RADIOLOGICAL ACCIDENT IN GOIÂNİA RADIOLOGICAL ACCIDENT IN GOIÂNİA Module XIX.

CLINICAL PROFILE, RADIOLOGICAL AND OPERATIVE
FINDINGS OF SURGICALLY MANAGED INTERNAL CAROTID
ARTERY COMMUNICATING SEGMENT ANEURYSM:
A RETROSPECTIVE STUDY
Submitted for M.Ch Neurosurgery
By
Dr. Shashank Aroor
October 2017
Department of Neurosurgery
Sree ChitraTirunal Institute for Medical Sciences
& Technology
Thiruvananthapuram – 695011

CLINICAL PROFILE, RADIOLOGICAL AND OPERATIVE
FINDINGS OF SURGICALLY MANAGED INTERNAL CAROTID
ARTERY COMMUNICATING SEGMENT ANEURYSM:
A RETROSPECTIVE STUDY
Submitted by : Dr. Shashank Aroor
Programme : M.Ch Neurosurgery
Month & year of submission : October, 2017

DECLARATION
This thesis titled ―Clinical profile, radiological and
operative findings of surgically managed Internal Carotid Artery
communicating segment aneurysm: A retrospective study‖, is a
consolidated report based on a bonafide study of the period from
January 2013 to May 2017, done by me under the Department of
Neurosurgery, Sree Chitra Tirunal Institute for Medical Sciences
& Technology, Thiruvananthapuram.
This thesis is submitted to SCTIMST in partial fulfillment
of rules and regulations of MCh Neurosurgery examination.
Dr. Shashank Aroor,
Department of Neurosurgery,
SCTIMST,
Thiruvananthapuram.

CERTIFICATE
This is to certify that the thesis entitled ―Clinical profile,
radiological and operative findings of surgically managed Internal
Carotid Artery communicating segment aneurysm: A retrospective
study‖ is a bonafide work of Dr.Shashank Aroor and was conducted in
the Department of Neurosurgery, Sree Chitra Tirunal Institute for
Medical Sciences & Technology, Thiruvananthapuram (SCTIMST),
under my guidance and supervision.
Prof. Mathew Abraham,
Professor and Head of the Department,
Department of Neurosurgery,
SCTIMST,
Thiruvananthapuram

ACKNOWLEDGEMENT
The guidance of Prof. Mathew Abraham, Professor and Head of the
Department of Neurosurgery, has been invaluable and I am extremely
grateful and indebted for his contributions and suggestions, which were
of invaluable help during the entire work. He will always be a constant
source of inspiration to me.
I owe a deep sense of gratitude to Dr. Suresh Nair for his
invaluable advice, encouragement and guidance, without which this work
would not have been possible. His critical remarks, suggestions, helped
me in achieving a high standard of work.
I am deeply indebted to Dr. Easwer H. V, Dr. Krishnakumar K.,
Dr. George Vilanilam, Dr Jayanand Sudhir, Dr. Prakash Nair, Dr Tobin
George and colleagues and I thank them for their constant encouragement
and support.
I am also deeply indebted to Dr Santhosh Kumar (Department of
imaging sciences and interventional radiology, SCTIMST) for guiding
and helping me in the radiological interpretation.
I owe a deep sense of gratitude to all my patients without whom
this work would not have been possible.
I am very grateful to my family for their constant encouragement
and moral support.

INDEX
INTRODUCTION 1
AIM AND OBJECTIVE 3
MATERIALS AND METHODS 4
REVIEW OF LITERATURE 9
RESULTS 42
DISCUSSION 63
CONCLUSION 79
LIMITATION OF THE STUDY 80
BIBLIOGRAPHY 81
ANNEXURES 98
i. Proforma
ii. IEC approval
iii. Originality index
iv. Master chart abbreviations
v. Master Chart

Introduction
1
INTRODUCTION
The communicating segment of the internal carotid artery is the
segment between the origin of posterior communicating artery (PcoA)
and the bifurcation of internal carotid artery (ICA).(1,2) The
communicating artery aneurysm are the second most common location
for anterior circulation aneurysm. The incidence of PcoA aneurysm as
quoted in the literature is 15%–25% of all intracranial aneurysms. (12,30)
Communicating segment aneurysm can present with subarachnoid
hemorrhage or third nerve palsy. Successful surgical management of
aneurysms of the PCoA depends on precise understanding of their unique
microsurgical anatomy, avoidance of pitfalls, and the surgeon’s
experience. PCoA gives rise to many important branches supplying the
optic chiasm, oculomotor nerve, mammillary body, tuber cinerum,
cerebral crura, ventral thalamus, and rostral portion of the caudate
nucleus. (3) Interruption of flow through these vessels may result in
ischemic damage to the diencephalon with significant morbidity, even
after an apparently uneventful surgical procedure.
The outcome depends on pre operative, intra operative and post
operative factors. Various factors like Glasgow coma scale at the time of
admission, Fischer grade on computerised tomography scan, presence of

Introduction
2
third nerve palsy, intra operative rupture, need for temporary clipping,
direction of aneurysm, presence of hydrocephalus, post operative
vasospasm will affect the final outcome. The literature available till date
is descriptive of risk factors, clinical presentation and surgical outcome of
communicating segment aneurysms. (5,7)There are comparisons in
literature on endovascularly and surgically treated aneurysms. (24)
Studies to determine the outcome based on multiple preoperative,
intra operative and post operative factors are lacking. In this study we
have tried identifying multiple pre operative , intra operative and post
operative risk factors which could affect outcome.

Aim and objective
3
AIM AND OBJECTIVE
AIM : To understand the varied clinical picture, radiological and
operative findings of good grade patients with symptomatic,
angiographically proven, surgically managed ICA communicating
segment aneurysm.
OBJECTIVE:
1.To study the outcome of operated posterior communicating artery
aneurysm.
2.Factors influencing outcome
The outcome would be measured as quality of life, presence or
absence of neurological deficit and independence to work using modified
rankin score.

Material and Methods
4
MATERIAL AND METHODS
Total of 100 consecutive patients who underwent surgical clipping
for symptomatic angiographically proven Internal carotid artery (ICA)
communicating segment aneurysm between January 2013 and May 2017
were analysed. Retrospective data of patients was recorded from the
SCTIMST database. Follow up at 3 months was done based on SCTIMST
records database.
Inclusion criteria:
Patients who presented with symptomatic angiographically proven
ICA communicating segment aneurysm and then underwent
surgical management.
WFNS grade 1 and 2
Exclusion criteria:
Giant aneurysm; size > 2.5 cm
Patient lost to follow up

Material and Methods
5
The following factors were studied:
Pre operative factors :
1. Age
2. Sex
3. Symtom to surgery
4. Presenting complaints like headache, vomiting, diplopia, seizure.
5. Neurological deficits like third nerve palsy, hemiparesis or
hemiplegia.
6. Radiological features like Fischer grading, presence of
hydrocephalus, infarct, intraventricular blood, hematoma.
7. Aneurysmal factors like shape, number of lobes, direction of
fundus, size of aneurysm and neck, relation to PCoA and
perforators, presence of teet or bleb, fetal PCoA.
Intra operative factors:
1. Intra operative rupture
2. Temporary clipping
3. Duration of temporary clipping

Material and Methods
6
4. Type of clip used
5. Number of clip
6. Fundus opened or not
7. Relation to third nerve
8. Presence of atherosclerosis and calcification
9. Opening of lamina terminalis
Post operative factors:
1. Early and late infarct
2. Hematoma
3. Vasospasm
4. Need for CSF diversion like VP shunt
5. Decompressive craniectomy
6. Tracheostomy
7. Duration on ventilator
8. Post operative hospital stay
9. GCS at day 5 and discharge

Material and Methods
7
10. Rankin score at disharge
11. Deficit at discharge
12. Death
Follow up at 3 months:
1. Rankin score
2. Deficit
3. GCS
Outcome parameters: Rankin score at discharge and follow up at 3
months was primary outcome parameter. Factors predicting the outcome
were studied. Rankin score 0 and 1 was considered as excellent functional
outcome, 2 as mild disability, 3 and more as poor outcome. (43,61)
Statistical analysis: All pre operative, intra operative and post
operative variables were compared between the groups based on outcome
variables. Two -tailed Student t-tests , Mann- Whitney U test and Kruskal
Wallis test for continuous variables and Fisher exact test or Chi square
test for categorical variables was used. For factors which had association
with outcome variables simple logistic regression analysis was performed
to look at the odds ratio and confidence interval. For those which were

Material and Methods
8
significant after simple regression analysis multivariable regression
analysis was performed to adjust the effect in order to see the independent
factors predicting outcome. A p value of 0.05 or less was considered
statistically significant. All statistical calculations were made with widely
available SPSS software (SPSS 22.0).

Review of Literature
9
REVIEW OF LITERATURE
Posterior communicating artery aneurysm are the aneurysm that
arise from the communicating segment of internal carotid artery.
ANATOMY:
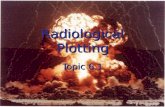
The posterior communicating artery (PCoA) bisects the supra-
clinoid internal carotid artery (ICA) into an ophthalmic segment from the
distal dural ring to the PCoA, and a communicating segment from the
PCoA to ICA bifurcation. (Fig 1)The PCoA originates from the
posterolateral surface of the proximal internal carotid artery, curves after
its origin and then sweeps posteromedially. It travels along the superior
surface of the oculomotor nerve, and intersects the posterior cerebral
artery (PCA) to mark the end of the P1 segment and the beginning of the
P2 segment. Approximately eight anterior thalamoperforating arteries
originate from the superior surface of the PCoA along its course and
ascend to the hypothalamus, anterior thalamus, internal capsule, tuber
cinereum, floor of third ventricle, posterior perforated substance, optic
chiasm and tract, and pituitary stalk.(1-3). PCoA aneurysms almost
always arise from the superior aspect of the PCoA along the lateral
surface of the ICA.(Fig 2)The anterior choroidal artery (AChA) is the
most important branch associated with PCoA aneurysms, lying adjacent

Review of Literature
10
to the distal neck. The AChA arises from the posterior wall of the
communicating segment, but can also arise from the PCoA,ICA
bifurcation and the proximal M1 segment. Damage to AchA can cause
hemiplegia, hemianesthesia, and hemianopsia. Hence while treating
PCoA Aneurysm PCoA, thalamoperforators and AchA should be taken
care of. (3)
Figure 1:Superior view showing origin of Posterior communicating
artery dividing ICA into communicating and ophthalmic segment.
Figure 2: Showing the origin of PCoA aneurysm.
BA: Basilar artery, Tent: Tentorium, MCA: Middle cerebral artery, ICA: Internal carotid artery, OphA:
Ophthalmic artery, PCA: Posterior cerebral artery, SCA, Superior cerebellar artery, III: Third nerve, II:
Optic nerve
Figure 1 Figure 2

Review of Literature
11
Fetal posterior cerebral artery (PCA) is an important variant.
During embryogenesis, the PCoA initially supplies the occipital lobe, but
the P1 segment enlarges to supply this territory and the PCoA shrinks to
produce the classic circle of Willis anatomy. The transformation fails to
occur in as many as 20% of patients, and the P1 segment remains
hypoplastic or atretic. The fetal PCA must be recognised and preserved
when clipping PCoA aneurysms because its compromise can result in
occipital lobe infarction.(4)
The direction of the dome of the PCoA aneurysm has significant
surgical implications. A classification system was described by
Yasargil.(4) When the fundus points anterolaterally, the origin of the
PCoA artery may be hidden by the aneurysm. In addition, the aneurysm
may be adherent to the clinoid process requiring careful dissection so that
the fundus may be mobilised and the origin of the PCoA is visualised
during application of a clip. A superolateral fundus is occasionally
encountered in which the dome points into the sphenoid ridge.
Haemorrhage of these aneurysms may cause a subdural hematoma. In
contrast, a posterolateral superior fundus points into the temporal lobe
and is often associated with an intraparenchymal hemorrhage and/or
hemorrhage into the temporal horn of the ventricle. A posterolateral
inferior fundus often penetrates the Liliquist membrane pointing into the

Review of Literature
12
interpeduncular fossa. These aneurysms are also associated with
oculomotor nerve palsy. A posteromedial inferior dome is rarely
encountered. These aneurysms are often sidewall aneurysms of the
ICA.(5)
Pathology of formation of aneurysm:
The underlying mechanism in formation of aneurysm are
multifactorial (6).Cebral JR et al in their study on aneurysm have
analysed that the rupture of saccular aneurysm is the consequence of the
inability of the wall to contain the hemodynamic loads and rupture occurs
when wall stress exceeds wall strength (7). Aneurysm occur by
degenerative changes secondary to hemodynamic stress (8). Degeneration
and repair have a balance until aneurysm rupture. Hemodynamic stress
leads to degenerative endothelial damage which exposes collagen leading
to formation of a fibrin matrix that triggers a repair process that remodels
the wall of the aneurysm, modifying the geometry and creating aberrant
flow conditions in the lumen. As the repair and degeneration process
continues the repair mechanisms are interrupted and the aneurysm wall
matrix degenerates and becomes too fragile to resist hemodynamic
pressure and eventually the aneurysm ruptures (9)
The location of the aneurysm is an important factor that influences
the hemodynamics, wall structure and determines whether the peri-

Review of Literature
13
aneurysmal environment is constraining or protective for aneurysmal
rupture. (7). Saccular aneurysms usually arise at the distal carina of
arterial bifurcations, where the vessels are exposed to maximum impact
of wall shear stress.(10). PCoA aneurysm tend to be more common
because of the turbulence created by the arterial origin at an angulation
with ICA. Several studies have shown that smooth contact of the
aneurysm with surrounding structures provide protective support to the
aneurysm dome by decreasing the wall stresses near the fundus, while
increased wall stresses can be created by sharp contacts(11). PCoA
aneurysm touch the surrounding intra cisternal and juxta cisternal
structures including cranial nerves, adjacent brain parenchyma, cranial
base bone, dural folds, dura mater, bridging and surface veins, small
arteries, and arachnoid trabeculae. A PCoA aneurysm projecting laterally
will be unable to extend beneath the oculomotor nerve and will compress
the superomedial aspect of the oculomotor nerve. In addition, when the
PCoA aneurysm extends laterally, the aneurysm dome comes into contact
with surrounding hard structures such as the tentorial free edge and
deformation may be observed on the dome(12). Hence PCoA aneurysm
attached to tentorium are more susceptible for rupture whereas those
attached to third nerve can present with symptomatic third nerve palsy.

Review of Literature
14
Risk factors for aneurysmal rupture:
Age and gender: The incidence of aneurysm increase with
increasing age. The maximum incidence is between 50 - 70 years
thereafter decreases(12, 13). Female gender is considered to be risk factor
for both aneurysm formation and growth, with aneurysms 1.6 times more
likely to occur in women than in men.(12) The cause of increased female
predilection is not clear as most of the risk factors like smoking,
hypertension, atherosclerosis are more common in men. (14) As the
incidence of subarachnoid haemorrhage (SAH) is found to occur more in
the post-menopausal period, a mechanism involving compromised arterial
integrity as a result of a drop in estrogen levels has been proposed. (14,
15)
Hypertension: Hypertension is considered as an independent risk
factor for SAH. Rivero Rodriguez et al in their study on patients with
subarachnoid haemorrhage found unfavourable outcome with
hypertension.(16). The underlying mechanism is proposed to be the
endothelial damage and remodelling created by hypertension leads to
increase incidence of aneurysmal formation and rupture.Intracranial
arteries are composed of the outer layer of the adventitia, a muscular
media that maintains most of the vessel wall integrity and the inner layer
of intima. They are different from other vessels in the body as they do not

Review of Literature
15
possess external elastic lamina. Therefore, there is less elasticity of the
media in addition to the thinner adventitia compared to the extracranial
artery wall. These vessels are also situated in the subarachnoid space,
which has no surrounding connective tissue to support the vessels. These
factors make intracranial arteries susceptible to the formation of saccular
aneurysms, making their occurrence fairly common in hypertensive
patients. (17,18,19)
Hyperglycemia: Hyperglycemia has been associated with
morbidity and poor outcome in patients with SAH(16, 20). Several
studies have shown that systemic glucose levels affect glucose
availability to the brain and can impact cellular metabolism and energy
production. Aneurysmal SAH patients have impaired glucose transport
and systemic glucose levels fluctuation can significantly affect the
cerebral metabolic demand(16, 21)
Other like ethnic race, family history, cigarette smoking are
considered as risk factors for aneurysm formation and rupture. Prevalence
of aneurysm is higher in Caucasian than in African American patients.
(7). Autosomal Dominant Polycystic Kidney Disease (ADPKD) or Ehlers
- Danlos Syndrome (EDS) Type IV, have been associated with
intracranial aneurysms.(7)

Review of Literature
16
Clinical presentation:
Symptomatic third nerve palsy and sub arachnoid haemorrhage
(SAH) are the most common presentations of PCoA aneurysm. 1.3-7.9%
of aneurysms may present with a subdural hematoma (SDH) and PCoA
aneurysm is responsible for the haemorrhage is 43% of cases.(5, 22)
Presentation as third nerve palsy:
The course of the oculomotor nerve parallels the PCoA. The nerve
originates from the interpeduncular fossa of the midbrain, courses
between the P1 PCA and superior cerebellar artery (SCA). It attaches to
the membrane of Liliequist and climbs to the oculomotor triangle, a dural
space bordered by the tentorial edge laterally, the petrous apex
posteriorly, and the interclinoidal line medially (the line between the
anterior and posterior clinoid processes). The nerve enters its dural sleeve
at the triangle’s anterior apex to exit the subarachnoid space and travel in
the roof of the cavernous sinus, just below the anterior clinoid process.
PcoA aneurysm projecting posteriorly laterally and slightly inferiorly will
impact the nerve in the cisternal segment of nerve. Resulting palsy will
cause diplopia, the eye deviation laterally and inferiorly, or the ―down
and out‖ eye. Involvement of pupillary fibres will cause mydriasis. Palsy
of levator palpebrae superioris will cause ptosis. (23). These palsies may
be complete or incomplete.(24)

Review of Literature
17
Approximately 38% of patients with PCoA aneurysms develop
oculomotor palsy as their presenting symptom(3, 25). Roughly 70% of
patients present with a complete oculomotor nerve palsy, while 30%
present with a partial oculomotor nerve palsy (5). Acute third nerve palsy
can occur with an expanding PCoA aneurysm. Therefore, such a clinical
presentation requires urgent evaluation and treatment. Compression,
either by enlargement of the aneurysm or pulsation of the aneurysm, is
considered as the main cause for third nerve palsy.(26). Absence of
oculomotor palsy indicates that the aneurysm may either be small in size,
or be projecting posterolaterally above the tentorium or medially
involving the inferior wall of the ICA.(3) Treatment of intracranial
aneurysms should not be delayed even if patients do not have
subarachnoid haemorrhage(26). Long-term nerve compression results in
neuronal injury and neural degeneration affecting postoperative recovery.
Several studies found that oculomotor palsy is irreversible even after
decompression if the symptoms lasted more than 4 weeks.(26)
The size of the aneurysm is considered to be one of the most
important reasons for direct compression of the nerve. Teasdale et al.
reported in their series of 27 patients with unruptured PCoA aneurysms
found that third nerve palsy is caused by anuerusym that are 7 mm or
greater (81). The curve of ICA also determines the risk of third nerve

Review of Literature
18
palsy. Yanaka et al. has mentioned that unruptured aneurysms measuring
less than 10 mm can cause third nerve palsy when the anterior cavernous
genu of the ICA forms an acute angle and the supraclinoid portion runs
posterolaterally.(29) Kurokawa et al. also pointed out that when the
intracranial part of the ICA ran horizontally, rather than vertically, along
the cranial base, even small ICA–AChA aneurysms could cause third
nerve palsy(27, 28)
The ICA to anterior -posterior clinoid process distance is the novel
concept used to explain the presence of absence of third nerve palsy. All
ICAs run under the anterior–posterior clinoid (ACP) process, and it is
easy to measure the ICA–APC distance using the recently developed
radiological modalities. In study by Anan et al, the ICA– APC distance
was significantly shorter in patients with positive third neve palsy than in
the negative third nerve palsy group. (27, 29). This means that the PCoA
aneurysm should be closer to the third nerve when the ICA runs closer to
the skull base. The pulsatility of the ICA may more easily affect the nerve
when the ICA–APC distance is short.(27)

Review of Literature
19
Presentation as SAH:
Size, location, shape and projection determining risk of rupture :
PCoA aneurysm even if they are unruptured carries a high risk of
rupture. International Study of Unruptured Intracranial Aneurysms
(ISUIA) study gives the impression that small aneurysms < 7mm in
anterior circulation have a minimal risk of rupture(12). But the rupture
risk for PCoA aneurysm matches that of rupture risk of posterior
circulation aneurysm. (5)The prevalence of small ruptured PCoA
aneurysms are particularly high, with 87.5% of aneurysms measuring less
than 10 mm in diameter and 40% measuring less than 5 mm in diameter.
(7, 12). According to Laplace’s law (which states that the tension
required to withstand a given pressure increases with the diameter of a
vessel), the critical diameter for rupture is proportional to the average
wall thickness. This suggests that aneurysms at smaller arteries may
rupture at smaller sizes since they had initially thinner walls. These
observations seem to indicate that rupture risk depends on the location,
and that aneurysms at the PCoA are more prone to rupture than
aneurysms at other locations even in smaller size(7)
Japanese study on the natural course of unruptured cerebral
aneurysms (Unruptured Cerebral Aneurysm Study [UCAS]) also showed
that a PCoA aneurysm is more likely to rupture(12) .

Review of Literature
20
The bleb formation is frequently associated with rupture. In a
recent study focusing on bleb formation in an effort to gain insight into
the mechanisms underlying aneurysm rupture, the highest shear stress
values were at or adjacent to the bleb formation(12). Non-spherical
shapes (oval, oblong and multilobulated) are found to be associated with
rupture. (7) Similarly true PCoA aneurysm have also higher chance of
rupture at smaller size. (5)
Similarly laterally projecting aneurysm are more likely to rupture
due to peri aneurysmal environment characteristics like attachment to
tentorium.
Morphological and hemodynamic factors affecting rupture:
Morphological factors like Aspect ratio, size ratio, inflow angle
and hemodynamic factors like wall shear stress, oscillatory shear index,
normalised wall shear stress are considered as risk factors for aneurysmal
rupture. The aspect ratio (AR) between ruptured and unruptured
aneurysms was found to be significantly different, with almost 80% of
ruptured aneurysms having AR>1.6 while almost 90% of unruptured
aneurysm having AR<1.6 (7). In a study by Lv N et al the inflow angle
was considered as significant factor for aneurysm rupture.Aneurysm with
more inflow angle had higher risk of rupture.(30). But once the aneurysm

Review of Literature
21
ruptures it is difficult to measure these morphological and hemodynamic
factors.
True PcoA aneurysm and risk of rupture:
―True‖ PCoA aneurysms are the on in which the aneurysm actually
arises from the PCoA artery as opposed to the junction with the ICA.
They are rare, accounting for 4.6–13% of PCoA aneurysms (0.1–2.8% of
all intracranial aneurysms)(31) True PCoA aneurysms typically arise
within 2–3 mm of the ICA (31, 32). They tend to be smaller than
junctional PCoA aneurysms, but have higher risk of rupture(7)They have
have a classic appearance on imaging where dome projects posteriorly.
True PCoA aneurysms are often associated with a dominant PCoA, in
which the PCoA is the major blood supply to the posterior cerebral artery.
(31).The thalamoperforating arteries can arise from the PCoA both
proximal and distal to the aneurysm(31). Hence preservation of both
PcoA and thalamoperforating arteries are important in clipping of these
aneurysms. (31)

Review of Literature
22
Imaging of PCoA aneurysm:
CT plain:Plain CT is used as an initial investigating tool for
detecting subarachnoid blood. In acute setting the higher attenuation of
blood as compared to normal parenchyma allows 100 % sensitivity for
diagnosis SAH within first 6 hours.(33). Although CT is an excellent
modality for evaluating acute subarachnoid hemorrhage, in the subacute
setting, from six hours to one week after hemorrhage, the ability to detect
subarachnoid hemorrhage with CT drops dramatically because of the
brain’s normal degradation of hemorrhagic blood products. The
sensitivity drops as the days passes after SAH and comes down to 85 %
after five days, 50 % after one week, and 30 % after two weeks (33, 34)
In one study the sensitivity of CT to detect SAH dropped to 36.5% after
five days. (33)A ruptured PCoA aneurysm is suggested when clots are
located in the ipsilateral carotid cistern, which may extend into the
interpeduncular and the Sylvian cisterns. Massive rupture of an aneurysm
may cause a temporal lobe hematoma or an intraventricular hemorrhage.
Persistent localised clot on delayed CT confirms the location of the
ruptured aneurysm in cases of multiple aneurysms.(3). Attention should
be paid to the calcified ICA because temporary clips cannot be applied to
the stiff ICA. Exposure of the carotid artery from the neck is mandatory
in such patients.

Review of Literature
23
Several grading systems have come through ages to predict the
severity of SAH and risk of developing vasospasm. Davis et al used a
four-point scale and correlated with development of vasospasm (35, 36).
The primary limitation of this classification was that it did not allow
distinctions to be made between large and small collections of blood in a
specific subarachnoid compartment.
Friedman et al in a retrospective study found a high correlation
between severe vasospasm and the presence of subarachnoid clots greater
than 5 X 3 mm in diameter in cisterns and fissures in horizontal plane and
clot greater than 1 mm thickness in vertical plane. They graded the blood
in cisterns and fissures to assess the risk of vasospasm. (36, 37). Fischer
grade is used to assess the degree of SAH based on the cisternal blood.
Hijdra and colleagues demonstrated the importance of intra
ventricular blood(IVH). (36, 38). Classen et al used the IVH in addition
to cisternal blood and demonstrated that a modified Fischer scale is better
predictor of outcome in terms of vasospasm. (36, 39)

Review of Literature
24
Table 1: Showing modified Fischer grading for SAH(36,38):
Grade Description
0 No subarachnoid blood
1 Minimal / thin SAH, no IVH in both lateral ventricle
2 Minimal / thin SAH, with IVH in both lateral ventricle
3 Thick SAH and no IVH in both lateral ventricle
4 Thick SAH with IVH in both lateral ventricle
CT angiogram: This is helpful in determining the location and
aetiology of the haemorrhage.(33)Studies have shown 97 % sensitivity
rate for detection of all aneurysm sizes(33, 40) The relationship between
anterior clinoid process and aneurysm can be found on CT angiogram.
Prominent posterior clinoid process can hinder the process of clip
placement and can be assessed pre operatively on CT angiogram. (3)
MRI for detection of SAH and aneurysm: MRI has advantages
over CTA in that it does not use ionising radiation and offers the ability to
obtain images without the need for administration of intravenous contrast
agents. Fluid attenuated inversion recovery (FLAIR) sequences produce
strong T2 weighting while suppressing the cerebrospinal fluid (CSF)
signal and can be particularly useful for detecting subarachnoid

Review of Literature
25
haemorrhage especially in subacute period. (33) Rocha et al had
demonstrated 100 % sensitivity for subacute SAH for MRA as compared
to 66 % for CTA (41). The use of time-of-flight (TOF) sequences on
MRA eliminates the need for administration of contrast agents(33). MRA
is generally not the diagnostic test of choice for the evaluation of cerebral
aneurysms in the acute setting and is reserved as a screening test or for
follow-up.
Angiogram: Angiography is the most reliable study to define the
precise location, size, neck, shape, and direction of the aneurysm, and to
confirm the presence of multiple aneurysms. It can separately evaluate
the arterial, capillary, and venous phases. (33) The direction of PCoA
aneurysm gives the idea of attachment to surrounding structures. Postro
laterally projecting aneurysm can be attached to oculomotor nerve or
tentorium while laterally projecting aneurysm may be attached to
temporal lobe. The latter condition might require removal of uncus. A
short and dilated ICA or closed carotid siphon hinders use of a temporary
clip on the ICA proximal to the PCoA. It may be necessary to drill off the
anterior crinoid process or expose the carotid artery in the neck for
proximal control in such cases. PCoA is found medial to the ICA on the
anterior-posterior view of the angiogram. This means that the PCoA can
be exposed easily in the opticocarotid triangle. Fetal type PCoA appears

Review of Literature
26
overlapped with the ICA on the anterior-posterior projection of the
angiogram.The relationship between the AChoA and the aneurysm
should be defined to ensure that this vital artery remains patent after clip
placement. The assessment of collateral circulation on cross- compression
study may predict the tolerance of temporary occlusion of the ICA. It is
also important to assess the venous drainage pattern of the sylvian and the
deep venous systems, all of which should be preserved to prevent
postoperative venous infarction. (3)
Predicting whether the anterior clinoidectomy is needed or not can
be done by pre operative angiogram. It was first mentioned by Ochiai et
al. in 1989 (42). In the study by Ochiai et al, anterior clinoidectomy was
necessary in 3 patients with internal carotid–PCoA aneurysms. The
authors noted that the distance between the posterior wall of the carotid
―knee‖ of the clinoidal ICA and the proximal neck of the aneurysm on
lateral angiography in 3 cases of anterior crinoid process resection was
shorter than 9.6 mm. (42) However, the number of cases was too small to
reveal any statistical significance. Along with measurement of the
distance from the aneurysm to the ACP, evaluation of the tortuosity of the
ICA, provide valuable parameters to predict the necessity of ACP
removal in PCoA aneurysm surgery. (15)

Review of Literature
27
Treatment options:
The treatment options for ruptured PCoA aneurysm is either
clipping or coiling. Several studies have shown that the mortality and
morbidity is equal for both clipping and coiling with respect to ruptured
PCoA aneurysm. International Subarachnoid Hemorrhage Aneurysm
Trial (ISAT) showed that coiling is better in terms of functional outcome
based on mRS score with respect to PCoA aneurysm.(43). But the rate of
rebreeding and recurrence was higher in coiling group. Several
drawbacks are associated with ISAT trial as only 20% of patients were
randomised, study was done mainly in European centres, predominantly
small aneurysm and low grade haemorrhages were taken to consideration,
used CT angiogram to randomise instead of angiogram.
This lead to Barrow ruptured aneurysm trial and Chinese trial. (44,
45) BRAT 6 year follow up showed clipping is as good as coiling for
anterior circulation aneurysm and coiling to be better for posterior
circulation aneurysm. In BRAT trial PCoA was grouped under anterior
circulation. Chinese study had also not shown difference between coiling
and clipping for PCoA aneurysm. Lanzino et al conducted a meta-
analsysis on the 3 prospective controlled studies. Pooled data showed
poor outcome at 1 year to be lower in the immobilisation group and no
difference in mortality between group. Rebleeding rates within the first

Review of Literature
28
month were higher in coiled patients. Long term follow up showed
similar results between the groups(46). Surgical clipping has lower re
operative rates, lower rebelled rates and can also relieve the
hydrocephalus. The treatment for ruptured PCoA aneurysm is mainly
clipping. Over the years due to microsurgical techniques the outcome of
clipped PCoA aneurysm have significantly improved.(47,48)
Intra operative characters and technique of clipping:
Craniotomy:
The standard pterional craniotomy position, head elevation with
neck extension and rotation of 30 degree to opposite side is used for
clipping of these aneurysm. (3). In patients with short supraclinoid
ophthalmic segment of the ICA, dilated and calcified arteriosclerotic ICA
or closed carotid siphon, the draping of neck for cervical carotid exposure
is required for proximal control. (3)A standard pterional craniotomy is
fashioned for an exposure allowing a wide range of inclination for the
clip-applying forceps.The sphenoid ridge is drilled off down to the
superior orbital fissure, and the orbital roof and the subtemporal bone are
flattened to get an unobstructed view along the cranial base. The dura is
incised based on sphenoid ridge and margin of dura is everted and pulled
over a sponge with traction stitches to minimise epidural bleeding and to
prevent blood from dripping into the field (3)

Review of Literature
29
Brain relaxation:
Brain relaxation is the key to the rapid and atraumatic exposure of
PCoA aneurysms in the carotid cistern. Adequate brain relaxation can be
obtained by opening the cisterns. It may sometimes be necessary to open
the Liliequist membrane or lamina terminalis to relieve the intracranial
pressure. Opening of lamina terminalis is an effective way of relieving
intra cranial pressure. (3,4)
Opening of sylvian fissure:
The frontal operculum can be detached from the temporal lobe by
opening the Sylvian fissure. Incision of the arachnoid membrane
connecting the fissure is easy and atraumatic when the brain is fully
relaxed and the fissure is filled with CSF or blood. (Fig 4 )After
assessment of the cerebral venogram including the venous drainage
pattern through the Sylvian and deep venous system, the distal Sylvian
fissure is entered on the frontal side of the Sylvian vein (86).One or more
veins bridging the Sylvian fissure may be encountered, and these may be
sacrificed as necessary. Deep cerebral veins such as the deep middle
cerebral vein, the basal vein of Rosenthal, and the deep vein of the orbital
lobe in the fissure should be preserved to prevent venous infarction even
if the deep veins limit the opening of the fissure. A sharp dissection
prevents injury of the pial membrane of the frontal operculum.

Review of Literature
30
As the fissure is split, the frontal lobe can be mobilised and
retracted progressively. Dissection is then directed to the chiasmatic
cistern overlying the optic nerve. As the thick arachnoid bands connect
the frontal side of the proximal Sylvian fissure with the temporal side, it
is necessary to cut the bands to release the frontal and temporal lobes.
Wide opening of the Sylvian fissure exposes the M1 and M2 segments of
the middle cerebral artery and the carotid bifurcation. After this
procedure, the whole length of the supraclinoid ICA as well as the
aneurysm can be exposed with minimal brain retraction.(3,4,86)
Figure 4: Steps of dissection for approaching posterior communicating
artery aneurysm (86)
Approach to neck of aneurysm:
The carotid cistern is opened along the medial border of the ICA.
The proximal ICA is prepared for temporary occlusion. If the exposed
ophthalmic segment of the ICA is too short for temporary clip placement,

Review of Literature
31
it is necessary to drill off the anterior clinoid process. Sometimes the
aneurysm is hidden under the uncus or embedded in a large amount of
clot. Therefore, it can be very dangerous to expose the aneurysm by
removing the clot from the dome of the aneurysm before applying the
temporary clips. The distal PCoA is usually identified in the opticocarotid
triangle, which is the space formed by the ICA, the optic nerve, and the
A1 segment of the anterior cerebral artery. It may be difficult to expose
the fetal type PCoA before clip placement because the artery is usually
hidden beneath the ICA or the aneurysm. As the dissection is continued
toward the carotid bifurcation, the AChoA can be identified, and the
distal neck of the aneurysm is usually found immediately proximal to the
artery. It may be much safer to remove the uncus around the aneurysm by
a small subpial resection than by attempting hazardous dissection and
retraction to expose the neck of the aneurysm and the proximal PCoA.
This subpial dissection is an appropriate technique for safe exposure of
the aneurysm, because it leaves the pia and arachnoid attached to the
dome, and reduces the risk of mechanical violation. (3)Temporary clips
may be used when further dissection of the neck of the aneurysm appears
risky.

Review of Literature
32
Identification of aneurysm neck:
Majority of PCoA artery aneurysm originate distal to the PCoA
origin. Tracing the posterolateral wall of the proximal ICA can help in
identification PCoA origin, which is often visualised as a knuckle (Fig
4)(47).
In contrast to traditional PCoA aneurysms, for which the aneurysm
dome may be readily visible, true PCoA aneurysms most commonly arise
in what is typically an intra-operative blind spot 2–3 mm posterior to the
origin of the PCoA at the ICA. The PCoA should thus be followed
posteriorly to visualise the neck of the aneurysm. (31)
Clip placement:
Once the neck of the aneurysm is defined, the clip is advanced
between the PCoA and the AChoA. For wide-necked aneurysms, the clip
is placed parallel to the ICA to avoid ―dog ear‖ remnants or stenosis of
the ICA. Care should be taken to exclude branches of the ICA from the
clip blades.
When it is impossible to clip an inferior wall aneurysm of the ICA
because of the branches, wrapping-with-clipping can be done. Wrapping
includes placing a muscle or cellulose fabric circumferentially which
leads to fibrosis around the aneurysm. A bent clip is applied over the

Review of Literature
33
fabric that is encircling the ICA and the aneurysm, while both ends of the
fabric are held together with forceps (3). When branches or perforators
prevent circumferential application of the fabric, it may be necessary to
split the fabric partially into two or three strips to accommodate the
branches or perforators without squeezing. If the neck of the aneurysm is
torn during dissection or clip placement, a piece of cellulose fabric sheet
or muscle is placed on the torn site and a clip is used to seal the tear.
Papaverine solution is instilled around the ICA and its major
branches to relieve possible vasospasm caused by manipulation after
removing the temporary clips. Direct application of concentrated
papaverine on the oculomotor nerve is avoided as it may cause mydriasis.
The clip and the aneurysm neck are inspected to confirm the
complete occlusion of the aneurysm and the sparing of the branches,
including the PCoA and the AChoA and perforators.
It is also important to check for the possibility of clip movement or
rotation after release of the brain retractors, because the repositioning of
the frontal operculum or the temporal pole may push the handle of the
clip. (3)

Review of Literature
34
Complications:
Intra operative complications relating to the nature of aneurysm:
PCoA aneurysms with a posterior projection is correlated with a
higher incidence of intraoperative complications than those with a lateral
projection. Posterior projecting aneurysm will have adhesions to
perforators, the posterior part of aneurysm is obscured behind the ICA,
and the dome is surrounded by only arachnoid trabeculae. All these
factors contribute to difficulty in clipping of these aneurysm and high
incidence of intra operative rupture. (49). On the other hand, the dome of
an aneurysm with a lateral projection often attaches to the brain
parenchyma of the temporal lobe, which enables subpial dissection of the
aneurysm, decreasing the risk of rupture. Posterior projecting aneurysms
often have a wide neck involving the origin of a fetal PCoA. At
intraoperative rupture, clamping of not only the ICA but also the fetal
PCoA is required for flow control, and a longer clip blade must be
applied to the wide neck in the limited surgical corridor created by
multiple temporary clips. (49)
PCoA aneurysms with lateral projection are more likely to cause
intracerebral hematoma as a result of attachment to the temporal lobe.
Patients with these aneurysms presents with poorer initial neurological
status by rapidly increasing intracranial pressure(49, 50). Thus the poor

Review of Literature
35
outcome of laterally projecting aneurysm is related to poor initial grade
than the aneurysm factor per se.
Superolateral projecting aneurysm are also reported to have worse
prognosis. One theory might be that the hemodynamics of its location
produce more shear stress on the wall of the aneurysm making it more
prone to rupture and produce a greater amount of SAH and/or that they
have more space to grow quickly debilitating the aneurysm wall at a
higher rate. (51)
Large/giant size is reported as another risk factor of procedure
related complications of the aneurysm surgery.(49)The size of an
aneurysm is not a good predictor of rupture. Aneurysms develop and
grow at different rates and the hemodynamics of their location differ
depending on their orientation in the parent vessel. (51)
Post operative complications:
Vasospasm: Blood released under high pressure into the basal
subarachnoid cisterns as a result of a ruptured aneurysm can trigger a
cascade of molecular events that leads to a narrowing of the major
intracranial arteries, which is called cerebral vasospasm. Extreme
vasospasm can lead to infarction. Vasospasm follows a typical time
course in that its onset usually occurs within 1 week after the

Review of Literature
36
hemorrhage, it reaches its maximum severity between Days 7 and 10
post-SAH, and it usually dissipates after 14 to 21 days. 5 to 11% of
patients continue to suffer permanent disability as a result of
vasospasm.(36)
A mainstay in the prophylaxis and treatment of cerebral vasospasm
in the past was hyperdynamic therapy, also known as ―triple-H therapy,‖
which utilised the three approaches of hypervolemia, induced
hypertension, and slight hemodilution with the aim of improving cerebral
blood ow (CBF). Lennihan et al. demonstrated that hypervolemic therapy
resulted in increased cardiac filling pressures and fluid intake but did not
increase CBF or blood volume compared with normovolemic therapy,
concluding that prophylactic hypervolemic therapy is unlikely to confer
benefit. (52, 53)Prophylactic hyperdynamic therapy was found to have
greater costs and more frequent complications such as excess bleeding,
congestive heart failure, and infections (53) Hence at present the
recommendation for hyper dynamic therapy is for treatment and not for
prophylaxis.(53)
Hydrocephalus: Acute hydrocephalus within the first 24 h of
hemorrhage may develop due to blood within the basal cisterns or in the
ventricular system causing CSF obstruction. Acute hydrocephalus within
the first 24 h of hemorrhage may develop due to blood within the basal

Review of Literature
37
cisterns or in the ventricular system causing CSF obstruction. In a study
by Varelas et al on 108 patients, hydrocephalus was present in 30% of the
patients with aneurysmal SAH and found that shunt dependent
hydrocephalus was more in patients who underwent coiling. The
rationale behind this being subarachnoid blood may be cleared by intra
operative lavage which is not possible for coiling group. (54)However, in
a an another retrospective study comparing 100 matched patients who had
suffered SAH, either clipping or coil embolization, did not significantly
affect the development of chronic hydrocephalus.(55) In an another study
by Woernle et al shunt dependency was found in 23.6 % of patients and
GCS 3-7 at admission and coiling were predictors of shunt
dependency.(56)
Infarct: The incidence of infarct in aneurysm surgery is reported to
be between 24 to 35 %(57). Early onset infarct are those infarcts which
develops within 0–5 days. Etiology of such infarct is mostly related to
site of ruptured aneurysm. They are thought to be due to either perforator
injury or due to permanent or temporary occlusion of artery or retraction
injuries. They are usually deep or cortical in distribution and are mostly
ipsilateral to the parent vessel bearing aneurysm. Secondly, late onset
infarcts were those infarcts that develops mostly after first week of
surgery. They are mostly diffuse, patchy, multiple and bilateral,

Review of Literature
38
etiologically perhaps due to a diffuse process like vasospasm.The
mortality among late onset infarct is also higher. (57). In PcoA aneurysm
the deep infarcts are secondary to occlusion of perforators supplying
basal ganglia and internal capsule. Literature quotes poor grade at
presentaion, higher Fisher’s grade on CT, intraoperative rupture and
prolonged temporary clipping as predictors of developing infarct in
operated cases of aneurysm.(57)
Outcome:
Approximately 10% to 15% of patients with ruptured aneurysm die
before reaching hospital. Of those who survive, 42% will be dependent,
46% will have some form of disability, and 12% will be left severely
impaired.(58)
Population based study informed mortality rates range from 8% to
67% with a significant morbidity among survivors (16). Some factors has
been related with mortality are female sex, severity of clinical
presentation, rebleeding, older age, preexisting severe medical illness,
global cerebral edema on computed tomography (CT) scan,
intraventricular and intracerebral haemorrhage, symptomatic vasospasm,
delayed cerebral infarction (especially if is multiple), hyperglycemia,
fever, anaemia, and other systemic complications such as pneumonia and
sepsis (16)

Review of Literature
39
In the ISAT trial involving 2143 patients, the long term mortality
among the clipped aneurysms was 14%. (43)
In a study by Ghani et al at three months after discharge, 33.3%
had the mRS score of 0 with no symptoms at all, and 33.3% had the mRS
score of 6 or had died. (19)
In a study by Lee K chang et al in their study on 424 operated cases
of PCoA aneurysm found that 7.3% had poor outcome.(3)
Hop et al.analyzed disabilities 1-48 months after the onset and
found that on average, 10-20% of survivors of aneurysmal SAH become
so disabled that they lose their independence and have to rely on others to
carry on in their daily lives(59)
In the meta-analysis by Nieuwkamp et al,55% of patients remained
independent and 19% were dependent on help for activities of daily living
1-12 months after the onset. (60)
In a study by Pegoli et al excellent outcome was noted in 236
patients (63.3%), including an mRS score of 0 in 122 (32.7%) and an
mRS score of 1 in 114 (30.6%). (61)

Review of Literature
40
Third nerve recovery
Some studies that compared coiling and clipping showed no
difference in results between these two treatments. Chen et al described a
series of 13 patients of whom 6 were treated with coil embolisation and 7
were treated with surgical clipping. Only two patients in the endovascular
cohort made a complete recovery, while six patients in the surgical cohort
made a complete recovery . Also they reported that 86% vs 33% of
patients had complete resolution of third nerve palsy after clipping and
coiling, respectively.(5, 62) Chang SI et al study showed a 70% complete
recovery rate which is similar to recovery rates in previous studies(26) .
In the case of a ruptured PCoA aneurysm, the aim of the treatment
is not only to safely exclude the aneurysm but also to increase the chance
of third nerve recovery. In meta-analysis by Gabarel et al, they have
shown that clipping achieved better oculomotor outcomes than coiling.
(24)
Although the studies done on oculomotor nerve recovery are small
and non randomised the general conclusion in literature is that patients
with can have slightly higher chance of recovery with clipping as
compared to coiling. (5)

Review of Literature
41
Study by Golshani et al have also shown that factors associated with a
higher likelihood of recovery include time to treatment, partial third nerve
deficit, and presence of sub arachnoid hemorrhage.(5)

Results
42
RESULTS
Total of 100 consecutive cases of communicating segment aneurysm
clipped between January 2013 to May 2017 were analysed. All cases had
underwent surgery at SCTIMST, Trivandrum.
The total number 554 aneurysm cases were clipped during this period.
Incidence: As per the aneurysm cases operated the incidence of PcoA
aneurysm was 18.05 %.
Age: The average age of presentation was 55.2 years.(Median 56 years).
Age didn't affect the outcome and there was no difference in outcome
whether patient is young or old. (Table 2)
Table 2: Relationship of age with mRS at 3 month follow up
Age median Total
Less than 56
years
More than
56 years
Modified
Rankin score
(mRS) at 3
month follow
up
Excellent (mRS 0
and 1)
42 38 80
Mild (mRS 2) 2 3 5
Moderate to
severe including
death(mRS 3 - 6)
6 9 15
Total 50 50 100

Results
43
Sex: Out of 100 patients 75 were male and 25 were female. The incidence
of SAH was more in female as compared to male. Other than the
incidence ,the functional outcome based on mRS, recovery from third
nerve palsy, duration of hospital and ventilatory stay and death was not
statistically significant between male and female.
Comorbidities:
Hypertension: The incidence of hypertension in the study was 42%.
There was no statistical significance for poor or good outcome with
hypertension.
Other comorbidities and risk factors: Diabetes was found in 11%, asthma
3%, hypothyroid 4 %, dylipidemia 12%, seizure and history of cerebral
25%
75%
Male Female

Results
44
vascular accident in 1% each. 14 % had multiple comorbidites and 52 %
had no comorbidity at all. None of these factors were predictors of
outcome.
Smoking and alcohol consumption was found in 32 % and 27 %
respectively and was not significantly associated with outcome.
Symptom, deficits and severity at presentation:
Headache was the most common presenting symptom seen in 90 % of
patients. Vomiting was seen in 40 %, third nerve palsy 27 %, loss of
consciousness 28 %, seizure 4 % and focal weakness in 7 %.
16 patients presented as unbled aneurysm out of which 8 patients had
third nerve palsy and the rest were incidentally detected or had multiple
aneurysm.
42
11
21
58
89
52
0.0
50.0
100.0
Hypertension Diabetes Other
Per
cen
tag
e
Present Absent

Results
45
27 patients had third nerve palsy at presentation and 20 patients had
associated SAH.(Table 3)
Table 3: Frequency of occurrence of third nerve palsy
Third nerve palsy Percent
Yes 27.0
No 73.0
Total 100.0
The GCS was 15 for 95 % of patients, 14 and 13 for 2% each and 12 for
1%.
90
40
27 28
4 7
0.0
50.0
100.0
Headache Vomiting 3rd nervepalsy
LOC Seizure Focalweakness
Per
cen
tage
Symptom at presentation (Percentage)

Results
46
The WFNS grade at presentation was 68% for Grade 1 and 16 % for
grade 2. 16 % were unbled aneurysm.
1 2 2
95
0.0
50.0
100.0
12 13 14 15
Per
cen
tag
e
GCS at presentation
68
16 16
0.0
50.0
100.0
1 2 Unbled aneurysm
Per
cen
tag
e
WFNS grade at presentation

Results
47
Radiological factors:
CT plain was done in all patients. CT angiogram (CTA) was done
in 90 % of patients, MRI angiogram (MRA) in 25 % and angiogram
(DSA) was done in 38 % of patients.
Modified Fischer grading was used to assess the severity of SAH.
16 % of patients were unbled, 11 % were in grade 1, 27 % in grade II, 25
% in grade III and 21 % in grade IV.
0
25
50
75
100
CTAMRA
DSA
Pre op radiology

Results
48
The severity of SAH based on modified Fischer grading didn't
affect the outcome. 8 patients had post operative vasospasm and its
relation with pre operative Fischer grading couldn't achieve statistical
significance as the number was small. (Table 4)
Table 4: Modified Fischer grade relation with Vasospasm
Vasospasm Total
0 1
Modified Fischer
grade
0 16 0 16
1 10 1 11
2 24 3 27
3 24 1 25
4 18 3 21
Total 92 8 100
16 11
27 25 21
0.0
50.0
100.0
0 1 2 3 4
Perc
enta
ge
CT Fischer grade

Results
49
Pre operative imaging features hydrocephalus, IVH, infarct, hematoma
didn't affect the outcome in terms of mRS or recovery from third nerve
deficit or death.
Although the number of patients with vasospasm was small, none of these
factors predicted the occurrence of vasospasm.
Similarly only one patient required VP shunt out of 13 patients who had
hydrocephalus.
20 16
7 13
2
80 84
93 87
98
0.0
50.0
100.0
IVH NoSAH(Unbled)
Pre op infarct Hydrocephalus Hematoma
Per
cen
tage
Pre op CT findings
Present Absent

Results
50
Aneurysmal factors:
All patients had PCoA aneurysm. 31% had multiple aneurysm. 5
patients had mirror aneurysm. Acom was the most common location
found in cases of multiple aneurysm.
Direction and relation of PCoA to aneurysm: Most of the aneurysm
were directed poster infer lateral direction (68 %). 64 % of the cases
PCoA was arising proximal to aneurysm 19 % from neck of aneurysm
and 17 % opposite to the origin of the aneurysm .
Morphology and size: 92 % were saccular aneurysm and 13 had
complex morphology in terms of bi or multilobes. Average neck size was
2.52 mm and average dome height was 5.2 mm and dome width 3.6 mm.
39 % of the aneurysm had a narrow neck(< 2.5 mm) and 49 % had wide
neck (2.5 - 5mm) with 5.4 % having very wide neck(> 5 mm). 90% of the
aneurysm were smaller than 10 mm.
47%
43%
10%
Aneurysm size
< 5mm 5-10 mm >10 mm

Results
51
Fetal PCoA and attachment to third nerve: 10 % of the patients had
fetal PCoA. The aneurysm was attached to third nerve in 22 % of
patients.
Intra operative factors:
Intra operative rupture occurred in 24 %. Clip and wrap technique was
used in 20 patients. Fundus was opened in 21 patients. 17 % had
atherosclerosis and 3 % had into aneurysmal thrombus.
Lamina terminals was opened in 24 % of patients and uncus was removed
in 4 % and clinoidectomy was done in 6 %.
Bilateral PCoA was operated at interval in 6 patients.
Temporary clipping was used in 38 patients and the average duration of
temporary clipping was 2.4 minutes.
Calcification was present in 2 % and atherosclerosis was present in 17%.
22 % had attachment to third nerve.
Straight clip was used in 47 % , curved in 25 %, right angled in 10 % and
fenestrated in 9 %.

Results
52
Post operative factors:
Post operative hospital stay was less then 12 days in 71 % of
patients and > 12 days in 29 % of patients. 94 % of the patient had
hospital stay of < 20 days. 17 patients had hemiparesis, with only 6
patients having immediate post op hemiplegia. Presence of hemiparesis ,
any post operative complication and duration of temporary clipping > 12
minutes affected the post operative hospital stay (> 12 days) after simple
logistic regression. (p < 0.05).
Duration on ventilator: 74 % of the patients had stay < 1 day on
ventilator. The presence of any complication prolonged ventilator stay.
Presence of third nerve palsy, intra operative rupture, temporary clipping,
presence of hemiparesis were significant after univariate analysis. No
factor was statistically significant for predicting the duration on ventilator
after multivariate analysis.
Infarct: The incidence of pre op infarct was 7 %. 22 patients developed
post operative infarct. Out of which 11 had early radiological infarct and
11 had late infarct which manifested clinically. 14 out of 22 (63.63%)
patients had underwent temporary clipping. 24 out of 78 (30.7%) patients
had underwent temporary clipping in the other group who didn't had
infarct (Table 5). Temporary clip, intra op rupture and use of complex
clip were predictors of infarct after simple logistic regression. No factor

Results
53
was statistically significant for predicting the infarct after multivariate
analysis.
The average duration of temporary clipping was 5.72 minutes as
compared to 1.48 minutes for those patients who didn't had infarct. The
incidence of infarcts in WFNS grade I and II patients was 20 % and 31.5
%.
Table 5: Relation of infarct with temporary clipping
Temp clip Total
No Yes
Early plus late
infract
(Radiological and
clinical)
No 54 24 78
Yes 8 14 22
Total 62 38 100

Results
54
The post operative complications are listed in the table 6.
Table 6: Post operative complications
POST Operative complication
Complication Number
Early infarct 11
Late infarct 11
Hematoma 3
Decomp craniectomy 6
Vasospasm 8
Tracheostomy 7
Hemiparesis 17
3rd nerve deficit 16
Aphasia 1
Vegetative state 1
Hyponatremia 5
Pulmonary embolism 6
DVT 1
VP shunt 1
COPD 1
Pneumothorax 1
MI 1
EDH 1
Chemical angioplasty 3
SDH/ EDH 2

Results
55
OUTCOME:
FUNCTIONAL OUTCOME:
Modified rankin score was used to assess the outcome at discharge
and at follow up of 3 months. mRS 0 and 1 were considered excellent
functional outcome, 2 as mild disability including the presence of third
nerve palsy, 3 or more than three as poor outcome including death
48 % had excellent outcome, 23% had mild disability, 29 % had
moderately to severe disability which includes 9% mortality. Follow up at
3 months patients had significant recovery with 80 % showing excellent
functional outcome with 5 % having mild disability and 6 % severe
disability.
Intra operative rupture, temporary clip and post operative infarct
were significant predictors of poor outcome after simple logistic
regression (Table 7,8). Presence of post operative infarct (OR : 0.125 95
% CI 0.030 - 0.531) affected the outcome in terms of mRS at discharge
after multivariable logistic regression analysis. This included radiological
and clinical infarct. Out of 27 patients who had poor outcome 12 patients
had intra operative rupture and 18 had temporary clipping.

Results
56
None of the factors affected improvement in terms of rankin score at
follow up of 3 months.
None of the factors predicted poor outcome as per the GCS at discharge
or follow up
Table 7 : Relationship of intra operative rupture(IOR) Vs mRS at
discharge
IOR Total
Absent Present
mRS at discharge Excellent 40 8 48
Mild 19 4 23
Poor 17 12 29
Total 76 24 100
Table 8: Relationship of temporary clip vs mRS at discharge
Temp clip
Total Present Absent
mRS at discharge Excell
ent 37 11 48
Mild 14 9 23
Poor 11 18 29
Total 62 38 100

Results
57
THIRD NERVE DEFICIT:
Factor affecting the recovery of third nerve deficit:
In 16 patients who had third nerve deficit after surgery the dome
was attached to the nerve in 10 patients, 10/16 (62.5 %) as against 10/66 (
37.5 %) in those who didn't have deficit(Table 9). This was statistically
significant (p < 0.05). The average size of aneurysm for third nerve
deficit and without deficit are 6.2mm and 4.3mm respectively. This was
not statistically significant.
Temporary clipping was also significant predictor of long term
third nerve deficit at 3 months. (p < 0.05) 68.5% of patients who had third
nerve palsy with associated SAH recovered after surgery. But only 37.5
% of patients who had third nerve palsy as the presenting symptom
recovered(Table 10).

Results
58
Table 9: Relation of third nerve deficit in post operative (op) period
with attachment of dome of the aneurysm to nerve during surgery
Relation to 3rd
nerve to
dome of aneurysm
Total
Not
attached Attached
3 rd nerve
deficit post
op
No 56 10 66
Yes 6 10 16
Total 62 20 82
Table 10: Recovery of third nerve palsy and relationship to SAH
THIRD NERVE DEFICIT and RECOVERY
Before surgery After surgery 3 months
Third nerve
palsy present
27 16 11
Third nerve
palsy absent
73 84 89
100 100 100
Relation of third nerve palsy and associated SAH
Third nerve +
Unbled
Third nerve +
SAH
Total
Pre op third
nerve deficit
8 19 27
Post op third
nerve at 3
months
5 6 11
Recovery
percentage
3/8(37.5%) 13/19(68.5 % )

Results
59
Table 11: mRS at discharge and factors affecting outcome.
Excellent
functional
outcome
Mild
disability
mod to
severe
disability
Percentag
e(%)
p value
Age
< 56 years 27 12 11 50 0.289
> 56 years 21 11 18 50
Sex 0.881
Male 13 5 7 25
Female 35 18 22 75
Co morbidities
Hyppertension 21 9 12 42 0.931
Diabetes 4 3 3 11 -
Other co
morbidities
Presenting symptoms
Vomiting 19 15 6 40 0.15
Third nerve
deficit
11 10 6 27 0.53
Focal deficit 3 0 4 7 -
GCS
15 47 23 25 95
14 1 0 1 2
13 0 0 2 2
12 0 0 1 1
WFNS
2 6 5 5 16
1 35 16 19 70
Unbled 7 4 5 16

Results
60
Pre op CT characteristics
IVH 8 4 8 20 0.478
Pre op infarct 4 1 2 7
Cisternal blood 31 15 19 65 0.996
Hydrocephalus 5 2 6 13
Pre op investigations
MRA 9 9 7 25 0.177
CTA 41 22 27 90
DSA 21 6 11 38 0.357
Multiple
aneurysm
13 8 10 31 0.718
Aneurysm characters
Direction 0.484
Posteriorly
inferiorly
laterally
31 18 19 68
Other direction 17 5 10 32
Relation to
PCoA
0.864
Arising distal to
PCoA
32 14 18 64
Arising from
neck/opposite to
PCoA
16 9 11 36
Aneurysm size
< 5 mm 37 14 22 73
5 - 10 mm 11 8 4 23
> 10 mm 0 1 3 4
Operative characters
IOR 8 4 12 24 0.02
Temporary
clipping
11 9 18 38 0.003

Results
61
Wrap + clip 6 5 9 20 0.140
Attached of
aneurysm to 3 rd
nerve
8 5 9 22 0.337
Open lamina
terminalis
7 5 12 24 0.27
Fetal PCoA 1 3 6 10 -
Atherosclerosis 6 4 7 17 -
Duration of temporary clip
< 3min 39 18 13 70
3- 6 min 5 3 8 16
6- 12 min 3 2 5 10
> 12 min 1 0 3 4
Post operative factors
Tracheostomy 0 3 5 8
Infarct 0 2 20 22 0.04
Decompressive
craniotomy
0 1 5 6
Vasospasm 0 2 6 8
Hemiparesis 0 2 11 13
GCS at
discharge
-
15 48 23 15 86
13-15 0 0 1 1
<13 0 0 4 4
MRS at
discharge
48 23 29

Results
62
Mortality:
Nine patients expired out of operated 100 patients. Only 3 patients
died due to complication related to subarachnoid haemorrhage like
vasospasm. 6 patients died due to medical complication (2 patients
COPD, 1 patients due to MI and 3 patients due to pulmonary embolism).
The number was too small to derive any statistical significance or
to find any factor that predicted mortality.

Discussion
63
DISCUSSION
Incidence of PCoA: 100 cases out of 554 clipped aneurysms between
January 2013 and May 2017 were PCoA aneurysm. The incidence of
PCoA in our study was 18.05 %. The incidence of PCoA aneurysm as
quoted in the literature is 15%–25% of all intracranial aneurysms. (12,
30)
PRE OPERATIVE CHARACTERS:
Age : The average age of presentation of PCoA aneurysm in this study
was 55.2 years. The median was 56 years. In a study by Matsukawa et al
the average was less than 60 years. Several studies have shown that
incidence of SAH increased with increasing age, reaching the maximum
level at the age of 50–70 years but declined after that. (12). In an another
study the average age at presentation was 55.8 +/- 13.3 years. (61)
Sex: In our study 75 % were female and 25 % were male. The incidence
of aneurysm being higher in female is reported in literature. Park et al in
their study on 53 patients have found that the incidence is more common
in female as compared to men(15). In a study by Ghods et al on
unruptured aneurysms, the incidence among women was 54–37% and
29– 15% among men(14). Similarly in a study by Pegoli et al 64% of
their 381 patients were female. The most important mechanism quoted in

Discussion
64
literature for increased incidence in female is due to altered hemodynamic
stress and vascular remodelling secondary to decreased oestrogen level.
In our study difference in sex didn't affect the outcome parameters (61).
Risk factors and comorbidities:
Hypertension and smoking: Hypertension has been considered as
an independent risk factor for aneurysmal formation. Our results co relate
with previous studies with 42% of patients having hypertension. In a
study by Taylor et al the prevalence of hypertension in patients with
unruptured aneurysms was 43.2% compared with 34.4% in the random
sample.(63) In a meta analysis by Backes et al hypertension was
significant factor in 11 studies and had 1.24 (0.98–1.58) risk ratio of
aneurysmal formation and rupture as compared to the control group. (64)
32 % of patients in our study had history of smoking. In a study
smoking had risk ratio of 2.03 (1.52–2.71) over the control group.(64)
The mechanism cited for both hypertension and smoking as a risk
factor for aneurysm formation and rupture ,is the endothelial damage
leading to repair and regeneration process ultimately leading to aneurysm
formation and rupture.(16, 63, 64)

Discussion
65
Other comorbidities and risk factors like diabetes, asthma,
dyslipidemia, hypothyroidism, alcohol consumption, did not significantly
affect the outcome in our study.
Symptom at presentation: Ninty percent of patients had headache at
presentation. Vomiting and third nerve palsy were also common
presenting symptoms. 16 % of the patients were unbled aneurysm.
Presentation as 3rd
nerve palsy:
In our study 27 % had third nerve palsy at presentation and
19/27(71.8 %) of those patients had associated SAH. The incidence of
oculomotor nerve palsy in patients with posterior communicating
aneurysm has been reported to vary from 9% to 50% (26, 62, 65). In
study by Chang et al among a total of 99 patients with 103 aneurysms, 13
(13.1%) patients had oculomotor palsy.(26)
The mechanisms by which PCoA aneurysm causes oculomotor
nerve palsy are through direct compression by the enlarging aneurysm or
through pulsation of the aneurysm(26). In unbled aneurysm the palsy is
usually secondary to some conformational change in dome of the
aneurysm and often indicates an impending rupture.(5, 65)

Discussion
66
RADIOLOGICAL FINDINGS AND PARAMETERS AFFECTING
OUTCOME:
CT angiogram was done in 90 % of patients, MRA in 25 % and
angiogram was done in 38 % of patients. Modified Fischer grading was
used to assess the severity of SAH. Even though 46% were among grade
III and grade IV group, this didn't affect the outcome or the occurrence of
vasospasm.
Pre operative imaging features like hydrocephalus, IVH, infarct,
hematoma didn't affect the outcome in terms of mRS or recovery from
third nerve deficit.
Aneurysm characters :
Projection: Most of the aneurysm were directed posteriorly,
inferiorly and laterally(51 %). Sola T et al studied the projection of
aneurysm with outcome. In their study inferolateral was the most
common projection. (51)
The incidence of intra operative rupture (IOR) is co related with
direction of aneurysm. In our study the incidence of intra operative
rupture was higher for aneurysm that were not directed posteriorly,
inferiorly and laterally. (62.5 % vs 20.2 %) In a study by Fukuda et al
pure posteriorly directed aneurysm had higher chance of rupture , need of

Discussion
67
complex clipping like use of fenestrated clip, risk of injury to perforators
as compared to laterally directed aneurysm. (49). Also superolateral
projecting aneurysm are reported to have worse prognosis. (51)
Table 12: Direction of aneurysm with intra operative rupture.
Direction Number IOR Percentage
Posterior inferior lateral 84 17 20.2
Other direction 16 7 62.5
Size: Most of the aneurysm were less than 10 mm . (90%) Average neck
size was 2.52 mm and average dome height was 5.2 mm and dome width
3.6 mm.In a study on PCoA aneurysm 90 % were < 10mm, 40 % < 5mm
in diameter. (66). Forget et al showed that the prevalence of small
ruptured PCoA aneurysms is high, with 87.5% of aneurysms measuring
less than 10 mm in diameter and 40% measuring less than 5 mm in
diameter having ruptured. (7, 12, 66).Similarly in our study aneurysm <
5mm were 47 % and had ruptured. This contradicts the ISUIA trial
stating that aneurysm < 7mm of anterior circulation have less chance of
rupture. PCoA Aneurysm have rupture risk equal to that of posterior
circulation aneurysm.(5)
Bleb and large aneurysm: The percentage of aneurysm with bleb in
our study was 3%. Tsukahara et al.reported a global rupture rate of 3.42%

Discussion
68
per year and a rupture rate of 28.3% per year in aneurysms that contained
bleb formation. (67) The poor outcome on large sized aneurysm is
reported. In a study by Thiarawat et al large aneurysm (15 - 25 mm)
required longer time of surgery, higher incidence of intra operative
rupture and longer temporary clipping. (47)10 % of our study had
aneurysm had size > 10 mm.
INTRA OPERATIVE CHARACTERS :
Adequate drainage of CSF, minimal brain retraction, and
identification of all perforators are the important steps in clipping of
PCoA aneurysm. (47) Selecting the proper clip, use of temporary clipping
when needed with achieving proximal and distal control is of utmost
importance. (47)
Intra Operative Rupture: Intraoperative rupture occurred in 24% of the
patients and 50 % of them had moderate to severe disability at discharge.
There are multiple factors which can affect intra operative rupture. As
said earlier postero medially directed aneurysm have high chance of
rupture. Similarly aneurysm attached to temporal lobe or uncus have high
chance of rupture. The retraction of temporal lobe should be avoided
because dome of the aneurysm might be attached to the medial wall of
temp lobe. This can lead to premature rupture of aneurysm. (47) Patients

Discussion
69
who had intra operative rupture had higher chance of poor functional
outcome at discharge but this was nullified at follow up of 3 months.
Leipzig et al, reviewed a large series of aneurysm clipping looking
for risk factors of intra-operative rupture. PCoA aneurysms had the
second highest rate of intra-operative rupture amongst anterior circulation
aneurysms (9.3%). (68) Risk factors for intra-operative rupture included
an immediate history of subarachnoid hemorrhage as well as temporary
clipping.(5, 68)
Wrapping: Wrapping and clipping is a technique applied to
ruptured aneurysms where the lesion is wrapped with autogenous tissue
or absorbable material to reconstruct the integrity of the vessel and then
clip is placed over it.(58) This is helpful when there is avulsion at neck of
aneurysm.
Barrow and Spetzler reported a cotton-clipping technique using
cotton as bolster and clip together with an aneurysm. (69) The use of
muscle as a replacement for cotton has been reported in very few studies.
We used muscle as a replacement for cotton. The pieces of muscle are
used to cover the perforate site of the neck, and they are held in place
with a suction tip. Then, muscle is clipped onto the torn neck together
with the aneurysm neck(47)

Discussion
70
The rationale for using muscle is that the foreign body reaction is
less but it still can form a good coagulum. Skeletal muscle is very
vascularised. The arterioles and capillaries that are present in muscle are
known for releasing several procoagulative factors after a piece of muscle
is harvested (70, 71) This is much more aggravated when it is smashed or
crushed. Pro coagulant factors along with platelets, amplify, and
propagate the natural hemostasis process at the point of injury.This,
combined with a mechanical tamponade resulting from the muscle piece
results in a strong hemostatic plug. Sometimes just placing the piece of
muscle against the bleeding point for 2 minutes may be sufficient to stop
the bleeding(71, 72) This can be used when the neck of aneurysm gets
avulsed.
Relation to 3rd
nerve: The infratentorial with laterally projecting
aneurysms have a higher tendency to present with preoperative
oculomotor palsy. In 20 patients aneurysm was attached to third nerve.
The recovery of third nerve deficit in patients who present with SAH with
oculomotor nerve palsy was better than patients who presented with third
nerve deficit without SAH. The identification of the oculomotor nerve
before clip application should be avoided because of the increased risk of
premature aneurysm rupture.(22, 47)

Discussion
71
Lamina terminalis opening: Lamina terminals was opened in 24 %
of cases. This is achieved after identification of optic nerve and chiasm.
With release of CSF the dissection of sylvan fissure becomes more easier
with less need for retraction. (47)In almost all patients with pre operative
hydrocephalus and intraventricluar blood lamina terminals was opened.
This has lead to decreased incidence of shunt in post operative period.
Temporary Clipping: Temporary clipping is done on proximal
ICA. The average time for temporary clipping in our study was 2.4
minutes. Studies have shown that temporary clipping upto 12 minutes is
safe and temporary clipping with intermittent release can safely be done
as long as 27 minutes (47) In our study the use of temporary clipping has
affected functional outcome at discharge but there was no difference in
outcome at follow up of 3 months.

Discussion
72
POST OPERATIVE COMPLICATIONS:
Hydrocephalus:
In our study thirteen patients had pre op hydrocephalus and only
one patient required VP shunt.
Clipping patients have less incidence of long term hydrocephalus
as compared to coiling patients. Literature also supports this fact. Varelas
et al in their study on 108 patients found that hydrocephalus was present
in 30% of the patients with aneurysmal SAH and shunt dependent
hydrocephalus was more in patients who underwent coiling.(54). In a
study by Woernele et al the shunt dependency for aneurysmal SAH was
26.5 %. GCS 3- 7 at admission and coiling were predictors for shunt
dependency. (56)
The very low incidence of requirement of VP shunt in our study
can be explained by the aggressive opening of lamina terminals in cases
of hydrocephalus. In our study lamina terminals was opened for all
patients who had pre operative hydrocephalus or IVH on pre op scan.
This lead to effective drainage of CSF and there by reducing the
incidence of requirement of shunt.

Discussion
73
Infarct:
The incidence of pre op infarct was 7 %. The incidence of post op
infarct in our study was 22%. This included the radiological presence of
infarct. The average incidence of infarct in various studies is around 39%.
In a study done by Umbredkar et al the quoted incidence of infarct
was24.5% for Fischer grade 1 patients and 33% for Fischer grade II
patients. The incidence of infarct co relate with grade of SAH at
presentation. (57). In our study all good grade SAH were included hence
poor grade patients affecting infarct was not studied. The average
duration of temporary clipping was 5.72 minutes for patients who
developed infarct as compared to 1.48 minutes for those patients who
didn't had infarct.This was statistically significant. Patients with infarct
had prolonged hospital stay and poor recovery. Also the incidence of
mortality is high among the group who develop late infarct.(73, 74).
Decompressive craniectomy : In our study 6 patients required
decompressive craniectomy secondary to vasospasm induced infarct. In a
study by Schirmer et al decompressive craniotomy was performed in 16
patients with poor grade SAH. They found that 64 % had good outcome
in terms of mRS score and early craniectomy ( < 48 hrs) is associated
with good outcome. In our study the number was too small for any
statistical conclusion. (75)

Discussion
74
Vasospasm: The incidence of vasospasm reported in literature is 15 to 35
%. (76, 77). In our series only 8 % developed vasospasm.Symptomatic
vasospasm patients were treated with chemical angioplasty. The number
was small to derive any statistical significance.
Seventeen patients had developed hemiparesis which improved
gradually. Hyponatremia (5%), pulmonary embolism(6%), DVT (1%)
were other complications.
OUTCOME:
In our study the functional outcome was measured in terms of
excellent outcome (mRS score 0 and 1), mild disability (mRS score of 2)
and poor functional outcome (mRS > 3)
At discharge 48 % had excellent outcome, 23% had mild disability,
29 % had moderately to severe disability which includes 9% mortality.
Follow up at 3 months patients had significant recovery with 80 %
showing excellent functional outcome with 5 % having mild disability
and 6 % severe disability. The presence of third nerve palsy was included
in mild disability.
In the multicenter International Study of Aneurysm Treatment
(ISAT), 49% of patients has an mRS score of 0–1 at 1 year (21% with
mRS score of 0 and 28% with mRS score of 1)(43)

Discussion
75
Pegoli et al in their study on 373 patients of clipped aneurysm
considered mRS 0 and 1 as excellent functional outcome. Excellent
outcome was noted in 236 patients (63.3%), including an mRS score of 0
in 122 (32.7%) and an mRS score of 1 in 114 (30.6%). The factors that
predicted good functional outcome in their study was good grade at
presentation, no intraparenchymal hematoma, no infarct, not recieving
blood transfusion. (61)
In a study by Lee K chang et al on 424 operated cases of PCoA
aneurysm , the incidence of poor outcome at follow up was 7.3%. (3)
In the meta-analysis by Nieuwkamp et al55% of patients remained
independent and 19% were dependent on help for activities of daily living
1-12 months after the onset. (60)
Hop et al analysed disabilities 1-48 months after the onset and
found that on average, 10-20% of survivors of aneurysmal SAH become
so disabled that they lose their independence and have to rely on others to
carry on in their daily lives (59)
Our series shows the functional outcome of operated cases of
PCoA aneurysm is better than what quoted in literature. The factors that
predicted moderate to severe disability at discharge were intra operative
rupture, temporary clipping and post operative infarct. The presence of
post operative infarct predicted poor outcome at discharge after multi

Discussion
76
variable logistic regression analysis. None of the factors determined poor
outcome at follow up of 3 months.
Sanai et al in their study on technical difficulties in clipping of
PCoA aneurysm have found that temporary clipping and use of
fenestrated clip is associated with poor outcome indicating the
complexity of aneurysm. (78)
Recovery of 3rd
nerve deficit
In our study 27 patients had third nerve palsy at presentation and
20 patients had associated SAH. After surgery 11 patients recovered.
(40.7%) 16 patients had either partial or complete third nerve deficit.
Full recovery of third nerve palsy has been reported to range
between 32% and 85% after treatment.(24, 79)Several studies have been
conducted to predict the recovery of occulomotor nerve palsy. In a study
by Guresier et al after multivariate analysis they found that patients with
incomplete third nerve palsy at admission were more likely to attain full
recovery from the palsy than were those with complete third nerve palsy
at admission(79)
In our study the usage of temporary clipping more than 7 minutes
affected the outcome in terms of post operative third nerve palsy at
discharge and at 3 months. The recovery of third nerve palsy was
significantly better for those patients who had presented with SAH. This

Discussion
77
can be attributed to the fact that along with clipping the decompression of
hematoma or blood surrounding the nerve might have benefited in
recovery. In other studies other factors like symptom to surgery,
aneurysm size has found to affect the third nerve palsy recovery but these
were not significant in our study.(27, 80)
Teasdale et al. in their series of 27 patients with unruptured PCoA
aneurysms found that aneurysm measuring 7mm or greater had higher
incidence of third nerve deficit. (81)In our study the average size of
aneurysm for third nerve deficit and without deficit are 6.2mm and
4.3mm respectively showing that the size of aneurysm was larger in
patients who presented with third nerve palsy. But this was not
statistically significant.
Time duration from presentation to clipping determines the
outcome. The average duration from symptom to surgery for those who
had permanent deficit was 60.5 days as against 23.5 days for those who
improved. The number was small to derive statistical significance.
Botterell et al, and Grayson et al, found that presence of oculomotor
nerve palsy greater than 10 days prior to operative intervention was
associated with a reduced likelihood of a full recovery.(82, 83). In an
another study by Chang et al the time to surgery and the severity at
presentation were the predictors of recovery.(26) The mechanism

Discussion
78
underlying non improvement for patients presenting late are long-term
nerve compression leading to neuronal injury and neural degeneration..
Kyriakides et al reported that most of the patients operated on in the first
week had a complete recovery and they also found a statistical correlation
between incomplete palsies and good postoperative recovery. (84)
Mortality:
Nine patients expired out of operated 100 patients. Only 3 patients
died due to complication related to sub arachnoid haemorrhage like
vasospasm. 6 patients died due to medical complication( 2 patients
COPD, 1 patients due to MI and 3 patients due to pulmonary
embolism).The reported rates of mortality in literature is 7 - 45 %. Case
fatality rates have decreased by 17% during the last three decades.(61).
Various factors predicting the mortality have been studied in literature.
like female sex, severity of clinical presentation, re bleeding, older age,
preexisting severe medical illness, cerebral edema on computed
tomography (CT) scan, intraventricular and intracerebral hemorrhage,
symptomatic vasospasm, delayed cerebral infarction (especially if is
multiple), hyperglycemia, fever, anemia, and other systemic
complications such as pneumonia and sepsis (16, 85) In our study the
number was too small to derive any statistical significance or to find any
factor that predicting mortality.

Conclusion
79
CONCLUSION
The following conclusions can be made from our study on PCoA
aneurysm
• The presence of post operative infarct predicted poor outcome in terms
of modified rankin score at discharge. (mRS ≥ 3). But no factors
predicted poor outcome at 3 month follow up.
• The incidence of intra operative rupture was more in aneurysms that
were not directed posteriorly, laterally and inferiorly.
• The wrap clip technique using autologous muscle was an effective way
of securing the neck of aneurysm.
• Opening of lamina terminals significantly reduced the need for post
operative CSF diversion in patients who had hydrocephalus at
presentation.
• The recovery of third nerve palsy was better if the patient had an
associated SAH as compared to the patients who had only third nerve
palsy as presentation. The use of temporary clipping > 7 minutes was
associated with long term third nerve deficit.
Successful surgical management of PCoA aneurysm depends on
precise understanding of their unique microsurgical anatomy, avoidance
of pitfalls and the surgeon’s experience.

Limitation of the study
80
LIMITATION OF THE STUDY
A deficiency of our analysis is that it was a retrospective study. All
data was collected retrospectively from database including the imaging
data, operative records and follow up details. Even though the database
was well maintained there were some missing details in records. mRS
was used as a functional outcome measurement but still some patients
might have cognition impairment which required neuropshychometric
testing. However mRS score of o and 1 indicate excellent functional
outcome with almost near to normal life activities. Also most of the
patients who were doing well despite third nerve palsy were grouped
under mild disability according to modified rankin scale (mRS). This
affected the mRS scores at discharge and follow up.The factors predicting
mortality was not done due to low number of patients who expired after
surgery. Further prospective studies can overcome these drawbacks faced
in this study.

Bibliography
81
BIBLIOGRAPHY
1. Gibo H, Lenkey C, Rhoton Jr AL. Microsurgical anatomy of the
supraclinoid portion of the internal carotid artery. Journal of
neurosurgery. 1981;55:560-74.
2. Pedroza A DM, Artero JC, Umansky F, Berman SK, Diaz FG,
Ausman JI, Mirchandani HG. Microanatomy of the posterior
communicating artery; Neurosurgery. 1987;20:228–35.
3. Lee KC, Lee KS, Shin YS, Lee JW, Chung SK. Surgery for
posterior communicating artery aneurysms. Surgical Neurology.
2003;59:107-13.
4. Yasargil MG. Microneurosurgery, vol. II. New York: Thieme;
1984. p. 71 - 98.
5. Golshani K, Ferrell A, Zomorodi A, Smith TP, Britz GW. A review
of the management of posterior communicating artery aneurysms in
the modern era. Surgical neurology international. 2010;1
6. Sforza DM, Putman CM, Cebral JR. Hemodynamics of cerebral
aneurysms. Annual review of fluid mechanics. 2009;41:91-107.

Bibliography
82
7. Cebral JR, Raschi M. Suggested Connections Between Risk Factors
of Intracranial Aneurysms: A Review. Annals of Biomedical
Engineering. 2013;41:1366-83.
8. William E. Stehbens. Etiology of intracranial berry aneurysms.
Journal of Neurosurgery.1989;70:823-31.
9. Kataoka K TM, Asai T, Kinoshita A, Ito M, Kuroda R. Structural
Fragility and Inflammatory Response of Ruptured Cerebral
Aneurysms. A Comparative Study between Ruptured and
Unruptured Cerebral Aneurysms. Stroke. 1999; 30:1396–1401.
10. Stehbens WE. Familial Intracranial Aneurysms: An Autopsy Study.
Neurosurgery.1998;43:1258-9.
11. Seshaiyer P, Humphrey JD. On the potentially protective role of
contact constraints on saccular aneurysms. Journal of
Biomechanics.2001;34:607-12.
12. Lv N, Wang C, Karmonik C, Fang Y, Xu J, Yu Y, Cao W, Liu J,
Huang Q. Morphological and Hemodynamic Discriminators for
Rupture Status in Posterior Communicating Artery Aneurysms.
PloS one. 2016 ;11:e0149906.

Bibliography
83
13. Inagawa T IS, Aoki H, Takahashi M, Yoshimoto H: Aneurysmal
subarachnoid hemorrhage in Izumo City and Shimane Prefecture of
Japan. Incidence. Stroke.1988; 19:170–175.
14. Ghods AJ, Lopes D, Chen M. Gender differences in cerebral
aneurysm location. Frontiers in neurology. 2012;3.
15. Park SK, Shin YS, Lim YC, Chung J. Preoperative predictive value
of the necessity for anterior clinoidectomy in posterior
communicating artery aneurysm clipping. Neurosurgery.
2009;65:281-5.
16. Rivero Rodríguez D, Scherle Matamoros C, Cúe LF, Miranda
Hernández JL, Pernas Sánchez Y, Pérez Nellar J. Predictor’s of
Mortality in Patients with Aneurysmal Subarachnoid Haemorrhage
and Reebleding. Neurology research international. 2015;2015.
17. Shi C, Awad IA, Jafari N, Lin S, Du P, Hage ZA, Shenkar R, Getch
CC, Bredel M, Batjer HH, Bendok BR. Genomics of human
intracranial aneurysm wall. Stroke. 2009;40:1252-61.
18. Krischek B, Tatagiba M. The influence of genetics on intracranial
aneurysm formation and rupture: current knowledge and its possible
impact on future treatment. InAdvances and technical standards in
neurosurgery 2008;131-147.

Bibliography
84
19. Ghani AA, Nayan SA, Kandasamy RE, Rosman AK, Ghani AR.
Characteristics and outcomes of patients with anterior circulation
intracranial aneurysm managed with clipping in Hospital Sungai
Buloh. The Malaysian journal of medical sciences. 2016;23:113
20. F. Schlenk AN, D. Graetz, and A. S. Sarrafzadeh, Hyperglycemia
and cerebral glucose in aneurysmal subarachnoid hemorrhage,
Intensive Care Medicine, 2008; 34:1200– 07.
21. Kurtz P, Claassen J, Helbok R, Schmidt JM, Fernandez L, Presciutti
M, Stuart RM, Connolly ES, Lee K, Badjatia N, Mayer SA.
Systemic glucose variability predicts cerebral metabolic distress and
mortality after subarachnoid hemorrhage: a retrospective
observational study. Critical Care. 2014;18:R89.
22. Gelabert-Gonzalez M I-PM, Fernandez-Villa J. Acute subdural
haematoma due to ruptured intracranial aneurysms. Neurosurgery
Review. 2004;27:259–62.
23. Rhoton Jr AL. The supratentorial arteries. Neurosurgery.
2002;51:S1-53.
24. Gaberel T, Borha A, di Palma C, Emery E. Clipping Versus Coiling
in the Management of Posterior Communicating Artery Aneurysms

Bibliography
85
with Third Nerve Palsy: A Systematic Review and Meta-Analysis.
World Neurosurgery. 2016;87:498-506.
25. Schmidek HH. Surgical management of posterior communicating
artery, and carotid bifurcation aneurysms. In: HH Schmidek, ed.
Schmidek & Sweet Operative Neurosurgical Techniques:
Indications, Methods, and Results. Vol 1. Philadelphia: WB
Saunders, 2000:1129 –34.
26. Anevrizma OS. Posterior communicating aneurysm with
oculomotor nerve palsy: clinical outcome after aneurysm clipping.
Turkish neurosurgery. 2014;24:170-3.
27. Anan M, Nagai Y, Fudaba H, Kubo T, Ishii K, Murata K, Hisamitsu
Y, Kawano Y, Hori Y, Nagatomi H, Abe T. Third nerve palsy
caused by compression of the posterior communicating artery
aneurysm does not depend on the size of the aneurysm, but on the
distance between the ICA and the anterior–posterior clinoid process.
Clinical neurology and neurosurgery. 2014;123:169-73.
28. Kurokawa Y, Ishizaki E, Inaba KI. Incomplete oculomotor nerve
palsy caused by an unruptured internal carotid-anterior choroidal
artery aneurysm. Neurologia medico-chirurgica. 2005;45:143-7.

Bibliography
86
29. Yanaka K MY, Mashiko R, Hyodo A, Sugimoto K, Nose T. Small
unruptured cerebral aneurysms presenting with oculomotor nerve
palsy. Neurosurgery 2003;52:553–7.
30. Lv N, Wang C, Karmonik C, Fang Y, Xu J, Yu Y, Cao W, Liu J,
Huang Q. Morphological and Hemodynamic Discriminators for
Rupture Status in Posterior Communicating Artery Aneurysms.
PloS one. 2016;11:e0149906.
31. Kuzmik GA, Bulsara KR. Microsurgical clipping of true posterior
communicating artery aneurysms. Acta neurochirurgica.
2012;154:1707-10.
32. He W GC, Quinn J, Karimi R, Prestigiacomo CJ .True aneurysms of
the posterior communicating artery: a systematic review and meta-
analysis of individual patient data. World Neurosurgery.
2011;75:64–72.
33. Yoon NK, McNally S, Taussky P, Park MS. Imaging of cerebral
aneurysms: a clinical perspective. Neurovascular Imaging.
2016;2:6.
34. Perry JJ SI, Sivilotti ML, Bullard MJ, Emond M, Symington C, et
al. Sensitivity of computed tomography performed within six
hours of onset of headache for diagnosis of subarachnoid

Bibliography
87
haemorrhage: prospective cohort study. British medical journal.
2011;343:d4277.
35. Davis JM, Davis KR, Crowell RM. Subarachnoid hemorrhage
secondary to ruptured intracranial aneurysm: prognostic
significance of cranial CT. American Journal of Roentgenology.
1980;134:711-5.
36. Klimo P, Jr., Schmidt RH. Computed tomography grading schemes
used to predict cerebral vasospasm after aneurysmal subarachnoid
hemorrhage: a historical review. Neurosurgical focus. 2006;21:E5.
37. Friedman JA, Goerss SJ, Meyer FB, Piepgras DG, Pichelmann MA,
McIver JI, Toussaint III LG, McClelland RL, Nichols DA, Atkinson
JL, Wijdicks EF. Volumetric quantification of Fisher Grade 3
aneurysmal subarachnoid hemorrhage: a novel approach to predict
symptomatic vasospasm on admission computerized tomography
scans. Journal of neurosurgery. 2002;97:401-7.
38. Hijdra A BP, Vermeulen M, van Gijn J Grading the amount of
blood on computed tomograms after subarachnoid hemorrhage.
Stroke;1990 21:1156–61.
39. Claassen J BG, Kreiter K, Bates J, Du YE, Cope- land D, et al:
Effect of cisternal and ventricular blood on risk of delayed cerebral

Bibliography
88
ischemia after subarachnoid hemorrhage. The Fisher Scale revisited.
Stroke. 2001;32:2012–20.
40. Guo W, He XY, Li XF, Qian DX, Yan JQ, Bu DL, Duan CZ. Meta-
analysis of diagnostic significance of sixty-four-row multi-section
computed tomography angiography and three-dimensional digital
subtraction angiography in patients with cerebral artery aneurysm.
Journal of the neurological sciences. 2014 15;346:197-203.
41. Da Rocha AJ, da Silva CJ, Gama HP, Baccin CE, Braga FT, de
Araújo Cesare F, Veiga JC. Comparison of magnetic resonance
imaging sequences with computed tomography to detect low-grade
subarachnoid hemorrhage: role of fluid-attenuated inversion
recovery sequence. Journal of computer assisted tomography. 2006
1;30:295-303.
42. Ochiai C, Wakai S, Inou S, Nagai M. Preoperative angiographical
prediction of the necessity to removal of the anterior clinoid process
in internal carotid-posterior communicating artery aneurysm
surgery. Acta neurochirurgica. 1989;99:117-21.
43. Molyneux A, International Subarachnoid Aneurysm Trial (ISAT)
Collaborative Group. International Subarachnoid Aneurysm Trial
(ISAT) of neurosurgical clipping versus endovascular coiling in

Bibliography
89
2143 patients with ruptured intracranial aneurysms: a randomised
trial. The Lancet. 2002;360:1267-74.
44. Li ZQ, Wang QH, Chen G, Quan Z. Outcomes of endovascular
coiling versus surgical clipping in the treatment of ruptured
intracranial aneurysms. Journal of International Medical Research.
2012;40:2145-51
45. McDougall CG SR, Zabramski JM, Partovi S, Hills NK, Nakaji P,
Albuquerque FC. The Barrow Ruptured Aneurysm Trial. Journal of
Neurosurgery. 2012; 116:135–44.
46. Lanzino G, Murad MH, d'Urso PI, Rabinstein AA. Coil
embolization versus clipping for ruptured intracranial aneurysms: a
meta-analysis of prospective controlled published studies. American
Journal of Neuroradiology. 2013;34:1764-8.
47. Thiarawat P, Jahromi BR, Kozyrev DA, Intarakhao P, Teo MK,
Choque-Velasquez J, et al. Microneurosurgical Management
of Posterior Communicating Artery Aneurysm: A Contemporary
Series from Helsinki. World Neurosurgery. 2017;101:379-88.
48. Kraus RR KJ, Borlotti C, Lanzino G. Oculomotor palsy from an
unruptured posterior communicating artery aneurysm presenting

Bibliography
90
with cerebrospinal fluid pleocytosis and enhancement of the third
cranial nerve. Case report. J Neurosurgery. 2004;101:352-353.
49. Fukuda H, Hayashi K, Yoshino K, Koyama T, Lo B, Kurosaki Y,
Yamagata S. Impact of aneurysm projection on intraoperative
complications during surgical clipping of ruptured posterior
communicating artery aneurysms. Neurosurgery. 2015;78:381-90.
50. Yoshimoto Y WS, Satoh A, Hirose Y. Intraparenchymal and
intrasylvian haematomas secondary to ruptured middle cerebral
artery aneurysms: prognostic factors and therapeutic considerations.
British Journal of Neurosurgery. 1999;13:18-24.
51. Sola T BE, Vivas E, Cuellar H, Nasis N, Guimaraens L. Clinical
and Radiological Features of Posterior Communicating Artery
Aneurysms. Interventional Neuroradiology. 2008;14:247-251.
52. Lennihan L, Mayer SA, Fink ME, Beckford A, Paik MC, Zhang H,
Wu YC, Klebanoff LM, Raps EC, Solomon RA. Effect of
hypervolemic therapy on cerebral blood flow after subarachnoid
hemorrhage. Stroke. 2000 ;31:383-91.
53. Lee Y, Zuckerman SL, Mocco J. Current controversies in the
prediction, diagnosis, and management of cerebral vasospasm:
where do we stand?. Neurology research international. 2013;2013.

Bibliography
91
54. Varelas P HA, Sinson G, Spanaki M, Hacein Bey L. Clipping or
coiling of ruptured cerebral aneurysms and shunt-dependent
hydrocephalus. Neurocritical care. 2006 ;4:223-8.
55. Sethi H, Moore A, Dervin J, Clifton A, MacSweeney JE.
Hydrocephalus: comparison of clipping and embolization in
aneuryson treatment. Journal of neurosurgery. 2000 ;92:991-4
56. Woernle CM WK, Burkhardt JK, Haile SR, Bellut D, Neidert MC,
Bozinov O, Krayenbühl N, Bernays RL. Hydrocephalus in 389
patients with aneurysm-associated subarachnoid hemorrhage.
Journal of clinical neuroscience. 2013 ;20:824-6.
57. Umredkar A, Gupta SK, Khandelwal N, Chhabra R, Mathuriya SN,
Pathak A, Tiwari MK, Mukherjee KK, Mohindra S, Singla N,
Salunke P. Intracerebral infarcts following clipping of intracranial
aneurysms: incidence, clinical correlation and outcome. British
journal of neurosurgery. 2010 ;24:156-62.
58. Zhao J, Lin H, Summers R, Yang M, Cousins BG, Tsui J. Current
Treatment Strategies for Intracranial Aneurysms: An Overview.
Angiology 2017:3319717700503.

Bibliography
92
59. Hop JW RG, Algra A, Van Gijn J. Case-fatality rates and functional
outcome after subarachnoid hemorrhage: a systematic review.
Stroke. 1997;28:660-64.
60. Nieuwkamp DJ SL, Algra A, Linn FHH, de Rooij NK, Rinkel GE.
Changes in case fatality of aneurysmal subarachnoid haemorrhage
over time, according to age, sex, and region: a meta-analysis.
Lancet Neurology. 2009;8:635-42.
61. Pegoli M, Mandrekar J, Rabinstein AA, Lanzino G. Predictors of
excellent functional outcome in aneurysmal subarachnoid
hemorrhage. Journal of Neurosurgery. 2015;122:414-8.
62. Chen PR, Amin-Hanjani S, Albuquerque FC, McDougall C,
Zabramski JM, Spetzler RF. Outcome of oculomotor nerve palsy
from posterior communicating artery aneurysms: comparison of
clipping and coiling. Neurosurgery. 2006;58:1040-6.
63. Taylor CL YZ, Selman WR, Ratcheson RA, Rimm AA. Cerebral
arterial aneurysm formation and rupture in 20,767 elderly patients:
hypertension and other risk factors. Journal of neurosurgery.
1995;83:812-9.
64. Backes D, Rinkel GJ, Laban KG, Algra A, Vergouwen MD.
Patient- and Aneurysm-Specific Risk Factors for Intracranial

Bibliography
93
Aneurysm Growth: A Systematic Review and Meta-Analysis.
Stroke. 2016;47:951-7.
65. Yang MQ, Wang S, Zhao YL, Zhang D, Zhao JZ. Postoperative
recovery from posterior communicating aneurysm complicated by
oculomotor palsy. Chinese Medical Journal 2008;121:1065.
66. Forget TR Jr, Benitez R, Veznedaroglu E, et al. A review of size
and location of ruptured intracranial aneurysms. Neurosurgery
2011;49:1322-1326.
67. Tsukahara T MN, Sakurai Y, Yonekura M, Takahashi T, Inoue T, et
al: Treatment of unruptured cerebral aneurysms; a multi-center
study at Japanese national hospitals. Acta Neurochirurgia
Supplement 2005;94:77–85.
68. Leipzig TJ MJ, Horner TG, Payner T, Redelman K, Johnson CS.
Analysis of intraoperative rupture in the surgical treatment of 1694
saccular aneurysms. Neurosurgery. 2005;56:455
69. Barrow DL, Spetzler RF. Cotton-clipping technique to repair
intraoperative aneurysm neck tear: a technical note. Neurosurgery.
2011;68:294-99;

Bibliography
94
70. Taubman MB WL, Miller C. The role of smooth muscle derived
tissue factor in mediating thrombosis and arterial injury.
Thrombosis Research. 2008;122:S78–S81.
71. Menovsky T, de Vries J, Grotenhuis JA. Cotton-clipping technique:
piece of smashed muscle as an alternative. Neurosurgery.
2011;69:E1183-85
72. Kretz CA, Vaezzadeh N, Gross PL. Tissue factor and thrombosis
models. Arteriosclerosis, thrombosis, and vascular biology.
2010;30:900-8.
73. Adams HP Jr KN, Torner JC, Haley EC Jr. Predicting cerebral
ischemia after aneurysmal subarachnoid hemorrhage:
Influences of clinical condition, CT results, and antifibrinolytic
therapy. A report of the Cooperative Aneurysm Study. Neurology
1987;37:1586–91.
74. Rabinstein AA FJ, Weigand SD, McClelland RL,, Fulgham JR ME,
Atkinson JL, Wijdicks EF. Predictors of cerebral infarction in
aneurysmal subarachnoid hemorrhage. Stroke 2004;35:1862–66.
75. Schirmer CM, Hoit DA, Malek AM. Decompressive
hemicraniectomy for the treatment of intractable intracranial

Bibliography
95
hypertension after aneurysmal subarachnoid hemorrhage. Stroke.
2007;38:987-92.
76. Taha MM, Nakahara I, Higashi T, Iwamuro Y, Iwaasa M, Watanabe
Y, Tsunetoshi K, Munemitsu T. Endovascular embolization vs
surgical clipping in treatment of cerebral aneurysms: morbidity and
mortality with short-term outcome. Surgical neurology. 2006
;66:277-84
77. Murayama Y, Malisch T, Guglielmi G, Mawad ME, Viñuela F,
Duckwiler GR, Gobin YP, Klucznick RP, Martin NA, Frazee J.
Incidence of cerebral vasospasm after endovascular treatment of
acutely ruptured aneurysms: report on 69 cases. Journal of
neurosurgery. 1997 ;87:830-5.
78. Sanai N, Caldwell N, Englot DJ, Lawton MT. Advanced technical
skills are required for microsurgical clipping of posterior
communicating artery aneurysms in the endovascular era.
Neurosurgery. 2012;71:285-94.
79. Guresir E, Schuss P, Seifert V, Vatter H. Oculomotor nerve palsy
by posterior communicating artery aneurysms: influence of surgical
strategy on recovery. Journal of neurosurgery. 2012;117:904-10.

Bibliography
96
80. Guresir E, Schuss P, Setzer M, Platz J, Seifert V, Vatter H.
Posterior communicating artery aneurysm-related oculomotor nerve
palsy: influence of surgical and endovascular treatment on recovery:
single-center series and systematic review. Neurosurgery.
2011;68:1527-33.
81. Teasdale E, Statham P, Straiton J, Macpherson P. Non-invasive
radiological investigation for oculomotor palsy. Journal of
Neurology, Neurosurgery & Psychiatry. 1990;53:549-53
82. Botterell EH, Lloyd LA, Hoffman HJ. Oculomotor palsy due to
supraclinoid internal carotid artery berry aneurysm. American
journal of ophthalmology. 1962;54:609-16.
83. Grayson MC, Soni SR, Spooner VA. Analysis of the recovery of
third nerve function after direct surgical intervention for posterior
communicating aneurysms. The British journal of ophthalmology.
1974;58:118
84. Kyriakides T, Aziz TZ, Torrens MJ. Postoperative recovery of third
nerve palsy due to posterior communicating aneurysms. British
journal of neurosurgery. 1989;3:109-11
85. Lee SH, Song KJ, Shin SD, Ro YS, Kim MJ, Holmes JF. The
Relationship between Clinical Outcome in Subarachnoidal

Bibliography
97
Hemorrhage Patients with Emergency Medical Service Usage and
Interhospital Transfer. Journal of Korean medical science.
2015;30:1889-95
86. Lawton MT. Seven aneurysms. Vol. 53, Thieme. 2013. p 45-65.

Annexures
98
ANNEXURE I
PROFORMA
A. GENERAL INFORMATION
Anonymized Patient ID:
Age, sex, comorbidites:
B.CLINICAL DETAILS
Symptom:
Symtom to surgery
Neurological deficits:
GCS on admission:
WFNS grade at admission:
Radiological features: Fischer grading, presence of hydrocephalus,
infarct, intraventricular blood, hematoma
Aneurysmal factors : Shape, number of lobes, direction of fundus, size of
aneurysm and neck, relation to PCoA , fetal PCoA.
C. INTRAOPERATIVE EVENTS
Clipping or wrapping:
Intra operative rupture:
Temporary clipping
Duration of temporary clipping
Type of clip used
Number of clip
Fundus opened or not
Relation to third nerve

Annexures
99
Presence of atherosclerosis and calcification
Opening of lamina terminalis
Relation to perforator:
D. POST-OPERATIVE EVENTS
Vasospasm:
Infract Early:
Late:
Re-exploration / Decompression
Duration of the ventilator support:
Tracheostomy:
Duration of ICU stay:
Duration of post-op hospital stay:
GCS on POD 5
Need for other procedures like VP shunt
E. STATUS ON DISCHARGE
GCS
Motor and speech status
Any other deficit
Modified rankin score
F. Follow up (3 months)
GCS
Motor and speech status
Any other deficit
Modified rankin scale

Annexures
100
Glasgow coma scale: (GCS):
WFNS Grade:
Grade 1 – Glasgow Coma Score (GCS) of 15, motor deficit absent
Grade 2 – GCS of 13-14, motor deficit absent
Grade 3 – GCS of 13-14, motor deficit present
Grade 4 – GCS of 7-12, motor deficit absent or present
Grade 5 – GCS of 3-6, motor deficit absent or present
Modified Fischer grade:
Grade Description
0 No subarachnoid blood
1 Minimal / thin SAH, no IVH in both lateral ventricle
2 Minimal / thin SAH, with IVH in both lateral ventricle
3 Thick SAH and no IVH in both lateral ventricle
4 Thick SAH with IVH in both lateral ventricle

Annexures
101
MODIFIED RANKIN SCALE (mRs)
Score Description
0 No symptoms at all
1 No significant disability despite symptoms; able to carry out all usual duties
and activities
2 Slight disability; unable to carry out all previous activities, but able to look
after own affairs without assistance
3 Moderate disability; requiring some help, but able to walk without assistance
4 Moderately severe disability; unable to walk without assistance and unable to
attend to own bodily needs without assistance
5 Severe disability; bedridden, incontinent and requiring constant nursing care
and attention 6 Dead
TOTAL (0–6): _______
Reference:
1 Risselada R, Lingsma HF, Molyneux AJ, Kerr RS, Yarnold J, Sneade M,
Steyerberg EW, Sturkenboom MC. Prediction of two month modified Rankin
Scale with an ordinal prediction model in patients with aneurysmal
subarachnoid haemorrhage. BMC medical research methodology. 2010;10:86.
2.Bonita R, Beaglehole R. ―Modification of Rankin Scale: Recovery of motor
function after stroke.‖ Stroke 1988;19:1497-1500

Annexures
102
ANNEXURE II

Annexures
103

Annexures
104
ANNEXURE III
INTERNET SOURCES: ------------------------------------------------------------------------------------------- 0% - https://en.wikipedia.org/wiki/Internal_c 0% - Empty 1% - http://www.sciencedirect.com/science/art 0% - http://www.tandfonline.com/doi/full/10.3 0% - http://www.sciencedirect.com/science/art 0% - http://www.sciencedirect.com/science/art 0% - http://dspace.sctimst.ac.in/jspui/bitstr 0% - https://www.researchgate.net/publication 0% - https://www.researchgate.net/publication 0% - https://www.hindawi.com/journals/nri/201 0% - http://www.pjo.com.pk/23/3/Abid%20Naseem 0% - https://jbppni.biomedcentral.com/article 0% - https://link.springer.com/content/pdf/10 0% - https://link.springer.com/article/10.100 0% - http://thejns.org/doi/10.3171/jns.1995.8 0% - https://www.researchgate.net/publication 1% - http://www.turkishneurosurgery.org.tr/pd 1% - http://www.turkishneurosurgery.org.tr/pd 1% - http://surgicalneurologyint.com/surgical 0% - https://www.researchgate.net/publication 1% - http://surgicalneurologyint.com/surgical 0% - http://europepmc.org/articles/PMC3779399 0% - http://europepmc.org/articles/PMC2859623 0% - http://thejns.org/doi/full/10.3171/2013. 0% - https://2475432.r.bat.bing.com/?ld=d36Pt 1% - http://europepmc.org/articles/PMC3011114 1% - http://surgicalneurologyint.com/surgical 1% - http://surgicalneurologyint.com/surgical 1% - http://surgicalneurologyint.com/surgical 0% - https://www.researchgate.net/profile/Jun

Annexures
105
1% - http://www.sciencedirect.com/science/art 0% - http://www.tpub.com/corpsman/144.htm 1% - http://www.sciencedirect.com/science/art 1% - http://www.sciencedirect.com/science/art 0% - http://thejns.org/doi/10.3171/2014.10.JN 0% - http://thejns.org/doi/abs/10.3171/2014.1 0% - http://thejns.org/doi/full/10.3171/2012. 0% - http://www.sciencedirect.com/science/art 1% - http://surgicalneurologyint.com/surgical 1% - http://www.turkishneurosurgery.org.tr/pd 0% - https://www.hindawi.com/journals/nri/201 0% - https://www.researchgate.net/publication 1% - http://www.sciencedirect.com/science/art

Annexures
106
ANNEXURE IV
CODING
1. Sex; Male - 1, Female 2
2. Hypertension- Yes - 1, No - 0
3. Diabetes - Yes - 1, No - 0
4. Other comorbidity - Seizure 1, Cerebovascular accident 2, Asthma- 3,
Dyslipidemia 4, Hypothyroid 5, Alcohol 7, Smoking 8
5. Headcahe- Yes - 1, No - 0
6. Vomiting - Yes - 1, No - 0
7. 3 rd nerve palsy- Yes - 1, No - 0
8. Other symptoms - Giddiness 1, Previous hematoma/bleed/sentinel headache 2,
LOC 3, Seizure 4, Focal weakness 5
9. 3 rd nerve - Yes - 1, No - 0
10. Focal deficit - Yes - 1, No - 0
11. IVH: Yes - 1, No - 0
12. Unbled - Yes - 1, No - 0
13. Infarct- Yes - 1, No - 0
14. Cisternal blood- Yes - 1, No - 0
15. Hydrocephalus- Yes - 1, No - 0
16. Other - Hematoma , Yes - 1 , No- 0
17. Pcom aneurysm Yes - 1, No - 0
18. Other location - Prom 1 Acom 2, ICA bifn 3, Choroidal 4,Ant choroidal 5, MCA
bifurcation 6, PCA 7, ACA 8, Vertebral 9, Basilar 10, Superior hypophyseal 11,
Cavernous 12, SCA 13, Ophthalmic segment 14.
19. Multiple- Yes - 1, No - 0
20. Direction: Posterior + inf + Lat 1, Posterior + Inferior 2, Posterior + Lateral 3,
Post + superior + Lateral 4,Post + inf + medial 5, Post medial 6, Post+ superior +
Medial 7, Anterior + Inf + Lat 8.
21. Relation to Pcom: Proximal1, Neck 2, opposite 3
22. Teet, Bleed, Perforator loss, Fetal PCOM , Intra op rupture ,temp clip, wrap,
perforator loss,calcification, atherosclerosis, thrombus, open lamina terminalis—-
Yes - 1, No -0
23. Type of clip - Curved 1,Straight 2,Right angle 3,Fenestrated 4,Angled 5
24. Relation to 3 rd nerve - Attached -1, Not attached - 0
25. Other features - Clinoidectomy 1, Uncus removed 2, B/l pcom 3
26. Early and late infarct, decompressive craniectomy, vasospasm, hematoma,
hydertensive (HHH) therapy, tracheostomy - Yes - 1, No - 0
27. Neurodeficit - Hemiparesis 1 ,3rd nerve deficit 2, Aphasia 3, Vegetative state 4.
28. Severity of hemiparesis- No weakness 0, flicker 1, Movement with gravity 2,
Against gravity 3, against minimal resistance 4, against full resistance 5
29. Other complication- Hyponatremia 1 ,SDH 2 ,Pulmonary embolism 3, DVT 4, VP
shunt 5, COPD 6, Pneumothorax 7, MI 8, EDH 9, Chemical angioplasty 10, SDH
11.
30. Deficit at follow up of 3 months- Hemiparesis 1 ,3rd nerve deficit 2, Aphasia 3,
Vegetative state 4, Patients who have expired: No entry
31. Death - Yes -1 No 0
32. Cause of death- COPD 1, MI 2, Vasospasm 3, Pilmonary embolism 4

Cas
e n
um
ber
Hos
p N
um
ber
Age
Sex
Hyp
erte
nsi
on
Dia
bet
es
Oth
er c
omo
rbid
ity
oth
er C
omo
rbid
ity
Hea
dac
he
Vom
itin
g
3rd
ner
ve p
als
y
Oth
er s
ymp
tom
s
Sym
tom
to
su
rger
y
3 rd
ner
ve
Foc
al d
efic
it
GC
S
WF
NS
Mod
ifie
d F
isch
er g
rad
e
IVH
No
SA
H
Infa
rct
Cis
tern
blo
od
Hyd
roce
ph
alu
s
oth
er
CT
A
MR
A
DS
A
PC
OM
Oth
er l
oca
tio
n
Mu
ltip
le
Dir
ecti
on
Rel
atio
n T
o P
com
No
of l
obes
Sh
ape
of a
neu
rysm
Siz
e of
nec
k (
)
Dom
e h
eig
ht
Dom
e w
idth
Tee
t
Ble
ed
Per
fora
tor
loss
1 355496 53 1 0 0 1 7 1 0 0 1 11 0 0 15 0 0 0 1 0 0 0 0 1 0 0 1 2 1 1 1 0 1 0 0 0 0 0 0
2 355711 48 2 1 1 2 0 1 1 0 2 9 0 0 15 1 2 0 0 0 1 0 0 1 1 0 1 0 0 1 1 0 1 4 5.2 4 0 0 0
3 356594 60 2 0 0 0 0 1 0 0 3 4 0 0 15 1 3 0 0 0 1 0 0 1 0 0 1 6 1 3 1 0 1 0 6 3 0 0 0
4 356391 38 2 0 0 0 8 1 0 1 4 16 0 0 15 2 2 0 0 0 1 1 0 1 0 0 1 0 0 3 1 1 2 3.3 15 0 0 0 0
5 356697 58 2 1 0 0 0 1 1 0 3 4 0 0 15 1 2 0 0 0 1 0 0 0 0 1 1 0 0 2 1 2 2 4.4 6.9 4.9 0 0 0
6 357985 43 2 1 0 0 8 1 1 0 3 19 0 0 15 1 3 0 0 0 1 0 0 0 1 0 1 0 0 3 2 0 1 0 5.8 3.7 0 0 0
7 349946 50 1 1 0 0 8 0 0 0 3 730 0 0 15 0 0 0 1 0 0 0 0 1 0 1 1 6 1 3 1 0 3 3.1 2.5 3.1 0 0 0
8 358975 62 1 1 0 0 8 1 0 0 5 84 0 0 15 1 4 1 0 0 1 1 1 1 0 1 1 0 0 1 1 0 2 2.7 3.5 5 0 0 0
9 360908 60 2 0 0 0 0 1 1 0 0 8 0 0 15 1 2 0 0 0 1 0 0 1 0 0 1 0 0 1 3 0 1 5.5 5 0 0 0 0
10 361832 32 1 0 0 0 7 1 1 0 0 12 0 0 15 1 4 1 0 0 1 0 0 1 0 0 1 5 1 3 1 0 1 2 4 3.7 0 1 0
11 367077 54 2 1 0 0 8 1 1 1 0 7 1 0 15 2 2 0 0 0 0 0 0 1 0 0 1 0 0 1 1 1 1 2.7 6.6 1.7 0 0 0
12 367445 25 1 0 0 0 7 1 1 0 0 2 0 0 15 1 3 0 0 0 1 0 0 1 0 0 1 2 1 1 1 0 1 2.2 2.3 0 0 0 0
13 367443 70 2 0 0 0 7 1 1 0 3 5 0 0 15 1 3 0 0 0 1 0 0 0 1 0 1 0 0 1 3 0 1 0 12.2 9 0 0 0
14 367589 60 2 0 0 0 0 1 0 0 0 7 0 0 15 1 2 0 0 0 0 1 0 1 0 0 1 0 0 1 1 0 1 0 0 0 0 0 0
15 368006 64 1 0 0 3 8 1 0 1 4 8 1 0 15 2 2 0 0 0 0 0 0 1 0 0 1 0 0 1 1 0 1 0 0 0 0 0 0
16 210991 43 2 0 0 0 0 1 0 0 0 4 0 0 15 1 3 0 0 0 1 0 0 0 0 1 1 7 1 5 3 0 3 1.7 0 0 0 0 0
17 369390 57 2 0 0 0 7 1 1 0 0 23 0 0 15 1 3 0 0 0 1 0 0 1 0 1 1 8 1 1 1 0 3 0 0 0 0 0 0
18 369914 50 2 0 0 0 8 1 0 0 0 8 0 0 15 1 2 0 0 0 0 0 0 1 0 0 1 9 0 1 1 0 1 0 0 0 0 0 0
19 370627 65 1 0 0 0 0 1 0 1 0 8 1 0 15 0 0 0 1 0 0 0 0 1 0 1 1 0 0 1 3 0 1 0 0 0 0 0 0
20 371396 54 2 0 0 0 0 1 1 1 0 10 1 0 15 2 4 1 0 0 1 0 0 0 1 1 1 0 0 1 1 0 1 2.9 4.7 7 0 0 0
21 371474 74 2 1 1 0 8 1 0 1 3 12 1 0 15 0 0 0 1 0 0 0 0 0 1 0 1 0 0 2 1 0 1 0.3 1.1 0.7 0 0 0
22 371748 55 1 0 0 0 7 1 0 0 5 9 0 1 15 2 3 0 0 1 1 0 0 0 1 0 1 0 0 3 3 0 1 0 0 0 0 0 0
23 372614 47 2 1 0 0 8 1 1 1 3 22 1 0 15 2 3 0 0 0 1 0 0 1 1 0 1 0 0 3 1 0 1 4.5 9 6.5 0 0 0
24 372679 50 2 0 0 0 7 0 0 1 3 23 1 1 12 2 4 1 0 0 1 1 0 1 0 0 1 1 1 6 1 0 1 3.7 4.2 3.5 1 1 0
25 372891 48 2 0 0 0 7 1 1 1 0 1 1 0 15 2 4 0 0 0 1 0 1 1 1 0 1 0 0 1 2 0 1 0 0 0 0 0
26 357861 57 2 0 0 0 7 0 0 0 0 360 0 0 15 0 0 0 1 0 0 0 0 1 0 1 1 6 1 1 1 0 1 1.3 2.6 1.1 0 0 1
27 374109 65 2 0 0 0 0 1 0 1 3 10 1 0 15 2 2 0 0 0 1 0 0 1 0 0 1 0 0 6 1 0 1 2.6 5.3 4.1 0 0 0
28 374399 58 1 0 0 0 8 1 0 0 0 3 0 0 15 1 3 0 0 0 1 0 0 1 0 0 1 0 0 1 2 0 1 2 2.8 2.9 0 0 0
29 212280 52 2 0 0 0 0 1 0 0 0 3 0 0 14 2 4 1 0 0 1 1 0 1 0 0 1 8 1 1 1 0 1 0 0 0 0 1 0
30 376238 64 2 0 0 0 7 0 0 0 3 1 0 0 15 1 3 0 0 0 1 0 0 1 0 0 1 0 0 1 1 2 2 5 8 9 1 0 0
31 374509 31 1 0 0 0 0 1 0 0 1 90 0 0 15 0 0 0 1 0 0 0 0 0 0 1 1 0 0 2 1 0 1 3.6 3.9 0 0 0 0
32 377343 57 2 1 0 0 0 1 0 1 0 6 1 0 15 1 2 0 0 0 1 0 0 1 0 0 1 0 0 7 1 0 1 4.6 13.5 8.6 0 0 0
33 379741 47 2 0 0 0 8 1 0 0 0 3 0 0 15 1 4 1 0 0 1 1 0 1 0 0 1 0 0 3 1 0 1 2.3 6.3 5.1 0 0 0
1

Cas
e n
um
ber
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
Fet
al P
CO
M
IOR
Tem
p c
lip
Typ
e of
cli
p
No
of c
lip
Wra
p
Du
rati
on o
f te
mp
cli
p(M
in)
Per
fora
tor
loss
Cal
cifi
cati
on
Ath
eros
cler
osi
s
Th
rom
bu
s
Rel
atio
n t
o 3
rd
ver
ve
Op
en l
amin
a t
erm
ina
lis
Oth
er
Ear
ly i
nfa
rct
Lat
e in
farc
t
Hem
atom
a
Dec
omp
cra
nie
cto
my
Vas
osp
asm
HH
H
Tra
cheo
sto
my
Neu
rod
efic
it
Sev
erit
y of
hem
ipa
resi
s
Oth
er c
omp
lica
tio
n
Du
rati
on o
n v
enti
lato
r
Du
rati
on o
f IC
U s
tay
Pos
t op
ho
spit
al
sta
y
GC
S a
t d
ay
5
Dis
char
ge G
CS
Ran
kin
at
dis
cha
rge
Ran
kin
at
foll
ow
up
foll
ow u
p G
CS
Def
icit
Sev
erit
y of
hem
ipa
resi
s
Dea
th
Cau
se o
f d
eath
0 2 1 1 3 0 2 0 0 1 0 0 1 0 1 0 0 0 0 0 0 1 3 0 2 3 11 15 15 4 2 15 1 4 0 0
1 0 0 1 1 1 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 1 2 0 5 8 22 13 15 5 4 15 1 3 0 0
1 1 1 1 1 0 5 0 0 0 0 0 0 0 1 0 0 1 0 0 1 1 1 0 21 34 49 4 10 5 4 13 1 1 0 0
0 0 1 3 1 0 3 0 0 0 0 0 0 0 0 0 0 0 0 0 0 3 0 0 0 1 7 15 15 1 1 15 3 0 0 0
0 0 0 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 5 15 15 1 0 15 0 0 0 0
0 0 0 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 0 0 1 1 1 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 0 0 3 1 1 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 6 15 15 1 0 15 0 0 0 0
0 0 0 5 1 0 0 0 0 0 0 0 0 2 0 0 0 0 0 0 0 0 0 0 2 3 15 15 15 2 1 15 0 0 0 0
0 0 1 1 1 1 2 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 2 11 15 15 2 1 15 0 0 0 0
0 0 0 4 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 12 15 15 2 1 15 2 0 0 0
0 0 1 0 1 1 6 0 0 0 0 0 1 0 0 0 0 0 1 1 0 0 0 0 1 2 13 15 15 2 0 15 0 0 0 0
0 0 0 5 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 1 0 1 16 15 15 3 0 15 0 0 0 0
0 0 0 5 1 0 0 0 0 0 0 1 1 0 0 0 0 0 0 0 0 0 0 5 1 3 13 15 15 3 1 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 1 0 0 1 1 0 1 1 6 5 5 0 3 6 0 1 1
0 1 1 4 1 0 12 0 0 0 0 0 0 0 0 1 0 0 0 0 0 1 2 7 5 6 20 12 13 5 3 15 1 3 0 0
0 0 0 0 1 1 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 1 3 3 4 7 21 13 15 4 2 15 1 4 0 0
0 1 1 4 1 0 9 0 0 0 0 0 0 2 0 0 0 0 0 0 0 0 0 0 2 3 17 15 15 3 1 15 0 0 0 0
0 0 0 3 1 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 2 0 0 0 1 6 15 15 1 0 15 2 0 0 0
0 0 1 2 1 0 2 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 1 12 15 15 2 0 15 0 0 0 0
0 1 1 2 1 0 5 0 0 0 0 1 0 2 0 0 0 0 0 0 0 2 0 0 0 1 11 15 15 1 1 15 2 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 1 4 0 1 2 13 15 15 1 0 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2 0 0 0 1 8 15 15 2 1 15 2 0 0 0
0 1 1 5 1 1 5 0 1 1 1 0 1 0 1 0 1 0 0 0 0 1 1 0 2 2 0 0 6 1 1 1
0 0 0 1 1 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 1 2 11 15 15 2 0 15 0 0 0 0
0 0 0 2 1 1 0 0 0 0 0 0 0 3 0 0 0 0 0 0 0 0 0 0 1 2 9 15 15 1 0 15 0 0 0 0
0 1 0 2 1 0 0 0 0 1 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 1 1 2 1 0 2 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 1 1 1 1 1 5 0 0 0 0 0 1 3 0 0 0 1 1 1 0 4 0 8 7 7 0 0 6 0 1 3
0 0 1 2 1 0 9 0 0 0 0 1 0 0 0 0 0 0 0 0 0 1 4 0 1 2 7 15 15 1 0 15 0 0 0 2
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 0 0 3 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 10 15 15 1 0 15 0 0 0 0
2

Cas
e n
um
ber
Hos
p N
um
ber
Age
Sex
Hyp
erte
nsi
on
Dia
bet
es
Oth
er c
omo
rbid
ity
oth
er C
omo
rbid
ity
Hea
dac
he
Vom
itin
g
3rd
ner
ve p
als
y
Oth
er s
ymp
tom
s
Sym
tom
to
su
rger
y
3 rd
ner
ve
Foc
al d
efic
it
GC
S
WF
NS
Mod
ifie
d F
isch
er g
rad
e
IVH
No
SA
H
Infa
rct
Cis
tern
blo
od
Hyd
roce
ph
alu
s
oth
er
CT
A
MR
A
DS
A
PC
OM
Oth
er l
oca
tio
n
Mu
ltip
le
Dir
ecti
on
Rel
atio
n T
o P
com
No
of l
obes
Sh
ape
of a
neu
rysm
Siz
e of
nec
k (
)
Dom
e h
eig
ht
Dom
e w
idth
Tee
t
Ble
ed
Per
fora
tor
loss
34 379978 34 2 0 0 3 0 1 1 0 0 50 0 0 15 1 1 0 0 1 1 0 0 1 0 1 1 3 1 2 2 0 1 2.1 2.1 1.7 0 1 0
35 349951 57 2 1 0 0 0 1 1 0 0 312 0 0 15 0 0 0 1 0 0 0 0 1 0 1 1 1 1 1 3 1 1 4.5 1.7 1.3 0 0 0
36 379816 25 2 0 0 0 7 1 0 1 0 10 1 0 15 2 1 0 0 0 0 0 0 1 1 0 1 0 0 3 3 0 1 2.7 7.9 6.2 0 1 0
37 381087 60 2 1 0 0 8 1 1 1 0 7 1 0 15 1 4 1 0 0 0 0 0 1 0 0 1 0 0 2 1 0 1 5 6.9 4.8 0 0 0
38 327026 70 2 1 0 0 0 0 0 0 0 381 0 0 15 0 0 0 1 0 0 0 0 1 0 1 1 0 0 1 1 0 1 5.1 5.1 2.4 0 0 0
39 381895 56 1 1 0 0 7 1 1 0 0 3 0 0 15 1 3 0 0 0 1 0 0 0 0 1 1 0 0 1 1 0 1 3.2 6.1 2.9 1 1 0
40 382453 53 2 1 0 0 8 1 0 0 0 8 0 0 15 1 2 0 0 0 1 0 0 1 0 0 1 0 0 1 2 2 1 0 0 0 0 1 0
41 380465 38 1 0 0 0 8 1 0 0 0 1460 0 0 15 1 0 0 0 0 0 0 0 1 0 1 1 0 0 6 2 0 1 3.6 13.2 8.7 0 0 0
42 382831 49 2 0 0 0 8 1 0 1 0 5 1 0 15 1 4 1 0 0 1 0 0 1 1 0 1 0 0 1 1 0 1 2.8 13.6 10 1 1 0
43 383010 51 2 1 0 0 7 1 1 0 3 15 0 0 15 1 2 0 0 1 0 0 0 1 1 1 1 2 1 1 1 0 2 0 0 0 0 0 0
44 382898 56 2 1 0 0 0 0 0 0 5 42 0 1 15 0 0 0 1 1 0 0 0 1 1 1 1 10 0 4 3 0 1 4.9 12.1 16.9 0 0 0
45 383745 51 1 0 0 0 0 0 0 1 0 150 1 0 15 0 0 0 1 0 0 0 0 1 0 0 1 0 0 2 2 0 1 2.6 10 6 0 0 0
46 385280 54 1 0 0 0 7 1 0 0 1 13 0 0 13 2 4 1 0 0 1 0 0 1 0 0 1 0 0 1 1 0 1 0 0 0 0 0 0
47 385806 77 2 1 1 0 0 1 0 0 0 7 0 0 15 1 3 0 0 0 1 0 0 1 0 0 1 3 1 2 3 0 1 2.2 3.6 2.8 0 1 0
48 387281 53 1 0 0 0 7 1 0 1 0 15 1 0 15 1 1 0 0 0 1 0 0 1 1 0 1 0 0 2 1 0 1 1.2 2.5 1.6 0 0 0
49 386650 53 1 0 1 0 8 1 1 0 3 28 0 0 15 1 4 1 0 0 1 1 0 1 0 0 1 1 1 3 2 0 1 0.7 2.3 2 0 1 0
50 387696 70 2 1 0 0 0 1 0 1 0 8 1 0 15 1 2 0 0 0 1 0 0 1 1 0 1 12 1 1 2 0 1 3 7.4 4.6 0 0 0
51 389334 50 2 0 0 0 0 1 1 1 0 16 1 0 15 1 4 1 0 1 1 0 0 1 1 0 1 1 1 1 1 0 1 0 0 0 0 1 0
52 389295 67 2 0 0 0 8 1 0 1 0 22 1 0 15 1 2 0 0 0 1 0 0 1 1 0 1 0 1 1 1 0 1 4 6.3 4.3 0 0 0
53 390365 60 2 1 1 0 7 1 1 0 0 8 0 0 15 1 1 0 0 0 0 0 0 1 0 0 1 0 0 1 1 2 1 0 0 0 0 0 0
54 390480 72 2 1 0 3 0 1 1 0 3 67 0 0 15 1 3 0 1 0 1 0 0 1 0 0 1 0 0 1 1 0 1 3 5.6 3 0 1 0
55 391656 60 2 1 1 0 0 1 1 1 0 15 1 0 15 1 2 0 0 0 1 0 0 1 1 0 1 0 0 2 2 0 1 2.5 8 4 0 0 0
56 391729 50 2 0 0 0 8 1 0 0 0 12 0 1 15 1 0 0 0 0 0 0 0 1 0 1 5 0 1 1 1 0 1 1.7 5.2 2.7 0 0 0
57 392592 59 2 1 0 0 0 1 0 0 0 18 0 0 14 2 2 0 0 0 0 0 0 1 0 1 1 13 1 1 2 1 1 0 0 0 0 0 0
58 393383 60 1 0 0 0 0 0 0 0 3 7 0 1 13 2 3 0 0 0 1 0 0 1 0 0 1 0 0 1 3 0 1 0 0 0 0 0 0
59 394625 51 1 1 1 0 7 1 0 0 0 20 0 0 15 1 2 0 0 0 1 0 0 1 0 0 1 0 0 1 1 0 1 0 0 0 0 0 0
60 395114 43 2 0 0 0 8 1 0 0 4 12 0 0 15 1 2 0 0 0 0 0 0 1 0 1 1 0 0 3 1 0 1 0 0 0 0 0 0
61 395523 61 2 1 0 0 7 1 1 0 0 4 0 0 15 1 1 0 0 0 0 0 0 1 0 0 1 0 0 2 1 0 1 3.2 8.3 7.7 0 0 0
62 397738 47 1 0 0 0 0 1 0 0 3 8 0 0 15 1 2 0 0 0 0 0 0 1 0 0 1 0 0 3 3 0 1 0 0 0 0 0 0
63 398015 37 2 0 0 4 0 1 0 0 3 25 0 0 15 1 2 0 0 0 1 0 0 1 0 0 1 0 0 1 1 0 1 0 0 0 0 0 0
64 398155 62 2 1 0 5 8 0 0 1 0 21 1 0 15 0 0 0 0 0 0 0 0 1 1 1 1 0 0 5 2 0 1 4 1.6 1.2 0 0 0
65 398775 65 2 0 0 0 0 1 1 0 0 9 0 0 15 1 1 0 0 0 0 0 0 1 0 0 1 0 0 1 2 0 1 3.2 4 3.3 0 0 0
66 398739 85 2 1 0 0 7 1 0 0 3 10 0 0 15 1 2 0 0 0 1 0 0 1 1 0 1 2 1 4 1 0 1 3.2 8 6 1 0 0
3

Cas
e n
um
ber
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
Fet
al P
CO
M
IOR
Tem
p c
lip
Typ
e of
cli
p
No
of c
lip
Wra
p
Du
rati
on o
f te
mp
cli
p(M
in)
Per
fora
tor
loss
Cal
cifi
cati
on
Ath
eros
cler
osi
s
Th
rom
bu
s
Rel
atio
n t
o 3
rd
ver
ve
Op
en l
amin
a t
erm
ina
lis
Oth
er
Ear
ly i
nfa
rct
Lat
e in
farc
t
Hem
atom
a
Dec
omp
cra
nie
cto
my
Vas
osp
asm
HH
H
Tra
cheo
sto
my
Neu
rod
efic
it
Sev
erit
y of
hem
ipa
resi
s
Oth
er c
omp
lica
tio
n
Du
rati
on o
n v
enti
lato
r
Du
rati
on o
f IC
U s
tay
Pos
t op
ho
spit
al
sta
y
GC
S a
t d
ay
5
Dis
char
ge G
CS
Ran
kin
at
dis
cha
rge
Ran
kin
at
foll
ow
up
foll
ow u
p G
CS
Def
icit
Sev
erit
y of
hem
ipa
resi
s
Dea
th
Cau
se o
f d
eath
1 0 0 1 1 1 0 0 0 0 0 0 0 3 0 0 0 0 0 0 0 0 0 0 0 1 12 15 15 1 0 15 0 0 0 0
1 0 0 1 1 0 0 0 0 0 0 0 0 3 0 0 0 0 0 0 0 0 0 0 0 1 6 15 15 1 0 15 0 0 0 0
0 1 1 2 2 1 3 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 2 1 15 2 0 0 0
0 0 0 1 1 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 2 0 0 0 1 11 15 15 1 1 15 2 0 0 0
0 0 0 1 1 0 0 0 0 0 0 0 0 3 0 1 0 0 0 0 0 1 4 0 0 1 13 15 15 4 3 15 1 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 6 15 15 1 0 15 0 0 0 0
0 1 1 2 2 1 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 6 15 15 1 0 15 0 0 0 0
0 0 1 2 1 0 16 1 0 0 0 1 0 0 1 0 0 0 0 0 0 1 1 0 2 5 16 15 15 4 2 15 1 4 0 0
0 0 0 0 0 1 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 1 11 15 15 1 0 15 0 0 0 0
0 0 1 1 2 1 10 0 1 1 0 1 1 4 0 0 0 0 0 0 0 2 4 0 2 3 13 15 15 4 1 15 1 4 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 2 0 0 0 1 7 15 15 2 1 15 2 0 0 0
0 0 1 2 1 0 3 0 0 0 0 0 0 4 0 1 0 0 0 0 1 1 3 0 6 8 18 10 14 4 1 15 1 4 0 0
0 0 1 5 2 0 7 0 0 0 0 0 1 0 1 0 0 0 0 0 1 2 1 0 8 8 8 10 6 0 1 2
0 0 0 1 1 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 2 0 0 0 1 6 15 15 1 0 15 0 0 0 0
0 0 0 2 2 1 0 0 0 0 0 1 0 3 0 0 0 0 0 0 0 0 0 1 1 3 13 15 15 2 0 15 0 0 0 0
0 1 1 2 1 0 1 0 0 1 0 1 0 0 0 0 0 0 0 0 0 2 0 0 0 1 7 15 15 2 1 15 2 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2 0 0 1 2 9 15 15 2 0 15 0 0 0 0
0 0 0 1 1 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 2 0 0 0 1 7 15 15 2 0 15 0 0 0 0
1 0 0 2 1 0 0 0 0 0 0 0 0 2 0 1 0 0 0 0 0 1 4 0 2 4 19 15 15 2 1 15 1 4 0 0
0 0 0 2 1 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 1 0 3 1 2 11 15 15 2 1 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 14 15 15 1 1 15 0 0 0 0
0 1 0 2 1 0 0 0 0 0 0 1 0 4 0 0 0 0 0 0 0 0 0 0 0 1 10 15 15 1 0 15 0 0 0 0
0 0 0 4 1 0 0 0 0 0 0 0 1 0 0 1 0 1 0 0 1 1 3 9 6 6 6 4 6 0 1 2
0 0 0 2 1 0 0 0 0 0 0 1 0 0 0 1 0 0 0 0 0 0 0 3 8 8 8 6 6 0 1 4
0 1 1 2 1 0 8 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 0 1 2 1 0 4.5 0 0 1 0 0 0 0 0 0 0 0 1 0 0 1 3 10 1 2 21 12 15 2 0 15 0 0 0 0
0 0 0 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 8 15 15 1 0 15 0 0 0 0
0 1 1 1 1 1 6 0 0 0 1 1 0 0 1 0 0 0 0 0 0 2 3 0 1 2 14 15 15 3 2 15 0 0 0 0
0 0 1 2 1 0 3 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
1 0 0 1 1 1 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 2 0 1 1 2 19 15 15 2 0 15 0 0 0 0
4

Cas
e n
um
ber
Hos
p N
um
ber
Age
Sex
Hyp
erte
nsi
on
Dia
bet
es
Oth
er c
omo
rbid
ity
oth
er C
omo
rbid
ity
Hea
dac
he
Vom
itin
g
3rd
ner
ve p
als
y
Oth
er s
ymp
tom
s
Sym
tom
to
su
rger
y
3 rd
ner
ve
Foc
al d
efic
it
GC
S
WF
NS
Mod
ifie
d F
isch
er g
rad
e
IVH
No
SA
H
Infa
rct
Cis
tern
blo
od
Hyd
roce
ph
alu
s
oth
er
CT
A
MR
A
DS
A
PC
OM
Oth
er l
oca
tio
n
Mu
ltip
le
Dir
ecti
on
Rel
atio
n T
o P
com
No
of l
obes
Sh
ape
of a
neu
rysm
Siz
e of
nec
k (
)
Dom
e h
eig
ht
Dom
e w
idth
Tee
t
Ble
ed
Per
fora
tor
loss
67 399446 65 2 1 1 0 8 1 1 0 0 13 0 0 15 1 4 1 0 0 1 1 0 1 0 1 1 6 0 4 3 0 1 0 0 0 0 1 0
68 399576 57 2 0 0 5 0 1 0 1 0 186 1 0 15 0 0 0 1 0 0 0 0 1 0 1 1 11 1 4 2 0 1 2.3 9.1 4.8 0 0 0
69 399842 59 2 0 0 0 0 1 0 0 0 8 0 0 15 1 1 0 0 0 0 0 0 1 0 1 1 4 1 4 2 0 1 0 5.9 4.1 0 0 0
70 400315 62 1 0 0 0 7 1 0 0 0 8 0 0 15 1 2 0 0 0 1 0 0 1 1 1 1 14 0 2 1 0 1 7.5 13 11.2 0 0 0
71 401123 45 2 1 0 0 0 1 1 0 3 12 0 0 15 1 4 1 0 0 1 1 0 1 0 0 1 0 0 1 1 0 1 2.2 7.4 4.3 0 0 0
72 401066 55 1 0 0 0 8 1 1 0 3 9 0 0 15 1 4 1 0 1 1 0 0 1 1 0 1 2 1 1 1 0 1 2.7 4.7 4.3 0 0 0
73 401354 38 2 0 0 0 0 1 1 0 0 5 0 0 15 1 3 0 0 0 1 0 0 1 0 0 1 0 0 4 1 0 1 2.5 8 5 0 0 0
74 403299 60 2 1 0 4 7 1 0 0 3 2 0 0 15 1 2 0 0 0 1 0 0 1 0 0 1 0 0 2 1 0 1 2 5.5 3.5 0 0 0
75 403570 66 2 0 0 0 0 1 0 1 3 16 1 0 15 1 0 0 1 0 0 0 0 1 1 1 1 0 0 1 1 1 1 3.5 10.5 10.3 0 0 0
76 404655 59 1 0 0 0 8 1 1 0 0 25 0 0 15 1 2 0 0 0 1 0 0 1 1 1 1 0 0 2 1 0 1 3 8 5 0 0 0
77 408056 58 1 1 0 0 8 1 0 0 5 5 0 0 15 1 3 0 0 1 1 0 0 1 0 0 1 0 0 4 1 0 1 3.2 6 2.7 1 1 0
78 255645 46 2 0 0 0 7 1 1 0 3 13 0 0 15 1 3 0 0 0 1 0 0 1 0 1 1 0 0 3 1 0 1 0 0 0 0 0 0
79 408681 48 2 0 0 0 8 1 0 0 3 15 0 0 15 1 4 1 0 0 1 0 0 1 0 0 1 0 0 1 3 0 1 2 5.6 3.8 0 0 0
80 410050 57 2 0 0 0 7 1 1 0 0 6 0 0 15 1 3 0 0 0 1 0 0 1 0 0 1 0 0 1 1 0 1 4.8 4.5 4.3 0 0 0
81 409762 55 2 0 0 0 8 1 0 0 0 22 0 0 15 1 2 0 0 0 0 0 0 1 0 0 1 0 0 1 3 0 1 3.1 9.7 4.9 0 0 0
82 410234 48 2 1 0 0 0 1 1 0 3 3 0 0 15 1 3 0 0 0 1 0 0 1 0 0 1 0 0 8 1 0 1 3.7 8.2 9.4 0 0 0
83 411866 67 2 1 1 0 0 1 1 0 0 4 0 0 15 1 4 1 0 0 1 1 0 1 0 1 1 0 0 2 1 0 1 2.2 5 3 0 0 0
84 413050 68 2 0 0 0 0 0 0 0 3 7 0 0 15 1 4 1 0 0 1 0 0 1 0 1 1 0 0 1 3 0 1 4.2 13.2 11.7 0 0 0
85 413150 60 2 1 1 5 8 1 0 0 0 7 0 0 15 1 1 0 0 0 1 0 0 1 0 1 1 11 1 1 1 0 1 2.2 5 3.8 1 1 0
86 399526 57 2 0 0 5 0 1 0 1 0 420 1 0 15 0 0 0 1 0 0 0 0 1 0 1 1 11 1 1 1 0 1 5.4 9.1 4.8 0 0 0
87 416458 65 2 1 0 0 8 1 0 0 0 10 0 0 15 1 3 0 0 0 1 0 0 1 0 1 1 5 1 1 1 0 1 3.9 4.5 3.8 1 1 0
88 289935 43 2 0 0 0 0 1 1 1 0 6 1 0 15 1 0 0 1 0 0 0 0 1 0 1 1 0 0 3 2 0 1 4.2 9.6 5.5 0 0 0
89 419437 53 2 1 0 0 0 1 1 0 0 7 0 0 15 1 4 1 0 0 1 1 0 1 1 0 1 0 0 1 1 0 1 0 6.7 5.3 0 0 0
90 419732 65 2 1 0 0 7 1 0 0 3 7 0 0 15 1 3 0 0 0 1 1 0 1 0 1 1 0 0 1 3 1 1 6.3 12.6 7.5 0 0 0
91 421018 62 2 0 0 0 8 1 0 1 0 7 1 0 15 0 0 0 1 0 0 0 0 1 1 0 1 0 0 3 2 0 1 3.2 8.8 6.2 0 0 0
92 422045 73 1 1 0 0 7 1 1 0 0 3 0 1 15 1 3 0 0 0 1 0 0 1 0 0 1 0 0 2 2 0 1 3.7 6.9 5.1 0 0 0
93 422161 48 2 1 0 0 0 1 0 0 0 7 0 0 15 1 3 0 0 0 1 0 0 1 0 0 1 0 0 1 3 1 1 4.8 8.6 6 1 1 0
94 422182 70 2 1 0 0 0 1 0 0 3 5 0 0 15 1 4 1 0 0 1 1 0 1 0 1 1 2 1 3 2 0 1 4 6 4 0 0 0
95 423300 44 1 0 0 0 8 1 0 1 0 6 1 0 15 1 2 0 0 0 1 0 0 1 0 0 1 0 0 1 1 0 1 3.2 7 5.3 0 0 0
96 395816 54 2 1 0 0 7 1 0 0 5 23 0 1 15 2 3 0 0 0 1 0 0 1 0 1 1 12 1 4 1 0 1 3 3 2.7 0 0 0
97 426826 57 2 0 0 0 8 1 1 0 0 13 0 0 15 1 4 1 0 0 1 0 0 1 0 1 1 10 1 5 1 0 1 3.6 3.9 2.7 0 0 0
98 428811 55 2 1 0 0 0 1 1 1 3 7 1 0 15 2 3 0 0 0 1 0 0 1 0 0 1 0 0 2 1 0 1 3 4.8 2 0 0 0
99 429360 48 2 0 0 0 8 1 1 0 4 21 0 0 15 1 1 0 0 0 0 0 0 0 0 1 1 1 1 1 1 2 1 2.5 5 3.4 0 0 0
5

Cas
e n
um
ber
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
Fet
al P
CO
M
IOR
Tem
p c
lip
Typ
e of
cli
p
No
of c
lip
Wra
p
Du
rati
on o
f te
mp
cli
p(M
in)
Per
fora
tor
loss
Cal
cifi
cati
on
Ath
eros
cler
osi
s
Th
rom
bu
s
Rel
atio
n t
o 3
rd
ver
ve
Op
en l
amin
a t
erm
ina
lis
Oth
er
Ear
ly i
nfa
rct
Lat
e in
farc
t
Hem
atom
a
Dec
omp
cra
nie
cto
my
Vas
osp
asm
HH
H
Tra
cheo
sto
my
Neu
rod
efic
it
Sev
erit
y of
hem
ipa
resi
s
Oth
er c
omp
lica
tio
n
Du
rati
on o
n v
enti
lato
r
Du
rati
on o
f IC
U s
tay
Pos
t op
ho
spit
al
sta
y
GC
S a
t d
ay
5
Dis
char
ge G
CS
Ran
kin
at
dis
cha
rge
Ran
kin
at
foll
ow
up
foll
ow u
p G
CS
Def
icit
Sev
erit
y of
hem
ipa
resi
s
Dea
th
Cau
se o
f d
eath
0 1 1 3 1 0 25 0 0 1 0 0 0 0 0 1 0 0 0 0 1 1 3 3 13 17 63 7 13 4 1 15 1 4 0 0
0 0 1 1 1 0 4 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 2 11 15 15 2 0 15 0 0 0 0
0 1 1 3 2 0 3.5 0 0 1 0 1 0 1 0 0 0 0 0 0 0 0 0 3 1 1 1 0 6 0 1 4
0 1 1 1 1 0 8 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 3 3 6 16 15 15 2 0 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
1 0 1 1 1 0 3 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 1 13 15 15 1 0 15 0 0 0 0
0 2 1 3 1 0 14 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 10 15 15 1 0 15 0 0 0 0
0 2 1 2 1 1 2 0 0 0 0 0 0 0 0 1 0 1 1 1 1 0 0 0 9 9 9 5 6 0 1 3
0 0 1 4 2 0 5 0 0 0 0 1 0 0 1 0 0 0 0 0 0 1 3 0 1 3 15 15 15 4 3 15 2 4 0 0
0 0 0 2 1 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 1 1 3 1 0 4 0 0 0 0 0 1 0 1 0 0 0 0 0 0 1 4 0 2 4 14 15 15 3 1 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 4 0 1 8 15 15 2 0 15 0 0 0 0
0 0 0 3 1 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 1 9 15 15 1 0 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 10 15 15 1 0 15 0 0 0 0
1 0 0 1 1 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 6 15 15 1 0 15 0 0 0 0
0 1 1 2 2 0 4 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
0 1 1 3 1 1 29 0 0 0 0 0 1 1 1 0 0 1 1 1 1 1 1 0 4 4 0 3 6 0 1 3
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 0 0 1 9 15 15 1 1 15 0 0 0 0
0 0 0 4 1 0 0 0 0 0 0 1 1 0 0 0 0 0 0 0 0 2 0 0 1 2 8 15 15 4 2 15 2 0 0 0
0 0 0 2 2 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 2 11 15 15 1 0 15 0 0 0 0
0 1 1 2 2 0 1 0 0 0 0 0 0 0 0 0 1 0 0 0 0 2 0 0 1 2 13 15 15 2 0 15 1 0 0 0
0 1 1 1 2 1 5 1 0 0 0 1 1 0 1 0 0 1 0 0 0 1 2 0 3 5 20 9 12 4 4 15 1 2 0 0
0 0 0 2 1 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 1 12 15 15 2 0 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 1 0 0 0 0 0 0 0 0 0 2 0 0 0 1 9 15 15 1 0 15 0 0 0 0
0 0 0 2 1 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 1 4 11 3 5 18 12 15 3 1 15 0 0 0 0
1 0 0 5 1 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 1 0 2 12 15 15 1 0 15 0 0 0 0
0 1 0 4 2 0 0 0 0 1 0 0 0 0 0 1 0 0 0 0 1 0 0 11 7 10 27 9 15 4 1 15 0 0 0 0
0 0 0 2 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 2 0 0 0
0 0 0 1 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 10 15 15 1 0 15 0 0 0 0
1 0 0 4 1 0 0 0 0 0 0 0 0 0 0 0 0 0 1 1 0 0 0 10 1 2 12 15 15 1 0 15 0 0 0 0
0 1 1 2 2 0 6 0 0 1 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 1 11 15 15 1 0 15 0 0 0 0
0 0 0 5 1 0 0 0 0 1 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 1 7 15 15 1 0 15 0 0 0 0
6




![Immunocytochemical Detection of Interaction Products of ...cancerres.aacrjournals.org/content/canres/47/24_Part_1/6719.full.pdf · [CANCER RESEARCH 47, 6719-6725, December 15, 1987]](https://static.fdocuments.us/doc/165x107/5e1ea8f4a2d0a84ffb345031/immunocytochemical-detection-of-interaction-products-of-cancer-research-47.jpg)


![10772 - Senate of the Philippines 10772.pdf · 10772] AN ACT RENEWING FOR ANOTHER TWEhmr.FI\rE (25) '^'EARS THE FRANCHISE GRANTED TO CHRISTIAN ERA BROADCASTING SERVICE INTERNATIONAL.](https://static.fdocuments.us/doc/165x107/5f1c0c1e95f41a11cc4aa1f2/10772-senate-of-the-philippines-10772pdf-10772-an-act-renewing-for-another.jpg)