Clinical Pathophysiology Review 3 8:30 AM, March 4, 2003 Fred A. Zar, MD, FACP Director, M2...
188
Clinical Clinical Pathophysiology Pathophysiology Review 3 Review 3 8:30 AM, March 4, 8:30 AM, March 4, 2003 2003 Fred A. Zar, MD, FACP Fred A. Zar, MD, FACP Director, M2 Clinicopathophysiology Director, M2 Clinicopathophysiology Course Course Professor of Clinical Medicine Professor of Clinical Medicine University of Illinois at Chicago University of Illinois at Chicago
-
Upload
audra-stevens -
Category
Documents
-
view
215 -
download
2
Transcript of Clinical Pathophysiology Review 3 8:30 AM, March 4, 2003 Fred A. Zar, MD, FACP Director, M2...

Clinical PathophysiologyClinical PathophysiologyReview 3Review 3
8:30 AM, March 4, 20038:30 AM, March 4, 2003
Fred A. Zar, MD, FACPFred A. Zar, MD, FACP
Director, M2 Clinicopathophysiology CourseDirector, M2 Clinicopathophysiology Course
Professor of Clinical MedicineProfessor of Clinical Medicine
University of Illinois at ChicagoUniversity of Illinois at Chicago

Respiratory PathophysiologyRespiratory Pathophysiology

COPD: Pathophysiology and ConsequencesCOPD: Pathophysiology and Consequences• Airway inflammationAirway inflammation– Increased mucus and protease activityIncreased mucus and protease activity– Cough and sputumCough and sputum
• Increased Airway ResistanceIncreased Airway Resistance– Wheeze and rhonchiWheeze and rhonchi– Pursed lip breathingPursed lip breathing
• Increased Work of BreathingIncreased Work of Breathing– Decreased exercise yet increased metabolismDecreased exercise yet increased metabolism– Breathing may require 25–35% of energy (nml 3–5%)Breathing may require 25–35% of energy (nml 3–5%)– Weight lossWeight loss
• HyperinflationHyperinflation– Inspiratory muscle dysfunctionInspiratory muscle dysfunction– Hoover’s sign, increased AP diameterHoover’s sign, increased AP diameter
• Impaired Regional VentilationImpaired Regional Ventilation– V/Q mismatch –> hypoxemia –> pulmonary HTNV/Q mismatch –> hypoxemia –> pulmonary HTN

Smoking and COPDSmoking and COPD• Smoking leads to activation of macrophages and Smoking leads to activation of macrophages and
neutrophilsneutrophils
• Pulmonary inflammation Pulmonary inflammation – > chronic bronchitis> chronic bronchitis
• Proteases released: Proteases released: elastase, cathepsins, metalloproteinaseselastase, cathepsins, metalloproteinases
– > inhibited by antiproteases> inhibited by antiproteases• alpha–1 antitrypsin, elafin, secretory leukoprotease inhibitoralpha–1 antitrypsin, elafin, secretory leukoprotease inhibitor
– > injury to extracellular matrix –> emphysema> injury to extracellular matrix –> emphysema

EmphysemaEmphysema• DefinitionDefinition– Airspace enlargement distal to terminal bronchioleAirspace enlargement distal to terminal bronchiole– Due to destruction of alveolar wallDue to destruction of alveolar wall
• LocationsLocations– CentrilobularCentrilobular– PanacinarPanacinar

Chronic BronchitisChronic Bronchitis• DefinitionDefinition– Cough and sputumCough and sputum– Most days for 3 months Most days for 3 months – 2 consecutive yrs2 consecutive yrs
• Pathologic CorrelatePathologic Correlate– Mucus gland hypertrophyMucus gland hypertrophy– Goblet cell hyperplasiaGoblet cell hyperplasia

COPD: TherapyCOPD: TherapyDrugDrug MechanismMechanism Clinical EffectClinical Effectß2 agonistsß2 agonists Smooth muscle relaxationSmooth muscle relaxation BronchodilationBronchodilation
Decreases mast cell degranDecreases mast cell degran
AnticholinergicsAnticholinergics Muscarinic antagonistsMuscarinic antagonists BronchodilationBronchodilation
CorticosteroidsCorticosteroids Inhibit cytokine productionInhibit cytokine production Do not alter courseDo not alter course
Decreases eosinophilsDecreases eosinophils Decreases reactivityDecreases reactivity
Increases ß responsiveness Increases ß responsiveness Decreases inflammationDecreases inflammation
TheophyllineTheophylline Phosphodiesterase inhib.Phosphodiesterase inhib. BronchodilationBronchodilation
Adenosine receptor inhib.Adenosine receptor inhib. Better resp. muscle functionBetter resp. muscle function
Skeletal muscle contractionSkeletal muscle contraction

AsthmaAsthma• Chronic inflammatory disorder with reversible airways obstructionChronic inflammatory disorder with reversible airways obstruction
• Cell mediatedCell mediated– Mast cells, eosinophils, T lymphs, macros, PMNs, epithelialMast cells, eosinophils, T lymphs, macros, PMNs, epithelial
• Increased bronchial responsiveness to a variety of stimuliIncreased bronchial responsiveness to a variety of stimuli– Allergens, exercise, cold, pollution, infection, drugs, GERDAllergens, exercise, cold, pollution, infection, drugs, GERD
• Symptoms and signsSymptoms and signs– Wheeze, SOB, coughing, chest tightnessWheeze, SOB, coughing, chest tightness
– Can be induced with histamine or methacholine challengeCan be induced with histamine or methacholine challenge– Pulsus paridoxicus: drop of SBP with inspiration of > 10 mm HgPulsus paridoxicus: drop of SBP with inspiration of > 10 mm Hg
• Dual responseDual response– Early(5 min) due to mast cell release of histamine, LT, PG, PAFEarly(5 min) due to mast cell release of histamine, LT, PG, PAF
– Late (4 hr) due to eosinophil release of LT and cytokinesLate (4 hr) due to eosinophil release of LT and cytokines

Asthma ClassificationAsthma ClassificationClassClass SymptomsSymptoms Night SxNight Sx FEV1FEV1 TherapyTherapy
Mild IntermittentMild Intermittent < 2x/wk< 2x/wk < 2x/mo< 2x/mo > 80%> 80% PRN ß-agonistPRN ß-agonist
Mild PersistentMild Persistent 3–6x/wk3–6x/wk > 2x/mo> 2x/mo > 80%> 80% Daily: GC or LADaily: GC or LA
or MCDor MCD
PRN ß-agonistPRN ß-agonist
Moderate PersistentModerate Persistent DailyDaily >> 1x/wk 1x/wk 60–80%60–80% Above + long–Above + long–
acting ß–agonistacting ß–agonist
± anticholinergic± anticholinergic
± theophylline± theophylline
Severe PersistentSevere Persistent ContinuousContinuous NightlyNightly < 60%< 60% Above + high–Above + high–
dose inhaled GCdose inhaled GC

Asthma: Blood GasesAsthma: Blood Gases
StageStage pO2pO2 pCO2pCO2 pHpH
II NmlNml NmlNml NmlNml
IIII NmlNml LowLowHighHigh
IIIIII LowLow LowLowHighHigh
IVIV LowLow HighHigh LowLow

Asthma: TherapyAsthma: TherapyDrugDrug MechanismMechanism Clinical EffectClinical Effectß2 agonistsß2 agonists Smooth muscle relaxationSmooth muscle relaxation BronchodilationBronchodilation
Decreases mast cell degranDecreases mast cell degranAnticholinergicsAnticholinergics Muscarinic antagonistsMuscarinic antagonists BronchodilationBronchodilationCorticosteroidsCorticosteroids Inhibit cytokine productionInhibit cytokine production Decreases inflammationDecreases inflammation
Decrease eosinophilsDecrease eosinophils Decreases reactivityDecreases reactivityIncreases ß responsivenessIncreases ß responsiveness
TheophyllineTheophylline Phosphodiesterase inhib.Phosphodiesterase inhib. BronchodilationBronchodilationAdenosine receptor inhib.Adenosine receptor inhib. Better resp. muscle functionBetter resp. muscle functionSkeletal muscle contractionSkeletal muscle contraction
Leukotreine inhLeukotreine inh Decrease leukotreine effectDecrease leukotreine effect Anti–inflammatoryAnti–inflammatoryCromolyn/Cromolyn/ Mast cell stabilizationMast cell stabilization Anti–inflammatoryAnti–inflammatoryNedocromilNedocromil

Pulmonary FibrosisPulmonary Fibrosis• PathogenesisPathogenesis– Initial insult –> immune response –> alveolitis –> WBC/macro Initial insult –> immune response –> alveolitis –> WBC/macro
cytokine release–> injury to epithelial cells and alveolar basal cytokine release–> injury to epithelial cells and alveolar basal lamina –> repair with fibrosislamina –> repair with fibrosis
• Associated DiseasesAssociated Diseases– Idiopathic (cryptogenic fibrosing alveolitis)Idiopathic (cryptogenic fibrosing alveolitis)– CTD: RA, scleroderma, PMSCTD: RA, scleroderma, PMS– SarcoidosisSarcoidosis– Occupational lung disease: silicosis, asbestosisOccupational lung disease: silicosis, asbestosis– Hypersensitivity pneumonitisHypersensitivity pneumonitis– Eosinophilic granulomaEosinophilic granuloma– DrugsDrugs

Pulmonary Fibrosis: ManifestationsPulmonary Fibrosis: Manifestations
• DyspneaDyspnea
• Rapid shallow breathingRapid shallow breathing
• Inspiratory crackles (Velcro®)Inspiratory crackles (Velcro®)
• Digital clubbingDigital clubbing
• Later right heart failureLater right heart failure

Pressure–Volume CurvePressure–Volume CurveObjectively assesses elastic recoilObjectively assesses elastic recoil
• ParametersParameters– X–axis = lung volumeX–axis = lung volume– Y–axis = pleural (esophageal) pressureY–axis = pleural (esophageal) pressure– Compliance = slope (∆Y/∆X or ∆P/∆V)Compliance = slope (∆Y/∆X or ∆P/∆V)– Vmax = maximum expiratory flow rateVmax = maximum expiratory flow rate• Dependent on recoil and airway resistanceDependent on recoil and airway resistance
• Alterations in disease statesAlterations in disease states– Emphysema: loss of elastic recoilEmphysema: loss of elastic recoil• Increased slope, shift to left, higher volumesIncreased slope, shift to left, higher volumes
– Pulmonary fibrosis: increased elastic recoilPulmonary fibrosis: increased elastic recoil• Decreased slope, shift to right, lower volumesDecreased slope, shift to right, lower volumes

Pressure–Volume CurvesPressure–Volume CurvesObstructive vs. Restrictive DiseaseObstructive vs. Restrictive Disease
ObstructiveObstructive RestrictiveRestrictiveExampleExample EmphysemaEmphysema Pulmonary Pulmonary
fibrosisfibrosis
Elastic recoilElastic recoil DecreasedDecreased IncreasedIncreased
ComplianceCompliance Increased Increased DecreasedDecreased
P–V slopeP–V slope Increased Increased DecreasedDecreased
Curve shiftCurve shift Left Left RightRight
VolumesVolumes Higher Higher LowerLower

Pathophysiologic ConsequencesPathophysiologic Consequences(Emphysema, Decreased Elastic Recoil)(Emphysema, Decreased Elastic Recoil)
• Increased lung complianceIncreased lung compliance– Increased lung distensionIncreased lung distension– Increased airway collapseIncreased airway collapse– Decreased VmaxDecreased Vmax
• Increased work of breathingIncreased work of breathing• Increased ventilatory driveIncreased ventilatory drive• Increased FRC and RVIncreased FRC and RV• V/Q mismatchV/Q mismatch• Decreased diffusion capacityDecreased diffusion capacity

Pathophysiologic ConsequencesPathophysiologic Consequences(Pulmonary Fibrosis, Increased Elastic Recoil)(Pulmonary Fibrosis, Increased Elastic Recoil)
• Decreased lung complianceDecreased lung compliance– Decreased lung distensionDecreased lung distension– Increased VmaxIncreased Vmax
• Increased work of breathingIncreased work of breathing
• Increased ventilatory driveIncreased ventilatory drive
• Decreased TLC, FRC, RVDecreased TLC, FRC, RV
• V/Q mismatchV/Q mismatch
• Decreased diffusion capacityDecreased diffusion capacity

Respiratory MusclesRespiratory Muscles• InspiratoryInspiratory– DiaphragmDiaphragm• Contracts–> increased intra–abd pressure –> pushes abd outContracts–> increased intra–abd pressure –> pushes abd out
–> pushes lower rib cage and chest wall –> pushes lower rib cage and chest wall outout
• Contractility best with low lung volumesContractility best with low lung volumes– Accessory musclesAccessory muscles (SCM) (SCM)• Recruited during increased ventilatory demandsRecruited during increased ventilatory demands• Elevate rib cageElevate rib cage
• ExpiratoryExpiratory– Abdominal musclesAbdominal muscles• Increase abd pressure, displace diaphragm upwardIncrease abd pressure, displace diaphragm upward

Pulmonary Function TestingPulmonary Function Testing• Dynamic Lung FunctionDynamic Lung Function– SpirometrySpirometry– Flow loopsFlow loops– Maximum voluntary ventilationMaximum voluntary ventilation
• Static Lung FunctionStatic Lung Function– Lung volumesLung volumes– Lung capacitiesLung capacities
• Gas exchangeGas exchange– Diffusion capacity (CO)Diffusion capacity (CO)– Arterial blood gasesArterial blood gases

Indications For Pulmonary Function TestingIndications For Pulmonary Function Testing
• Assess SOBAssess SOB
• Determine presence/degree of pulmonary diseaseDetermine presence/degree of pulmonary disease
• Determine pathophysiology of pulmonary diseaseDetermine pathophysiology of pulmonary disease
• Assess course, prognosis and response to therapyAssess course, prognosis and response to therapy
• Assess disabilityAssess disability

Dynamic Lung Function AbnormalitiesDynamic Lung Function Abnormalities
• Obstructive Lung DiseasesObstructive Lung Diseases– Decreased FEVDecreased FEV11/FVC/FVC
– Decreased Vmax (FEFDecreased Vmax (FEF25–25–
7575,FEF,FEF5050))
– Inward–bowed decrease slope Inward–bowed decrease slope of exp flow–volume loopof exp flow–volume loop
• Restrictive Lung DiseaseRestrictive Lung Disease– Decreased FVC and FEVDecreased FVC and FEV11
– Normal to high FEVNormal to high FEV11/FVC/FVC
– Preserved Vmax (FEFPreserved Vmax (FEF25–25–
7575,FEF,FEF5050))
– Outward–bowed increase slope Outward–bowed increase slope of exp flow–volume loopof exp flow–volume loop

PFT Classification of Pulmonary DiseasesPFT Classification of Pulmonary Diseases
• Obstructive Lung DiseaseObstructive Lung Disease– Chronic BronchitisChronic Bronchitis
– EmphysemaEmphysema
– AsthmaAsthma
– Acute BronchitisAcute Bronchitis
– BronchiectasisBronchiectasis
– Bronchiolitis ObliteransBronchiolitis Obliterans
• Restrictive Lung DiseaseRestrictive Lung Disease– PulmonaryPulmonary
• Pulmonary FibrosisPulmonary Fibrosis• Pulmonary EdemaPulmonary Edema• Focal Lung DiseaseFocal Lung Disease
– TumorTumor– PneumoniaPneumonia– AtelectasisAtelectasis
• Lung ResectionLung Resection– Extra–PulmonaryExtra–Pulmonary
• ObesityObesity• KyphoscoliosisKyphoscoliosis• Neuromuscular DiseaseNeuromuscular Disease• Pleural EffusionPleural Effusion

Spirometry in Pulmonary DiseasesSpirometry in Pulmonary Diseases
ObstructiveObstructiveRestrictiveRestrictive
FVCFVC
FEVFEV11
FEVFEV11/FVC/FVC
FEFFEF5050
MVVMVV

ObstructiveObstructiveRestrictiveRestrictive
TLCTLC
VCVC
FRCFRC
RVRV
DLDLCOCO
Lung Volumes in Pulmonary DiseasesLung Volumes in Pulmonary Diseases

Respiratory FailureRespiratory Failure• DefinitionsDefinitions– Hypoxemic respiratory failure = PaOHypoxemic respiratory failure = PaO22 < 50 mmHg < 50 mmHg
– Hypercapnic respiratory failure = PaCOHypercapnic respiratory failure = PaCO22 > 50 mmHg > 50 mmHg
• Mechanisms of HypoxemiaMechanisms of Hypoxemia– HypoventilationHypoventilation– V/Q MismatchV/Q Mismatch– Pulmonary ShuntsPulmonary Shunts

Hypoventilatory Respiratory FailureHypoventilatory Respiratory Failure
• Due to inappropriate volume and/or frequency of Due to inappropriate volume and/or frequency of respirations respirations
• Increased PaCOIncreased PaCO22 with concomitant decrease PaO with concomitant decrease PaO22
• Acutely causes: acidosis, pulmonary hypertensionAcutely causes: acidosis, pulmonary hypertension
• CausesCauses– CNS disease: any destructive processCNS disease: any destructive process
– Endocrine/metabolic: hypothyroidism, metabolic alkalosisEndocrine/metabolic: hypothyroidism, metabolic alkalosis
– Neuromuscular: lesions of anterior horn cells, peripheral nerves, Neuromuscular: lesions of anterior horn cells, peripheral nerves, motor end plate, muscle itselfmotor end plate, muscle itself
– Structural: COPD, kyphoscoliosis, obesityStructural: COPD, kyphoscoliosis, obesity

V/Q Mismatch Respiratory FailureV/Q Mismatch Respiratory Failure• The most common respiratory failureThe most common respiratory failure• Usually with some hypoventilationUsually with some hypoventilation• Ideal gas exchange occurs with a V/Q ratio of 0.8Ideal gas exchange occurs with a V/Q ratio of 0.8– 4L/min alveolar ventilation and 5l/min cardiac output4L/min alveolar ventilation and 5l/min cardiac output
• If V/Q decreasesIf V/Q decreases– Less air reaches alveoli per given amount of perfusionLess air reaches alveoli per given amount of perfusion– Less exchange of OLess exchange of O22 and CO and CO22– Alveolar end–capillary POAlveolar end–capillary PO22 drops and PCO drops and PCO22 increases increases– ““Healthier” alveoli can compensate for COHealthier” alveoli can compensate for CO22 but not O but not O22– ABG shows low PaOABG shows low PaO22 and low PaCO and low PaCO22
• If V/Q increasesIf V/Q increases– More air reaches alveoli per given amount of perfusionMore air reaches alveoli per given amount of perfusion– More exchange of OMore exchange of O22 and CO and CO22– Alveolar end–capillary POAlveolar end–capillary PO22 increases and PCO increases and PCO22 drops drops– OO2 2 dissociation curve flat at high levels, can’t compensate dissociation curve flat at high levels, can’t compensate

Pulmonary Shunt Respiratory FailurePulmonary Shunt Respiratory Failure• Completely unventilated alveoli (extreme V/Q mismatch)Completely unventilated alveoli (extreme V/Q mismatch)
• CausesCauses– Atelectasis, edema, consolidation, ARDSAtelectasis, edema, consolidation, ARDS
• Venous blood is “shunted” from pulmonary into systemic Venous blood is “shunted” from pulmonary into systemic arterial system without getting oxygenatedarterial system without getting oxygenated
• V/Q ~ 0 (no ventilation to a perfused alveolus)V/Q ~ 0 (no ventilation to a perfused alveolus)
• Results in hypoxemia and hypocapnia like V/Q mismatchResults in hypoxemia and hypocapnia like V/Q mismatch

Clinical Approach to Respiratory FailureClinical Approach to Respiratory Failure
• What’s the PaCOWhat’s the PaCO22??– If normal or low –> excludes hypoventilationIf normal or low –> excludes hypoventilation– If high, compute alveolar–arterial OIf high, compute alveolar–arterial O22 gradient gradient
• Calculating the A–a gradientCalculating the A–a gradient– PaOPaO22 is measured via an arterial blood gas is measured via an arterial blood gas– PAOPAO22 is calculated is calculated• (Pb – PH(Pb – PH22O)FIOO)FIO2 2 – PACO– PACO22/r/r• (747 – 47)0.21 – PaCO(747 – 47)0.21 – PaCO22 x 1.2 x 1.2• 147 – (PaCO147 – (PaCO22 x 1.2) x 1.2)
– Normal gradient is 10–15 mmHgNormal gradient is 10–15 mmHg– If increased = poor gas exchange = V/Q mismatch or shuntIf increased = poor gas exchange = V/Q mismatch or shunt

Treatment of Respiratory Failure By TypeTreatment of Respiratory Failure By Type
TypeType TreatmentTreatmentHypoventilationHypoventilation Mechanical ventilationMechanical ventilation
V/Q mismatchV/Q mismatch Controlled increased FIOControlled increased FIO22
Target PAOTarget PAO22 = 50–60 mmHg = 50–60 mmHg
Bronchodilators, antibiotics, Rx CHFBronchodilators, antibiotics, Rx CHF
ShuntingShunting Mechanical ventilationMechanical ventilation
Positive End–Expiratory Pressure (PEEP)Positive End–Expiratory Pressure (PEEP)
Target PAOTarget PAO22 = 50–60 mmHg = 50–60 mmHg
Target FIOTarget FIO22 < 60% < 60%

Respiratory Acidosis and AlkalosisRespiratory Acidosis and Alkalosis• Acute Respiratory AcidosisAcute Respiratory Acidosis– pH decreases 0.08 pH units / 10 mmHg PCOpH decreases 0.08 pH units / 10 mmHg PCO22 increase increase– HCOHCO33
–– increases 1 meq/L / 10 mmHg PCO increases 1 meq/L / 10 mmHg PCO22 increase increase• Compensated (Chronic) Respiratory AcidosisCompensated (Chronic) Respiratory Acidosis– pH decreases 0.03 pH units / 10 mmHg PCOpH decreases 0.03 pH units / 10 mmHg PCO22 increase increase– HCOHCO33
–– increases 3.5 meq/L / 10 mmHg PCO increases 3.5 meq/L / 10 mmHg PCO22 increase increase• Acute Respiratory AlkalosisAcute Respiratory Alkalosis– pH increases 0.08 pH units / 10 mmHg PCOpH increases 0.08 pH units / 10 mmHg PCO22 decrease decrease– HCOHCO33
–– decreases 2 meq/L / 10 mmHg PCO decreases 2 meq/L / 10 mmHg PCO22 decrease decrease• Compensated (Chronic) Respiratory AlkalosisCompensated (Chronic) Respiratory Alkalosis– pH usually normalpH usually normal– HCOHCO33
–– decreases 5.0 meq/L / 10 mmHg PCO decreases 5.0 meq/L / 10 mmHg PCO22 decrease decrease

Consequences of Acute CO2 RetentionConsequences of Acute CO2 Retention
• AcidosisAcidosis– Impaired tissue metabolismImpaired tissue metabolism
• Cerebral VasodilationCerebral Vasodilation– Cerebral edemaCerebral edema
• Pulmonary VasoconstrictionPulmonary Vasoconstriction– Pulmonary hypertension Pulmonary hypertension
• CO2 NarcosisCO2 Narcosis– Lethargy –> comaLethargy –> coma
• HypoxemiaHypoxemia– Organ dysfunctionOrgan dysfunction

DyspneaDyspnea• DefinitionDefinition– Synonyms: Breathlessness, shortness of breath (SOB), Synonyms: Breathlessness, shortness of breath (SOB),
difficulty in breathing (DIB)difficulty in breathing (DIB)– Uncomfortable awareness of breathing difficultyUncomfortable awareness of breathing difficulty
• Pathophysiologic CausePathophysiologic Cause– Discrepancy between the drive to breath and the level of Discrepancy between the drive to breath and the level of
ventilation achieved.ventilation achieved.

Acute And Chronic DyspneaAcute And Chronic Dyspnea• Acute DyspneaAcute Dyspnea– Pulmonary edemaPulmonary edema
– AsthmaAsthma
– Chest wall injuryChest wall injury
– PneumothoraxPneumothorax
– Pulmonary embolismPulmonary embolism
– PneumoniaPneumonia
– ARDSARDS
– Pleural effusionPleural effusion
– Pulmonary hemorrhagePulmonary hemorrhage
• Chronic, Progressive DyspneaChronic, Progressive Dyspnea– COPDCOPD– CHFCHF– Interstitial FibrosisInterstitial Fibrosis– AsthmaAsthma– EffusionsEffusions– Thromboembolic diseaseThromboembolic disease– Pulmonary vascular diseasePulmonary vascular disease– Psychogenic dyspneaPsychogenic dyspnea– Anemia (Hb < 7.0)Anemia (Hb < 7.0)– Tracheal stenosisTracheal stenosis– Hypersensitivity disordersHypersensitivity disorders

Systemic vs. Pulmonary CirculationSystemic vs. Pulmonary Circulation
• Systemic CirculationSystemic Circulation– Normal pressures = 120/80Normal pressures = 120/80
– SVR = 19.6 torr/L/minSVR = 19.6 torr/L/min
• Pulmonary CirculationPulmonary Circulation– Normal pressures = 25/15Normal pressures = 25/15
– SVR = 2.6 torr/L/minSVR = 2.6 torr/L/min

Pulmonary Vascular ResistancePulmonary Vascular Resistance
• Normal parametersNormal parameters– Pressures = 25/15Pressures = 25/15– Vascular resistance = 2.6 Vascular resistance = 2.6
torr/L/mintorr/L/min
• Decreased vascular resistanceDecreased vascular resistance– Parasympathetic toneParasympathetic tone– AcetylcholineAcetylcholine– Beta–2 agonistsBeta–2 agonists– BradykininBradykinin
– Prostaglandins: PGEProstaglandins: PGE1,1, PGI PGI22
– Nitric oxideNitric oxide
• Increased vascular resistanceIncreased vascular resistance– Sympathetic toneSympathetic tone
– Prostaglandins: PGFProstaglandins: PGF2a,2a, PGF PGF22
– ThromboxaneThromboxane
– AngiotensinAngiotensin
– HistamineHistamine
– SerotoninSerotonin
– Alveolar hypoxia or hypercapniaAlveolar hypoxia or hypercapnia
– AcidosisAcidosis

Pulmonary Hypertension: EtiologiesPulmonary Hypertension: Etiologies• Increased Left Atrial PressureIncreased Left Atrial Pressure– Congestive heart failureCongestive heart failure– Mitral stenosisMitral stenosis
• Increased Pulmonary FlowIncreased Pulmonary Flow– Left to right shuntLeft to right shunt
• Increased Pulmonary Vascular ResistanceIncreased Pulmonary Vascular Resistance– VasoconstrictionVasoconstriction• HypoxiaHypoxia
– ObstructiveObstructive• Primary pulmonary hypertension Primary pulmonary hypertension • Pulmonary embolism (clot, tumor, fat, parasite)Pulmonary embolism (clot, tumor, fat, parasite)
– ObliterativeObliterative• EmphysemaEmphysema• Pulmonary fibrosisPulmonary fibrosis

Pulmonary Hypertension: SignsPulmonary Hypertension: Signs
• Heart ExamHeart Exam– Increased PIncreased P22
– Wide split of SWide split of S22
– R ventricular heaveR ventricular heave
– SS44
• PressuresPressures– Increased R ventricular end–diastolic pressureIncreased R ventricular end–diastolic pressure– Increased RA pressureIncreased RA pressure– Increased CVPIncreased CVP

Risk Factors for DVT/Pulmonary EmbolismRisk Factors for DVT/Pulmonary Embolism
• Venous StasisVenous Stasis– Immobility: age, obesity, bed rest, trauma, surgery, neuro DxImmobility: age, obesity, bed rest, trauma, surgery, neuro Dx– Heart disease: CHF, atrial arrhythmia, myocardial infarctionHeart disease: CHF, atrial arrhythmia, myocardial infarction– PregnancyPregnancy
• Vein Wall InjuryVein Wall Injury– Prior DVTPrior DVT– Pelvic, hip, leg fracture or surgeryPelvic, hip, leg fracture or surgery
• Hypercoagulable StatesHypercoagulable States– MalignanciesMalignancies– Estrogen: pregnancy, exogenousEstrogen: pregnancy, exogenous– Nephrotic syndromeNephrotic syndrome– Hereditary: Ptn C and S deficiencies, factor V Leiden, homocystinemia, Hereditary: Ptn C and S deficiencies, factor V Leiden, homocystinemia,
prothrombin gene mutations, high factor levels, antiphospholipid Abprothrombin gene mutations, high factor levels, antiphospholipid Ab

Pulmonary Embolism: PathophysiologyPulmonary Embolism: Pathophysiology• Release of Platelet FactorsRelease of Platelet Factors– Serotonin and thromboxane ASerotonin and thromboxane A22
– Vasoconstriction –> pulmonary HTN, RV dysfunction, chest pain, low BP, Vasoconstriction –> pulmonary HTN, RV dysfunction, chest pain, low BP, hypoxemiahypoxemia
• Decreased alveolar perfusionDecreased alveolar perfusion– Increased dead space (increased V/Q) –> hypoxemia and hypocapniaIncreased dead space (increased V/Q) –> hypoxemia and hypocapnia
– Reflex bronchoconstriction –> wheezingReflex bronchoconstriction –> wheezing
• Loss of surfactantLoss of surfactant– Atelectasis, alveolar edema and bleed –> SOB, crackles, chest painAtelectasis, alveolar edema and bleed –> SOB, crackles, chest pain
– Decreased V/Q –> hypoxemiaDecreased V/Q –> hypoxemia
– Irritant and J receptor stimulation –> hyperventilation and SOB Irritant and J receptor stimulation –> hyperventilation and SOB

Pulmonary Embolism: SymptomsPulmonary Embolism: Symptoms
• DyspneaDyspnea
• Pleuritic chest painPleuritic chest pain
• CoughCough
• HemoptysisHemoptysis
• SyncopeSyncope

Pathophysiology of Chronic Pulmonary HTNPathophysiology of Chronic Pulmonary HTN
PhenomenonPhenomenon Physical Exam (Sx)Physical Exam (Sx)Increased pulmonary artery pressure –>Increased pulmonary artery pressure –> Increased PIncreased P22
Right ventricular hypertrophy –> Right ventricular hypertrophy –> RV SRV S44
Right heart failure –> Right heart failure –> RV SRV S33
Increased JVP, edemaIncreased JVP, edemaHepatomegalyHepatomegaly(Fatigue and dyspnea)(Fatigue and dyspnea)

Sleep MedicineSleep Medicine

Sleep ArchitectureSleep Architecture(Cycles every 90–120 minutes)(Cycles every 90–120 minutes)
• Non–Rapid Eye Movement (NREM) Sleep Non–Rapid Eye Movement (NREM) Sleep – Stage 1: Transition from wakefulnessStage 1: Transition from wakefulness• EEG fast theta (4–7 Hz); easily aroused and deny being asleepEEG fast theta (4–7 Hz); easily aroused and deny being asleep
– Stage 2: Intermediate sleep, 40–50% of total sleep timeStage 2: Intermediate sleep, 40–50% of total sleep time• EEG: slower and higher amplitude, sleep spindles: 12–14 Hz bursts, EEG: slower and higher amplitude, sleep spindles: 12–14 Hz bursts,
k–complexes: double negative wavek–complexes: double negative wave– Stage 3 and 4: Deep sleep, 20% of sleepStage 3 and 4: Deep sleep, 20% of sleep• EEG: High amplitude, slow (1–3 Hz)EEG: High amplitude, slow (1–3 Hz)
• Rapid Eye Movement (REM) SleepRapid Eye Movement (REM) Sleep– EEGEEG: Low voltage, high frequency ~ wakefulness: Low voltage, high frequency ~ wakefulness– EMGEMG: atonic: atonic– EYEEYE: rapid eye movements: rapid eye movements

Determinants of SleepDeterminants of Sleep• HomeostasisHomeostasis– Enough sleep = amount that allows alertness for the dayEnough sleep = amount that allows alertness for the day– ~ 8 hours, yet highly variable~ 8 hours, yet highly variable
• Circadian RhythmsCircadian Rhythms– Suprachiasmatic nucleus near hypothalamusSuprachiasmatic nucleus near hypothalamus– Receives input via the retino–hypothalamic tractReceives input via the retino–hypothalamic tract
• Changes With AgeChanges With Age– Arousals increase, deep sleep decreases, latency increasesArousals increase, deep sleep decreases, latency increases

Obstructive Sleep ApneaObstructive Sleep Apnea• DefinitionDefinition– Repetitive episodes of upper airway obstructionRepetitive episodes of upper airway obstruction– Frequent apnea and hypoxemiaFrequent apnea and hypoxemia
• SymptomsSymptoms– Nighttime symptomsNighttime symptoms• Snoring, apnea/gasping, flailing of limbs, frequent awakenings, GE reflux Snoring, apnea/gasping, flailing of limbs, frequent awakenings, GE reflux
urinationurination
– Daytime symptomsDaytime symptoms• Tiredness upon awakening, morning HA, excessive sleepiness, loss of Tiredness upon awakening, morning HA, excessive sleepiness, loss of
libido/impotencelibido/impotence• MVA, work accidents, school/work problems, social embarrassment, MVA, work accidents, school/work problems, social embarrassment,
marital problems, memory/concentration trouble, depressionmarital problems, memory/concentration trouble, depression

OSA: Predisposing FactorsOSA: Predisposing Factors
• AgeAge
• ObesityObesity
• M>F 2:1M>F 2:1
• Upper airway obstructionUpper airway obstruction
• Craniofacial anomaliesCraniofacial anomalies
• MedicationsMedications
• AlcoholAlcohol
• SmokingSmoking
• GeneticsGenetics

OSA: Physical ExamOSA: Physical Exam• Short fat neckShort fat neck
• ObesityObesity
• Upper airway narrowing Upper airway narrowing – Large tonsilsLarge tonsils– Enlarged uvulaEnlarged uvula– Long soft palateLong soft palate
• Micrognathia/retrognathiaMicrognathia/retrognathia

Sleep Apnea: Clinicopathologic EffectsSleep Apnea: Clinicopathologic Effects
• AcuteAcute– Brady/tachyarrhythmiasBrady/tachyarrhythmias
• ChronicChronic– Systemic HTNSystemic HTN– Pulmonary HTNPulmonary HTN– CHFCHF– Myocardial infarctionMyocardial infarction– StrokeStroke– Hypercapneic respiratory failureHypercapneic respiratory failure

OSA: Polysomnographic FindingsOSA: Polysomnographic Findings
• ApneasApneas– >> 30 per hour 30 per hour– Terminated by arousalTerminated by arousal– Often occur over 50% of sleep timeOften occur over 50% of sleep time
• ArchitectureArchitecture– DestroyedDestroyed– Decreased Stage 3 and 4Decreased Stage 3 and 4– Decreased REMDecreased REM

OSA: TherapyOSA: Therapy• Discontinue medications and alcoholDiscontinue medications and alcohol
• Weight lossWeight loss
• Tennis ball on backTennis ball on back
• Nasal CPAPNasal CPAP
• Surgical correctionSurgical correction– UvulopharyngoplatoplastyUvulopharyngoplatoplasty– TracheotomyTracheotomy

Narcolepsy ManifestationsNarcolepsy Manifestations(Due to sudden onset of REM sleep)(Due to sudden onset of REM sleep)
• CataplexyCataplexy– Bilateral loss of muscle tone after strong emotionBilateral loss of muscle tone after strong emotion
• Laughter, anger, amusement, exertionLaughter, anger, amusement, exertion
• Last seconds to minutesLast seconds to minutes
• Hypnagogic hallucinationsHypnagogic hallucinations– Vivid nightmares at sleep onsetVivid nightmares at sleep onset
• Sleep ParalysisSleep Paralysis– Unable to move at sleep onset (hypnagogic) or offset (hypnapompic)Unable to move at sleep onset (hypnagogic) or offset (hypnapompic)
• Sleep AttacksSleep Attacks– Episodic overwhelming sleepiness during the dayEpisodic overwhelming sleepiness during the day

Multiple Sleep Latency Criteria for NarcolepsyMultiple Sleep Latency Criteria for Narcolepsy
• Mean sleep latency of < 8 minutesMean sleep latency of < 8 minutes
• > 2 sleep onset REM periods during naps> 2 sleep onset REM periods during naps
• No other apparent cause (i.e. sleep deprivation)No other apparent cause (i.e. sleep deprivation)

Narcolepsy TreatmentNarcolepsy Treatment• BehavioralBehavioral– Structured sleep schedule with napsStructured sleep schedule with naps– Diet: avoid heavy mealsDiet: avoid heavy meals– Physical activity during the dayPhysical activity during the day
• PharmacologicalPharmacological– Sleep attacks: pemoline, methylphenidate, dex–Sleep attacks: pemoline, methylphenidate, dex–
amphetamine, metamphetamine, modafinilamphetamine, metamphetamine, modafinil– Cataplexy: TCA’s, fluoxetine, GHBCataplexy: TCA’s, fluoxetine, GHB
• PsychosocialPsychosocial

Sports MedicineSports Medicine

Sports Medicine: Ligament SprainsSports Medicine: Ligament Sprains• Definition of a ligamentDefinition of a ligament– Dense fibrous collagen, connects bone to boneDense fibrous collagen, connects bone to bone
• Grading of sprain injuriesGrading of sprain injuries– Grade 1: partial tear, no functional laxityGrade 1: partial tear, no functional laxity
heals in 2–4 weeksheals in 2–4 weeks– Grade 2: partial tear, some laxity, intact endpointGrade 2: partial tear, some laxity, intact endpoint
heals in 4–6 weeksheals in 4–6 weeks– Grade 3: complete ligament injuryGrade 3: complete ligament injury
heals in 2–3 monthsheals in 2–3 months• EvaluationEvaluation– History of injuryHistory of injury– Exam for site of pain and laxityExam for site of pain and laxity– ImageImage

The Ligament Healing ProcessThe Ligament Healing Process• Hemorrhagic PhaseHemorrhagic Phase– ImmediateImmediate– Clot forms in injured areaClot forms in injured area
• Inflammatory PhaseInflammatory Phase– 1–2 weeks1–2 weeks– WBCs enter and phagocytize debrisWBCs enter and phagocytize debris– Clot converted to granulation tissueClot converted to granulation tissue
• Reparative PhaseReparative Phase– 1–8 weeks1–8 weeks– Fibroblasts lay down extracellular matrix and immature collagen fibersFibroblasts lay down extracellular matrix and immature collagen fibers
• Remodeling PhaseRemodeling Phase– 4 weeks to 1 year4 weeks to 1 year– Maturation to mature collagenMaturation to mature collagen

Treatment of Ligament SprainsTreatment of Ligament Sprains
• RICERICE– Rest, Ice, Compression, ElevationRest, Ice, Compression, Elevation
• ImmobilizationImmobilization– Some initially yet not too long (prevents full healing)Some initially yet not too long (prevents full healing)
• Anti–inflammatoriesAnti–inflammatories– OK, but need to allow some inflammationOK, but need to allow some inflammation
• ProlotherapyProlotherapy– Injections of sugar/salt solutions to increase inflammationInjections of sugar/salt solutions to increase inflammation

Sports Medicine: Tendon StrainsSports Medicine: Tendon Strains• Definition of a tendonDefinition of a tendon
– Dense fibrous collagen, connects muscle to boneDense fibrous collagen, connects muscle to bone
• Grading of strain injuriesGrading of strain injuries– Grade 1: partial tear, no weaknessGrade 1: partial tear, no weakness– Grade 2: partial tear, some weaknessGrade 2: partial tear, some weakness– Grade 3: complete tear, loss of motor function, palpable defectGrade 3: complete tear, loss of motor function, palpable defect
• Evaluation and diagnosisEvaluation and diagnosis– History of injuryHistory of injury– Exam for functionExam for function– Image usually not necessaryImage usually not necessary
• Repair mechanismRepair mechanism– Same as for sprainsSame as for sprains– Muscles will atrophy from disuseMuscles will atrophy from disuse
• TreatmentTreatment– RICE, ? NSAIDs, steroid injections vs. prolotherapyRICE, ? NSAIDs, steroid injections vs. prolotherapy– Surgical repairSurgical repair

TendinosisTendinosis
• Tendon degeneration from tendon overuseTendon degeneration from tendon overuse
• Minimal inflammatory cellsMinimal inflammatory cells
• Normal repair does not occurNormal repair does not occur

DislocationDislocation• BackgroundBackground– Usually due to major traumaUsually due to major trauma– Named by distal bone over proximal boneNamed by distal bone over proximal bone– Common injury to multiple ligamentsCommon injury to multiple ligaments
• ExaminationExamination– Gross joint deformityGross joint deformity– Check neurovascular integrityCheck neurovascular integrity
• TreatmentTreatment– Emergent joint reductionEmergent joint reduction

Bone Fractures: DescriptionsBone Fractures: Descriptions
• Bone nameBone name
• ComminutionComminution– Number of piecesNumber of pieces
• AngulationAngulation– Which way is it pointingWhich way is it pointing
• TranslationTranslation– Bones separated and not Bones separated and not
overlappingoverlapping
• ShorteningShortening
• Other DescriptorsOther Descriptors– Segmental (a series of Fx)Segmental (a series of Fx)
– ImpactionImpaction
– Avulsion (bone pulled off)Avulsion (bone pulled off)
– PatternPattern• spiral/oblique/transversespiral/oblique/transverse

Fracture Healing and TreatmentFracture Healing and Treatment
• Day 1 – 3Day 1 – 3– Bleeding and clot formationBleeding and clot formation
• Week 1Week 1– Macrophage migrationMacrophage migration
• Weeks 1 – 6Weeks 1 – 6– Clot reorganizes into callousClot reorganizes into callous
• Months 2 – 12Months 2 – 12– Remodeling to mature boneRemodeling to mature bone
• TreatmentTreatment– RICERICE
– ImmobilizeImmobilize
– NSAIDsNSAIDs
– Bone stimulationBone stimulation

Developmental Bone DiseaseDevelopmental Bone Disease

AchondroplasiaAchondroplasia
• GeneticsGenetics– Autosomal dominantAutosomal dominant– Mutation on chromosome 4 of fibroblast growth factor Mutation on chromosome 4 of fibroblast growth factor
receptor 3 (FGFR–3) (Arg –> gly)receptor 3 (FGFR–3) (Arg –> gly)
• PathophysiologyPathophysiology– Failure of enchondrial bone ossification (long bones)Failure of enchondrial bone ossification (long bones)– Intramembranous ossification (skull/spine) normalIntramembranous ossification (skull/spine) normal– Thus, normal head and trunk size, small arms and legsThus, normal head and trunk size, small arms and legs

Spina BifidaSpina Bifida• PathophysiologyPathophysiology– Failure of posterior neural tube closure (weeks 3 – 6)Failure of posterior neural tube closure (weeks 3 – 6)– 1: 1,000 births1: 1,000 births– Decreased by prenatal AFP screening and folate administrationDecreased by prenatal AFP screening and folate administration
• Clinical manifestationsClinical manifestations– OccultaOcculta: occult failure of arches to fuse, no Sx, hair tuft: occult failure of arches to fuse, no Sx, hair tuft– MeningoceleMeningocele: Meninges herniate through defect, no neurologic : Meninges herniate through defect, no neurologic
defectdefect– MeningomyeloceleMeningomyelocele: Meninges and cord herniate, leg paralysis : Meninges and cord herniate, leg paralysis
and hydrocephalusand hydrocephalus

Other Congenital Bone/Joint DiseasesOther Congenital Bone/Joint Diseases• Down’s SyndromeDown’s Syndrome– Weak C1–C2 ligaments –> subluxationWeak C1–C2 ligaments –> subluxation
• Osteogenesis imperfectaOsteogenesis imperfecta– Defective type I collagenDefective type I collagen– Brittle bones, osteoporosis, ± transparent scleraBrittle bones, osteoporosis, ± transparent sclera
• Congenital clubfootCongenital clubfoot– 1:800 births1:800 births– Adducted, inverted forefootAdducted, inverted forefoot– No motor or nerve deficitNo motor or nerve deficit
• Developmental Dysplasia of the HipDevelopmental Dysplasia of the Hip– Due to external or inherited forcesDue to external or inherited forces
• Legg Calve Perthes DiseaseLegg Calve Perthes Disease– Avascular necrosis of femoral headAvascular necrosis of femoral head
• Slipped Capital Femoral EpiphysisSlipped Capital Femoral Epiphysis

ScoliosisScoliosis• Lateral curvature of spineLateral curvature of spine
• Measured by Cobb’s angle –>Measured by Cobb’s angle –>
• TreatmentTreatment– Immature spineImmature spine
• Brace if > 25Brace if > 25oo
– Mature spineMature spine• Fusion if > 40Fusion if > 40oo
ScoliosisScoliosis KyphosisKyphosis

Breast DiseaseBreast Disease

Nipple DischargeNipple Discharge• NormalNormal– Physiologic, pregnancyPhysiologic, pregnancy
• SpontaneousSpontaneous– Papilloma 70%Papilloma 70%– Ductal ectasia + fibrocystic disease (20%)Ductal ectasia + fibrocystic disease (20%)– Cancer 10%Cancer 10%
• WorkupWorkup– ExamExam– MammogramMammogram

Breast Cancer: EpidemiologyBreast Cancer: Epidemiology
• The most common female non–skin cancerThe most common female non–skin cancer• The second most common cancer death (lung)The second most common cancer death (lung)• The most common cause of death in women 45–55The most common cause of death in women 45–55• Known Risk FactorsKnown Risk Factors– Sex, age, geneticsSex, age, genetics– Proliferative breast diseases with or without atypiaProliferative breast diseases with or without atypia– Lobular carcinoma in situLobular carcinoma in situ– Prolonged estrogenProlonged estrogen• menarche, menopause, parity, exogenousmenarche, menopause, parity, exogenous

The National Surgical Adjuvant Breast ProjectThe National Surgical Adjuvant Breast Project Antiestrogens and breast cancerAntiestrogens and breast cancer
• The StudyThe Study– 13,388 woman at risk for breast CA13,388 woman at risk for breast CA• Over 60 or 35–59 with 5–year risk > 1.66%, lobular CA in situOver 60 or 35–59 with 5–year risk > 1.66%, lobular CA in situ
– Randomized to tamoxifen vs. placebo x 5 yearsRandomized to tamoxifen vs. placebo x 5 years
• The resultsThe results– Less: breast CA by 50%, bone FxLess: breast CA by 50%, bone Fx– More: Endometrial CA x 2.5, DVT/PEMore: Endometrial CA x 2.5, DVT/PE

Prognostic Factors for Breast CAPrognostic Factors for Breast CA
• Number of axillary lymph nodesNumber of axillary lymph nodes
• Tumor sizeTumor size
• TNM stageTNM stage
• Histologic gradeHistologic grade
• Nuclear gradeNuclear grade
• Absence of estrogen and/or progestin receptorsAbsence of estrogen and/or progestin receptors
• HER–2 positivity (coded for by c-erbB-2 oncogene)HER–2 positivity (coded for by c-erbB-2 oncogene)

Treatment of Invasive Breast CATreatment of Invasive Breast CA• Breast Conserving Therapy (BCT)Breast Conserving Therapy (BCT)– Excision with clean margins and XRTExcision with clean margins and XRT
• BCT vs. mastectomyBCT vs. mastectomy– disease–free survivaldisease–free survival– overall survivaloverall survival
• Contraindications for lumpectomyContraindications for lumpectomy– Locally far advanced CA by exam or mammogramLocally far advanced CA by exam or mammogram– Multicentric carcinomaMulticentric carcinoma– Persistent (+) margins during surgeryPersistent (+) margins during surgery– Pregnancy (1Pregnancy (1stst and 2 and 2ndnd trimester) trimester)– CTD (esp. scleroderma)CTD (esp. scleroderma)– Large tumor:breast ratioLarge tumor:breast ratio

Adjuvant Systemic Therapy Adjuvant Systemic Therapy for Breast Cancerfor Breast Cancer
• Indications for ChemotherapyIndications for Chemotherapy–Tumor > 2 cm or positive lymph nodesTumor > 2 cm or positive lymph nodes
• Indications for Hormone TherapyIndications for Hormone Therapy–Receptor positivityReceptor positivity

Family Hx Reasons to screen for BRCA1/2Family Hx Reasons to screen for BRCA1/2
• BRCA 1 or BRCA 2 mutationBRCA 1 or BRCA 2 mutation
• Breast Breast ANDAND ovarian cancer ovarian cancer
• Male breast cancerMale breast cancer
• >> 2 members < 50 with breast cancer 2 members < 50 with breast cancer
• Ashkenazi and Ashkenazi and >> 1 members < 50 with breast cancer 1 members < 50 with breast cancer
• Ashkenazi and ovarian cancerAshkenazi and ovarian cancer

Other Female MalignanciesOther Female Malignancies

Ovarian Cancer Risk FactorsOvarian Cancer Risk Factors(The most common fatal genital cancer)(The most common fatal genital cancer)
• AgeAge– Peaks at 56, declines after 80Peaks at 56, declines after 80
• ““Incessant” OvulationIncessant” Ovulation– Early menarche, late menopause, nulliparousEarly menarche, late menopause, nulliparous– Fertility drugsFertility drugs– Risk Risk declinesdeclines with OCPs with OCPs
• GeneticGenetic– Family history, BRCA 1 and BRCA 2Family history, BRCA 1 and BRCA 2– CaucasianCaucasian

Ovarian NeoplasmsOvarian Neoplasms• Epithelial (85%)Epithelial (85%)– 45:55 malignant (M) vs. benign (B)45:55 malignant (M) vs. benign (B)– Serous (M=B) > mucinous (B)> endometrioid (M), Brenner (B), Serous (M=B) > mucinous (B)> endometrioid (M), Brenner (B),
Clear cell (M), Undifferentiated (M)Clear cell (M), Undifferentiated (M)
• Germ CellGerm Cell– Teratoma (dermoid) (B); all others (M): teratocarcinoma, Teratoma (dermoid) (B); all others (M): teratocarcinoma,
dysgerminoma, endodermal sinus tumor, choriocarcinoma, dysgerminoma, endodermal sinus tumor, choriocarcinoma, embryonal cell CA, gonadoblastomaembryonal cell CA, gonadoblastoma
• StromalStromal– Granulosa cell (makes Est), Sertoli–Leydig Cell (makes Tt), Granulosa cell (makes Est), Sertoli–Leydig Cell (makes Tt),
ovarian fibroma, ovarian sarcomaovarian fibroma, ovarian sarcoma

Ovarian Cancer: ManagementOvarian Cancer: Management
• SurgerySurgery– Debulking as much as possibleDebulking as much as possible
• Adjuvant chemotherapyAdjuvant chemotherapy– If metastatic or high–riskIf metastatic or high–risk
• Radiation TherapyRadiation Therapy– DysgerminomasDysgerminomas

Endometrial CarcinomaEndometrial Carcinoma(The most common gynecologic CA in USA)(The most common gynecologic CA in USA)
• Risk FactorsRisk Factors– Unopposed estrogenUnopposed estrogen• Anovulatory cycles, nulliparous, tamoxifen, obesityAnovulatory cycles, nulliparous, tamoxifen, obesity
– FamilialFamilial• e.g. Lynch syndromee.g. Lynch syndrome
– OCPs are protectiveOCPs are protective• Clinical PresentationClinical Presentation– Abnormal uterine bleedingAbnormal uterine bleeding• Post–menopausal or heavy premenopausalPost–menopausal or heavy premenopausal
• Prognosis (5–year survivals)Prognosis (5–year survivals)– Stage 1 = 95%, Stage III–IV = 26%)Stage 1 = 95%, Stage III–IV = 26%)

Squamous Intraepithelial Neoplasia (SIN) Squamous Intraepithelial Neoplasia (SIN) and Cervical CAand Cervical CA
• SIN DefinitionSIN Definition– Dysplasia confined to the epithelium of GI/CU tractDysplasia confined to the epithelium of GI/CU tract– Gynecologic foci: cervix, endometrium, vaginalGynecologic foci: cervix, endometrium, vaginal
• RisksRisks– HPV, immunosuppressionHPV, immunosuppression– Early sex, multiple partners, high risk partners, prior STDs, high parityEarly sex, multiple partners, high risk partners, prior STDs, high parity– Smoking, low SE statusSmoking, low SE status– Other gynecologic malignanciesOther gynecologic malignancies
• Clinical ManifestationsClinical Manifestations– Usually asymptomaticUsually asymptomatic– Vaginal bleed, post–coital bleed, vaginal DCVaginal bleed, post–coital bleed, vaginal DC

Papanicolaou Smear IndicationsPapanicolaou Smear Indications
• BeginningBeginning– Age 18 or sexual activity, whichever is firstAge 18 or sexual activity, whichever is first
• FrequencyFrequency– Every year until 3 negative and not high riskEvery year until 3 negative and not high risk
• CessationCessation– Age 60 – 75Age 60 – 75– ? Total hysterectomy? Total hysterectomy

Reproductive EndocrinologyReproductive Endocrinologyand Gynecologyand Gynecology

Gonadotropin PhysiologyGonadotropin Physiology• HypothalamusHypothalamus– Pulsatile release of GnRHPulsatile release of GnRH– Stimulates pit FSH and LHStimulates pit FSH and LH– Inhibited by Est and ProgInhibited by Est and Prog
• Anterior PituitaryAnterior Pituitary– Releases FSH and LHReleases FSH and LH– Stimulates ovarian Est and ProgStimulates ovarian Est and Prog– Inhibited by Est and ProgInhibited by Est and Prog
• OvariesOvaries– Release Est and ProgRelease Est and Prog– Release androgensRelease androgens

Menstrual PhasesMenstrual Phases
Follicular PhaseFollicular Phase Luteal PhaseLuteal Phase
PituitaryPituitary FSH > LH secretionFSH > LH secretion LH surge (also FSH)LH surge (also FSH)
OvaryOvary Estradiol secretionEstradiol secretion Prog > Est secretionProg > Est secretion
Follicular maturationFollicular maturation Ovulation–>corpus Ovulation–>corpus
luteumluteum
UterusUterus ProliferativeProliferative SecretorySecretory

Ovarian Hormone SynthesisOvarian Hormone Synthesis
• Theca CellsTheca Cells– Respond to LHRespond to LH– Produce androgens from cholesterolProduce androgens from cholesterol• Androstenedione, testosteroneAndrostenedione, testosterone
• Granulosa CellsGranulosa Cells– Respond to FSHRespond to FSH– Produce estrogen from androgensProduce estrogen from androgens– Requires aromatase enzymeRequires aromatase enzyme

Abnormal Uterine BleedingAbnormal Uterine Bleeding• Dysfunctional Uterine BleedingDysfunctional Uterine Bleeding– Vaginal bleeding not associated with an anatomical source or a Vaginal bleeding not associated with an anatomical source or a
systemic disease. Usually anovulatory. Dx of exclusion.systemic disease. Usually anovulatory. Dx of exclusion.• Menorrhagia/HypermenorrheaMenorrhagia/Hypermenorrhea– Heavy cyclic bleeding (> 80 ml)Heavy cyclic bleeding (> 80 ml)
• MetrorrhagiaMetrorrhagia– Bleeding that is prolonged menstrual or intramenstrualBleeding that is prolonged menstrual or intramenstrual
• MenometrorrhagiaMenometrorrhagia– Combination of the aboveCombination of the above
• OligomenorrheaOligomenorrhea– Cycles > 35d, often unpredictableCycles > 35d, often unpredictable
• PolymenorrheaPolymenorrhea– Cycles < 21d – 24dCycles < 21d – 24d

Uterine Leiomyomatas (Myomas, Fibroids)Uterine Leiomyomatas (Myomas, Fibroids)
• EpidemiologyEpidemiology– 20% over 30, >40% over 4020% over 30, >40% over 40– African American 3–6 fold higherAfrican American 3–6 fold higher
• AnatomyAnatomy– Submucosal, intramural, subserosal, pedunculated, parasiticSubmucosal, intramural, subserosal, pedunculated, parasitic
• PathogenesisPathogenesis– Estrogen dependentEstrogen dependent
• SymptomsSymptoms– Abnormal uterine bleedingAbnormal uterine bleeding– Pelvic pain, urinary frequency, rectal discomfortPelvic pain, urinary frequency, rectal discomfort
• DiagnosisDiagnosis– PE, US, hysterosalpingogram, hysteroscopy, MRIPE, US, hysterosalpingogram, hysteroscopy, MRI
• TherapyTherapy– Hormones, minimally invasive surgery, myomectomy, hysterectomyHormones, minimally invasive surgery, myomectomy, hysterectomy

Endometriosis: ClinicalEndometriosis: Clinical• DefinitionDefinition– Presence of ectopic uterine mucosal tissuePresence of ectopic uterine mucosal tissue
• LocationsLocations– Ovarian > uterine > ureterosacral ligaments, peritoneum, Ovarian > uterine > ureterosacral ligaments, peritoneum,
retroperitoneum, bowel, pleuraretroperitoneum, bowel, pleura• PathogenesisPathogenesis– Retrograde menstruationRetrograde menstruation– Vascular or lymphatic disseminationVascular or lymphatic dissemination– Coelemic metaplasiaCoelemic metaplasia
• SymptomsSymptoms– Pain, dysmenorrhea, dyspareunia, abnormal uterine bleeding, Pain, dysmenorrhea, dyspareunia, abnormal uterine bleeding,
infertilityinfertility

Endometriosis: TreatmentEndometriosis: Treatment• ObservationObservation
• HormonalHormonal– OCPs, depo–provera, danazol, GNRH agonist, pregnancyOCPs, depo–provera, danazol, GNRH agonist, pregnancy
• SurgicalSurgical– Excision, fulguration, TAH–BSOExcision, fulguration, TAH–BSO

PubertyPuberty• Definitions and sequenceDefinitions and sequence– ThelarcheThelarche: breast development, mean age = 10: breast development, mean age = 10– AdrenarcheAdrenarche: Body hair development, mean age = 10: Body hair development, mean age = 10– MenarcheMenarche: Menses onset, mean age = 13: Menses onset, mean age = 13– Age of onset one year earlier in African AmericansAge of onset one year earlier in African Americans
• Precocious pubertyPrecocious puberty– 2.5 SD below mean age2.5 SD below mean age
• Delayed pubertyDelayed puberty– No changes at 14No changes at 14– No thelarche age 15No thelarche age 15– No menses within 2 years of thelarche and adrenarche or by age 16No menses within 2 years of thelarche and adrenarche or by age 16

MenopauseMenopause• DefinitionsDefinitions– Menopause = cessation of menstrual cycles for one yearMenopause = cessation of menstrual cycles for one year– Perimenopause = Menstrual irregularities, Sx of Est lossPerimenopause = Menstrual irregularities, Sx of Est loss– Mean age = 51 – 52Mean age = 51 – 52
• Related ovarian follicular physiologyRelated ovarian follicular physiology– Fetus has 7,000,000 folliclesFetus has 7,000,000 follicles– At menarche = 400,000 folliclesAt menarche = 400,000 follicles– At menopause = 10,000 follicles (non–functional)At menopause = 10,000 follicles (non–functional)


Primary AmenorrheaPrimary Amenorrhea((No menarche by age 16, usually genetic or anatomic)No menarche by age 16, usually genetic or anatomic)
• Chromosomal abnormalities (45%)Chromosomal abnormalities (45%)– Androgen insensitivity syndrome: 46 XY, defective Tt receptor, testes make MIFAndrogen insensitivity syndrome: 46 XY, defective Tt receptor, testes make MIF– Vanishing testes syndrome: 46 XY, failure of full testicular developmentVanishing testes syndrome: 46 XY, failure of full testicular development– Absent testes determining factor: 46 XY, no testes so no Tt or MIFAbsent testes determining factor: 46 XY, no testes so no Tt or MIF– 5–alpha reductase deficiency: 46 XY, female phenotype yet virilization after puberty 5–alpha reductase deficiency: 46 XY, female phenotype yet virilization after puberty
with deep voice, baldness, increase muscle masswith deep voice, baldness, increase muscle mass– 17–OHase deficiency: 46 XX or XY, cannot make gonadotropins, female with HTN17–OHase deficiency: 46 XX or XY, cannot make gonadotropins, female with HTN– Turner’s: 45 XO, streak ovaryTurner’s: 45 XO, streak ovary
• Physiologic delay in pregnancy (20%)Physiologic delay in pregnancy (20%)• Müellarian agenesis (15%)Müellarian agenesis (15%)
– Absence of fallopian tubes, uterus, upper 1/3 vagina Absence of fallopian tubes, uterus, upper 1/3 vagina • Transverse vaginal septum/imperforate hymen (5%)Transverse vaginal septum/imperforate hymen (5%)• Hypothalamic GnRH deficiency (5%)Hypothalamic GnRH deficiency (5%)
– 11oo: congenital (with anosmia = Kallman’s): congenital (with anosmia = Kallman’s)– 22oo: Anorexia nervosa, exercise, wt loss, stress, invasion: Anorexia nervosa, exercise, wt loss, stress, invasion
• Hypopituitarism (2%)Hypopituitarism (2%)

Approach to Primary AmenorrheaApproach to Primary Amenorrhea
• Puberty present (eugonadal, makes Est)Puberty present (eugonadal, makes Est)– Check uterine/vaginal anatomyCheck uterine/vaginal anatomy– Check karyotype, testosterone levelCheck karyotype, testosterone level– Pregnancy testPregnancy test
• Puberty absent (hypogonadal, no Est)Puberty absent (hypogonadal, no Est)– Check LH and FSH (can’t measure GnRH)Check LH and FSH (can’t measure GnRH)• Low: stress?, low BW?, pit failure?Low: stress?, low BW?, pit failure?• High: Gonadal failureHigh: Gonadal failure
– Check karyotype (XO or XY)Check karyotype (XO or XY)
– Check prolactin and TSHCheck prolactin and TSH

Secondary AmenorrheaSecondary Amenorrhea((No menses x 6 months or 3 cycles)No menses x 6 months or 3 cycles)
• Pregnancy most commonPregnancy most common• Ovarian (40%)Ovarian (40%)
– Polycystic ovary syndrome (40%)Polycystic ovary syndrome (40%)– High testosterone –> anovulation, endometrial atrophyHigh testosterone –> anovulation, endometrial atrophy– Ovarian failure (if < 40 yo = primary)Ovarian failure (if < 40 yo = primary)– Autoimmune oophoritisAutoimmune oophoritis
• Hypothalamic (35%)Hypothalamic (35%)– Functional GnRH deficiency (same reasons as under 1Functional GnRH deficiency (same reasons as under 1oo amenorrhea) amenorrhea)– InfiltrativeInfiltrative
• Pituitary (20%)Pituitary (20%)– Hyperprolactinemia (90%) –> decreased GnRHHyperprolactinemia (90%) –> decreased GnRH– Empty sella, hypothyroidism, other pituitary tumors, Sheehan’s, infiltrativeEmpty sella, hypothyroidism, other pituitary tumors, Sheehan’s, infiltrative
• Uterine (5%)Uterine (5%)– Asherman’s (>90%), endometriosisAsherman’s (>90%), endometriosis

Approach to Secondary AmenorrheaApproach to Secondary Amenorrhea• Rule out pregnancyRule out pregnancy
– ß–HCGß–HCG
• Physical examPhysical exam– R/O Asherman’sR/O Asherman’s
• Prolactin levelProlactin level– If very high, CT or MRI of pituitaryIf very high, CT or MRI of pituitary
• TSHTSH– If very high = hypothyroidismIf very high = hypothyroidism
• FSH and LHFSH and LH– If very high = ovarian failure, if < 30 –> karyotypeIf very high = ovarian failure, if < 30 –> karyotype– If low = If low = stress?, low BW?, pit failure?stress?, low BW?, pit failure?
• DHEA–S and testosteroneDHEA–S and testosterone– Only if virilized, looking for PCOSOnly if virilized, looking for PCOS
• 17OH–progesterone17OH–progesterone– Looking for congenital adrenal hyperplasiaLooking for congenital adrenal hyperplasia

Progestin Withdrawal TestProgestin Withdrawal Test• If bleeding occursIf bleeding occurs– Uterus and endometrium are intactUterus and endometrium are intact– Estrogen is sufficient, progesterone was lackingEstrogen is sufficient, progesterone was lacking– AnovulationAnovulation• Hypothalamic dysfunction (stress)Hypothalamic dysfunction (stress)• Polycystic ovarian syndromePolycystic ovarian syndrome• Late–Onset Congenital Adrenal Hyperplasia (17–OH)Late–Onset Congenital Adrenal Hyperplasia (17–OH)
• If bleeding does not occurIf bleeding does not occur– Insufficient estrogen or uterine causeInsufficient estrogen or uterine cause– Hypothalamic dysfunction (stress)Hypothalamic dysfunction (stress)– Pituitary dysfunction Pituitary dysfunction – Uterine causeUterine cause

GeriatricsGeriatrics

Pathophysiology of BedrestPathophysiology of Bedrest
• PulmonaryPulmonary– Decreased oxygenationDecreased oxygenation
– Decreased ability to clear Decreased ability to clear secretionssecretions
• VascularVascular– Venous stasis –> DVT –> PEVenous stasis –> DVT –> PE
– OrthostasisOrthostasis
• SkinSkin– Pressure ulcersPressure ulcers
• MusculoskeletalMusculoskeletal– Atrophy and contracturesAtrophy and contractures
– OsteoporosisOsteoporosis
• ElectrolytesElectrolytes– Hypercalciuria –> stonesHypercalciuria –> stones
• GastrointestinalGastrointestinal– Reflux esophagitisReflux esophagitis
– ConstipationConstipation
– AnorexiaAnorexia

Geriatrics: Vision Changes in the ElderlyGeriatrics: Vision Changes in the Elderly• Visual AcuityVisual Acuity– Decreased accommodation (presbyopia)Decreased accommodation (presbyopia)
• Color VisionColor Vision– Lens yellows, blue green blendingLens yellows, blue green blending
• Extraocular MusclesExtraocular Muscles– WeakenWeaken
• Tear ductsTear ducts– Less tear production –> corneal irritationLess tear production –> corneal irritation
• Illumination disturbancesIllumination disturbances– Require more light yet more glareRequire more light yet more glare– Poor night visionPoor night vision

Geriatrics: Hearing Changes in the ElderlyGeriatrics: Hearing Changes in the Elderly
• PresbycusisPresbycusis– Age–related hearing loss, usually > 65 yoAge–related hearing loss, usually > 65 yo– Higher frequency lossHigher frequency loss– Loss of speech discriminationLoss of speech discrimination
• Interview techniquesInterview techniques– Turn off all background noiseTurn off all background noise– Sit them in a corner and at eye levelSit them in a corner and at eye level– Well-lighted areaWell-lighted area– Speak clearly and slowly, low toneSpeak clearly and slowly, low tone– MimeMime– Use amplifiersUse amplifiers

NeurologyNeurology

Pyramidal Motor SystemPyramidal Motor System• AnatomyAnatomy– Corticospinal and corticobulbar systemCorticospinal and corticobulbar system– Originates: motor, premotor, sensory cortexOriginates: motor, premotor, sensory cortex– Terminates: on alpha motor neurons in the intermediate gray of Terminates: on alpha motor neurons in the intermediate gray of
spinal cord and brain stemspinal cord and brain stem• FunctionFunction– Executes isolated dextrous muscle movementsExecutes isolated dextrous muscle movements– Present only in primates and abovePresent only in primates and above– Modified by reticulospinal, tectospinal and vestibulospinal tractsModified by reticulospinal, tectospinal and vestibulospinal tracts
• Effect of lesionsEffect of lesions– Upper motor neuron paralysisUpper motor neuron paralysis

Extrapyramidal Motor SystemExtrapyramidal Motor System• AnatomyAnatomy– Originates: basal ganglia and cerebellumOriginates: basal ganglia and cerebellum– Links indirectly to pyramidal system via thalamus and cortexLinks indirectly to pyramidal system via thalamus and cortex
• FunctionFunction– Basal ganglia: initiation and planning of movementBasal ganglia: initiation and planning of movement– Cerebellum: monitors, smoothes and terminates movementsCerebellum: monitors, smoothes and terminates movements– No direct initiation of movementsNo direct initiation of movements
• LesionsLesions– Basal ganglia: bradykinesiaBasal ganglia: bradykinesia– Cerebellum: ataxiaCerebellum: ataxia

Basal Ganglia DysfunctionBasal Ganglia Dysfunction• AnatomyAnatomy– Caudate nucleusCaudate nucleus
– PutamenPutamen
– Globus pallidusGlobus pallidus
– Substantia nigraSubstantia nigra
– Subthalamic nucleusSubthalamic nucleus
– (Thalamus)(Thalamus)
• Effects of dysfunctionEffects of dysfunction– Involuntary movementsInvoluntary movements
– Altered voluntary movementsAltered voluntary movements• SlowSlow
• InterruptedInterrupted
• UncoordinatedUncoordinated
– Posture and tone alteredPosture and tone altered
• Neurotransmitter correlatesNeurotransmitter correlates– Dopamine > Ach = hyperkineticDopamine > Ach = hyperkinetic
– Ach > Dopamine = hypokineticAch > Dopamine = hypokinetic

Upper Motor Neuron (Central) WeaknessUpper Motor Neuron (Central) Weakness
• HemiparesisHemiparesis
• HyperreflexiaHyperreflexia
• Unilateral clasp – knife spasticity (“rigidity”)Unilateral clasp – knife spasticity (“rigidity”)
• May see spontaneous spasms May see spontaneous spasms
• Anatomic associationsAnatomic associations– LE: external rotationLE: external rotation
– UE: decreased arm swing, internal rotation when extendedUE: decreased arm swing, internal rotation when extended
– Facial: spares forehead, eye wider, nasolabial fold flatFacial: spares forehead, eye wider, nasolabial fold flat

Localizing an Upper Motor Neuron Localizing an Upper Motor Neuron (Central) Weakness(Central) Weakness
• Cerebral CortexCerebral Cortex– Trouble with language, spatial attention, touch recognition, visionTrouble with language, spatial attention, touch recognition, vision
• Internal CapsuleInternal Capsule– Face, UE and LE weak but no other cranial nerve or cortical symptoms Face, UE and LE weak but no other cranial nerve or cortical symptoms
• BrainstemBrainstem– Cranial nerves involved Cranial nerves involved
• Spinal cordSpinal cord– Face not involvedFace not involved

Lower Motor Neuron (Peripheral) WeaknessLower Motor Neuron (Peripheral) Weakness
• Anterior horn cell to muscleAnterior horn cell to muscle
• Muscle atrophyMuscle atrophy
• Fasciculations and fibrillationsFasciculations and fibrillations
• Decreased/absent reflexesDecreased/absent reflexes
• FlaccidityFlaccidity
• CrampingCramping

UMN vs. LMN WeaknessUMN vs. LMN WeaknessUMNUMN LMNLMN
LocationLocation Cortex –> SCCortex –> SC Ant. horn cell–Ant. horn cell–>muscle>muscle
Muscle sizeMuscle size NormalNormal AtrophicAtrophic
ReflexesReflexes IncreasedIncreased DecreasedDecreased
FasciculationsFasciculationsAbsentAbsent PresentPresent
ToneTone Clasp knife rigidityClasp knife rigidity Decreased (flaccid)Decreased (flaccid)

Babinski’s SignBabinski’s Sign• Primitive defensive flexion of hip, knee and Primitive defensive flexion of hip, knee and
dorsiflexion of ankledorsiflexion of ankle
• In primates, dorsiflexion of toesIn primates, dorsiflexion of toes
• When we start walking, the latter is inhibited to When we start walking, the latter is inhibited to allow toe plantar flexionallow toe plantar flexion
• Thus a normal response in an adult is flexion of the Thus a normal response in an adult is flexion of the hip, knee and dorsiflexion of the ankle with plantar hip, knee and dorsiflexion of the ankle with plantar flexion of the toes.flexion of the toes.
• Abnormal = “upgoing” toesAbnormal = “upgoing” toes

Guillain–Barré SyndromeGuillain–Barré Syndrome
• PathogenesisPathogenesis– Immunologic attack on peripheral myelinated fibersImmunologic attack on peripheral myelinated fibers
• EtiologyEtiology– Campylobacter jejuniCampylobacter jejuni, other infections, vaccinations, other infections, vaccinations
• Clinical ManifestationsClinical Manifestations– Ascending weaknessAscending weakness– Peripheral sensory lossPeripheral sensory loss– Loss of reflexesLoss of reflexes– CSF: increased protein but not cellsCSF: increased protein but not cells

Peripheral NeuropathiesPeripheral Neuropathies• Axonal Degeneration (“Dying Back”)Axonal Degeneration (“Dying Back”)– Toxic injury to neuronsToxic injury to neurons– Etiologies: EtOH, DM, Pb, paraneoplasticEtiologies: EtOH, DM, Pb, paraneoplastic– Symmetric, longest fibers firstSymmetric, longest fibers first
• IschemicIschemic– Loss of peripheral vascular or vaso nervorum blood supplyLoss of peripheral vascular or vaso nervorum blood supply– Etiologies: DM, pressure induced neuropathies, vasculitisEtiologies: DM, pressure induced neuropathies, vasculitis– AsymmetricAsymmetric
• DemyelinationDemyelination– Immune mediated injury to myelinated fibersImmune mediated injury to myelinated fibers– Etiologies: e.g. Guillain Barré syndromeEtiologies: e.g. Guillain Barré syndrome– Symmetric loss of motor and sensory function and DTR’sSymmetric loss of motor and sensory function and DTR’s

Muscle Motor WeaknessMuscle Motor Weakness• EtiologiesEtiologies– Inflammation: dermatomyositis, inclusion body myositisInflammation: dermatomyositis, inclusion body myositis– Abnormal proteins: muscle dystrophiesAbnormal proteins: muscle dystrophies– ToxinsToxins– Metabolic: high Ca, low K, low glucose, hypothyroidMetabolic: high Ca, low K, low glucose, hypothyroid– Neuromuscular junction: myasthenia gravis, Eaton–LambertNeuromuscular junction: myasthenia gravis, Eaton–Lambert
• Clinical ManifestationsClinical Manifestations– Proximal > distal muscle weaknessProximal > distal muscle weakness– No sensory lossNo sensory loss– Preservation of reflexesPreservation of reflexes

Brain EdemaBrain EdemaIncreased brain volume due to increased water contentIncreased brain volume due to increased water content
VasogenicVasogenic CytotoxicCytotoxic InterstitialInterstitialPathophysiologyPathophysiology EndothelialEndothelial NeuronalNeuronal PressurePressure
injuryinjury injuryinjury
CausesCauses TumorTumor HypoxiaHypoxia Hydroceph-Hydroceph-
InfectionInfection Hypoosmo–Hypoosmo– alusalus
TraumaTrauma larity larity MeningitisMeningitis
InfarctInfarct
HTNHTN
TherapyTherapy SteroidsSteroids NoneNone ShuntShunt

AphasiaAphasia• DefinitionDefinition– Disorder of language due to brain dysfunctionDisorder of language due to brain dysfunction
• ClassificationClassification– Expressive (Broca)Expressive (Broca)– Receptive (Wernicke)Receptive (Wernicke)– GlobalGlobal
• Other CharacteristicsOther Characteristics– Fluent vs. non–fluentFluent vs. non–fluent– ComprehensionComprehension– RepetitionRepetition

Memory TypesMemory Types• EpisodicEpisodic– Memory of eventsMemory of events
• Remote (mos to yrs), long–term memory, hardest to lose Remote (mos to yrs), long–term memory, hardest to lose • Recent (min to days), new learned ability, test by asking patient to remember 3 Recent (min to days), new learned ability, test by asking patient to remember 3
common words for a few minutescommon words for a few minutes• Immediate (s), not encoded, max ~ 7 items, easiest to loseImmediate (s), not encoded, max ~ 7 items, easiest to lose
test via digit repetitiontest via digit repetition
– Easiest to loseEasiest to lose
• SemanticSemantic– Memory of words and meaningsMemory of words and meanings– Test via naming of objects or personsTest via naming of objects or persons
• ProceduralProcedural– SkillsSkills– Toughest t loseToughest t lose

Memory LossMemory Loss• Failure to create memoriesFailure to create memories– Hippocampal systemHippocampal system
• Failure to have adequate storageFailure to have adequate storage– Loss of neuronsLoss of neurons
• Failure to retrieveFailure to retrieve– Loss of neurons that used to “contain” memoriesLoss of neurons that used to “contain” memories

Acute Pain TypesAcute Pain Types• First painFirst pain– A–delta fibersA–delta fibers– Immediate, brief, sharp, localizedImmediate, brief, sharp, localized
• Second painSecond pain– C fibersC fibers– Seconds later, enduring, dull/burning, not localizedSeconds later, enduring, dull/burning, not localized

Pain PathwaysPain Pathways• Ascending PathwayAscending Pathway– Pain receptorsPain receptors
– Synapse in dorsal hornSynapse in dorsal horn
– Cross to form ascending Cross to form ascending spinothalamic tractspinothalamic tract
– ThalamusThalamus• Lateral thalamic nucleusLateral thalamic nucleus
– To somatosensory cortex –> To somatosensory cortex –> “feel” pain“feel” pain
• Medial thalamic nucleusMedial thalamic nucleus– To frontal cortex –> To frontal cortex –>
“realize” pain“realize” pain
• Descending PathwayDescending Pathway– Periaqueductal gray regionPeriaqueductal gray region
• SerotoninSerotonin
• To frontal cortexTo frontal cortex– Suppress response to painSuppress response to pain
• To spinal cordTo spinal cord– Suppress sensation of painSuppress sensation of pain

Diseases of the Pain PathwaysDiseases of the Pain Pathways• Reflex Sympathetic Dystrophy (Causalgia)Reflex Sympathetic Dystrophy (Causalgia)– Post–nerve injury hypersensitivity to catecholamines released Post–nerve injury hypersensitivity to catecholamines released
by sympathetic nervous systemby sympathetic nervous system– Hypereshtesia, vasoconstriction, muscle atrophy, contractureHypereshtesia, vasoconstriction, muscle atrophy, contracture– Rx: analgesics, sympathetic blockadeRx: analgesics, sympathetic blockade
• FibromyalgiaFibromyalgia– Decreased descending serotonin releaseDecreased descending serotonin release– Increased perception of pain from non–noxious stimuliIncreased perception of pain from non–noxious stimuli– Rx: SSRIsRx: SSRIs

Myasthenia GravisMyasthenia Gravis• PathophysiologyPathophysiology– Autoimmune destruction of post–synaptic neuromuscular junction nicotinic Autoimmune destruction of post–synaptic neuromuscular junction nicotinic
acetylcholine receptors (AchRs)acetylcholine receptors (AchRs)– Antibody binds and induces cell mediated attackAntibody binds and induces cell mediated attack– Accelerated loss of AchRsAccelerated loss of AchRs
• Clinical ManifestationsClinical Manifestations– Weak: proximal muscles, eye lids and EOM, cranial nerves, diaphragmWeak: proximal muscles, eye lids and EOM, cranial nerves, diaphragm
• DiagnosisDiagnosis– Improvement after acetycholinesterase inhibitor (edrophonium, Tensilon®) Improvement after acetycholinesterase inhibitor (edrophonium, Tensilon®)
challengechallenge– EMG: Decrement in action potentials with repetitive stimulationEMG: Decrement in action potentials with repetitive stimulation– Assay for anti–acetylcholine receptor antibodies (80–90% +)Assay for anti–acetylcholine receptor antibodies (80–90% +)
• TherapyTherapy– Long acting acetylcholinesterase inhibitors, steroids, cytotoxics, Long acting acetylcholinesterase inhibitors, steroids, cytotoxics,
thymectomy, plasmapheresis, IVIGthymectomy, plasmapheresis, IVIG

Duchenne Muscular DystrophyDuchenne Muscular Dystrophy• PathophysiologyPathophysiology– Variable mutations of dystrophin gene at Xp21 locus (X–linked rec)Variable mutations of dystrophin gene at Xp21 locus (X–linked rec)– Dystrophin protects sarcolemmal membrane from degradation by intracellular Dystrophin protects sarcolemmal membrane from degradation by intracellular
proteases, absence –> muscle necrosis, Ca influxproteases, absence –> muscle necrosis, Ca influx
• Clinical ManifestationsClinical Manifestations– Male onset ~2–3 years, wheelchair in teens, death in 20sMale onset ~2–3 years, wheelchair in teens, death in 20s– Proximal weakness with calf pseudohypertrophy (fat, fibrosis, inflam)Proximal weakness with calf pseudohypertrophy (fat, fibrosis, inflam)– Protruberant abdomen, lumbar lordosisProtruberant abdomen, lumbar lordosis– Cardiac: CHF, arrhythmiasCardiac: CHF, arrhythmias– CPK elevatedCPK elevated– EMG: myopathic small polyphasic potentialsEMG: myopathic small polyphasic potentials
• Treatment and PrognosisTreatment and Prognosis– Symptomatic, prednisone slows progressionSymptomatic, prednisone slows progression– Usually death in 3rd decade from respiratory or cardiac diseaseUsually death in 3rd decade from respiratory or cardiac disease

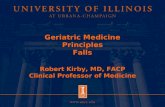
Duchenne Muscular DystrophyDuchenne Muscular Dystrophy
Gower’s SignGower’s Sign Calf pseudohypertrophyCalf pseudohypertrophy

PolymyositisPolymyositis• PathophysiologyPathophysiology– T–cell mediated muscle injuryT–cell mediated muscle injury– Secondary Ab formation (Jo–1, Mi–2, SRP) Secondary Ab formation (Jo–1, Mi–2, SRP)
• Clinical Diagnostic FindingsClinical Diagnostic Findings– Symmetric proximal muscle weakness with painSymmetric proximal muscle weakness with pain– Elevated plasma muscle enzymesElevated plasma muscle enzymes– Myopathic changes on electromyographyMyopathic changes on electromyography– Characteristic muscle biopsy abnormalities and the absence of Characteristic muscle biopsy abnormalities and the absence of
histopathologic signs of other myopathieshistopathologic signs of other myopathies• DermatomyositisDermatomyositis– Gottron’s papules and heliotrope eyelidsGottron’s papules and heliotrope eyelids– Humorally mediated vasculitisHumorally mediated vasculitis– Adult form associated with malignancyAdult form associated with malignancy
• TherapyTherapy– Steroids, cytotoxics, plasmapheresis, IVIGSteroids, cytotoxics, plasmapheresis, IVIG

DermatomyositisDermatomyositis
Gottron’s papulesGottron’s papules Heliotrope eyelidsHeliotrope eyelids

Myophosphorylase DeficiencyMyophosphorylase Deficiency(McArdle’s Disease)(McArdle’s Disease)
• PathophysiologyPathophysiology– Autosomal recessive mutation of myophosphorylase gene on 11q13Autosomal recessive mutation of myophosphorylase gene on 11q13
– Phosphorylase removes 1,4 glucosyl residues from glycogen releasing G–1 Phosphorylase removes 1,4 glucosyl residues from glycogen releasing G–1 phosphate.phosphate.
– Absence drastically reduces glucose availability for muscleAbsence drastically reduces glucose availability for muscle
• Clinical ManifestationsClinical Manifestations– Exercise intolerance with cramping and myoglobinuriaExercise intolerance with cramping and myoglobinuria
– Second wind once FFA utilization kicks inSecond wind once FFA utilization kicks in
– Elevated CPKElevated CPK
• TreatmentTreatment– NoneNone

Tremor CharacteristicsTremor Characteristics
• To–and–fro oscillation around a jointTo–and–fro oscillation around a joint
• Regular or irregularRegular or irregular
• Predictable and simplePredictable and simple

Resting (Repose) TremorResting (Repose) Tremor• CharacteristicsCharacteristics– Occurs with inactivity of limbOccurs with inactivity of limb
• ExaminationExamination– Resting hand = pill rollingResting hand = pill rolling– Resting tongueResting tongue
• EtiologyEtiology– Parkinsonism (4 – 6 Hz)Parkinsonism (4 – 6 Hz)• Parkinson’s disease, heavy metal toxicity (Fe, Cu), drug (MPTP)Parkinson’s disease, heavy metal toxicity (Fe, Cu), drug (MPTP)
– Midbrain strokeMidbrain stroke• TreatmentTreatment– Dopamine agonistsDopamine agonists

ParkinsonismParkinsonism• Classical CharacteristicsClassical Characteristics– BradykinesiaBradykinesia– Tremor (4–6 Hz, initially unilateral)Tremor (4–6 Hz, initially unilateral)– Cogwheel rigidityCogwheel rigidity– Loss of postural reflexesLoss of postural reflexes
• EtiologyEtiology– Death of dopaminergic neurons in substantia nigraDeath of dopaminergic neurons in substantia nigra– Dopamine antagonistsDopamine antagonists
• TherapyTherapy– L–dopa, dopamine agonistsL–dopa, dopamine agonists– Amantadine (blocks DA re–uptake)Amantadine (blocks DA re–uptake)– COMT inhibitorsCOMT inhibitors– Selegeline (MOA inhibitor)Selegeline (MOA inhibitor)

Intention (Action) TremorIntention (Action) Tremor• CharacteristicsCharacteristics– Occurs with action of an extremityOccurs with action of an extremity
• ExaminationExamination– Finger–to–nose and heel–to–shin testFinger–to–nose and heel–to–shin test
• EtiologyEtiology– Cerebellar disease (3–4 Hz)Cerebellar disease (3–4 Hz)• EtOH, trauma, stroke, tumor, degeneration, MSEtOH, trauma, stroke, tumor, degeneration, MS
– Midbrain strokeMidbrain stroke• TreatmentTreatment– Physical therapyPhysical therapy

Postural TremorPostural Tremor• CharacteristicsCharacteristics– Occurs with antigravity posturingOccurs with antigravity posturing
• ExaminationExamination– Outstretched arms and fingersOutstretched arms and fingers– Tongue protrusionTongue protrusion
• EtiologyEtiology– Exaggerated physiologic tremor (10–12 Hz)Exaggerated physiologic tremor (10–12 Hz)
• Catecholamine excess:Catecholamine excess:– Endocrine: pheo, hyperthyroid, hypoglycemiaEndocrine: pheo, hyperthyroid, hypoglycemia– Drugs: ß–agonists, reuptake inhibitors, xanthine oxidase inhibitors, catecholaminesDrugs: ß–agonists, reuptake inhibitors, xanthine oxidase inhibitors, catecholamines– StressStress
– Essential tremor (4–10 Hz)Essential tremor (4–10 Hz)• Etiology unknownEtiology unknown• 50% inherited (familial tremor)50% inherited (familial tremor)
• TreatmentTreatment– ß–blockers, EtOH, primidoneß–blockers, EtOH, primidone

Tremor SummaryTremor SummaryTremor TypeTremor Type FrequencyFrequency CauseCause TreatmentTreatmentRestingResting 4 – 6 Hz4 – 6 Hz Parkinson’sParkinson’s DopaminergicsDopaminergics
ActionAction 3 – 4 Hz3 – 4 Hz CerebellarCerebellar NoneNone
PosturalPostural
ExaggeratedExaggerated 10 – 12 Hz10 – 12 Hz CatecholsCatechols Treat causeTreat cause
physiologicphysiologic ß–blockersß–blockers
EssentialEssential 4 – 10 Hz 4 – 10 Hz UnknownUnknown ß–blockers,ß–blockers,
primidoneprimidone

ChoreaChorea• DefinitionDefinition– Irregular, unpredictable, random, rapid, jerkyIrregular, unpredictable, random, rapid, jerky
• PathophysiologyPathophysiology– Dopamine excess in striatumDopamine excess in striatum– Estrogen effect (mild)Estrogen effect (mild)
• EtiologyEtiology– Huntington’s disease (and misc. hereditary forms)Huntington’s disease (and misc. hereditary forms)– Sydenham’s chorea (acute rheumatic fever)Sydenham’s chorea (acute rheumatic fever)– Cerebral palsyCerebral palsy– Pregnancy, OCP’sPregnancy, OCP’s
• TreatmentTreatment– Dopamine antagonistsDopamine antagonists

Huntington’s DiseaseHuntington’s Disease• EtiologyEtiology– Autosomal dominant progressive chorea and dementiaAutosomal dominant progressive chorea and dementia– Defective huntingtin protein (chromosome 4)Defective huntingtin protein (chromosome 4)– Degeneration of cholinergic and GABA–ergic cells in BGDegeneration of cholinergic and GABA–ergic cells in BG– Relative excess dopamineRelative excess dopamine
• ManifestationsManifestations– Middle age onsetMiddle age onset– ChoreaChorea– Violent outbursts, psychosis, withdrawalViolent outbursts, psychosis, withdrawal
• TreatmentTreatment– Dopamine antagonistsDopamine antagonists– Genetic screeningGenetic screening

Tardive DyskinesiaTardive Dyskinesia• PathogenesisPathogenesis– Chronic (> 6 weeks) exposure to dopamine antagonistsChronic (> 6 weeks) exposure to dopamine antagonists– Hypersensitive striatal dopamine receptorsHypersensitive striatal dopamine receptors
• Clinical ManifestationsClinical Manifestations– Orofacial repetitive movementsOrofacial repetitive movements– Limb and trunk involuntary movementsLimb and trunk involuntary movements
• TreatmentTreatment– Discontinue neurolepticDiscontinue neuroleptic– Reserpine Reserpine

HemiballismusHemiballismus• DefinitionDefinition– Violent, sudden, large amplitude, unilateral gyrationsViolent, sudden, large amplitude, unilateral gyrations
• PathophysiologyPathophysiology– Stroke in subthalamic nucleusStroke in subthalamic nucleus
• TreatmentTreatment– Dopamine antagonists, usually resolves in several monthsDopamine antagonists, usually resolves in several months

TicsTics• DefinitionDefinition– Brief, stereotypic, suppressibleBrief, stereotypic, suppressible– May be vocalizations, swearing, gesturesMay be vocalizations, swearing, gestures– Worse with stressWorse with stress
• PathophysiologyPathophysiology– UnclearUnclear– Dopamine excess causing disinhibition of limbic systemDopamine excess causing disinhibition of limbic system
• TreatmentTreatment– TimeTime– Dopamine antagonistsDopamine antagonists

DystoniasDystonias• DefinitionsDefinitions– Sustained, involuntary contracturesSustained, involuntary contractures– Focal: cervical (torticollis), fingers (writer’s cramp), Focal: cervical (torticollis), fingers (writer’s cramp),
orbicularis oculi (blepharospasm)orbicularis oculi (blepharospasm)– GeneralizedGeneralized
• EtiologyEtiology– Often occupational, worse with stressOften occupational, worse with stress– Some focal are hereditarySome focal are hereditary– Generalized may be due to central lesionsGeneralized may be due to central lesions
• TreatmentTreatment– AnticholinergicsAnticholinergics– Botulinum toxin injectionsBotulinum toxin injections

Bedside Visual Field TestingBedside Visual Field Testing• Macular Function TestingMacular Function Testing– Visual acuity: form (letter) discrimination (Snellen)Visual acuity: form (letter) discrimination (Snellen)– Color vision testing: subjective red discriminationColor vision testing: subjective red discrimination
• Peripheral Visual Field Function TestingPeripheral Visual Field Function Testing– Motion detectionMotion detection– Light detectionLight detection– Dynamic perimetry: confrontational or GoldmannDynamic perimetry: confrontational or Goldmann
• Higher Cortical Function TestingHigher Cortical Function Testing– Object recognitionObject recognition– Object sortingObject sorting– Face recognitionFace recognition– Visual–motor coordinationVisual–motor coordination– Geographic directionsGeographic directions


Neuroanatomy of the Visual System Neuroanatomy of the Visual System
• Anterior visual pathwayAnterior visual pathway– Carries axons from retinal ganglion cells to lateral geniculate bodiesCarries axons from retinal ganglion cells to lateral geniculate bodies
• Optic nerves –> chiasm –> tracts –> LGN Optic nerves –> chiasm –> tracts –> LGN
• Nasal fibers cross at chiasm, lesion there gives bitemporal hemianopsiaNasal fibers cross at chiasm, lesion there gives bitemporal hemianopsia
• Tracts carry fibers from one side of each eye –> lesion gives homonomous hemianopsia (e.g. Tracts carry fibers from one side of each eye –> lesion gives homonomous hemianopsia (e.g. L sided lesion gives a R homonomous hemianopsia)L sided lesion gives a R homonomous hemianopsia)
• Posterior visual pathwayPosterior visual pathway– ––> radiations –> occipital lobe –> calcarine/peristriate/parastriate cortex–> occipital > radiations –> occipital lobe –> calcarine/peristriate/parastriate cortex–> occipital
cortex (Brodmann 17)cortex (Brodmann 17)
• ExaminationExamination– Foveal functions: VA, color, contrastFoveal functions: VA, color, contrast
– Retina/optic nerve: visual fieldsRetina/optic nerve: visual fields

Total BlindnessTotal Blindness• Loss of function of both globes/retina/optic nervesLoss of function of both globes/retina/optic nerves
• Chiasmal destructionChiasmal destruction
• Bilateral occipital lobe infarctionBilateral occipital lobe infarction

Partial BlindnessPartial Blindness• ScotomaScotoma– Non–seeing visual field surrounded by seeing visual fieldNon–seeing visual field surrounded by seeing visual field– Same stimulusSame stimulus
• HemianopsiaHemianopsia– Visual loss with a vertical marginVisual loss with a vertical margin
• Central lossCentral loss– Poor acuity, colorPoor acuity, color– Do not act blindDo not act blind
• Peripheral lossPeripheral loss– VA OKVA OK– Act blindAct blind– Subjective dimnessSubjective dimness

Occipital BlindnessOccipital Blindness• Blood SupplyBlood Supply– Medial surface from PCAMedial surface from PCA– Pole supplied by MCAPole supplied by MCA
• InfarctionInfarction– Usually spares the maculaUsually spares the macula
• HypoperfusionHypoperfusion– Usually spares the peripheryUsually spares the periphery

EndocrinologyEndocrinology

Hypothalamic HormonesHypothalamic HormonesHormoneHormoneStructureStructure MadeMade EffectEffect (–) Feedback(–) Feedback
TRHTRH 3 aa3 aa A. HTA. HT ˝˝ TSH, Pl, GHTSH, Pl, GH TSHTSH
GnRHGnRH 10 aa10 aa A. HTA. HT ˝˝ FSH, LH,GHFSH, LH,GH Est, Pr, Est, Pr, GCGC
CRHCRH 41 aa41 aa CNSCNS ˝˝ ACTH, ß–endACTH, ß–end GCGC
GHRHGHRH 40 + 44 aa40 + 44 aa Arcuate n.Arcuate n. ˝˝ GH, eat, sleepGH, eat, sleep GH, IGF1,SSGH, IGF1,SS
SSSS 14 + 28 aa14 + 28 aa CNSCNS GH,TSH,ADH,TSHGH,TSH,ADH,TSH ManyMany
PIFPIF DADA CNSCNS ProlactinProlactin
PRFPRF ?? CNSCNS ˝˝ ProlactinProlactin

HypopituitarismHypopituitarism• EtiologiesEtiologies– Tumor, ischemia, genetic, vascular, infiltration, inflam, Tumor, ischemia, genetic, vascular, infiltration, inflam,
iatrogenic, infection, traumaiatrogenic, infection, trauma• DiagnosisDiagnosis– Basal hormone levels and target gland hormone levelsBasal hormone levels and target gland hormone levels
• TherapyTherapy– ACTH deficiency: GC, ± MCACTH deficiency: GC, ± MC– TSH deficiency: thyroxineTSH deficiency: thyroxine– FSH/LH deficiency: Est/Prog/TtFSH/LH deficiency: Est/Prog/Tt– GHRH deficiency: hGH in childrenGHRH deficiency: hGH in children– Prolactin: noneProlactin: none– Vasopressin: DDAVPVasopressin: DDAVP

Pituitary TumorsPituitary TumorsSecretionSecretion DiseaseDisease DiagnosisDiagnosis TherapyTherapyNoneNone ± hypopituitarism± hypopituitarism Levels/MRILevels/MRI surgery, XRT, drugssurgery, XRT, drugs
GHGH gigantism/acromegaly gigantism/acromegaly Post glu GH, IGF1Post glu GH, IGF1 surgery, drugs, XRTsurgery, drugs, XRT
ProlactinProlactin galact/infertility/impot galact/infertility/impot Pro level > 250ng/mlPro level > 250ng/ml drugs, surgery, XRTdrugs, surgery, XRT
ACTHACTH Cushing’s diseaseCushing’s disease Dex suppressDex suppress surgery, drugs, XRT surgery, drugs, XRT
TSHTSH hyperthyroidismhyperthyroidism TSH and T4TSH and T4 surgery, XRT/drugssurgery, XRT/drugs
LH/FSHLH/FSH may be nonemay be none LevelsLevels surgery, XRT/drugssurgery, XRT/drugs

Regulation of Body CalciumRegulation of Body Calcium• Basic DistributionBasic Distribution– Total body = 1–2 kg: 99% boneTotal body = 1–2 kg: 99% bone– In blood, 50% ionized, ~50% bound to albuminIn blood, 50% ionized, ~50% bound to albumin
• Hormonal ControlHormonal ControlHormoneHormone BoneBone RenalRenal Small BowelSmall Bowel
PTHPTH ReleaseRelease ReabsorpReabsorp AbsorptionAbsorption
Vitamin DVitamin D Sl. releaseSl. release ExcretionExcretion AbsorptionAbsorption
CalcitoninCalcitonin Incorp.Incorp. ExcretionExcretion NoneNone

Manifestations of HypercalcemiaManifestations of Hypercalcemia• NeuropsychiatricNeuropsychiatric– Altered MSAltered MS
• GastrointestinalGastrointestinal– Anorexia, N+V, constipationAnorexia, N+V, constipation
• CardiovascularCardiovascular– Short QTShort QT– Increased contractilityIncreased contractility– Digitalis toxicityDigitalis toxicity
• RenalRenal– Nephrogenic DINephrogenic DI– Impaired GFRImpaired GFR– NephrocalcinosisNephrocalcinosis– NephrolithiasisNephrolithiasis

Causes of HypercalcemiaCauses of Hypercalcemia• EndocrineEndocrine
– HyperparathyroidismHyperparathyroidism– HyperthyroidismHyperthyroidism– Addison’s diseaseAddison’s disease– PheochromocytomaPheochromocytoma– Familial hypocalcuric hypercalcemiaFamilial hypocalcuric hypercalcemia
• MalignancyMalignancy– MetastasesMetastases– Ectopic PTH, PTHrP, 1,25(OH)DEctopic PTH, PTHrP, 1,25(OH)D
• Granulomatous DiseasesGranulomatous Diseases– SarcoidosisSarcoidosis– TBTB– FungalFungal
• MiscellaneousMiscellaneous– ImmobilizationImmobilization
– AcuteAcute renal failure renal failure
– Milk–alkali syndromeMilk–alkali syndrome
– MedicationsMedications• ThiazidesThiazides
• LithiumLithium
• Vitamin AVitamin A
• Vitamin DVitamin D
• AminophyllineAminophylline

Primary HyperparathyroidismPrimary Hyperparathyroidism
• Epidemiology/EtiologyEpidemiology/Etiology– 1–2/1,000/yr > 60yo1–2/1,000/yr > 60yo
– Single adenoma 85%, 4 gland hyperplasia 12%, CA 3%Single adenoma 85%, 4 gland hyperplasia 12%, CA 3%
• AssociationsAssociations– MEN 1: 95% hyperplasia + pancreatic and pituitary tumorsMEN 1: 95% hyperplasia + pancreatic and pituitary tumors
– MEN 2A: 50% hyperplasia + medullary CA thyroid and pheoMEN 2A: 50% hyperplasia + medullary CA thyroid and pheo
• Biochemical FeaturesBiochemical Features– Serum: high Ca and Cl, low P and HCOSerum: high Ca and Cl, low P and HCO33, high PTH, high alk phos, high PTH, high alk phos
– Urine: high calcium, phosphorus and cAMPUrine: high calcium, phosphorus and cAMP

Non–Primary HyperparathyroidismNon–Primary Hyperparathyroidism
• SecondarySecondary– EtiologyEtiology
• Renal failure or malabsorption –> Renal failure or malabsorption –> hypocalcemia –> increased PTHhypocalcemia –> increased PTH
– DiagnosisDiagnosis• High serum PTH with low/nml CaHigh serum PTH with low/nml Ca
• High phosphorusHigh phosphorus
• Low 25 or 1–25 OH DLow 25 or 1–25 OH D33
– TherapyTherapy• Calcium supplementsCalcium supplements
• Calcitrol (1–25 OH DCalcitrol (1–25 OH D33))
• TertiaryTertiary– EtiologyEtiology
• Renal failure –> chronic Renal failure –> chronic hypocalcemia –> chronic hypocalcemia –> chronic increased PTH –> permanent increased PTH –> permanent parathyroid hyperplasiaparathyroid hyperplasia
– DiagnosisDiagnosis• High serum PTH with high CaHigh serum PTH with high Ca
– TherapyTherapy• As for secondaryAs for secondary
• Surgery if severe or symptomaticSurgery if severe or symptomatic

Hyperparathyroidism SummaryHyperparathyroidism Summary
TypeType Primary EventPrimary Event Serum PTH Serum PTH Serum Serum CalciumCalcium
PrimaryPrimary PTH autonomyPTH autonomy ElevatedElevated ElevatedElevated
SecondarySecondary Low serum CaLow serum Ca ElevatedElevated Low/normalLow/normal
TertiaryTertiary PTH autonomyPTH autonomy ElevatedElevated ElevatedElevated

Evaluation of HypercalcemiaEvaluation of Hypercalcemia• RequiredRequired– Serum Ca, PTH, 24h urine CaSerum Ca, PTH, 24h urine Ca
• Only if indicatedOnly if indicated– PTHrPPTHrP– Vitamin D levelsVitamin D levels– Vitamin A levelVitamin A level– Lithium levelLithium level

Therapy of HypercalcemiaTherapy of Hypercalcemia
• Specific therapySpecific therapy– Treat underlying disorderTreat underlying disorder
• Nonspecific therapyNonspecific therapy– NS hydrationNS hydration– Loop diureticsLoop diuretics– BiphosphonatesBiphosphonates– CalcitoninCalcitonin– GlucocorticoidsGlucocorticoids– Gallium nitrateGallium nitrate

Multiple Endocrine Neoplasia SyndromesMultiple Endocrine Neoplasia SyndromesGeneral RulesGeneral Rules
• Autosomal Dominant inheritance Autosomal Dominant inheritance
• Hyperplasia precedes neoplasiaHyperplasia precedes neoplasia
• Tumors usually multifocalTumors usually multifocal
• Familial screening criticalFamilial screening critical

Multiple Endocrine Neoplasia SyndromesMultiple Endocrine Neoplasia Syndromes• MEN 1MEN 1– Primary hyperparathyroidism (~100%), from hyperplasiaPrimary hyperparathyroidism (~100%), from hyperplasia– Pancreatic tumors (50–70%)Pancreatic tumors (50–70%)
• Gastrinoma > insulinoma, VIP, glucagonoma, PP, non–secretingGastrinoma > insulinoma, VIP, glucagonoma, PP, non–secreting– Pituitary tumors (50%)Pituitary tumors (50%)
• Prolactin > GH, ACTH, null cellProlactin > GH, ACTH, null cell
• MEN 2aMEN 2a– Medullary CA thyroid (>90%)Medullary CA thyroid (>90%)– Pheochromocytoma (40–50%)Pheochromocytoma (40–50%)– Primary hyperparathyroidism (10–50%), hyperplasiaPrimary hyperparathyroidism (10–50%), hyperplasia– Cutaneous lichen amyloidosisCutaneous lichen amyloidosis
• MEN 2bMEN 2b– Medullary CA thyroid (>90%)Medullary CA thyroid (>90%)– PheochromocytomaPheochromocytoma– Mucosal neuromas, intestinal ganglioneuromas, marfanoidMucosal neuromas, intestinal ganglioneuromas, marfanoid

Osteoporosis: EtiologyOsteoporosis: Etiology• EpidemiologyEpidemiology– 1/3 and 1/6 of elderly men and women –> hip Fx1/3 and 1/6 of elderly men and women –> hip Fx– > 25 million people in US> 25 million people in US
• Risk factorsRisk factors– BehavioralBehavioral: inactivity, EtOH, smoking: inactivity, EtOH, smoking– NutritionalNutritional: low Ca or vitamin D intake, caffeine, low body mass: low Ca or vitamin D intake, caffeine, low body mass– HereditaryHereditary: Caucasian/Asian, family history, body build: Caucasian/Asian, family history, body build– Gender relatedGender related: female, early menopause: female, early menopause– MedicationsMedications: GC, thyroxine, anticonvulsants, heparin/warfarin, MTX, : GC, thyroxine, anticonvulsants, heparin/warfarin, MTX,
cyclosporin, GnRH, lithiumcyclosporin, GnRH, lithium– EndocrineEndocrine: Cushing’s, hypogonadism, hyperthyroidism, hyperparathyroidism: Cushing’s, hypogonadism, hyperthyroidism, hyperparathyroidism– End organEnd organ: Renal, liver: Renal, liver– Bone resorptionBone resorption: RA, immobilization: RA, immobilization

Osteoporosis: Diagnosis and TreatmentOsteoporosis: Diagnosis and Treatment
• DiagnosisDiagnosis– Bone densitometryBone densitometry
– T score = SD above or below mean of sex–matched young adultsT score = SD above or below mean of sex–matched young adults• Normal > –1.0, osteopenia –2.5 to – 1.0, osteoporosis < –2.5Normal > –1.0, osteopenia –2.5 to – 1.0, osteoporosis < –2.5
• TreatmentTreatment– Lifestyle modificationLifestyle modification: exercise, dietary Ca and vitamin D, stop : exercise, dietary Ca and vitamin D, stop
smoking and EtOH and caffeinesmoking and EtOH and caffeine
– MedicationsMedications: Estrogens, Ca, vitamin D, calcitonin, biposphonates, : Estrogens, Ca, vitamin D, calcitonin, biposphonates, SERMsSERMs

Iodine MetabolismIodine Metabolism• Requirements and bioavailabilityRequirements and bioavailability– Requirement = 60 µg/dRequirement = 60 µg/d– Typical intake = 250–300 µgTypical intake = 250–300 µg– 20% thyroid uptake, rest excreted in urine20% thyroid uptake, rest excreted in urine
• Thyroid hormone synthesisThyroid hormone synthesis– >90% organified: bound to tyrosine on thyroglobulin>90% organified: bound to tyrosine on thyroglobulin– Forms monoiodotyrosine and diiodotyrosineForms monoiodotyrosine and diiodotyrosine– These are enzymatically coupled to form T3 and T4These are enzymatically coupled to form T3 and T4– Digestion of thyroglobulin releases T3 and T4Digestion of thyroglobulin releases T3 and T4

Thyroid HormonesThyroid HormonesThyroxineThyroxine TriiodothyronineTriiodothyronine Reverse Reverse
T3T3
T4T4 T3T3 RT3RT3
CreationCreation Thyroid 100%Thyroid 100% T4 80% T4 80% T4 > T4 > 90%90%
Thyroid 20%Thyroid 20%
Activity (T4=1)Activity (T4=1) 1 1 10 10 00
TT1/21/2 5–7d 5–7d 1 d 1 d 4 h 4 h

Thyroid Hormone RegulationThyroid Hormone Regulation
• Increased byIncreased by– TSHTSH• Increases I uptake, digestion of Tg, release of T4 and T3Increases I uptake, digestion of Tg, release of T4 and T3
– Iodine deficiencyIodine deficiency• Enhanced response to TSHEnhanced response to TSH
• Decreased byDecreased by– Iodine excessIodine excess• Reduces organification (Wolff–Chaikoff effect)Reduces organification (Wolff–Chaikoff effect)
• Decreases secretion of T4 and T3Decreases secretion of T4 and T3

Hypothalamic TRH RegulationHypothalamic TRH Regulation
• Increased byIncreased by– CatecholaminesCatecholamines
• Decreased byDecreased by– T4 and T3T4 and T3– SomatostatinSomatostatin

Pituitary TSH RegulationPituitary TSH Regulation
• Increased byIncreased by– TRH from hypothalamusTRH from hypothalamus• Increased production and releaseIncreased production and release
• Decreased byDecreased by– T3T3– DopamineDopamine– GlucocorticoidsGlucocorticoids

Radioactive Iodine UptakeRadioactive Iodine Uptake
• MethodologyMethodology– Oral radiolabeled I, scan thyroid and determine amount of uptakeOral radiolabeled I, scan thyroid and determine amount of uptake
• UseUse– Determines etiology of hyperthyroidismDetermines etiology of hyperthyroidism
• If high: increased production = Grave’s, Hashimoto, Plummer’s, adenoma, TSHIf high: increased production = Grave’s, Hashimoto, Plummer’s, adenoma, TSH
• If low: inflammatory release = subacute thyroiditis; exogenous thyroid hormoneIf low: inflammatory release = subacute thyroiditis; exogenous thyroid hormone
– Helps calculate dose of radioactive iodine ablative therapyHelps calculate dose of radioactive iodine ablative therapy
– Evaluates suppressibility of thyroidEvaluates suppressibility of thyroid

Hyperthyroidism: Clinical ManifestationsHyperthyroidism: Clinical Manifestations• GeneralGeneral– Weakness and fatigueWeakness and fatigue
• CardiovascularCardiovascular– Palpitations, tachycardia, (atrial fibrillation)Palpitations, tachycardia, (atrial fibrillation)
• NeurologicNeurologic– Nervousness, tremor, (psychosis)Nervousness, tremor, (psychosis)– Sweat, heat intoleranceSweat, heat intolerance– InsomniaInsomnia
• GIGI– Weight loss with decreased appetite, hyperdefecationWeight loss with decreased appetite, hyperdefecation
• ReproductiveReproductive– Oligo–amenorrhea, infertility, gynecomastiaOligo–amenorrhea, infertility, gynecomastia
• LabLab– Anemia, low chol, high alk phos, high CaAnemia, low chol, high alk phos, high Ca

Etiologies of HyperthyroidismEtiologies of Hyperthyroidism• Graves’ DiseaseGraves’ Disease– Thyroid stimulating immunoglobulin –> TSH receptorThyroid stimulating immunoglobulin –> TSH receptor– Diffuse toxic goiter, high RAIU, T4, low TSHDiffuse toxic goiter, high RAIU, T4, low TSH– Ophthalmopathy and pretibial myxedemaOphthalmopathy and pretibial myxedema– Associated with MG, vitiligo, ITPAssociated with MG, vitiligo, ITP
• Plummer’s DiseasePlummer’s Disease– Elderly, etiology not clearElderly, etiology not clear– Toxic multinodular goiter, high RAIU, T4, low TSHToxic multinodular goiter, high RAIU, T4, low TSH
• Subacute (de Quervain’s) ThyroiditisSubacute (de Quervain’s) Thyroiditis– Destructive release of T4, PAINFUL, fever, high ESRDestructive release of T4, PAINFUL, fever, high ESR– Viral infection in many casesViral infection in many cases– low RAIU, T4, low TSHlow RAIU, T4, low TSH

Etiologies of HyperthyroidismEtiologies of Hyperthyroidism• Lymphocytic thyroiditisLymphocytic thyroiditis– ? Variant of Hashimoto’s, may be post–partum ? Variant of Hashimoto’s, may be post–partum – Painless, low RAIU, high T4, low TSHPainless, low RAIU, high T4, low TSH– Antithyroid antibodies in 50%Antithyroid antibodies in 50%
• Toxic AdenomaToxic Adenoma– Nodule > 3cm, high RAIU, high T4, low TSHNodule > 3cm, high RAIU, high T4, low TSH– Focal scan uptakeFocal scan uptake
• FactitiousFactitious• Jod BasedowJod Basedow• TSH or TRH secreting tumorsTSH or TRH secreting tumors

Hypothyroidism: Clinical ManifestationsHypothyroidism: Clinical Manifestations• GeneralGeneral– Weakness and fatigue, muscle crampsWeakness and fatigue, muscle cramps
• CardiovascularCardiovascular– BradycardiaBradycardia
• NeurologicNeurologic– Slow mentation, (psychosis)Slow mentation, (psychosis)– Dry skin from decreased sweatingDry skin from decreased sweating– Cold intoleranceCold intolerance– Carpal tunnel syndromeCarpal tunnel syndrome– Pituitary enlargementPituitary enlargement
• GIGI– Weight gain, constipationWeight gain, constipation
• ReproductiveReproductive– Oligo–amenorrhea, infertility, galactorrheaOligo–amenorrhea, infertility, galactorrhea
• LabLab– Anemia, hi CPK, high chol and TG, low NaAnemia, hi CPK, high chol and TG, low Na

Etiologies of HypothyroidismEtiologies of Hypothyroidism• Hashimoto’s thyroiditis (chronic lymphocytic)Hashimoto’s thyroiditis (chronic lymphocytic)– Autoimmune destruction, may be initially hyperthyroidAutoimmune destruction, may be initially hyperthyroid– Antibody to thyroperoxidase (90%) and thyroglobulin (70%)Antibody to thyroperoxidase (90%) and thyroglobulin (70%)– Associations: Addison’s (Schmidt syndrome), PA, DMAssociations: Addison’s (Schmidt syndrome), PA, DM
• IatrogenicIatrogenic– Post–surgery or RAI for hyperthyroidismPost–surgery or RAI for hyperthyroidism– Post XRT for Hodgkin's or head/neck CAPost XRT for Hodgkin's or head/neck CA– Drugs: lithium, aminoglutethimide, amiodaroneDrugs: lithium, aminoglutethimide, amiodarone
• MiscellaneousMiscellaneous– Postpartum, burnt–out Graves’, iodide excess, gland replaced, Postpartum, burnt–out Graves’, iodide excess, gland replaced,
congenital absence or mutationscongenital absence or mutations
• RareRare– Iodine deficiency, TSH blocking AbIodine deficiency, TSH blocking Ab

Thyroxine TherapyThyroxine Therapy• Slower ifSlower if– Older, severe, long–standingOlder, severe, long–standing
• DoseDose– Maintenance = 50–175 µg/day (< if old)Maintenance = 50–175 µg/day (< if old)– Measure TSH in 4 – 6 wksMeasure TSH in 4 – 6 wks
• Things to watch forThings to watch for– Addisonian crisisAddisonian crisis– AnginaAngina

Euthyroid Sick SyndromeEuthyroid Sick Syndrome• Thyroid Function AbnormalitiesThyroid Function Abnormalities– Decreased conversion of T4 to T3 –> low T3Decreased conversion of T4 to T3 –> low T3– May see low T4 and rarely low FTIMay see low T4 and rarely low FTI– rT3 usually highrT3 usually high– TSH usually low or normalTSH usually low or normal
• TreatmentTreatment– NONENONE

Drug Effects on Thyroid FunctionDrug Effects on Thyroid Function
• TSH SecretionTSH Secretion– Decreased: Dopamine, GC, somatostatinDecreased: Dopamine, GC, somatostatin
• T4 and T3 productionT4 and T3 production– Increased: I (acutely), amiodaroneIncreased: I (acutely), amiodarone– Decreased: Li, I, amiodarone, aminoglutethimideDecreased: Li, I, amiodarone, aminoglutethimide– Increased metab: phenobarb, carbamazepine, dilantinIncreased metab: phenobarb, carbamazepine, dilantin
• T4–>T3 conversionT4–>T3 conversion– Decreased: ß–blockers, amiodarone, ipodate, PTU, GCDecreased: ß–blockers, amiodarone, ipodate, PTU, GC
• TBG productionTBG production– Increased: Est, tamoxifen, clofibrate, 5FU, narcoticsIncreased: Est, tamoxifen, clofibrate, 5FU, narcotics– Decreased: androgens, anabolic steroids, GCDecreased: androgens, anabolic steroids, GC– Displaces: ASA, dilantin, furosemide, fenclofenac, phenylbutazoneDisplaces: ASA, dilantin, furosemide, fenclofenac, phenylbutazone

Cushing’s Syndrome: ManifestationsCushing’s Syndrome: Manifestations(glucocorticoid excess)(glucocorticoid excess)
• HistoryHistory– Wt gain, weak, fatigueWt gain, weak, fatigue
– Acne, hirsuitism, bruising, poor Acne, hirsuitism, bruising, poor healinghealing
– Infertility, amenorrheaInfertility, amenorrhea
– Emotional labilityEmotional lability
– FracturesFractures
• Physical ExamPhysical Exam– Truncal obesityTruncal obesity
– SC, temporal and dorsal fat SC, temporal and dorsal fat pads increasedpads increased
– Moon faciesMoon facies
– PlethoraPlethora
– StriaeStriae
– Proximal muscle weaknessProximal muscle weakness
– HypertensionHypertension

Cushing’s Syndrome: LaboratoryCushing’s Syndrome: Laboratory
• Glucose intolerance or diabetesGlucose intolerance or diabetes
• Hypokalemic metabolic alkalosisHypokalemic metabolic alkalosis
• Hypercalcuria ± hypercalcemiaHypercalcuria ± hypercalcemia
• PolycythemiaPolycythemia
• Decreased lymphocytes and eosinophilsDecreased lymphocytes and eosinophils

Cushing’s Syndrome: EtiologiesCushing’s Syndrome: Etiologies
• ACTH DependentACTH Dependent– Pituitary Tumor (Disease)Pituitary Tumor (Disease)
• ACTH secreting tumorACTH secreting tumor
• ACTH suppressible by high dose ACTH suppressible by high dose dexamethasonedexamethasone
– Ectopic ACTHEctopic ACTH• Small cell CA lungSmall cell CA lung
• CarcinoidCarcinoid
• Not suppressibleNot suppressible
• ACTH IndependentACTH Independent– Exogenous steroidsExogenous steroids
– Adrenal sourcesAdrenal sources• AdenomaAdenoma
– Most common; surgical cureMost common; surgical cure
• CarcinomaCarcinoma– May secrete other steroidsMay secrete other steroids
• Micronodular hyperplasiaMicronodular hyperplasia
• Macronodular hyperplasiaMacronodular hyperplasia

Cushing’s Syndrome: Diagnostic TestsCushing’s Syndrome: Diagnostic Tests
• Elevated spot cortisolElevated spot cortisol– Many false (+)Many false (+)
• Elevated 24h urine free cortisolElevated 24h urine free cortisol– > 250 µg, < 65 µg r/o Cushing’s> 250 µg, < 65 µg r/o Cushing’s
– Best screen (have creat also)Best screen (have creat also)
• Overnight dex suppressionOvernight dex suppression– 1 mg at MN –> AM cortisol1 mg at MN –> AM cortisol
– < 5 µg/dl r/o Cushing’s < 5 µg/dl r/o Cushing’s
– F(+); obesity, depressionF(+); obesity, depression
• Low–dose dex suppressionLow–dose dex suppression– 0.5 mg q6h x 2d0.5 mg q6h x 2d– Measure 24h urine and AM Measure 24h urine and AM
cortisol on 2nd daycortisol on 2nd day– < 25µg and 5 µg/dl< 25µg and 5 µg/dl
• High dose dex suppressionHigh dose dex suppression– 2 mg q 6h x 2d2 mg q 6h x 2d– Measure 24h urine cortisol Measure 24h urine cortisol
baseline and on 2nd daybaseline and on 2nd day– If suppresses > 50% = pituitaryIf suppresses > 50% = pituitary– If not = ectopicIf not = ectopic
• ACTHACTH– Differentiates dependencyDifferentiates dependency

Cushing’s Disease: TherapyCushing’s Disease: Therapy• SurgerySurgery– AdenectomyAdenectomy– HypophysectomyHypophysectomy– Adrenalectomy + XRTAdrenalectomy + XRT
• Medical (adjunctive)Medical (adjunctive)– Decrease ACTH: Bromocriptine, cyproheptadine, valproateDecrease ACTH: Bromocriptine, cyproheptadine, valproate– Decrease cortisol: ketoconazole, metyrapone, Decrease cortisol: ketoconazole, metyrapone,
aminoglutethimide, and othersaminoglutethimide, and others– Block cortisol effect: RU456Block cortisol effect: RU456
• XRTXRT

Adrenal Insufficiency: ManifestationsAdrenal Insufficiency: Manifestations• HistoryHistory– Anorexia, nauseaAnorexia, nausea– Weak, fatigueWeak, fatigue
• Physical ExamPhysical Exam– Hypotension, orthostasisHypotension, orthostasis
• LaboratoryLaboratory– Low Na, high K (not seen if secondary), low glucoseLow Na, high K (not seen if secondary), low glucose– EosinophiliaEosinophilia
• ACTH stim test: ACTH stim test: – ACTH (1–24) (cosyntropin) 250 µg IV, measure cortisol in 30–ACTH (1–24) (cosyntropin) 250 µg IV, measure cortisol in 30–
60 min. (+) if < 18 µg/dl60 min. (+) if < 18 µg/dl

Diabetes Mellitus: Diagnostic CriteriaDiabetes Mellitus: Diagnostic CriteriaAny one of the following:Any one of the following:
• Symptoms and a casual plasma glucose of 200 mg/dlSymptoms and a casual plasma glucose of 200 mg/dl– Symptoms = polyuria, polydipsia and weight lossSymptoms = polyuria, polydipsia and weight loss– Casual = any time, no relation to foodCasual = any time, no relation to food
• Fasting plasma glucose of 126 mg/dlFasting plasma glucose of 126 mg/dl– Fasting = no caloric intake for 8 hoursFasting = no caloric intake for 8 hours
• 2–hour plasma glucose of 200 mg/dl on an oral GTT2–hour plasma glucose of 200 mg/dl on an oral GTT– Glucose load of 75 mg of anhydrous glucose in waterGlucose load of 75 mg of anhydrous glucose in water
Diabetes Care 21:S5–19, 1998.Diabetes Care 21:S5–19, 1998.

Type I Diabetes MellitusType I Diabetes Mellitus• PathophysiologyPathophysiology– Antibody–mediated destruction of ß cells (Type 1A)Antibody–mediated destruction of ß cells (Type 1A)– Idiopathic destruction of ß cells (Type 1B)Idiopathic destruction of ß cells (Type 1B)– Genetic predisposition (HLA–DR3 and DR4)Genetic predisposition (HLA–DR3 and DR4)– Twin concordance < 50%Twin concordance < 50%– ““complete” absence of insulincomplete” absence of insulin• Hyperglycemia, weight loss, ketoacidosis, polysHyperglycemia, weight loss, ketoacidosis, polys
• Other causesOther causes– Surgical removal or gland injurySurgical removal or gland injury– Fibrocalcific/fibrocalculus pancreatic diseaseFibrocalcific/fibrocalculus pancreatic disease

Type II Diabetes MellitusType II Diabetes Mellitus• EpidemiologyEpidemiology– > 10% of US population> 10% of US population
• PathophysiologyPathophysiology– Insulin resistance (post–receptor cascade)Insulin resistance (post–receptor cascade)– Decreased insulin response to plasma glucoseDecreased insulin response to plasma glucose
• Risk factorsRisk factors– Family HxFamily Hx– >> 20% above ideal BW 20% above ideal BW– Age Age >> 45 45– Prior glucose intolerance or gestational DMPrior glucose intolerance or gestational DM– HypertensionHypertension– HDL HDL << 35 mg/dl or triglyceride 35 mg/dl or triglyceride >> 250 mg/dl 250 mg/dl– Sedentary life styleSedentary life style– Baby > 9 lbsBaby > 9 lbs

Diabetes Mellitus: ComplicationsDiabetes Mellitus: Complications
• Vascular (micro and macro)Vascular (micro and macro)
• RenalRenal
• RetinopathyRetinopathy
• Joint/connective tissueJoint/connective tissue
• PeriodontalPeriodontal
• NeurologicNeurologic

Chronic Therapy of DiabetesChronic Therapy of Diabetes
• Diet and ExerciseDiet and Exercise– Attempt to maintain a reasonable (not ideal) weightAttempt to maintain a reasonable (not ideal) weight– 60% CHO, 10–20 % ptn, 20–30% fat, < 10% saturated fat60% CHO, 10–20 % ptn, 20–30% fat, < 10% saturated fat
• InsulinInsulin– Required for all type I diabeticsRequired for all type I diabeticsNameName OnsetOnset PeakPeak DurationDurationMonemeric (Lispro)Monemeric (Lispro) 10–15 m10–15 m 60 m60 m 3–4 h3–4 hRegularRegular 30 m30 m 2 h2 h 4–8 h4–8 hNPH/LenteNPH/Lente 40–60 m40–60 m 6–10 h6–10 h 16 h16 hUltralenteUltralente 50–70 m50–70 m 12 – 16 h12 – 16 h 24 h24 hGlargineGlargine 70 – 105 m70 – 105 m nonenone > 24 h> 24 h

Drugs For Type II DiabetesDrugs For Type II Diabetes• SulfonylureasSulfonylureas– Stimulates insulin releaseStimulates insulin release
• BiguanidesBiguanides– Improve peripheral sensitivity to insulinImprove peripheral sensitivity to insulin
• ThiazolidonesThiazolidones– Improve peripheral sensitivity to insulinImprove peripheral sensitivity to insulin
• MeglitinidesMeglitinides– Stimulates insulin release Stimulates insulin release
• Glucosidase InhibitorsGlucosidase Inhibitors– Interfere with absorption of carbohydratesInterfere with absorption of carbohydrates