Clinical protocol, Workflow Primary and metastatic liver ...
51
Clinical protocol, Workflow Primary and metastatic liver tumors SBRT Amsterdam 2017
Transcript of Clinical protocol, Workflow Primary and metastatic liver ...
Clinicalprotocol,Workflow
Primary and metastatic liver tumors SBRTAmsterdam2017

Nodisclosures
Learning objective
• Specifics ofliver SBRTcompared toother sites(lung)

Basic principle:
StartSBRTprogramwith lung
Copy asmuch aspossible from experience inlung SBRT!
àLiver SBRTis“identical”but morecomplex
LiverSBRT:
Bothprimarytumorsandmets
NW-Europe:livermets!
Inmanyothercountries:primarylivercancer

SBRTLIVER
•DOESITWORK??

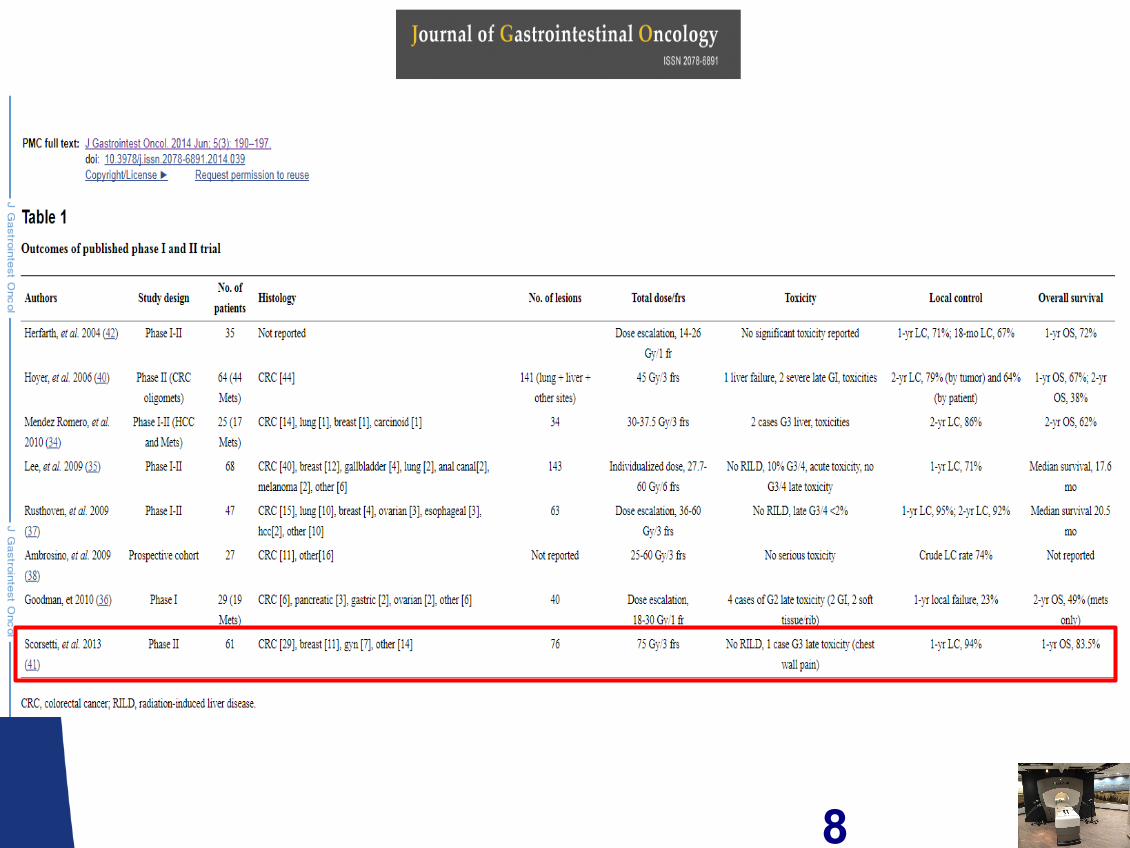
Publishedresultsbothmets andprimarylever:• Widevarietyoftechniquesanddoseschedules,>10yearsexperience
Author Nooflesions Dose Localcontrol Remarks
Blomgren1995 42 4x7.7Gy– 1x30Gy@50%
80%
Wulf 2006 56 Various:4x7Gy-1x26Gy@80%
Actuarial:HCC:100%Mets:1yr:92%
2yr:66%2yrOS:32%
Localcontrolincreasedathigherdoses(trend)
Tse2008 31HCC10IHC
6x4-9Gyisoc 1yr:65%
Chiba2005 192HCC Various,median16x4.5Gy
5yr87% Protons/gating/chemo-embolisation
Kavanagh2006
36 Max3x20Gy 93% Doseescalation,MTDnotreached
8
Consider when starting SBRTliver program
• Getting patients
• Imaging (planningandtreatment)
• Motionmanagement(Tumorand OAR!)
• Followup

Radiationtherapyinlivertumors:
• Historicalproblem:RILDà Radiationinducedliverdisease
• Wholeliverradiation:RILDafter>30Gy• 30Gynotenoughforlocalcontrol(mosttumors>60Gy)
àRadiationoncologists:-nohistory/notmuchinterest-notinvolvedinspecificlivertumorboards/liverguidelines-specificknowledgerequired!
Getting patients referred
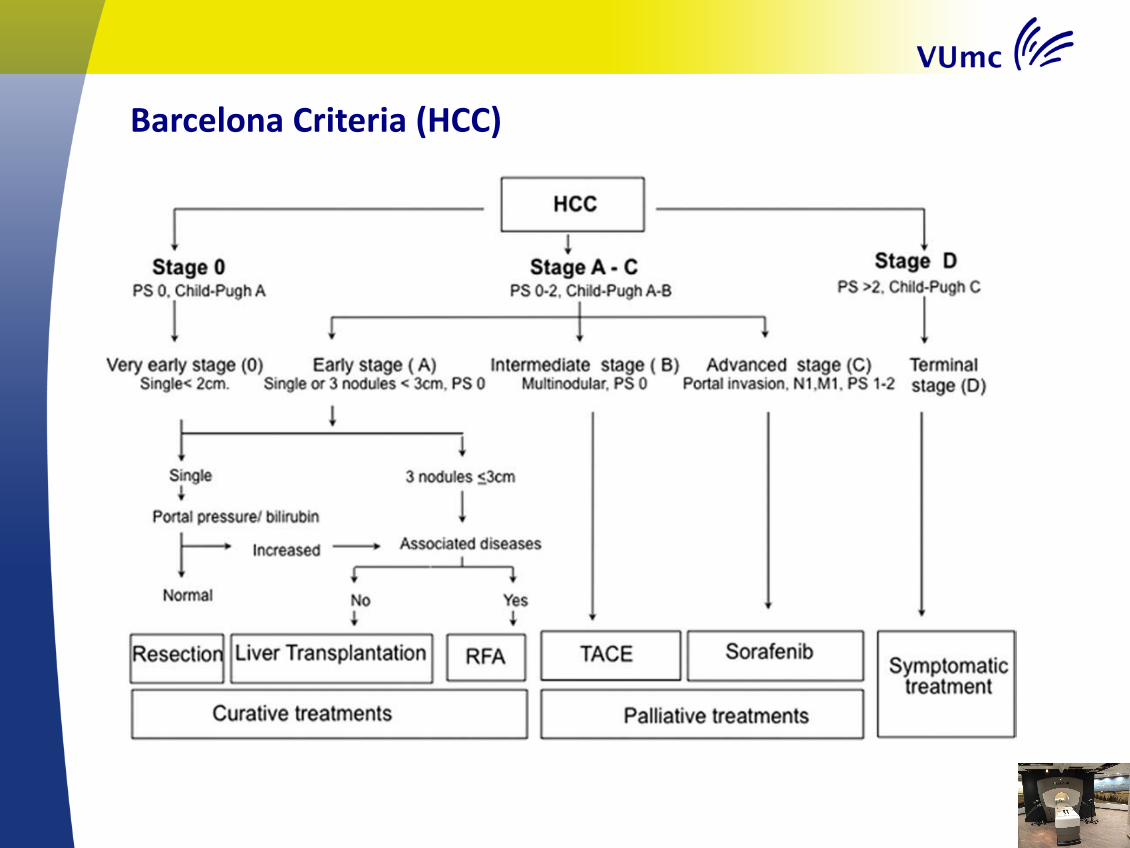
BarcelonaCriteria(HCC)
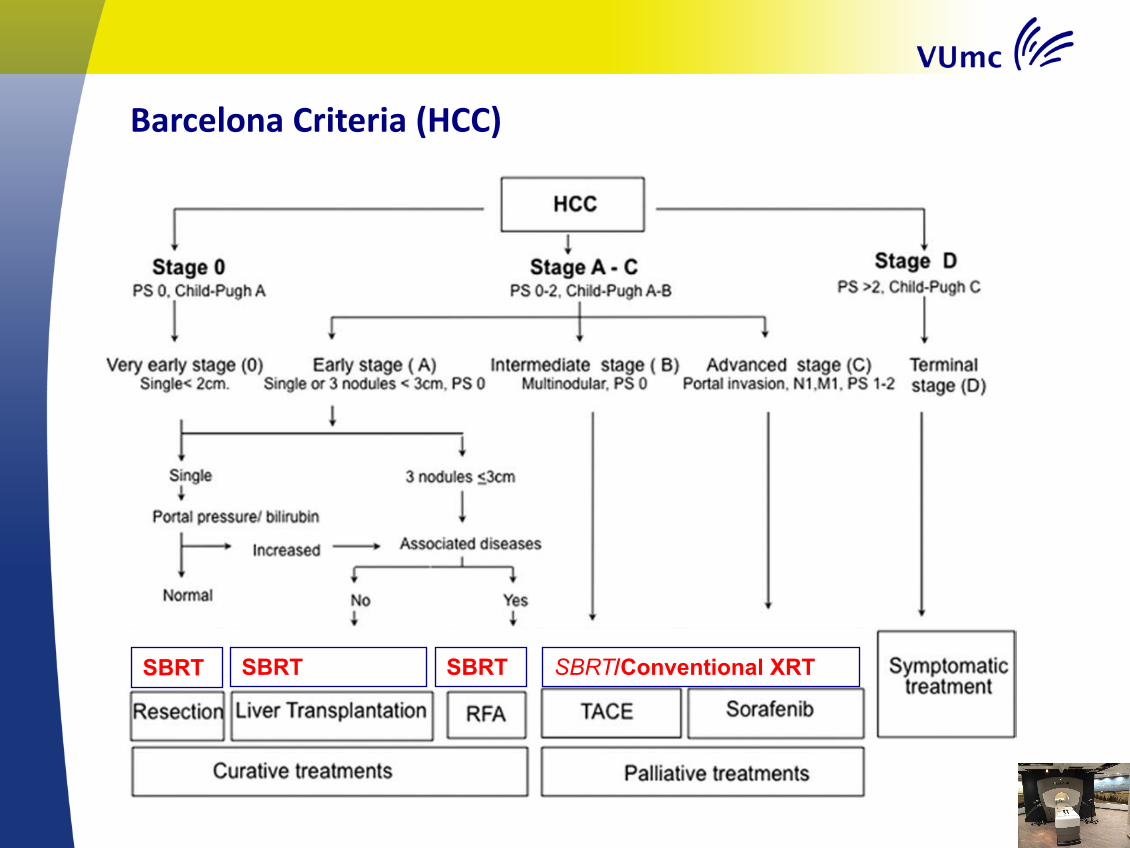
SBRT SBRT SBRT SBRT/Conventional XRT
BarcelonaCriteria(HCC)


Gettingpatientsreferred:Manycompetinglocaltreatmentoptions:
• Surgery• RFA• TACE/Radioembolisation• Electroporation (“IRE/Nanoknife”)
• Alltreatmentshavedifferent:– (contra)indications(anesthesia/bleedingdisordersetc)– localcontrol(tumorsize)– “difficult”locations

ProSBRT(attumorboardmeetings):• Highlocalcontrol(especiallylargertumorscomparedtocompetingtechniques)
• Overlapwithlargevessels/hilar structuresnoproblem• Outpatientprocedure• Nogeneralanesthesia• Completelynon-invasive(ifwithoutfiducials)• Bleedingdisorders:noproblem

Patientselection:
• “Oligometastases”oroligoprogression– Nopatientswithactivewidespreaddisease– Reasonablelifeexpectancy
• Nomaximumsizeornumber– dependingonsparednormalliver– mostcommon:one(ortwo)mets
• Somemarginneededbetweentumorandbowel/stomach/esophagusà SBRT-likedoseshouldbepossible

Diagnostics• Mostcasesheavilypretreated:tissueproofofM1diseaseavailableformostpatients
• 4-phase CTscan(contrastenhancementpattern)– DifferentcontrasttimingHCCvs mets
• PET-CTscan– Ruleoutwidespreaddistantmets– LesionFDGpos??(usefulnessofmakingplanningPETCT)
• OftenMRIisavailable– RoleofPET-MRIstillunclear
Step by step CASE(pre-MRIdian)
• Mr X• Age 66• Excellent performance score
• Dec 2010 sigmoid carcinoma: resection• Widespread synchronous liver metastases: chemotherapy (capecitabine +
oxaliplatin + bevacizumab)• July 2011: RFA liver metastases segment I, II, III, VI, 2 x VII and 2 x in VIII. • December 2011: 6 liver metastases: 4 x RFA (segment II, III, IVa, IV) and 2 x
microwave ablation (segment III, VIII). • April 2012: Multifocal recurrence ablation cavity segment 8. No extrahepatic
disease: • Microwafe +TACE. • October 2012: recurrence same location• SABR???

Livermetastases:referralpatterns• WhoarereferredforSBRT:
– Colorectal liver metastases– (very)poorperformancescore– Afterresection– AftermultipleRFA/TACE– Centrallocation- overlaplargevessels– Contra-indicationorrefusalinvasivetreatment– Inmostcasesalloftheabove
-NonColorectallivermetastasespatients-lessheavilypretreated-lessaggressivelocaltreatmentànon-invasive
treatmentmoreimportant!
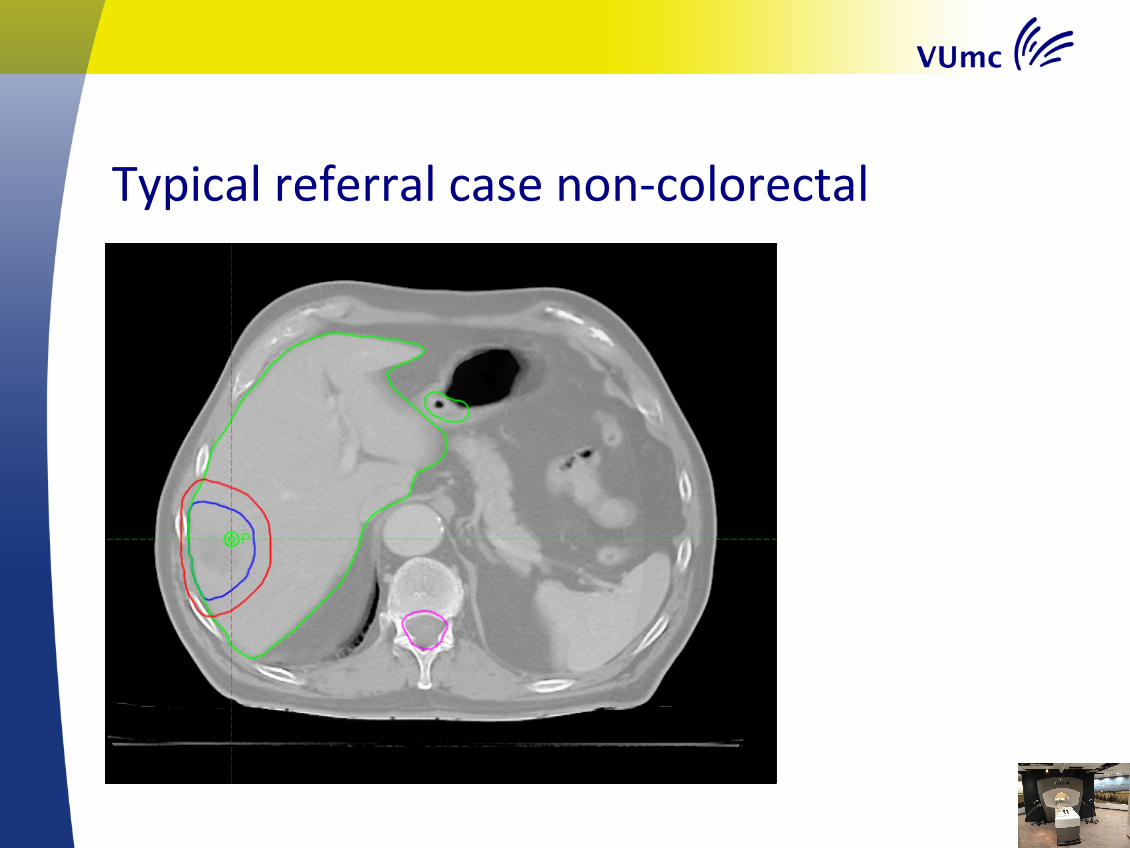
Typicalreferralcasenon-colorectal

Typicalcolorectalcase(dosereductionatOAR~local control)

Step by step CASE
• July:Diagnostic4-phaseCTscan

Step by step CASE
• October: Diagnostic 4-phase CT scan
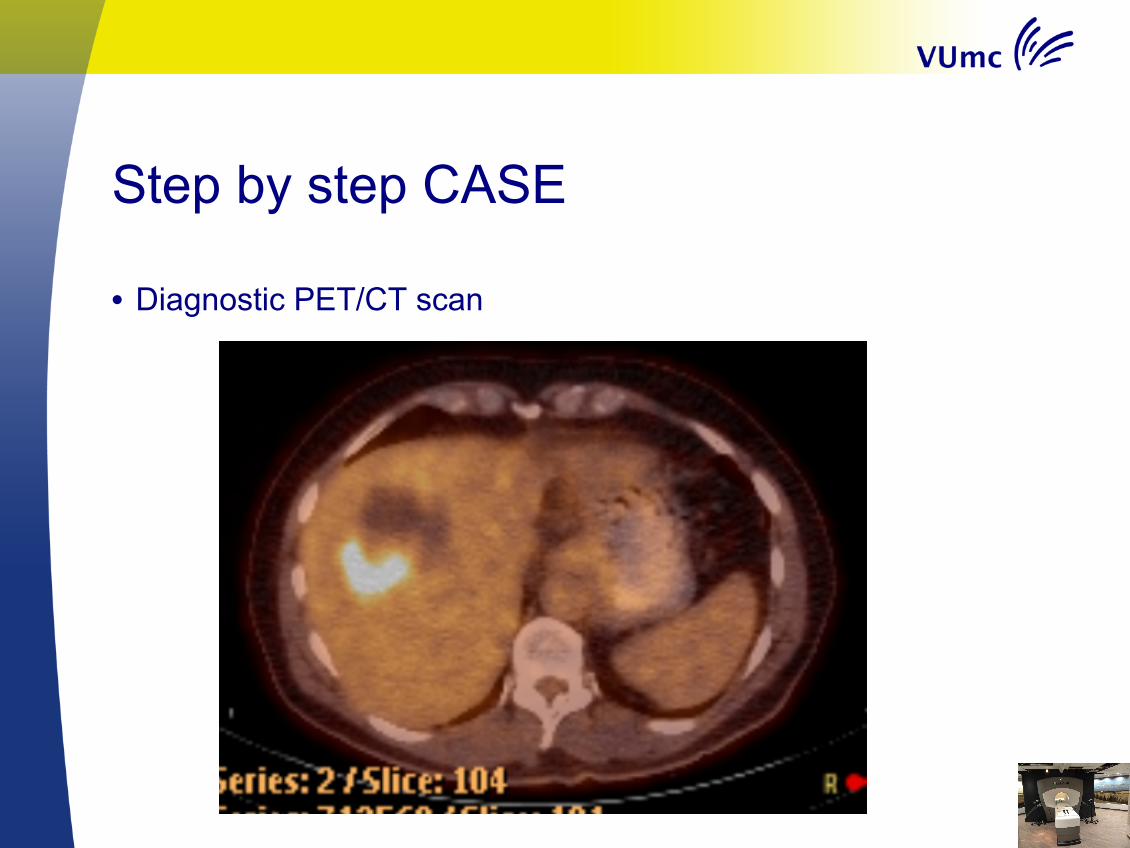
Step by step CASE
• Diagnostic PET/CT scan
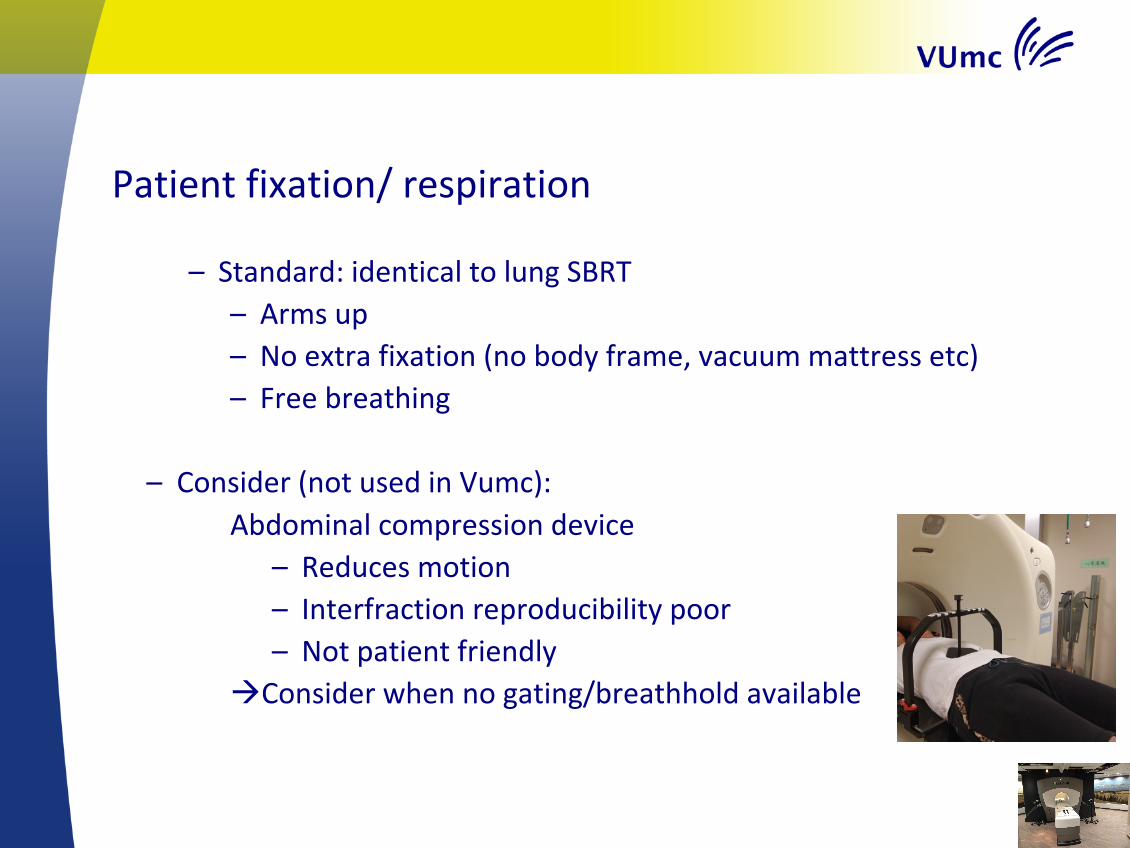
Patientfixation/respiration
– Standard:identicaltolungSBRT– Armsup– Noextrafixation(nobodyframe,vacuummattressetc)– Freebreathing
– Consider(notusedinVumc):Abdominal compression device
– Reduces motion– Interfraction reproducibility poor– Not patient friendly
àConsider when no gating/breathhold available

ImagingforliverSABR• ‘Large’area4DCTscanwithoutivcontrast
– Dosecalculation
• ‘Smallarea’4DCTscanofliverareawithivcontrast– Contrasttimingeasierwithsmallscanarea

ImagingforSABR• Insomecases:double4DCTwithivcontrast(differentdays)• Duringplanning4DCTand4DPETCT
– Influenceofrespiratorybeltonanatomyandbreathingpattern– RPMsystemonlyavailableon4DCT– Difficultimagingandivcontrasttiming:doubleismore…

• Noroutinelyimplantedfiducials– Logistical
– Time– Somerad oncs implantmarkersthemselves…
– KeeptreatmentNon-invasive!– Complications
• Manypatientshavecavities/clipsfromprevioustreatmentsthatcanbeused
• Thinktwiceaboutusinggoldmarkers…
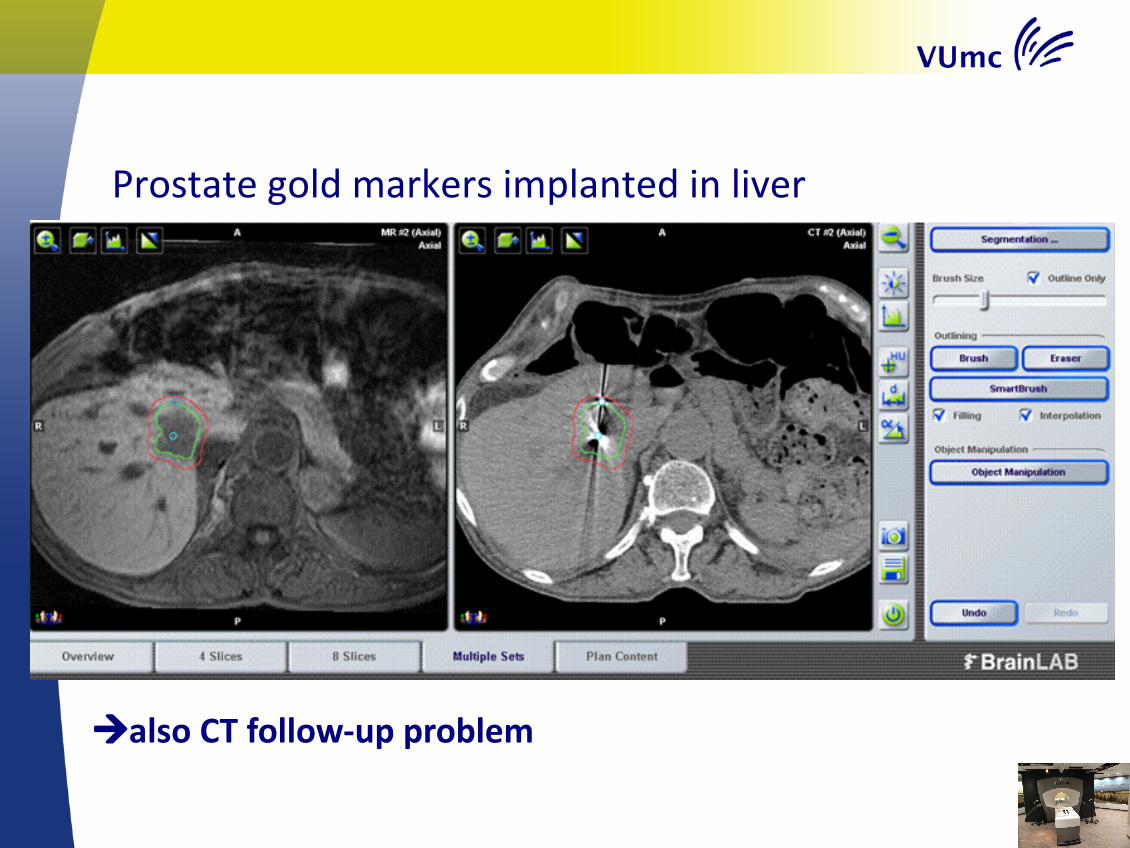
Prostategoldmarkersimplanted inliver
àalso CTfollow-upproblem
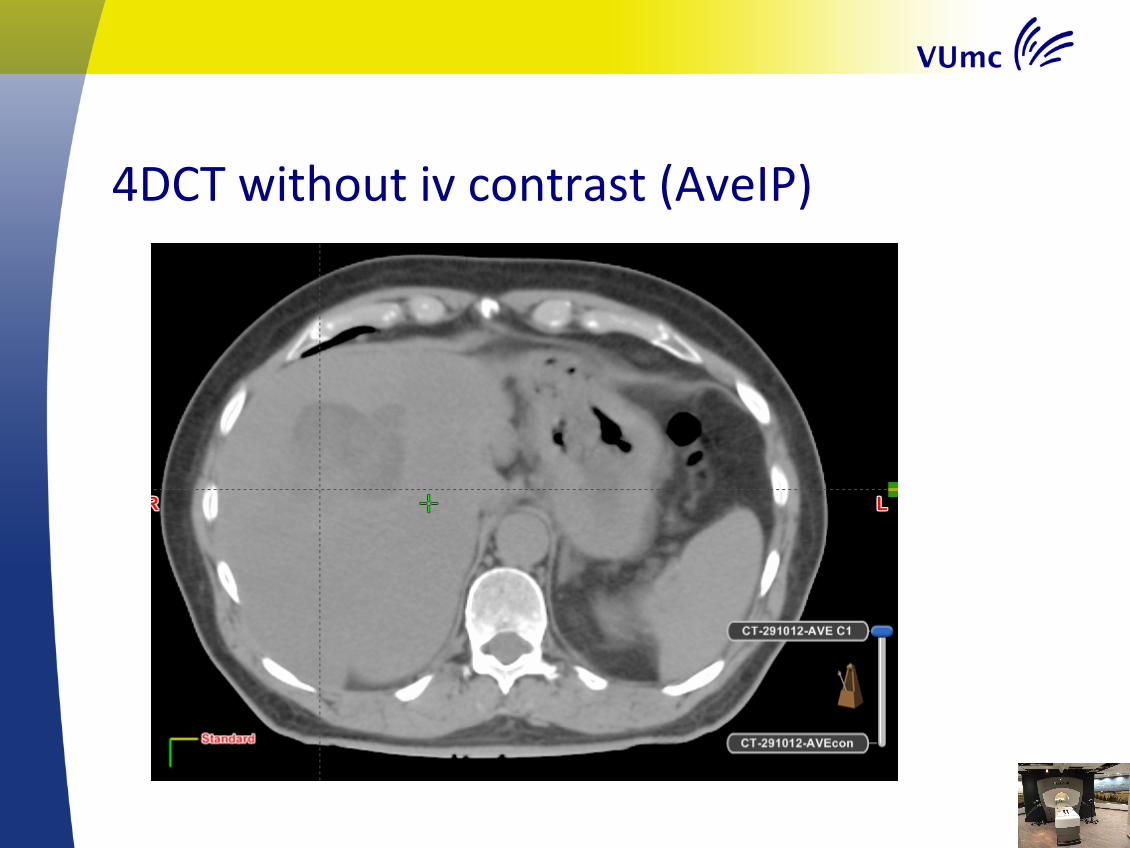
4DCTwithoutivcontrast(AveIP)

4DCTwithivcontrast(AveIP)
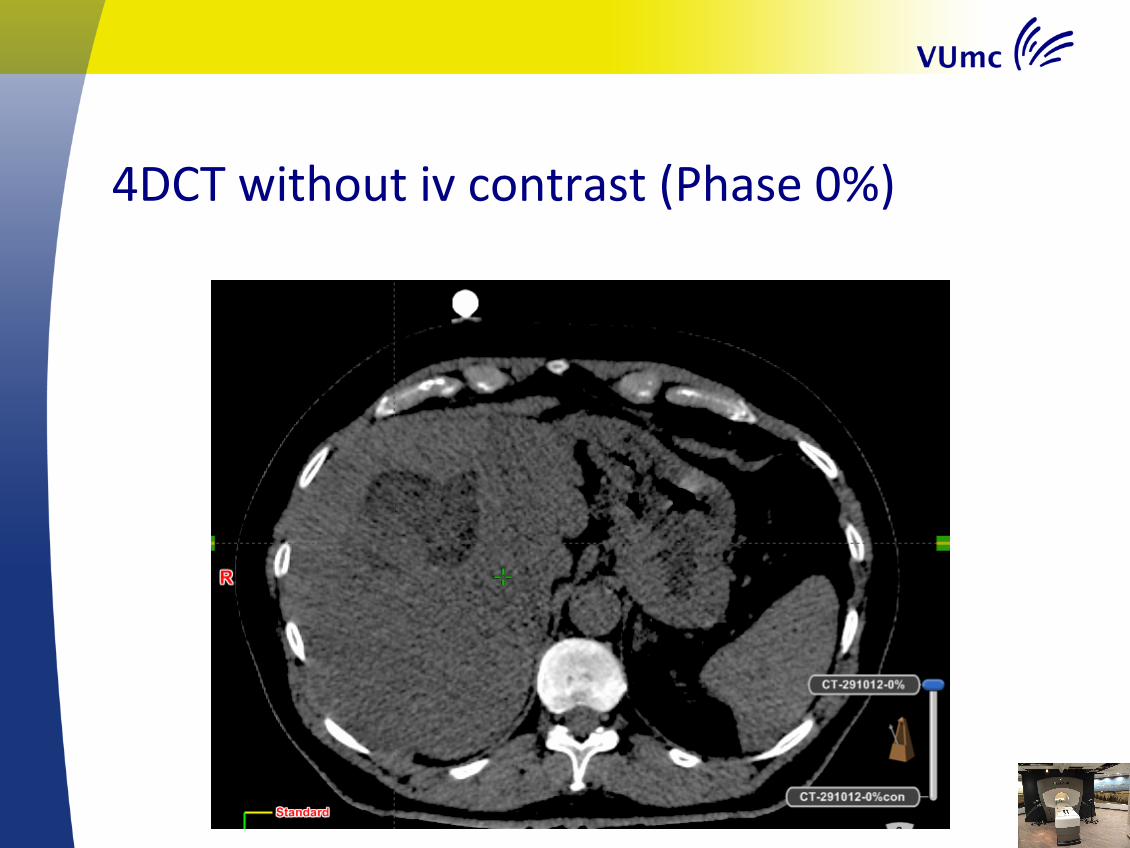
4DCTwithoutivcontrast(Phase0%)

4DCTwithivcontrast(Phase0%)
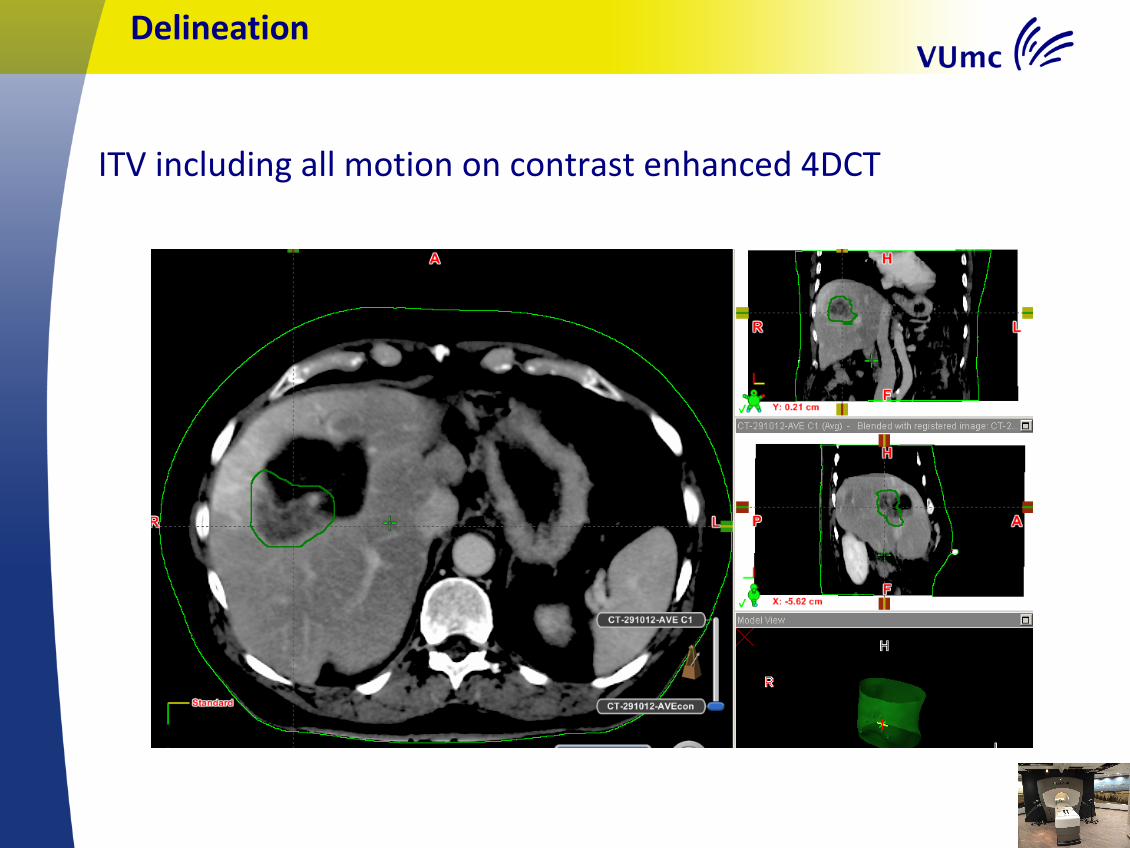
ITVincludingallmotiononcontrastenhanced4DCT
Delineation

MatchofdiagnosticPETtocontrastenhanced4DCT
Mismatchbetween diagnostic PETCTandplanning4DCT-mismatchPETCTand4DCT?-mismatchPETenlowdoseCT?-deformation ofliver?-differentbreathing pattern?(à insome centersmax inspiration diagnostic CTduring PET)
àDonot rely on diagnostic PETCTonly,dedicated RTimaging neededàSame problem applies todiagnostic MRI
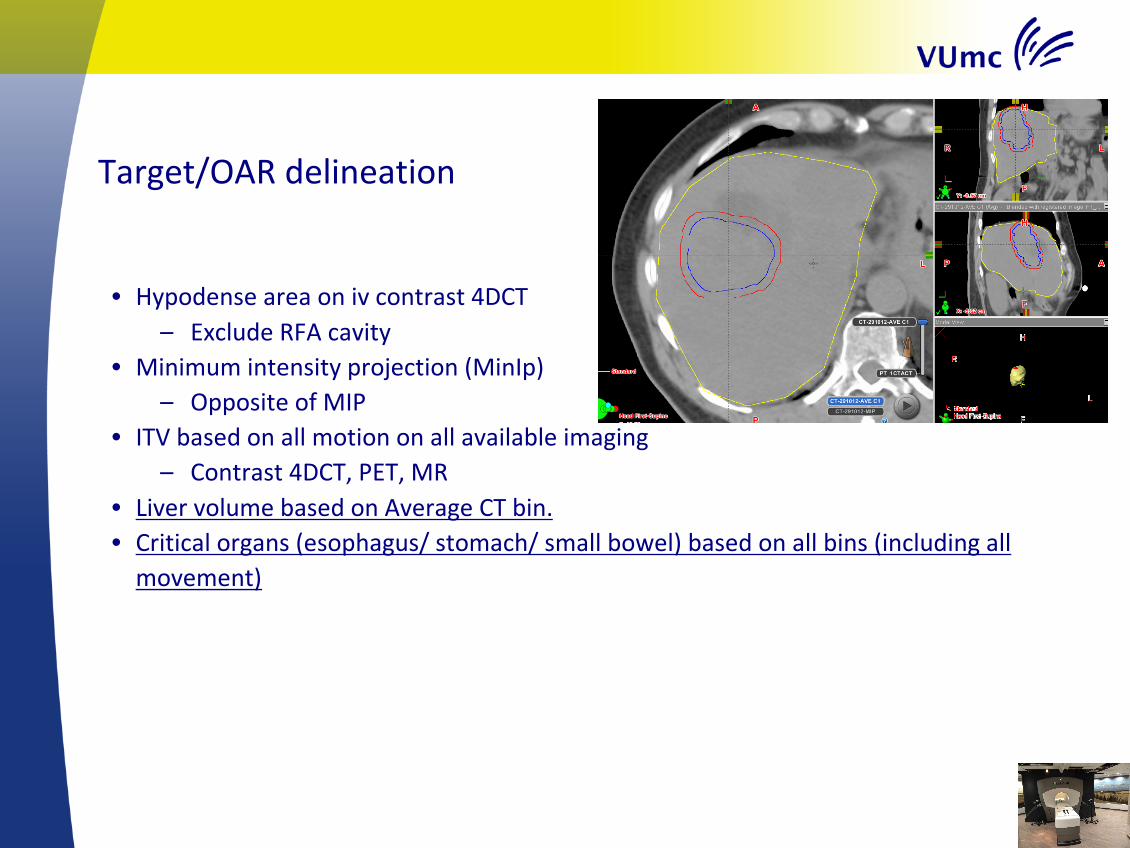
Target/OARdelineation
• Hypodense areaonivcontrast4DCT– ExcludeRFAcavity
• Minimumintensityprojection(MinIp)– OppositeofMIP
• ITVbasedonallmotiononallavailableimaging– Contrast4DCT,PET,MR
• LivervolumebasedonAverageCTbin.• Criticalorgans(esophagus/stomach/smallbowel)basedonallbins(includingallmovement)

ITV-PTVmargin5mm
Planning• DoseschedulesandplanningidenticaltolungSBRT
– Prescriptionisodose covers95%ofPTVvolume
– DosereductionofpartofPTVifnecessaryfororgansatrisk,andusemorefractionatedschedules(8-12x)
– RapidArc:2(partial)arcs

Constraints(Dutchnationalconsensusguideline):3x 5x 8x 12 Equivalent 2Gy
Liver (α/ß=3) >700ml max 3x5=15Gy
>700ml max 5x3.6=18Gy
>700ml max 8x2,7=21.6Gy
>700ml max 12x2=24Gy
24Gy
Myelum (α/ß=2)
3 x 6 =18Gy 5 x 4,5 =22,5Gy 8 x 3,5 =28Gy 12 x 2.7 = 32 36 Gy
Esophagus (α/ß=3)
3 x 9 =27Gy 5 x 6,5 =32,5Gy 8 x 5,0 =40Gy 12 x 4.0 = 48 66 Gy
Small bowel/ stomach (α/ß=3)
3 x 10 =30Gy 5 x 7,3 =36,5 8 x 5,5 =44Gy 12x4.4=53Gy 78Gy
Kidneys (α/ß=3)
67% volume r kidney max 3x5=15Gy
And:35% Total
volume kidneys (r +l) max 3x5=15Gy
67% volume r kidney max 5x3.6=18Gy
And:35% Total
volume kidneys (r +l) max 5x3.6=18Gy
67% volume r kidney max 8x2,7=21.6Gy
And:35% Total
volume kidneys (r +l) max 8x2,7=21.6Gy
67% volume r kidney max 12x2=24Gy
And:35% Total
volume kidneys (r +l) max 12x2=24Gy
24Gy

55Gy
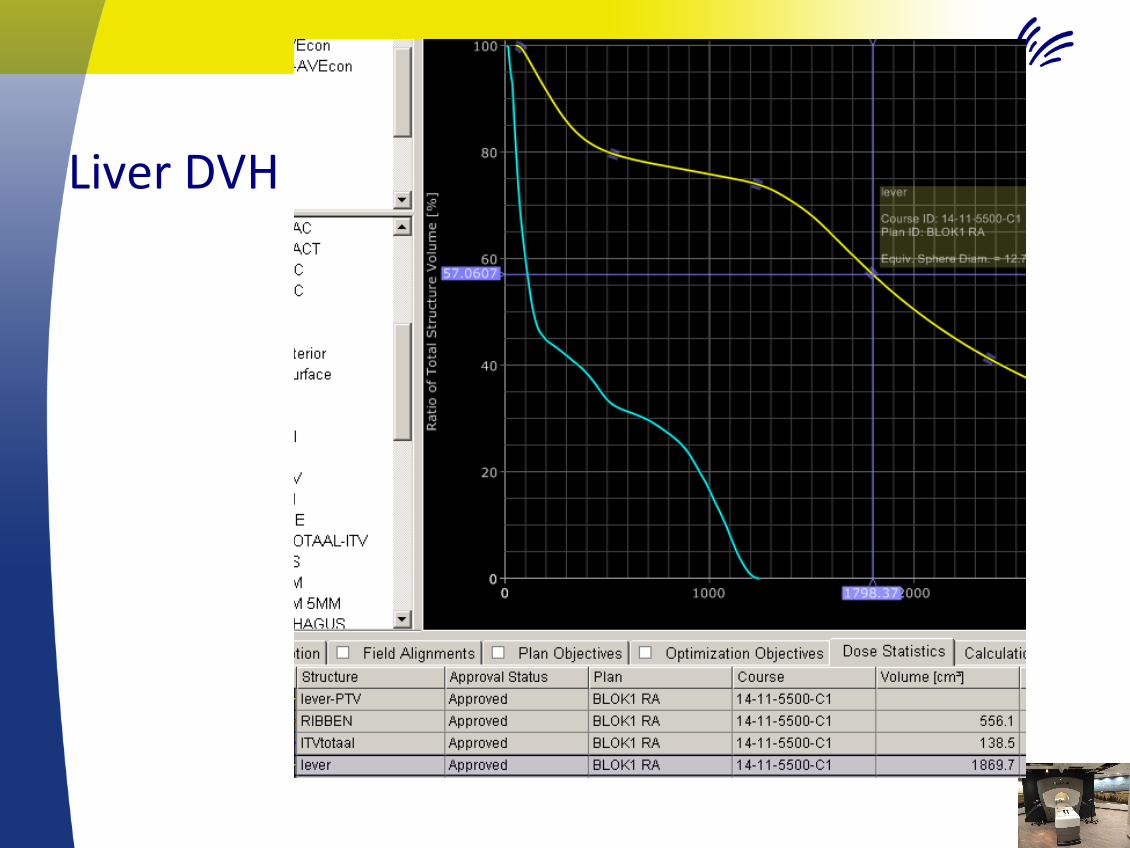
LiverDVH

Planning/treatmentdelivery:
• Standard:freebreathing
• Onlyinexceptionalcases(overlapboweletc):– Gatingduringin- orexpirationphases(audiocoaching)– Breathhold(FFF)
– Newimaging(breathhold oraudiocoachedCT)neededL
Treatmentdelivery• Patientpositioning:
– Dayly onlineCBCTsetupduringfreebreathing– CBCTqualitypoor– PTVmatchoftennotsensible(ITV/PTV/liverallgrey…)– Matchonlivercontourand/orcriticalorganatrisk– MakeuseofoldclipsandRFAcavities
– Intra-fractionmonitoringbreathingandpatientmotion:– RPMsystem/ExacTrac

CBCTPTVmatchimpossibe
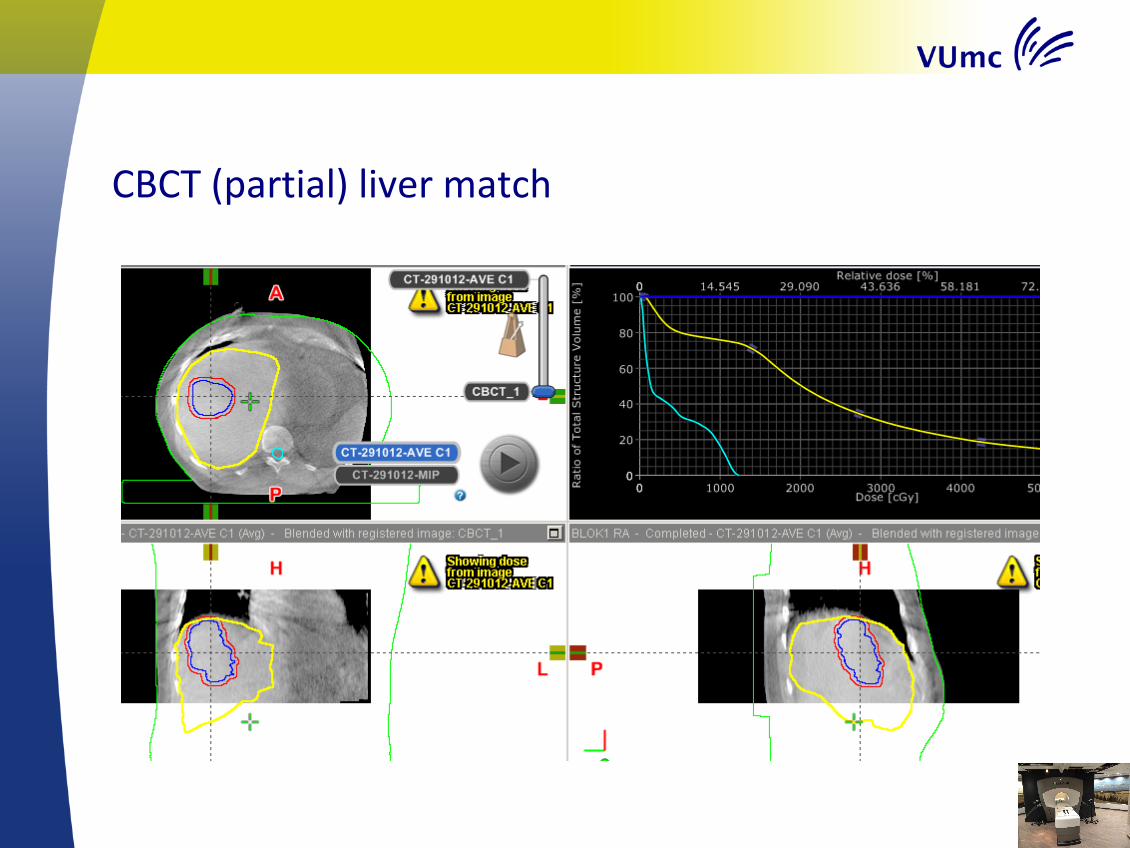
CBCT(partial)livermatch

PTVmargins
• Theoretically5mmshouldbeenough….
• Clinicalpractice:liversmuchmoredifficultthanlung– ITVàPTVmargin1cmiffeasible(liverandotherconstraints).

Followup
• IfinRad Onc department:– 3-modiagnosticCTwithivcontrast.
• Bothhyperandhypodens areas(halo’s)described inthe>30GySBRTarea after 3-6months!
• Heavilypretreatedpatients:– OftenFUonlybyreferringphysician
– FrequentCTorPET/CT

GeneralPatientinformation
• Promisingtreatmentwithhighlocalcontrol(~lung>80%)
• Possibleacutetox:Nausea/pain
• Chanceofhighgradetoxicity– Dependingontumorlocation
– Smallbowel/esophagus/stomachperforation– Fibrosis/stenosis biliary tract
• Mostpatients:notoxicity!
àMostpatientsheavilypretreated- noother/betteroptions..

Generalremarks
• Nostandard profylactic medication (no dexa,no anti-emetics)
• Noroutineblood tests(except creatinine for iv contrast)

Conclusions/Takehome- LiverSBRT:
• ExcellentresultsforhighdoseSBRT
• Keepitsimple(useexperienceinlungSBRT)!
• Bewareofoverlapwithesophagus/stomach/bowelandlargechangesbetweenfractions
• Additionalcomparedtolung:– 4DCTusingivcontrast(extraprotocols/equipment)– Consider larger PTVmargin
• Liver istheideal indication for MRguided SBRT!

Questions…




![Metastatic Lesions to the Liverdownloads.hindawi.com/journals/specialissues/258563.pdffact that most metastatic liver tumors are supplied by the hepatic artery [6, 7], hepatic artery](https://static.fdocuments.us/doc/165x107/601645b97fef143ef6536e4f/metastatic-lesions-to-the-fact-that-most-metastatic-liver-tumors-are-supplied-by.jpg)