![PERIODONTAL DISEASE [Read-Only] · STAGES OF DISEASE z1.Gingivitis zAffects soft tissue only (gums) zDisease changes are reversible z2.Periodontitis zAffects hard tissues (bone) zDisease](https://static.fdocuments.us/doc/165x107/5f6ce50dac3cab166049359c/periodontal-disease-read-only-stages-of-disease-z1gingivitis-zaffects-soft-tissue.jpg)
CLINICAL PEDIATRIC DENTISTRY I DSV 441 CHAPTER 20 GINGIVITIS AND PERIODONTAL DISEASE (413-452)...
17
CLINICAL PEDIATRIC DENTISTRY I DSV 441 CHAPTER 20 GINGIVITIS AND PERIODONTAL DISEASE (413-452) PERIODONTAL DISEASES IN CHILDREN (429-441) McDonald, Avery, Dean. Dentistry For The Child And Adolescent, 8th Ed. 20 Tuesday 10\3\2015 1:00 pm-2:00 pm OTHMAN AL-AJLOUNI 1
-
Upload
kelley-nicholson -
Category
Documents
-
view
223 -
download
1
Transcript of CLINICAL PEDIATRIC DENTISTRY I DSV 441 CHAPTER 20 GINGIVITIS AND PERIODONTAL DISEASE (413-452)...

CLINICAL PEDIATRIC DENTISTRY I DSV 441
CHAPTER 20
GINGIVITIS AND PERIODONTAL DISEASE(413-452)
PERIODONTAL DISEASES IN CHILDREN (429-441)McDonald, Avery, Dean. Dentistry For The Child And Adolescent, 8th Ed.
20
Tuesday 10\3\2015
1:00 pm-2:00 pm
OTHMAN AL-AJLOUNI 1

LECTURE OUTLINEPERIODONTAL DISEASES IN CHILDRENEarly-Onset Periodontitis
Prepubertal Periodontitis
Localized Early-Onset Periodontitis (Localized Juvenile Periodontitis)
Generalized Early-Onset Periodontitis (Generalized Juvenile Periodontitis)
Treatment of Early-Onset Periodontitis
Premature Bone Loss in the Primary Dentition
Papillon-Lefevre Syndrome (Precocious Periodontosis)
Gingival Recession
Self-Mutilation
Abnormal Frenum Attachment
Frenectomy and Frenotomy
Techniques for Mandibular Frenectomy and Vestibular Depth Increase
Free Gingival Autograft Procedure 2

EARLY-ONSET PERIODONTITIS
EOP is used as a GENERIC term to describe a HETEROGENEOUS group of periodontal disease occurring in YOUNG individuals who are otherwise HEALTHY.
Categories of EOP may overlapping etiologies and clinical presentations:
(1)Localized form (localized juvenile periodontitis 0.53% (LJP),
(2)Generalized form (generalized juvenile periodontitis 0.13%(GJP), and
(3)Prepubertal category that have both localized and generalized forms (localized and generalized prepubertal periodontitis).
3

PREPUBERTAL PERIODONTITIS
PP localized (LPP) and generalized (GPP) form.
LPP is localized attachment loss and alveolar bone loss only in PRIMARY dentition in an otherwise HEALTHY child. Exact time of onset is unknown, but it appears to arise around or before 4 years of age.
•Abnormal probing depths
•Minor gingival inflammation
•Rapid bone loss
•Minimal to varying amounts of plaque
•Abnormalities in host defenses (e.g., Leukocyte chemotaxis),
•Extensive proximal caries facilitating plaque retention and bone loss
•Family history of periodontitis associated with LPP
•As the disease progresses, the child's periodontium shows signs of gingival inflammation with gingival clefts and localized ulceration of gingival margin
4

PREPUBERTAL PERIODONTITISOnset of (GPP) is DURING OR SOON after eruption of primary teeth.
It results in severe gingival inflammation
Generalized attachment loss
Tooth mobility
Rapid alveolar bone loss with premature exfoliation of teeth.
Chronic cases display presence of clefting and pronounced recession with associated acute inflammation.
High prevalence of leukocyte adherence abnormalities and an impaired host response against bacterial infections. Alveolar bone destruction proceeds rapidly, and primary teeth may be lost by 3 years of age.
Micro-organisms predominating in gingival pockets include actinobacillus actinomycetemcomitans (Aa), porphyromonas (bacteroides) gingivalis, bacteroides melaninogenicus, prevotella intermedia, capnocytophaga sputigena, and fusobacterium nucleatum.
Major periodontal pathogens are transmitted among family members.
Past medical history reveals a history of RECURRENT INFECTIONS. (E.G., Otitis media, skin infections, upper respiratory tract infections)
5

PREPUBERTAL PERIODONTITISConsultation with pediatrician to RULE OUT SYSTEMIC DISEASES.
Treatment of LPP or GPP depends on early diagnosis, dental curettage, root planing, prophylaxis, oral hygiene instruction, restoration of decayed teeth, removal of primary teeth that have lost bony support, and more frequent recalls.
Use of antimicrobial rinses (chlorhexidine) and therapy with broad-spectrum antibiotics are effective in eliminating periodontal pathogens. Amoxicillin (Augmentin) has been used in children (250-mg liquid three times a day for 10 days).
Because tetracycline (250-mg elixir twice a day for 10 days), or a derivative, is an effective antibiotic against Aa and other gram-negative anaerobic microorganisms, child's parents should be aware of potential for pigmentation change in developing permanent teeth and an increased susceptibility to oral candidiasis as a result of tetracycline therapy.
Treatment of GPP is less successful overall and sometimes requires extraction of all primary teeth
Children with LPP or GPP may experience severe periodontitis of permanent teeth.
6

LOCALIZED EARLY-ONSET PERIODONTITIS (LOCALIZED JUVENILE PERIODONTITIS)LJP
LJP occurs in HEALTHY children and adolescents without clinical evidence of systemic disease. It is characterized by rapid and severe loss of alveolar bone around more than one permanent tooth, usually first molars and incisors.
It appears selflimiting
Bone loss around primary teeth can be an early finding.
Prevalence range from 0.1% to 1.5% with a bilaterally symmetric pattern of bone loss, prevalence in black population is greater, at 2.5%.
Clinically, little or no tissue inflammation and very little supragingival dental plaque or calculus. Progression of bone loss is three to four times faster than in adult periodontitis.
LJP is not single disease entity. Probable causative microbial species are Aa or Aa in combination with bacteroides-like species. A variety of neutrophil defects.
Hereditary basis; some believe mode of transmission is autosomal recessive, but others is an Xlinked dominant mode. 7

GENERALIZED EARLY-ONSET PERIODONTITIS (GENERALIZED JUVENILE PERIODONTITIS)GJP
Generalized form of EOP occurs at or around PUBERTY in older juveniles and young adults. It affects ENTIRE dentition. Because of its wide distribution and rapid rate of alveolar bone destruction.
Neutrophils suppressed chemotaxis.
Marked periodontal inflammation and have heavy accumulations of plaque and calculus.
8

TREATMENT OF EARLY-ONSET PERIODONTITIS
Successful treatment of EOP depends on early diagnosis
Use of tetracyclines (sometimes in combination with metronidazole), such as a 2-week course of doxycycline (a synthetic tetracycline) (1 g per day).
Surgical removal of infected crevicular epithelium and debridement of root surfaces during surgery Meticulous scaling and root planing of all teeth, with concomitant irrigation to probing depth of saturated inorganic salt solutions and 1% chloramine.
Patient home care treatment included daily application of a paste of sodium bicarbonate and 3% hydrogen peroxide and inorganic salt irrigations. 9

PREMATURE BONE LOSS IN THE PRIMARY DENTITION
Advanced alveolar bone loss associated with systemic disease occurs in children and adolescents as well as adults.
Most premature tooth loss from nonsystemic disease results from trauma or caries.
Bony destruction in primary dentition in absence of local factors is highly suggestive of systemic disease: Hypophosphatasia,
P-Lsyndrome,
Histiocytosis x,
Agranulocytosis,
Leukocyte adherence deficiency,
Neutropenias,
Leukemias,
Diabetes mellitus,
Scleroderma,
Fibrous dysplasia,
Acrodynia,
Down syndrome, and
Chediak-Higashi syndrome. 10

PAPILLON-LEFEVRE SYNDROME PLS (PRECOCIOUS PERIODONTOSIS)
Rare and cause unknown.
Familial predisposition, an autosomal recessive mode of inheritance. Causative gene by linking it to chromosome band 11q14-q2l. Primary teeth erupted at normal time. However, as early as 2 years of age, gingival bleeding, painful.
Hyperkeratosis of palms and soles at 8 months of age. Hyperkeratotic lesions of elbows and knees.
Laboratory tests, including complete blood count, urinalysis, and microserum calcium and phosphorus determinations, normal.
All primary teeth showed looseness, and full-mouth radiographs revealed severe horizontal bone resorption.
Normal pulp tissue, cementum.
Periodontal pathogens (Actinobacillus actinomycetemcomitans, F. nucleatum, Capnocytophaga species, and Eikenella corrodens) have been isolated
11

GINGIVAL RECESSIONSeveral factors predispose patients to gingival recession.
Presence of : Narrow band of attached or keratinized gingiva, Alveolar bony dehiscence, Toothbrush trauma, Tooth prominence, Impinging frenum attachment, Soft tissue impingement by opposing occlusion, Orthodontic tooth movement, Use of impression techniques including subgingival tissue retraction, Oral habits, Periodontitis, and Pseudorecession (extrusion of teeth). Recession is dealt with conservatively by elimination stimulus if possible, while excellent oral hygiene. If recession remains unchanged (nonprogressive) or improves (less recession observed) over time, continued periodic monitoring is recommended. If recession has progressed after a 4-8-wk, other periodontal procedures based on identified predisposing factor. 12

SELF-MUTILATION
Children purposely traumatize their oral structures. Dentists should be aware of possibility of this condition and should approach problem in same manner as they do thumb sucking. An attempt should be made to determine the CAUSE. If it is found to be result of local dental factors, it can be corrected. However, majority an emotional problem Is involved, and family must be directed to competent counseling services.Traumatized free and attached gingival tissues with a fingernail, to extent that supporting alveolar bone has been destroyed. Traumatization of gingiva between maxillary primary molars with index fingernail. Bilateral stripping of buccal tissue in maxillary premolar areas with fingernail and a bobby pin with a fingernail and a hairpin. PSYCHOLOGIC problem and referred to a child guidance clinic. After treatment of emotional problem habit discontinued. The self-mutilation an escape from reality. Tension and conflicts unhappiness and conflict in home. Traumatic gingival recession in infants resulting from a dummy (pacifier) sucking habit.
13

ABNORMAL FRENUM ATTACHMENT
Normal frenum attaches apically to free gingival margin so as not to exert a pull on zone of attached gingiva, usually terminating at mucogingival junction. Some frenums have bifid and trifid attachments to alveolar process. An abnormal or high frenum is present when there is inadequate attached gingiva in terminal insertion area. A frenum attached too closely to gingival margin may interfere with proper toothbrush, cause opening of gingival crevice during function, or interfere with speech. High frenum attachments associated with isolated gingival recessions and diastemas. A mandibular anterior frenum inserts into free or marginal gingival tissue and causes subsequent recession and pocket formation. Abnormal frenum attachment is most often observed in the central incisor area. Fibers extending to papilla between central incisors with branching auxiliary fibers inserting into marginal tissue, may involve labial tissue in canine areas. Abnormal attachment is frequently associated with a vestibular trough throughout anterior region that is more shallow. 14
ABNORMAL FRENUM ATTACHMENT
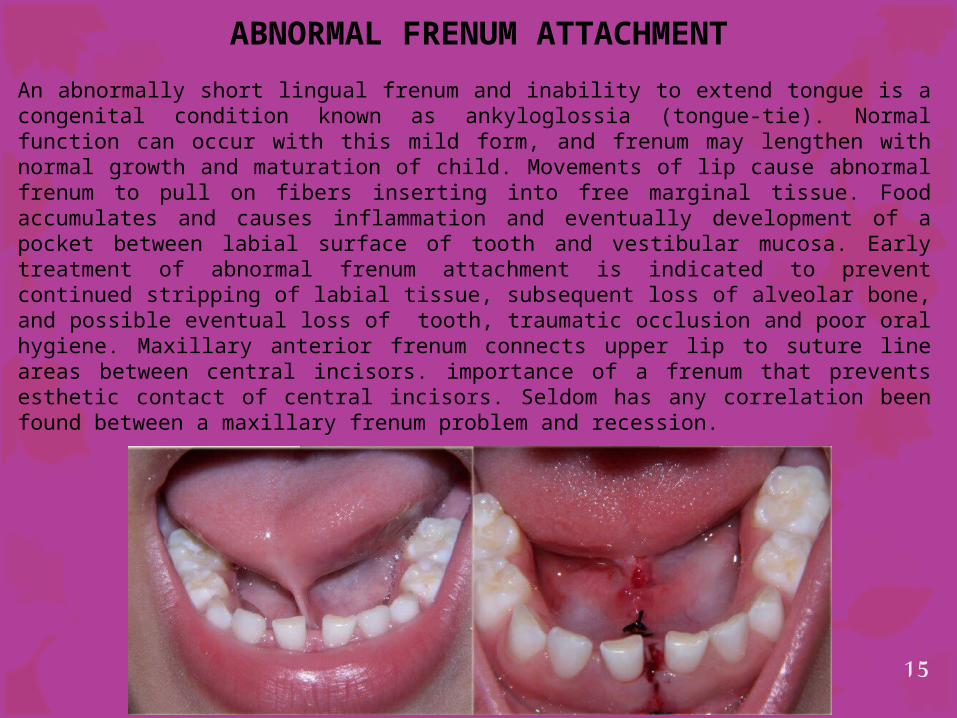
An abnormally short lingual frenum and inability to extend tongue is a congenital condition known as ankyloglossia (tongue-tie). Normal function can occur with this mild form, and frenum may lengthen with normal growth and maturation of child. Movements of lip cause abnormal frenum to pull on fibers inserting into free marginal tissue. Food accumulates and causes inflammation and eventually development of a pocket between labial surface of tooth and vestibular mucosa. Early treatment of abnormal frenum attachment is indicated to prevent continued stripping of labial tissue, subsequent loss of alveolar bone, and possible eventual loss of tooth, traumatic occlusion and poor oral hygiene. Maxillary anterior frenum connects upper lip to suture line areas between central incisors. importance of a frenum that prevents esthetic contact of central incisors. Seldom has any correlation been found between a maxillary frenum problem and recession.
15

1- Hart TC, Hart PS, Michalec MD, Zhang Y, Marazita ML, Cooper M, Yassin OM, Nusier M, Walker S: LOCALISATION OF A GENE FOR PREPUBERTAL PERIODONTITIS TO CHROMOSOME 11Q14 AND IDENTIFICATION OF A CATHEPSIN C GENE MUTATION. J Med Genet. 2000; 37: 95- 101. Original Article USA. PMID: 10662808 [PubMed - indexed for MEDLINE]2- Hattab FN, Al- Momani AS, and Ajlouni OM: PAPILLON-LEFEVRE SYNDROME: CLINICAL FEATURES AND HISTOPATHOLOGICAL INVESTIGATION. Journal of the Royal Medical Services, June 1995; 2(1): 63-66. Original Article.3- Hattab FN, Rawashdeh MA, Yassin OM, Al- Momani AS, and Al- Ubosi MM: PAPILLON-LEFEVRE SYNDROME: A REVIEW OF LITERATURE AND REPORT OF 4 CASES. J Periodontol, May 1995; 66(5): 413-420. Review USA. PMID: 7623262 [PubMed - indexed for MEDLINE]
MY PUBLICATIONS
16












![High Throughput Sequencing Detects Gingivitis and ... · exposure to both gingivitis and periodontal disease promoted AD pathogenesis [11,12]. Furthermore, a prospective laboratory-based](https://static.fdocuments.us/doc/165x107/5e6419678ae9c83e4e4b47fb/high-throughput-sequencing-detects-gingivitis-and-exposure-to-both-gingivitis.jpg)






