Clinical, Microbiologic and Therapeutic Aspects of ... · tients with purulent pericarditis. had...
11
REVIEWS Clinical, Microbiologic and Therapeutic Aspects of Purulent Pericarditis ROBERT H. RUBIN, M.D. ROBERT C. MOELLERING. Jr., M.D. Boston, Massachusetts From the Department of Medicine, Harvard Medical School; and the Medical Service (Infec- tious Disease Unit) of the Massachusetts Gener- al Hospital, Boston, Massachusetts. Requests for reprints should be addressed to Dr. Robert H. Rubin. Infectious Disease Unit, Massachu- setts General Hospital, Fruit Street, Boston, Massachusetts 02114. Manuscript accepted September 26, 1974. Twenty-six patients wlth purulent perlcarditls were seen at the Massachusetts General Hospital between 1960 and 1974. The dl- agnosls was made in 16 of them during life, but only 6 survived, with an over-all mortality rate of 77 per cent. In eight patients, purulent pericarditls developed In the early postoperative period after thoraclc surgery. In seven, purulent pericardltls was the re- sult of contiguous spread of lnfectlon from a pleural, medlastinal or pulmonary focus In nonsurgical patients. In five patients, it was the result of direct spread to the pericardium from an intra- cardiac Infection. In the remaining six patients, puruient pericar- dltls developed as the result of a systemic bacteremia. Immuno- suppresslve therapy, extensive thermal burns, lymphoprolifera- tive disease and other systemic processes affecting host resis- tance were present in at least half the patlents. Staphylococcus aureus was the etiologic agent in the largest number of patients (6 of 26 In this report). However, in contrast to previous studies, In a significant number of the patients (five), purulent pericarditis was the result of fungal infection (In three patients subjected to thoracic surgery and In two immunosuppressed patients). This report confirms that purulent perlcardltls is an acute dis- ease with a fulminant course. The diagnosis is easily missed since classic signs of pericarditis (Including chest pain, friction rub and diagnostic electrocardiographic abnormalities) may be absent. The echocardiogram shows considerable promise in al- lowing earlier diagnosis of the pericardial effusion which accom- panies purulent pericardltls. Optimal therapy consists of pro- longed antlblotlc therapy and aggressive drainage of the pericar- dium. In this series, there were 6 survivors among the 11 patients (55 per cent) who received appropriate therapy. Although purulent pericarditis has been recognized since Galen’s day [ 11, the nature of the disease has changed-changed even from that described in Boyle, Pearce and Guze’s classic review in 1961 [2]. These investigators documented the overwhelming im- portance of pleuropulmonary disease and uncontrolled gram-posi- tive coccal infection-that due to Staphylococcus aureus, Strepto- coccus pneumoniae and Streptococcus pyogenes-in the patho- genesis of suppurative infection of the pericardium in the preanti- biotic and early antibiotic eras. Even in their series, however, sev- eral trends were noted: a marked decrease in the incidence of con- comitant pleuropulmonary infection; a fall-off in the occurrence of 69 July 1975 The American Journal of Medlclne Vdume 59
Transcript of Clinical, Microbiologic and Therapeutic Aspects of ... · tients with purulent pericarditis. had...

REVIEWS
Clinical, Microbiologic and Therapeutic Aspects of
Purulent Pericarditis
ROBERT H. RUBIN, M.D.
ROBERT C. MOELLERING. Jr., M.D.
Boston, Massachusetts
From the Department of Medicine, Harvard Medical School; and the Medical Service (Infec- tious Disease Unit) of the Massachusetts Gener- al Hospital, Boston, Massachusetts. Requests for reprints should be addressed to Dr. Robert H. Rubin. Infectious Disease Unit, Massachu- setts General Hospital, Fruit Street, Boston, Massachusetts 02114. Manuscript accepted September 26, 1974.
Twenty-six patients wlth purulent perlcarditls were seen at the Massachusetts General Hospital between 1960 and 1974. The dl- agnosls was made in 16 of them during life, but only 6 survived, with an over-all mortality rate of 77 per cent. In eight patients, purulent pericarditls developed In the early postoperative period after thoraclc surgery. In seven, purulent pericardltls was the re- sult of contiguous spread of lnfectlon from a pleural, medlastinal or pulmonary focus In nonsurgical patients. In five patients, it was the result of direct spread to the pericardium from an intra- cardiac Infection. In the remaining six patients, puruient pericar- dltls developed as the result of a systemic bacteremia. Immuno- suppresslve therapy, extensive thermal burns, lymphoprolifera- tive disease and other systemic processes affecting host resis- tance were present in at least half the patlents. Staphylococcus aureus was the etiologic agent in the largest number of patients (6 of 26 In this report). However, in contrast to previous studies, In a significant number of the patients (five), purulent pericarditis was the result of fungal infection (In three patients subjected to thoracic surgery and In two immunosuppressed patients).
This report confirms that purulent perlcardltls is an acute dis- ease with a fulminant course. The diagnosis is easily missed since classic signs of pericarditis (Including chest pain, friction rub and diagnostic electrocardiographic abnormalities) may be absent. The echocardiogram shows considerable promise in al- lowing earlier diagnosis of the pericardial effusion which accom- panies purulent pericardltls. Optimal therapy consists of pro- longed antlblotlc therapy and aggressive drainage of the pericar- dium. In this series, there were 6 survivors among the 11 patients (55 per cent) who received appropriate therapy.
Although purulent pericarditis has been recognized since Galen’s day [ 11, the nature of the disease has changed-changed even from that described in Boyle, Pearce and Guze’s classic review in 1961 [2]. These investigators documented the overwhelming im- portance of pleuropulmonary disease and uncontrolled gram-posi- tive coccal infection-that due to Staphylococcus aureus, Strepto- coccus pneumoniae and Streptococcus pyogenes-in the patho- genesis of suppurative infection of the pericardium in the preanti- biotic and early antibiotic eras. Even in their series, however, sev- eral trends were noted: a marked decrease in the incidence of con- comitant pleuropulmonary infection; a fall-off in the occurrence of
69 July 1975 The American Journal of Medlclne Vdume 59

PURULENT PERICARDITIS-RUBIN. MOECLERING
pneumococcal disease; an increase in the incidence
of hospital-acquired, antibiotic-resistant infection; and
an increase in the number of cases in elderly patients
and in patients with complicating systemic illnesses.
In the years since then, these trends have continued,
and today puruient pericarditis is more commonly a
disease of the debilitated patient with impaired host
defenses: of the patient who has undergone exten-
sive thoracic and/or cardiac surgery: of the patient
with preexisting, nonpyogenic inflammatory disease
of the pericardium; and of the patient with uncon-
trolled myocardial and/or endocardial infection. In ad-
dition, more traditional forms of the disease still
occur. Two aspects of purulent pericarditis that have
not changed since Galen’s day are the insidiously
subtle presentation it may have, and the large per
cent of cases that go undiagnosed until postmortem
examination.
Our purpose is to review the experience with this
disease at the Massachusetts General Hospital during
the period 1960 to 1974, emphasizing the following
points: the clinical and epidemiologic settings within
which purulent pericarditis now occurs, the microbio-
logic culprits of the disease today, the pathogenetic
mechanisms by which the disease is produced, and
modern methods of diagnosis and therapy. It is hoped
that such information will provide a basis for a more
effective attack on this ancient problem.
MATERIALS AND METHODS
The records of all patients with purulent infection of the
pericardium seen at the Massachusetts General Hospital
from July 1, 1960, to June 30, 1974, were reviewed, and
form the basis for this study. Four of the patients have
been the subjects of separate reports [3-61. All patients
included in this study fulfilled at least two of the three fol-
lowing criteria: (1) The demonstration of gross or micro-
scopic evidence of an acute pericarditis with a predomi-
nance of polymorphonuclear leukocytes in the inflammato-
ry infiltrate in material obtained at autopsy or surgery; or
the demonstration of purulent fluid (more than 30,000
white blood cells/mm3 with more than 90 per cent poly- morphonuclear leukocytes) at pericardiocentesis. (2) The demonstration of bacteria or fungi on gram stain of peri- cardial fluid. (3) The isolation of a bacterium (other than
Mycobacterium tuberculosis) or fungus from cultures of
pericardial tissue or fluid, or from cultures of immediately
contiguous structures and/or blood.
Excluded from the series were patients who had a vari-
ety of infections and evidence of pericardial effusions by
either echocardiogram, roentgenogram, radioisotope scan or electrocardiogram, but who recovered without precise definition of the pericardial process.
Specimens for culture were inoculated on Brucella agar plates containing 5 per cent horse blood, McConkey agar
and thioglycollate broth, and were incubated at 37°C in air
enriched with 5 per cent carbon dioxide. During the last 5
years covered by this report, primary anaerobic cultures
were usually performed as well. In selected patients, Sa-
boraud’s medium was used for fungal isolation.
The patients with purulent pericarditis have been
grouped according to the portal of infection and whether
the disease occurred as a result of a surgically-induced in-
fection or was acquired de novo as part of a “medical” ill-
ness. Group I: Patients with contiguous spread from a postoperative infection. Group II: Nonsurgical patients with contiguous spread from a pleural, mediastinal or pulmo-
nary focus. Group III: Nonsurgical patients with contiguous spread from intracardiac infections. Group IV: Nonsurgical patients with noncontiguous spread during systemic bac-
teremia
RESULTS
Twenty-six patients with purulent pericarditis were
identified during the 14 years of this study. Twenty of
these patients died, for an over-all mortality of 77 per cent. The diagnosis of purulent pericarditis was made
during life in 18 of the 26 (69 per cent) and at autop-
sy in the remainder. No particular age group had- a
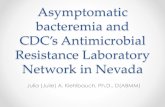
preponderance of cases (Figure 1). Fifteen of the 26
patients were male.
Predisposing Conditions. Table I delineates the
clinical settings in which purulent pericarditis oc-
curred. In eight patients (group I), the disease devel-
oped in the early postoperative period (1 to 3 weeks
after thoracic surgery). In two, transthoracic esopha-
geal surgery was associated with esophageal perfo-
ration and contiguous spread of infection from the
mediastinum to the pericardium: in the remaining six,
open heart surgery was complicated by extensive
sternal wound infection, sternal osteomyelitis, medi-
astinitis and, again, contiguous spread to the pericar-
dium. In seven patients (group II), the disease devel-
oped in association with primary pleural, mediastinal
and/or pulmonary infection. Four of these patients
had left-sided pneumonia and empyema (two of
these had bilateral pneumonias and empyemas); two
had pneumonia in the lower lobe of the left lung with-
out accompanying pleural space involvement. The
pulmonary infection was believed to be the primary
event in these six patients, with contiguous spread
occurring to the adjacent pleural and/or pericardial spaces. In the remaining patient, a patient with 50
per cent third degree total body burns and persistent
Salmonella bacteremia, purulent pericarditis was
secondary to contiguous spread from a mediastinal
abscess that had developed. In five patients (group Ill), it was a complication of intracardiac infection; as
a result of contiguous spread from infected heart
valves (two aortic and one mitral) in three and as a
result of contiguous spread from a myocardial ab-
scess in two. Six patients (group IV) had purulent
pericarditis as a result of a systemic bacteremia.
July 1975 The American Journal of Medicine Volume 59 69

PURULENT PERICARDITIS-RUBIN. MOELLERING
7
6 c
I SURVIVED rl
o-9 IO-19 20-29 30-39 40-49 50-59 60-69 70+
AGE, years
Two of the six patients with pleuropulmonary infec-
tion (group II) and four of the six with bacteremia
(group IV) survived. None of the patients in groups I (postsurgical) and Ill (intracardiac infection) survived:
the development of purulent pericarditis represented
the final coupe-de-grace in a desperately ill group of
patients.
Associated systemic diseases that may have im-
paired host resistance were present in 12 patients
(hepatic failure in 2, uremia in 1, diabetes mellitus in
3, leukopenia in 1, extensive third degree burns in 2,
acute lymphoblastic leukemia in 1 and large dose
corticosteroid and azathioprine therapy in 2). Two
patients with preexisting nonsuppurative pericarditis
had a secondary infection from a transient bacter-
emia originating from an extrathoracic site. One of
TABLE I Classification of the 26 Patients with Purulent Pericarditis According to Route of Infection, Clinical Setting and Outcome
No. of Patients
Group Description Survived Died
I Patients with contiguous
spread from a postopera-
tive infection 0 8 II Nonsurgical patients with
contiguous spread from a
pleural, mediastinal or pul- monary f0cUS 2 5
III Nonsurgical patients with
contiguous spread from in-
tracardiac infections 0 5 IV Nonsurgical patients with
noncontiguous spread to the pericardium during sys-
temic bacteremia 4 2
these patients
Figure 7. Age and mortality in 26 pa- tients with purulent pericarditis.
had bacteremia due to Klebsiella
pneumoniae from a site of acute pyelonephritis, with
the development of a Klebsiella pericarditis superim-
posed on preexisting uremic pericarditis. The other
patient had idiopathic (presumably viral) pericarditis
for 3 weeks [4] with partial recovery before the de-
velopment of an acute decompensation due to Bac-
teroides species superinfection of the pericardial
space.
Microbiology. A wide variety of organisms caused
purulent pericarditis in these patients (Table II). The
most common were Staph. aureus (eight patients);
fungi (five patients: due to Candida species infection
in three, to Aspergillus species in one, and to both
Aspergillus and Candida species in one); Strep. pneu-
moniae (two patients) and H. influenzae (two pa-
tients). Purulent pericarditis due to staphylococci oc-
curred after cardiac surgery in three patients (group
I), after intracardiac infection in three patients (group
Ill) (resulting from acute bacterial endocarditis of the
aortic valve in two and from a myocardial abscess in
one patient with staphylococcal bacteremia), was
secondary to pneumonia in one (group II) and due to
bacteremia in one. Purulent pericarditis due to fungi
occurred postoperatively in three patients (after car-
diac surgery in two and after esophageal surgery in
one), and after pulmonary infection in two immuno-
suppressed patients (one had leukemia and one was receiving large doses of corticosteroid). Both patients
with purulent pericarditis due to pneumococci had pneumonia and empyema. Meningitis with septicemia
preceded the onset of pericarditis in both cases due
to H. influenzae.
Relatively unusual organisms causing single cases of purulent pericarditis included the following: Salmo-
nella typhimurium in the previously described burn patient with mediastinal infection and persistent bac-
70 July 1975 The American Journal of Medicine Volume 59

PURULENT PERICARDITIS-RUBIN MOELLERING
TABLE II Microbiology of 26 Cases of Purulent
Pericarditis -.
Patients
Organism __ _ _ _~~_....
Staphylococcus aureus
Fungal infection*
Streptococcus pneumoniae
Hemophilus influenzae
Neisseria meningitidis
Klebsiella pneumoniae
Pseudomonas aeruginosa
Bacteroides species
Salmonella typhimurium
Nocardia asteroides
Streptococcus mitis
Mixed bacterial infectiont
No. %
8 30.8 5 19.2 2 7.7 2 7.7 1 3.8 1 3.8 1 3.8 1 3.8 1 3.8 1 3.8 1 3.8 2 7.7
* Candida species infection in three, Aspergillus species in
one and mixed Aspergillus and Candida infection in one.
t Escherichia coli, Klebsiella pneumoniae, and nonhemolytic
streptococci in one and Klebsiella pneumoniae, Enterobacter
species, Escherichia coli and Citrobacter species in the other.
teremia; Nocardia asteroides in a renal transplant pa-
tient receiving large doses of corticosteroids and
azathioprine in whom disseminated nocardial infec-
tion developed, including a myocardial abscess that
spread into the pericardial space; Streptococcus
mitis that spread from an infected aortic valve to the aortic root and then to the pericardium: Pseudomo-
nas aeruginosa in a patient with Pseudomonas pneu-
monia and contiguous spread to the pericardium; and
Bacteroides species infection in a patient with proba-
ble antecedent viral pericarditis and no source identi-
fied for the preceding Bacteroides bacteremia.
Clinical Manifestations. Purulent pericarditis is
clearly an acute illness of few days’ duration (the
mean length of symptoms before hospitalization was
3 days, with a range of 1 to 6 days*) characterized
by high spiking fevers, frank rigors and complaints
referrable to the cardiorespiratory systems (Table Ill).
Noteworthy in these patients was the absence of
chest pain: only 7 of the 26 patients had chest dis-
comfort, and of these, 5 had other intrathoracic sites
of infection (1 mediastinal, 4 pleuropulmonary) that
could have been the cause of the pain. The presen-
tation of the disease varied, depending on the portal
by which the pericardium became infected.
In group I patients (postsurgical) the picture was
reasonably uniform. Between 1 and 3 weeks after
initial survival of extensive surgery, the patients showed signs of systemic infection with hectic tem-
* In four patients (two with pneumococcal. one with staphylo- coccal and one with mixed bacterial pericarditis) precise data concerning the duration of symptoms prior to hospitalization were not available.
perature curves, rigors and cardiorespiratory com-
promise. Frequently, there was evidence of signifi-
cant wound infection and/or pneumonia. There was
little difficulty in making a diagnosis of infection, or
even infection in the chest, in these patients; the diffi-
culty lay in making the diagnosis of pericardial in-
volvement. Typically, the patients subjected to cardi-
ac surgery had had a stormy immediate postopera-
tive course, with bleeding points that required second
and even third explorations of the wound, placement
of drainage tubes within the pericardium or mediasti-
num, and prolonged hypotension with resuscitative
efforts. Since the pericardium is not closed after car-
diac surgery, it is understandable that tamponade
was not noted in these patients. However, tampo-
nade was present and was the immediate cause of
death in one of the patients who had had esophageal
surgery. Of the eight patients in group I, the diagnosis
of purulent pericarditis was made before autopsy in
only two.
In group II patients (pleuropulmonary disease) the
presenting symptoms were those of an acute, severe
bacterial pneumonia with respiratory embarrass-
ment, cough and purulent sputum production, spiking
fevers and pleuritic chest pain. Approximately 2 to 4
days after the development of this symptom com-
plex, evidence of circulatory compromise developed,
with five of these seven patients manifesting some
evidence of impaired venous return to the heart or
frank tamponade. The two patients in whom circula-
TABLE III Clinical Manifestations in 26 Patients with
Purulent Pericarditis -_ ________.. ._ ~~- -----.-
Per cent of
Manifestations Patients -._____._____ ._._. ~~~ .~. _.
Symptoms
Fever 96
Chills 62
Night sweats 62
Dyspnea 54
Cough 42
Chest pain* 27
Signs
Tachycardia (pulse rate greater than lOO/
min) 100
Friction rubs? 46
Hypotension and/or pulse pressure less
than 25 mm Hg 42
Pulsus paradoxus more than 10 mm Hg 38
Elevated central venous pressure (more
than 10 cm H20) 31
Hepatomegaly 15 .___~.._____. ~ _ --.- --
*Seven patients had chest pain; it was pleuritic in four, precordial and nonpleuritic in two and both pleuritic and pre-
cordial in one. t Twelve patients had a friction rub; it was pericardial in origin
in nine, pleural in two, both pericardial and pleural in one.
July 1975 The American Journal of Medicine Volume 59 71

PURULENT PERICARDITIS-RUBIN. MOELLERING
tory compromise did not develop had only minimal,
microscopic changes at autopsy, and the pericarditis
was not an important part of the clinical course.
In group Ill patients (intracardiac infection) the
major manifestations were those of the underlying in-
fections, acute bacterial endocarditis in three pa-
tients and myocardial abscess secondary to a bac-
teremia in two. However, the sudden circulatory de-
compensation that led to death in all five of these pa-
tients included spread of infection into the pericar-
dium with resulting hemodynamic embarrassment. All patients were receiving appropriate antimicrobial
therapy for their infections, and in none would sur-
gery have been likely to alter the outcome: in all in-
stances, spread of infection within the myocardium,
as well as within the pericardium, would have made
these patients inoperable.
In group IV patients (systemic bacteremia) fever,
chills and tachycardia of sudden onset with subse-
quent development of hemodynamic embarrassment
was the typical presentation. The duration of illness
from onset to either death or recognition and therapy
was less than 5 days in all cases. Five of these six
patients had evidence of impaired venous return; four
of them manifested significant pulsus paradoxus. The
one patient without circulatory manifestations, and
the only one in this group who died before a diagno-
sis was made, was a 17 year old boy with acute
meningococcemia of less than 16 hours’ duration
who only had microscopic evidence of disease (plus
positive cultures) at postmortem. Despite the pre-
dominance of cardiac findings in these patients, fric-
tion rubs were present in only one of the group IV pa-
tients, being found predominantly in group I and group
II patients.
Laboratory Findings. The presence of significant
acute inflammation was reflected in the white blood
cell counts of virtually all the patients, white blood
cell counts of more than 12,000/mm3 (with 20 of the
26 patients having white blood cell counts of more
than 17,000/mm3) and marked shifts to the left in the
polymorphonuclear leukocyte population being pres-
ent in all but 3 patients. The three exceptions includ-
ed one patient with leukemia, one renal transplant
patient who was receiving large doses of corticoste-
roids and azathioprine, and one patient with underly- ing neutropenia of unknown etiology-all adequate
reasons for lack of a leukocytosis. Moderate anemia
(hematocrit values between 30 and 35 per cent) was
present in 15 of the patients (58 per cent), but other blood tests were less helpful, with only minimal ab-
normalities of liver function and cardiac muscle en-
zymes being noted.
Chest roentgenograms were performed in 25 of
the 26 patients. Twenty-four of these showed abnor- malities (increased heart size in 19 (76 per cent),
pneumonia in 12 (48 per cent), pleural effusion in 8
(32 per cent) and mediastinal widening in 3 (12 per
cent)). In the majority of instances, the roentgeno-
gram suggested the pathologic process (such as
pneumonia, empyema or mediastinitis) accompa-
nying the purulent pericarditis without giving clear-cut evidence of pericardial disease. In 11 instances, the
finding of progressive enlargement of the cardiac sil-
houette with a “waterbottle-like” configuration in the
absence of pulmonary vascular congestion was high-
ly suggestive of significant pericardial fluid accumula-
tion. Three echocardiograms were carried out, and
all three were positive, including two in patients in
whom neither the chest roentgenogram nor electro-
cardiogram was particularly helpful. A right heart
catheterization was carried out in one patient, reveal-
ing the elevated central venous pressure, poor cardi-
ac pulsations, typical pressure tracing and increased
thickness between right atrial endocardium and peri-
cardial border that are characteristically found in pa-
tients with cardiac tamponade.
Electrocardiograms were obtained in 23 patients.
The tracings were normal or showed no changes
from a previous electrocardiogram in eight patients,
and were abnormal in 15. Nonspecific S-T and T
wave changes were noted in seven patients and
were the most common findings. More classic abnor-
malities associated with pericarditis, including diffuse
S-T wave elevation (five patients) and diffuse T wave
inversion (three patients, one of whom also demon-
strated low QRS voltage and electrical alternans),
were seen in the other eight patients. Arrhythmias
that could be ascribed to the pericarditis and not to
digitalis, electrolyte disturbances, hypoxia, acid-base
disturbances, myocardial abscesses and the like
were distinctly unusual.
Detailed analyses were carried out on pericardial
fluid obtained from five patients. The white blood cell
counts of the fluid ranged from 6,100 to 241 ,OOO/
mm3, being greater than 50,000/mm3 in four of the
five. Differential counts revealed more than 90 per
cent polymorphonuclear leukocytes in all instances.
Sugar levels were less than 35 mg/ 100 ml in all but
one patient, and the protein level ranged from 3.3 to
6.2 g/100 ml (mean 4.7 g/100 ml). In one patient, a
patient with pleuropulmonary disease, fluid was rela- tively clear, the white blood cell count was only
6,1 00/mm3 (94 per cent polymorphonuclear leuko- cytes), the sugar level was 79 mg/ 100 ml and the
protein level was 4.2 g/100 ml, but gram-positive
cocci were seen on gram stain and Staph. aureus
grew on culture. All the other patients had low sugar levels and higher white blood cell counts. Pericardial
fluid lactic dehydrogenase values were determined in
two patients and were 4,800 and 6,700 units/ml, re-
spectively (normal values are 60 to 120 units/ml).
72 July 1975 The American Journal of Medicine Volume 59

PURULENT PERICARDITIS-RUBIN, MOELLERING
Therapy and Complications. Eleven patients re- which is at first clear, then contains organisms, has ceived treatment consisting of more than 2 days of fibrin deposition and only later becomes grossly puru- appropriate antibiotics and at least one pericardio- lent [2,7]. In this series, four of the five patients who centesis. Six of these survived, for a mortality rate of underwent detailed pericardial fluid examination had 44 per cent in those in whom adequate therapy was the “late picture” of gross purulence, high white instituted. Two of the survivors were treated only with blood cell count and low sugar content. However, in pericardiocentesis plus antibiotics. The four others one patient with purulent pericarditis accompanying required thoracotomy and at least partial pericardiec- Staph. aureus bronchopneumonia. there was a rela- tomy in addition to this. In two of these, the indication tively low white blood cell count in the pericardial fluid for surgery was repeated reaccumulation of fluid; in and a normal sugar content. When comparing this two, acute pericardial constriction developed 1 and 3 last patient with the other four, it is apparent that this weeks, respectively, after therapy had been institut- patient had had an acute staphylococcal infection for ed. In one of these, a large epicardial abscess was less than 36 hours, whereas the others had been found and drained at the time of surgery. Antimicro- sick for more than 4 days. It is believed that these bial therapy was continued for 4 to 6 weeks in all sur- findings correspond to a very early stage in the vivors pathogenetic series of events.
Of the remaining 15 patients, the correct diagnosis was made during life in 7 and at autopsy in 8. The seven diagnosed but inadequately treated patients in- cluded two from group I (postsurgical) and five from group Ill (intracardiac infection). All of these, in addi- tion to six of the eight in whom the diagnosis was made at autopsy, had received at least 10 days of appropriate antibiotic therapy without pericardial
drainage before they died.
COMMENTS
The microbiologic, clinical and therapeutic features of purulent pericarditis have changed dramatically
over the past decade. Previously, it was a disease of children and young adults [2] ; today, it is found equally in all age groups. Previously pleuropulmonary disease was the cause of approximately 50 per cent of the cases [2]; today, less than 25 per cent occur in this setting. Once Staph. aureus and Strep. pneu- moniae accounted for at least half of all cases [2] ; today, fungi, gram-negative bacilli and associated un- usual pathogens are the cause of many cases. Once primary infection in healthy patients was the rule;
today, major thoracic and cardiac surgery, immuno- suppressive therapy, extensive thermal burns, lym- phoproliferative diseases and other systemic pro- cesses are the substrata within which this disease occurs. The major area in which there has been no change, however, is in the unacceptably high mortali- ty rate. In view of this a reexamination of the patho- genesis, clinical presentations, etiologies, and the di- agnostic and therapeutic approaches available ap- pears to be in order. Pathogenesis. The pathogenesis of purulent peri- carditis has been best worked out in those cases ac- companying intrathoracic disease and occurring by contiguous spread of infection. The first lesion ob- served is a local area of acute inflammation of the parietal pericardium adjacent to the site of contigu- ous infection. Next there is an accumulation of fluid,
Direct extension from the pleural space or lung accounts for the majority of cases of pericarditis ac- companying thoracic infections, but the observation that right-sided pneumonia or empyema may accom- pany purulent pericarditis has suggested that other mechanisms may be at work [2,7-131. Although systemic bacteremia may well be the final common
denominator, Hahn et al. [ 1 l] and others [ 121 have suggested that microscopic septic emboli from a pul- monary focus of suppuration may go directly to the pericardium, myocardium or mediastinum via the bronchial arteries, without involving the rest of the
systemic circulation. Clinical Setting and Presentation. Purulent pericar- ditis is a disease that almost always occurs as a complication of another illness [ 2,14,15], be it surgi- cal wound infection, intrathoracic infection or bacter- emia. In all instances that we have observed, it is an
acute progressive, septic process of less than 6 days’ duration that requires prompt and aggressive attention. Early recognition and effective therapy of pericardial disease is impossible unless the physician is alert to the disease settings in which spread of the
infection to the pericardium may take place. Pericardial disease occurring in the postoperative
patient (group I) in this series did not ever present as an isolated phenomenon, but rather as part of gross intrathoracic infection in patients with sternal wound infection or mediastinal abscess. Aggressive surgical drainage plus prolonged antibiotic therapy may be successful even in this group of desperately ill pa- tients [ 161. In patients who have undergone esopha- geal surgery, recognition that pericardial involver ent can occur via esophageal perforation and mediasti- nai contamination should prompt the attending physi- cian to look closely for the clinical and laboratory correlates of pericardial disease, particularly in the presence of circulatory compromise and a febrile postoperative course.
Purulent pericarditis secondary to intracardiac in-
July 1975 The American Journal of Medicine Volume 59 73

PURULENT PERICARDITIS-RUBIN, MOELLERING
fection (group III) is likewise difficult to treat. Ideal therapy is eradication of cardiac infection before spread to the pericardium rather than after. Evidence of pericarditis has been noted in 13.2 per cent of pa- tients with bacterial endocarditis examined at nec- ropsy [ 171. Myocardial abscesses have been found at autopsy in about 20 per cent of patients with en- docarditis, and in a small percentage of patients with bacteremia [ 18,191. The risk of development of both myocardial abscesses and purulent pericarditis ap- pears to be especially high in patients with endocar- ditis due to Staph. aureus. In one recent report [20] of autopsies, in 39 patients who died with Staph. au- reus endocarditis, 36 per cent had myocardial ab- scesses and 10 per cent had purulent pericarditis. In bacterial endocarditis, myocardial abscesses may develop as localized lesions secondary to the sys- temic bacteremia or from direct extension from the infected ualvular vegetation [ 19,2 1,221. They are dif- ficult to detect clinically. Their presence should be suspected under the following circumstances: con- tinuing evidence of infection in patients with bacterial endocarditis receiving effective antibiotic chemother- apy [ 18,191, particular electrocardiographic abnor- malities [ 18,231 and circulatory compromise not ex- plainable by valvular dysfunction alone. Infection spreading from aortic valve vegetations into the ad- joining high septal tissue may be associated with the following electrocardiographic findings: a prolonged P-R interval, atrioventricular dissociation, left bundle branch block and multifocal ventricular ectopic beats [23]. In mitral valve infection, accelerated junctional rhythms and Wenckebach type block may occur be- cause of the close relation of the mitral valve and junctional tissue. Unfortunately, isolated, scattered myocardial abscesses are often silent until after irre- versible spread to adjoining tissues has occurred. Several workers [24,25] have stressed the impor- tance of erosion of the aortic valve annulus due to in- fection in the pathogenesis of pericarditis in patients with endocarditis, pointing out that this is relatively common in patients with Staph. aureus infection but quite rare in those with Strep. viridans infection.
Group II (pleuropulmonary) and group IV (bactere- mic) patients are worthy of the most attention since they are the most likely to survive. In this series, 6 of the 12 patients in these two groups survived (mortali- ty 50 per cent). It is in these patients that circulatory measurements and close observation for evidence of cardiac tamponade can be most helpful. Ten of these 12 patients manifested such abnormalities. On the other hand, chest pain and pericardial friction rubs were seen only infrequently in this group. The lack of chest pain is not surprising since the visceral and inner surface of the parietal pericardium are in- sensitive to pain [26]. Accordingly, ancillary diag-
nostic clues must be sought. These include the fol- lowing: (1) Echocardiography may be the most help- ful noninvasive technic available. It provides a very sensitive indicator of a pericardial fluid collection and distinguishes clearly pericardial fluid from enlarge- ment of the cardiac silhouette due to tumor or cham- ber dilatation [ 27-321. (2) Electrocardiographic ab- normalities, especially in patients without known cor- onary artery disease, can be useful. However, a di- agnostic pattern [33] is relatively uncommon and was present in only 8 of 23 patients in this series. (3) Enlargement or change in configuration of the cardi- ac silhouette in the absence of pulmonary vascular engorgement on chest roentgenogram may provide evidence of pericardial effusion, although this is rela- tively nonspecific. (4) Cardiac catheterization is the traditional definitive but highly invasive technic that can be used in making the diagnosis prior to surgical intervention.
In this series, associated systemic diseases that interfered with host defense against infection were present in at least 50 per cent of the patients. Of particular interest were two patients with extensive third degree burns who died with purulent pericarditis: one of contiguous spread from a mediastinal site in the setting of a persistent gram-negative bacteremia, and one from bacteremic spread to the myocardium and pericardium. A recent review from the U.S. Army Institute of Surgical Research has documented the importance of suppurative infections of the heart in burn victims, reporting 64 cases over a 17 year peri- od [34]. Among these were four cases of purulent pericarditis, three secondary to contiguous spread from a myocardial abscess and one from mediastini- tis.
Two of the patients in this series had preceding nonsuppurative pericardial disease. This possibility was first suggested by Solomon et al. [35], who cul- tured streptococci at postmortem examination from the pericardium of four patients with uremic pericar- ditis. Others [36-381, reviewing the data in patients with uremic and viral pericarditis, were unable to confirm this association. However, two of our pa- tients, in whom bacterial pericarditis appeared to have complicated preexisting nonsuppurative peri- carditis, reopen this question. At the least, the diag- nosis of bacterial superinfection should be consid- ered and pursued aggressively in any patients with preceding nonsuppurative pericardial disease who suddenly show signs of unexplained infection, espe- cially when there is evidence of circulatory impair- ment [4].
A variety of unusual conditions have been reported to lead to purulent pericarditis, although they were not seen in this series; bacteremic seeding of a site of myocardial infarction with subsequent spread to
74 July 1975 The American Journal oi Medicine Volume 59

PURULENT PERICARDITIS--RUBIN MOEILLERING
the adjacent pericardium [39-411, contiguous
spread through the diaphragm due to a congenital
abnormality or catastrophic rupture through the dia-
phragm (perforated ulcer [42], infected choledochal
cyst [ 431, a pericardioperitoneal communication in a
patient with peritonitis [ 441, subphrenic abscess
[45], etc.), contiguous spread from a retropharyn-
geal abscess to the mediastinum and pericardium
[8] and, finally, penetrating wounds [42,46]. Fortu-
nately, these are rare occurrences.
The pediatric population merits special attention
when considering purulent pericarditis, because sup-
purative disease ranks second only to rheumatic
fever among the causes of pericarditis in this age
group [ 15,471. In this subset of patients, bacteremia
and pleuropulmonary infection are the major etiologic
considerations, with Staph. aureus, Strep. pneumo-
niae, H. influenzae and N. meningitidis being the most
common organisms [ 15,47-501. The major diag-
nostic problem is to distinguish pericardial fluid col-
lections from acute dilatation of the heart secondary
to myocarditis and heart failure [3,48,49]. Friction
rubs are present in only 15 per cent of pediatric pa-
tients with purulent pericarditis [ 151, electrocardio-
graphic abnormalities seen with pericarditis are diffi-
cult to distinguish from those due to myocarditis
[3,15,32,47], and, especially in infants with respira-
tory distress, measurements of pulsus paradoxus are
often inaccurate [3]. The echocardiogram can be
most useful here, and is perhaps the greatest single
advance in the early diagnosis of purulent pericarditis
in this age group [ 321.
Microbiology. Staph. aureus remains the most fre-
quent cause of purulent pericarditis. In this series, in-
fections in 8 of 26 patients were due to Staph. au-
reus. Three of these represented hospital-acquired
infection, one a nosocomial pneumonia and two re-
lated to contaminated intravenous lines and bacter-
emia. Since 1935, at least 15 per cent of cases of
staphylococcal pericarditis have been hospital-ac-
quired [ 21. Boyle’s report [2] and our experience
would suggest that hospital-acquired disease is even
more important today. Complications, particularly
acute constriction [2,47,48,51-531, associated my-
cotic aneurysms of the proximal aorta [54] and sys-
temic bacteremia with metastatic infection, are quite
prevalent in staphylococcal pericardial disease. Be-
cause of the dangers of acute cardiac tamponade or
constriction, circulatory status of patients with staph-
ylococcal pericarditis should be closely monitored to
assess the possible need for thoracotomy and peri-
cardiectomy [2,47,48,51-531.
Kauffman et al. [lo] recently described five pa- tients with pneumococcal pericarditis, reminding us
that this disease has not become extinct. These in- vestigators made the following important clinical ob-
servations: (1) Pericardial friction rubs, pulsus para-
doxus and an enlarged cardiac silhouette may be ab-
sent in this form of the disease despite circulatory
embarrassment. (2) A preceding pneumonia was
present in 93.1 per cent of 113 patients described in
the medical literature, and in 66.6 per cent both
pneumonia and empyema were present. (3) In most
circumstances, pericardial involvement occurs as a
late event in patients, such as alcoholics, in whom
there is a long delay between onset of pneumonia
and initiation of penicillin therapy. Among the cases
recorded since 1945, this delay in obtaining therapy
averaged 21 days [ 10,55-581. Both of our patients
with pneumococcal pericarditis had pneumonia and
empyema; both had been ill and presumably had
pneumonia for some days prior to their admission to
the hospital (one was an alcoholic who had been on
a binge and one was an elderly resident in a nursing
home); both lacked friction rubs, although other evi-
dence of pericardial disease was present.
In 1950, Zimmerman [59] predicted an increase in
the incidence of infection due to fungi because of the
wide use of antimicrobial and cytotoxic agents. At
the time of Boyle’s review article [ 21 (all cases re-
ported up through 1957), no case of Candida or As-
pergillus infection had been described. Since then a
variety of single case reports of Aspergillus pericardi-
tis have appeared [60], but the finding in this series
of five cases of fungal pericarditis is the first major
confirmation of Zimmerman’s prediction as far as
pericardial infection is concerned. In this series all
the patients with fungal pericarditis had received
broad-spectrum antimicrobial therapy. Three had
underlying diseases or were receiving drugs that ren-
dered them immunosuppressed, and two had recent-
ly undergone major surgical procedures. A closely
related case was that due to Nocardia asteroides in a
renal transplant patient who was receiving cortico-
steroids, azathioprine and broad-spectrum antibiot-
ics. Other cases due to Nocardia have been reported
[ 6 1,621 and, like the true fungal cases, carry a mor-
tality rate approaching 100 per cent.
H. influenzae infection was documented in two pa-
tients: one a 26 year old healthy adult with a probable
H. influenzae infection of the upper respiratory tract complicated by bacteremia that infected the pericar-
dium: and one a 14 month old child with bacteremia
and meningitis. H. influenzae pericarditis has not
been uncommon in the pediatric population, particu-
larly in the age group under 5 [3,15,47-491. Usually
these patients had a history of acute respiratory dis-
ease (laryngitis or pneumonia); meningitis was fre-
quently present; and in only one did pericarditis occur
without evidence of infection elsewhere [63-66 1. All
but three of the previously described patients with H. influenzae pericarditis have been less than 12 years
July 1975 The American Journal of Medicine Volume 59 75

PURULENT PERICARDITIS-RUBIN. MOELLERING
of age [66,67]. Crossley et al. [66] surveyed this subject in detail and pointed out that there may be an increasing incidence of H. influenzae type b disease in adults, not only of the pericardium, but also of the lungs, epiglottis, joints and meninges. This perhaps reflects a decrease in the prevalence of bactericidal antibody against type b H. influenzae in the adult pop- ulation [ 68-7 1 ] .
There have been a large number of reports [72- 88] of pericarditis associated with meningococcal disease, and there has been some confusion as to when in the course of meningococcal infection the pericardium becomes infected and whether or not immunologic mechanisms may play a role [87,88]. Our single case of meningococcal disease demon- strates that the pericardium may become infected very early in the bacteremic process. Others [83- 86] have pointed out that meningococcal pericarditis may occur without evidence of meningococcal dis- ease elsewhere, presumably due to a transient bac- teremia that had no other clinical effects. In addition, in several recent reports [87,88], it has been sug- gested that late pericarditis may commonly occur in the convalescent stage of meningococcal disease. This seems to represent a hypersensitivity phenome- non, does not require antimicrobial therapy, and usu- ally responds to salicylate and/or corticosteroid ther-
apy. A wide variety of miscellaneous causes of purulent
pericarditis were noted in this series and others have been reported in the literature: Clostridium species [89], Salmonella species [41,90-921, a variety of other gram-negative enteric bacilli [2], P. tularensis [2], H. pertussis [93], N. gonorrhoeae [2,94], mixed cases of granulomatous (either tuberculous or acti- nomycotic) and pyogenic infection [2], Vibrio fetus [95], Listeria monocytogenes [96] and others [2]. One of the more interesting single cases in this se- ries was that due to Strep. mitis. In this patient, Strep. mitis infection of the aortic valve spread to the aortic root and then to the pericardium. Strep. mitis is a “viridans” Streptococcus, usually causing a sub- acute form of disease [97]. In our patient, however, an acute bacterial endocarditis was caused, analo- gous to that usually associated with Staph. aureus in- fection. This is an example of the point emphasized by Weinstein et al. [ 181 in their recent review of bac-
terial endocarditis-the differentiation of acute and subacute disease is a clinical one based not on the organism, but rather on the pace of the infection and the virulence of the etiologic agent.
Since such a large variety of organisms can po- tentially cause purulent pericarditis, and since ob- taining material for culture requires invasive technics, it is essential that appropriate culture media and methods be employed from the beginning. Pericardial fluid should routinely be cultured for aerobic and an- aerobic bacterial pathogens, as well as for acid-fast bacilli and fungi. Treatment. As with any localized form of infection, the therapy of purulent pericarditis requires adequate drainage and appropriate antimicrobial therapy. Some workers have advocated the use of repeated pericardiocenteses for drainage [98], and this was successful in two of our six patients who survived, in association with 4 to 6 weeks of antimicrobial thera- py. However, recurrences of effusions are the rule and multiple pericardial aspirations may be hazard- ous [99], so we, and others [ 10,48,56] have quickly resorted to open drainage if one or two pericardio- centeses are not successful in controlling fluid accu- mulation. Acute pericardial constriction also de- mands prompt surgical intervention. Whether peri- cardiectomy or just a pericardial window will be nec- essary is dependent upon what is found at operation: adherent, thickened pericardium with or without thick pus requires pericardiectomy; whereas thinner fluid, with acutely rather than chronically inflammed peri- cardium, may be treated with a pericardial window. Both the transthoracic and the subxiphoid approach have been utilized for pericardial windows [ lOO,lOl]. The latter has the advantage that it does not require violation of the pleural space.
Antimicrobial therapy is the basis of the medical management. A variety of reports of intrapericardial instillation of antibiotics in such patients have ap- peared [2,6,102,103], but a recent study by Tan et al. [ 1041 showing excellent penetration of antimicro- bial agents into pericardial fluid suggest that this is not necessary. In our limited experience, prompt drainage and adequate drug therapy prevented the occurrence of chronic constrictive pericarditis, a complication noted in the past in some patients with purulent pericarditis.
REFERENCES
1. Galen C: De Anatomicus Administrationibus (translated by Dis Child 124: 591. 1972. Singer C), New York, Oxford University Press, 1956. p 4. 192.
Spiegel AM, Sherwood GK, Hyslop NE Jr: Purulent peri- carditis due to Bacteroides. Manuscript in preparation.
2. Boyle JD, Pearce ML, Guze LB: Purulent pericarditis: re- 5. Case Records of the Massachusetts General Hospital view of literature and report of 11 cases. Medicine 40: (Case 30-1968). N Engl J Med 279: 206, 1968. 119, 1961. 6. Case Records of the Massachusetts General Hospital
3. Rubenstein JJ, Goldblatt A, Daggett WM: Acute constric- (Case 53-1989). N Engl J Med 281: 1473, 1969. tion complicating purulent pericardiiis in infancy. Am J 7. Still GF: Observations on suppurative pericarditis in chil-
76 July 1975 The American Journal of Medlclne Volume 59

8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
dren. Br Med J 2: 606. 1901. Chatard JA: Acute pericarditis complicating acute lobar
pneumonia. Johns Hopkins Hosp Rep 15: 155, 1910. Pyrah LN, Pain AB: Acute suppurative pericarditis, two
cases successfully treated by operation. Lancet 1: 905. 1933.
Kauffman CA, Watanakunakorn C. Phair JP: Purulent pneumococcal pericarditis; a continuing problem in the antibiotic era. Am J Med 54: 743, 1973.
Hahn RS, Holman E, Frerichs JB: The role of the bronchial artery circulation in the etiology of pulmonary and peri- cardial suppuration. J Thorac Surg 27: 121, 1954.
Munnell ER, Hammarsten JM: Purulent pericarditis; a PO-
tential surgical problem. Am Rev Respir Dis 86: 917, 1962.
Nikolaew GF: Du role des abces du myocarde dans la pa- thogenie des pericardites suppurees. Presse Med 45: 926, 1937.
Streider JW, Sandusky WR: Pericardiostomy for suppura- tive pericarditis. N Engl J Med 225: 317, 1941.
Keith JD, Rowe RD, Vlad P: Heart Disease in Infancy and Childhood, 2nd ed, New York and London, The MacMil- Ian Co.. 1967, p 970.
Abu-Nassar HJ, Yow EM, Alexander JK, Lewis JM: Pri- mary staphylococcal pericarditis complicating cardio- tomy. Ann Intern Med 60: 135. 1964.
Buchbinder NA, Roberts WC: Left-sided valvular active in- fective endocarditis. Am J Med 53: 20. 1972.
Weinstein L, Rubin RH: Infective endocarditis-1973. Progr Cardiovasc Dis 16; 239, 1973.
Lerner PI. Weinstein L: Infective endocarditis in the antibi- otic era. N Engl J Med 274: 199, 259, 323, 387, 1966.
Watanakunakorn C, Tan JS, Phair JP: Some salient fea- tures of Staphylococcus aureus endocarditis. Am J Med 54: 473, 1973.
Sanson J. Slodki S, Gruhn JG: Myocardial abscesses. Am Heart .I 66: 301, 1963.
Ryon DS. Pastor BH, Myerson RM: Abscess of the myo- cardium. Am J Med Sci 251: 698, 1966.
Roberts NK. Somerville J: Pathological significance of electrocardiographic changes in aortic valve endocardi- trs (abstract). Br Heart J 31: 395, 1969.
Utley JR. Mills J: Annular erosion and pericarditis; compli- cations of endocarditis of the aortic root. J Thorac Car- diovasc Surg 64: 76, 1972.
McCall I: Pericarditis due to a mycotic aneurysm in sub- acute bacterial endocarditis. Guys Hosp Rep 107: 34, 1958.
Kapps JA: Pain from pleura and pericardium. Association for Research in Nervous and Mental Disease, Research Publication No. 23, 1943, p 263.
Feigenbaum H, Zaky A, Grabhorn LI: Cardiac motion in patients with pericardial effusion: a study using reflect- ed ultrasound. Circulation 34: 6 11, 1966.
Feigenbaum H. Walhausen JA, Hyde LP: Ultrasound diag- nosis of pericardial effusion. JAMA 191: 7 11, 1965.
Rothman J, Chase NE, Kricheff II, Mayoral R, Berenbaum ER: Ultrasonic diagnoses of pericardial effusion. Circu- lation 35: 358, 1967.
Feigenbaum H, Zaky A, Waldhausen JA: Use of ultra- sound in the diagnosis of pericardial effusion. Ann In- tern Med 65: 443, 1966.
Feigenbaum H, Zaky A, Waldhausen JA: Use of reflected ultrasound in detecting pericardial effusion. Am J Car- diol 19: 84, 1967.
Pieroni DR, Park SC, Holbrook PR, Houghton PB: Echocar- diographic diagnosis of septic pericarditis in infancy, J Pediatr 82: 689, 1973.
Surawicz B. Lasseter KC: Electrocardiogram in pericardi- tis. Am J Cardiol 26: 471, 1970.
Munster AM, DiVincenti FC. Foley FD. Pruitt BA Jr: Cardi-
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
PURULENT PERICARDITIS--RUBIN. MOELLERING
ac infection in burns. Am J Surg 122: 524, 1971 Solomon C, Roberts JE, Lisa JR: The heart in uremia. Am
J Pathol 18: 729, 1942. Bailey GL, Hampers CL, Hager EB, Merrill JP: Uremic peri-
carditis: clinical features and management. Circulation 38: 582, 1968.
Koontz CH. Ray CG: Coxsackie virus infection in myoperi- carditis. Am Heart J 82: 750, 1971.
Saiainani GS, Krompati E, Slodli SJ: Heart disease due to Coxsackie virus B infection. Medicine 47: 133, 1968.
Katz A: Abscess of the myocardium complicating infarc- tion: report of two cases. Can Med ASSOC J 91’ 1225. 1964.
Murray M: Suppurative pericarditis complicating myocar- dial infarction. Br Med J 1: 223, 1968.
Schatz JW, Wiener L, Gallagher HS, Eberly RJ: Salmonel- la pericarditis: an unusual complication of myocardial infarction. Chest 64: 267, 1973.
Romhilt DW, Alexander JW: Pneumopyopericardium sec- ondary to perforation of benign gastric ulcer. JAMA 191: 140, 1965.
Barzel US, Friedman R, Glotzer P: Choledochal cyst and acute purulent pericarditis. N Engl J Med 276: 1247, 1967.
Devin J, Merdinger WF: Pericardio-peritoneal communica- tion-an additional etiologic factor in purulent pericardi- tis. Dis Chest 56: 454, 1969.
Ochsner A, DeBakey M: Subphrenic abscess: collective review and an analysis of 3608 collected and personal cases. Int Abstr Surg 66: 426, 1938.
Meyer HW: Pneumopyopericardium. J Thorac Surg 17: 62, 1948.
Nadas AS, Levy JM: Pericarditis in children. Am J Cardiol 7: 109. 1961.
Benzing G Ill, Kaplan S: Purulent pericarditis. Am J Dis Child 106: 289, 1963.
Gersony WM, McCracken GH Jr: Purulent pericarditis in infancy. Pediatrics 40: 224, 1967.
Tahernia AC, Sharif H: Purulent pericarditis in childhood, one due to anaerobic streptococcus. Clin Pediatr 9: 499, 1970.
Thomas GI. Gregores BJ, Perry DM. Andrus W: Pericardi- ectomy for acute constrictive staphylococcal pericardi- tis; report of a case. N Engl J Med 267: 440. 1962.
Caird R. Conway N, McMillan IKR: Purulent pericarditis fol- lowed by early constriction in young children. Br Heart J 35: 201. 1973.
Folger GM Jr: Buppurative pericarditis; review of the prob- lem plus observations on two patients. Clin Pediatr 5: 225, 1966.
Fitzgerald JD, McNicol MW: Acute suppurative pericardi- tis, with death from ruptured mycotic aneurysm of the aorta. Postgrad Med J 40: 36, 1964.
Grossman C: Pneumococcal pericarditis treated with in- trapericardial penicillin: report of a case. N Engl J Med 233: 689, 1945.
McKusick VA. Harvey A McG: Diseases of the pericar- dium. Adv Intern Med 7: 157, 1955.
Case Records of the Massachusetts General Hospital (Case 45221). N Engl J Med 260: 1135, 1959.
lturino JL. Holland RH: Emergency surgical management of acute pericarditis. J Thorac Cardiovasc Burg 45: 324, 1963.
Zimmerman LE: Candida and Aspergillus endocarditis. Arch Pathol 50: 591, 1950.
Fraumeni JF Jr, Fear RE: Purulent pericarditis in aspergit- losis. Ann Intern Med 57: 823, 1962.
Busens GP, Al-Shamma A, Rowe JC, Herbert CC, Bassis ML. Coggs GC: Purulent constrictive pericarditis caused by Nocardia asteroides. Ann Intern Med 67: 1021, 1967.
July 1975 The American Journal of Medicine Volume 59 77

PURl KENT PERICARDITIS-RUBIN, MOELLERING
62.
63.
64.
65.
66.
67.
66.
69.
70.
71.
72.
73.
74.
75.
76.
77.
76.
79.
80.
81.
Chavez CM, Causey WA, Conn JH: Constrictive pericardi- tis due to infection with Nocardia asteroides. Chest 61: 79, 1972.
Gotoff SP, Fousek MD: Purulent pericarditis due to Hemo- philus influenzae, type b. J Pediitr 61: 576, 1962.
Beck PD, Kahn LB: Purulent pericarditis: report of a case. South African Med J 43: 1450.1969.
Hawker RE, Celermajer JM. Robertson SW: Pericardial effusion complicating Haemophilus influenzae meningi- tis. Aust Paediitr J 8: 102. 1972.
Crossley K, Bigos T, Joffe CD: Hemophilus influenzae per- icarditis; a report of two cases in adults with a summa- ry of the literature. Am Heart J 85: 246, 1973.
Hensler L: lnfluenzabazillen Perikardiiis. Cardiologia 27: 154,1955.
Fothergill LD, Wright J: Influenza1 meningitis: the relation- ship of age incidence to the bactericidal power of the blood against the causal organism. J lmmunol 24: 273, 1933.
Collier AM, Connor JD, Nyhan WL: Systemic infection with Hemophilus influenzae in very young infants. J Pediatr 70: 539, 1967.
Norden CW, Callerame ML, Baum J: Hemophilus meningi- tis in an adult. N Engl J Med 282: 190, 1970.
Gump DW, Tarr P. Phillips CA, Forsyth BR: Bactericidal antibodies to Hemophilus influenzae. Proc Sot Exp Biol Med 138: 76,197l.
Herrick WW: Meningococcic pericarditis. Report of 12 cases. Med Clin North Am 2: 411, 1918.
Lowe CU, Diamond LK: Myocardiiis and pericardiiis in meningococcic infections. Am J Dis Child 75: 860, 1948.
Lukash WM: Massive pericardial effusion due to meningo- coccic pericarditis. JAMA 185: 598, 1963.
Wolf RE. Bribara CA: Meningococcal infections at an Army training center. Am J Med 44: 243, 1968.
Saslaw S. Diserens RV: Purulent pericardiil effusion com- plicating meningococcal meningitis. N Engl J Med 263: 1074.1960.
Maron BJ, Macoul KL, Benaron P: Unusual complications of meningococcal meningitis. Johns Hopkins Med J 131: 64, 1972.
Williams DN, Geddes AM: Meningococcal meningitis com- plicated by pericarditis, panophthalmitis, and arthritis. Br Med J 2: 93, 1970.
Lebowitz WB, Nespole AJ: Purulent pericardiiis complicat- ing meningococcal meningitis. Am J Dis Chikt 113: 385, 1967.
Penny JL, Grace WJ. Kennedy RJ: Meningococcic peri- carditis; a case report and review of the literature. Am J Cardiol 18: 281, 1966.
Scott LP, Knox D. Perry LW, Pineros-Torres FJ: Meningo- coccal pericarditis; report of two cases, one complicat- ed by acute constrictive pericarditis. Am J Cardiol 29: 104,1972.
82.
83.
84.
85.
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.
96.
99.
100.
101.
102.
103.
104.
O’Connell B: Pericarditis following meningococcic menin- gitis. Am J Dis ChiM 126: 265. 1973.
Orgain ES, Poston MA: Pericardiiis with effusion due to the meningococcus. Am. Heart J 18: 368.1939.
Roberts KB, Neff JM: Meningococcal pericarditis without meningitis in a child. Am J Dis Child 124: 440, 1972.
Wansbrough-Jones MH, Wong OP: Meningococcal peri- carditis without meningitis. Br Med J 2: 344, 1973.
Herman RA, Rubin HA: Meningococcal pericarditis without meningitis presenting as tamponade. N Engl J Med 290: 143,1974.
Morse JR, Oretsky MI, Hudson JAM: Pericarditis as a com- plication of meningococcal meningitis. Ann Intern Med 74: 212, 1971.
Pierce HI, Cooper EB: Meningococcal pericarditis; clinical features and therapy in five patients. Arch Intern Med 129: 918, 1972.
Brown R: Clostridial pericarditis diagnosed antemortem. Am Heart J 70: 801, 1965.
Levis HS, Hosier DM: Salmonella pericarditis: report of a case and review of the literature. Ann Intern Med 55: 817. 1961.
Shilkin KB: Salmonella typhimurium pancarditis. Postgrad Med J 45: 40, 1969.
Bird T: Salmonella typhimurium pericarditis. Br Heart J 3 1: 659, 1969.
Ross DE: Suppurative pericarditis. Am J Surg 43: 134, 1939.
Victzke WM: Gonococcal arthritis with pericarditis. Arch Intern Med 117: 270, 1966.
Killam HAW, Crowder JG. White AC, Edmonds JH Jr: Peri- carditis due to Vibrio fetus. Am J Cardiol 17: 723, 1966.
Kahn A, Rosen KM, Rahimtoola SH, Gunnar RM: Listeria bacteremia with acute pericarditis. Chest 60: 496, 1971.
Rosebury T: Bacterial and Mycotic Infections of Man, 4th ed (Dubos RJ, Hirsch JG, eds), Philadelphia, J.B. Lippin- cott Co., 1965, p 326.
Horan JM: Acute staphylococcal pericarditis. Pediatrics 19: 36. 1957.
Fowler NO, Manitsas GT: Infectious pericarditis. Progr Cardiovasc Dis 16: 323, 1973.
Schlein EM, Bartley TD, Spooner GR, Cade R: A simplified surgical approach to therapy of uremic pericarditis with tamponade. Ann Thorac Surg 10: 548, 1970.
Baue AE, Blakemore WS: The pericardium. Ann Thorac Surg 14: 81, 1972.
Lamb AE: Treatment of acute infectious pericarditis and chronic constrictive pericarditis. Dis Chest 35: 212, 1959.
Schweitzer RS: Purulent pericarditis. Am J Surg 91: 906, 1956.
Tan JS. Holmes JC, Fowler NO, Manitsas GT. Phair JP: Antibiotic levels in pericardiil fluid. J Clin Invest 53: 7, 1974.
78 July 1975 The American Journal of Medklne Volume 59