CLINICAL PRACTICE GUIDELINES FOR THE MANAGEMENT … · hypersomnia), in sexual function (decrease...
37
CLINICAL PRACTICE GUIDELINES FOR THE MANAGEMENT OF DEPRESSION Document prepared by : Dr. Shiv Gautam, Dr. Lalit Batra Department of Psychiatry, S. M. S. Medical College, Jaipur IPS GUIDELINE COMMITTEE ON DEPRESSION : Dr. Shiv Gautam - Jaipur, Dr. Lalit Batra - Jaipur, Dr. M. L. Gada - Mumbai, Dr. M. M. Bhojak - Jaipur, Dr. V. G. Jhanwar - Varanasi, Dr. Anil Tambi - Jaipur, Dr. Udai Choudhary - Kolkata, Dr. Yussuf Machiswala - Mumbai, Dr. Manaswi Gautam - Mumbai INTRODUCTION Depression is a complex diagnostic construct, applied to individuals with a particular set of symptoms among which the essential ingredients are a depressed mood and a loss of interest (1,2,4). Depression has substantial short term and long term consequences for the individuals affected, their families and society. The symptoms can cause immense distress to patients and are often associated with a variety of social and occupational impairments. The social and economic burden it poses for the community makes it one of the most serious health problems faced by the society. The depression is an all too common disorder that can affect anyone. Indeed chances of developing a depressive illness is estimated to be 1 in 5 for women and 1 in 10 for men for making it a particularly common affliction of man kind.The World Health Organization estimated that within 20 years, recurrent depressive disorder will be the second most serious cause of morbidity and burden of disease in the world. (20) The studies (Epidemiological Catchment Area Study) indicates that major depression has a 1 month prevalence of 2.2% and life time prevalence of 5.8% in Americans(11) Other studies estimated lifetime prevalence to be as high as 26% for females and 12% for males.Studies from diverse settings ranging from rural Chile, to slums of S. Africa and Urban General Practices of India reveal prevalence figures of depression exceeding 30% in Community Samples and approximately 50% in Primary Care Samples Indian studies also indicate a similar trend of prevalence of depression in Indian society (12,13,14). Depression may begin at any age, but average age at onset is late 20s. The symptoms of major depressive disorder typically develop over days to weeks. The prodromal symptoms including generalized anxiety, Panic Attacks, Phobias, or other depressive symptoms that do not meeting the diagnostic threshold may occur over the preceding several months. In some cases a sudden onset may occur.The duration of major depressive episode is also variable, if untreated, the episode typically lasts 6 months or longer. Clinical Presentation of Depression / Depressive episode (ICD-10) General Criteria • The depressive episode should last for at least 2 weeks • No hypomanic or manic symptoms sufficient to meet the criteria for hypomanic or manic episode at any time in the individual's life. • Not attributable to psychoactive substance use or to any organic mental disorder Typical Symptoms • Depressed mood to a degree that is definitely abnormal for the individual present for most of the (83)
Transcript of CLINICAL PRACTICE GUIDELINES FOR THE MANAGEMENT … · hypersomnia), in sexual function (decrease...

CLINICAL PRACTICE GUIDELINES FOR THE MANAGEMENT OF DEPRESSION
Document prepared by : Dr. Shiv Gautam, Dr. Lalit Batra Department of Psychiatry, S. M. S. Medical College, Jaipur
IPS GUIDELINE COMMITTEE ON DEPRESSION :
Dr. Shiv Gautam - Jaipur, Dr. Lalit Batra - Jaipur, Dr. M. L. Gada - Mumbai,
Dr. M. M. Bhojak - Jaipur, Dr. V. G. Jhanwar - Varanasi, Dr. Anil Tambi - Jaipur,
Dr. Udai Choudhary - Kolkata, Dr. Yussuf Machiswala - Mumbai, Dr. Manaswi Gautam - Mumbai
INTRODUCTION
Depression is a complex diagnostic construct, applied to individuals with a particular set of symptoms among which the essential ingredients are a depressed mood and a loss of interest (1,2,4). Depression has substantial short term and long term consequences for the individuals affected, their families and society. The symptoms can cause immense distress to patients and are often associated with a variety of social and occupational impairments. The social and economic burden it poses for the community makes it one of the most serious health problems faced by the society.
The depression is an all too common disorder that can affect anyone. Indeed chances of developing a depressive illness is estimated to be 1 in 5 for women and 1 in 10 for men for making it a particularly common affliction of man kind.The World Health Organization estimated that within 20 years, recurrent depressive disorder will be the second most serious cause of morbidity and burden of disease in the world. (20)
The studies (Epidemiological Catchment Area Study) indicates that major depression has a 1 month prevalence of 2.2% and life time prevalence of 5.8% in Americans(11) Other studies estimated lifetime prevalence to be as high as 26% for females and 12% for males.Studies from diverse settings ranging from rural Chile, to slums of S. Africa and Urban General Practices of India reveal prevalence figures of depression exceeding 30% in Community Samples and approximately 50% in Primary Care Samples Indian studies also indicate a similar trend of prevalence of depression in Indian society (12,13,14).
Depression may begin at any age, but average age at onset is late 20s. The symptoms of major depressive disorder typically develop over days to weeks. The prodromal symptoms including generalized anxiety, Panic Attacks, Phobias, or other depressive symptoms that do not meeting the diagnostic threshold may occur over the preceding several months. In some cases a sudden onset may occur.The duration of major depressive episode is also variable, if untreated, the episode typically lasts 6 months or longer.
Clinical Presentation of Depression / Depressive episode (ICD-10)
General Criteria
• The depressive episode should last for at least 2 weeks
• No hypomanic or manic symptoms sufficient to meet the criteria for hypomanic or manic episode at any time in the individual's life.
• Not attributable to psychoactive substance use or to any organic mental disorder
Typical Symptoms • Depressed mood to a degree that is definitely abnormal for the individual present for most of the
(83)

day and almost every day, largely unresponsive to circumstances, and sustained for at least 2 weeks
• Loss of interest or pleasure in activities that are normally pleasurable
• Decreased energy or increased fatigability
Additional Symptoms
• Loss of confidence and self-esteem
• Unreasonable feelings of self-reproach or excessive and inappropriate guilt
• Recurrent thoughts of death or suicide, or any suicidal behaviour • Complaints or evidence of diminished ability to think or concentrate, such as indecisiveness or
vacillation
• Bleak and pessimistic views of the future
• Sleep disturbances of any type.
» Change in appetite (decrease or increase) with corresponding weight change
Source-[2]. DEPRESSIVE EPISODE
The symptom criteria for the depressive episode according to ICD 10 are listed in table 1. The typical symptoms are depressed mood, lack of interest, pleasure and energy. Symptoms may not be stable during the episode and their change over times adds to the polymorphic presentation of each particular depressed patient.
There is no one single pathognomic symptom that in itself would identify DE/ depression and would allow its monothetic classification. However the symptoms listed in table 1 are described more extensively below.
Depressed mood
Depressed mood is the hallmark of all depressions. The depressed mood is always there, it only needs to be elicited. Depressed mood is a sustained emotional state that is characterized by sadness, low moral, misery, discouragement, hopelessness, emptiness, unhappiness, distress, pessimism and other related affects that if assessed in isolation, cannot easily be delineated from the emotional states universally experienced by all human beings when faced with life's adversities. The main differentiating features of the depressed mood from the non-morbid emotional reaction of sadness are as follows. The intensity and the depth of the pain become so unbearable that often the death wish provides a comforting remedy. The depressed mood lasts long enough to be felt as an unalterable affective state.
Anhedonia - Loss of Interest
Anhedonia and loss of interest are symptoms closely associated with the depressed mood, varying in intensity along with the feeling of sadness.They are unable to draw pleasure from previously enjoyable activities. In severe cases they disregard and abandon most of the things they valued in life Cognitive Disturbance
Difficulty in concentrating, negative thoughts, low self - esteem and self - confidence, hopelessness, self - depreciation and self - reproach, a sense of worthlessness and sinfulness, negative out look on the world and suicidal thoughts are some of the most common cognitive features accompanying the depressed person's state of feeling
Psychomotor Disturbance Psychomotor disturbances can be readily observed and even objectively measured.They include,
on the one hand, agitation (hyperactivity) and on the other, retardation (hypo activity). Although agitation,
(84)

usually accompanied by anxiety, irritability and restlessness, is a common symptom of depression, it lacks specificity. In contrast, retardation, manifesting as slowing of bodily movements, mask like facial expression, lengthening of reaction time to stimuli, increased speech paucity and at its extreme as an inability to move or to be mentally & emotionally activated (stupor) is considered a core symptom of depression.
Vegetative Symptoms
Vegetative symptoms constitute the most biologically rooted clinical features of depressive disorders and are commonly used as reliable indicators of severity (sever depression with somatic symptoms in ICD-10 and melancholia in DSM-4). They are manifested as profound disturbance in eating (anorexia and weight loss, or the reverse, bulimia and weight gain), in sleep (insomnia or hypersomnia), in sexual function (decrease sexual desire or in minority of cases the reverse), loss of vitality, motivation, energy and capacity to respond positively to pleasant events.
Disturbances of biorhythms are frequent and are considered as characteristic features of melancholia.
Anxiety Symptoms
Although anxiety symptoms are essential for the diagnosis of anxiety disorders, they are so frequently encountered in depression. In ICD-10, the admixture of anxiety and depressive symptoms is listed as a distinct category under the term "mixed anxiety and depressive disorders".
SUBTYPES OF DEPRESSIVE EPISODE
The main criteria for subtyping DE are basically quantitative. The following are subtypes, which are included in the current two major diagnostic systems.
Depression with Somatic Symptoms (Melancholia) This subtype is listed as severe depressive episode with somatic symptoms in ICD-10 and as
melancholia in DSM-4. Melancholia is the oldest diagnostic term used in psychiatry characterized by vegetative disturbances and other clinical features that indicate a profound dysfunction of neurobiological mechanisms [7.8,10,22]. The main features of this clinical entity include psychomotor retardation or agitation, late insomnia, loss of weight and appetite, Anhedonia (lack of reactivity to pleasurable stimuli), diurnal variation of mood and libido disturbances. In a recent study, in which the question of diagnostic validity of melancholic major depression was explored in a population based sample of female twins, it was concluded that it is a valid subtype of MD with distinct clinical features and a particularly higher familial liability to depressive illness (23).
Depression with Psychotic Symptoms This subtype of depression is listed as severe episode with psychotic symptoms in ICD-10 and
major depression with psychotic features (mood congruent and mood incongruent)in DSM-4.lt is also commonly cited in the literature as psychotic or delusional depression. On the basis of its presenting symptoms, it was found in the ECA study to cover 14% of all major depressions representing their most severe form [24].
Clinically this subtype is identified by the presence of delusion in conjunction with psychomotor disturbances, vegetative symptoms and occasional hallucinations. Depending on the delusional content, distinction is made between mood congruent and mood incongruent forms.
It has long been controversial issue and is still debated whether delusions and other psychotic features in depression denote a qualitatively distinct psychopathological entity or merely manifest a greater severity of the depressive disorder continuum [25].
Atypical Depression
The specifying criteria for atypical depression, according to DSM-4, are basically the reverse
(85)

vegetative-somatic symptoms most commonly encountered in typical melancholia (hypersomnia instead of insomnia, hyperphagia and weight gain instead of anorexia and weight loss), while the mood is responsive to actual or potential positive events. The symptoms have to predominate in the past recent 2 weeks of an episode of major depression. Although the validity of atypical depression has been frequently challenged in the past [26], a recent review assessing published studies on the subject and applying Kendell's criteria for clinical validity concluded that atypical depression complies with two out of six validation criteria (27).
Recurrent Brief Depression (RBD)
According to ICD-10, to make the diagnosis of RBD, depression should have occurred about once a month over the past year, and each episode should have lasted less than 2 weeks (typically 2-3 days with complete recovery), not having occurred only in relation to menstrual cycle otherwise fulfilling the symptom criteria for a mild, moderate or severe depressive episode.
It has still to be clarified whether RBD, represents a discrete form of depressive disorder or one of the clinical variations of recurrent depressive episodes.
Dysthymia according to ICD-10
Criteria
• At least 2 years of constant or constantly recurring depressed mood
• Intervening periods of normal mood rarely last for longer than a few weeks; no episode of hypomania
• None, or very few, of the individual episodes of depression within the 2 year period should be sufficiently severe or long lasting to meet the criteria for recurrent mild depressive disorder
• During at least some of the periods of depression, at least three of the symptoms listed below should be present
Symptoms
• Reduced energy or activity
• Insomnia
• Loss of self confidence and feeling of inadequacy
• Difficulty in concentrating
• Frequent tearfulness
• Loss of interest in or enjoyment of sex and other pleasurable activities
• Feeling of hopelessness or despair
• A perceived inability to cope with routine responsibilities of everybody life
• Pessimism about the future or brooding over the past
• Social withdrawal
• Reduced talkativeness
Source-[2]
OTHER DEPRESSIVE TYPES
Seasonal Depression
Seasonal depression is characterized by recurrent depressive episodes in temporal relationship with a particular period of the year (regular onset in fall or winter and offset usually in the spring). Full remission from depression (or change to mania or hypomania) in the spring or somewhat later, and the seasonal depressive episodes outnumbering the lifetime major depressive episodes without seasonal pattern are two of the qualifying criteria for inclusion in this disorder (29).
(86)

Subsyndromal Depressive Symptoms (SSD)
Neither ICD-10 nor DSM-4 make any reference to SSD as a separate subtype of depressive disorder. This entity involves a cluster of symptoms that do not differ from those of the MD but do not meet the full criteria of a depressive "case".The symptoms are fewer than formally required, are not severe enough and vary overtime. Nevertheless, although subthreshold, the symptoms have a disabling impact on the individual, seriously impairing his mental, occupational and psychosocial functioning.
Although falling short of full fledged depression, SSD are very close to the mild depressive episode of ICD-10 and to many other conditions which in the past were known as "neurotic" or "characterological" (30).
Premenstrual Syndrome (PMS)
It is still debated whether symptoms which occur during the last week of luteal phase and remit a few days after menses constitute a distinct syndrome or are either part of or superimposed on other depressive and mental disorder DSM-4 [5,10]lists the premenstrual syndrome among those that may be a focus of attention, while ICD-10 [2,3] does not attach syndromal significance to premenstrual symptoms.
Epidemiological studies yield prevalence rates of 80% for mild to moderate and 3-8% for severe premenstrual symptoms [31]. Among the many symptoms, the most frequent are depressed mood, anxiety, irritability, mood lability, tiredness, sleep and eating disturbances and difficulty in concentrating. Differential diagnosis lies mainly on symptom duration and on premenstrual history.
In a recent study, it was concluded that PMS are substantially heritable, but the associated genetic and environmental factors are not closely related to lifetime major depression (32).
Depression and Menopause
The prevalence of depressive disorders does not seem to increase during menopause [33]. However further investigation may be needed. Negative beliefs about menopause and experiencing a longer than usual menopause are associated with an increased risk of developing a depressive disorder.
Postnatal Depressive Disorder
These disorders present in three forms. The first is a transient anxiety depressive state known as postpartum blues that occurs a few days after delivery, peaks within 10 days and subsides usually within 3 weeks after delivery. About half of the mothers experience the blues in various degrees (4, 10). The second form occurs in almost 10-15% of mothers [35], as a rule within the first month after delivery. The symptoms do not essentially differ from the moderate and severe non-psychotic DE/MD. They have a disrupting and long-term effect on the personal and family life of the mother. The third as postpartum depression with psychotic features in about one out of 1000 mothers. In this form of postnatal depression, the first month after delivery is characterized, in addition to DE/MD symptomatology, by psychotic features among which are delusional thoughts, mainly concerning the newborn, in association with severe crying spells, guilt feelings, suicidal ideation and occasionally with hallucinatory experiences [5,34].
ASSOCIATION WITH AND DIFFERENTIAL DIAGNOSIS
FROM MEDICAL ILLNESS
Prevalence rates of depressive disorders among patients suffering from a medical illness vary from 22% to 33% [45], while it has been estimated that in the primary health setting the median prevalence rate for depressive disorder is more than 10% [40]. It may be difficult to distinguish a primary from a secondary depression occurring during or as a consequence of a physical disease or as a side effect of various prescribed drugs (4, 8, 9). Depression is frequently associated with or is consequent to other medical conditions (46-61)
(87)
• Depression^ Neurological Illness
1. Epilepsy
2. Post stroke
3. Parkinson's Disease
4. Multiple Sclerosis
5. Degenerative Brain Disease
6. Alzheimer's Disease
• Depression in Cardiovascular IHness
• ' Depression in Cancer
• Depression in Endocrine Disorders
1. Hypothyroidism
2. Hyperthyroidism
3. Hyper parathyroidism
4. Cushing's Syndrome
5. Addison's disease
6. Diabetes mallitus
• Medication Induced Depression
1. Reserpine
2. Withdrawal from amphatamines
3. PhenobarbitaJ
4. Steroids
And drugs with possible effects are:-
1. Alpha-methyldopa
2. Beta-blockers
3. Oral contraceptives
4. Clomiphene
5. Tamoxifene
6. Cimetidine
7. Acetazolamide.
• Drug abuse/dependence and Depression

PHARMACOTHERAPY FOR DEPRESSIVE DISORDERS Antidepressant Drugs -TCAs Antidepressant drugs -Tricyclics
TABLE-3 ANTIDEPRESSANT -TCAS
Tricyclics
Amitriptyline
Clomipramine
Dosulepin (dothiepin)
Doxepin
Indications
Depression
Nocturnal enuresis in children
Depression
Phobic and obsessional states
Adjunctive treatment of cataplexy associated with narcolepsy
Depression
Depression
Doses (elderly doses not included)
30-200 mg/day
7-1 Oyr; 10-20 mg11-16yr; 25-50 mg at night for max. 3 months
10-250 mg/day
10-150 mg/day
10-75 mg/day
75-225 mg/day
10-300 mg/day (up to 100 mg is a single dose)
Main adverse effects
Sedation, often with hangover; postural hypotension; Tachycardia/ arryhythmias; dry mouth, blurred vision, Constipation, urinary retention
As for Amitriptyline
As for Amitriptyline
As for Amitriptyline
Major interactions
SSRIs (except citalopram), phenothiazines, cimetidine -plasma levels of TCAs alcohol antimuscarinics, antipsychotics (esp. pimozide/ thioridazine) MAOIs
As for Amitriptyline
As for Amitriptyline
As for Amitriptyline
Approx. half-life (h)
9-25
18-96 active metabolite (nortriptyline)
19-37
54-77 Active metabolite (desmethyl-clomipramine)
11-40
22-60 Active metabolite (desmethyld-osulepin)
8-25
28-52 Active metabolite (desmethyl-dexopin)
(89)

Tricyclics
Imipramine
Lofepramine
Nortriptyline
Trimipramine
Indications
Depression
Nocturnal enuresis in children
Depression
Depression
Nocturnal enuresis in children
Depression
Doses (elderly doses not included)
10-200 mg/day (up to 100 mg is a single dose; up to 300 mg in hospital patients)
7 yr; 25 mg 8-11 yr; 25-50 mg >11 yr; 50-75 mg at night for maximum 3 month
140-21 Omg/ day
30-150 mg/day
7yr; 10mg 8-11 yr; 10-20 mg >11 yr; 25-35 mg at night for maximum 3 month
30-300 mg/day
Main adverse effects
As for Amitriptyline but less sedative
As for Amitriptyline but less sedative/ anticholinergic/ cardiotoxic
As for Amitriptyline but less sedative/ anticholinergic/ hypotensive Constipation may be problematic
As for Amitriptyline but more sedative
Major interactions
As for Amitriptyline
As for Amitriptyline
As for Amitriptyline
As for Amitriptyline Safer with MAOIs than other tricyclics
Approx. half-life (h)
4-18
12-24 Active metabolite (desipramine)
1.5-6
12-24 Active metabolite (desipramine)
18-96
7-23
Source-62,103
(90)

TABLE - 4 Antidepressant drugs - SSRIs
SSRI
Citalopram
Escitalo-pram
Fluoxetine
Indication
Depression treatment of the initial phase &as maintenance therapy relapse or recurrence
Panic disorder +/-agoraphobia
Depression
Panic disorder +/-agoraphobia
Depression +/- anxiety
OCD
Bulimia nervosa
Premenstrual dysphoric disorder
Doses (elderly
doses are not included) 20-60 mg/ day
10 mg for one week, increasing up to 60 mg/day
10-20mg/ day
5 mg/day for one week, increasing up to 20 mg
20 mg/day
20-60 mg/ day
60 mg/day
20 mg/day
Main adverse Effects
Nausea, vomiting, dyspepsia, abdominal pain, diarrhoea, rash, sweating, agitation, anxiety, headache, insomnia, tremor, sexual dysfunction (male & female). Discontinuation may occur.
As for citalopram
As for citalopram but insomnia and agitation more common.
Rash may occur more frequently
May alter insulin requirements
Major interactions
Not a potent inhibitor of cytochrome enzymes.
MAOIs-avoid.
Avoid-St .Johns wort
Caution with alcohol (although no interaction seen)/NSAIDs/ tryptophan/ warfarin.
As for citalopram
Inhibits CYP2D6, CYP3A4, increases plasma levels of some antipsychotics/ some benzos/ carbamazepine MAOIs - never
Avoid -selegiline / St. Johns wort
Caution - alcohol (although no interaction seen) / NSAIDs/ tryptophan/ warferin
Approx-half life (h)
33
has week metabolites
30
has week metabolites
2-3 days
4-16 days
Active metabolite
(norfluoxetine)
(91)
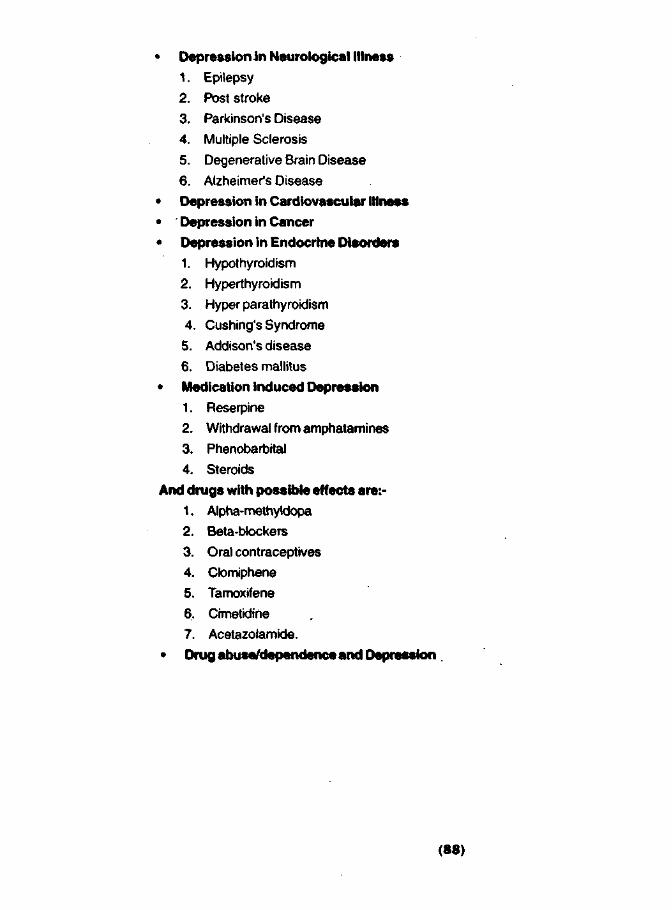
SSRI
Paroxetine
Indication
Depression +/- anxiety
OCD
Panic disorder +/-agoraphobia
Social phobia
PTSD
Generalised anxiety
Doses (elderly
doses are not included)
20-50 mg/ day
20-60 mg/ day
10-50mg/ day
20-50 mg/ day
20-50 mg/ day
20 mg/day disorder |
Main adverse Effects
As for citalopram but antimuscarinics effects and sedation more common
Extrapyramidal symptoms more common but rare. Discontinuation symptoms common -withdraw slowly
Major interactions
Potent inhibitor of CYP2D6. Increase plasma level of some antipsychotics/ tricyclics.
MAOIs - never
Avoid: St. Johns Wort.
Caution: alcohol/ lithium/
Approx-half life (h)
Source-62,103
TABLE - 5 Antidepressant drugs - MAOIs
MAOl
Isocarbox-azid
Indication
Depression
Doses (elderly
doses are not included)
30 mg/day in single or divided doses, increased after 4 weeks to max. 60 mg/day for 4-6 weeks
10-40 mg/ day maintenance
Main adverse effects
Postural hypotension, dizziness, drowsiness, insomnia, headaches,
Adverse effects,
Nervousness, paraesthesia, weight gain, hypertensive crisis
Major interactions
Tyramine in food, sympathomimetics, alcohol, opioids, levadopa, 5HT, agonists
Approx half-life (h)
36
(92)

MAOI
Phenelzine
Tranylcypr-omin
Moclobemide
(Reversible inhibitor of MAO-A)
Indication
Depression
Depression
Depression
Social phobia
Doses (elderly
doses are not included)
15 mg tds -qid (hospital patient: max. 30 mg tds) consider reducing to lowest possible maintenance dose
10mgbd
Doses > 30 mg/day under close supervision only
Usual maintenance: 10 mg/day
Last dose no later then 3 pm
150-600 mg/day
bd after food
300-600 mg/day
bd after food
last dose no later then 3 pm
Main adverse effects
As for Isocarboxazid but more postural hypotension, less hepatotoxicity
As for Isocarboxazid but insomnia, nervousness, hypertensive crisis more common than with other MAOIs; hepatotoxicity less common
Mild dependence as amphetamine - like Structure
Sleep disturbances, nausea, agitation, confusion
Hypertension reported may be related to tyramine ingestion
Major interactions
As for Isocarboxazid.
Probably safest of MAOIs and is the one that should be used if combinations are considered
As for Isocarboxazid but interactions more severe. Never use in combination therapy with other antidepressants
Tyramine interaction rare and mild but possible if high doses(>600 mg/day) used or if large quantities of tyramine ingested CNS excitation/depression with dextromethorphan/ pethidine Avoid: C l o m i p r a m i n e / levadopa/ selegiline/ sympathomimetics/ SSRIs Caution with: Fentanyl/ morphine/ tricyclics Cimetidine-use half dose of moclobemide
Approx half-life (h)
1.5
2.5
2-4
(93)

TABLE - 6 Antidepressant drugs - others
Antidepressant
Mianserin
Mirtazapine
Nefazodone (now withdrawn in many countries)
Indication
Depression
Depression
Depression including depressive syndromes associated with anxiety or sleep disturbances
Doses (elderly doses are not included)
30-90 mg daily
15-45 mg daily •
100-300 mg/day
Main adverse effects
Sedation, rash; rarely; blood discresias, jaundice, arthralgia
No anticholinergic effects
Sexual dysfunction uncommon
Low cardio toxicity
Increased appetite, weight gain, drowsiness, oedema, dizziness, dizziness, headache, blood discresias
Nausea / Sexual dysfunction are relatively uncommon
Dizziness, postural hypotension, somnolence, nausea/ sexual dysfunction are relatively uncommon
Major interactions
Other sedative, alcohol
MAOIs; avoid
Effect on hepatic enzymes unclear, so caution is required
Minimal effect on CYPD6 / IA2 / 3A
Caution: alcohol/ sedative
Potent inhibitor of CYP3A4. increases plasma levels of some benzos/ buspirone / carbamazepine/ c i c l o a p o r i n / digoxin/ terfenadine
Avoid : MAOIs/ p i m o z i d e / s i b u t r a m i n e / s i m v a s t a t i o n Fluxetine increases plasme levels of mCPP (anxiogenic metoblite). Caution: alcohol (although no interaction seen).
Approx half life(h)
10-20
2-desmethyl mianserinis major metabolite (? active)
20-40
25
active metabolite (demethyl Mirtazapine)
2-4 (dose-dependent)
active metabolites:
2-4 (hydroxyn-efazodone)
18-33 (desthyl hydroxy)
4-9(mCPP: minor)
(94)

Antidepressant
Reboxe-tine
Trazodone
Venlafax-ine
Indication
Depression - acute and maintenance
Depression +/- anxiety
Anxiety
Depression +/- anxiety and prevention of replace or recurrence of depression
Generalised anxiety disorder (XL prep only)
Doses (elderly doses are not included)
4-6 mg by day
150-300 mg/day (up to 600 mg/ day in hospitalized patients)
By day dosing above 300 mg/day
75-300 mg/ day
75-375 mg/ day(bd) with food 75-225 mg XL/day (od) with food
75 mg XL/ day (discontinue if no response after 8 weeks)
Main adverse effects
Insomnia, sweating, dizziness, dry mouth, constipation, tachycardia, urinary hesitancy
Erectile dysfunction may occur rarely
Sedation, dizziness, headache, nausea, vomiting, tremor postural, hypotension, tachycardia, priapism. Not anticholinergic, less cardiotoxicthan tricyclics
Nausea, insomnia, dry mouth, somnolence, dizziness, sweating, nervousness, headache,sexual dysfunction
Elevation of blood Pressure at higher doses. Discontinuation symptoms common -withdraw slowly
Major interactions
Metabolized by CUP3A4-avoid drugs inhibiting this enzyme (e.g. erythromycin/ Nefazodone/ ketoconazole). Minimal effect on CYPD6/3A4. MAOIs: avoid No interaction with alcohol
Caution: Sedatives / alcohol/ other antidepressants/ digoxin/phenytoin MAOIs: avoid
Metabolized by CYP2D6/3A4 -Caution with drugs known to inhibit both isozymes. Minimal effects on CTP2D6. No effect on CYPIA2/2C9/ 3A4. MAOIs: avoid Caution: alcohol (although no interaction seen)/ cimetidine/ clozapine/warferin
Approx half life(h)
13
5-13 (biphasic)
4-9 Active metabolite (mCPP)
5
11
Active metabolite (O-desmethyl venlafaxine)
Source-62,103
(95)

PSYCHOTHERAPIES FOR DEPRESSIVE DISORDERS -
"Psychotherapy" has different objectives, including improved adherence to medication, symptom reduction or attainment of symptom remission, reduction of disability, prevention of relapses /recurrence or prevention or delay of the onset /progression of depressive condition.
Psychoeducation may be seen as a more extensive /intensive effort at providing information about the longer term management, including more about the benefits and side-effects of treatment option problem solving therapy may be viewed as an extension of clinical management.
Formal psychotherapies may also be used to reduce symptoms or restore function. Therapies designed to reduce symptoms acutely, include interpersonal, cognitive, behavioral, marital and brief psychodynamic therapy.
Finally whether or not full symptom remission and function restoration is accomplished, psychotherapy may also aim at prophylaxis. There is growing evidence that continuation /maintenance phase therapy may help to delay relapses /recurrences. In sum the aims and types of therapy change during the course of managing depression (63,64).
There are a range of psychosocial interventions that may be useful in the acute treatment of major depressive disorder. In practice, psychiatrists use a combination or synthesis of various approaches and strategies; these in turn are determined by and individually tailored to each patient on the basis of that person's particular condition and coping capacities.
1 . Clinical Management/Psychoeducation
The education concerning major depressive disorder and its treatment should be provided to all patients. When appropriate, education should also be provided to involved family members. Largely consistent evidence indicates that educating patient about the nature of illness, treatment options, medication side effects and expected outcome increases knowledge, improves attitude and enhances medication adherence. (65,66)
Psychoeducation may be used to encourage healthy life styles, to enhance coping strategies, and to address psychosocial difficulties associated with the illness (67).
2. Interpersonal Therapy (IPT) - Interpersonal therapy focuses on losses, role disputes and transitions, social isolation, deficits in social skills, and other interpersonal factor that may impact on the development of depression. Interpersonal therapy attempts to intervene by facilitating mourning and promoting recognition of related affects, resolving role disputes and transitions, and overcoming deficits in social skills to permit the acquisition of social supports (68, 69)
In one trial conducted among depressed psychiatric patients, interpersonal therapy was found to be superior to nonscheduled controls and comparable to other active treatments, including cognitive therapy or antidepressant medication (68). In a subsequent study among depressed HIV positive patients, greater improvements were observed after interpersonal therapy plus imipramine than supportive psychotherapy or cognitive behavioral therapy (70). Conversely, interpersonal therapy has been proposed to be more effective than cognitive therapy for patients with major depressive disorder with obsessive personality traits and for patients who are single and noncohabitating (71).
3. Cognitive Therapy (CT) - CBT is classically a time limited (16-20 Sessions, 12-16 weeks) directive therapy designed to reduce symptom by countering patient's negative view of self, world and future and to prevent or delay relapses/recurrence by changing schemas or beleifs (72). Cognitive behavioral therapy maintains that irrational beliefs and distorted attitudes towards the self, the environment, and the future perpetuate depressive affects. The goal of cognitive behavioral therapy is to reduce depressive symptoms by challenging and reversing these beliefs and attitudes (73).
(96)

The cognitive behavioral therapy has been extensively studied in trials. Several meta-analytic studies have quantified the efficacy ofcognitive behavioral therapy. For example, some metaanalyses have concluded that effect sizes for cognitive behavioral therapy are larger than for pharmacotherapy (74, 68), whereas others suggest they are equally effective (75). Effect sizes for cognitive behavioral therapy have generally been at least as large as, and in some cases larger than, for other forms of psychotherapy such as behavior therapy, interpersonal therapy, brief dynamic psychotherapy (68).
There have been suggestions on the basis of individual clinical trials that the efficacy of cognitive behavioral therapy may differ on the basis of the severity of major depressive disorder.
4. Behavioral Therapy (BT) - Behavior therapy of major depressive disorder is based on theoretical models drawn from behavior theory (76) and social learning theory (77). Specific behavior the'rapy techniques includes activity scheduling (78), self control therapy (79), social skills training (80), and problem solving (81). BT aims to elevate mood by ameliorating the covarying target responses or by changing the low rate of response contingent to positive reinforcement.
Although the efficacy of behavior therapy has been examined in a substantial number of trials the results of individual clinical trials have suggested that behavior therapy may be superior in efficacy to brief dynamic psychotherapy (82) and generally comparable in efficacy to cognitive therapy (83) or pharmacotherapy (84).
Clinical trial data found that response to behavior therapy may be more likely in patients with less initial severity of major depressive disorder symptoms.
5. Marital Therapy (MT) - Marital and family problems are common in the course of mood disorders. Comprehensive treatment often demands that these problems be assessed and addressed. According to Jacobson et al (85) marital therapy is effective for depression because of several reasons. Depression and marital satisfaction are inversely related (86), disruptions in close relationship often precipitate depression (87,101) and marital distress often predicts depressive relapse following recovery (88).
Marital therapy conceptualizes depression as an interpersonal context such that both members of the marital dyad are included in therapy.Treatment includes 20 sessions focused on behavioral exchange and then move on to training in communication and problem solving (89,90). In the later, couples are taught to resolve conflict around issues such as financial, sex, affection, parenting, and intimacy. The techniques are both cognitive and behavioral in nature.
6. Brief Psychodynamic Psychotherapy (BPD) - The term "psychodynamic psychotherapy" encompasses a number of psychotherapeutic interventions, share a basis in psychodynamic theories regarding the etiologic nature of psychological vulnerability, personality development, and symptom formation as shaped by development deficit and conflict occurring during the life cycle from earliest childhood forward. Some of these theories focus predominantly on conflicts related to guilt, shame, interpersonal relationships, the management of anxiety, and repressed or unacceptable impulses. Others are more focused on developmental psychological deficits produced by inadequacies or problems in the relationship between the child and emotional caretakers, resulting in problems of self-esteem and a sense of psychological cohesiveness (91,92).
Psychodynamic psychotherapy is most often of longer-term duration than other psychotherapies and is usually associated with goals beyond that of immediate symptom relief. These goals are usually associated with an attempt to modify the underlying psychological conflicts and deficits that increase the patient's vulnerability to major depression. The premise of brief psychodynamic psychotherapy is that depressive symptoms remit as patient learns new methods to cope with inner conflicts. Several different approaches to BPD include those of Malan (94), Mann (95), and Wolberg (96). Specific treatment manuals have been developed (97,98).
(97)

Result of two meta-analyses suggest that brief psychodynamic psychotherapy for the treatment of major depressive disorder is more effective than a waiting list control condition but probably less effective than other forms of psychotherapy (93,68).
ORGANIZATION OFTHESE GUIDELINES
These practice guidelines are important tool for clinicians in the management of major depressive disorder and its associated conditions.
The recommendations are based on the best available data and expert clinical consensus from following sources:
1. Recommendation of Expert group of IPS at National workshop on CPG for psychiatrists in India (July 2004 at Jaipur).
2. American Psychiatric Association: Practice guidelines for the treatment of patient with depression. (102)
3. The Moudsley's and The South London and Moudsley NHS Trust's 2003 Prescribing guidelines. (103)
4. WPA Series evidence and experience in Psychiatry: Depressive Disorders 2nd Edition (104)
5. National Institute for clinical Excellence (NICE): Depression Guidelines (105)
6. Texas Medication Algorithm Project (TMAP): Depression Algorithm.(106)
7. Available Indian Literature Published in Indian Journals (107,108,109,110,111)
CLINICAL PRACTICE GUIDELINES — RECOMMENDATIONS
1. Goals - The successful treatment of patient with major depressive disorder is promoted by an initial thorough assessment of the patient. Treatment then consists of an acute phase lasting a minimum of 6-12 weeks, during which remission is induced. Remission is defined as a return to the patient's baseline level of the symptom severity and functioning and should not be confused with substantial but incomplete improvement. After achieving remission, the patient enters the continuation phase, which usually lasts for 16-24 weeks, during which time the remission is preserved and relapse is prevented. Relapse is generally defined as the reemergence of significant depressive symptoms or dysfunction following a remission. Patients who successfully complete the continuation phase with out relapse then enter the maintenance phase of treatment.The goal during the maintenance phase is to protect susceptible patients against recurrence of subsequent major depressive episodes; the duration of the maintenance phase will vary depending on the frequency and severity of prior major depressive episodes
Psychiatrists initiating treatment of an episode of major depressive disorder have at their disposal a number of medications, a variety of psychotherapeutic approaches, ECT, and other treatment modalities (e.g. light therapy).These various interventions may be used alone or in combination (102)
2. Management of Acute phase
General principles -
• Assessment &Diagnosis -
Patient with major depressive disorder should receive a thorough diagnostic evaluation both to determine the diagnosis of depression and to reveal the presence of other psychiatric or physical conditions. The assessment should include a history of present illness and current symptoms, psychiatric history, treatment history, responses to previous treatment, general medical history, history of substance use, personal history, social and occupational history, mental status examination and physical medical examination with diagnostic tests. Efforts should be made to obtain information from all sources, particularly family and friends. Investigations such as drug screens, thyroid tests neuro
(98)

immaging can be used as and when required.
A diagnosis of depression should be made according to structured diagnostic criteria keeping in mind the various conditions mimicking depression. Standardized rating scales are reliable and accurate ways of assessing severity of depression. Such instruments e.g. Hamilton Rating Scale for Depression (HDRS), Montgomery-Asberg Depression Rating Scale (MADRAS), Beck Depression Inventory (BDI) Etc. (112,113,114,115) should be used wherever necessary and possible.
Safety -
A careful assessment of patient's risk for suicide is important. An assessment of presence of suicidal ideation is essential, including the degree to which the patient has made plans for or begins to prepare for suicide. The availability of means for suicide and lethality of those means should be inquired. The clinical factors like presence of psychotic features, command hallucination, severe anxiety, alcohol or substance abuse may increase the likely hood of patient acting on suicidal ideation. Patients who are found to possess suicidal or homicidal ideation, and or intention require close monitoring. Measures such as hospitalization (involuntarily when indicated) should be considered for those at risk. Various standardized rating scales may be used for evaluation of risk.
Assessment of Functional Impairments -
Major depressive disorder is frequently associated with functional impairments such as deficits in interpersonal relationships, work, living conditions and other medical and health related needs. After careful assessment of impairments by psychiatrists, patient should be encouraged to set realistic, attainable goals for themselves in term of desirable functioning.
• Treatment settings
The psychiatrists should chose an appropriate site of treatment after evaluating the patient's clinical condition, including symptom severity, comorbidity, suicidality, homicidality, level of functioning, and available support system. Patient with suicidal or homicidal ideation, requires a close monitoring and hospitalization. If patients refuse, they can be hospitalized involuntarily as per law. Severally ill patients who lack adequate social support outside a hospital setting should be considered for admission to a hospital. Additionally, those patients who also have complicating psychiatric or general medical conditions or who have not responded adequately to outpatient treatment may need to be hospitalized.
• Therapeutic alliance
Irrespectively of the treatment modalities selected for patients, it is important for the psychiatrist to establish a therapeutic alliance with the patient. A strong treatment alliance between patient and psychiatrist is crucial for poorly motivated, pessimistic depressed patient who remained hyper sensitive to side effect of drugs. A positive therapeutic alliance always generate hope for good outcome.
• Enhanced treatment compliance
The successful treatment of major depressive disorder requires strict compliance to treatment plans. Patients with major depressive disorder may be poorly motivated, unduly pessimistic over their chances of recovery with treatment. In edition, the side effect or requirements of treatment may lead to non-adherence. Psychiatrist should recognize these possibilities, encourage the patient to articulate any concerned regarding adherence and emphasize the importance of adherence for successful treatment. A message to patients that have been shown to improve compliance include emphasizing: -
• When and how often to take medicines
• The need for at least 2-4 weeks before beneficial effects may be noticed
• The need to take medication even after feeling better
(99)

• Explanation of side effects, if seeking by patients
• The need to consult with psychiatrist before discontinuing medications
• What to do if problems or questions arise.
• Reporting of a new symptoms arise.
• Watch early signs of relapse
Given the chronic, episodic nature of major depressive disorder, exacerbations are common. Patients as well as their families if appropriate, should be instructed about the significant risk of relapse. They should be educated to identify early signs and symptoms of new episodes.
Treatment of Acute phase
In acute phase psychiatrist may choose between several initial treatment modalities, including pharmacotherapy, psychotherapy, the combination of medication and psychotherapy, or ECT. Selection of an initial treatment modality should be influenced by both clinical (e.g. severity of symptoms) and other factors (e.g. patient preference)
- Pharmacotherapy
• Antidepressant drugs
Antidepressant medication shall be used as initial treatment modality by patients with mild, moderate, or severe major depressive disorder. Clinical features that may suggest that medication are the preferred treatment modality include history of prior positive response to antidepressant medication, severity of symptoms, significant sleep and appetite disturbance or agitation, or anticipation of the need for maintenance therapy. Patients with major depressive disorder with psychotic features require either the combined use of antidepressant and antipsychotic medication or ECT.
• Choice of antidepressant drugs
Antidepressant medications that have been shown to be effective are listed in table 3,4,5 & 6. The effectiveness of antidepressant medication is generally comparable between classes and within classes of medication. Therefore, the initial selection of an antidepressant medication will largely be based on the anticipated side effects, the safety or tolerability of these side effects for individual patients, patient preference, quantity and quality of clinical trial data regarding the medication. On the basis of these considerations, the following medication is likely to be optimal agents for most patients: SSRIs, TCAs Mirtazepine, bupropion, and vanlafaxine. Additional considerations that may influence include a history of prior response to a medication and the presence of comorbid psychiatric or general medical conditions. For example, secondary amine tricyclic antidepressant medication Imipramine, Amitriptyline Etc. may not be optimal in patients with cardiovascular conditions, cardiac conduction defects, closed angle glaucoma, urinary retention, or significant prostatic hypertrophy. SSRIs carry a risk of sexual side effects and may be more expensive. Similarly, the specific side effect profiles and higher costs should be considered in decisions regarding use of antidepressant medication.
Dose and duration of antidepressants
Once an antidepressant medication has been selected, it can be started at doses suggested in table (3,4,5,6) Patient who have started taking an antidepressant medication should be carefully monitored to assess the response to pharmacotherapy as well as the emergence of side effects, clinical conditions, and safety. Factors to consider when determining the frequency of monitoring include severity of illness, patients co-operation with treatment, the availability of social support, the presence of comorbid general medical problems. Visit should also be frequent enough to monitor and address suicidality and to promote treatment adherence. Improvement with pharmacotherapy can be observed after 4-8 weeks of treatment. If at least a moderate improvement is not observed in this time period, reappraisal and adjustment of the pharmacotherapy should be considered.
(100)

• Failure to response
If at least moderate improvement is not observed following 6-8 week of pharmacotherapy, a reappraisal of the treatment regimen should be conducted. Following any change in treatment, the patient should continue to be closely monitored. If there is not at least a moderate improvement in major depressive disorder symptoms after an additional 6-8 weeks of treatment, the psychiatrist should conduct another thorough review. An algorithm depicting the sequence of subsequent steps that can be taken for the patients who fail to respond fully to treatment provided is given below.
Psychotherapy
A specific, effective psychotherapy may be considered as an initial treatment modality for patients with mild to moderate major depressive disorder. Clinical features that may suggest the use of a specific psychotherapy include the presence of significant psychosocial stressors, intrapsychic conflict, interpersonal difficulties. Patients preference for psychotherapeutic approaches is an important factor that should be considered in the decision to use psychotherapy as the initial treatment modality. Pregnancy, lactation, or the wish to become pregnant may also be an indication for psychotherapy as an initial treatment.
Choice of specific psychotherapy
Cognitive behavioral therapy and interpersonal therapy are the psychotherapeutic approaches that have the best documented efficacy in the literature for the specific treatment of major depressive disorder (69,72,74). When psychodynamic psychotherapy is used as specific treatment, in addition to symptom relief, it is frequently with broader long term goals. Patient preference and availability of clinicians with appropriate training and expertise in the specific approach are also factors in the choice of particular form of psychotherapy
Implementation
The psychiatrist should take into account multiple factors when determining the frequency for individual patients, including the specific type and goals of psychotherapy, the frequency necessary to create and maintain a therapeutic relationship, the frequency of visits required to ensure treatment adherence, and the frequency necessary to monitor and address suicidality. The frequency of out patient visits during the acute phase generally varies from once a week in routine cases to as often as several times a week. Regardless of the type of psychotherapy selected, the patient's response to treatment should be carefully monitored. For a given patient time spent and frequency of visit should be decided by the psychiatrist.
Failure to respond
If after 4-8 weeks of treatment, if a moderate improvement is not observed, then a thorough review and reappraisal of the diagnosis, complicating conditions and issues, and treatment plan should be conducted. The treatment plan can be revised by the addition or substitution of pharmacotherapy. Following any revision or refinement of treatment, the patient should continue to be closely monitored. Even if there is not a sign of moderate improvement in major depressive disorder symptoms after an additional 4-8 weeks of treatment, another thorough review and revision of therapy should be conducted.
Combination of pharmacotherapy and Psychotherapy
There is class of patients who require the combination therapy. In general, the same issues that influence the choice of medication or psychotherapy when used alone should be considered when choosing treatments for patients receiving combined therapy. Patients receiving combined therapy should also be monitored closely for treatment effect, side effects, clinical condition, and safety. If after 4-8 weeks there is not at least a moderate improvement, a thorough review should be conducted. After an additional 4-8 weeks trial, if a moderate improvement is not there, then a another thorough
(101)

review should be conducted.
Assessment of Response
The goal of acute phase treatment is to return patients to their baselines level of symptomatic and functional status. Many times patients have incomplete response in term of symptoms reduction or improvement in functioning during acute phase treatment. It is advisable not to conclude the acute phase treatment in such patients and a change in treatment should be considered.
3. Treatment in Continuation phase
Patients who have been treated with antidepressants in acute phase should be maintained on same dose of these agents for 16-24 weeks to prevent relapse(total period of 6-9 month from initiation of treatment).
• There are evidences to support the use of specific psychotherapy in continuation phase to prevent relapse.
• The use of other somatic modelaties (e.g. ECT) may be useful in patients where pharmacology and/or psychotherapy have failed to maintain stability in continuation phase.
• The frequency of visit must be determined by patient's clinical condition as well as the specific treatment being provided.
4. Treatment in maintenance phase
On average, 50-85%of patients with a single episode of major depression have at least one more episodes. Therefore maintenance phase treatment should be considered to prevent recurrence.
• The duration of treatment should be decided keeping in view the previous treatment history and number of depressive episodes the person has had in the past.
• Mostly the treatment that was effective for Acute and continuation phase should be used in the maintenance phase.
• Antidepressants doses should be employed in same dose to which the patient had responded in previous phase.
• The frequency of visit for cognitive behavior therapy and interpersonal therapy decreases in maintenance phase (once a month).
5. Discontinuation of treatment
• The decision to discontinue maintenance treatment should include consideration on following facto rs:-
• Probability of recurrence
• The frequency and severity of past episodes
• Persistence of depressive symptoms after recovery
• The presence of comorbid disorders
• Patient's preference
• Explanation of discontinuation syndrome
• The manner in which the discontinuation of psychotherapeutic treatment in maintenance phase is done should be individualized to the patient's need and will depend on the type of psychotherapy, duration, and intensity of treatment.
• When the decision is made to discontinue maintenance pharmacotherapy, it is best to taper the medication over several weeks. Such tapering may allow for the detection of emerging symptoms or recurrence.
(102)
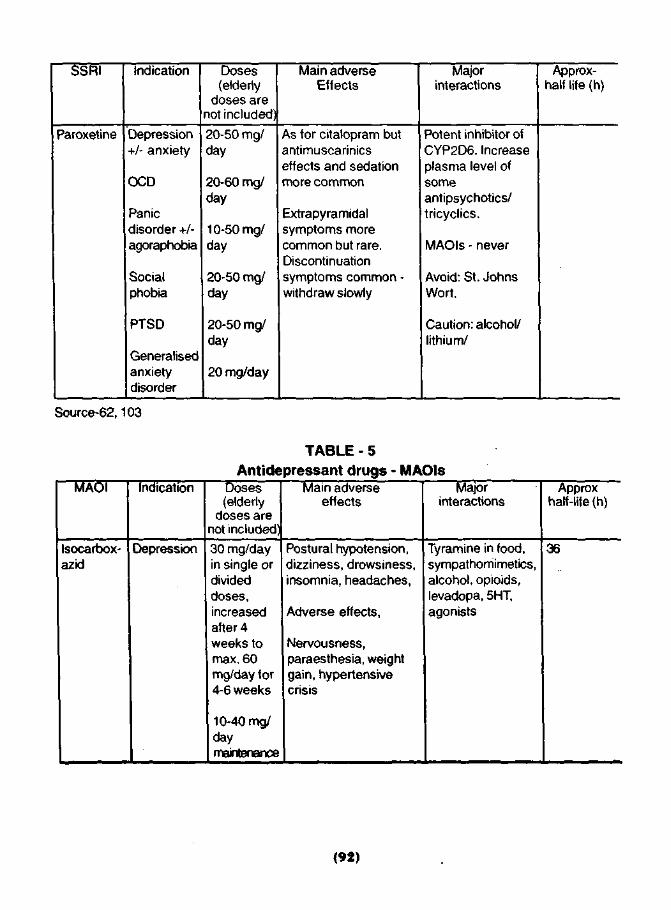
• After the discontinuation of active treatment, patient should be reminded of potential for a depressive relapse and should continue to be monitor over the next several months to identify in whom a relapse has occurred. If a patient suffers a relapse upon discontinuation of medication, treatment should be promptly reinitiated.
ROLE OFYOGA IN DEPRESSION
The studies related to role of traditional therapies like Meditation, Yoga and other techniques have been mostly published in documents of various organizations propagating that particular technique. Well designed scientific studies to authenticate these claims need to be conducted, however efficacy of these techniques as supportive therapy is widely accepted.
ALGORITHM FOR DRUG TREATMENT OF DEPRESSION
Discuss choice of the drug with the patient Include: theraputic effects, Adverse effects,
Discontinuation effects
V Start antidepressant
Titrate to recognised theraputic dose. Assess efficacy over 4-6 weeks
No Effect f Effective Poorly Tolerated 1 Increase dose Assess over a further2 weeks
No Effect >
Effective
Continue for 4-6 months at full treatment dose Cons ide r l o n g e r - t e r m treatment in recurrent
Effective
,
Effective
Pc or
Give an antidepressant from a different class Titrate to theraputic dose. Assess over 4-6 weeks
•orly Tolerated No Effect , '
Give an antidepressant from a different class Titrate to theraputic dose.
Assess over 4-6 weeks, increase dose as necessary
No Effect
< v >
Refer to suggested treatments for refractory depression
(103)
MANAGEMENT OF SPECIAL CONDITIONS
A. Treatment-Resistant Depression
Initial treatment with antidepressant medication fails to achieve a satisfactory response in approximately 20%-30% of patients with major depressive disorder; in some cases the apparent lack of treatment response is actually a result of faulty diagnosis, inadequate treatment, or failure to appreciate and remedy coexisting general medical and psychiatric disorders or other complicating psychosocial factors (116). Adequate treatment for at least 6-8 weeks is necessary before concluding that a patient is not responsive to a particular medication (117). Some clinicians require two successive trials of medications of different categories for adequate duration before they consider a patient treatment resistant.
Review of diagnosis
First step in care of a patient who has not responded to medication should be a thorough review and reappraisal of the psychosocial and biological information base, aimed at revarifying the diagnosis and identifying any neglected and possibly contributing factors, including the general medical problems^ alcohol or substance abuse or dependence, other psychiatric disorders, and general psychosocial issues impeding recovery.
Addition of an adjunct to an antidepressant
Lithium is the drug primarily used as an adjunct; other agents in use are thyroid hormone and stimulants. Opinion differs as to the relative benefits of lithium and thyroid supplementation. It is reported that lithium is useful in over 50% of antidepressant nonresponders and is usually well tolerated (118). The interval before full response to adjunctive lithium is said to be in the range of several days to 3 weeks. If effective and well tolerated, lithium should be continued for the duration of treatment of the acute episode. Thyroid hormone supplementation, even in euthyroid patients, may also increase the effectiveness of antidepressant treatment (119). The dose proposed for this purpose is 25 mg/day of triidothyronine increased to 50 mg/day in a week.
Simultaneous use of multiple antidepressants
Depression is a chronic disabling condition in case patient does not respond to single drug regimen, clinicians may use combination/polytherapy with close monitoring of side effects and drug interaction profile.
Combinations of antidepressant carry a risk of adverse interaction and sometimes require dose adjustments. A selective serotonin-reuptake inhibitor in combination with tricyclic agents has been reported to induce a particularly rapid antidepressant response (120). However, Fluoxetine added to tricyclic antidepressant causes an increased blood level and delayed elimination of the tricyclic drug, predisposing the patient to tricyclic drug toxicity unless the dose of the tricyclic is reduced (121). Another strategy combined use of a tricyclic antidepressant and a MAO inhibitor, a combination that is sometimes effective in alleviating severe medication-resistant depression, but the risk of toxic interactions necessitates careful monitoring. Reaction is sometime referred to as the "serotonin syndrome" with the hazards of so doing, should carefully weigh the relative risks and benefits (122,123).
Electroconvu Isive therapy
ECT has the as good response rate like any form of antidepressant treatment and should be considered in virtually all cases of moderate or severe major depression not responsive to pharmacologic intervention. ECT is considered safer. Approximately 50% of medication resistant patients exhibit a satisfactory response to ECT (124). Lithium should be discontinued before initiation of ECT, as it has been reported to prolong postictal delirium and delay recovery from neuromuscular blockade (125).
(104)

ALGORITHM FOR ARRIVING AT DIAGNOSIS OF RESISTANT DEPRESSION
DEPRESSION NO RESPONSE TO TREATMENT
5*> REVIEW DIAGNOSIS AS PER ICD10/DSMIV ^
CORRECTTHE DIAGNOSIS AND TREAT ACCORDINGLY
sz. HAS PATIENT
RECEIVED ADEQUETE DOSAGE AND/FOR
SUFFICIENT DURATION?
^ IS COMPLIENCE
PROPER? ARE SIDE EFFECTS NOT
INTERFERRINGWITH TREATMENT
Sz. RULE OUT ORGANIC CAUSES, RULE OUT
ANY OTHER COMORBIDITY
} RESISTANT DEPRESSION
(105)

ALGORITHMS FOR TREATMENT OF RESISTANT DEPRESSION
RESISTANT DEPRESSION
X Z Augmentation with Lithium/Thyroid / Buspirone
Response : >
Partial or No Response
^Z Combination Antidepressants (TCA + SSRI) or (Bupropion + SSRI)
Response : >
Partial or No Response
iz ECT Response
>
Partial or No Response
iz Other e.g. Lamotrigine, fluvoxamine, Mirtazipine + Bupropion), Olanzapine etc. (Provide Rationale)
>
Continuation Phase
V Maintenance Phase
When Indicated
Response 0
(106)

B. Patients with suicidal risk
Patients with major depression are at increased risk for suicide. Suicide risk should be assessed initially and over the course of treatment. If the patient has suicidal ideation, intention, and/or a plan, close surveillance is necessary. Factors to be considered in determining the nature and intensity of treatment include (but are not limited to) the nature of the doctor patient alliance, the availability and adequacy of social supports, access to and lethality of suicide means, and past history of suicidal behavior. The risk of suicide in some patients recovering from depression increases transiently as they develop the energy and capacity to act on self destructive plans made earlier in the course of their illness. However, it is not possible to predict with certainly whether a given patient will kill himself or herself. Therefore, even with the best possible care, a small proportion (15%) of depressed patients are likely to die by suicide. A careful selection of antidepressants and ECT is an important decision to be taken by psychiatrist after considering all related factors.The suicidal ideation of patient should be informed to family members and they should be instructed for various safety measures to be taken. The prescribed drugs should not be in the possession or reach of patient having suicidal intention.The reported frequency of overdose with SSRIs is small compared to that associated with TCAs(127).The TCAs generally have fatality index because of their narrow theraputic window and greater toxicity in overdose (126). It has been reported that addition of lithium is useful for long term prevention of suicide because of it's antisuicidal properties.
C. Recurrent depression
Depression is often a recurrent disorder. Of those patients who have one episode of major depression, 50-85% will go on to have a second episode and 80-90% of those who have second episode will go on to have third (128). Patients who have sustained repetitive bouts of major depression should be carefully considered for maintenance therapy after the remediation of the current episode. When deciding on course of treatment for individuals who have been treated for prior episodes, the psychiatrist should carefully ascertain the degree of response to and tolerance of the prior treatment modalities. Patients should know the following key points: • A single episode of depression should be treated for 6 month after recovery. • The risk of recurrence of depressive illness is high and increases with each episode. • Those who have had a multiple episodes may require treatment for many years. • The chances of staying well are greatly increased by taking antidepressants. • Antidepressants are:
• effective • not addictive • most do not lose their efficacy over time
D. Depression with psychotic features
Depression with psychotic features carries a higher risk of suicide than does major depression uncomplicated by psychosis. It also constitutes a risk factor for recurrent depression. Depression with psychotic features responds better to treatment with a combination of antidepressants and antipsychotics than to treatment with either component alone (129). ECT is highly effective in depression with psychotic features, a first line treatment for this disorder (132). There are fewer studies on use of newer antidepressants and atypical antipsychotics either alone or in combination, and reports a 56% response rate with combined olanzapine and fluoxetine (130). Amoxapine, is a TCA that also has an antipsychotic like effect (131), and advocated by some. Lithium augmentation is helpful in some case refractory to combined antidepressant antipychotic treatment.
E. Depression with atypical features
Atypical depressive feature include severe anxiety, vegetative symptoms of reserved polarity
(107)

(i.e., increased rather than decreased sleep, appetite, and weight), marked mood reactivity, sensitivity to emotional rejection, phobic symptoms, and a sense of severe fatigue that creates a sensation of "leaden paralysis" or extreme heaviness of the arms or legs (133). In some patients symptoms of anxiety predominate, while others have predominantly vegetative symptoms. There is some overlap between patients with atypical depression and patient with anergic bipolar depression. Tricyclic antidepressants yield response rates of only 35%-50%. MAO inhibitors response rates of 55%-75% in patients with atypical depression. If it is determined that the patient does not wish to, cannot, or is unlikely to adhere to the dietary and drug precautions associated with MAO inhibitor treatment, the use of an alternative antidepressant is indicated. The results of several studies suggest that SSRIs, MAOIs, and possibly bupropion maybe more effective treatment for Atypical depression (134,135).
F. Alcohol and/or substance abuse or dependence
Because of the frequent comorbidity of depression and alcohol or other substance abuse, the psychiatrist should make every effort to obtain a detailed history of the patient's substance use. If the patient is found to have a substance use disorder, a program to secure abstinence should be regarded as a principle priority in the treatment. A patient suffering from major depression with comorbid addiction is more likely to attempt suicide, and less likely to comply with treatment than is a patient with depression of similar severity not complicated by this factor. Some alcohol-and/or substance-abusing patients reduce their consumption of these substance upon remediation of an underlying depressive disorder, making the recognition and treatment of depression doubly important for such individuals. It is also advisable, if other factors permit, to detoxify such a patient before initiating antidepressant therapy. Identifying which patient should be started on a regimen of antidepressant therapy earlier, is difficult. A positive family history of depression, a history of depression preceding alcohol or other substance abuse, or a history of major depression during periods of sobriety raises the likelihood that the patient would benefit from antidepressant treatment.
Benzodiazepines and other sedative hypnotics carry the potential for abuse or dependence and should be used cautiously except as part of a detoxification regimen. Hepatic dysfunction and hepatic enzyme induction frequently complicate pharmacotherapy of patients with alcoholism and other substance abuse; these conditions require careful monitoring of blood levels. SSRI & Bupropion are preferred drugs for treatment of Atypical Depression.
G. Depression with features of obsessive-compulsive disorder
Obsessive-compulsive symptoms are also common in patients of Major Depressive episodes. Clomipramine and the selective serotonin reuptake blockers have demonstrated efficacy in the management of obsessive-compulsive symptoms in addition to their antidepressants efficacy (136,137)
H. Depression with panic and/or other anxiety disorders
Panic disorder complicates major depression in 15%-30% of the cases (138). Individual with symptom of both disorder manifest greater degrees of impairment than do patients with major depression only. Imipramine has been shown to be effective in this context. Tricyclic antidepressants and selective serotonin reuptake inhibitors may initially worsen rather than alleviate anxiety and panic symptoms; these medications should therefore be introduced at a low dose and slowly increased when used to treat such patients. However the efficacy of high potency benzodiazepine like alprazolam & clonazepam may sometimes be used with benefit either in combination with antidepressants or as the sole pharmacological agent for anxiety, with or without panic, coupled with milder forms of depressions.
I. Depression with cognitive dysfunction (pseudo dementia)
Signs and symptoms of cognitive inefficiency routinely accompany major depression. Some patients have both depression and dementia, while others have depression that causes cognitive impairment (i.e., pseudodementia). In the latter case, the treatment of depression should reverse the
(108)

signs and symptoms of cognitive dysfunction. Many patients complain that their thought are slowed and their capacity to process information is reduced. Transient cognitive impairments, especially involving attention, concentration, and memory storage and retrieval, are demonstrable through neuropsychological testing (139).Several clinical features help differentiating pseudo dementia from true dementia. Pseudo demented patients generally exert relatively less effort but report more incapacity than do demented patients.The demented group in more advanced stage, typically neither recognize nor complain of their cognitive failure. It is vital that patients with major depression with cognitive disturbance should not be misdiagnosed and thereby denied the antidepressant medication or ECT. Depression related cognitive dysfunction is a reversible condition that resolves with treatment of the underlying depression (140).
J. Post Psychotic Depression
Depressive symptoms complicate the course of schizophrenia in as many as 25% of the cases( 141). The depressive symptoms may coexist with the manifestations of the schizophrenic illness or may appear after the resolution of the acute schizophrenic psychosis, a pattern referred to as "Postpsychotic depression".The recognition of this syndrome is complicated by an overlap with the negative symptoms of schizophrenia (142).
The depressive manifestations are severe enough to represent the equivalent of major depression in only a minority of cases of true postpsychotic depression, but when they are represent they result in accrued and prolonged disability and may increase the risk of suicide. Adding an antidepressant agent to the patient's antipsychotic regimen has effectively treated postpsychotic depression (143).
K. Depression during pregnancy or following childbirth
Major depression occurring during pregnancy is a difficult therapeutic problem. Women of childbearing potential in psychiatric treatment should be carefully counseled as to the risk of becoming pregnant while taking psychotropic medications. Whenever possible, a pregnancy should be planned in consultation with psychiatrist so that medication may be discontinued before conception if feasible. The clinicians must carefully weigh the risks and benefits of prescribing psychotropic agents to the pregnant patient, taking into consideration the possibilities of physical (especially during the first trimester) and behavioral teratogenesis. Although tricyclic antidepressants, MAO inhibitors, and the newer antidepressant medication have not been specify incriminated as causing physical birth defects (144). Benzodiazepines have been inconclusively implicated in the development of cleft lip and palate when used in the first trimester. Although lithium exposure in the first trimester has been associated with an increased risk of cardiac malformations (145).
The relative risks and benefits of prescribing antidepressants must be particularly carefully weighed in the treatment of a pregnant woman. In patients whose safety and well being require antidepressants medications, a tricyclic or any of the newer antidepressant compounds may be justifiably used, after the I - trimester, if possible. ECT may be used as an alternative treatment; the current literature supports the safety for mother and fetus, as well as the efficacy of ECT during pregnancy (146).
Several depressive conditions may follow childbirth.The transient 7 to 10 days depressive conditions referred to as "postpartum blues" typically is too mild to meet the criteria for major depressive disorder and does not require medication. Puerperal psychosis is a more severe disorder complicating 1 -2 per 1,000 births; more than one half of the episodes of this type meet the criteria for major depression. Women whose maintenance antidepressant treatment was discontinued during pregnancy appear to be particularly at risk for recurrence of depression; such individuals should have their medications restored after delivery, in the absence of a contraindication. Postpartum depressive illness should be treated according to the same principles delineated for other depressive condition (147).
L. Seasonal depression Some individuals suffer annual episode of depression whose onset is in the fall or early winter,
(109)

usually at the same time each year.The depressive episodes frequently have atypical features such as hypersomnia and overeating. The entire range of treatments for depression may also be used to treat seasonal affective disorder, either in combination with or as an alternative to light therapy.
M. Depression in elderly -
The presentation of depression in the elderly is similar to younger adults in the "core" features, but different in having less dysphoric mood and more somatic concern (148,149) various subtypes of depression are being considered. Delusional depression and vascular depression appear to have some clinical validity (150,151). The current categorical diagnostic system (lCD-10, DSM-4) do not include a large number of elderly with significant depressive symptoms which do not satisfy syndromic criteria, and who therefor are not include in prevalence and other studies. A "subsyndrome" category may need to be considered in the future revisions of diagnostic systems. Outcome of depression in the elderly is little different to that in younger patients. Poor outcome is associated with physical illness, cognitive impairment and severity of depressive symptoms. Depression in the elderly is associated with excess physical disability and increased mortality.
Antidepressants are effective in treatment of depression in old age. The high rate of adverse affects of the tricyclic group mitigates against its use in the elderly. The lower rate of adverse events in the newer antidepressants (SSRIs) makes them more acceptable. However, notriptyline has a role in severe depression in the elderly. Psychosocial interventions are useful in major and non-major depression, cognitive therapy is a preferred modality of choice.
Electroconvulsive therapy (ECT) has demonstrated efficacy in treatment of old age depression with the benefit of rapid response in the severely ill with and without psychotic symptoms.The suicide rate in the elderly is high. Presentation with somatic complaints to a physician preceding the suicidal acts is frequent. Deliberate self-harm is usually associated with depressive disorders and other mental disorders.
N. Post- Stroke Depression
Post Stroke Depression is a common problem seen in at least 30-40% of survivors of intracerebral hemorrhage (152,153). Antidepressant drugs may be beneficial through relieving depressive symptoms and allow faster Post Stroke rehabilitation (154). Treatment is complicated by medical co-morbidity and by the potential for interaction with other co-prescribed drugs. Fluoxetine and Nortriptyline are probably the most standard and seen to be effective (155). The high incidence of depression after stroke makes proplylaxis worthy of consideration. Nortriptyline and Fluoxetine may prevent Post Stroke Depression (156).
O. Depression in Children
Depressive Disorders in children are associated with significant impairment, such as poor peer relationships, and impaired academic performance. Moreover, they are seen as a serious psychiatric condition. Adolescent with moderate depression respond effectively to Cognitive Behavior Therapy (CBT). Interpersonal psychotherapy, counseling and other non pharmacological approaches. Medication should be used in addition to non pharmacologic approaches to improve interpersonal, social and academic functioning.There are evidences that SSRIs are effective in child and adolescent depression and should generally be the first choice of drug. The commonly used SSRIs includes Sertraline, Fluoxetine, Paroxetine and Citalopram (157). In contrast TCAs are probably relatively ineffective in children (158).Other newer antidepressants have not been adequately evaluated in childhood and use of all these classes of drugs should be in only with specialist monitoring in special circumstances.
P. Depression in or with other medical condition
The presence of specific medical condition complicates or contraindicates certain forms of antidepressant medication therapy.
(110)

• Avoid use of MAOIs in-patient of Bronchial Asthma because of their interaction with sympathomimetic bronchodilators. Other antidepressant like SSRIs, TCAs, etc may be used for patient with Asthma without fear of interaction.
• A particular care should be taken in using tricyclics for patients with a history of specific cardiac conditions like Ventricular Arryhythmia, Subclinical Sinus node dysfunction, Conduction defects, prolong QT intervals or history of recent Ml. The SSRIs, Bupropion, newer antidepressant and ECT appears to be safer for patients with preexisting cardiac disease. (159-163).
• Individuals with dementia are particularly susceptible to the toxic effect of muscarinic blockade or memory and attention. Therefore, individuals suffering from dementia generally do best when given antidepressant with the lowest possible degree of anticholinerigic effect ex. SSRIs, Bupropion and of the TCAs desipramine or Nortriptyline. ECT is also effective in major depressive disorder super imposed on dementia. (164,165).
• Patients with glaucoma may be treated with antidepressants lacking anticholinerigic activity (like Bupropion, SSRIs and Trazodone). (166)
• Antihypertensive agents and TCAs may interact to either intensify or counteract the effect of antihypertensive therapy. TCA may antagonize the theraputic actions of many antihypertensives like guanethidine, clonidine and alpha methyldopa. Concurrent antihypertensive treatment especially with trazodone, or MAOIs will induced symptomatic orthostatic hypotension. Dose dependent elevation in blood pressure with venlafaxine makes this agent less preferable in patients with hypertension. (167)
REFFERENCES
1. Klerman G. (1980) - Overview of affective disorders. In comprehensive text books of psychiatry, 3rd edition vol 2nd (Eds. H.LKaplen, A.H.freddman, B.J. Sodok) pp-1305-1319, Williams SWilkins, Baltimore.
2. World Health Organization (1992): classification of mental & behavioral disorders. Clinical description &diagnostic guidelines, WHO- Geneva.
3. World Health Organization (1993): classification of mental & behavioral disorders. Diagnostic criteria for research, WHO Geneva.
4. Kendell R. E. (1993): Mood (affective) disorders. In comparison to psychiatric studies: 5th edition (Eds. R.E. Kendell, A.K.Zealley) p.p. 427-457 Churchill Living stone, London.
5. American Psychiatric Association (1994) - diagnostic & statistical manual of mental disorders, 4th edition, American Psychiatric Association, Washington D.C.
6. Hippius H. Stefanis C.N. (1994) - research in mood disorders, Hogeref & Huber, Bern.
7. Akiskal H. S. (1995) Mood disorders: clinical features in comprehensive textbook of psychiatry, 6th edition (Eds. H.I. Kaplen, B.J. Sodole) Williams & Wilkinson, Baltimore
8. Gelder M. Gath D., Mayor R., Cowen P., (1996): Oxford textbook of psychiatry, 3rd edition, Oxford University press New York.
9. World Psychiatric Association/International Committee for prevention & Treatment of Depression (1997): Educational program on depressive disorders, modulel, overview & fundamental aspects, cure booklet, NCM Publishers New York.
10. Kaplen H.I., Sadock B.J. (1998): symptoms of psychiatry, behavioral sciences/clinical psychiatry, and 8th edition, Williams & Wilkinson Baltimore.
11. Regier D.A., Boyd J.H., Burke J.D. Jr., Rae D. S., Myers J.K., Kramer M., Robins L.N., George L.K., Karno M., Locke B.Z.: one month prevalence of mental-disorders in the united states: based on five epidemilogic Catchment area sites. Arch Gen psychiatry 1988; 45: 977-986 [A],
(111)

12. Araya R., Robert W., Richard L, Lewis G: psychiatry morbidity in primary health care in Santiago, Chile preliminary findings. Br. J. psychiatry 1994; 165:530-2
13. Shamasunder C, Krishna Murthy S., Prakash O., Prabhakar N., Subbakrishna D.: psychiatric morbidity in a general practice in an Indian city. BMJ 1986; 292:1713-5
14. Holifield M., Katon W., and Spain D., Pule L.: Anxiety & depression in a village in Lesotho, Africa: a comparison with United States. Br. J. psychiatry 1990; 156:343-50.
15. Ormel J., Von Kroff M., Ustun T.B. Pini S. Korten A., Oldehinkel T.: common mental disorders & disability across cultures. JAMA 1994; 272: 1741 -8.
16. Australian Bureau of Statistics (1998): Mental health and wellbeing: Profile of adults, Australia 1997, Australian Bureau of Statistics, Canberra
17. Mueller T.L., Leon AC, Keller M.B., Solomon D.A. Endicott J., Coryell W., Warshaw M., Maser J.D.: recurrence after recovery from major depressive disorder during 15 years of observational
• follow up. AM. J. Psychiatry 1999; 156: 1000-1006(B)
18. Klerman G.L., Weissman N.M.: the course morbidity & costs of depression arch of psychiatry 1992,49: 831-834 (G).
19. Keller M D, Beardslee W R, Dorer D.J., Lavori P W, Samuelson H., Klerman G L: impact of severity & chronicity of parental affective illness on adoptive functioning & psychopathology in children, Arch gen psychiatry 1986; 43: 930-937 (B).
20. British Medical Bulletin (2001): "Depression" edited by Malcolm H. Lader and Philip J. Cowen, Vol. 57, 2001, Oxford University Press.
21. Stefanis C.N, Stefanis N.C (2002): Diagnosis of depressive disorder: A review in WPA series evidence and experience in Psychiatry on depressive disorders. Edited by Mario Maj and Norman Sartorious
22. Zimmerman M, Black D.W., Coryell W. (1989): Diagnosis Criteria for melancholia.The comparative validity of DSM 3 and DSM 4R. Arch. Gen. Psychiatry. 46: 361 -368 -
23. Kendler K.S.(1997):The diagnosis validity of melancholic major depression in population based sample of female twings. Arch. Gen. Psychiatry. 54:299-304.
24. Johnson J., Howarth E., Weissman M.M.(1991): The validity of major depression with psychotic features based on community study. Arch. Gen. Psychiatry. 48:1075-1081.
25. Maj. M., Pirozzi R., Dicaprio E.L. (1990): Major depression with mood congruent psychotic features: A distinct diagnostic entity or a more severe subtype of depression? Acta. Psychiatry Scand, 82: 439-444.
26. Paykel E.S., Parker R.R., Rowen PR., Rao B.M., Taylor C.N. (1983): Nosology and atypical depression, psychol. Med. 13:131-139.
27. Larn R.W., Stewart J.N. (1996):The validity of atypical depression in DSM 4 Compr. Psychiatry 37: 375-383.
28. Keller M.B., Shapiro R. W. (1982): "Double Depression" super imposition of acute depression episodes on Chronic depressive disorder. Am. J. Psychiatry 139:438-442.
29. Rosenthal N.E., Sack D.A., Gillin J.C., Lewy A.J., Goodwin F.K., Davenport Y, Mueller P.S., Newsome D.A., WehrT.A. (1984) seasonal affective disorder. A description of the syndrome and preliminary findings with light therapy. Arch. Gen. Psychiatry, 41: 72-80
30. Judd L.L., Akiskal H.S., Maser J.D., Zeller P.J., Endicott J., Coryell W., Paulus MP., Kunovac J.L., Leon A.C., Mueller T.I., et al (1998): A prospective 12 year study of subsyndromal and
(U2)

syndromal depressive symptoms in unipolar major depressive disorder. Arch. Gen. Psychiatry.55i 694-700.
31. Pearl Stein T, Stone A.B. (1998): Pramenstrual syndrome. Psychiatr. Clin. North Am. 21:577-590
32. Kendler S.K., Karkowski L.M., Corey LA., Neale M.C. (1998): Longitudinal population based twin study of retrospectively reported premenstrual syndroms and life time major depression. Am. J. Psychiatry, 155:1234-1240
33. Hunter M.S., (1996): Depression and the menopause, Br. Med. J. 313:1217-1218.
34. Kumar R., Robson K.M. (1984): A prospective study on emotional disorders in child bearing women. Br. J. Psychiatry. 29:250-264.
35. O'Hara M.W., Swain A.M., (1996): Rates and risk of postpartum depression: a meta analysis. Int. Rev. Psychiatry, 8:37-54.
36. Zisook S., Paulus M., Shuchter S.R., Judd L.L. (1997): The many faces of depression following spousal bereavement. J. Affect. Disord., 45: 85-95
37. Montgomery S.A. (1990): Anxiety and depression, Wrightson Biomedical Publications, London.
38. Rwiger D.A., Farmer M.E., Rae D.S., Locke B.Z., Keith S.J., Goodwin F.K., (1990): Comorbidity of mental disorders with alcohol and other drug abuse. Result from Epidemiologic Catchment Area (ECA) Study. JAMA, 264: 2511 -2518.
39. Kessler R.C., Nelson C.B., McGonagle K.A., Liu J., Swartz M., Blazer D.G., (1996): Comorbidity of DSM 3 R major depressive disorder in general population: results from US National Comorbidity Survey. Br. J. Psychiatry, 168:17-30.
40. Ustun T.B., Sartorious N. (Eds) (1995): Mental Illness in General Health Practice: An International Study, Wiley, Chichester.
41. Sartorious N., UstunT.B., LecrubierY, Wittchen H.U., (1996): Depression comorbid with anxiety: result from the WHO study on Psychological Disorders in Primary Health Care. Br. J. Psychiatry, 168:38-43.
42. Green M.F., Nuechterlein K.H., Ventura J., Mlintz J. (1990): The temporal relationship between depressive and psychotic symptoms in recent-onset schizophrenia. Am. J. Psychiatry, 147:179-182.
43. Roy A., Thompson R., Kennedy S. (1983): Depression in chronic schizophrenia. Br. J. Psychiatry, 142:465-470.
44. Davidson J.R.T., Foa A., (1992): Post Traumatic Stress Disorder: DSM 4 and Beyond, American Psychiatric Press, Washington, DC.
45. Treatment Of Depression (1998): World Psychiatric Association, International Committee for diagnosis and Educational programs on depressive disorders, Module2, depressive disorders in Physical Illness, Part-1:2, NCM Publishers New York.
46. Currie S., Heathfield K.W., Henson R. A., Scott D.F., (1971): Clinical sources and prognosis of temporal lobe epilepsy: a survey of 666 patients. Brain, 94:173-190.
47. Mendez M.F., Cummings J.L., Benson D.F., (1986): Depression in epilepsy: significance and phenomenology. Arch Neurol., 43:766-770.
48. Robertson M.M., Trimble M.R., Townsend H.R.A., (1987): The phenomenology of depression in epilepsy. Epilepsia, 28:364-372.
49. Robertson M.M., (1997): Depression in neurological disorders. In depression and physical illness (Eds M.M. Robertson, C.L.E. Katona), pp. 305-340, Wiley Chichester.
(113)

50. O'Shea B. (1997): A review of Huntington's disease. Int. J, Psychiatry Clin. Pract., 1:135-140.
51. Shaprio P.A., Lidasgoster L, Glassman A.H., (1997): Depression and heart disease. Psychiatr. Anm., 27: 347-352.
52. Barsky A.J. (1997): Palpitations, cardie awareness, and panic disorder. Am. J. Med., 92:315-345.
53. Spiegel D. (1996): Cancer and depression. Br. J. Psychiatry, 30:109-116.
54. Hendricks V., Alsthuler L, Whybrow P. (1998): Psychoneuroendocrinology of mood disorders.The hypothalamic-pitutary-thyroid axis. Psychiatr. Clin. North. Am., 21:277-292.
55. Lahey F.H., (1931): Apathetic hyperthyroidism. Anm., Surg., 93:1026-1036. •>
56. Fava G.A., (1994): Affective disorders and endocrine disease: new insight from psychosomatic studies. Psychosomatics, 35:341-353.
57. Popkin M.K., Callies A. L, Lentz R.D., Colon E.A., Sutherland D.E. (1988): Prevalence of major depression, simple phobia, and other psychiatric disorders in patients with long standing type 1 diabetes mellitus. Arch. Gen. Psychiatry, 45:64-68.
58. Long T.D., Kathol R.G., (1993): Critical review of data supporting affective disord caused by nonpsychotropic medication. Ann. Clin. Psychiatry, 5:259-270.
59. Patten S.B., Love E.J., (1993): Can drugs cause depression? A review of the evidence. J. Psychiatry Neurosci., 19: 92-102.
60. Muldoon M.F., Manuck S.B., Mathews K.A., (1990): Lowering cholesterol concentration and mortality: a quantitative review of primary prevention trials. Br. Med. J., 301:309-314.
61. Merikangas K.R., Angst J., Eaton W., Canino G., Rubio-Stipec M., Wacker H., Wittchen H.U., Andrade L., Essau C, Whitaker A., et al (1996): Comorbidity and boundaries of affective disorders with anxiety disorders and substance misuse: result of an international task Force. Br. J. Psychiatry., 30:58-67.
62. Rush A.J. (1986): Pharmacotherapy and psychotherapy. In clinical psychopharmacology (Ed. L.R. Derogatis), pp.46-47, Addison-wesley, Menlo Park, Ca.
63. Jerett R.B., Basco M.R., Riser R., Ramanan J., Marwill M„ Rush A.J., (1998): Is there a role for continuation phase cognitive therapy for depressed outpatients? J. consult. Clin. Psychol., 66: 1036-1040.
64. Frank E., kupfer D.J., Perel J.M., Cornes C, Jerett D.B., Mallinger A.G., Thase M.E., Mc Eachran A.B., Grochocinski V.J., (1990): Three year outcomes for maintenance therapies in recurrent depression. Arch. Gen. Psychiatry, 47:1093-1099.
65. Basco M.R., Rush A.J. (1995): Compliance with Pharmacotherapy in mood disorders. Psychiatr. Ann., 25: 269-279.
66. Youssel F. A.( 1983): compliance with theraputic regimens: a follow up study for patients with affective disorder. J. Adv. Nurs., 8: 513-517.
67. Seltzer A., Roncari I., Grafinkel P. (1980): Effect of Patient Education on medication compliance. Can. J. Psychiatry 25:638-645
68. Jarett RB, Rush AJ (1994): Short term Psychotherapy of depressive disorder: Current status and future directions, Psychiatry; 57:115-132.
69. Klerman GL, Weissman MM, Rounsaville BJ, Chevron ES (1984): Interpersonal psychotherapy of depression, New York, Basic Books.
70. Mackowitz JC, Kocsis J, Fishman B, Spielman LA, Jacobsberg LB, Frances AJ, Klerman GL, Perry SW (1998): Treatment of depressive symptoms in human immunodeficiency virus positive
(114)

patients. Arch Gen. Psychiatry; 55:452-457.
71. Barber JP, Muenz LR (1996): The role of avoidance and obsessive ness in matching patients to cognitive and interpersonal psychotherapy: empirical findings from the treatment for depression collaborative research program. J. Consult Clin. Psychol. 64: 951-958.
72. Beck AT., Rush A.J., Shaw B.F., Emery G. (1979): Cognitive therapy of depression, Guilford Press, New York.
73. Wilkes T.C.R., Belsher G., Rush A.J., Frank E., and Associates (1994): Cognitive Therapy for depressed adolescents, Guilford Press, New York.
74. Gloaguen V, Cottraux J, Cucherat M, Blackburn M (1998): A meta analysis of the effect of cognitive therapy in depressed patients. J. Affect Disord; 49:59-72.
75. Clark DM, Salkovskis PM, Hackmann A, Middleton H, Anastasiades P, Gelder M (1994): A comparison of cognitive therapy, applied relaxation and imipramine in the treatment of panic disorder. Br. J. Psychiatry; 164:759-769.
76. Ferster CB (1973): A functional analysis of depression. Am. Psychol.; 10: 857-870.
77. Bandura A (1977): Social learning theory. Englewood cliffs, NJ, Prentice Hall.
78. Lewinshon PM, Clarke G (1984): Group treatment of depressed individuals: the coping with depression course. Advance in behavioral research and therapy; 6: 99-114.
79. Rehm LP (1979): Behavior therapy of depression. New York Academic Press.
80. Bellack AS, Hersen M (1983): A comparison of social skills training, pharmacotherapy and psychotherapy for depression. Behav. Res.Ther. 21:101 -107.
81. Nezu AM (1986): Efficacy of a social program solving therapy for unipolar depression. J. Consult. Clin. Psychol. 54: 196-102.
82. Mc Lean PD, Hakstian AR (1979): Clinical depression: comparative efficacies of outpatients treatment. J. Consult. Clin. Psychol. 47:818-836.
83. Thompson JK, Williams DE (1987): An interpersonally based cognitive behavioral psychotherapy. Prog. Behav. Modif. 21:230-258.
84. Miller IW, Norman WH, Keitner Gl, Bishop SB (1989): Cognitive behavioral treatment of depressed inpatients. Behavior therapy. 20:25-47.
85. Jacobson N.S., Dobson K., Fruzzetti A.E., Schmaling K.B., Salusky S. (1991): Marital Therapy as a treatment for depression. J. Consult. Clin. Psychol., 59: 547-557.
86. Coleman R.E., Miller A.G., (1975):The relationship between depression and marital maladjustment in a clinic population: a multitrait - multimethods study. J. Consult. Clin. Psychol., 43:647-651.
87. Paykel E.S., Myers J.K., Dienelt M.N., Klerman G.L., Lindenthal J.J., Pepper M.P. (1969): Life events and depression: a controlled study. Arch Gen. Psychiatry, 21:753-760.
88. Hooley J.M., Teasdale J.D., (1989): Predictors of relapse in unipolar depressive expressed emotion, marital distress, and perceived criticism. J. Abnorm. Psychol., 98: 229-235.
89. Jacobsen N.S., Margolin G., (1979): Marital therapy: Strategies Based on Social Learning and Behaviour Exchange Principal, Brunner/Mazel,New York.
90. Jacobson N.S., Holtzworth-Munroe A.(1986): Marital therapy:a social learning/congnitive perspective.In Clinical Handbook of Marital therapy(Eds N.S. Jacobson,A.s.Gurman),pp.29-70,Guilford press.NewYork.
91. Bibring E (1954): Psychoanalysis and the dynamic psychotherapies. J. Am. Psychoanal. Assoc. 2:745-770.
(115)
92. Brenner C (1976): Psychoanalytic Techniques and Psychic Conflict. New York, International Universities Press.
93. Depression Guideline Panel (1993): Clinical Practice Guideline Number 5: Depression in primary care, Treatment of major depression: HHS Publications 93-051. Rock Ville, Md, Agency for health care policy and research.
94. Malan D (1976): The frontiers of brief psychotherapy, Plenum Press, New York.
95. Mann J (1973): Time Limited psychotherapy, Harvard University Press, Cambridge, MA.
96. Wolberg L.R. (1967): Short term Psychotherapy, Grunn & Stratton, New York.
97. Luborsky L. (1984): Principle of psychoanalytic Psychotherapy: A manual for supportive expressive treatment, Basic Books, New York.
98. Strupp H.H., Binder J.L. (1984): Psychotherapy in a new key, Basic Books, New York..
99. Lader MH, Cowen PJ, (2001): Depression, Published by British Medical Bulletin, Oxford University Press .
100. Angst J., Merikangs K., Scheidegger P., Wicki W. (1990): Recurrent brief depression: A new subtype of affective disorder. J. Affect. Disorder, 1987-98
101. Batra L., Gautam S., (1995): Psychiatric morbidity and personality profile in divorce seeking couples. Indian Journal of Psychiatry. Vol-34 (4) 179-185
102. Practice Guidelines for theTreatment of patients with Major Depressive Disorder (2000): Published by American Psychiatry Association, Washington D.C., and London U.K.,
103. The Maudsley's Prescribing guidelines( 2003) The South London and maudsley NHS Trust's 2003 Prescribing guidelines, Edited by David Taylor,Carol Paton, Robert Kerwin. Published by Martin Dunitz Taylor & Francis Group London and NY.
104. WPA Series (2002) - Evidence & Experience in Psychiatry : Depressive disorders. Edited by Mario Maj & Norman Sartorious .
105. National Institute for Clinical Excellence (NICE): Depression guidelines. WWW. Nice. Org/Clinical guidelines/Depression 2002
106. Texas Medicat ion Algor i thm Project (TMAP) (1999):Depression Algorythm.J.CI in. Psychiatry60:649-657.
107. Chakrabarthi S and Kulhara P. (2000): Pattern of antidepressant prescriptions; Acute p*hase treatment. JP 42 (1) P21 -28.
108. Chakrabarthi S and Kulhara P. (2000): Pattern of antidepressant prescriptions; II Continuation Phase Treatment
109. Pereira J. and Patel V. (1999): Which antidepressants are best tolerated in primary care? A pilot randomized trial from Goa. 41 (4)P-358-363
110. Selvan CP, MayurPM, GangadharBN, Janakiramaiah N, DKSubbakrishnaand Murli N, (1990): Comparision of Theraputic efficacy of ECT and imipramine: a randomized control trial 41(3) P 228-235.
111. Channabasavanna SM (1996): Drug therapy in India critical Issues in the quality of care. A DLN Murthy Roa oration 38(2)67-68.
112. Hamilton M. (1960): A rating scale for depression J. Neurol. Neurosurg. Psychiatry. 23:56-62.
113. Paykel E.S. (1990): Use of the Hamilton Depression Scale in general practice. Psychopharmacol. Ser. 9:40-47.
(116)

114. Beck A T, Ward CH, Mendelson M, Mock J. Erbaugh J.(1961): An inventory for measuring depression. Arch. Gen. Psychiatry. 4:561 -585.
115. Davidson J. Tumball CD, Strickland R., Miller R., Graves K., (1986): The montomery Asberg Depression Scale: reliability and validity, Acta. Psychiatry. Scand. 73:544-548.
116. Quitkin FM, Rabkin JG, Ross D, Mc Grath PJ (1984): Duration of antidepressant drug treatment: what is an adquate trial? Arch. Gen. Psychiatry. 41:238-254[G]
117. Guscott R, Grof P (1991 ):The clinical meaning of refractory depression: A review for the clinicians. Am. J. Psychiatry. 148:695-704.
118. Price LH, Charney DS, HeningerGR, (1986): Variability of response to lithium augmentation in refractory depression. Am. J. Psychiatry. 143:1387-1392.
119. Prange AJ, Loosen PT, Wilson IC, Lipton MA, (1984): The theraputic use of hormones of the thyroid axis in depression, in the Neurobiology of Mood Disorders. Edited by Post R, Ballenger J. Baltimore, MD, Williams & Wilkins, pp 311 -322 [E].
120. Nelson JC, Mazure CM, Bowers MB Jr, Jatlow PI, (1991): A preliminary, open study of the combination of fluoxetine and desipramine for rapid treatment of major depression. Arch Gen. Psychiatry. 48:303-307 [C].
121. Roseintein DL, Takeshita J. Nelson JC, (1991): Fluoxetine induced elevation and prolongation of tricyclic levels in overdose (letter). Am. J. Psychiatry. 148-807 [E].
122. Razani J.White KL, White J. Simpson G, Sloane RB, Redal R, Palmer R, (1983):The safety and efficacy of combined Amitriptyline and tranylcypromine antidepressant treatment: a controlled trial. Arch Gen. Psychiatry. 40:657-661 .[A].
123. Young JPR, LaderMH, Hughes WC, (1979): Controlled trial of trimipramine, monoamine, oxidase inhibitors, and combined treatmentin depressed out patients. Br Med J. 2:1315-1317 [A].
124. Prudice J. Sackeim HA, (1990): Refractory depression and Electroconvulsive therapy, in Treatment Strategies for refractory depression. Edited by Roose SP, Glassman AH, Washington, DC, American Psychiatric Press, pp 111 -128 [G].
125. Penny JF, (1990): Concurrent and close temporal administration of lithium ECT. Convuls.Therapy. 6:139-145. [D].
126. D'Mello DA, Finkbeiner DS, Kochar KN, (1995): The cost of antidepressant overdose. Gen. Hospi. Psychiatry. 17:454-455.
127. Cassidy S, Henry JA, (1987): Fatal toxicity of antidepressants drugs in overdose of antidepressants. Br. Med. J. 310:221 -224.
128. Forshall S, Nutt D, (1999): Maintanence pharmacotherapy of unipolar depression. Psychiatric Bulletin. 23:370-373
129. Spiker DG, Weiss JC, Dealy RS, Griffin SJ, Hanin I, Neil JF, Perel JM, Rossi AJ, Soloff PH, (1985): The phenamacological treatment of delusional depression. Am. J. Psychiatry. 140:318-322.
130. Corya S, Dube S, Anderson SW, (2002): Olanzapine-fluoxetine Combination for psychotic major depression. International Journal of Neuropsychopharmacology 5 (Suppl. 1): 5144.
131. Anton RF. Burch EA, (1990): A comparison study of amoxapineVs Amitriptyline plus perphenazine in the treatment of psychotic depression. Am. J. Psychiatry. 147:1203-1218.
132. Parker G, Roy K, Hadzi Pavlovic D, Pedic F,(1992): Psychotic (delusional) depression: A metaanalysis of physical treatmenmt. Journal of Affective Disorders, 24: 17-24.
(117)

133. Leibowitz Mr, Quitkin FM, Stewart JW, Mc Grath PJ, Harrison WM, Markowitz JS, Rabkin JG, Tricamo E, Goetz DM, Klein DF, (1998): Antidepressant specificity in atypical depression. Arch Gen. Psychiatry. 45:129-137.
134 Goodnick PJ(1991): Actue and long-term bupropion therapy: response and side effects, Ann Clin Psychiatry 3:311-313
135. Pande AC, Birkett M, Fechner-Bates S, Haskett RF, Greden JF(1996) Fluoxetine Versus phenelzing in atypical depression. Biol Psychiatry 40:1017-1020
136. Clomipramine Collaborative Study Group(1991) Clomipramine in the treatment of patients with obsessive-compulsive disorder. Arch Gen Psychiatry 48:730-738
137. Jenike MA, Buttolph L, Baeer L.Ricciardi J, Holland A(1989) Open trial of fluoxetine in obsessive-compulsive disorder. Am J Psychiatry 146:909-911
138. Grunhaus L(1988)Clinical and psychobiological Characteristics of simultaneous Panic disorder and major depression. Am J Psychiatry 145:1214-1221
139. Stoudemire A, Hill C, Gulley LR, Morris R( 1989) Neuropsychological and biomedical assessment of depression-dementia syndromes. J Neuroshychiatry Clin Neurosci 1:347-361
140. Caine ED(1981 )Pseudodementia: current concepts and future direction. Arch Gen Psychiatry 38:1359-1364
141. .Mc Glashn TH, Carpenter WT, Jr.(1976): Postpsychotic depression in Schizophrenia. Arch Gen. Psychiatry. 33:231 -239
142. Siris SG, Afan F, Cohen M, Mandeli J., Aronson A, Casey E, (1998): Postpsychotic depression and negative symptoms: an investigation of syndromal overlap. Am. J. Psychiatry. 145:1532-1537.[A]
143. Siris SG, Morgan V, Fagerstorm R, Rifkin A, Cooper TB (1987): Adjunctive imipramine in the treatment of postpsychotic depression: a controlled trial. Arch Gen. Psychiatry. 44:533-539 [A].
144. Elia J., Simpson GM (1990): Antidepressant medication during pregnancy and lactation: fetal teratogenic and toxic effects, in Pharmacotherapy of Depression. Edited by Amsterdam JD. New York, Marcel Dekker [G].
145. Norra JJ, Norra HA, Towes WH (1974): Lithium, Ebstein's anomaly, and other congential heart defects. Lancet 2:594-595.
146. Nurnberg HG (1989): An overview of somatic treatment of psychosis during pregnancy and postpartum. Gen. Hosp. Psychiatry. 11:328-338
147. Ananth J.,(1978): Side effect in the neonate from psychotropic agents excreted through breast feeding. Am. J. Psychiatry. 135:801-805.
148. Baldwin RC, (1990): Age of onset of depression in the elderly. Br.J.Psychiatry. 156:445-446.
149. Burvill PW, Hall WD, Stampfer HG, Emmerson JP (1989): A Comparision of early onset and late onset depressive illness in the elderly. Br.J.Psychiatry. 155:673-679
150. Georgotas A (1983): Affective Disorders in the elderly: Diagnostic and research consideration. Agg. Ageing. 12:1-10
151. Gurland BJ, (1976): The comparative frequency of depression in various adult age group. J. Gerontol. 31.283-292
152. Gainotti G, Antonucci G, Marra C, et al (2001): Relationship between depression after stroke, antidepressant therapy and functional recovery. Journal of Neurology, Neurosurgical Psychiatry. 71:258-261.
(118)

153. Hayee MA, Akhtar N, Haque A et al (2001): Depression after stroke analysis of 297 stroke patients. Bangla Desh Medical research Council Bulletin 27:96-102.
154. Gainotti G., Marra C, (2002): Determinants and consequences of post stroke depression. Current opinion in Neurology. 15:85-89.
155. Robinson R, Schultz SK, Castillo C et al (2000): Nortriptyline Vs Fluoxetine in the treatment of depression and in short term recovery after stroke: A placebo control double blind study. American Journal of Psychiatry. 157:351 -359.
156. Narushima K, Koseir JT, Robinson RG (2002): Preventing post stroke depression : a 12 week double blind randomized treatment trial and 21 month follow up. Journal of Nergv. Mental Disease. 190:296-303.
157. Findling RL, Reed MD, Blumer JL (1999) Pharmacological treatment of Depression in Children and Adolescents. Pediatric Drugs jul-sep.1 :161-182
158. Hazell R OConnel D, Heathcote D, et. Al (1995) Efficacy of Tricyclic drugs in treating child & adolescents depression: A metaanalysis. BMJ 310:897-901
159. Nelson JC, Giardina EG,Perel JM, Pollock BG, Laghrissi(1999)Thode F, Narayan M, Nobler MS, Robin DW.Gergel I, McCafferty J, Roose S:Treatment of major depression with nortriptyline and paroxetine in patients with ischemic heart disease. Am J Psychiatry ;156:1024-1028
160. Bigger JT, Giardina EG, Perel JM, KantorSJ, Glassman AH(1977)Cardacantiarhythmic effect of imipramine hydrochloride. N Engl J Med ;296:206-208
161. Applegate RJ(1997)Diagnosis and management of ischemic heart disease in the patient scheduled to undergo electroconvulsive therapy. Convuls Ther 13:128-144
162. Roose SR Dalack GW, Glassman AH, Woodring S, Walsh BT, Giardina EGV (1991 )Cardiovascular effects of bupropion in depressed patients with heart disease. Am J Psychiatry 148;512-516
163. The Practice of Electroconvulsive Therapy(1990): Recommendations for treatment, Training, and Privileging: A Task Force Report of the American Psychiatric Association. Washington, DC,
164. Weiner RD, Coffey CE, Krystal AD(1999) Electroconvulsive therapy in the medical and neurologic patient, in Psychiatric Care of the Medical Patient, 2nd ed. Edited by Stoudemire A, Forget B. Greenberg D. New York, Oxford University Press
165. Krystal AD.Coffey CE(1997) Neuropsychiatry considerations in the use of electroconvulsive therapy. J Neuropsychiatry Clin Neurosci;9:283-292
166. Lieberman E, Stoudemire A(1987)Use of tricyclic antidepressants in patients with glaucoma. Psychosomatics 28:145-148
167. Thase ME(1998) Effects of venlafaxine on blood pressure: a meta-analysis of original data on 3744 depressed patients/ J Clin Psychiatry 59:502-508
(119)