment allocation according to relapse features is shownin Table 2
Follow-up data for a minimum of 25 years were availablefor 55 out of 65 patients and are presented in Table 3 Gas6concentration did not differ according to annualized relapserate either in CSF (Studentrsquos t test ge025year 84 plusmn 46 versuslt025year 80 plusmn 32 ngmL 119875 = ns) or in plasma (215 plusmn64 versus 213 plusmn 124 119875 = ns) and according to annualizedEDSS progression either in CSF (ge02 EDSS pointsyear 79 plusmn31 versus lt02 81 plusmn 48 119875 = ns) or in plasma (218 plusmn 88versus 234 plusmn 76 ngmL 119875 = ns) Moreover neither CSF norplasma Gas6 concentration correlated to annualized relapse
Mediators of Inflammation 5
Table 2 Treatment allocation according to relapse features
Relapse features Type of treatment1205942 analysis
No Oral PDNlowast IVMPlowastlowast
Duration le60gt60 days 2210 75 165 115 119875 = nsNumber of FS involved (le2gt2) 267 84 164 088 119875 = nsSeverity ΔEDSS (le25gt25) 2211 75 119 078 119875 = nsPDN prednisone IVMP intravenous methylprednisone FS functional system and ΔEDSS variation from baseline of Expanded-Disability-Status ScalelowastOral prednisone was administered at 50mgday for the first 5 days then 25mgday for the following 5 days and 125mgday for further 5 days and thendiscontinuedlowastlowastIntra venous methylprednisone was administered at 1000mgday iv infusion for 5 consecutive days
Table 3 Follow-up cohort features
M plusmn SD MedianFollow-up duration (years) 59 plusmn 18 52Annualized relapse rate (relapseyear) 032 plusmn 025 025Annualized relapse progression (ΔEDSSyear) 16 plusmn 10 10
rate or EDSS progression in linear regression analysis (datanot shown 119875 = ns)
4 Discussion
The present paper shows that CSF Gas6 concentration isslightly higher in patients suffering a first relapse of MS thanin control patients Interestingly a significant and substantialincrease in CSF was observed in patients suffering fromshorter less severe and less FS involved relapses Converselypatients who suffered from more severe relapse did notshow any variations of CSF Gas6 concentration with respectto control subjects This apparent paradox is reconciliatedby considering Gas6 as a protective protein able to limitinflammatory demyelination This hypothesis is sustained byseveral in vitro and in vivo studies that indicate forGas6 a roleas inhibitor of macrophages activation [7 9] and as a survivalfactor for neurons and oligodendrocytes [11 15 16] IndeedGas6 knock-out mice challenged with cuprizone displayincreased demyelination damage with greater lesions anda higher number of apoptotic oligodendrocytes infiltratingmacrophages and microglial cells [6] In absence of Gas6there is a delay in remyelination of the lesions induced bycuprizone [17] Moreover Gas6 concentration is raised in theCSF of patients suffering from CIDP a chronic autoimmunedemyelinating disease of the peripheral nerves which sharessome similarities with MS [26] In summary our results fitwell the data in the literature suggesting that MS patientswith higher CSF Gas6 might be able to limit the extentof inflammatory demyelination On the other hand Gas6elevation in CSF seems to be related to relapse features ratherthan to the presence of MS itself Additionally since analtered Gas6TAM ratio has been evidenced in establishedMS lesions [27] an impaired expression of TAM-receptor inabsence of alteration of Gas6 concentration may concurr toinfluence the disease course Further studies are needed toaddress this hypothesis
Themechanisms by which Gas6 might exert this putativeprotection by the effects of inflammatory demyelinationremain speculative Gas6 could act on macrophages andorglial cells this hypothesis is supported by the observationsindicating that Gas6 downregulates the production of proin-flammatory cytokines such as IL-6 and TNF-alpha andenhances the phagocytosis of cellular debris and apoptoticbodies through Mer receptor by activated macrophagesdendritic and microglial cells [7 9 28ndash30] Thus Gas6 maybe able to limit the activation of the innate immune responseand consequently the aggression to myelin fibers favoringcell debris and apoptotic bodies clearance which are in turninflammatory triggers Since mononuclear activation withcytokine production is crucial in the amplification of theautoimmune aggression to myelin and the failure to clearapoptotic cells iswidely considered a trigger of autoimmunityGas6 may have an important role in this context Alterna-tively Gas6TAM interaction could be relevant in processesof recovery after inflammatory demyelination since it is welldemonstrated that it enhances the survival of oligodendro-cytes and neurons [11 15] as happening for other cell lines[31] and mice lacking Gas6 have demyelinating lesions witha higher proportion of apoptotic oligodendrocytes duringcuprizone-induced demyelination [6] Consequently Gas6may participate actively in oligodendrocyte survival aftermyelin damage favoring a prompt repair It is conceivable thatpatients who suffer frommore severe relapse and who do notpresent an increase in CSF Gas6 concentration may have adefect in Gas6 expression and consequently present a defectin mechanisms of self-limitation to immune aggression toCNS or in myelin damage repair It must be pointed outhowever that we were unable to identify a relation betweenGas6 concentration in CSF and lack of complete recoveryafter the relapse which could be considered the clinicalcorrelate of an efficient recovery system
The putative role of Gas6 in the control of immuneaggression in the nervous system is strengthened by the find-ing that plasma and CSF Gas6 concentration are unrelatedin MS patients therefore the increase of Gas6 in the CSFwas not dependent on an increased plasma concentrationandor the breakdown of the blood-brain barrier but likelyon production by inflammatory cells within the CNS Theseresults are in line with previous results from our group con-cerning autoimmune polyneuropathies [26 32] Moreoverthe relation between CSF Gas6 and EDSS score was stricterin pyramidal and cerebellar relapses possibly because EDSS
6 Mediators of Inflammation
is more sensitive to the damage extension in pyramidal andcerebellar relapses with respect to other symptoms that aremainly subjective and less easy to score
Although the sample size was small and only a fewpatients had an active disease with a significant number ofrelapses or severe disability progression our data suggest thatmeasuring Gas6 concentration in CSF of MS patients canonly be useful to predict the evolution of a first relapse but notthe subsequent disease course Thus Gas6 may be importantin limiting the acute inflammatory demyelination during arelapse but less than so in the pathogenic mechanisms thatdetermine relapse recurrences and cumulative disability
In conclusion CSF Gas6 protein concentration is signifi-cantly increased inmilderMS relapses suggesting an involve-ment of this protein in limiting autoimmune demyelinatingprocesses or in favouring myelin repair after damage Gas6measurement in CSF during a relapse can be useful to predicthow a relapse will evolve but not the disease course in thelong term Further studies are warranted to clarify the Gas6and TAM receptors role in the pathogenesis of MS-relapsesand its clinical applications
Conflict of Interests
The authors declare no conflict of interest
Acknowledgments
This work was supported by (Fondazione Italiana SclerosiMultiplaItalian Multiple Sclerosis Foundation) FISM 2010research Grant During the paper preparation ProfessorFrancescoMonaco prematurely died All investigatorswish todedicate this paper to his memory honouring his dedicationto clinical research in neurological diseases
References
[1] D A Hafler J M Slavik D E Anderson K C OrsquoConnor P DeJager and C Baecher-Allan ldquoMultiple sclerosisrdquo ImmunologicalReviews vol 204 pp 208ndash231 2005
[2] GManfioletti C Brancolini G Avanzi and C Schneider ldquoTheprotein encoded by a growth arrest-specific gene (gas6) is a newmember of the vitamin K-dependent proteins related to proteinS a negative coregulator in the blood coagulation cascaderdquoMolecular and Cellular Biology vol 13 no 8 pp 4976ndash49851993
[3] P J Godowski M R Mark J Chen M D Sadick H Raaband R G Hammonds ldquoReevaluation of the roles of protein Sand Gas6 as ligands for the receptor tyrosine kinase RseTyro3rdquo Cell vol 82 no 3 pp 355ndash358 1995
[4] B C Varnum C Young G Elliot et al ldquoAxl receptor tyrosinekinase stimulated by the vitamin K-dependent protein encodedby growth-arrest-specific gene 6rdquo Nature vol 373 no 6515 pp623ndash626 1995
[5] D R Joseph ldquoSequence and functional relationships betweenandrogen-binding proteinsex hormone-binding globulin andits homologs protein S Gas6 laminin and agrinrdquo Steroids vol62 no 8-9 pp 578ndash588 1997
[6] M D Binder and T J Kilpatrick ldquoTAM receptor signalling anddemyelinationrdquo NeuroSignals vol 17 no 4 pp 277ndash287 2009
[7] G Lemke and Q Lu ldquoMacrophage regulation by Tyro 3 familyreceptorsrdquoCurrent Opinion in Immunology vol 15 no 1 pp 31ndash36 2003
[8] Q Lu and G Lemke ldquoHomeostatic regulation of the immunesystem by receptor tyrosine kinases of the Tyro 3 familyrdquoScience vol 293 no 5528 pp 306ndash311 2001
[9] F Alciato P P Sainaghi D Sola L Castello and G C AvanzildquoTNF-120572 IL-6 and IL-1 expression is inhibited by GAS6 inmonocytesmacrophagesrdquo Journal of Leukocyte Biology vol 87no 5 pp 869ndash875 2010
[10] A L Prieto J LWeber S TracyM J Heeb and C Lai ldquoGas6 aligand for the receptor protein-tyrosine kinase Tyro-3 is widelyexpressed in the central nervous systemrdquo Brain Research vol816 no 2 pp 646ndash661 1999
[11] H Funakoshi T Yonemasu T Nakano K Matumoto and TNakamura ldquoIdentification of Gas6 a putative ligand for Sky andAxl receptor tyrosine kinases as a novel neurotrophic factor forhippocampal neuronsrdquo Journal of Neuroscience Research vol68 no 2 pp 150ndash160 2002
[12] A L Prieto S OrsquoDell B Varnum and C Lai ldquoLocalizationand signaling of the receptor protein tyrosine kinase Tyro3 incortical and hippocampal neuronsrdquo Neuroscience vol 150 no2 pp 319ndash334 2007
[13] T Yagami K Ueda K Asakura et al ldquoGas6 rescues corticalneurons from amyloid 120573 protein-induced apoptosisrdquo Neu-ropharmacology vol 43 no 8 pp 1289ndash1296 2002
[14] R H Li J Chen G Hammonds et al ldquoIdentification ofGas6 as a growth factor for human Schwann cellsrdquo Journal ofNeuroscience vol 16 no 6 pp 2012ndash2019 1996
[15] S L Shankar K OrsquoGuin M Cammer et al ldquoThe growtharrest-specific gene product Gas6 promotes the survival ofhuman oligodendrocytes via a phosphatidylinositol 3-kinase-dependent pathwayrdquo Journal of Neuroscience vol 23 no 10 pp4208ndash4218 2003
[16] S L Shankar K OrsquoGuin M Kim et al ldquoGas6Axl signalingactivates the phosphatidylinositol 3-kinaseAkt1 survival path-way to protect oligodendrocytes from tumor necrosis factor120572-induced apoptosisrdquo Journal of Neuroscience vol 26 no 21 pp5638ndash5648 2006
[17] M D Binder J Xiao D Kemper G Z M Ma S S Murrayand T J Kilpatrick ldquoGas6 increases myelination by oligoden-drocytes and its deficiency delays recovery following cuprizone-induced demyelinationrdquo PLoS ONE vol 6 no 3 article e177272011
[18] V Tsiperson X Li G J Schwartz C S Raine and B Shafit-Zagardo ldquoGAS6 enhances repair following cuprizone-induceddemyelinationrdquo PLoS ONE vol 5 no 12 article e15748 2010
[19] D Miller F Barkhof X Montalban A Thompson and MFilippi ldquoClinically isolated syndromes suggestive of multiplesclerosis part I natural history pathogenesis diagnosis andprognosisrdquo Lancet Neurology vol 4 no 5 pp 281ndash288 2005
[20] W I McDonald A Compston G Edan et al ldquoRecommendeddiagnostic criteria for multiple sclerosis Guidelines from theInternational Panel on the Diagnosis of Multiple SclerosisrdquoAnnals of Neurology vol 50 no 1 pp 121ndash127 2001
[21] G A Schumacker G Beebe R F Kibler et al ldquoProblems ofexperimental trials of therapy in multiple sclerosis report bythe panel on the evaluation of experimental trials of therapy inmultiple sclerosisrdquo Annals of the New York Academy of Sciencesvol 122 pp 552ndash568 1965
[22] M A Leone S Bonissoni L Collimedaglia et al ldquoFactors pre-dicting incomplete recovery from relapses in multiple sclerosis
Mediators of Inflammation 7
A Prospective Studyrdquo Multiple Sclerosis vol 14 no 4 pp 485ndash493 2008
[23] J F Kurtzke ldquoRating neurologic impairment in multiple sclero-sis an expanded disability status scale (EDSS)rdquo Neurology vol33 no 11 pp 1444ndash1452 1983
[24] F Alciato P P Sainaghi L Castello L Bergamasco SCarnieletto and G C Avanzi ldquoDevelopment and validation ofan ELISA method for detection of Growth Arrest Specific 6(GAS6) protein in human plasmardquo Journal of Immunoassay andImmunochemistry vol 29 no 2 pp 167ndash180 2008
[25] P P Sainaghi F Alciato S Carnieletto et al ldquoGas6 evaluationin patients with acute dyspnea due to suspected pulmonaryembolismrdquo Respiratory Medicine vol 103 no 4 pp 589ndash5942009
[26] P P Sainaghi L Collimedaglia F Alciato et al ldquoEleva-tion of Gas6 protein concentration in cerebrospinal fluid ofpatients with chronic inflammatory demyelinating polyneu-ropathy (CIDP)rdquo Journal of the Neurological Sciences vol 269no 1-2 pp 138ndash142 2008
[27] J G Weinger K M Omari K Marsden C S Raine and BShafit-Zagardo ldquoUp-regulation of soluble Axl andMer receptortyrosine kinases negatively correlates with Gas6 in establishedmultiple sclerosis lesionsrdquo American Journal of Pathology vol175 no 1 pp 283ndash293 2009
[28] WH Shao Y Zhen R A Eisenberg and P L Cohen ldquoTheMerreceptor tyrosine kinase is expressed on discrete macrophagesubpopulations and mainly uses Gas6 as its ligand for uptake ofapoptotic cellsrdquoClinical Immunology vol 133 no 1 pp 138ndash1442009
[29] C Grommes C Y D Lee B L Wilkinson et al ldquoRegulation ofmicroglial phagocytosis and inflammatory gene expression byGas6 acting on the AxlMer family of tyrosine kinasesrdquo Journalof NeuroImmune Pharmacology vol 3 no 2 pp 130ndash140 2008
[30] P Sen M A Wallet Z Yi et al ldquoApoptotic cells induce Mertyrosine kinase-dependent blockade of NF-120581B activation indendritic cellsrdquo Blood vol 109 no 2 pp 653ndash660 2007
[31] P P Sainaghi L Castello L BergamascoMGalletti P Bellostaand G C Avanzi ldquoGas6 induces proliferation in prostatecarcinoma cell lines expressing the Axl receptorrdquo Journal ofCellular Physiology vol 204 no 1 pp 36ndash44 2005
[32] P P Sainaghi L Collimedaglia F Alciato et al ldquoThe expressionpattern of inflammatorymediators in cerebrospinal fluid differ-entiates Guillain-Barre syndrome from chronic inflammatorydemyelinating polyneuropathyrdquoCytokine vol 51 no 2 pp 138ndash143 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
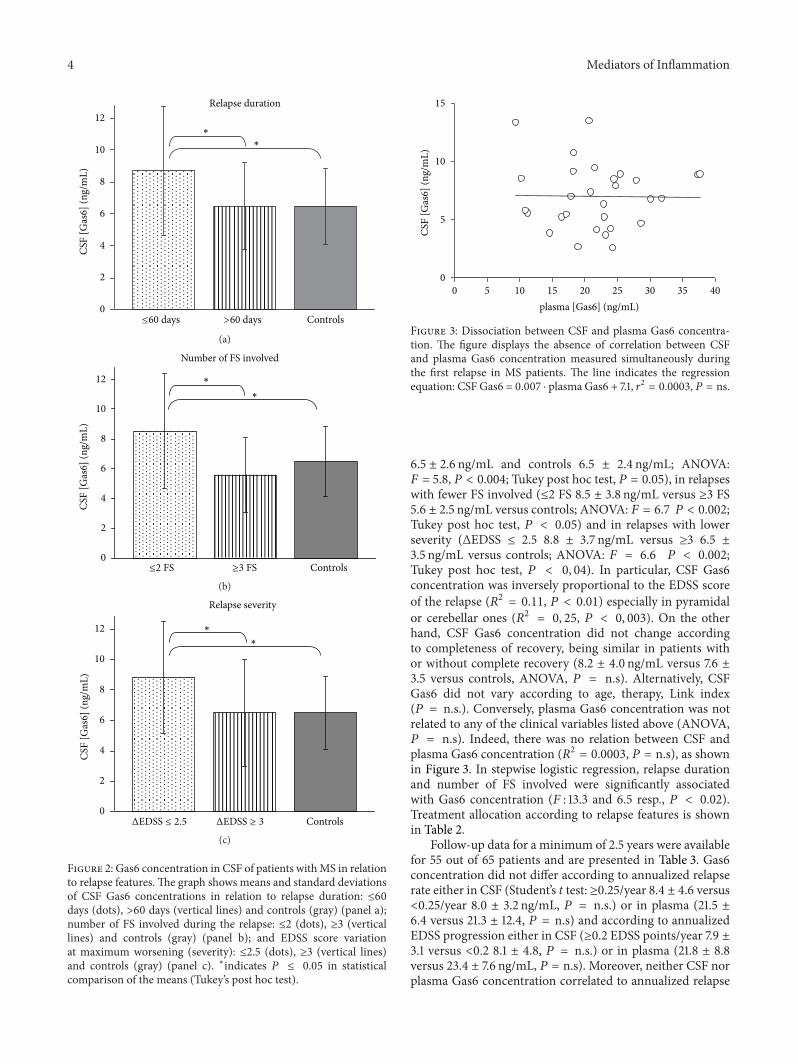
4 Mediators of Inflammation
Relapse duration
0
2
4
6
8
10
12
le60 days gt60 days Controls
lowast
lowast
CSF
[Gas
6] (n
gm
L)
(a)
0
2
4
6
8
10
12
le2 FS ge3 FS Controls
lowast
lowast
Number of FS involved
CSF
[Gas
6] (n
gm
L)
(b)
Relapse severity
0
2
4
6
8
10
12
ΔEDSS le 25 ΔEDSS ge 3 Controls
lowast
lowast
CSF
[Gas
6] (n
gm
L)
(c)
Figure 2 Gas6 concentration in CSF of patients withMS in relationto relapse features The graph shows means and standard deviationsof CSF Gas6 concentrations in relation to relapse duration le60days (dots) gt60 days (vertical lines) and controls (gray) (panel a)number of FS involved during the relapse le2 (dots) ge3 (verticallines) and controls (gray) (panel b) and EDSS score variationat maximum worsening (severity) le25 (dots) ge3 (vertical lines)and controls (gray) (panel c) lowastindicates 119875 le 005 in statisticalcomparison of the means (Tukeyrsquos post hoc test)
0
5
10
15
0 5 10 15 20 25 30 35 40plasma [Gas6] (ngmL)
CSF
[Gas
6] (n
gm
L)
Figure 3 Dissociation between CSF and plasma Gas6 concentra-tion The figure displays the absence of correlation between CSFand plasma Gas6 concentration measured simultaneously duringthe first relapse in MS patients The line indicates the regressionequation CSF Gas6 = 0007 sdot plasma Gas6 + 71 1199032 = 00003 119875 = ns
65 plusmn 26 ngmL and controls 65 plusmn 24 ngmL ANOVA119865 = 58 119875 lt 0004 Tukey post hoc test 119875 = 005) in relapseswith fewer FS involved (le2 FS 85 plusmn 38 ngmL versus ge3 FS56 plusmn 25 ngmL versus controls ANOVA 119865 = 67 119875 lt 0002Tukey post hoc test 119875 lt 005) and in relapses with lowerseverity (ΔEDSS le 25 88 plusmn 37 ngmL versus ge3 65 plusmn35 ngmL versus controls ANOVA 119865 = 66 119875 lt 0002Tukey post hoc test 119875 lt 0 04) In particular CSF Gas6concentration was inversely proportional to the EDSS scoreof the relapse (1198772 = 011 119875 lt 001) especially in pyramidalor cerebellar ones (1198772 = 0 25 119875 lt 0 003) On the otherhand CSF Gas6 concentration did not change accordingto completeness of recovery being similar in patients withor without complete recovery (82 plusmn 40 ngmL versus 76 plusmn35 versus controls ANOVA 119875 = ns) Alternatively CSFGas6 did not vary according to age therapy Link index(119875 = ns) Conversely plasma Gas6 concentration was notrelated to any of the clinical variables listed above (ANOVA119875 = ns) Indeed there was no relation between CSF andplasma Gas6 concentration (1198772 = 00003 119875 = ns) as shownin Figure 3 In stepwise logistic regression relapse durationand number of FS involved were significantly associatedwith Gas6 concentration (119865 133 and 65 resp 119875 lt 002)Treatment allocation according to relapse features is shownin Table 2
Follow-up data for a minimum of 25 years were availablefor 55 out of 65 patients and are presented in Table 3 Gas6concentration did not differ according to annualized relapserate either in CSF (Studentrsquos t test ge025year 84 plusmn 46 versuslt025year 80 plusmn 32 ngmL 119875 = ns) or in plasma (215 plusmn64 versus 213 plusmn 124 119875 = ns) and according to annualizedEDSS progression either in CSF (ge02 EDSS pointsyear 79 plusmn31 versus lt02 81 plusmn 48 119875 = ns) or in plasma (218 plusmn 88versus 234 plusmn 76 ngmL 119875 = ns) Moreover neither CSF norplasma Gas6 concentration correlated to annualized relapse
Mediators of Inflammation 5
Table 2 Treatment allocation according to relapse features
Relapse features Type of treatment1205942 analysis
No Oral PDNlowast IVMPlowastlowast
Duration le60gt60 days 2210 75 165 115 119875 = nsNumber of FS involved (le2gt2) 267 84 164 088 119875 = nsSeverity ΔEDSS (le25gt25) 2211 75 119 078 119875 = nsPDN prednisone IVMP intravenous methylprednisone FS functional system and ΔEDSS variation from baseline of Expanded-Disability-Status ScalelowastOral prednisone was administered at 50mgday for the first 5 days then 25mgday for the following 5 days and 125mgday for further 5 days and thendiscontinuedlowastlowastIntra venous methylprednisone was administered at 1000mgday iv infusion for 5 consecutive days
Table 3 Follow-up cohort features
M plusmn SD MedianFollow-up duration (years) 59 plusmn 18 52Annualized relapse rate (relapseyear) 032 plusmn 025 025Annualized relapse progression (ΔEDSSyear) 16 plusmn 10 10
rate or EDSS progression in linear regression analysis (datanot shown 119875 = ns)
4 Discussion
The present paper shows that CSF Gas6 concentration isslightly higher in patients suffering a first relapse of MS thanin control patients Interestingly a significant and substantialincrease in CSF was observed in patients suffering fromshorter less severe and less FS involved relapses Converselypatients who suffered from more severe relapse did notshow any variations of CSF Gas6 concentration with respectto control subjects This apparent paradox is reconciliatedby considering Gas6 as a protective protein able to limitinflammatory demyelination This hypothesis is sustained byseveral in vitro and in vivo studies that indicate forGas6 a roleas inhibitor of macrophages activation [7 9] and as a survivalfactor for neurons and oligodendrocytes [11 15 16] IndeedGas6 knock-out mice challenged with cuprizone displayincreased demyelination damage with greater lesions anda higher number of apoptotic oligodendrocytes infiltratingmacrophages and microglial cells [6] In absence of Gas6there is a delay in remyelination of the lesions induced bycuprizone [17] Moreover Gas6 concentration is raised in theCSF of patients suffering from CIDP a chronic autoimmunedemyelinating disease of the peripheral nerves which sharessome similarities with MS [26] In summary our results fitwell the data in the literature suggesting that MS patientswith higher CSF Gas6 might be able to limit the extentof inflammatory demyelination On the other hand Gas6elevation in CSF seems to be related to relapse features ratherthan to the presence of MS itself Additionally since analtered Gas6TAM ratio has been evidenced in establishedMS lesions [27] an impaired expression of TAM-receptor inabsence of alteration of Gas6 concentration may concurr toinfluence the disease course Further studies are needed toaddress this hypothesis
Themechanisms by which Gas6 might exert this putativeprotection by the effects of inflammatory demyelinationremain speculative Gas6 could act on macrophages andorglial cells this hypothesis is supported by the observationsindicating that Gas6 downregulates the production of proin-flammatory cytokines such as IL-6 and TNF-alpha andenhances the phagocytosis of cellular debris and apoptoticbodies through Mer receptor by activated macrophagesdendritic and microglial cells [7 9 28ndash30] Thus Gas6 maybe able to limit the activation of the innate immune responseand consequently the aggression to myelin fibers favoringcell debris and apoptotic bodies clearance which are in turninflammatory triggers Since mononuclear activation withcytokine production is crucial in the amplification of theautoimmune aggression to myelin and the failure to clearapoptotic cells iswidely considered a trigger of autoimmunityGas6 may have an important role in this context Alterna-tively Gas6TAM interaction could be relevant in processesof recovery after inflammatory demyelination since it is welldemonstrated that it enhances the survival of oligodendro-cytes and neurons [11 15] as happening for other cell lines[31] and mice lacking Gas6 have demyelinating lesions witha higher proportion of apoptotic oligodendrocytes duringcuprizone-induced demyelination [6] Consequently Gas6may participate actively in oligodendrocyte survival aftermyelin damage favoring a prompt repair It is conceivable thatpatients who suffer frommore severe relapse and who do notpresent an increase in CSF Gas6 concentration may have adefect in Gas6 expression and consequently present a defectin mechanisms of self-limitation to immune aggression toCNS or in myelin damage repair It must be pointed outhowever that we were unable to identify a relation betweenGas6 concentration in CSF and lack of complete recoveryafter the relapse which could be considered the clinicalcorrelate of an efficient recovery system
The putative role of Gas6 in the control of immuneaggression in the nervous system is strengthened by the find-ing that plasma and CSF Gas6 concentration are unrelatedin MS patients therefore the increase of Gas6 in the CSFwas not dependent on an increased plasma concentrationandor the breakdown of the blood-brain barrier but likelyon production by inflammatory cells within the CNS Theseresults are in line with previous results from our group con-cerning autoimmune polyneuropathies [26 32] Moreoverthe relation between CSF Gas6 and EDSS score was stricterin pyramidal and cerebellar relapses possibly because EDSS
6 Mediators of Inflammation
is more sensitive to the damage extension in pyramidal andcerebellar relapses with respect to other symptoms that aremainly subjective and less easy to score
Although the sample size was small and only a fewpatients had an active disease with a significant number ofrelapses or severe disability progression our data suggest thatmeasuring Gas6 concentration in CSF of MS patients canonly be useful to predict the evolution of a first relapse but notthe subsequent disease course Thus Gas6 may be importantin limiting the acute inflammatory demyelination during arelapse but less than so in the pathogenic mechanisms thatdetermine relapse recurrences and cumulative disability
In conclusion CSF Gas6 protein concentration is signifi-cantly increased inmilderMS relapses suggesting an involve-ment of this protein in limiting autoimmune demyelinatingprocesses or in favouring myelin repair after damage Gas6measurement in CSF during a relapse can be useful to predicthow a relapse will evolve but not the disease course in thelong term Further studies are warranted to clarify the Gas6and TAM receptors role in the pathogenesis of MS-relapsesand its clinical applications
Conflict of Interests
The authors declare no conflict of interest
Acknowledgments
This work was supported by (Fondazione Italiana SclerosiMultiplaItalian Multiple Sclerosis Foundation) FISM 2010research Grant During the paper preparation ProfessorFrancescoMonaco prematurely died All investigatorswish todedicate this paper to his memory honouring his dedicationto clinical research in neurological diseases
References
[1] D A Hafler J M Slavik D E Anderson K C OrsquoConnor P DeJager and C Baecher-Allan ldquoMultiple sclerosisrdquo ImmunologicalReviews vol 204 pp 208ndash231 2005
[2] GManfioletti C Brancolini G Avanzi and C Schneider ldquoTheprotein encoded by a growth arrest-specific gene (gas6) is a newmember of the vitamin K-dependent proteins related to proteinS a negative coregulator in the blood coagulation cascaderdquoMolecular and Cellular Biology vol 13 no 8 pp 4976ndash49851993
[3] P J Godowski M R Mark J Chen M D Sadick H Raaband R G Hammonds ldquoReevaluation of the roles of protein Sand Gas6 as ligands for the receptor tyrosine kinase RseTyro3rdquo Cell vol 82 no 3 pp 355ndash358 1995
[4] B C Varnum C Young G Elliot et al ldquoAxl receptor tyrosinekinase stimulated by the vitamin K-dependent protein encodedby growth-arrest-specific gene 6rdquo Nature vol 373 no 6515 pp623ndash626 1995
[5] D R Joseph ldquoSequence and functional relationships betweenandrogen-binding proteinsex hormone-binding globulin andits homologs protein S Gas6 laminin and agrinrdquo Steroids vol62 no 8-9 pp 578ndash588 1997
[6] M D Binder and T J Kilpatrick ldquoTAM receptor signalling anddemyelinationrdquo NeuroSignals vol 17 no 4 pp 277ndash287 2009
[7] G Lemke and Q Lu ldquoMacrophage regulation by Tyro 3 familyreceptorsrdquoCurrent Opinion in Immunology vol 15 no 1 pp 31ndash36 2003
[8] Q Lu and G Lemke ldquoHomeostatic regulation of the immunesystem by receptor tyrosine kinases of the Tyro 3 familyrdquoScience vol 293 no 5528 pp 306ndash311 2001
[9] F Alciato P P Sainaghi D Sola L Castello and G C AvanzildquoTNF-120572 IL-6 and IL-1 expression is inhibited by GAS6 inmonocytesmacrophagesrdquo Journal of Leukocyte Biology vol 87no 5 pp 869ndash875 2010
[10] A L Prieto J LWeber S TracyM J Heeb and C Lai ldquoGas6 aligand for the receptor protein-tyrosine kinase Tyro-3 is widelyexpressed in the central nervous systemrdquo Brain Research vol816 no 2 pp 646ndash661 1999
[11] H Funakoshi T Yonemasu T Nakano K Matumoto and TNakamura ldquoIdentification of Gas6 a putative ligand for Sky andAxl receptor tyrosine kinases as a novel neurotrophic factor forhippocampal neuronsrdquo Journal of Neuroscience Research vol68 no 2 pp 150ndash160 2002
[12] A L Prieto S OrsquoDell B Varnum and C Lai ldquoLocalizationand signaling of the receptor protein tyrosine kinase Tyro3 incortical and hippocampal neuronsrdquo Neuroscience vol 150 no2 pp 319ndash334 2007
[13] T Yagami K Ueda K Asakura et al ldquoGas6 rescues corticalneurons from amyloid 120573 protein-induced apoptosisrdquo Neu-ropharmacology vol 43 no 8 pp 1289ndash1296 2002
[14] R H Li J Chen G Hammonds et al ldquoIdentification ofGas6 as a growth factor for human Schwann cellsrdquo Journal ofNeuroscience vol 16 no 6 pp 2012ndash2019 1996
[15] S L Shankar K OrsquoGuin M Cammer et al ldquoThe growtharrest-specific gene product Gas6 promotes the survival ofhuman oligodendrocytes via a phosphatidylinositol 3-kinase-dependent pathwayrdquo Journal of Neuroscience vol 23 no 10 pp4208ndash4218 2003
[16] S L Shankar K OrsquoGuin M Kim et al ldquoGas6Axl signalingactivates the phosphatidylinositol 3-kinaseAkt1 survival path-way to protect oligodendrocytes from tumor necrosis factor120572-induced apoptosisrdquo Journal of Neuroscience vol 26 no 21 pp5638ndash5648 2006
[17] M D Binder J Xiao D Kemper G Z M Ma S S Murrayand T J Kilpatrick ldquoGas6 increases myelination by oligoden-drocytes and its deficiency delays recovery following cuprizone-induced demyelinationrdquo PLoS ONE vol 6 no 3 article e177272011
[18] V Tsiperson X Li G J Schwartz C S Raine and B Shafit-Zagardo ldquoGAS6 enhances repair following cuprizone-induceddemyelinationrdquo PLoS ONE vol 5 no 12 article e15748 2010
[19] D Miller F Barkhof X Montalban A Thompson and MFilippi ldquoClinically isolated syndromes suggestive of multiplesclerosis part I natural history pathogenesis diagnosis andprognosisrdquo Lancet Neurology vol 4 no 5 pp 281ndash288 2005
[20] W I McDonald A Compston G Edan et al ldquoRecommendeddiagnostic criteria for multiple sclerosis Guidelines from theInternational Panel on the Diagnosis of Multiple SclerosisrdquoAnnals of Neurology vol 50 no 1 pp 121ndash127 2001
[21] G A Schumacker G Beebe R F Kibler et al ldquoProblems ofexperimental trials of therapy in multiple sclerosis report bythe panel on the evaluation of experimental trials of therapy inmultiple sclerosisrdquo Annals of the New York Academy of Sciencesvol 122 pp 552ndash568 1965
[22] M A Leone S Bonissoni L Collimedaglia et al ldquoFactors pre-dicting incomplete recovery from relapses in multiple sclerosis
Mediators of Inflammation 7
A Prospective Studyrdquo Multiple Sclerosis vol 14 no 4 pp 485ndash493 2008
[23] J F Kurtzke ldquoRating neurologic impairment in multiple sclero-sis an expanded disability status scale (EDSS)rdquo Neurology vol33 no 11 pp 1444ndash1452 1983
[24] F Alciato P P Sainaghi L Castello L Bergamasco SCarnieletto and G C Avanzi ldquoDevelopment and validation ofan ELISA method for detection of Growth Arrest Specific 6(GAS6) protein in human plasmardquo Journal of Immunoassay andImmunochemistry vol 29 no 2 pp 167ndash180 2008
[25] P P Sainaghi F Alciato S Carnieletto et al ldquoGas6 evaluationin patients with acute dyspnea due to suspected pulmonaryembolismrdquo Respiratory Medicine vol 103 no 4 pp 589ndash5942009
[26] P P Sainaghi L Collimedaglia F Alciato et al ldquoEleva-tion of Gas6 protein concentration in cerebrospinal fluid ofpatients with chronic inflammatory demyelinating polyneu-ropathy (CIDP)rdquo Journal of the Neurological Sciences vol 269no 1-2 pp 138ndash142 2008
[27] J G Weinger K M Omari K Marsden C S Raine and BShafit-Zagardo ldquoUp-regulation of soluble Axl andMer receptortyrosine kinases negatively correlates with Gas6 in establishedmultiple sclerosis lesionsrdquo American Journal of Pathology vol175 no 1 pp 283ndash293 2009
[28] WH Shao Y Zhen R A Eisenberg and P L Cohen ldquoTheMerreceptor tyrosine kinase is expressed on discrete macrophagesubpopulations and mainly uses Gas6 as its ligand for uptake ofapoptotic cellsrdquoClinical Immunology vol 133 no 1 pp 138ndash1442009
[29] C Grommes C Y D Lee B L Wilkinson et al ldquoRegulation ofmicroglial phagocytosis and inflammatory gene expression byGas6 acting on the AxlMer family of tyrosine kinasesrdquo Journalof NeuroImmune Pharmacology vol 3 no 2 pp 130ndash140 2008
[30] P Sen M A Wallet Z Yi et al ldquoApoptotic cells induce Mertyrosine kinase-dependent blockade of NF-120581B activation indendritic cellsrdquo Blood vol 109 no 2 pp 653ndash660 2007
[31] P P Sainaghi L Castello L BergamascoMGalletti P Bellostaand G C Avanzi ldquoGas6 induces proliferation in prostatecarcinoma cell lines expressing the Axl receptorrdquo Journal ofCellular Physiology vol 204 no 1 pp 36ndash44 2005
[32] P P Sainaghi L Collimedaglia F Alciato et al ldquoThe expressionpattern of inflammatorymediators in cerebrospinal fluid differ-entiates Guillain-Barre syndrome from chronic inflammatorydemyelinating polyneuropathyrdquoCytokine vol 51 no 2 pp 138ndash143 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Mediators of Inflammation 5
Table 2 Treatment allocation according to relapse features
Relapse features Type of treatment1205942 analysis
No Oral PDNlowast IVMPlowastlowast
Duration le60gt60 days 2210 75 165 115 119875 = nsNumber of FS involved (le2gt2) 267 84 164 088 119875 = nsSeverity ΔEDSS (le25gt25) 2211 75 119 078 119875 = nsPDN prednisone IVMP intravenous methylprednisone FS functional system and ΔEDSS variation from baseline of Expanded-Disability-Status ScalelowastOral prednisone was administered at 50mgday for the first 5 days then 25mgday for the following 5 days and 125mgday for further 5 days and thendiscontinuedlowastlowastIntra venous methylprednisone was administered at 1000mgday iv infusion for 5 consecutive days
Table 3 Follow-up cohort features
M plusmn SD MedianFollow-up duration (years) 59 plusmn 18 52Annualized relapse rate (relapseyear) 032 plusmn 025 025Annualized relapse progression (ΔEDSSyear) 16 plusmn 10 10
rate or EDSS progression in linear regression analysis (datanot shown 119875 = ns)
4 Discussion
The present paper shows that CSF Gas6 concentration isslightly higher in patients suffering a first relapse of MS thanin control patients Interestingly a significant and substantialincrease in CSF was observed in patients suffering fromshorter less severe and less FS involved relapses Converselypatients who suffered from more severe relapse did notshow any variations of CSF Gas6 concentration with respectto control subjects This apparent paradox is reconciliatedby considering Gas6 as a protective protein able to limitinflammatory demyelination This hypothesis is sustained byseveral in vitro and in vivo studies that indicate forGas6 a roleas inhibitor of macrophages activation [7 9] and as a survivalfactor for neurons and oligodendrocytes [11 15 16] IndeedGas6 knock-out mice challenged with cuprizone displayincreased demyelination damage with greater lesions anda higher number of apoptotic oligodendrocytes infiltratingmacrophages and microglial cells [6] In absence of Gas6there is a delay in remyelination of the lesions induced bycuprizone [17] Moreover Gas6 concentration is raised in theCSF of patients suffering from CIDP a chronic autoimmunedemyelinating disease of the peripheral nerves which sharessome similarities with MS [26] In summary our results fitwell the data in the literature suggesting that MS patientswith higher CSF Gas6 might be able to limit the extentof inflammatory demyelination On the other hand Gas6elevation in CSF seems to be related to relapse features ratherthan to the presence of MS itself Additionally since analtered Gas6TAM ratio has been evidenced in establishedMS lesions [27] an impaired expression of TAM-receptor inabsence of alteration of Gas6 concentration may concurr toinfluence the disease course Further studies are needed toaddress this hypothesis
Themechanisms by which Gas6 might exert this putativeprotection by the effects of inflammatory demyelinationremain speculative Gas6 could act on macrophages andorglial cells this hypothesis is supported by the observationsindicating that Gas6 downregulates the production of proin-flammatory cytokines such as IL-6 and TNF-alpha andenhances the phagocytosis of cellular debris and apoptoticbodies through Mer receptor by activated macrophagesdendritic and microglial cells [7 9 28ndash30] Thus Gas6 maybe able to limit the activation of the innate immune responseand consequently the aggression to myelin fibers favoringcell debris and apoptotic bodies clearance which are in turninflammatory triggers Since mononuclear activation withcytokine production is crucial in the amplification of theautoimmune aggression to myelin and the failure to clearapoptotic cells iswidely considered a trigger of autoimmunityGas6 may have an important role in this context Alterna-tively Gas6TAM interaction could be relevant in processesof recovery after inflammatory demyelination since it is welldemonstrated that it enhances the survival of oligodendro-cytes and neurons [11 15] as happening for other cell lines[31] and mice lacking Gas6 have demyelinating lesions witha higher proportion of apoptotic oligodendrocytes duringcuprizone-induced demyelination [6] Consequently Gas6may participate actively in oligodendrocyte survival aftermyelin damage favoring a prompt repair It is conceivable thatpatients who suffer frommore severe relapse and who do notpresent an increase in CSF Gas6 concentration may have adefect in Gas6 expression and consequently present a defectin mechanisms of self-limitation to immune aggression toCNS or in myelin damage repair It must be pointed outhowever that we were unable to identify a relation betweenGas6 concentration in CSF and lack of complete recoveryafter the relapse which could be considered the clinicalcorrelate of an efficient recovery system
The putative role of Gas6 in the control of immuneaggression in the nervous system is strengthened by the find-ing that plasma and CSF Gas6 concentration are unrelatedin MS patients therefore the increase of Gas6 in the CSFwas not dependent on an increased plasma concentrationandor the breakdown of the blood-brain barrier but likelyon production by inflammatory cells within the CNS Theseresults are in line with previous results from our group con-cerning autoimmune polyneuropathies [26 32] Moreoverthe relation between CSF Gas6 and EDSS score was stricterin pyramidal and cerebellar relapses possibly because EDSS
6 Mediators of Inflammation
is more sensitive to the damage extension in pyramidal andcerebellar relapses with respect to other symptoms that aremainly subjective and less easy to score
Although the sample size was small and only a fewpatients had an active disease with a significant number ofrelapses or severe disability progression our data suggest thatmeasuring Gas6 concentration in CSF of MS patients canonly be useful to predict the evolution of a first relapse but notthe subsequent disease course Thus Gas6 may be importantin limiting the acute inflammatory demyelination during arelapse but less than so in the pathogenic mechanisms thatdetermine relapse recurrences and cumulative disability
In conclusion CSF Gas6 protein concentration is signifi-cantly increased inmilderMS relapses suggesting an involve-ment of this protein in limiting autoimmune demyelinatingprocesses or in favouring myelin repair after damage Gas6measurement in CSF during a relapse can be useful to predicthow a relapse will evolve but not the disease course in thelong term Further studies are warranted to clarify the Gas6and TAM receptors role in the pathogenesis of MS-relapsesand its clinical applications
Conflict of Interests
The authors declare no conflict of interest
Acknowledgments
This work was supported by (Fondazione Italiana SclerosiMultiplaItalian Multiple Sclerosis Foundation) FISM 2010research Grant During the paper preparation ProfessorFrancescoMonaco prematurely died All investigatorswish todedicate this paper to his memory honouring his dedicationto clinical research in neurological diseases
References
[1] D A Hafler J M Slavik D E Anderson K C OrsquoConnor P DeJager and C Baecher-Allan ldquoMultiple sclerosisrdquo ImmunologicalReviews vol 204 pp 208ndash231 2005
[2] GManfioletti C Brancolini G Avanzi and C Schneider ldquoTheprotein encoded by a growth arrest-specific gene (gas6) is a newmember of the vitamin K-dependent proteins related to proteinS a negative coregulator in the blood coagulation cascaderdquoMolecular and Cellular Biology vol 13 no 8 pp 4976ndash49851993
[3] P J Godowski M R Mark J Chen M D Sadick H Raaband R G Hammonds ldquoReevaluation of the roles of protein Sand Gas6 as ligands for the receptor tyrosine kinase RseTyro3rdquo Cell vol 82 no 3 pp 355ndash358 1995
[4] B C Varnum C Young G Elliot et al ldquoAxl receptor tyrosinekinase stimulated by the vitamin K-dependent protein encodedby growth-arrest-specific gene 6rdquo Nature vol 373 no 6515 pp623ndash626 1995
[5] D R Joseph ldquoSequence and functional relationships betweenandrogen-binding proteinsex hormone-binding globulin andits homologs protein S Gas6 laminin and agrinrdquo Steroids vol62 no 8-9 pp 578ndash588 1997
[6] M D Binder and T J Kilpatrick ldquoTAM receptor signalling anddemyelinationrdquo NeuroSignals vol 17 no 4 pp 277ndash287 2009
[7] G Lemke and Q Lu ldquoMacrophage regulation by Tyro 3 familyreceptorsrdquoCurrent Opinion in Immunology vol 15 no 1 pp 31ndash36 2003
[8] Q Lu and G Lemke ldquoHomeostatic regulation of the immunesystem by receptor tyrosine kinases of the Tyro 3 familyrdquoScience vol 293 no 5528 pp 306ndash311 2001
[9] F Alciato P P Sainaghi D Sola L Castello and G C AvanzildquoTNF-120572 IL-6 and IL-1 expression is inhibited by GAS6 inmonocytesmacrophagesrdquo Journal of Leukocyte Biology vol 87no 5 pp 869ndash875 2010
[10] A L Prieto J LWeber S TracyM J Heeb and C Lai ldquoGas6 aligand for the receptor protein-tyrosine kinase Tyro-3 is widelyexpressed in the central nervous systemrdquo Brain Research vol816 no 2 pp 646ndash661 1999
[11] H Funakoshi T Yonemasu T Nakano K Matumoto and TNakamura ldquoIdentification of Gas6 a putative ligand for Sky andAxl receptor tyrosine kinases as a novel neurotrophic factor forhippocampal neuronsrdquo Journal of Neuroscience Research vol68 no 2 pp 150ndash160 2002
[12] A L Prieto S OrsquoDell B Varnum and C Lai ldquoLocalizationand signaling of the receptor protein tyrosine kinase Tyro3 incortical and hippocampal neuronsrdquo Neuroscience vol 150 no2 pp 319ndash334 2007
[13] T Yagami K Ueda K Asakura et al ldquoGas6 rescues corticalneurons from amyloid 120573 protein-induced apoptosisrdquo Neu-ropharmacology vol 43 no 8 pp 1289ndash1296 2002
[14] R H Li J Chen G Hammonds et al ldquoIdentification ofGas6 as a growth factor for human Schwann cellsrdquo Journal ofNeuroscience vol 16 no 6 pp 2012ndash2019 1996
[15] S L Shankar K OrsquoGuin M Cammer et al ldquoThe growtharrest-specific gene product Gas6 promotes the survival ofhuman oligodendrocytes via a phosphatidylinositol 3-kinase-dependent pathwayrdquo Journal of Neuroscience vol 23 no 10 pp4208ndash4218 2003
[16] S L Shankar K OrsquoGuin M Kim et al ldquoGas6Axl signalingactivates the phosphatidylinositol 3-kinaseAkt1 survival path-way to protect oligodendrocytes from tumor necrosis factor120572-induced apoptosisrdquo Journal of Neuroscience vol 26 no 21 pp5638ndash5648 2006
[17] M D Binder J Xiao D Kemper G Z M Ma S S Murrayand T J Kilpatrick ldquoGas6 increases myelination by oligoden-drocytes and its deficiency delays recovery following cuprizone-induced demyelinationrdquo PLoS ONE vol 6 no 3 article e177272011
[18] V Tsiperson X Li G J Schwartz C S Raine and B Shafit-Zagardo ldquoGAS6 enhances repair following cuprizone-induceddemyelinationrdquo PLoS ONE vol 5 no 12 article e15748 2010
[19] D Miller F Barkhof X Montalban A Thompson and MFilippi ldquoClinically isolated syndromes suggestive of multiplesclerosis part I natural history pathogenesis diagnosis andprognosisrdquo Lancet Neurology vol 4 no 5 pp 281ndash288 2005
[20] W I McDonald A Compston G Edan et al ldquoRecommendeddiagnostic criteria for multiple sclerosis Guidelines from theInternational Panel on the Diagnosis of Multiple SclerosisrdquoAnnals of Neurology vol 50 no 1 pp 121ndash127 2001
[21] G A Schumacker G Beebe R F Kibler et al ldquoProblems ofexperimental trials of therapy in multiple sclerosis report bythe panel on the evaluation of experimental trials of therapy inmultiple sclerosisrdquo Annals of the New York Academy of Sciencesvol 122 pp 552ndash568 1965
[22] M A Leone S Bonissoni L Collimedaglia et al ldquoFactors pre-dicting incomplete recovery from relapses in multiple sclerosis
Mediators of Inflammation 7
A Prospective Studyrdquo Multiple Sclerosis vol 14 no 4 pp 485ndash493 2008
[23] J F Kurtzke ldquoRating neurologic impairment in multiple sclero-sis an expanded disability status scale (EDSS)rdquo Neurology vol33 no 11 pp 1444ndash1452 1983
[24] F Alciato P P Sainaghi L Castello L Bergamasco SCarnieletto and G C Avanzi ldquoDevelopment and validation ofan ELISA method for detection of Growth Arrest Specific 6(GAS6) protein in human plasmardquo Journal of Immunoassay andImmunochemistry vol 29 no 2 pp 167ndash180 2008
[25] P P Sainaghi F Alciato S Carnieletto et al ldquoGas6 evaluationin patients with acute dyspnea due to suspected pulmonaryembolismrdquo Respiratory Medicine vol 103 no 4 pp 589ndash5942009
[26] P P Sainaghi L Collimedaglia F Alciato et al ldquoEleva-tion of Gas6 protein concentration in cerebrospinal fluid ofpatients with chronic inflammatory demyelinating polyneu-ropathy (CIDP)rdquo Journal of the Neurological Sciences vol 269no 1-2 pp 138ndash142 2008
[27] J G Weinger K M Omari K Marsden C S Raine and BShafit-Zagardo ldquoUp-regulation of soluble Axl andMer receptortyrosine kinases negatively correlates with Gas6 in establishedmultiple sclerosis lesionsrdquo American Journal of Pathology vol175 no 1 pp 283ndash293 2009
[28] WH Shao Y Zhen R A Eisenberg and P L Cohen ldquoTheMerreceptor tyrosine kinase is expressed on discrete macrophagesubpopulations and mainly uses Gas6 as its ligand for uptake ofapoptotic cellsrdquoClinical Immunology vol 133 no 1 pp 138ndash1442009
[29] C Grommes C Y D Lee B L Wilkinson et al ldquoRegulation ofmicroglial phagocytosis and inflammatory gene expression byGas6 acting on the AxlMer family of tyrosine kinasesrdquo Journalof NeuroImmune Pharmacology vol 3 no 2 pp 130ndash140 2008
[30] P Sen M A Wallet Z Yi et al ldquoApoptotic cells induce Mertyrosine kinase-dependent blockade of NF-120581B activation indendritic cellsrdquo Blood vol 109 no 2 pp 653ndash660 2007
[31] P P Sainaghi L Castello L BergamascoMGalletti P Bellostaand G C Avanzi ldquoGas6 induces proliferation in prostatecarcinoma cell lines expressing the Axl receptorrdquo Journal ofCellular Physiology vol 204 no 1 pp 36ndash44 2005
[32] P P Sainaghi L Collimedaglia F Alciato et al ldquoThe expressionpattern of inflammatorymediators in cerebrospinal fluid differ-entiates Guillain-Barre syndrome from chronic inflammatorydemyelinating polyneuropathyrdquoCytokine vol 51 no 2 pp 138ndash143 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Mediators of Inflammation
is more sensitive to the damage extension in pyramidal andcerebellar relapses with respect to other symptoms that aremainly subjective and less easy to score
Although the sample size was small and only a fewpatients had an active disease with a significant number ofrelapses or severe disability progression our data suggest thatmeasuring Gas6 concentration in CSF of MS patients canonly be useful to predict the evolution of a first relapse but notthe subsequent disease course Thus Gas6 may be importantin limiting the acute inflammatory demyelination during arelapse but less than so in the pathogenic mechanisms thatdetermine relapse recurrences and cumulative disability
In conclusion CSF Gas6 protein concentration is signifi-cantly increased inmilderMS relapses suggesting an involve-ment of this protein in limiting autoimmune demyelinatingprocesses or in favouring myelin repair after damage Gas6measurement in CSF during a relapse can be useful to predicthow a relapse will evolve but not the disease course in thelong term Further studies are warranted to clarify the Gas6and TAM receptors role in the pathogenesis of MS-relapsesand its clinical applications
Conflict of Interests
The authors declare no conflict of interest
Acknowledgments
This work was supported by (Fondazione Italiana SclerosiMultiplaItalian Multiple Sclerosis Foundation) FISM 2010research Grant During the paper preparation ProfessorFrancescoMonaco prematurely died All investigatorswish todedicate this paper to his memory honouring his dedicationto clinical research in neurological diseases
References
[1] D A Hafler J M Slavik D E Anderson K C OrsquoConnor P DeJager and C Baecher-Allan ldquoMultiple sclerosisrdquo ImmunologicalReviews vol 204 pp 208ndash231 2005
[2] GManfioletti C Brancolini G Avanzi and C Schneider ldquoTheprotein encoded by a growth arrest-specific gene (gas6) is a newmember of the vitamin K-dependent proteins related to proteinS a negative coregulator in the blood coagulation cascaderdquoMolecular and Cellular Biology vol 13 no 8 pp 4976ndash49851993
[3] P J Godowski M R Mark J Chen M D Sadick H Raaband R G Hammonds ldquoReevaluation of the roles of protein Sand Gas6 as ligands for the receptor tyrosine kinase RseTyro3rdquo Cell vol 82 no 3 pp 355ndash358 1995
[4] B C Varnum C Young G Elliot et al ldquoAxl receptor tyrosinekinase stimulated by the vitamin K-dependent protein encodedby growth-arrest-specific gene 6rdquo Nature vol 373 no 6515 pp623ndash626 1995
[5] D R Joseph ldquoSequence and functional relationships betweenandrogen-binding proteinsex hormone-binding globulin andits homologs protein S Gas6 laminin and agrinrdquo Steroids vol62 no 8-9 pp 578ndash588 1997
[6] M D Binder and T J Kilpatrick ldquoTAM receptor signalling anddemyelinationrdquo NeuroSignals vol 17 no 4 pp 277ndash287 2009
[7] G Lemke and Q Lu ldquoMacrophage regulation by Tyro 3 familyreceptorsrdquoCurrent Opinion in Immunology vol 15 no 1 pp 31ndash36 2003
[8] Q Lu and G Lemke ldquoHomeostatic regulation of the immunesystem by receptor tyrosine kinases of the Tyro 3 familyrdquoScience vol 293 no 5528 pp 306ndash311 2001
[9] F Alciato P P Sainaghi D Sola L Castello and G C AvanzildquoTNF-120572 IL-6 and IL-1 expression is inhibited by GAS6 inmonocytesmacrophagesrdquo Journal of Leukocyte Biology vol 87no 5 pp 869ndash875 2010
[10] A L Prieto J LWeber S TracyM J Heeb and C Lai ldquoGas6 aligand for the receptor protein-tyrosine kinase Tyro-3 is widelyexpressed in the central nervous systemrdquo Brain Research vol816 no 2 pp 646ndash661 1999
[11] H Funakoshi T Yonemasu T Nakano K Matumoto and TNakamura ldquoIdentification of Gas6 a putative ligand for Sky andAxl receptor tyrosine kinases as a novel neurotrophic factor forhippocampal neuronsrdquo Journal of Neuroscience Research vol68 no 2 pp 150ndash160 2002
[12] A L Prieto S OrsquoDell B Varnum and C Lai ldquoLocalizationand signaling of the receptor protein tyrosine kinase Tyro3 incortical and hippocampal neuronsrdquo Neuroscience vol 150 no2 pp 319ndash334 2007
[13] T Yagami K Ueda K Asakura et al ldquoGas6 rescues corticalneurons from amyloid 120573 protein-induced apoptosisrdquo Neu-ropharmacology vol 43 no 8 pp 1289ndash1296 2002
[14] R H Li J Chen G Hammonds et al ldquoIdentification ofGas6 as a growth factor for human Schwann cellsrdquo Journal ofNeuroscience vol 16 no 6 pp 2012ndash2019 1996
[15] S L Shankar K OrsquoGuin M Cammer et al ldquoThe growtharrest-specific gene product Gas6 promotes the survival ofhuman oligodendrocytes via a phosphatidylinositol 3-kinase-dependent pathwayrdquo Journal of Neuroscience vol 23 no 10 pp4208ndash4218 2003
[16] S L Shankar K OrsquoGuin M Kim et al ldquoGas6Axl signalingactivates the phosphatidylinositol 3-kinaseAkt1 survival path-way to protect oligodendrocytes from tumor necrosis factor120572-induced apoptosisrdquo Journal of Neuroscience vol 26 no 21 pp5638ndash5648 2006
[17] M D Binder J Xiao D Kemper G Z M Ma S S Murrayand T J Kilpatrick ldquoGas6 increases myelination by oligoden-drocytes and its deficiency delays recovery following cuprizone-induced demyelinationrdquo PLoS ONE vol 6 no 3 article e177272011
[18] V Tsiperson X Li G J Schwartz C S Raine and B Shafit-Zagardo ldquoGAS6 enhances repair following cuprizone-induceddemyelinationrdquo PLoS ONE vol 5 no 12 article e15748 2010
[19] D Miller F Barkhof X Montalban A Thompson and MFilippi ldquoClinically isolated syndromes suggestive of multiplesclerosis part I natural history pathogenesis diagnosis andprognosisrdquo Lancet Neurology vol 4 no 5 pp 281ndash288 2005
[20] W I McDonald A Compston G Edan et al ldquoRecommendeddiagnostic criteria for multiple sclerosis Guidelines from theInternational Panel on the Diagnosis of Multiple SclerosisrdquoAnnals of Neurology vol 50 no 1 pp 121ndash127 2001
[21] G A Schumacker G Beebe R F Kibler et al ldquoProblems ofexperimental trials of therapy in multiple sclerosis report bythe panel on the evaluation of experimental trials of therapy inmultiple sclerosisrdquo Annals of the New York Academy of Sciencesvol 122 pp 552ndash568 1965
[22] M A Leone S Bonissoni L Collimedaglia et al ldquoFactors pre-dicting incomplete recovery from relapses in multiple sclerosis
Mediators of Inflammation 7
A Prospective Studyrdquo Multiple Sclerosis vol 14 no 4 pp 485ndash493 2008
[23] J F Kurtzke ldquoRating neurologic impairment in multiple sclero-sis an expanded disability status scale (EDSS)rdquo Neurology vol33 no 11 pp 1444ndash1452 1983
[24] F Alciato P P Sainaghi L Castello L Bergamasco SCarnieletto and G C Avanzi ldquoDevelopment and validation ofan ELISA method for detection of Growth Arrest Specific 6(GAS6) protein in human plasmardquo Journal of Immunoassay andImmunochemistry vol 29 no 2 pp 167ndash180 2008
[25] P P Sainaghi F Alciato S Carnieletto et al ldquoGas6 evaluationin patients with acute dyspnea due to suspected pulmonaryembolismrdquo Respiratory Medicine vol 103 no 4 pp 589ndash5942009
[26] P P Sainaghi L Collimedaglia F Alciato et al ldquoEleva-tion of Gas6 protein concentration in cerebrospinal fluid ofpatients with chronic inflammatory demyelinating polyneu-ropathy (CIDP)rdquo Journal of the Neurological Sciences vol 269no 1-2 pp 138ndash142 2008
[27] J G Weinger K M Omari K Marsden C S Raine and BShafit-Zagardo ldquoUp-regulation of soluble Axl andMer receptortyrosine kinases negatively correlates with Gas6 in establishedmultiple sclerosis lesionsrdquo American Journal of Pathology vol175 no 1 pp 283ndash293 2009
[28] WH Shao Y Zhen R A Eisenberg and P L Cohen ldquoTheMerreceptor tyrosine kinase is expressed on discrete macrophagesubpopulations and mainly uses Gas6 as its ligand for uptake ofapoptotic cellsrdquoClinical Immunology vol 133 no 1 pp 138ndash1442009
[29] C Grommes C Y D Lee B L Wilkinson et al ldquoRegulation ofmicroglial phagocytosis and inflammatory gene expression byGas6 acting on the AxlMer family of tyrosine kinasesrdquo Journalof NeuroImmune Pharmacology vol 3 no 2 pp 130ndash140 2008
[30] P Sen M A Wallet Z Yi et al ldquoApoptotic cells induce Mertyrosine kinase-dependent blockade of NF-120581B activation indendritic cellsrdquo Blood vol 109 no 2 pp 653ndash660 2007
[31] P P Sainaghi L Castello L BergamascoMGalletti P Bellostaand G C Avanzi ldquoGas6 induces proliferation in prostatecarcinoma cell lines expressing the Axl receptorrdquo Journal ofCellular Physiology vol 204 no 1 pp 36ndash44 2005
[32] P P Sainaghi L Collimedaglia F Alciato et al ldquoThe expressionpattern of inflammatorymediators in cerebrospinal fluid differ-entiates Guillain-Barre syndrome from chronic inflammatorydemyelinating polyneuropathyrdquoCytokine vol 51 no 2 pp 138ndash143 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
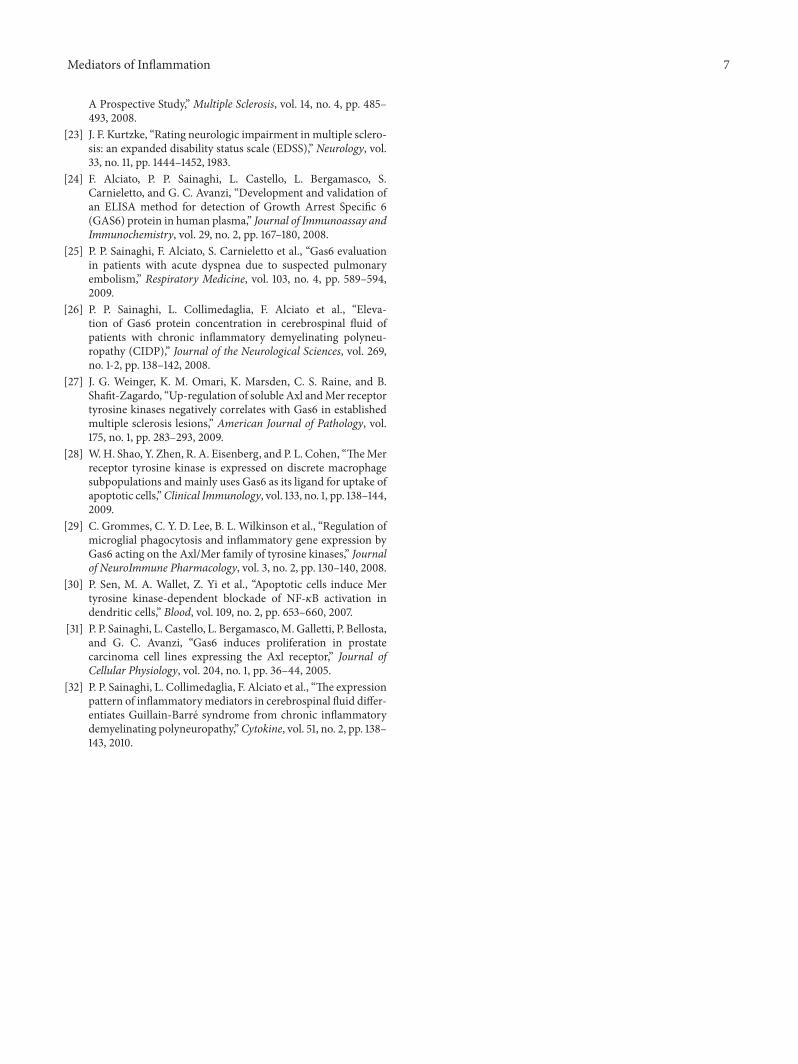
Mediators of Inflammation 7
A Prospective Studyrdquo Multiple Sclerosis vol 14 no 4 pp 485ndash493 2008
[23] J F Kurtzke ldquoRating neurologic impairment in multiple sclero-sis an expanded disability status scale (EDSS)rdquo Neurology vol33 no 11 pp 1444ndash1452 1983
[24] F Alciato P P Sainaghi L Castello L Bergamasco SCarnieletto and G C Avanzi ldquoDevelopment and validation ofan ELISA method for detection of Growth Arrest Specific 6(GAS6) protein in human plasmardquo Journal of Immunoassay andImmunochemistry vol 29 no 2 pp 167ndash180 2008
[25] P P Sainaghi F Alciato S Carnieletto et al ldquoGas6 evaluationin patients with acute dyspnea due to suspected pulmonaryembolismrdquo Respiratory Medicine vol 103 no 4 pp 589ndash5942009
[26] P P Sainaghi L Collimedaglia F Alciato et al ldquoEleva-tion of Gas6 protein concentration in cerebrospinal fluid ofpatients with chronic inflammatory demyelinating polyneu-ropathy (CIDP)rdquo Journal of the Neurological Sciences vol 269no 1-2 pp 138ndash142 2008
[27] J G Weinger K M Omari K Marsden C S Raine and BShafit-Zagardo ldquoUp-regulation of soluble Axl andMer receptortyrosine kinases negatively correlates with Gas6 in establishedmultiple sclerosis lesionsrdquo American Journal of Pathology vol175 no 1 pp 283ndash293 2009
[28] WH Shao Y Zhen R A Eisenberg and P L Cohen ldquoTheMerreceptor tyrosine kinase is expressed on discrete macrophagesubpopulations and mainly uses Gas6 as its ligand for uptake ofapoptotic cellsrdquoClinical Immunology vol 133 no 1 pp 138ndash1442009
[29] C Grommes C Y D Lee B L Wilkinson et al ldquoRegulation ofmicroglial phagocytosis and inflammatory gene expression byGas6 acting on the AxlMer family of tyrosine kinasesrdquo Journalof NeuroImmune Pharmacology vol 3 no 2 pp 130ndash140 2008
[30] P Sen M A Wallet Z Yi et al ldquoApoptotic cells induce Mertyrosine kinase-dependent blockade of NF-120581B activation indendritic cellsrdquo Blood vol 109 no 2 pp 653ndash660 2007
[31] P P Sainaghi L Castello L BergamascoMGalletti P Bellostaand G C Avanzi ldquoGas6 induces proliferation in prostatecarcinoma cell lines expressing the Axl receptorrdquo Journal ofCellular Physiology vol 204 no 1 pp 36ndash44 2005
[32] P P Sainaghi L Collimedaglia F Alciato et al ldquoThe expressionpattern of inflammatorymediators in cerebrospinal fluid differ-entiates Guillain-Barre syndrome from chronic inflammatorydemyelinating polyneuropathyrdquoCytokine vol 51 no 2 pp 138ndash143 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom