CLINICAL PRACTICE GUIDELINES - Ministry of Health Desa and was officiatedby Duli Yang Teramat Mulia...
58
CLINICAL PRACTICE GUIDELINES Smoking Cessation Guideline 2014 CLINICAL PRACTICE GUIDELINES Smoking Cessation Guideline 2014 Ministry of Health Brunei Darussalam I love smoke free Brunei!
Transcript of CLINICAL PRACTICE GUIDELINES - Ministry of Health Desa and was officiatedby Duli Yang Teramat Mulia...
CLINICAL PRACTICE GUIDELINESSmoking Cessation Guideline2014
CLINICAL PRACTICE GUIDELINESSmoking Cessation Guideline2014
Ministry of HealthBrunei Darussalam
I love smoke free B
runei!
Contents Pages
ForewordbyPermanentSecretary,MinistryofHealth
ForewordbyHeadofHealthPromotionCentre
Acknowledgements
BruneiDarussalam’sTobaccoControlInitiatives
CodeofPractice
INTRODUCTION
Introduction 1-2
HarmfulEffectsofTobacco 3-4
BenefitsofQuitting 5-6
COUNSELLING
ABCApproach 7
5‘A’sApproach 8-15
5‘R’sApproach 16-17
PHARMACOTHERAPY 19-23
REFERENCES 25-26
APPENDIX 27
APPENDIX1:ABCOFTOBACCOCESSATION 27
APPENDIIX2:5‘A’sAND5‘R’s 28
APPENDIX3:RESPONSESTOPATIENTSDIFFICULTIES 29-31
APPENDIX4:FLOWCHARTOFSMOKINGCESSATIONSERVICES 32-34
1
2
3
4
5

Globallynon-communicablediseases(NCDs)aretheleadingcauseofprematuredeathsandchronicdisabilities.NCDscomprisemainlyofcancers,diabetes,cardiovascularandchronic lung diseases, which account for 60% of all deaths worldwide, and kill anastounding36millionpeopleeachyear.Thevastmajority(86%)ofprematuredeathsfromNCDsoccurindevelopingcountries.
InBruneiDarussalam,NCDswereestimatedtoaccountfor82%ofalldeathsin2011.ThetopfourcausesofdeathinBruneiDarussalamwerecancer,cardiovasculardiseases,diabetesandcerebrovasculardiseases.Tobaccouseisoneofthebiggestcontributingagents as it increases the risk of diseases such as lung cancer, chronic obstructiveairway disease and cardiovascular disease. Furthermore, the secondNational Healthand Nutritional Status Survey (NHANSS) in 2011 reported that the overall smokingprevalence amongst Bruneianswas 17%with the prevalence of adultmale smokersincreasing slightly from 31.1% in 1997 to 32.8%.While prevalence of adult femalesmokersdecreasedfrom5.3%to3.7%.
Inthelastdecade,majorachievementshavebeenmadeinrelationtotobaccocontrol,startingwithratificationoftheFrameworkConventiononTobaccoControlinJune2004followedby theenactmentofTobaccoOrder2005, its subsequent amendmentsandimplementationaswellasestablishmentofsmokingcessationclinicsinthecommunity.However,sincetobaccoconsumptioncontinuestobetheleadingcauseofpreventabledeath,tobaccocontrolmustcontinuetobegiventhehighpriorityitdeserves.
To address this, the Brunei Darussalam National Multisectoral Action Plan for thePreventionandControlofNon-communicableDiseases2013-2018(BruMAP-NCD)whichwaslaunchedinSeptember2013,hasput“reducingtobaccouse”asitsfirstobjectivewithatargetofa30%reductioninprevalenceofcurrenttobaccouseinpersonsaged
Foreword By: Permanent Secretary
15+yearsby2018.Variousrecommendedactionshavealsobeenoutlinedinordertoachievethistarget,oneofwhichistostrengthensmokingcessationservices.
The first ‘Klinik Berhenti Merokok’ was first launched at Berakas ‘A’ Health Centre,AnggerekDesaandwasofficiatedbyDuliYangTeramatMuliaPadukaSeriPengiranMudaMahkotaPengiranMudaHajiAlMuhtadeeBillahIbniKebawahDuliYangMahaMuliaPadukaSeriBagindaSultanHajiHassanalBolkiahMu’izzadinWaddaulah,SeniorMinisteratthePrimeMinister’soffice,on4June2005.Inordertoexpandthesmokingcessationservicestoallhealthcentresandhospitalsinthecountry,theMinistryofHealth,BruneiDarussalam,namelytheHealthPromotionCentrehasorganizedanumberofsmokingcessationcounselingworkshopsforallhealthprofessionalsincludingdoctors,dentists,nurses,psychologists,dietitians,healtheducationofficersandpharmaciststobecomesmokingcessationcounsellors,sothattheycanprovidesmokingcessationservicesattheirrespectivehealthcentresandhospitals.
It is hoped that this clinical practice guideline will help to equip and assist healthprofessionalstodelivereffectiveinterventionstohelptobaccousersbecometobacco-free.IthereforewishtocongratulatemembersoftheCoreTeamfortheirsuccess inproducing thisguideline,whichwill surelyputus in the right track forachieving thetargetset inBruMAP-NCD, leadingustowardsagenerationfreefromTobacco inthefuture.
DATINPADUKADRHJHNORLILABTEDATOPADUKAHJABDULJALILPermanentSecretary
Foreword By: Permanent Secretary
Foreword by Head of Health Promotion Centre
Treatingtobaccouseanddependenceisanimportantandcomplimentaryaspectofanynational tobaccocontrolprogrammes.Theprovisionof smokingcessation services isessentialinhelpingsmokersandtheirfamiliesbecometobacco-freeandinthelongruncontributetoimprovingthequalityoflifeandhealthofallBruneiansgenerally.
The primary aim of this Smoking Cessation Clinical Practice Guidelines is to reducetheprevalenceoftobaccouseanddependencethroughcessationadvice,counsellingand treatment. This current Clinical Practice Guidelines is based on the first editionof the guidelines that was produced in 2005 and has been revised and updated toincludeinformationonharmfuleffectsoftobacco,benefitsofquitting,5‘A’scounsellingapproach,5‘R’smotivationalinterventionsandalsopharmacotherapythatarecurrentlyavailableinsmokingcessationservices.Ihopethatthisrevisededitionwillcontinuetobeausefulresourceandwillhelpguiderelevanthealthprofessionalsinidentifyingandscreeningfortobaccousersaswellasindeliveringevidence-basedtobacco-usecessationadviceandtreatmentforpatientswhousetobaccointheirdailypractice.
ThedevelopmentofthisguidelinesisalsoinlinewiththeactionsidentifiedunderObjective4(ToidentifypeopleatriskofNCDsandmanageeffectively)intheBruneiDarussalamNationalMultisectoralActionPlanforthePreventionandControlofNoncommunicableDiseases(BruMAP-NCD)2013–2018.
Lastly, I would like to take this opportunity to thank the Smoking Cessation ClinicalPractice Guidelines Working Group for their tireless efforts, commitment as well asvaluable contribution in revising and helping to develop this second edition of theSmokingCessationClinicalPracticeGuidelines.
Letusallworktogetherindeliveringqualitycessationservicestohelpreducethenumberofsmokersinourpopulationandultimately,towardsatobacco-freeBruneiinthefuture.
DRHJHNORHAYATIHJMDKASSIMHeadofHealthPromotionCentre
The committee of this Clinical Practice Guideline would like to express theirgratitudeandappreciationtothefollowingforprovidingexpertiseandsupportinthedevelopmentandpublicationofthisguideline:
DatinPadukaDrHjhNorlilabintiDatoPadukaHjAbdulJalil,Permanent Secretary,MinistryofHealth Dr.HjhMaslinabintiHjMohsin,DirectorofHealthServices,MinistryofHealth Dr.HjhNorhayatibintiHjKassim,HeadofHealthPromotionCentre, MinistryofHealth
MatronHjh.FatimahbintiAbdullah,DirectorofNursingServices, MinistryofHealth
Allthosewhohaveprovidedvaluableinputandfeedback
Coreteammembers:
Dr.ErninaNisdzarinahbintiHjAbdulRani,SeniorMedicalOfficer,Smoking CessationServices,HealthPromotionCentre
NurliyanabintiHjMdNoor,Psychologist,HealthPromotionCentre
SuffianbinAwangJulidy,StaffNurse,Berakas‘A’HealthCentre
NoorizanbintiHjIdris,StaffNurse,HealthPromotionCentre
AsnirahbintiApelah,StaffNurse,BelaitSchoolHealth
Pg.AnuarHusainibinPgRambli,HealthEducationOfficer, HealthPromotionCentre
Acknowledgements:
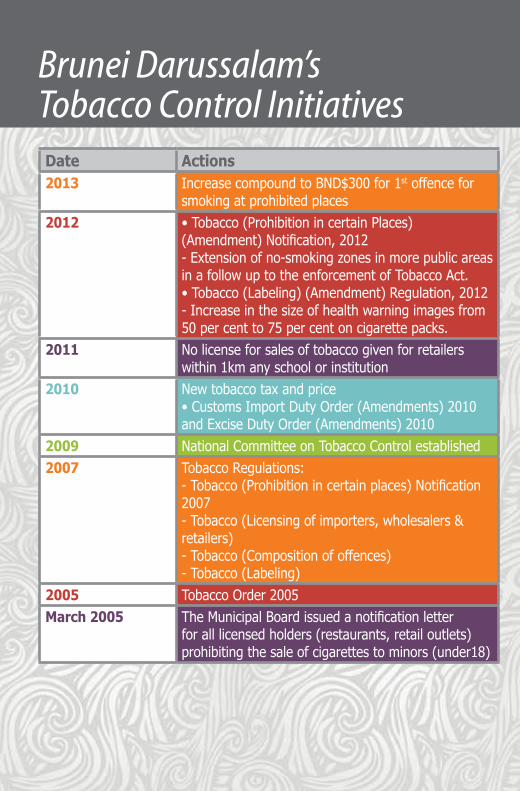
Brunei Darussalam’s Tobacco Control InitiativesDate Actions2013 IncreasecompoundtoBND$300for1stoffencefor
smokingatprohibitedplaces2012 •Tobacco(ProhibitionincertainPlaces)
(Amendment)Notification,2012-Extensionofno-smokingzonesinmorepublicareasinafollowuptotheenforcementofTobaccoAct.•Tobacco(Labeling)(Amendment)Regulation,2012-Increaseinthesizeofhealthwarningimagesfrom50percentto75percentoncigarettepacks.
2011 Nolicenseforsalesoftobaccogivenforretailerswithin1kmanyschoolorinstitution
2010 Newtobaccotaxandprice•CustomsImportDutyOrder(Amendments)2010andExciseDutyOrder(Amendments)2010
2009 NationalCommitteeonTobaccoControlestablished2007 TobaccoRegulations:
-Tobacco(Prohibitionincertainplaces)Notification2007-Tobacco(Licensingofimporters,wholesalers&retailers)-Tobacco(Compositionofoffences)-Tobacco(Labeling)
2005 TobaccoOrder2005March2005 TheMunicipalBoardissuedanotificationletter
foralllicensedholders(restaurants,retailoutlets)prohibitingthesaleofcigarettestominors(under18)
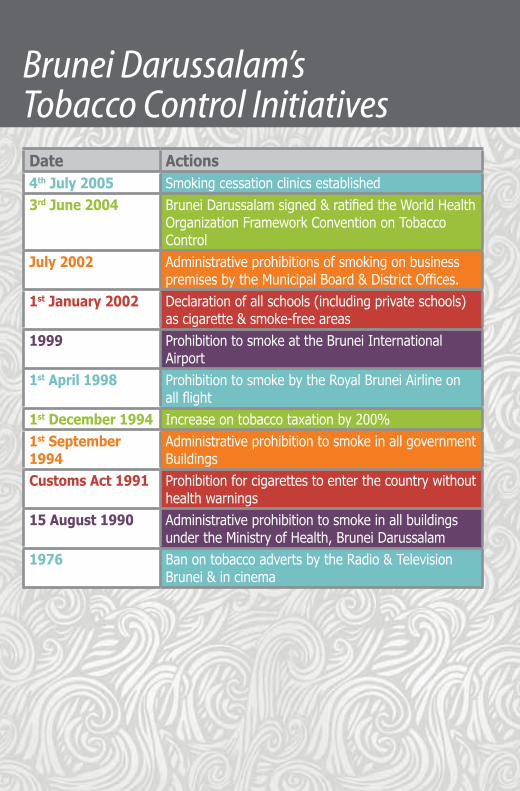
Date Actions4thJuly2005 Smokingcessationclinicsestablished3rdJune2004 BruneiDarussalamsigned&ratifiedtheWorldHealth
OrganizationFrameworkConventiononTobaccoControl
July2002 AdministrativeprohibitionsofsmokingonbusinesspremisesbytheMunicipalBoard&DistrictOffices.
1stJanuary2002 Declarationofallschools(includingprivateschools)ascigarette&smoke-freeareas
1999 ProhibitiontosmokeattheBruneiInternationalAirport
1stApril1998 ProhibitiontosmokebytheRoyalBruneiAirlineonallflight
1stDecember1994 Increaseontobaccotaxationby200%1stSeptember1994
AdministrativeprohibitiontosmokeinallgovernmentBuildings
CustomsAct1991 Prohibitionforcigarettestoenterthecountrywithouthealthwarnings
15August1990 AdministrativeprohibitiontosmokeinallbuildingsundertheMinistryofHealth,BruneiDarussalam
1976 BanontobaccoadvertsbytheRadio&TelevisionBrunei&incinema
Brunei Darussalam’s Tobacco Control Initiatives
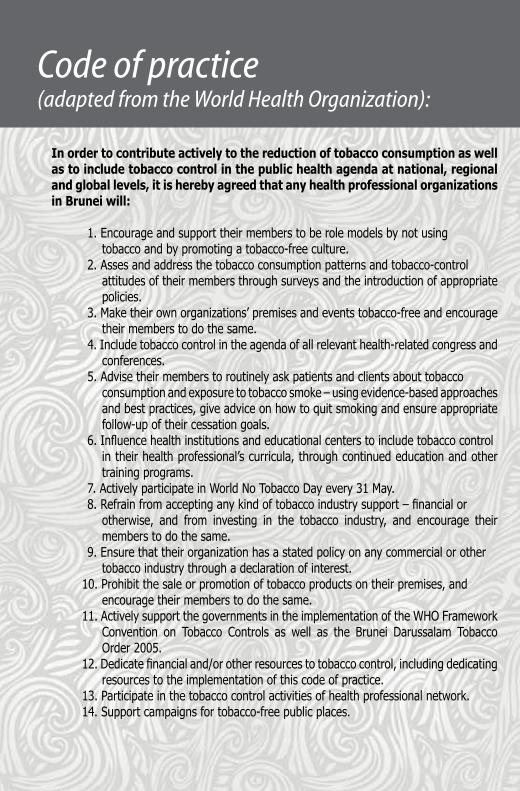
Code of practice (adapted from the World Health Organization):
Inordertocontributeactivelytothereductionoftobaccoconsumptionaswellastoincludetobaccocontrolinthepublichealthagendaatnational,regionalandgloballevels,itisherebyagreedthatanyhealthprofessionalorganizationsinBruneiwill:
1.Encourageandsupporttheirmemberstoberolemodelsbynotusingtobaccoandbypromotingatobacco-freeculture.
2.Assesandaddressthetobaccoconsumptionpatternsandtobacco-controlattitudesoftheirmembersthroughsurveysandtheintroductionofappropriatepolicies.
3.Maketheirownorganizations’premisesandeventstobacco-freeandencouragetheirmemberstodothesame.
4.Includetobaccocontrolintheagendaofallrelevanthealth-relatedcongressandconferences.
5.Advisetheirmemberstoroutinelyaskpatientsandclientsabouttobaccoconsumptionandexposuretotobaccosmoke–usingevidence-basedapproachesandbestpractices,giveadviceonhowtoquitsmokingandensureappropriatefollow-upoftheircessationgoals.
6.Influencehealthinstitutionsandeducationalcenterstoincludetobaccocontrolintheirhealthprofessional’scurricula,throughcontinuededucationandothertrainingprograms.
7.ActivelyparticipateinWorldNoTobaccoDayevery31May.8.Refrainfromacceptinganykindoftobaccoindustrysupport–financialorotherwise, and from investing in the tobacco industry, and encourage theirmemberstodothesame.
9.Ensurethattheirorganizationhasastatedpolicyonanycommercialorothertobaccoindustrythroughadeclarationofinterest.
10.Prohibitthesaleorpromotionoftobaccoproductsontheirpremises,andencouragetheirmemberstodothesame.
11.ActivelysupportthegovernmentsintheimplementationoftheWHOFrameworkConvention on Tobacco Controls as well as the Brunei Darussalam TobaccoOrder2005.
12.Dedicatefinancialand/orotherresourcestotobaccocontrol,includingdedicatingresourcestotheimplementationofthiscodeofpractice.
13.Participateinthetobaccocontrolactivitiesofhealthprofessionalnetwork.14.Supportcampaignsfortobacco-freepublicplaces.

1 Introduction
IntroductionHarmful Effects of TobaccoBenefits of Quitting
1 IN
TROD
UCTION

TheClinicalPracticeGuidelinesonSmokingCessationareanupdateoftheClinicalPracticeGuidelines ‘AGuideToAssistSmokersQuit ‘developedby theMinistryofHealth in2005.The revised guidelines provide updated evidence-based recommendations to support theeffectivenessofinterventionstotreattobaccouseanddependence.Tobaccodependenceisachronicconditionthatrequiresrepeatedinterventionsandmultipleattemptstoquit.
Objectivesofguidelines Theaimistoassistallhealthprofessionalstoidentifyandassessthetobaccouse statusofeverypatientandtodeliverevidence-basedeffectivetobaccouseand dependencetreatments.
Targetusers Theguidelinesareintendedforallhealthprofessionals,includingdoctors, dentists,psychologists,pharmacists,dieticians,socialworkers,occupational therapists,physiotherapistsandnursestoassistthemintheirtobaccousecessation initiatives.
Emergingtrendsoftobaccouse Tobaccoconsumptionisincreasingworldwide(1.3billionsmokers)andhasgrown substantiallyinlow-andmiddle-incomenations(82%oftheworld’ssmokers) includingintheASEANregion.Thishighlyaddictiveproductiscommonlyusedby allsegmentsofthepopulationincludingwomen,youthandchildren. Atpresent,thereare127millionadultssmokers(30%ofadultASEANpopulation) livinginASEANcountries.Tobaccouseremainsthesinglebiggestpreventable causeofdisease,disability,andprematuredeathsintheworld.TheWorldHealth Organizationestimatesthatabout5millionpeopledieprematurelyeachyearfrom tobacco—relateddiseases.Tobaccosmokersarenotonlyputtingthemselvesatrisk butalso1.8billionnon-smokersworldwide.In2004,itwasestimatedthat40% ofchildren,33%ofmaleand35%offemalenon-smokerswereexposedto environmentaltobaccosmoke(ETS).
Introduction
1
SmokingCessation Cigarettesmokingisanaddiction.Nicotineincigarettescausesbothphysicaland psychologicaldependence.Mosttobaccouserswhounderstandthefullrangeof harmscausedbytobaccousewanttoquit,butitisdifficultformanytodoso unaidedbecauseoftheextremeaddictivenessofnicotine.Mostsmokerswhoquit areabletodosowithoutassistance,butcessationinterventionsgreatlyincrease quitrates.Peoplewhoquittobaccouseexperienceimmediateandsignificanthealth benefits,andreducemostoftheirexcesshealthriskwithinafewyears.
Article14oftheWorldHealthOrganization(WHO)FrameworkConventionon TobaccoControl(FCTC)states“Eachpartyshalltakeeffectivemeasurestopromote cessationoftobaccouseandadequatetreatmentfortobaccodependence.Each partyshalldesignandimplementeffectiveprogrammesaimedatpromotingthe cessationoftobaccouse.”
Clinicalcessationinterventionsareeffective,andalsoextremelycost-effective.It hasbeenshownthatbriefadvicefromdoctorsandhealthcareworkersincreases quitratesandpharmacologicaltherapywithnicotinereplacementtherapy(NRT) aloneorincombinationwithotherprescriptioncessationmedicationscandoubleor triplequitrates.
Theprimarygoaloftheclinicalpracticeguidelinesistoreducetheprevalenceof tobaccouseanddependencethroughcessationtreatments.ThisupdatedClinical PracticeGuidelinesonSmokingCessationaredevelopedbasedoncomprehensive literaturereviewsonevidenceontobaccouseanddependencetreatments. Asuggestedframeworkfortreatingtobaccouseanddependencehasalsobeen developedtoprovideasimplestep-by-stepapproachthatallhealthprofessionals canuse.Theimportantmessagetoeveryhealthprofessionalistomaketreating tobaccouseanddependenceapriorityduringthepatient’svisit.
Introduction
2
Harmful Effects of Tobacco
Tobacco use is a major risk factor for many diseases and is also the number onepreventablecauseofdeathintheworld.Onaverage,asmokerdies14yearsprematurelyduetotobacco-relateddiseasescomparedtoanon-smoker.Theharmfuleffectsoftobaccousearewelldocumentedinnumerousstudies.
Ifonesmokes20cigarettesaday,theriskofcontractinglungcancerisabout10-15timesthatofanon-smoker.Onaveragetheriskofdevelopinglungcanceris1%fornon-smokersandupto30%forheavysmokers.
Smokingcausesdiseasesrelatedtotheheartanditsarteriesaswellasbloodvessels.Smokingincreasesthelikelihoodofcontractingcoronaryheartdiseasesby3-4times.Asmokeristwiceaslikelytosufferastrokeascomparedwithapersonwhohasneversmoked.
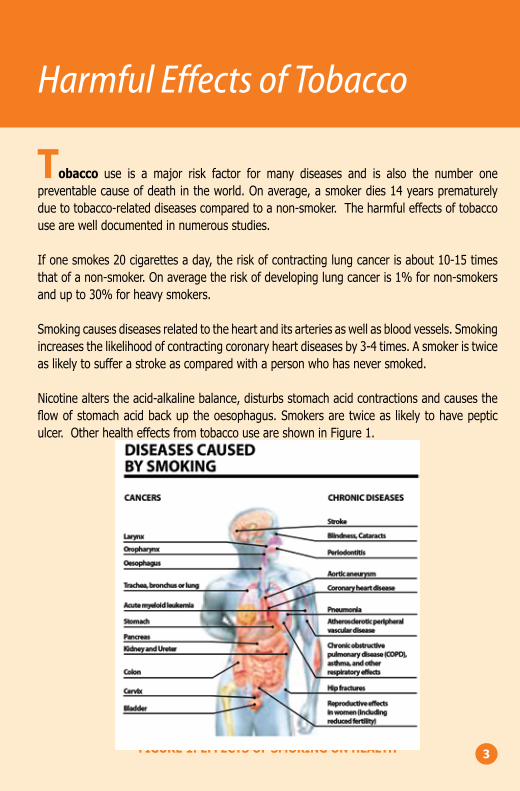
Nicotinealterstheacid-alkalinebalance,disturbsstomachacidcontractionsandcausestheflowofstomachacidbackuptheoesophagus.Smokersaretwiceas likelytohavepepticulcer.OtherhealtheffectsfromtobaccouseareshowninFigure1.
FIGURE1:EFFECTSOFSMOKINGONHEALTH 3
Harmful Effects of Tobacco
Second-handtobaccosmoke,alsoknownasenvironmentaltobaccosmoke(ETS),isacombinationofsidestreamsmoke(thesmokethat isgivenoutbytheburningof tobaccoproduct)andmainstreamsmoke(thesmokeexhaledbythesmoker).
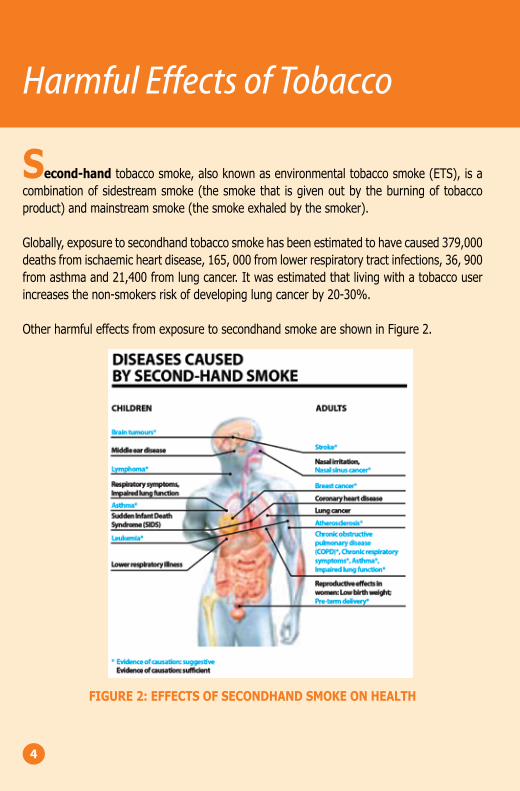
Globally,exposuretosecondhandtobaccosmokehasbeenestimatedtohavecaused379,000deathsfromischaemicheartdisease,165,000fromlowerrespiratorytractinfections,36,900fromasthmaand21,400fromlungcancer.Itwasestimatedthatlivingwithatobaccouserincreasesthenon-smokersriskofdevelopinglungcancerby20-30%.
OtherharmfuleffectsfromexposuretosecondhandsmokeareshowninFigure2.
FIGURE2:EFFECTSOFSECONDHANDSMOKEONHEALTH
4
Benefits of Quitting
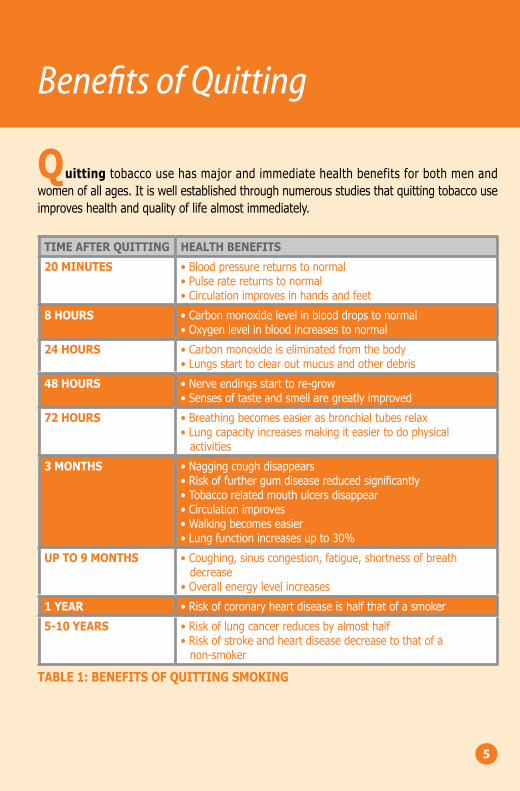
Quittingtobaccousehasmajorandimmediatehealthbenefitsforbothmenandwomenofallages.Itiswellestablishedthroughnumerousstudiesthatquittingtobaccouseimproveshealthandqualityoflifealmostimmediately.
TIMEAFTERQUITTING HEALTHBENEFITS
20MINUTES •Bloodpressurereturnstonormal•Pulseratereturnstonormal•Circulationimprovesinhandsandfeet
8HOURS •Carbonmonoxidelevelinblooddropstonormal•Oxygenlevelinbloodincreasestonormal
24HOURS •Carbonmonoxideiseliminatedfromthebody•Lungsstarttoclearoutmucusandotherdebris
48HOURS •Nerveendingsstarttore-grow•Sensesoftasteandsmellaregreatlyimproved
72HOURS •Breathingbecomeseasierasbronchialtubesrelax•Lungcapacityincreasesmakingiteasiertodophysicalactivities
3MONTHS •Naggingcoughdisappears•Riskoffurthergumdiseasereducedsignificantly•Tobaccorelatedmouthulcersdisappear•Circulationimproves•Walkingbecomeseasier•Lungfunctionincreasesupto30%
UPTO9MONTHS •Coughing,sinuscongestion,fatigue,shortnessofbreathdecrease
•Overallenergylevelincreases
1YEAR •Riskofcoronaryheartdiseaseishalfthatofasmoker
5-10YEARS •Riskoflungcancerreducesbyalmosthalf•Riskofstrokeandheartdiseasedecreasetothatofanon-smoker
TABLE1:BENEFITSOFQUITTINGSMOKING
5
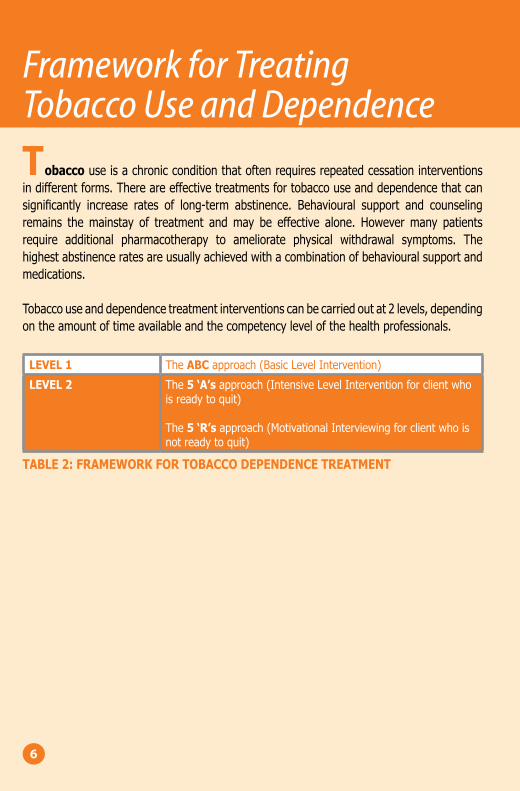
Tobaccouseisachronicconditionthatoftenrequiresrepeatedcessationinterventionsindifferentforms.Thereareeffectivetreatmentsfortobaccouseanddependencethatcansignificantly increase rates of long-term abstinence. Behavioural support and counselingremains themainstay of treatment andmay be effective alone. Howevermany patientsrequire additional pharmacotherapy to ameliorate physical withdrawal symptoms. Thehighestabstinenceratesareusuallyachievedwithacombinationofbehaviouralsupportandmedications.
Tobaccouseanddependencetreatmentinterventionscanbecarriedoutat2levels,dependingontheamountoftimeavailableandthecompetencylevelofthehealthprofessionals.
LEVEL1 TheABCapproach(BasicLevelIntervention)
LEVEL2 The5‘A’sapproach(IntensiveLevelInterventionforclientwhoisreadytoquit)
The5‘R’sapproach(MotivationalInterviewingforclientwhoisnotreadytoquit)
TABLE2:FRAMEWORKFORTOBACCODEPENDENCETREATMENT
Framework for Treating Tobacco Use and Dependence
6
2 Counselling
ABC Approach5 ‘A’s Approach 5 ‘R’s Approach
2 ABC APPRO
ACH

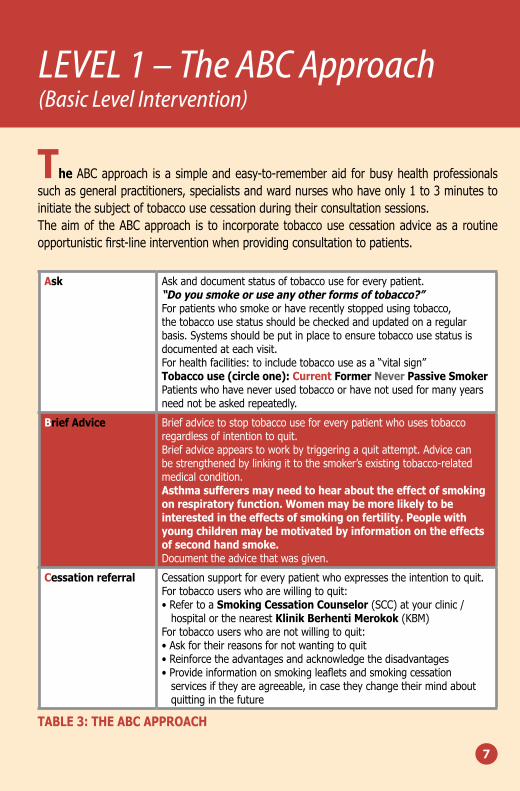
TheABCapproach isasimpleandeasy-to-rememberaidforbusyhealthprofessionalssuchasgeneralpractitioners,specialistsandwardnurseswhohaveonly1to3minutestoinitiatethesubjectoftobaccousecessationduringtheirconsultationsessions.Theaimof theABCapproach is to incorporate tobaccousecessationadviceasaroutineopportunisticfirst-lineinterventionwhenprovidingconsultationtopatients.
Ask Askanddocumentstatusoftobaccouseforeverypatient.“Doyousmokeoruseanyotherformsoftobacco?”Forpatientswhosmokeorhaverecentlystoppedusingtobacco,thetobaccousestatusshouldbecheckedandupdatedonaregularbasis.Systemsshouldbeputinplacetoensuretobaccousestatusisdocumentedateachvisit.Forhealthfacilities:toincludetobaccouseasa“vitalsign”Tobaccouse(circleone):CurrentFormerNeverPassiveSmokerPatientswhohaveneverusedtobaccoorhavenotusedformanyyearsneednotbeaskedrepeatedly.
BriefAdvice Briefadvicetostoptobaccouseforeverypatientwhousestobaccoregardlessofintentiontoquit.Briefadviceappearstoworkbytriggeringaquitattempt.Advicecanbestrengthenedbylinkingittothesmoker’sexistingtobacco-relatedmedicalcondition.Asthmasufferersmayneedtohearabouttheeffectofsmokingonrespiratoryfunction.Womenmaybemorelikelytobeinterestedintheeffectsofsmokingonfertility.Peoplewithyoungchildrenmaybemotivatedbyinformationontheeffectsofsecondhandsmoke.Documenttheadvicethatwasgiven.
Cessationreferral Cessationsupportforeverypatientwhoexpressestheintentiontoquit.Fortobaccouserswhoarewillingtoquit:•RefertoaSmokingCessationCounselor(SCC)atyourclinic/hospitalorthenearestKlinikBerhentiMerokok(KBM)
Fortobaccouserswhoarenotwillingtoquit:•Askfortheirreasonsfornotwantingtoquit•Reinforcetheadvantagesandacknowledgethedisadvantages•Provideinformationonsmokingleafletsandsmokingcessationservicesiftheyareagreeable,incasetheychangetheirmindaboutquittinginthefuture
TABLE3:THEABCAPPROACH
LEVEL 1 – The ABC Approach (Basic Level Intervention)
7
The5 ‘A’sapproach (Ask,Advise,Assess,AssistandArrange) isaneasy-to-implementinterventionforhealthprofessionalsinsettingsthatallowthemtospendalittlemoretimeon tobacco use cessation with their patients. This approach is recommended specificallyfor smoking cessation counselors (SCC) and other health professionals such as generalpractitioners,nurseeducatorswhohaveattendedsmokingcessationcounselingworkshop,tospend15-20minutestoinitiateassessmentandcessationinterventionswithpatientswhousetobacco.
1.ASKPATIENTABOUTSMOKINGSTATUS
Askanddocumentstatusoftobaccouseforeverypatient.Thisshouldbearoutinepracticeateveryconsultation.
“Doyousmokeoruseanyotherformsoftobacco?”
For patientswho smoke or have recently stopped using tobacco, the tobacco use statusshouldbecheckedandupdatedonaregularbasis.Systemsshouldbeputinplacetoensuretobaccousestatusisdocumentedateachvisit.
Forhealthfacilities:toincludetobaccouseasa“vitalsign”Tobaccouse(circleone):CurrentFormerNeverPassiveSmoker
Smokingstatusshouldbeupdatedregularlyanddocumentedinthefile.
Patientswhohaveneverusedtobaccoorhavenotusedformanyyearsneednotbeaskedrepeatedly.Non-smokers(especiallyyouthsandyoungadults)andex-smokersneedpositivereinforcementoftheirsmoke-freelifestyle.
Forsmokers,aroutinesmokinghistoryisessentialforallpatients,andshouldinclude:•Numberofcigarettessmokedperday•Durationofsmoking(years)
LEVEL 2 – THE 5 ‘A’s Approach(Intensive Level Interventions for patient who is ready to quit)
8
LEVEL 2 – THE 5 ‘A’s Approach(Intensive Level Interventions for patient who is ready to quit)
9
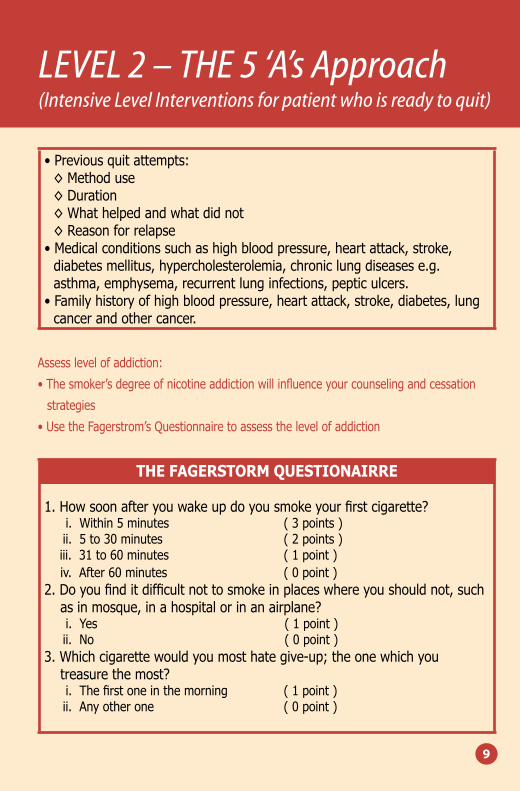
•Previousquitattempts:◊Methoduse◊Duration◊Whathelpedandwhatdidnot◊Reasonforrelapse•Medicalconditionssuchashighbloodpressure,heartattack,stroke,diabetesmellitus,hypercholesterolemia,chroniclungdiseasese.g.asthma,emphysema,recurrentlunginfections,pepticulcers.•Familyhistoryofhighbloodpressure,heartattack,stroke,diabetes,lungcancerandothercancer.
Assesslevelofaddiction:
•Thesmoker’sdegreeofnicotineaddictionwillinfluenceyourcounselingandcessation
strategies
•UsetheFagerstrom’sQuestionnairetoassessthelevelofaddiction
THEFAGERSTORMQUESTIONAIRRE
1.Howsoonafteryouwakeupdoyousmokeyourfirstcigarette?i.Within5minutes (3points)ii.5to30minutes (2points)iii.31to60minutes (1point)iv.After60minutes (0point)
2.Doyoufinditdifficultnottosmokeinplaceswhereyoushouldnot,suchasinmosque,inahospitalorinanairplane?i.Yes (1point)ii.No (0point)
3.Whichcigarettewouldyoumosthategive-up;theonewhichyoutreasurethemost?i.Thefirstoneinthemorning (1point)ii.Anyotherone (0point)
LEVEL 2 – THE 5 ‘A’s Approach(Intensive Level Interventions for patient who is ready to quit)
10
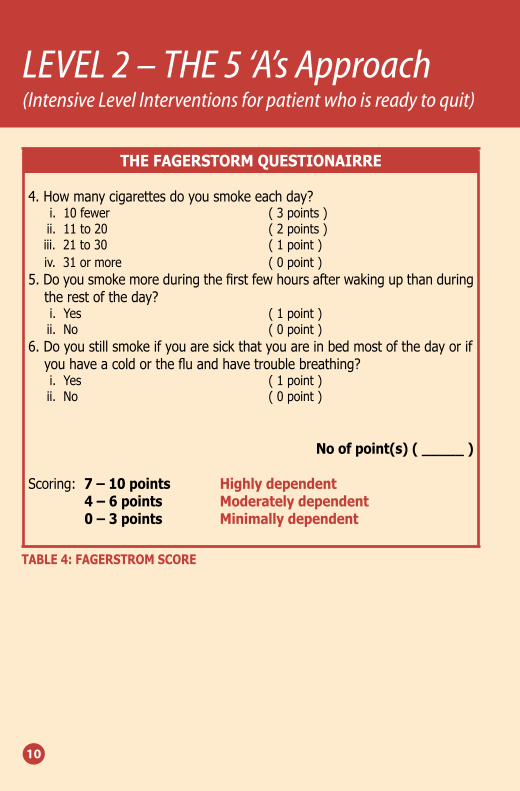
THEFAGERSTORMQUESTIONAIRRE
4.Howmanycigarettesdoyousmokeeachday?i.10fewer (3points)ii.11to20 (2points)iii.21to30 (1point)iv.31ormore (0point)
5.Doyousmokemoreduringthefirstfewhoursafterwakingupthanduringtherestoftheday?i.Yes (1point)ii.No (0point)
6.Doyoustillsmokeifyouaresickthatyouareinbedmostofthedayorifyouhaveacoldorthefluandhavetroublebreathing?i.Yes (1point)ii.No (0point)
Noofpoint(s)(_____)
Scoring:7–10points Highlydependent 4–6points Moderatelydependent 0–3points Minimallydependent
TABLE4:FAGERSTROMSCORE
2.ADVICEPATIENTTOSTOPSMOKING
Somereasonsforpatient’sreluctancetoquitare:•Lackofinformationontheharmfuleffectsoftobacco•Demoralisedbecauseofpreviousrelapse•Fearsorconcernsaboutquitting
Convincethepatienttoquitsmokingwithaclearadviceandstrongmanner.
•“Ireallythinkyoushouldstopsmokingnow”•“Stoppingsmokingisoneofthemostimportanthealthdecisionsyoucanmakeforyourself/yourchild”
Bearinmindyourpatient’sageintailoringyourmessagetohim/her:a.Demographics:Forexample,womenmaybemorelikelytobeinterestedintheeffectsofsmokingonfertilitythanmen.
b.Health:Asthmasufferersmayneedtohearabouttheeffectofsmokingonrespiratoryfunction,whilethosewithgumdiseasemaybe interested intheeffectsofsmokingonoralhealth.
c.SocialFactors:Peoplewithyoungchildrenmaybemotivatedbyinformationontheeffectsofsecondhandsmoke,whileapersonstrugglingwithmoneymaywanttoconsiderthefinancialcostsofsmoking.
Examplesoftailoredadviceinclude:•“Yourcoughwillsubsidemorequicklyandyourairpassageswillreturntonormal”
•“Youwillstopfurtherdamagetoyourlungwhichcausesyourcough/breathingdifficulty”
•“Yourriskofheartattackwilldropimmediately”•“Yourbloodpressurewilldropandyourriskofstrokewillbereducedimmediately”
•“Youwillincreaseyourchancesofhavingnormal,healthybaby”•“Youarelikelytohaveahealthierbaby/childbecauseyouarereducinghis/herriskofsufferingfromchestinfection”
•“Yourstaminawillimprove”
LEVEL 2 – THE 5 ‘A’s Approach(Intensive Level Interventions for patient who is ready to quit)
11
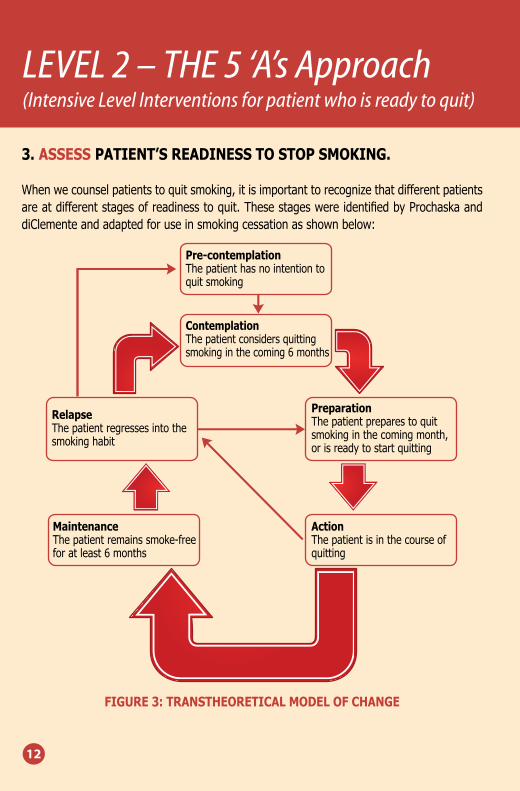
3.ASSESSPATIENT’SREADINESSTOSTOPSMOKING.
Whenwecounselpatientstoquitsmoking,itisimportanttorecognizethatdifferentpatientsareatdifferentstagesofreadinesstoquit.ThesestageswereidentifiedbyProchaskaanddiClementeandadaptedforuseinsmokingcessationasshownbelow:
FIGURE3:TRANSTHEORETICALMODELOFCHANGE
LEVEL 2 – THE 5 ‘A’s Approach(Intensive Level Interventions for patient who is ready to quit)
12
Pre-contemplationThepatienthasnointentiontoquitsmoking
PreparationThepatientpreparestoquitsmokinginthecomingmonth,orisreadytostartquitting
ContemplationThepatientconsidersquittingsmokinginthecoming6months
RelapseThepatientregressesintothesmokinghabit
ActionThepatientisinthecourseofquitting
MaintenanceThepatientremainssmoke-freeforatleast6months
4.ASSISTPATIENTINPREPARATIONFORQUITTING
Workoutwiththepatientonthesmokingcessationplan:
•Setaquitdate–preferablywithinthesubsequenttwoweeks.Makesurethatyourpatientselectsaperiodinhislifewhichisrelativelylowinstress.
•Encouragethepatienttotellfamilymembers,colleaguesandfriendsabouthis/herdecisiontoquitsmokingsoastoenlisttheirsupportandencouragement.Ifaprivatecommitmenttostopsmokingisthenmadepublic,itcreatessocialpressurestosupportthechange.
•Smokersshouldencouragefamily/friends/colleaguestoquitwiththemornotsmokeintheirpresencetominimizeriskoftreatmentfailureandexposuretosecondhandsmoking.
Provideappropriatetechniquesonproblemsolving:
•Identifyreasonsforquittingandbenefitsofquitting•Reviewpastquitattempts–whathelpedandwhatledtorelapse•Reducethenumberofcigarettessmokedgraduallybeforethesetdate.Youmaysuggesttoyourpatientthesetips:◊Trytodelaysmokingthefirstcigaretteforaslongaspossible◊Onlysmokehalfofacigaretteandthrowawaytheremainder◊Ifthereisacravingtosmoke,advisetodelaysmokingingraduation(e.g.15/20/30minutes)
◊Whensmoking,placethecigaretteontheashtrayanddonotholditallthetime◊Smoketheirowncigaretteandsay“no”offeredbyothers◊Changethebrandofcigarettetoaleastfavouredone
•Priortoquitting,avoidsmokinginplaceswherealotofsmoker’stimeisspent(e.g.work,home,car).Makeafewkeyareasas“nosmoking”zone(e.g.inthecar, infrontofthechildren,inthehouse)andputupremindersifnecessary.
•Discardcigarettes,lightersandallothersmoking-relateditemsonthequitdate.
LEVEL 2 – THE 5 ‘A’s Approach(Intensive Level Interventions for patient who is ready to quit)
13
•Anticipatechallengestoplanquitattempt,particularlyduringthecriticalfirstfewweeks.Theseincludenicotinewithdrawalsymptoms.Discusschallenges/triggersandhowsmokerwillsuccessfullyovercomethem.
•Thesmokershouldconsiderlimiting/abstainingfromalcoholwhilequittingasitcancauserelapses.
•Recommendtheuseofnicotinereplacementtherapyormedicationifindicated.•Remindyourpatientthattotalabstinenceisessential.Notevenasinglepuffafterthequitdate.
•Providerelevantsmokingcessationinformationsuchasquitdiarypack,pamphletsetc.•Assistbymakingreferraltoasmokingcessationcounseloratyourclinic/hospitalorthenearestsmokingcessationservicesavailable.
5.ARRANGEFOLLOW-UPFORTHEPATIENT
Workoutwiththeclientonthefollow-upscheduleandapproaches.
•Itispreferabletoconductthefirstfollow-upwithinthefirstweekafterthequitdayandthensubsequentencountersregularly.
•Providecounselingandencouragementduringeachfollow-up.•Recognizetheeffortsofthosewhohavesuccessfullyremainedsmoke-free,andremindthosewhoarestillunabletokickthehabittoregardoccasional‘slips’asanalert.
•Ifarelapseoccurs,encouragetheclienttorepeatquitattempt.
IftheclientisintheActionstage,andhasstoppedsmokingforlessthanamonth,heislikelytobeexperiencingwithdrawalsymptoms.Supportclientby:
•Reinforcethesmoker’sdecisiontoquit.•Praisehim/herforremainingsmokefreesofar.•Encouragethesmokertoactivelydiscussthebenefitsalreadyderivedfromcessation.•Encouragethesmokertoreportanydifficultiespromptlywhilecontinuingeffortstoremainabstinent.
•Stronglyencouragetothesmokertoremainabstinent.
LEVEL 2 – THE 5 ‘A’s Approach(Intensive Level Interventions for patient who is ready to quit)
14
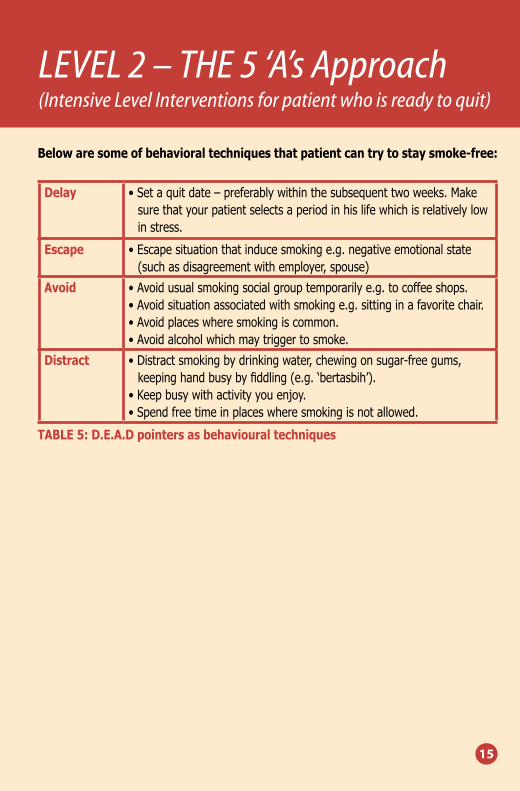
Belowaresomeofbehavioraltechniquesthatpatientcantrytostaysmoke-free:
Delay •Setaquitdate–preferablywithinthesubsequenttwoweeks.Makesurethatyourpatientselectsaperiodinhislifewhichisrelativelylowinstress.
Escape •Escapesituationthatinducesmokinge.g.negativeemotionalstate(suchasdisagreementwithemployer,spouse)
Avoid •Avoidusualsmokingsocialgrouptemporarilye.g.tocoffeeshops.•Avoidsituationassociatedwithsmokinge.g.sittinginafavoritechair.•Avoidplaceswheresmokingiscommon.•Avoidalcoholwhichmaytriggertosmoke.
Distract •Distractsmokingbydrinkingwater,chewingonsugar-freegums,keepinghandbusybyfiddling(e.g.‘bertasbih’).
•Keepbusywithactivityyouenjoy.•Spendfreetimeinplaceswheresmokingisnotallowed.
TABLE5:D.E.A.Dpointersasbehaviouraltechniques
LEVEL 2 – THE 5 ‘A’s Approach(Intensive Level Interventions for patient who is ready to quit)
15
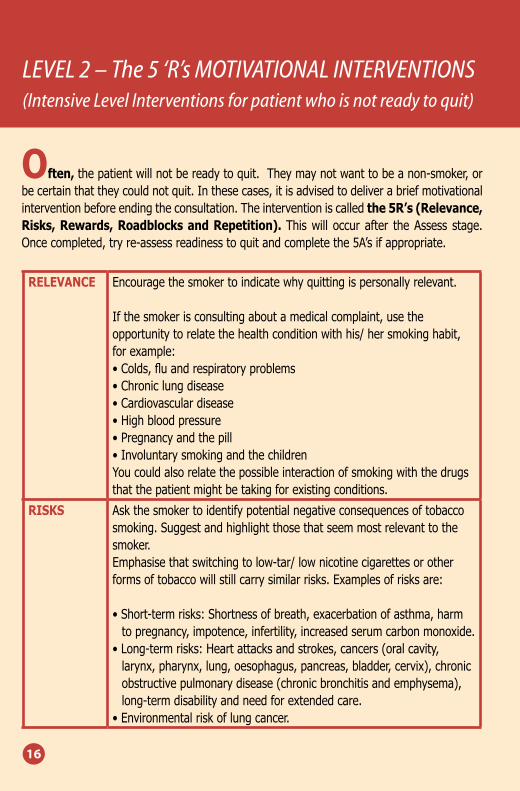
Often,thepatientwillnotbereadytoquit.Theymaynotwanttobeanon-smoker,orbecertainthattheycouldnotquit.Inthesecases,itisadvisedtodeliverabriefmotivationalinterventionbeforeendingtheconsultation.Theinterventioniscalledthe5R’s(Relevance,Risks,Rewards,RoadblocksandRepetition).Thiswill occurafter theAssess stage.Oncecompleted,tryre-assessreadinesstoquitandcompletethe5A’sifappropriate.
RELEVANCE Encouragethesmokertoindicatewhyquittingispersonallyrelevant.
Ifthesmokerisconsultingaboutamedicalcomplaint,usetheopportunitytorelatethehealthconditionwithhis/hersmokinghabit,forexample:•Colds,fluandrespiratoryproblems•Chroniclungdisease•Cardiovasculardisease•Highbloodpressure•Pregnancyandthepill•InvoluntarysmokingandthechildrenYoucouldalsorelatethepossibleinteractionofsmokingwiththedrugsthatthepatientmightbetakingforexistingconditions.
RISKS Askthesmokertoidentifypotentialnegativeconsequencesoftobaccosmoking.Suggestandhighlightthosethatseemmostrelevanttothesmoker.Emphasisethatswitchingtolow-tar/lownicotinecigarettesorotherformsoftobaccowillstillcarrysimilarrisks.Examplesofrisksare:
•Short-termrisks:Shortnessofbreath,exacerbationofasthma,harmtopregnancy,impotence,infertility,increasedserumcarbonmonoxide.
•Long-termrisks:Heartattacksandstrokes,cancers(oralcavity,larynx,pharynx,lung,oesophagus,pancreas,bladder,cervix),chronicobstructivepulmonarydisease(chronicbronchitisandemphysema),long-termdisabilityandneedforextendedcare.
•Environmentalriskoflungcancer.
LEVEL 2 – The 5 ‘R’s MOTIVATIONAL INTERVENTIONS(Intensive Level Interventions for patient who is not ready to quit)
16
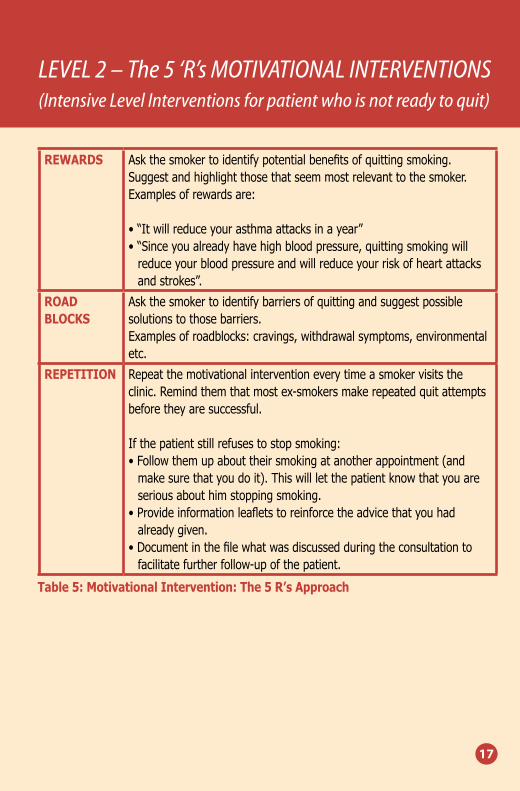
REWARDS Askthesmokertoidentifypotentialbenefitsofquittingsmoking.Suggestandhighlightthosethatseemmostrelevanttothesmoker.Examplesofrewardsare:
•“Itwillreduceyourasthmaattacksinayear”•“Sinceyoualreadyhavehighbloodpressure,quittingsmokingwillreduceyourbloodpressureandwillreduceyourriskofheartattacksandstrokes”.
ROADBLOCKS
Askthesmokertoidentifybarriersofquittingandsuggestpossiblesolutionstothosebarriers.Examplesofroadblocks:cravings,withdrawalsymptoms,environmentaletc.
REPETITION Repeatthemotivationalinterventioneverytimeasmokervisitstheclinic.Remindthemthatmostex-smokersmakerepeatedquitattemptsbeforetheyaresuccessful.
Ifthepatientstillrefusestostopsmoking:•Followthemupabouttheirsmokingatanotherappointment(andmakesurethatyoudoit).Thiswillletthepatientknowthatyouareseriousabouthimstoppingsmoking.
•Provideinformationleafletstoreinforcetheadvicethatyouhadalreadygiven.
•Documentinthefilewhatwasdiscussedduringtheconsultationtofacilitatefurtherfollow-upofthepatient.
Table5:MotivationalIntervention:The5R’sApproach
LEVEL 2 – The 5 ‘R’s MOTIVATIONAL INTERVENTIONS(Intensive Level Interventions for patient who is not ready to quit)
17

3 Pharmacotherapy
3 PH
ARMACO
THERAPY

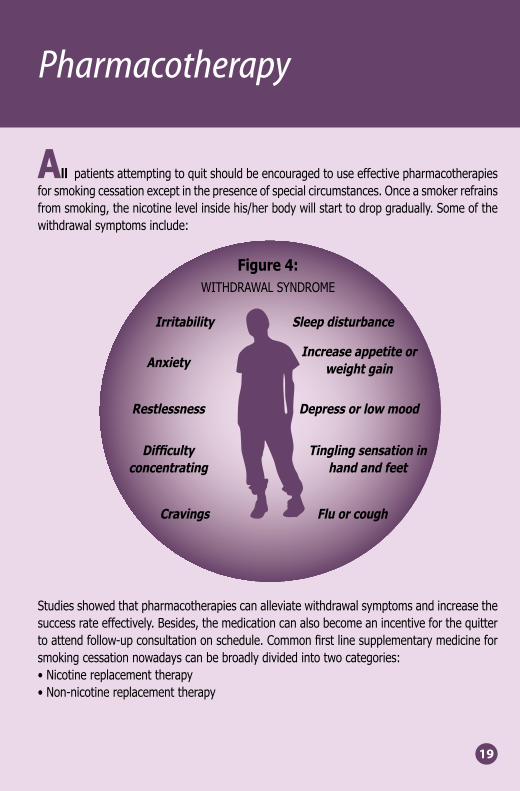
Allpatientsattemptingtoquitshouldbeencouragedtouseeffectivepharmacotherapiesforsmokingcessationexceptinthepresenceofspecialcircumstances.Onceasmokerrefrainsfromsmoking,thenicotinelevelinsidehis/herbodywillstarttodropgradually.Someofthewithdrawalsymptomsinclude:
Studiesshowedthatpharmacotherapiescanalleviatewithdrawalsymptomsandincreasethesuccessrateeffectively.Besides,themedicationcanalsobecomeanincentiveforthequittertoattendfollow-upconsultationonschedule.Commonfirstlinesupplementarymedicineforsmokingcessationnowadayscanbebroadlydividedintotwocategories:•Nicotinereplacementtherapy•Non-nicotinereplacementtherapy
Pharmacotherapy
19
Figure4:WITHDRAWALSYNDROME
SleepdisturbanceIrritability
IncreaseappetiteorweightgainAnxiety
DepressorlowmoodRestlessness
Tinglingsensationinhandandfeet
Difficultyconcentrating
FluorcoughCravings
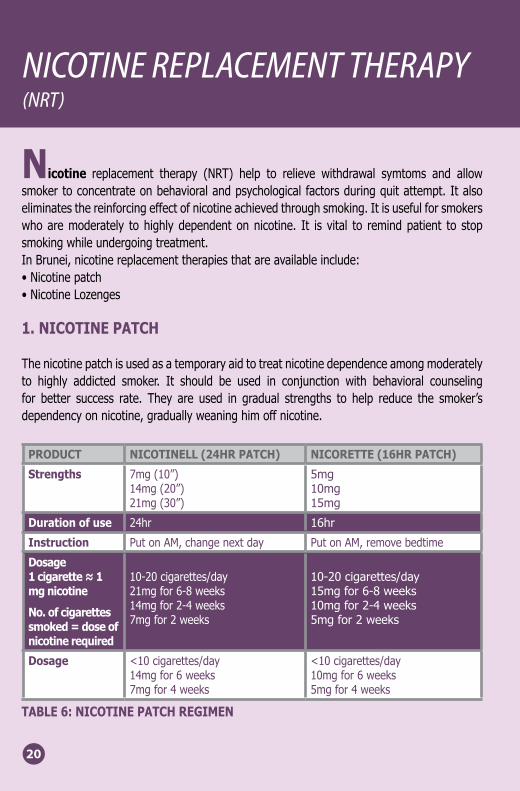
Nicotine replacement therapy (NRT) help to relieve withdrawal symtoms and allowsmokertoconcentrateonbehavioralandpsychologicalfactorsduringquitattempt.Italsoeliminatesthereinforcingeffectofnicotineachievedthroughsmoking.Itisusefulforsmokerswhoaremoderately tohighlydependentonnicotine. It is vital to remindpatient to stopsmokingwhileundergoingtreatment.InBrunei,nicotinereplacementtherapiesthatareavailableinclude:•Nicotinepatch•NicotineLozenges
1.NICOTINEPATCH
Thenicotinepatchisusedasatemporaryaidtotreatnicotinedependenceamongmoderatelyto highly addicted smoker. It should be used in conjunction with behavioral counselingfor better success rate. They are used in gradual strengths to help reduce the smoker’sdependencyonnicotine,graduallyweaninghimoffnicotine.
PRODUCT NICOTINELL(24HRPATCH) NICORETTE(16HRPATCH)
Strengths 7mg(10”)14mg(20”)21mg(30”)
5mg10mg15mg
Durationofuse 24hr 16hr
Instruction PutonAM,changenextday PutonAM,removebedtime
Dosage1cigarette≈1mgnicotine
No.ofcigarettessmoked=doseofnicotinerequired
10-20cigarettes/day21mgfor6-8weeks14mgfor2-4weeks7mgfor2weeks
10-20cigarettes/day15mgfor6-8weeks10mgfor2-4weeks5mgfor2weeks
Dosage <10cigarettes/day14mgfor6weeks7mgfor4weeks
<10cigarettes/day10mgfor6weeks5mgfor4weeks
TABLE6:NICOTINEPATCHREGIMEN
NICOTINE REPLACEMENT THERAPY (NRT)
20
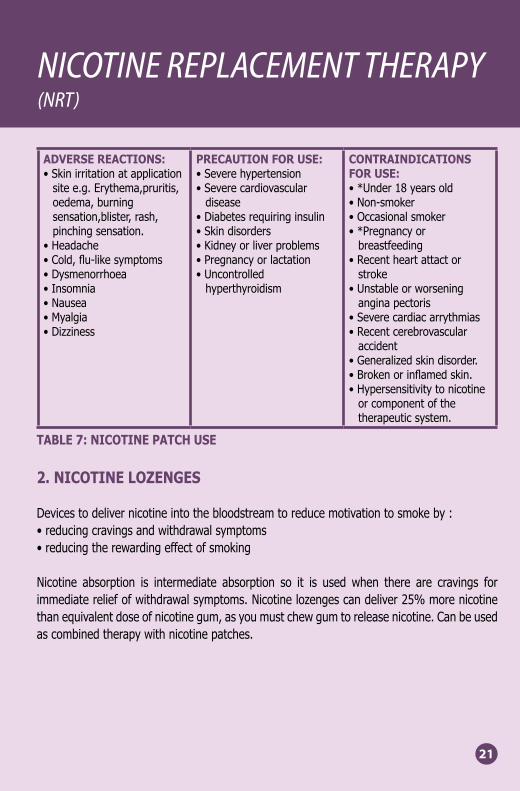
ADVERSEREACTIONS:•Skinirritationatapplicationsitee.g.Erythema,pruritis,oedema,burningsensation,blister,rash,pinchingsensation.
•Headache•Cold,flu-likesymptoms•Dysmenorrhoea•Insomnia•Nausea•Myalgia•Dizziness
PRECAUTIONFORUSE:•Severehypertension•Severecardiovasculardisease
•Diabetesrequiringinsulin•Skindisorders•Kidneyorliverproblems•Pregnancyorlactation•Uncontrolledhyperthyroidism
CONTRAINDICATIONSFORUSE:•*Under18yearsold•Non-smoker•Occasionalsmoker•*Pregnancyorbreastfeeding
•Recentheartattactorstroke
•Unstableorworseninganginapectoris
•Severecardiacarrythmias•Recentcerebrovascularaccident
•Generalizedskindisorder.•Brokenorinflamedskin.•Hypersensitivitytonicotineorcomponentofthetherapeuticsystem.
TABLE7:NICOTINEPATCHUSE
2.NICOTINELOZENGES
Devicestodelivernicotineintothebloodstreamtoreducemotivationtosmokeby:•reducingcravingsandwithdrawalsymptoms•reducingtherewardingeffectofsmoking
Nicotine absorption is intermediate absorption so it is used when there are cravings forimmediatereliefofwithdrawalsymptoms.Nicotinelozengescandeliver25%morenicotinethanequivalentdoseofnicotinegum,asyoumustchewgumtoreleasenicotine.Canbeusedascombinedtherapywithnicotinepatches.
NICOTINE REPLACEMENT THERAPY (NRT)
21
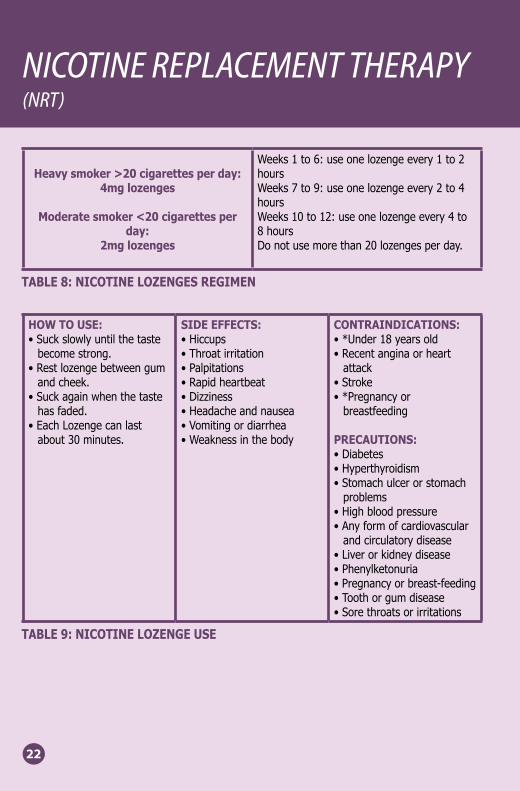
Heavysmoker>20cigarettesperday:4mglozenges
Moderatesmoker<20cigarettesperday:
2mglozenges
Weeks1to6:useonelozengeevery1to2hoursWeeks7to9:useonelozengeevery2to4hoursWeeks10to12:useonelozengeevery4to8hoursDonotusemorethan20lozengesperday.
TABLE8:NICOTINELOZENGESREGIMEN
HOWTOUSE:•Suckslowlyuntilthetastebecomestrong.
•Restlozengebetweengumandcheek.
•Suckagainwhenthetastehasfaded.
•EachLozengecanlastabout30minutes.
SIDEEFFECTS:•Hiccups•Throatirritation•Palpitations•Rapidheartbeat•Dizziness•Headacheandnausea•Vomitingordiarrhea•Weaknessinthebody
CONTRAINDICATIONS:•*Under18yearsold•Recentanginaorheartattack
•Stroke•*Pregnancyorbreastfeeding
PRECAUTIONS:•Diabetes•Hyperthyroidism•Stomachulcerorstomachproblems
•Highbloodpressure•Anyformofcardiovascularandcirculatorydisease
•Liverorkidneydisease•Phenylketonuria•Pregnancyorbreast-feeding•Toothorgumdisease•Sorethroatsorirritations
TABLE9:NICOTINELOZENGEUSE
NICOTINE REPLACEMENT THERAPY (NRT)
22
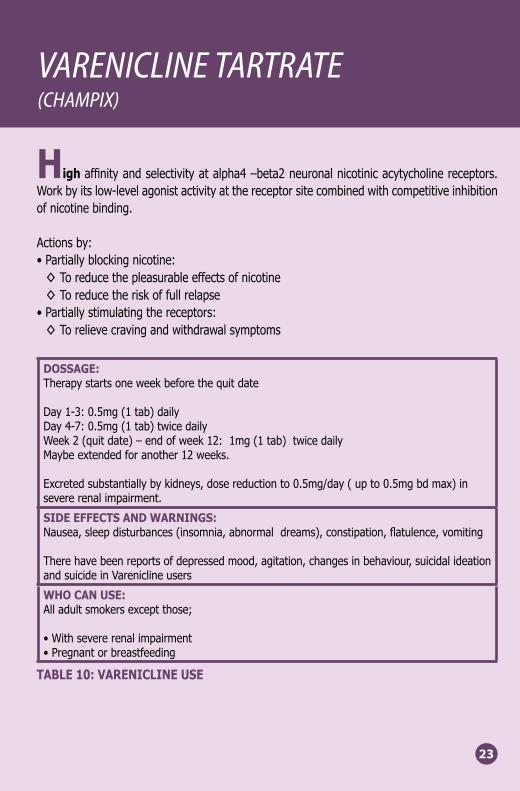
Highaffinityandselectivityatalpha4–beta2neuronalnicotinicacytycholinereceptors.Workbyitslow-levelagonistactivityatthereceptorsitecombinedwithcompetitiveinhibitionofnicotinebinding.
Actionsby:•Partiallyblockingnicotine:◊Toreducethepleasurableeffectsofnicotine◊Toreducetheriskoffullrelapse
•Partiallystimulatingthereceptors:◊Torelievecravingandwithdrawalsymptoms
DOSSAGE:Therapystartsoneweekbeforethequitdate
Day1-3:0.5mg(1tab)dailyDay4-7:0.5mg(1tab)twicedailyWeek2(quitdate)–endofweek12:1mg(1tab)twicedailyMaybeextendedforanother12weeks.
Excretedsubstantiallybykidneys,dosereductionto0.5mg/day(upto0.5mgbdmax)insevererenalimpairment.
SIDEEFFECTSANDWARNINGS:Nausea,sleepdisturbances(insomnia,abnormaldreams),constipation,flatulence,vomiting
Therehavebeenreportsofdepressedmood,agitation,changesinbehaviour,suicidalideationandsuicideinVareniclineusers
WHOCANUSE:Alladultsmokersexceptthose;
•Withsevererenalimpairment•Pregnantorbreastfeeding
TABLE10:VARENICLINEUSE
VARENICLINE TARTRATE (CHAMPIX)
23


4 References
4 REFEREN
CES

REFERENCES:
1.BuildingcapacityforTobaccocontrol/trainingpackage2013.WorldHealthOrganization,Switzerland
2.CertificationforQuitSmokingConsultants2005.HealthPromotionBoard,Singapore
3.ClinicalPracticeGuidelineaGuidetoAssistSmokerQuit2005.MinistryofHealth,BruneiDarussalam
4.Clinicalpracticeguidelines.Treatmentoftobaccosmoking&dependence2003.DiseaseControlDivision,MinistryofhealthMalaysia.Academyofmedicine,September2003.
5.FioreMC,BaileyWC,CohenSJ,etal.TreatingTobaccouseandDependence.ClinicalPracticeGuideline.Rockville,MD:U.S.DepartmentofHealthandHumanServices.PublicHealthService,June2000
6.FroomP.MelamedS,BenbassatJ.Smokingcessationandweightgain.[Review][61refs].JFamilyPractice1998;46(6):460-4
7.HelgasonA&LundK.Generalpractitioners’perceivedbarrierstosmokingcessation’ –results from four Nordic countries. Scand J Public Health2002;30(2):141-7
8.McEwenA,WestR.Smokingcessationactivitiesbygeneralpractitionersandpracticenurses.Tobaccocontrol2001:10:27-32.
9.TheNationalNutritionalStatusSurvey1998,MinistryofHealth,BruneiDarussalam
10.MasonP.HelpingsmokersChange.Aresourcepackfortraininghealthprofessionals.WorldHealthOrganization.
REFERENCES:
25
11.ProschaskaJ,GoldsteinMG.Processofsmokingcessation.Implicationforclinicians.ClinicalChestMedicine1991;12(4):727-35
12.Talktoyourpatientsaboutsmoking.Aguideforthebusyhealthprofessional.NationalhealthEducationaldepartment,MinistryofHealth,Singapore.
13.TreatingTobaccoUseandDependence.HPB-MOHClinicalPracticeGuidelines1/2013.HealthPromotionBoard,Singapore.
14.SmokingCessationInformationKit2009.TobaccoControlOffice,DepartmentofHealth,HongKong.
REFERENCES:
HEALTHLINE 145MINISTRY OF HEALTHBRUNEI DARUSSALAM
26

5 Appendix
APPENDIX 1: ABC OF TOBACCO CESSATION
APPENDIIX 2: 5 ‘A’s AND 5 ‘R’s
APPENDIX 3: RESPONSES TO PATIENTS DIFFICULTIES
APPENDIX 4: FLOWCHART OF SMOKING CESSATION SERVICES
5 APPEN
DIX

APPENDIX 1:
27
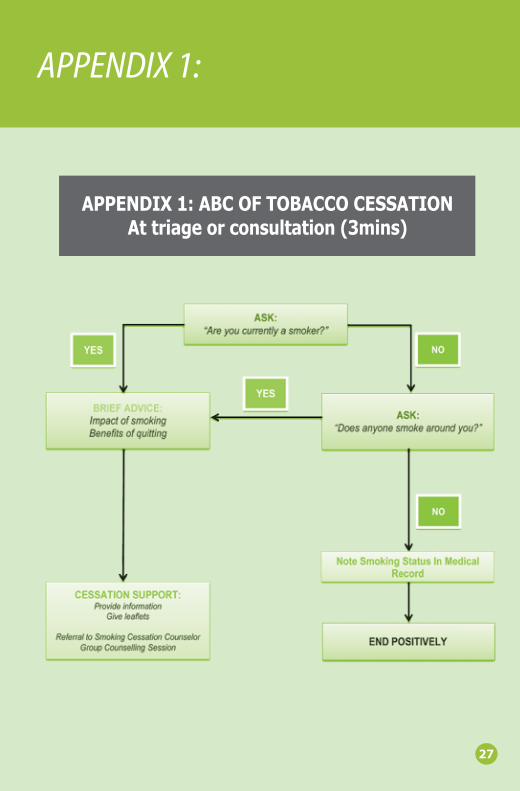
APPENDIX1:ABCOFTOBACCOCESSATIONAttriageorconsultation(3mins)
APPENDIX 2:
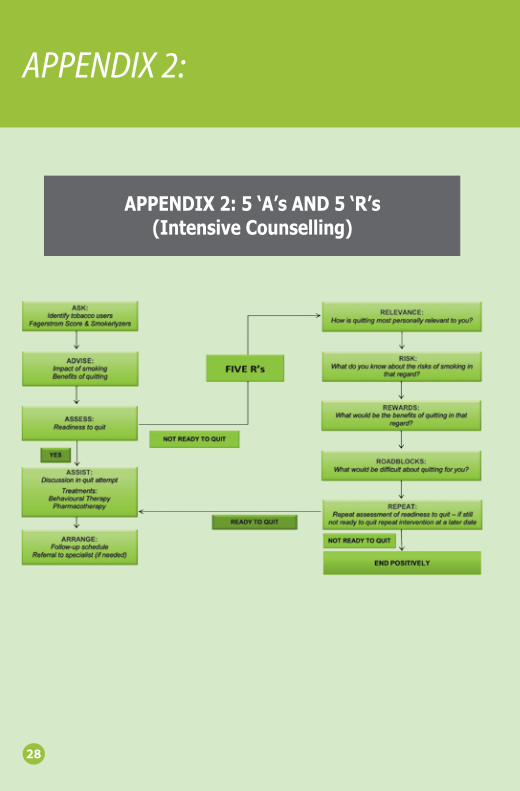
APPENDIX2:5‘A’sAND5‘R’s(IntensiveCounselling)
28
APPENDIX 3: RESPONSES TO PATIENTS DIFFICULTIES
29
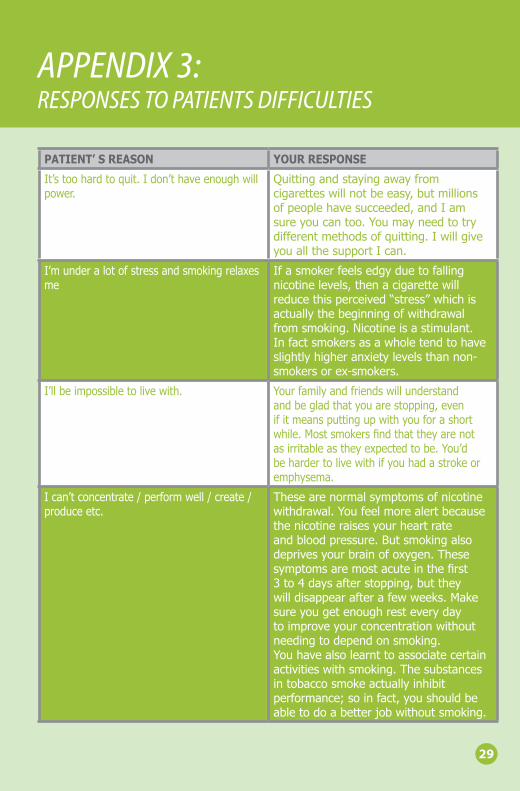
PATIENT’SREASON YOURRESPONSE
It’stoohardtoquit.Idon’thaveenoughwillpower.
Quittingandstayingawayfromcigaretteswillnotbeeasy,butmillionsofpeoplehavesucceeded,andIamsureyoucantoo.Youmayneedtotrydifferentmethodsofquitting.IwillgiveyouallthesupportIcan.
I’munderalotofstressandsmokingrelaxesme
Ifasmokerfeelsedgyduetofallingnicotinelevels,thenacigarettewillreducethisperceived“stress”whichisactuallythebeginningofwithdrawalfromsmoking.Nicotineisastimulant.Infactsmokersasawholetendtohaveslightlyhigheranxietylevelsthannon-smokersorex-smokers.
I’llbeimpossibletolivewith. Yourfamilyandfriendswillunderstandandbegladthatyouarestopping,evenifitmeansputtingupwithyouforashortwhile.Mostsmokersfindthattheyarenotasirritableastheyexpectedtobe.You’dbehardertolivewithifyouhadastrokeoremphysema.
Ican’tconcentrate/performwell/create/produceetc.
Thesearenormalsymptomsofnicotinewithdrawal.Youfeelmorealertbecausethenicotineraisesyourheartrateandbloodpressure.Butsmokingalsodeprivesyourbrainofoxygen.Thesesymptomsaremostacuteinthefirst3to4daysafterstopping,buttheywilldisappearafterafewweeks.Makesureyougetenoughresteverydaytoimproveyourconcentrationwithoutneedingtodependonsmoking.Youhavealsolearnttoassociatecertainactivitieswithsmoking.Thesubstancesintobaccosmokeactuallyinhibitperformance;soinfact,youshouldbeabletodoabetterjobwithoutsmoking.
APPENDIX 3: RESPONSES TO PATIENTS DIFFICULTIES
PATIENT’SREASON YOURRESPONSE
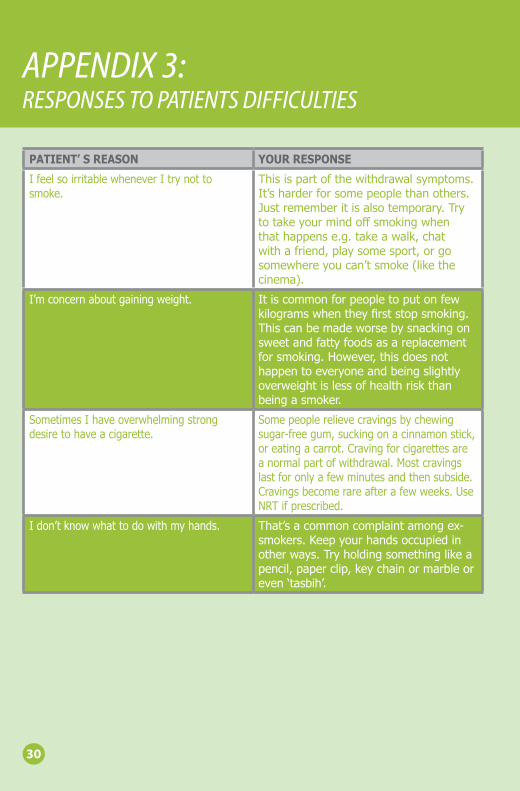
IfeelsoirritablewheneverItrynottosmoke.
Thisispartofthewithdrawalsymptoms.It’sharderforsomepeoplethanothers.Justrememberitisalsotemporary.Trytotakeyourmindoffsmokingwhenthathappense.g.takeawalk,chatwithafriend,playsomesport,orgosomewhereyoucan’tsmoke(likethecinema).
I’mconcernaboutgainingweight. Itiscommonforpeopletoputonfewkilogramswhentheyfirststopsmoking.Thiscanbemadeworsebysnackingonsweetandfattyfoodsasareplacementforsmoking.However,thisdoesnothappentoeveryoneandbeingslightlyoverweightislessofhealthriskthanbeingasmoker.
SometimesIhaveoverwhelmingstrongdesiretohaveacigarette.
Somepeoplerelievecravingsbychewingsugar-freegum,suckingonacinnamonstick,oreatingacarrot.Cravingforcigarettesareanormalpartofwithdrawal.Mostcravingslastforonlyafewminutesandthensubside.Cravingsbecomerareafterafewweeks.UseNRTifprescribed.
Idon’tknowwhattodowithmyhands. That’sacommoncomplaintamongex-smokers.Keepyourhandsoccupiedinotherways.Tryholdingsomethinglikeapencil,paperclip,keychainormarbleoreven‘tasbih’.
30
APPENDIX 3: RESPONSES TO PATIENTS DIFFICULTIES
31
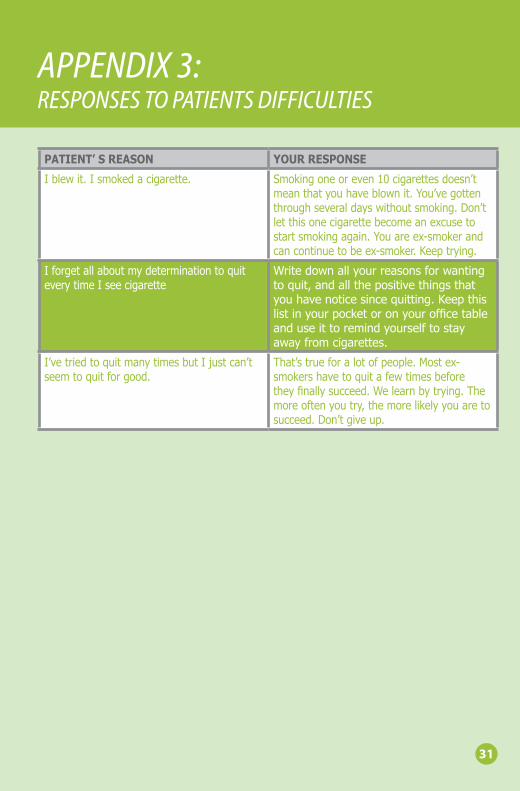
PATIENT’SREASON YOURRESPONSE
Iblewit.Ismokedacigarette. Smokingoneoreven10cigarettesdoesn’tmeanthatyouhaveblownit.You’vegottenthroughseveraldayswithoutsmoking.Don’tletthisonecigarettebecomeanexcusetostartsmokingagain.Youareex-smokerandcancontinuetobeex-smoker.Keeptrying.
IforgetallaboutmydeterminationtoquiteverytimeIseecigarette
Writedownallyourreasonsforwantingtoquit,andallthepositivethingsthatyouhavenoticesincequitting.Keepthislistinyourpocketoronyourofficetableanduseittoremindyourselftostayawayfromcigarettes.
I’vetriedtoquitmanytimesbutIjustcan’tseemtoquitforgood.
That’strueforalotofpeople.Mostex-smokershavetoquitafewtimesbeforetheyfinallysucceed.Welearnbytrying.Themoreoftenyoutry,themorelikelyyouaretosucceed.Don’tgiveup.
APPENDIX 4: FLOWCHART OF SMOKING CESSATION SERVICES
32
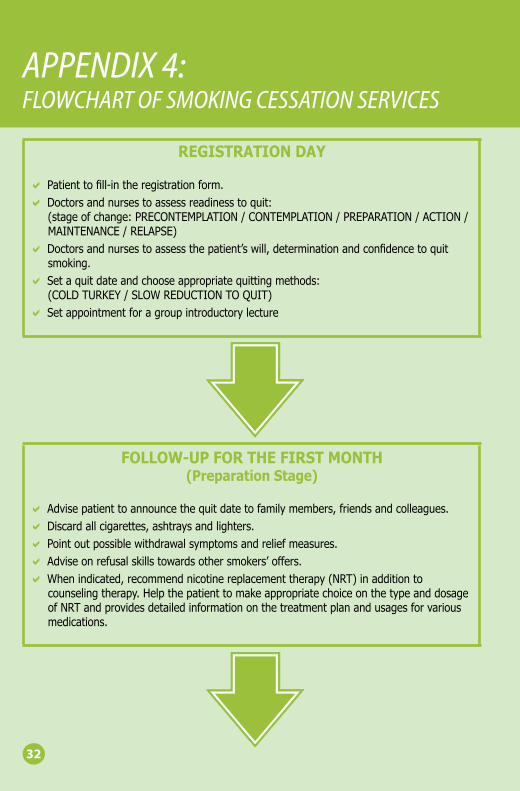
REGISTRATIONDAY
aPatienttofill-intheregistrationform.aDoctorsandnursestoassessreadinesstoquit:
(stageofchange:PRECONTEMPLATION/CONTEMPLATION/PREPARATION/ACTION/MAINTENANCE/RELAPSE)
aDoctorsandnursestoassessthepatient’swill,determinationandconfidencetoquitsmoking.
aSetaquitdateandchooseappropriatequittingmethods:(COLDTURKEY/SLOWREDUCTIONTOQUIT)
aSetappointmentforagroupintroductorylecture
FOLLOW-UPFORTHEFIRSTMONTH(PreparationStage)
aAdvisepatienttoannouncethequitdatetofamilymembers,friendsandcolleagues.aDiscardallcigarettes,ashtraysandlighters.aPointoutpossiblewithdrawalsymptomsandreliefmeasures.aAdviseonrefusalskillstowardsothersmokers’offers.aWhenindicated,recommendnicotinereplacementtherapy(NRT)inadditionto
counselingtherapy.HelpthepatienttomakeappropriatechoiceonthetypeanddosageofNRTandprovidesdetailedinformationonthetreatmentplanandusagesforvariousmedications.
APPENDIX 4: FLOWCHART OF SMOKING CESSATION SERVICES
FOLLOW-UPFORTHESECONDANDTHIRDMONTH(ActionStage:aftertheQUITDATE)
aMakeanoteontheQUITDATE.aCheckcarbonmonoxidelevelonthesmokerlyzers.aCheckurine/salivarycotininetest.aAssessthepatient'sprogress;assistthemtohandledifficultiesencounteredaccordingly.aAssessthemode,dosageandeffectivenessofNRT.aCoachandstrengthenpatient'sconfidenceandskillstoovercomedifficultiesandbarriers.aDiscusstheimportanceofbalanceddietandhealthylifestyles.Encourageregularexercise
anddecenthobbies.
FOLLOW-UPFORTHEFOURTH,FIFTHANDSIXTHMONTH(MaintenanceStage)
aMakeanoteonSmokingStatusat3monthsafterQuitdateaCheckcarbonmonoxidelevelonthesmokerlyzers.aAssessthepatient'sprogress;assistthemtohandledifficultiesencounteredaccordingly.aAssessthemode,dosageandeffectivenessofNRT.aCoachandstrengthenclients’confidenceandskillstoovercomedifficultiesandbarriers.aGuidethepatienttoidentifythesourceofpressureandfigureourappropriatestress
copingstrategies.aSharingofrefusalskillsandencouragethepatienttourgefamilymembers,friendsor
colleaguestoquitsmoking.
33
APPENDIX 4: FLOWCHART OF SMOKING CESSATION SERVICES
34
FOLLOW-UPAFTERSIXMONTHS(MaintenanceStage)
aDischargepatientat6thmonth,makenoteonthesmokingstatus.aCheckcarbonmonoxidelevelonthesmokerlyzers.aCheckurine/salivarycotininetestaGivepatientcertificateof‘successfulquitter’andinviteassupportgrouporspokepersonaOffernecessarycounselingandarrangementstounsuccessfulquitters,andpointoutthat
manysmokersneedseveralattemptstosucceed.aEncouragethepatienttocalltheHealthline145whennecessary.aEncouragesuccessfulquitterstourgefamilymembers,friendsorcolleaguestoquit
smokingaswell.aToremindclientthatafollow-upcallat1yearwillbemadetocheckpatient’sstatus.


Ministry of HealthBrunei Darussalam