CLINICAL L McCoy/Minneapolis MN ... John Koenig, Region VI ... 206 Introducing Clinical Laboratory...
68
JOURNAL OF THE AMERICAN SOCIETY FOR CLINICAL LABORATORY SCIENCE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . CLINICAL LABORATORY SCIENCE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Focus: Human Immunodeficiency Virus Fall 2006 Volume 19/Number 4
Transcript of CLINICAL L McCoy/Minneapolis MN ... John Koenig, Region VI ... 206 Introducing Clinical Laboratory...

JOURNAL OF THE AMERICAN SOCIETY FOR CLINICAL LABORATORY SCIENCE
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CLINICAL LABORATORY
SCIENCE. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Focus: Human Immunodeficiency Virus
Fall 2006 Volume 19/Number 4

ADDRESS CHANGES
ASCLS MEMBER EDITORSEditor-in-ChiefSusan J Leclair PhD CLS(NCA)Department of Medical Laboratory ScienceUniversity of Massachusetts DartmouthNorth Dartmouth MA [email protected]
Continuing Education EditorGeorge A Fritsma MS MT(ASCP)Pathology and Clinical Laboratory Sciences1705 University Boulevard RMSB 448U of Alabama at BirminghamBirmingham AL 35294-1212205-934-1348, fax [email protected]
Clinical Practice EditorBernadette Rodak MS CLSpH(NCA)Clinical Laboratory Science ProgramIndiana UniversityClarian Pathology Laboratory 6002F350 West 11th StreetIndianapolis IN 46202317-491-6218, fax [email protected]
Research and Reports EditorDavid G Fowler PhD CLS(NCA)University of Mississippi Medical CenterDept of Clinical Laboratory Sciences2500 North State StJackson MS [email protected]
Clinical Laboratory Science (ISSN 0894-959X) is published quarterly by the American Society for Clinical Laboratory Science, 6701 Democracy Blvd., Suite 300, Bethesda MD 20817; (301) 657-2768; (301) 657-2909 (fax). Annual Subscription Rates: USA Canada Non-USA Individuals $50 $65 $100 Institutions $65 $65 $100Questions related to subscriptions should be addresssed to: [email protected]. The cost of single copies is $10. Requests to replace missing issues free of charge are honored up to six months after the date of issue. Send requests to ASCLS headquarters. Annual membership dues of ASCLS are $92, $40 of which is allocated to a subscription of CLS. Periodical postage paid at Bethesda, MD and other additional mailing offices.
Contributing EditorsEileen Carreiro-Lewandowski/N Dartmouth MADeborah Josko/Newark NJElaine Kohane/Newark NJRebecca Laudicina/Chapel Hill NCConnie Mahon/San Antonio TXLinda Smith/San Antonio TXMichelle Wright-Kanuth/Galveston TX
REVIEW BOARDRichard Bamberg/Greenville NCKathleen Blevins/Oklahoma City OKDianne Cearlock/DeKalb ILPeter Colaninno/Jamaica NYJo Ann Fenn/Salt Lake City UTEllis Frohman/St Louis MOMildred Fuller/Norfolk VAAbraham Furman/Portland ORRichard Gregory/Indianapolis INJesse Guiles/Newark NJLester Hardegree/Bluffton SCDenise Harmening/Baltimore MDDaniel Hoefner/Elon, NCLinda Hogan/Wichita KSVirginia Hughes/Montgomery ALLinda Kasper/Indianapolis INNancy Konopka/Gettysburg PARobin Krefetz/Cherry Hill NJLinda Laatsch/Milwaukee WIHal Larsen/Lubbock TXDonna Larson/Gresham ORLouann Lawrence/New Orleans LACraig Lehmann/Stony Brook NYElizabeth Leinbach-Kenimer/Augusta GALynn Little/Dallas TXCarol McCoy/Minneapolis MNDavid McGlasson/Lackland AFB TXSharon Miller/St Charles ILIsaac Montoya/Houston TXHarriette Nadler/King of Prussia PAJoan Prince/Milwaukee WIMargaret Reinhart/Philadelphia PAJohn Seabolt/Lexington KYStephen Sodeke/Tuskegee AL
P.A.C.E.® LiaisonDiane Kumashiro/Kaneohe HISharon Miller/St Charles IL
ASCLS BOARD OF DIRECTORS 2005-2006Bernadette Bekken, PresidentShirlyn McKenzie, President-ElectSusan Morris, Past PresidentScott Aikey, Secretary TreasurerBobby Lee, Region IMary Ann McLane, Region IILynn Ingram, Region IIILinda Kasper, Region IVRick Panning, Region VJohn Koenig, Region VIDebra Faubion, Region VIISuzanne Zanto, Region VIIIDonna Reinbold, Region IXSheri Gon, Region XKarine Dunn, First Year ProfessionalSharon Bobryk, Student Forum Chair
ASCLS Headquarters Executive StaffElissa Passiment, Executive Director
EDITORIAL OFFICEIC Ink858 Saint Anne’s DriveIowa City IA 52245(319) 354-3861; (319) 338-1016 (fax)[email protected]/leadership/cls/index.htm
Managing EditorMargaret LeMay-Lewis MFA
PRODUCTIONBB Design Studio2416 E Avenue NECedar Rapids IA 52402
Advertising for CLS is accepted in accordance with the ad-vertising policy of the ASCLS. Contact the CLS advertising representative at (301) 657-2768.Manuscript Submissions: To encourage consistency in style, refer to guidelines in Scientific Style and Format – The Council of Biology Editors Manual for Authors, Editors, and Publishers, 6th ed. Detailed instructions for authors are available on the ASCLS site. Contact the CLS Editorial Office for more information. All articles published represent the opinions of the authors and do not reflect the official policy of ASCLS or the authors’ institutions unless specified. Microfilm and microfiche editions of CLS are available from University Microfilms, 300 N Zeeb Road, Ann Arbor MI 48106.
Correspondence related to editorial content should be mailed to: IC Ink, 858 Saint Anne’s Drive, Iowa City IA 52245; (319) 354-3861; (319) 338-1016 (fax). [email protected]
© Copyright 2006 American Society for Clinical Laboratory Science Inc. All rights reserved.
ASCLS Mission/Vision StatementThe American Society for Clinical Laboratory Science serves as the voice of all clinical laboratory professionals, creating a vision for the advancement of the clinical laboratory practice field, and advocating the value and role of the profession ensuring safe, effective, efficient, equitable, and patient centered healthcare.
AMERICAN SOCIETY FOR CLINICAL LABORATORY SCIENCE
6701 Democracy Blvd, Suite 300Bethesda, Maryland 20817(301) 657-2768, (301) 657-2909 (fax)www.ascls.org
ASCLS Core ValuesCore Values include enhancing quality standards and patient safety; providing professional development opportunities; promoting expanded roles and contributions of clinical laboratory professionals to the healthcare team; increasing the diversity in the profession; and expanding the voice and role of under-represented individuals and groups.
Inclusion in the journal of product names or author opinions does not constitute endorsement by either Clinical Laboratory Science or ASCLS.
Postmaster: Send address changes to Clinical Laboratory Science6701 Democracy Blvd, Suite 300Bethesda MD 20817
Postmaster: Send address changes to Clinical Laboratory Science6701 Democracy Blvd, Suite 300Bethesda MD 20817

CLINICAL LABORATORY
SCIENCE
DIALOGUE AND DISCUSSION194 United States Government Accountability Office (GOA) Targets Laboratory Quality
Judy Davis, Don Lavanty 196 The Rule of Law and Bioterrorism Cheryl R Caskey
CLINICAL PRACTICE203 Diegoa Antigen Frequency and Diegoa Frequency in a South Texas Community
Christina Thompson 206 Introducing Clinical Laboratory Science: CLS Students Help Shape the Future Barbara Sawyer, Joel D Hubbard, Lori Rice-Spearman 214 The Use of B-type Natriuretic Peptide to Diagnose Congestive Heart Failure Jeffery R Gray 218 Factor V Leiden: An Overview Donna M Shaw 222 Two Non-invasive Diagnostic Tools for Invasive Aspergillosis: (1-3)-β-D-Glucan and the Galacto-
mannan Assay Amy Kelaher
RESEARCH AND REPORTS225 Cessation of Menstruation Improves the Correlation of FPG to Hemoglobin A1c in Caucasian
Women Kristina Jackson Behan
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS231 An Overview of the Human Immunodeficiency Virus Featuring Laboratory Testing for Drug Resistance Emil Scosyrev
246 CONTINUING EDUCATION QUESTIONS
ELECTRONIC MEDIA REVIEW250 Image Atlas Series and in QUIZator Series James T Griffith
252 2006 ANNUAL INDEX
FALL 2006 VOLUME 19/NUMBER 4

194 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
Once again, the quality of services provided by clinical labo-ratories across the nation is under the scrutiny of the federal government. CLIA ’88 was implemented in 1992 to ensure that all laboratories meet the same minimal standards, based on the complexity of testing performed rather than by loca-tion. However, laboratory quality problems recently surfaced in several locations, prompting proposed federal legislation and a study of clinical laboratory quality by the US Govern-ment Accountability Office (GAO) to assess:
• the quality of laboratory testing, • the effectiveness of surveys, complaint investigations, and
enforcement actions in detecting problems and ensuring compliance, and
• the adequacy of the oversight provided by the Centers for Medicare and Medicaid Services (CMS) to the CLIA program.
The study, presented to Congress in June 2006, focused on oversight by CMS, state CLIA-exempt programs, and labora-tory accrediting agencies including the College of American Pathologists (CAP), Joint Commission on Accreditation of Healthcare Organizations (JCAHO), and COLA. Principal findings cited by GAO in the study include:
1. Insufficient data exists to identify the extent of the problem.CMS state survey data prior to 2004 is not available. When inspection guidelines changed in 2004, the prior data was purged. GAO is concerned that potential qual-ity problems are masked.
2. Announced inspections are problematic.Laboratories prepare specifically for inspection so an-nounced inspections fail to provide a true picture of the
laboratory’s quality. CAP and JCAHO inspections have since begun announced inspections. All agree that physi-cian office laboratory inspections should be announced due to disruption of patient care, but the amount of noti-fication provided should not exceed two weeks, the current maximum notice CMS allows for state agencies.
3. State agencies do not use consistent terminology to identify all serious deficiencies.Standard-level deficiencies cited in one state might be condition-level deficiencies in another state.
4. The balance between an educational approach and a regu-latory focus is skewed too much toward education.Most agencies emphasize the importance of using the inspection process to educate; however, GAO states that such an approach has resulted in phase-ins for new quality control requirements and cytology proficiency testing that are too lenient.
5. Few complaints have been submitted due to perceived risk of punitive action and individuals’ not knowing how/where to direct complaint.No federal whistleblower protection exists for laboratory workers regarding CLIA. CAP-substantiated complaints increased from 40 in 2003 to 70 in 2004. CAP-accred-ited laboratories are now required to display a poster with a number to report complaints and to have a non-retalia-tory policy, however, the poster was not implemented until the fall of 2004.
6. Proposed sanctions are not consistently implemented.GAO expressed concern about the number of laborato-ries that have the same condition-level deficiency survey after survey. In practice, laboratories sometimes correct problems during the grace period before sanctions are actually issued.
7. Proficiency testing (PT) is required three times per year and not four times as mandated by CLIA statute.Initially CMS did not want to overwhelm PT providers so frequently, since many more laboratories became sub-ject to PT when CLIA went into effect. GAO considers this to be a significant quality issue that may result in problems going undetected. CMS disagrees with this finding, contending three PT events per year allow time for laboratories to receive reports and take corrective action before retesting.
WASHINGTON BEAT
United States Government Accountability Office(GAO) Targets Laboratory Quality
JUDY DAVIS, DON LAVANTY
Washington Beat is intended to provide a timely synopsis of activity in the nation’s capitol of importance to clinical laboratory practitioners. This section is coordinated jointly by Judy Davis and Linda Comeaux, Co-chairs of the ASCLS Government Affairs Committee; and Don Lavanty, ASCLS Legislative Counsel. Direct all inquiries to ASCLS, (301) 657-2768 ext. 3022, (301) 657-2909 (fax); or mail to ASCLS, 6701 Democracy Boulevard, Suite 300, Bethesda MD 20817, attn: Washington Beat.

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 195
8. Too many validation surveys are done simultaneously.Validation surveys are required for one percent of state surveys and five percent of accreditation organization surveys. A mix of simultaneous and independent sur-veys should occur to provide a true picture; however, comparing results remains challenging since accrediting organization requirements differ.
9. CMS does not evaluate accrediting organization equiva-lency in a timely mannerAccrediting organizations submit changes in their standards or survey process to CMS but a review of the changes is not required prior to implementation. CMS says delays are due to staffing issues. Although CLIA is funded by fees paid by certified laboratories and funds are available for more staff, federal staffing limits prohibit hiring additional personnel.
10. Proficiency testing suggests quality has not improved in hospital laboratories.PT failures (two of three or two consecutive unsatisfac-tory PT events) in CAP laboratories have increased from 4.1% in 1999 to 6.8% in 2003.
11. CAP volunteer surveyors are less trained and may have a conflict of interest; in addition, conflicts with supervisory team members may affect findings.Although CAP says no factual data shows volunteers are less effective, the agency is increasing inspector-training requirements.
12. CMS does not effectively use available data to assess quality with proficiency testing, sanctions, and complaints.
GAO recommendations include:
• Standardize exempt-state and accrediting organization standards so meaningful comparisons can be done across organizations.
• Limit advance notice for POL inspections to two weeks.
• Focus inspections primarily on regulation, not educa-tion.
• Use appropriate sanctions for laboratories with consecu-tive condition-level deficiencies in the same areas.
• Require all survey organizations to require laboratories to post information on how to file anonymous com-plaints.
• Require quarterly proficiency testing.• Evaluate equivalency of survey organizations prior to expira-
tion of approval period. Review changes in survey organiza-tion inspection requirements prior to implementation.
• Use available revenue to hire enough CLIA staff to fulfill statutory responsibilities.
• Validate an adequate number of survey organizations’ surveys each year.
• Collect and review findings to ensure CLIA requirements are being enforced. Establish a database to monitor ac-tions taken on laboratories that lose accreditation.
CMS, CAP, JCAHO, and COLA all submitted comments and listed changes made in response to the GAO report. CMS and CAP both commented that laboratory quality has improved since CLIA ’88. CMS has implemented a complaint tracking system and is working with accrediting and CLIA-exempt state agencies to improve communication regarding quality issues.
JCAHO also commented, “The personnel standards enacted by CLIA are insufficient to adequately protect patients and the public health” and “the problems underlying failure in laboratory performance that are most often cited by experts in the field are the growing shortage of laboratory technolo-gists and the inadequacy of their training”. ASCLS has long held that competency of laboratory professionals is essential for laboratory quality.
WASHINGTON BEAT

196 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
DIALOGUE AND DISCUSSION
The Rule of Law and Bioterrorism
CHERYL R CASKEY
The Dialogue and Discussion Section is a forum for editorials, short articles, commentaries, and letters to the editor on clinical laboratory science topics and professional issues of general interest to readers includ-ing ASCLS activities and position papers. For more information about submissions to the Dialogue and Discussion section contact: Margaret LeMay-Lewis, Managing Editor, Clinical Laboratory Science Editorial Office, IC Ink, 858 Saint Anne’s Drive, Iowa City, IA 52245. (319) 354-3861. [email protected]
Bioterrorism is defined as the deliberate release of pathogens or their toxins into a civilian population for the purpose of causing illness or death.1 In a world made uncertain by ter-rorists, a chemical weapon or bioterrorism threat or even a hoax can shut down a business for days and create an unique new type of environmental liability, as well as lead to work-place safety issues and other liabilities.2 Physicians and public health officials would bear the brunt of the health nightmare caused by an act of bioterrorism. Mass casualties and the “worried well” would crowd healthcare facilities that barely cope with normal healthcare loads. Often overlooked in thinking about bioterrorism and its effects is the foundation that law provides for effective public health activities.3
The United States Commission on Civil Rights has been warned by the head of the Public Health Association that this country is unprepared for a bioterrorist attack and would be dramatically affected since a large segment of the population is already medically underserved.4
ABBREVIATIONS: BIC = business interruption insurance; BSL = biosafety level; BSC = biosafety cabinets; CDC = Centers for Disease Control and Prevention; COC = chain of custody; FBI = Federal Bureau of Investigation; HSPD-5 = Homeland Security Presidential Directive 5; OSHA = Oc-cupational Safety and Health Act; PPE = personal protective equipment; US = United States.
INDEX TERMS: bioterrorism; civil liberties; rule of law.
Clin Lab Sci 2006;(19)4:196
Cheryl R Caskey MA CLS CLSpIH(NCA) is the Compliance Officer for Omega Diagnostics, L.L.C. in Shreveport LA. She
is also a past president of ASCLS and is currently the editor of ASCLS News.
Address for correspondence: Cheryl R Caskey MA CLS CLSpIH(NCA), Compliance Officer, Omega Diagnostics, L.L.C., One St. Mary Place, Shreveport LA 71101. (318) 681-4531, (318) 681-6927 (fax). [email protected]
Opinions expressed herein are solely those of the author. Correspondence regarding this paper should be addressed to Cheryl R Caskey MA CLS CLSpIH(NCA) at Omega Diagnostics, L.L.C.
THE RULE OF LAWThe use of a biological weapon in the United States would trigger a public health and political emergency. Governmen-tal response to national emergencies in many countries has historically brought about the rule of law.3 The rule of law is the idea that human affairs are governed by law, not the arbi-trary exercise of power, and that under immense pressure, the latter could result in the abandonment of fundamental legal protections for populations. The internment by the United States of Japanese-Americans after Pearl Harbor stands as an example of the fact that governmental action in an emergency can challenge the boundaries of the rule of law and beyond.5 Fred Korematsu was a Japanese-American born in Oakland, California in March 1942, when President Franklin D. Roos-evelt was empowered through legislation to restrict movement of residents of any designated military area or war zone where he felt such restriction was necessary to national security. He issued Executive Order #9066 that declared, “The success-ful prosecution of the war requires every possible protection against espionage and against sabotage to national defense material, national defense premises, and national defense utili-ties.”5 The restrictions ranged from the imposition of curfews to forced removal to “relocation centers” outside Military Area I. Mr. Korematsu had been a loyal, law-abiding American citizen, but rather than submit to confinement, he ran away and posed as Chinese. He was arrested and tried in federal district court for knowingly violating the Civilian Exclusion Order.
More recent examples of the government’s acting in response to national security are President George W. Bush’s secret

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 197
DIALOGUE AND DISCUSSION
domestic spying and foreign bank money tracking programs, both implemented following the September 11, 2001, ter-rorist attacks. President Bush vigorously defended his order authorizing eavesdropping on overseas telephone calls and the email of US citizens with suspected terrorists. He con-tended he was obligated to protect US citizens against attack, which justified a circumvention of the traditional process in a fast-moving, high-tech battle with a shadowy enemy.6 The president did not offer details about how many people were under surveillance, what standard must be met to intercept communications, or what terrorist plots had been disrupted as a result of the program. The recent congressional debate over renewal of the US Patriot Act, a measure bolstering the powers of law enforcement agencies passed shortly after the September 11, 2001 attacks, was fueled by this National Security Agency spy program.
The money tracking program allows US counterterrorism analysts using broad government subpoenas to obtain financial information from a vast database maintained by a company based in Belgium.7 President Bush defended the program with much the same defense used for the National Security Agency’s warrantless wiretap program. Another article published in the wake of the money tracking report said the first newspaper to report this program ran afoul of Section 798 of title 18, the so-called Comint statute. This statute was written in the wake of Japan’s attack on Pearl Harbor and gives intelligence agen-cies a leg up against foreign adversaries by prosecuting anyone who passes on communications intelligence that “could be prejudicial to the safety or interest of the US or for the benefit of any foreign government to the detriment of the US”.
The American legal system is not designed to deal with such complex and insidious acts of violence caused by bio-weapons. The two areas of American law most immediately affected by bioweapons would be public health law and the law managing disasters or emergencies.5 The powers and provisions in these two areas of law relevant to responding to a bioterrorism event were created to deal with other types of emergencies, not something as unique as the intentional use of pathogenic microorganisms to make large numbers of individuals ill or die.
Tabletop exercises and simulated bioterrorism events have demonstrated that neither public health law nor emergency management law could currently support an effective re-sponse to a major bioweapons event.8 The government would be under extreme pressure to take actions that might sweep away the rule of law in the midst of panic or uncertainty.
Structurally, in the United States, political power is divided between state and federal governments. Under the US Con-stitution, state governments, not the federal government, have the primary legal authority and responsibility for public health.3 A bioweapons event would trigger a public health emergency and state governments and legal systems would be critical in addressing the event and its aftershocks.
The events surrounding Hurricane Katrina in August 2005 illustrate the constitutional framework created by our founders in which each state ceded some of its powers to the federal government to create one united yet limited central government. Accordingly, state and local govern-ments assume the first and foremost line of defense against civil disturbance and threats to public safety. President Harry Truman issued Executive Order 10427 in 1952 which emphasized that federal disaster assistance was intended to supplement, not supplant, the resources of state, local, and private sector organizations.9 State and local governments, who know the unique requirements of their citizens and geography and are best positioned to respond to incidents in their own jurisdictions, play a large role in disaster response. Today, the centerpiece legislation for providing federal aid in disaster relief is the Robert T. Stafford Disaster Relief and Emergency Assistance Act (Stafford Act) which reinforces the principle that response efforts should first utilize state and local resources.9 This act establishes a process for State governors to request assistance from the federal government when an incident overwhelms state and local resources and is frequently invoked in disaster and emergency response such as Katrina. Governors of affected states request a disaster declaration from the president.10 The Homeland Security Act was enacted in 2002 and President Bush issued Homeland Security Presidential Directive 5 (HSPD-5) in February 2003.9 This order established national policies, priorities, and guidelines to strengthen US homeland security. The components of the national response plan, when applied together, should provide for a unified command structure to serve as the local, multi-agency coordination center for the effective and efficient coordination of federal, state, local, tribal, nongovernmental, and private-sector organizations with primary responsibility for incident-related prevention, response, and recovery actions.
Soon after Katrina made landfall, state and local authorities understood the devastation was serious, but, due to the de-struction of infrastructure and response capabilities, lacked the ability to communicate with each other and coordinate a response. Federal officials struggled to perform responsi-

198 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
bilities generally conducted by state and local authorities.11 Shortfalls in the federal response to Hurricane Katrina high-light that current homeland security architecture, to include policies, authorities, plans, doctrine, operational concepts, and resources at the federal, state, local, private sector, and community levels, must be strengthened and transformed. At the most fundamental level, the current system fails to define federal responsibility for national preparedness in catastrophic events. Instead, the United States currently has guidelines and individual plans, across multiple agencies and levels of government that do not yet constitute an integrated national system that ensures unity of effort.
The legal authority and power to respond to traditional threats to US national security rests primarily with the federal government. The structural challenge to the rule of law here is that state governments and public health law are as or more important than the federal government and federal law. The US has no legal framework for dealing with a serious national security threat that depends so heavily on the quality of state public health law and its institutions.
Simulated bioterrorist events have shown how difficult co-operation between state and federal government personnel can be in times of emergency.8 Federal-state turf wars and lack of coordination could be deadly in preventing effective public health responses to such an event.
There are several components to a bioweapons challenge to the rule of law. First, such an event would implicate many different areas of the law, including public health, emergency management, civil rights, criminal, and national security law. Second, the law would have to:
• deter the development and use of bioweapons;• prepare state and federal governments for the possibility
of bioterrorism;• empower state and federal governments to respond ef-
fectively during a bioweapons event;• discipline governmental exercises of power to protect
individual rights as much as possible; and• facilitate identification of and retribution against the
bioterrorists.
Third, public health law would be on the forefront during such an event, but US public health law experts argue this body of law is antiquated.12 A bioweapons event would trigger many legal worries, including the liability of overrun hospi-tals and healthcare professionals operating in an emergency
environment, the liability of drug and vaccine manufacturers, and the inevitable lawsuits after the crisis is over.
Fourth, there are similar concerns about federal and state emergency management laws. Fifth, the US legal system is highly protective of individual rights. The US concept of government is that of a limited government, one that cannot infringe arbitrarily on the rights and freedoms of citizens. A bioweapons event could exert enormous pressure on the US government to infringe in drastic ways on individual rights without going through the normal procedural and substantive tests for such restrictions. Forced quarantine or isolation, compulsory treatment or vaccination, and seizure and destruction of property might be required.
Because state and federal governments must have effective and efficient procedures through which to exercise the public health and emergency powers they possess, there is also an implementation challenge.3 The state of Colorado had the legal authority to quarantine populations in Denver during the 2000 exercise there, but was unable to implement the quarantine effectively which undermined the substantive power to implement quarantine as a public health measure.8 Implementation not only touches on formal legal rules, but also on larger social values and norms such as fairness and equity. This will influence how public officials ration scarce resources such as antibiotics.
Considerable legal analysis needs to be done in connection with preparation for bioterrorist attacks. Diligent and creative work in this area will help ensure the rule of law does not become one of the casualties of the use of bioweapons.3
HISTORICAL PERSPECTIVESanitation laws are the oldest public health measures.13 The English statutory and common law recognized the right of the state to quarantine and limit the movement of plague carriers. The American colonies adopted the English laws on the control of diseases. The Constitution, when written, left public health power to the states because it was considered fundamental to the state’s police power.
Acknowledging the public’s justified fear of infectious disease, courts have given broad powers to public health officers.13 Questioning of the value of public health restrictions by a substantial segment of the population has only recently be-come more common. This diminishing support for public health restrictions is rooted more in a loss of fear of com-municable diseases than an increased sensitivity to individual
DIALOGUE AND DISCUSSION

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 199
liberties. The only successful attacks on the exercise of state police power to protect citizens from communicable disease have been based on federal preemption of state laws that restricted interstate commerce. If a state law or regulation is substantially related to health and safety, the Supreme Court will uphold it.13 Laws enacted to protect society, including vaccinations and quarantines, have been upheld even when individuals have been forced to sacrifice individual liberty and privacy. Public health jurisprudence is deeply rooted in the fear of pestilential diseases.
SOCIAL AND WORKPLACE ISSUESUninsured Americans are the most vulnerable in the event of a bioterrorist attack.4 Many Americans lack access to health-care in this country. Individuals who live in inner cities often lack access to healthcare, even when they have full insurance coverage. A bioterrorist attack will further exacerbate the dif-ficulties of the uninsured in obtaining any type of healthcare services. The level of casualties among the members of this group and the public at large could be considerable. For example, many substance abusers, minorities, and residents of rural communities have local public health systems lacking mechanisms to serve them in such an emergency.4
Claims of death and illness caused by the 2001 anthrax-laced letters received or opened in the workplace were covered by workers’ compensation policies.2 War exclusion that applies to many policies do not apply to workers’ compensation poli-cies. The September 11, 2001 attacks as well as the anthrax letters have had an economic impact on Americans. Accord-ing to an assistant vice president of workers’ compensation at the National Association of Independent Insurers, workers’ compensation rates, set by each state, were predicted to rise as a result of the attacks. Losses from bioterrorism have not previously been contemplated by insurers and the projected costs associated with such losses likely will be factored into future insurance rates.2
Employers are now trying to plan responses to bioterrorist and terrorist attacks such as car bombs, anthrax-tainted mail, and planes crashing into buildings. The general duty clause of the Occupations Safety and Health Act (OSHA) requires employers to provide a workplace free from recognized hazards that cause or are likely to cause death or injury. The definition of a recognized hazard is now in question. Employ-ers are well advised to put sensible mail handling procedures in place to let employees know prudent steps are being taken to protect them from tainted mail.
Employers must now also be concerned with forced business shutdowns as a result of bioterrorism or chemical attacks, the threat of such an attack, or even hoaxes. Business inter-ruption insurance (BIC) would possibly cover some such shutdowns. BIC covers lost business income, net profit or loss before income taxes, and, if incurred, continuing normal operating expenses including payroll. If a hospital is closed due to physical damage of the building caused by fire, its loss of income is covered.
A number of insurance companies denied BIC coverage for the events of September 11 on the grounds that the poli-cyholders did not suffer a total “suspension” of all of their operations and thus BIC was not triggered.14 Usually BIC language in most policy forms is so vague that it ensures if a claim is large enough, there will be a dispute. Some property insurance companies argued that business interruption re-covery was diminished by the wider economic effects of the September 11 attacks. The insurance industry in the wake of September 11 successfully contested BIC claims where the policyholder sought to increase the amount of lost income by including consideration of the widespread effect of the physical loss or damage. This type of coverage, however, can be voided if the policyholder does not give timely notice of its losses. An immediate review of coverages and time limits will be critical to any facility or organization seeking BIC damages in the wake of future bioterrorist attacks
If a trace of anthrax or another potential bioweapon is found in a healthcare facility and the facility has to shut down its operations at the affected site and move patients to other locations, its loss of income and extra expenses will probably be covered.2 Biological agents would cause physical damage to a facility because they must be cleaned and removed from the site and would trigger the physical damage obligation.
BIC usually has a clause that covers losses caused by action of civil authority that prohibits access to the business or as a result of civil authority orders from other locations. If, how-ever, a business shuts down as a precaution and not under civil authority orders, it is probably not covered. Facilities (including healthcare facilities) need to look at BIC policies and be aware of the coverage limitations.
PUBLIC HEALTH LAWWhat is the government’s duty to protect the public health in response to a bioterrorism event? State governments tradi-tionally have police powers to protect the health, safety, and general welfare of the public and such duty may be viewed as
DIALOGUE AND DISCUSSION

200 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
comprehensive and extensive.15 State public health authorities could take almost any action to protect the population from a threat. Authorities may have to temporarily constrain certain civil liberties, require private sector participation in public health objectives, shut down potentially harmful industries, destroy contaminated property, deport or prevent the entry of individuals who may infect others, ration supplies, and control the flow of information.15
Can authorities temporarily ignore constitutional principles that respect individual liberties, such as the right to due pro-cess, travel, or assembly? Can federal health officials who lack broad police powers command state public health officials to participate in a federal, national response to a bioterrorist event if limited to one state?
Proposed Model State Emergency Health Powers ActThis act was written as a response to concerns about bioter-rorism raised by the events of September 11, 2001. It is based on the assumption that existing state laws are wholly inadequate to confront a bioterrorism event and should be superseded by a comprehensive act that will override existing laws from different states.15 Even before September 11, the federal government wanted states to update public health laws, some of which date to the 19th century.16
The proposed Model State Emergency Health Powers Act would give public health authorities the ability to exercise enhanced powers to protect individuals and manage property upon the declaration of a public health emergency by the state governor.16,17 A large-scale bioterrorism event will ac-centuate existing uncertainties in the distribution of public health powers. The critical choice for public health authori-ties is not to decide where the power to protect public health lies or which level of government has the primary power to act, but rather from where the leadership to respond to a bioterrorism event will be derived. Public health authorities must also choose how to coordinate with law enforcement and national security authorities. Every bioterrorist attack involves a criminal investigation that is outside the purview of public health authorities.
The act and the December 2001 revision would give state authorities the right to mandate medical testing of its citizens, to isolate people deemed a threat to the public health, and to order private physicians and other healthcare professionals to assist public health officials.16 In a bioterrorism emergency, states could “require a healthcare facility to provide services or use of its facility if such services or use are reasonable and
necessary to respond to the public health emergency with the right to take immediate possession thereof”.18 Officials could also take over other property and “communication devices” believed necessary to stop a biological attack from killing huge numbers of people. The law would be triggered by the governor during a bioweapons event or an epidemic that posed substantial risk of significant casualties. It would provide authorities broad powers to close buildings, take over hospitals, and order quarantines during an attack. The act would also shield health officers from legal liability, along with anyone working under their direction.19
In almost any widespread and rapidly developing bioterrorist event, available public health resources will be quickly taxed. Scarce resources could include healthcare personnel such as laboratory professionals.15 The Model Act would allow state executive authorities to confiscate hoarded supplies, take pos-session of facilities or other property for public health purposes, and to seek the assistance of medical (including laboratory professionals) personnel during a public health emergency.
The September 11 attacks have seemed to create a new world order that appears out of order. Congress has grappled with bioterrorism. The Air Transportation Safety and System Sta-bilization Act limited the liability of airlines involved in the September 11 attacks and created a special fund for victims. The Bioterrorism Preparedness Act of 2001 strengthened the development of new countermeasures against bioterrorism and protection of existing ones. One of its primary goals was to facilitate the production of vaccines. The bill offered some legal protection to manufacturers of vaccines specifically developed as a priority countermeasure to treat or prevent infections by a biological pathogen and administered for such use by order or recommendation of the Secretary of Health and Human Services to respond to the use or threatened use of a biological agent.19
THE LABORATORYBioterrorist events may first be identified by local medical in-stitutions. The local laboratory will play an important part in providing rapid identification of the agent used influencing the administration of antidote or vaccine to affected victims.20 Lack of familiarization with the four levels of biosafety of the Centers for Disease Control and Prevention (CDC) criteria (see Table 1) represent potent barriers to the laboratory in responding to a bio-terrorist attack. It will be important for laboratories to coordinate all activities with the local and state health departments and the FBI. A chain-of-custody (COC) document should accompany a specimen from collection during these events.
DIALOGUE AND DISCUSSION

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 201
Laboratory personnel, as first respond-ers, should be familiar with the steps to take to assist in the diagnosis of each disease. The CDC Laboratory Re-sponse Network provides an organized system for the detection and diagnosis of biological agents based on labora-tory capacity and the degree of risk. Knowledge of the current biosafety lev-els within the laboratory; development and availability of protocols related to COC; collection, preservation, and shipment of specimens and cultures and detection and identification of targeted agents; location of the near-est higher-level reference laboratory; knowledge of current guidelines to ensure safe handling and shipment of biological agents; and knowledge of basic characteristics of current targeted agents will be important.
Authorities could require the assistance of laboratory personnel during a medical emergency as well as the sequestering of any laboratory supplies needed to ad-dress the situation. Personnel could be quarantined, if appropriate, or required to assist with testing or other tasks as mandated by authorities. In addition, the Healthcare Personnel Delivery Sys-tem, a standby plan developed for the Selective Service System at the request of Congress, could be used to draft healthcare personnel if it is implemented in connection with a national mobiliza-tion in an emergency, if Congress and the president approve the plan and pass and sign legislation to enact it.22
Threat and uncertaintyHow will the ongoing threat of terror-ism affect living in the US? Long-term consequences of trauma on people have been witnessed and studied.23 Kosovar families have been interviewed against the background of past and present terror to find out about cop-ing, historically and in the present. The
DIALOGUE AND DISCUSSION
Table 1. Biosafety levels for infectious agents21
Biosafety level (BSL) 1 Agents: Not known to consistently cause disease in healthy adultsPractices: Standard microbiological practicesSafety equipment (primary barriers): None requiredFacilities (secondary barriers): Open bench top, sink required
BSL 2Agents: Associated with human disease; ingestion, percutaneous injury,
mucous membrane exposure hazardPractices: BSL 1 practice PLUS limited access; biohazard warning signs;
“Sharps” precautions; biosafety manual defining any needed waste decontamination or medical surveillance policies
Safety equipment (primary barriers): Primary barriers = Class I or II Biosafety cabinets (BSC) or other physical containment devices used for all manipulations of agents that cause splashes or aerosols of in-fections materials; personal protective equipment (PPE): laboratory coats, gloves, face protection if needed
Facilities (secondary barriers): BSL 1 PLUS autoclave available
BSL 3Agents: Indigenous or exotic agents with potential for aerosol transmis-
sion; disease may have serious or lethal consequences Practices: BSL 2 practice PLUS controlled access; decontamination of
all waste; decontamination of laboratory clothing before laundering; baseline serum
Safety equipment (primary barriers): Primary barriers = Class I or II BSCs or other physical containment devices used for all open manipulations of agents; PPE: protective laboratory clothing, gloves, respiratory protection as needed
Facilities (secondary barriers): BSL 2 PLUS physical separation from access corridors; self-closing, double door access; exhausted air not re-circulated; negative airflow into laboratory
BSL 4Agents: Dangerous/exotic agents which pose high risk of life-threatening
disease, aerosol-transmitted laboratory infections, or related agents with unknown risk of transmission
Practices: BSL 3 practices PLUS clothing change before entering; shower on exit; all material decontaminated on exit from facility
Safety equipment (primary barriers): Primary barriers = all procedures conducted in Class III BSCs or Class I or II BSCs in combination with full-body, air-supplied personnel suit
Facilities (secondary barriers): BSL 3 PLUS separate building or isolated zone; dedicated supply and exhaust, vacuum, and decon systems; other requirements as indicated

202 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
process of family recovery has been witnessed for two years. Women stepped into leadership roles for murdered husbands and families reorganized roles to care for fatherless children. Family members were asked about lessons learned over the generations of living with uncertainty and the ongoing threat of violence. Professional individuals in Kosova have found that Kosovars have survived not by attempting a national defense, but by banding together as clans of extended fam-ily. In Kosova, a person is not an individual, but a family member. Each decision is made to support the survival of the family. What message does the Kosova experience have for Americans? America has been spared the worst of the world’s violent conflicts; when Americans fought wars, the fighting took place on foreign soil. The post-September 11 attacks and the threat of future attacks extend to an indefinite future. The lessons to be gleaned from the Kosova experience are:
• children are the American hope;• energy and attention must be focused on the work before
us and on the future; and• pain must be felt for each other.
Threat and uncertainty will remain a part of the US future and future generations will live differently because of it.
SUMMARYBioterrorism is multi-faceted. Its impact will extend beyond the victims, the agent used, and the perpetrator(s). The rule of law must be considered in the wake of September 11 and the fall 2001 anthrax attacks. Bioterrorism preparedness should address rule of law and social issues. Laboratory profession-als must be prepared for professional, civil justice, and social impact in the event of a future major bioweapons event.
REFERENCES: 1. Morse SA. Bioterrorism: laboratory security. Lab Med 2001;6:303-6. 2. Zall M. Held hostage by fear. (Risk in focus). Risk and Insurance
2002 Jan. 3. Fidler DP. The malevolent use of microbes and the rule of law: legal
challenges presented by bioterrorism. Clin Infect Dis 2001;33:686-9. 4. US commission on civil rights: US public health system unprepared
for bioterrorism attack, 40 million uninsured face greatest risk. PR Newswire 2002 Mar 14.
5. Fred Korematusu v. United States. 323 US 214, 65 S.Ct. 193, 89 L. Ed. 194. Argued 1944 Oct 11; Decided 1944 Dec 18.
6. Baker B, Babington C. Bush addresses uproar over spying. Washing-
DIALOGUE AND DISCUSSION
ton Post 2005 Dec 20; A01. Available from: http://www.washing-tonpost.com/wp-dyn/content/article/2005/12/19/AR2005121911.htm. Accessed 2006 Jun 30.
7. Bush calls disclosure of anti-terror bank records program ‘disgrace-ful.’ 2006 Jun 26. Available from http://www.foxnews.com/sto-ry/0,2933,200985,00.html. Accessed 2006 Jul 5.
8. Henderson DA, Grossman R, O’Toole T. A plague on your city: observations from TOPOFF. Clin Infect Dis 2001;32:436-45.
9. Hurricane Katrina: lessons learned – chapter two: national prepared-ness – a primer. Available from http://www.whitehouse.gov/reports/katrina-lessons-learned/chapter2.html Accessed 2006 Jun 30.
10. Emergency management. Wikipedia. Available from http://en.wikipedia.org/wiki/Emergency_management. Accessed 2006 Jun 30.
11. Hurricane Katrina: lessons learned – chapter five: lessons learned. Available from http://www.whitehouse.gov/reports/katrina-lessons-learned/chapter5.html. Accessed 2006 Jun 30.
12. Gostin LO, Burris S, Lazzarini Z. The law and the public’s health: a study of infectious disease law in the United States. Colum L Rev. 1999;99:59-128.
13. Richards EP. The jurisprudence of prevention: the right of societal self-defense against dangerous persons, 16 Hast Const L Q 320. 1989. Available from http://biotech.law.lsu.edu/cphl/articles/hast-ings/hastings-Contents.htm. Accessed 2002 Dec 17.
14. Lewis RP, Farrell JM. Disaster and business interruption coverages in the aftermath of Katrina. White paper. Available from http://www.andersonkill.com/pdfs/katrina_busint.pdf. Accessed 2006 Jun 30.
15. Hodge Jr. JG. Bioterrorism law and policy: critical choices in public health. J Law Med & Eth 2002;30:2.
16. Orr D. (CP-list) CDC releases draft of public health law. 2001;20:46:50-0700.
17. Model State Emergency Health Powers Act: as of December 21, 2001, (section) 1-104 (m). Centers for Disease Control and Prevention; 2001. Available from www.publichealthlaw.net/MSEHPA/MSE-PHA2.pdf. Accessed 2002 Oct 1.
18. Model State Emergency Health Powers Act: as of December 21, 2001. Centers for Disease Control and Prevention; 2001. Available from www.publichealthlaw.net/MSEHPA/MSEPHA2.pdf. Accessed 2002 Oct 1.
19. Loiacono K. Bioterrorism brings vaccine issue to congress. Trial. 2001;37:13:11.
20. Jortani SA, Snyder JW, Valdes Jr. R. The role of the clinical labo-ratory in managing chemical or biological terrorism.Clin Chem 2000;46:1883-93.
21. Biosafety in Microbiological and Biomedical Laboratories (BMBL). 4th Ed. Washington: Centers for Disease Control and Prevention and National Institutes of Health; 1999 May. Available from http://bmbl.od.nih.gov/.
22. Medical draft in standby mode. Arlington: Selective Service System, Office of Public and Intergovernmental Affairs; 2004. Available from http://www.sss.gov/FactSheets/FSmedical.pdf. Accessed 2002 Oct 1.
23. Griffith JL. “Living with threat and uncertainty: what the Kosavars tell us.Family Process 2002;41: 24-7.

OBJECTIVE: The objective of this study was to determine the percent of the donor population in a South Texas community positive for the red cell antigen Diegoa (Dia) and to determine the percent of anti-Dia in previously transfused patients.
DESIGN: Donor segments from 270 type A and type O do-nors were typed with anti-Dia and 305 previously transfused patients were screened for anti-Dia
SETTING: The study was conducted using donor segments from units collected by the South Texas Blood Center and blood samples from patients in three hospitals in Corpus Christi TX.
PATIENTS OR OTHER PARTICIPANTS: The typing serum was from a type A donor, so only A and O donors were used for the antigen typing. The sera used for the antibody screens were from patients with previous transfusions in the local hospitals. Duplicate samples were eliminated.
RESULTS: Of the 270 type A and O donors, seven (2.6%) were found to be Dia positive and four (1.3%) of the 305 previously transfused patients had anti-Dia.
CONCLUSIONS: In 1985, red blood cell antigen typing of Mexican American blood donors in the Corpus Christi area revealed a Dia antigen frequency of 14.7% with eight percent in Mexican American blood donors from two other areas of Texas. With an Hispanic population of 50.4%, it was expected that four percent to seven percent of the donor pop-ulation would be positive for the antigen. The finding of only 2.6% Dia positive donors demonstrates about a 20% Mexican American donor population. Anti-Dia was found in 1.3%
of the plasma samples from previously transfused patients. These results would indicate a 0.03% to 0.05% transfusion incompatibility in patients with a negative antibody screen for the Corpus Christi area. Areas of the United States with a higher percent Mexican American donor population would expect a higher percent incompatibility. Since the Mexican American population is increasing in South Texas and several other areas in the United States, the antibody may become increasingly important in transfusion therapy and as a cause of hemolytic disease of the newborn.
ABBREVIATIONS: Di = Diego; RPM = revolutions per minute.
INDEX TERMS: antibodies; antigens; blood group; genetics; immunology; isoantigens.
Clin Lab Sci 2006;19(4):203
Christina Thompson is of Texas A&M University-Corpus Christi, Corpus Christi TX.
Address for correspondence: Christina Thompson EdD CLS(NCA), Texas A&M University-Corpus Christi, 6800 Ocean Drive, Corpus Christi TX 78412. (361) 825-2473, (361) 825-3719 (fax). [email protected].
The Diego (Di) blood group system was established in 1967 after the discovery of anti-Dib. Anti-Dia was previously de-scribed as the cause of hemolytic disease of the newborn from the serum of a Venezuelan female in 1956.1 Often referred to as the “Mongolian antigen”, the Dia antigen is present in eight percent of Asian populations with Mongolian ancestry. The antigen has also been found in 20% to 40% of Mexican Indians.2,3 In the United States, Dib is a high frequency antigen found in 99.9% of the population and Dia is a low frequency antigen rarely found in the Caucasian and Black population. However, an increased incidence of the antigen is found in the Native American and Mexican American population.1 In 1985, Edwards-Moulds and Alperin4 typed 1685 Mexican American blood donors from three South Texas communities for Dia. They found an antigen frequency of 14.7% in Corpus Christi, 8.2% in Galveston, and 8.9% in McAllen.
203 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
CLINICAL PRACTICE
Diegoa Antigen Frequency andAnti-Diegoa Frequency in a South Texas Community
CHRISTINA THOMPSON
The peer-reviewed Clinical Practice Section seeks to publish case stud-ies, reports, and articles that are immediately useful, are of a practical nature, or contain information that could lead to improvement in the quality of the clinical laboratory’s contribution to patient care, includ-ing brief reviews of books, computer programs, audiovisual materials, or other materials of interest to readers. Direct all inquiries to Berna-dette Rodak MS CLS(NCA), Clin Lab Sci Clinical Practice Editor, Clinical Laboratory Science Program, Indiana University, Clarian Pathology Laboratory, 350 West 11th Street, 6002F, Indianapolis IN 46202. [email protected]

204 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
Since commercial antibody screening cells do not contain the Dia antigen, the purpose of this study was to deter-mine the need for adding a Dia positive cell to the routine antibody screen. Patient exposure to Dia antigen in the Corpus Christi area was assessed by the determination of the percent of the normal donor population positive for Dia. In addition, the incidence of anti-Dia in previously transfused patients was determined.
MATERIALS AND METHODSDonor segments from 270 type A and O donors were ob-tained and tested for Dia using anti-Dia supplied by Immucor. The typing serum was from a group A donor and contained anti-B, therefore, B and AB donors were not used for the screening. An 0.8% cell suspension from each donor was tested using the Micro Typing Systems gel cards by Ortho-Clinical Diagnostics. IgG gel cards were labeled with donor numbers then 50 microliters of 0.8% suspension of donor cells and 25 microliters of anti-Dia was added to each well. Dia positive and Dia negative cells were used as controls.
Plasma samples from 307 previously transfused patients were collected for antibody testing. The samples were centrifuged at 6000 revolutions per minute (RPM) for three minutes and the plasma was separated into a labeled tube and refrigerated at 2oC – 6oC until testing was performed. All samples were screened for unexpected antibodies using a commercial three cell screen. The detected antibodies were identified.
Two different Dia positive cells provided by Immucor were washed with normal saline and then diluted with saline to a 0.8% cell suspension. The Micro Typing Systems gel cards were labeled with identification numbers for each plasma sample. Fifty microliters of each Dia positive red cell sus-pensions were added to wells in the gel cards. Twenty-five microliters of each antibody negative plasma sample was added to the two cells. All gel cards were incubated at 37oC for fifteen minutes then centrifuged at 895 RPM to 905 RPM for ten minutes using the Micro Typing Systems Centrifuge. The cards were graded on a scale of 0, 1+, 2+, 3+, 4+ and MF according to the descriptions provided by the system.
The protocol was reviewed and approved by the Institutional Review Board at Texas A&M University-Corpus Christi.
RESULTSOf the 270 type A and O donors, seven (2.6%) were found to be Dia antigen positive. Using the routine three cell screen,
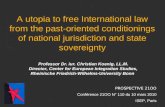
a total of 18 unexpected antibodies were found in 12 (3.9%) of the plasma samples. When the plasma samples were tested with the two Dia positive cells, an additional four samples (1.3%) were found with anti-Dia. Anti-Dia was the second most common antibody found in previously transfused patients after anti-K (Table 1).
DISCUSSIONSeveral reports in the literature describe hemolytic disease of the newborn and hemolytic transfusion reactions associ-ated with Diego antibodies.5-8 Although the Dia antigen is usually associated with Mongolian populations in Japan and China, the antigen is also found in eight percent to 40% of the populations with Native American ancestry.1-3
In the 2000 US Census, the Corpus Christi Hispanic popula-tion was 54.3% with most identified as Mexican American. Since 14% of the Corpus Christi Mexican American do-nors and eight percent of Mexican American donors from two other cities in southeast Texas tested in 1985 were Dia positive,4 the expected Dia antigen positive donors would be four percent to seven percent. The current study found 2.6% Dia positive donors, reflecting a Mexican American donor population of approximately 20%. When previously transfused patients were tested for the presence of anti-Dia, 1.3% of the patients with negative antibody screens were found positive with both Dia cells.
The transfusion services in the Corpus Christi routinely perform type and screen on patients for selected surgical procedures and only perform immediate spin crossmatches for antibody negative patients receiving transfusion. Only
Table 1. Unexpected antibodies found in 305 donors
Antibodies found Number Percent
Anti-K 6 1.9Anti-Dia 4 1.3Cold auto anti-I 3 0.9Anti-E 3 0.9Anti-c 2 0.6Anti-Lea 1 0.3Anti-M 1 0.3Anti-C 1 0.3Anti-e 1 0.3
VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 204
CLINICAL PRACTICE

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 205
patients with positive antibody screens are crossmatched us-ing an antiglobulin procedure with antigen negative blood. The commercial screen cells used for the type and screen are Dia negative. With a 2.6% to four percent Dia positive donor population and a 1.3% antibody incidence, a 0.03% to 0.05% incompatibility would be expected in patients with a negative antibody screen. Areas of the United States with a higher percent Mexican American donor population would expect a higher percent incompatibility.
The results of this study demonstrate a relatively high frequency of anti-Dia in previously transfused patients from an area with 20% to 54% Mexican donors. Since the Mexican American population is increasing in South Texas and several other areas in the United States, the antibody may become increasingly important. For those communities with Mexican American donors, it is recommended that antibody screens routinely include a Dia positive cell to prevent complications in transfu-sion therapy and hemolytic disease of the newborn.
ACKNOWLEDGEMENTSThe author thanks Immucor for providing the typing sera and Diegoa cells, the Coastal Bend Blood Center for provid-ing donor segments, Christus Spohn Shoreline and Corpus
Christi Medical Center for providing patient samples, Chris-tus Spohn Shoreline for providing Micro Typing Systems gel cards, and Nellie Neal, Nicole Peters, Tim Dewees, Bettina Martinez, Carla Stanfill, Tolu Adesanya, and Christy Aguilar for technical assistance.
REFERENCES 1. Poole J. The Diego blood group system-an update. Immunohematol
1999;15(4):135-43. 2. Kotmatsu F, Hasegawa K, Yanagisaw Y, and others. Prevalence of
diego blood group Dia antigen in Mongolians; comparison with that in Japanese. Transfus Apheresis Sci 2004;30(2):119-24.
3. Mallen MS, Arias T. Inheritance of Diego blood group in Mexican Indians. Science 1959;130(3368):164-5.
4. Edwards-Moulds JM, Alperin JB. Studies of the Diego blood group among Mexican-Americans. Transfusion 1986; 26(3):234-6.
5. Hundric-Haspl Z, Balen-Marunic S, Tomasic-Susanj E and others. Anti-Diegoa red blood cell alloantibody as a possible cause of anemia in a 3-week old infant. Archives of Medical Research 2003;34(2):149-51.
6. Hinckley ME, Huestis DW: Case report. An immediate hemolytic transfusion reaction apparently caused by anti-Dia. Rev Fr Transfus Imu Hematol 1979; 22(5):581-5.
7. Kusnierz-Alejska G, Bochenek S, Aukowska B. The first example of anti-Dia antibody in Poland. Mater Med Pol 1990;22(1):15-6.
8. Kusnierz-Alejska G, Bochenek S. Haemolytic disease of the newborn due to anti-Dia and incidence of the Dia antigen in Poland. Vox Sang 1992;62:124-6.
CLINICAL PRACTICE

OBJECTIVES: The profession of clinical laboratory science (CLS) is in dire need of increased exposure to young people. By introducing the clinical laboratory sciences to students at a critical point in their science education and by making it relevant to their lives, more choices are made available to them when considering future career options. With this in mind, the CLS faculty at Texas Tech University Health Sciences Center (TTUHSC) redesigned a recruitment pro-gram and developed it into one making use of CLS student knowledge, enthusiasm, and professionalism. CLS students were given the assignment of designing an entire curriculum for a ten day presentation of clinical laboratory science top-ics to middle and secondary school students. Following the presentations, participants in the program were asked to provide feedback regarding CLS student performance and overall opinion of their interest in clinical laboratory science. The objectives of this study were twofold: 1) to determine if educational methodologies could be appropriately applied by CLS students to present CLS disciplines to middle and high school students; and 2) to determine if the student presentation was successful in initiating interest in the CLS profession based on outcome measures.
DESIGN: As a component of the CLS laboratory manage-ment course, CLS students were instructed in education methodologies including objective writing, teaching-unit preparation, and evaluation tool design. In the following semester, these students were divided into groups and as-signed a specific CLS discipline that would then be presented to middle and secondary school students in a two week, 30 hour educational program. This program was offered by the TTUHSC CLS program in cooperation with the Institute for the Development and Enrichment of Advanced Learners
(IDEAL) at Texas Tech University. The curriculum prepared by the CLS students (with faculty supervision) provided the framework for the present study.
SETTING: Didactic instruction of the CLS students regard-ing objective writing, curriculum design, and preparation of evaluations was included as a component of a CLS laboratory management course. The educational program presented by IDEAL in conjunction with the TTUHSC CLS program within the School of Allied Health Sciences occurred in the CLS student laboratories located in Lubbock, Texas.
PARTICIPANTS: TTUHSC senior CLS students in a 2 +2 baccalaureate level CLS program acted as instructors in the educational program which was presented to middle and secondary school students from around the region. CLS program faculty served as supervisors of this program.
MAIN OUTCOME MEASURES: Questionnaires with Likert-scaled responses were used to evaluate outcomes. These questionnaires regarded 1) faculty assessment of CLS student performance relative to instruction in education methods; 2) participant feedback on the effectiveness and competence of the CLS student instructors and overall appeal of the pre-sented subject material; and 3) peer evaluations of attitude, contribution, and effort of the group members.
RESULTS: CLS faculty strongly agreed that the CLS stu-dents demonstrated a high level of competence when writing objectives, planning age-appropriate curriculum and activi-ties, and demonstrating a positive image of the profession. Regarding satisfaction of the IDEAL student participant, questionnaire responses demonstrated a high rate (84% or greater for middle school participants and 85% for high school students). The program design has been so success-ful that it has been implemented for several other programs offered by TTU and IDEAL.
CONCLUSION: The education methods used in presenting the IDEAL program mirror those found in clinical and aca-demic settings and is an effective technique to introduce CLS students to the varied aspects of educational methodology. The presentation by the CLS students also demonstrated that
VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 206
CLINICAL PRACTICE
Introducing Clinical Laboratory Science:CLS Students Help Shape the Future
BARBARA G SAWYER, JOEL HUBBARD, LORI RICE-SPEARMAN
The peer-reviewed Clinical Practice Section seeks to publish case stud-ies, reports, and articles that are immediately useful, are of a practical nature, or contain information that could lead to improvement in the quality of the clinical laboratory’s contribution to patient care, includ-ing brief reviews of books, computer programs, audiovisual materials, or other materials of interest to readers. Direct all inquiries to Berna-dette Rodak MS CLS(NCA), Clin Lab Sci Clinical Practice Editor, Clinical Laboratory Science Program, Indiana University, Clarian Pathology Laboratory, 350 West 11th Street, 6002F, Indianapolis IN 46202. [email protected]

introduction of clinical laboratory science disciplines early in the education of middle and secondary school students leads to an interest in the CLS profession and to the desire to learn more about it.
ABBREVIATIONS: CLS = clinical laboratory science; IDEAL = Institute for the Development and Enrichment of Advanced Learners; SHWYF = Shake Hands With Your Future; TTU = Texas Tech University; TTUHSC = Texas Tech University Health Sciences Center.
INDEX TERMS: clinical laboratory science; education methods; recruitment; teaching techniques.
Clin Lab Sci 2006;19(4):206
Barbara G Sawyer is Professor; Joel Hubbard is Associate Professor; and Lori Rice-Spearman is Associate Professor and Program Director; Texas Tech University Health Sciences Center, Clinical Laboratory Science Program, Lubbock TX.
Address for correspondence: Barbara G Sawyer PhD CLS(NCA) CLSp(MB), Professor, Texas Tech University Health Sciences Center, Clinical Laboratory Science Program, 3601 Fourth Street, STOP 6281, Lubbock TX 79430. (806) 743-3248, (806)743-3249 (fax). [email protected].
This manuscript has not been presented or accepted for presenta-tion at a future meeting.
Introduction of young people to the CLS profession should begin at the age at which a child first understands what medi-cal science involves. Most children comprehend the idea of using blood or other biological fluids to determine health status in the first grade, and further exposure to biological sciences (usually in fifth grade) continues to offer these young people a close look at human biology and physiology. By introducing them to the field of CLS at this stage in their education, these students begin to understand that there is a laboratory profession in which people are actually involved. Further presentation of this idea at a later stage in a child’s scientific education only serves to reiterate their understand-ing of this science.1 It can also serve as a recruitment tool to the profession. At the Summit on the Shortage of Clinical Laboratory Personnel held in 2000-2001, it was determined that there would be a shortfall of 4,000 individuals needed every year to fill positions in the clinical laboratory2, a short-age that begins with decreased enrollment in laboratory science programs at the university level. Because of this very
real deficit in the numbers of clinical laboratory professionals, it is clear that students in middle and secondary schools as well as those enrolled in college need to be made aware, first, of the existence of the clinical laboratory science profession, and secondly of the opportunities available in the field of laboratory science.
Funding to alleviate the shortage of laboratory personnel has been addressed as an amendment (H.R. 1175) to the Public Health Service Act. This bill endeavors to authorize appropriations for student loan forgiveness and for awards of grants or contracts to agencies that show initiative in expanding their CLS programs.3 To address personnel shortage and program expansion issues, we have devised an innovative program that trains our CLS students to act as both recruiters for the profession as well as instructors of the CLS disciplines. This training not only gives CLS students an introduction to the concepts of curriculum development and teaching that they will use later as clinical instructors, but it also gives them the opportunity to serve as ambassadors for a profession that continues to need increased exposure. To accomplish these training objectives, we have included in our CLS curriculum the presentation of education methodologies and have combined these methods with a unique enrichment program offered by the Texas Tech University Institute for the Development and Enrichment of Advanced Learners (IDEAL). This program is designed to introduce science and technology to students in middle and high schools and is titled Shake Hands With Your Future.4
Recruitment is a difficult procedure at best, hampered by cost, lack of focus and ideas, and lack of interest at the ad-ministrative level. It appears that CLS programs that do not actively recruit new students do not survive, and high cost per student in CLS programs around the country coupled with decreasing enrollments have caused administrators to close a number of programs to maintain fiscal responsibility. For a program to survive, it is obvious that “creative solutions”5 must be examined, including presenting all aspects of the clinical laboratory including research practice, veterinary laboratory medicine, the role of salesperson in the field, fo-rensic laboratory practice, educator, pre-pathology medical education, and so on. To meet a recruitment need and to en-hance the teaching effectiveness of future CLS professionals, the CLS faculty at TTUHSC developed a clinical laboratory offering within the TTU IDEAL program. This program is administered by IDEAL, the mission of which is “to pro-vide distinctive and unique academic enrichment programs that promote academic excellence, citizenship/leadership,
VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 207
CLINICAL PRACTICE

208 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
diversity, and an appreciation of the arts”.4 The institute has been involved in the recruitment of academically talented students to Texas Tech University and in the introduction of underprivileged students to a collegiate experience. IDEAL offers a number of programs to these students, including art, aerodynamics, geology, physics, photography, and clinical laboratory science. It became apparent to CLS faculty that this would be the perfect system in which to reach out to young students as well as to involve undergraduate CLS stu-dents in teaching activities that allow them the opportunity of participating in the introduction of young people to the CLS profession.
METHODSDuring the laboratory management course in our curriculum, senior CLS students are introduced to teaching methodolo-gies, including objective writing, curriculum preparation, and outcome measures. They are informed that these procedures will be put into practice over the summer semester when the IDEAL SHWYF program is offered. The seniors are then randomly divided into four groups that each focus on one CLS discipline: hematology, clinical chemistry, bacteriol-ogy, or immunology/immunohematology. For participants in grades nine through 12, one group is devoted to genetics testing instead of immunology/immunohematology. Each group is then responsible for choosing how it will present the assigned discipline, realizing that the presentations must take into account the age of the students who will be attend-ing; CLS faculty serve as supervisors who oversee one group each. Although class time is utilized for project preparation, the CLS students are also encouraged (not required) to meet outside of classroom hours. Student groups are given a budget to which to strictly adhere. Another aspect of their presenta-tion to the SHWYF participants was a thorough review of all safety issues including universal precautions. Although CLS faculty were always available to offer advice or constructive criticism to the students, most groups devised innovative and clever ways to present their assigned disciplines on their own. CLS students were required to furnish the presenta-tion packet to the faculty member in charge of their group; the packet included three to five objectives, the body of the presentation, questions, and references or web sites. This packet was used by the CLS faculty in the evaluation of the performance of the CLS student groups.
Although IDEAL’s programs maintain a limited budget, much of its support derives from grants and donations. Administrative support is provided by TTU and TTUHSC. In regard to the program involving CLS, information-con-
taining fliers are sent to middle and secondary schools across Texas, New Mexico, and Oklahoma. These info-letters are distributed to students in the appropriate grade levels by school administrators. Similar fliers are distributed to in-dividuals who have participated in past IDEAL programs. Elementary or secondary school students who are interested in the programs are required to have the approval of their science teacher based on the student’s science grades. The SHWYF program covers a two week period during which time students are allowed to enroll in two courses. Typically, the CLS course is offered only in the morning, and the pre-sentations last approximately three to four hours each day for ten days. The cost to the enrolled students covers dormitory stay, food, and travel from the dorm to the site of the course. Scholarships and grants are offered based on need.
The number of students enrolled in the CLS component of IDEAL’s SHWYF program is typically 20-25. The grade level of the participants alternates between calendar years: one year sixth through eighth graders participate and the next year it is ninth through twelfth graders. Roughly equivalent numbers of both sexes enroll in the program.
Actual laboratory activities are organized entirely by the CLS seniors with faculty supervision. Many begin their presenta-tions with topic-specific background information using either handouts or PowerPoint. The participants then begin the hands-on aspect of the discipline of the day. These laboratory exercises are presented by the CLS students and observed by the faculty. In this evaluation, the hematology group placed red and purple chewy candies (not to be eaten in the labora-tory, of course) in clean, closed test tubes to represent the ratio between red and white blood cells, then related these colors to those observed through a microscope on actual blood smears. The bacteriology group utilized marshmallows and agar plates to demonstrate disease transmission in a small population. To demonstrate how forensic medicine and toxicology apply to clinical chemistry, a crime scene, including a body and collectible evidence, was set up for the visiting scholars. In some instances, a Barbie doll house was used complete with toy wine glasses, plastic Barbie-size guns, and all the things that might be at the scene of a crime (Ken is dead) to give the students the opportunity to study a crime scene and test what might be evidence. The immunohematology group staged a “disappearing celebrity” show to illustrate the prin-ciples of blood typing for identification purposes. Genetics testing exercises involved restriction enzyme analysis and gel electrophoresis of DNA in a pseudo-parentage testing study. Following the laboratory exercises, a question-and-answer
CLINICAL PRACTICE

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 209
CLINICAL PRACTICE
Figure 1. AHMT 4320 – Laboratory management faculty evaluation of SHWYF presentation
Please return this form with your name on it to the faculty advisor that oversaw your SHWYF session. He/she will fill it out and hand it in to Mr. Le.
Student to evaluate: _____________________________ Total points: ________________
Please use the following scale to evaluate student performance. Circle your choice for each of the following statements.1 = Strongly disagree 2 = Disagree 3 = No opinion 4 = Agree 5 = Strongly agree
1. Planned age appropriate, meaningful activities 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
2. Wrote appropriate, testable objectives for the presentation 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
3. Prepared relevant, understandable hand-out materials 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐ 4. Was prepared and organized for each session 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
5. Demonstrated a positive image and attitude of caring for the project 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
6. Worked well with others in the group 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
7. Attended all sessions at the scheduled times 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
8. Answered SHWYF students’ questions accurately 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
9. Was respectful toward SHWYF students 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
10. Put forth an equal amount of effort as other members of the group 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐

210 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
session ensued and a questionnaire requesting participants’ feedback about the presentation was distributed. Question-naires were collected upon completion.
Outcome measures are based on the results of these question-naires that had been validated and edited to final form by faculty members in the TTUHSC School of Allied Health Sciences. Specific statements were presented followed by a Likert-scaled range of responses that include “strongly agree”, ranked as five, down to “strongly disagree”, ranked as one. One questionnaire involved faculty assessment of the performance of the CLS stu-dent groups (Figure 1). These questionnaires utilized statements with Likert-scaled responses and were collected by the instructor of the laboratory management course and used in assigning a grade to the CLS student presenters. A second questionnaire was designed by CLS students and validated by faculty members for distribution to the SHWYF student participants (Figure 2).
Validating faculty members were made aware that this ques-tionnaire would be distributed to young, varied-age partici-
pants. This questionnaire was distributed to the participating SHWYF students following the laboratory activities and requested their ranked opinion of the presentations and likeli-hood of their continuing interest in CLS. This questionnaire was considered to be the most critical in our assessment and in planning for the next IDEAL presentation. Respondents were asked to remain anonymous. Frequency of responses for each age group and each question was analyzed and converted to a percentage of the total sample.
The final questionnaire was distributed to CLS students and was an evaluation of their peers that worked within their assigned groups. Results of this survey are not reported in this manuscript.
RESULTSOutcome measures are limited to responses on two question-naires: one of CLS student assessment by CLS faculty (Figure 1) and one prepared by CLS students, validated by faculty, and distributed to SHWYF program participants (Figure
CLINICAL PRACTICE
Figure 2. AHMT 4320 – Laboratory management participant evaluation of SHWYF presentation
Please complete the following evaluation of this session of SHWYF. Use the following scale to evaluate the sentences below.
1 = Strongly disagree 2 = Disagree 3 = No opinion 4 = Agree 5 = Strongly agree
1. The instructors were well prepared and organized. 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
2. The instructors were courteous and respectful. 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
3. The activities were fun. 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
4. I learned new things about clinical laboratory science. 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐
5. I am interested in learning more about clinical laboratory science. 1 2 3 4 5 ⏐ ⏐ ⏐ ⏐ ⏐

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 211
2). Because in-person distribution of the questionnaires was performed, response rate was 100%. Each questionnaire was analyzed according to the frequency of responses and then converted to a percentage of the total sample.
Evaluation of CLS student presentations by CLS faculty demonstrated a very strong student performance overall. There would be an occasional student who would not contribute to the group effort or attend all scheduled planning sessions; however, the majority of students were enthusiastic and positive about their task. The entire pro-gram gives the CLS students the opportunity to “show off” their knowledge in their role as representatives of the profession. In addition, a learning experience concerning the preparation of a curriculum, maintenance of a bud-get, and working with peers was achieved based on the high scores the CLS students attained. All of these skills are considered important in the development of a well-rounded laboratory professional.
CLINICAL PRACTICE
Table 1. Percent response (number of total) to evaluation statements of student participants (n = 50) in grades six through eight evaluating clinical chemistry
Statement 1 = Strongly 2 = Disagree 3 = Neutral 4 = Agree 5 = Strongly number disagree agree
1 0 0 0 0 100 (50 of 50) 2 0 0 0 0 100 (50 of 50) 3 0 0 4 (2 of 50) 0 96 (48 of 50) 4 0 0 0 0 100 (50 of 50) 5 0 0 8 (4 of 50) 4 (2 of 50) 88 (44 of 50)
Table 2. Percent response (number of total) to evaluation statements of student participants (n = 50) in grades six through eight evaluating microbiology
Statement 1 = Strongly 2 = Disagree 3 = Neutral 4 = Agree 5 = Strongly number disagree agree
1 0 0 0 8 (4 of 50) 92 (46 of 50) 2 0 0 4 (2 of 50) 8 (4 of 50) 88 (44 of 50) 3 0 0 0 8 (4 of 50) 92 (46 of 50) 4 0 0 4 (2 of 50) 8 (4 of 50) 88 (44 of 50) 5 0 0 12 (6 of 50) 4 (2 of 50) 84 (42 of 50)
Regarding SHWYF program participant questionnaires, evaluation statements are the same for each discipline (hema-tology, clinical chemistry, etc.) and age group. Results of the clinical chemistry and microbiology SHWYF presentations to sixth through eighth graders are indicated in Tables 1 and 2. The majority of student participants expressed positive views of the activities presented and acknowledged the desire to further their knowledge of clinical laboratory science. Similar response rates were obtained from hematology and immunology/immunohematology presentations. Results regarding hematology and genetic testing presentations made to ninth through twelfth graders are indicated in Tables 3 and 4. The participants in this age group also responded in a positive way regarding the laboratory activities as well as their wish to learn more about the profession. Similar results were obtained for the other disciplines. These results are the compilation of two years (1998-2004) of evaluations for each age group. During two years of this time period our CLS program was not involved with SHWYF.

212 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
CLINICAL PRACTICE
Table 3. Percent response (number of total in parentheses) to evaluation statements of student participants (n = 40) in grades nine through twelve evaluating hematology
Statement 1 = Strongly 2 = Disagree 3 = Neutral 4 = Agree 5 = Strongly number disagree agree
1 0 0 0 0 100 (40 of 40) 2 0 0 0 0 100 (40 of 40) 3 0 0 0 5 (2 of 40) 95 (38 of 40) 4 0 0 0 0 100 (40 of 40) 5 0 0 5 (2 of 40) 10 (4 of 40) 85 (34 of 40)
Table 4. Percent response (number of total in parentheses) to evaluation statements of student participants (n = 40) in grades nine through twelve evaluating genetics testing
Statement 1 = Strongly 2 = Disagree 3 = Neutral 4 = Agree 5 = Strongly number disagree agree
1 0 0 0 0 100 (40 of 40) 2 0 0 0 0 100 (40 of 40) 3 0 0 0 5 (2 of 40) 95 (38 of 40) 4 0 0 5 (2 of 40) 0 95 (38 of 40)
Results of this study indicate that the majority of participants are strongly interested in the field of clinical laboratory sci-ence. The present study concerns a sample size of only 50 sixth through eighth grade and 40 ninth through twelfth grade participants; a larger sample might demonstrate dif-ferent responses. Of course, the final outcome measure of the success of the presentations in garnering interest in CLS would be actual enrollment figures in a CLS program of those who participated. This outcome remains to be assessed. However, the positive outcomes reported in this study come from young students who are beginning to form ideas about their future and could be construed as positive indicators of future CLS program enrollment.
CONCLUSIONAlthough there is a great deal of fun and inventiveness in-volved in the SHWYF presentations, there is a serious side to this presentation technique. The future of the CLS pro-fession and CLS university programs is in the hands of CLS professionals, faculty, and students. It is difficult to devise new ways to introduce individuals to the profession, particu-
larly to those who could be exposed early enough to have an effect on their educational choices. Through the SHWYF presentations, young children in the community and, more importantly, students about to enter college are exposed to clinical laboratory medicine and its many facets. Senior CLS students have a wonderful opportunity to be involved in the future of the CLS profession by taking on the role of instructors. By writing objectives, preparing age-appropriate presentations, and assessing outcomes, these seniors are also being prepared for their role in clinical instruction. However, the most compelling part of the CLS student involvement in this program was the observation of their eagerness to present a science that they had become intimately involved with over the course of their first year in the CLS program. They demonstrated their creativity and enthusiasm by sharing their knowledge to those who may be interested in following in their footsteps. Based on the outcome measures used, the participants indicated positive attitudes toward all aspects of the program. This is the kind of spark the CLS profession needs to advance and circumvent future shortfalls because of lack of interest.

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 213
CLINICAL PRACTICE
ACKNOWLEDGEMENTSThe authors acknowledge Ms. Martha Hise, director of the IDEAL program at Texas Tech University, for her administra-tive and personal support and guidance in the administra-tion of the Clinical Laboratory Science portion of the Shake Hands With Your Future program.
REFERENCES 1. Durrance S, Dopp A, O’Connor T, Sigsby L, Strong L, Walker N,
and Paulson J. Reaching out to future generations – introduction at the high school level. AORN Journal 2004;79(5):1001-5.
2. Summit on the shortage of clinical laboratory personnel. ASCLS Today 2001;XV(4):1-9.
3. United States Congress. Medical Laboratory Personnel Shortage Act of 2005, H.R. 1175. Available from http://www.govtrack.us/con-gress/bill.xpd. Accessed 2005 Jun 15.
4. Texas Tech University Institute for the Development and Enrichment of Advanced Learners (IDEAL) mission statement. Available from http://www.dce.ttu.edu/ec2k/. Accessed 2005 Jun 15.
5. M T p ro g r a m s r e s t r u c t u r i n g t o s u r v i v e . L a b Me d 2005;36(7):388,390.

CLINICAL PRACTICE
The Use of B-type Natriuretic Peptide to Diagnose Congestive Heart Failure
JEFFERY R GRAY
The peer-reviewed Clinical Practice Section seeks to publish case stud-ies, reports, and articles that are immediately useful, are of a practical nature, or contain information that could lead to improvement in the quality of the clinical laboratory’s contribution to patient care, includ-ing brief reviews of books, computer programs, audiovisual materials, or other materials of interest to readers. Direct all inquiries to Berna-dette Rodak MS CLS(NCA), Clin Lab Sci Clinical Practice Editor, Clinical Laboratory Science Program, Indiana University, Clarian Pathology Laboratory, 350 West 11th Street, 6002F, Indianapolis IN 46202. [email protected]
This paper explains the background and current use of B-type natriuretic peptide (BNP) assays to differentiate congestive heart failure (CHF) from other causes of dyspnea. With a large and growing elderly population, CHF is being diag-nosed much more often in emergency rooms in the United States. Doctors need a way to quickly distinguish whether a patient with respiratory distress is suffering from cardiac insufficiency or another etiology. BNP is released from the ventricles in response cardiac overload from CHF or some other form of left ventricular systolic dysfunction. Therefore, the detection and measurement of BNP is a fast and accurate method of determining if CHF is the cause of a patient’s breathing difficulties.
ABBREVIATIONS: ANP = atrial natriuretic peptide; BNP = B-type natriuretic peptide; CHF = congestive heart failure; CNP = C-type natriuretic peptide; COPD = chronic obstruc-tive pulmonary disease; ECG = electrocardiography; LVSD = left ventricular systolic dysfunction; POCT = point of care testing; RAAS = renin-angiotensin aldosterone system.
INDEX TERMS: B-type natriuretic peptide; congestive heart failure; dyspnea.
Clin Lab Sci 2006;19(4):214
Jeffery Gray MT(ASCP) is Research Specialist in the De-partment of Pathology at the University of Maryland School of Medicine, Baltimore MD.
Address for correspondence: Jeffery Gray MT(ASCP), Research Specialist, Department of Pathology, University of Maryland School of Medicine, 10 South Pine Street, MSTF 7th floor,
Aug-65, Baltimore MD 21201-1192. (410) 706-7734, (410) 706-4486 (fax). [email protected].
The maturing of the large baby-boomer population is lead-ing to an increase in the number of congestive heart failure (CHF) and left ventricular systolic dysfunction (LVSD) cases throughout the United States. Many of these individuals will not be diagnosed until they arrive at an emergency room seeking treatment for breathing difficulties. Although these patients suffer from respiratory distress caused by cardiac insuf-ficiency, this symptom is common to many other conditions and diseases. Even when CHF is suspected, it is difficult to evaluate and the diagnostic tests are non-specific. Therefore, physicians need a way to quickly distinguish this disease from other causes of dyspnea. Tests used to measure plasma levels of B-type natriuretic peptide (BNP) are becoming the preferred method of identifying CHF in dyspneic patients.1
Normally found in the ventricles of the heart, the BNP precur-sor (proBNP) is cleaved and released into the blood stream when the myocardium is stretched due to cardiac overload. Both the biologically active BNP fragment and the inactive NT-proBNP portion are clinically useful in the detection of LVSD and CHF.2 Tests to detect these markers are primarily used in acute care settings with patients exhibiting symptoms of heart failure.3 Studies show that assays used to quantitatively measure this peptide are quite accurate in differentiating CHF from other dyspneic patients.4 Additionally, BNP assays are faster and much less expensive than echocardiography – the current “gold standard” diagnostic tool for CHF. This means quicker treatment for those in distress due to heart failure while avoiding the expense, risk, and discomfort of additional testing for those who are not experiencing CHF. The results from the rapid implementation of BNP testing can be used to limit additional heart damage to the patient, allow better allocation of emergency room resources, and save heath care dollars used to diagnose this disease.
BACKGROUNDAccording to the 2005 statistics from the American Heart Association (AHA), CHF affects 4.9 million Americans with 550,000 new cases and 264,900 deaths annually. This report also notes that from 1979 to 2002 hospital discharges
VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 214

CLINICAL PRACTICE
for CHF rose from 377,000 to 970,000 – an increase of 157%. Furthermore, the death rate from this disease rose 35.3% from 1992 to 2002 while the overall death rate for the same time period saw only a 7.7% increase.5 Moreover, readmissions for heart failure are very high. Some surveys show that 50% of all CHF patients return to the emergency room within six months; in addition, 16% of those queried returned to the hospital more than once in the same time period.6 Although CHF can strike at any age, the AHA lists it as the leading cause of hospitalization among the elderly.5
This fact is important when you consider that by the year 2010 the growth rate of older Americans is expected to be as much as 3.5 times greater than the general population.7 Moreover, a US Census Bureau report on aging in the twenty-first century shows the number of Americans aged 60 or older growing from 16.5% in 1997 to a projected 24.6% in 2025. The overall costs of this disease were expected to top $27.9 billion in 2005.5
Congestive heart failure occurs when the heart muscle, weak-ened due to injury or disease, can no longer pump effectively. The loss of cardiac inotropy (contractility) results in a lower ventricular stroke volume and ejection fraction by decreasing end-systolic volume. This cardiac insufficiency means less blood is being pumped with every beat of the heart. With less oxygen-rich blood reaching and perfusing the tissues of the body, the patient is left feeling weak and easily fatigued. The kidneys respond to the lowered cardiac output by activating the renin-angiotensin aldosterone system (RAAS) in order to increase fluid volume by retaining sodium. Meanwhile, a compensatory rise in preload (the amount of blood returning to the heart) causes stretching of the myocardium. Also, the increased pressure in the ventricles, as well as direct oxida-tive damage from angiotensin II and aldosterone, causes left ventricular remodeling including myocyte hypertrophy, fibrosis, and necrosis.8 Besides further hindering the ability of the heart to pump blood, this increased fluid volume also allows liquid to accumulate throughout the body leading to edema (swelling). Right ventricular failure results in edema that is especially noticeable in the lower extremities. Left ventricular failure causes fluid to build up in the lungs; thus, leading to pulmonary edema characterized by shortness of breath, the most common symptom of CHF.
Other signs and symptoms of CHF include: chest pain, car-diomegaly, tachycardia, tachypnea, rales, ascites, third heart sounds, hepatojugular reflex (distended jugular veins due to an enlarged liver), increased blood pressure (early stage of CHF), decreased blood pressure (resulting from cardiogenic
shock in advanced CHF), and a decreased level of conscious-ness.9 These signs, however, do not specifically indicate CHF nor differentiate it from other conditions that have dyspnea as their major symptom. To make the diagnosis even more difficult, as many as 50% of CHF patients may present with no symptoms at all.10 Likewise, diagnostic tests such as elec-trocardiography (ECG) and chest radiography are helpful but by no means conclusive. Making the wrong diagnosis about CHF can lead to life-threatening consequences. While echo-cardiography has long been considered the “gold standard” diagnostic tool for CHF, it is not without its drawbacks. It is not a definitive test, but merely gives an indirect measure of left ventricular filling pressures.11 Also, echocardiography requires an expert operator to both perform the test and interpret the results, thus making this a costly procedure that is often not readily available in an acute care setting. The advent of BNP assays, however, has given clinicians a rapid, accurate and easy to use method to either confirm or exclude the diagnosis of CHF.
ACTION OF BNPBNP is produced and released by secretory granules of the heart in response to pressure overload and volume expan-sion.12 It belongs to a family of natriuretic peptides that includes atrial natriuretic peptide (ANP) found in the atria of the heart, C-type natriuretic peptide (CNP) found in en-dothelial cells, and urodilatin found in the tubular cells of the kidney. Natriuretics are a class of neurohormone that allows the heart to take part in vascular fluid balance by increasing sodium (natrium) excretion to control the amount of fluid loss (uresis) from the body. Neurohormonal peptides were initially described by Henry and Pearce in 1956 after they noted uresis following the inflation of a balloon placed in a dog’s atrium.13 In 1981, a similar response was observed when de Bold and others injected atria homogenate into rats.14 BNP, although first identified from the porcine brain in 1988, is found mainly in the ventricles of the heart.15 It is made up of a 17-amino acid residue ring structure consist-ing of a disulfide bridge between two cysteine residues with a 9-residue N-terminal extension and 6-residue C-terminal extension. BNP is cleaved from a 108 amino acid residue precursor called proBNP to yield the active 77 to 108 amino acid C-terminal molecule and the inactive one to 76 amino acid N-terminal proBNP (NT-proBNP) molecule. Recent studies have shown that both BNP and NT-proBNP are equally effective as markers in the diagnosis of CHF.16
BNP, along with atrial natriuretic peptide, works to regulate fluid balance and blood pressure.17 These molecules act to
VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 215

216 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
CLINICAL PRACTICE
counteract the vasoconstrictive, anti-diuretic, and sodium retentive properties of the renin-angiotensin aldosterone system of the kidneys. They do this by inhibiting the secretion of renin and aldosterone as well as increasing the glomerular filtration rate. This leads to vasodilation, diuresis, an increase in sodium excretion, and relaxation of the myocardium. Although the actions of this compensatory apparatus result in a decreased workload for the heart and reduced blood pressure, the event is short lived and eventually overcome by the sympathetic nervous system, RAAS, and endothelin-1.18
The decompensated CHF patient suffers from progressively worse left ventricular systolic dysfunction with a correspond-ing increase in symptoms. The level of BNP found in the blood likewise increases as the disease advances.12
BNP ASSAYSThere are several types of assays and instruments to determine plasma BNP levels. For example, the Access 2 BNP (Biosite Diagnostics, San Diego, CA), ADVIA Centaur BNP (Bayer Diagnostics, Tarrytown, NY), and the AxSYM BNP (Abbott Diagnostics, Abbott Park, IL) are automated instruments that measure the biologically active C-terminal BNP fragment. The automated E170 NT-proBNP (Roche Diagnostics, Indianapolis, IN), on the other hand, measures the inactive N-terminal portion of BNP. Although there are differences in these molecules (such as half-life and renal clearance), both BNP and NT-proBNP are able to effectively assess CHF.19
The Biosite Triage® (Biosite Diagnostics, San Diego, CA) is an example of a point of care testing (POCT) device for BNP that meets the needs of an emergency room setting. It is highly portable, simple to use, and capable of providing results in as little as 15 minutes.20 This test consists of a single-use fluorescence immunoassay “cartridge” and a meter used to read the device. It requires 250 µL of venous whole blood or plasma from an EDTA (purple top) collection tube. The specimen is added to the device using the included pipette and then placed in the meter. According to the manufacturer, the Triage meter has a reportable range of five pg/mL to 5000 pg/mL. BNP results of less than or equal to 100 pg/mL is considered normal (no CHF) while results of greater than 100 pg/mL are indicative of patients with CHF.20 A study of 1586 patients that showed the Triage test has a sensitivity of 90%, a specificity of 76%, and an overall accuracy of 83% in discriminating CHF from other causes of dyspnea with a BNP cutoff level of 100 pg/mL.21 When used to differentiate between CHF and other causes of dyspnea, BNP has an area under the receiver-operator curve (ROC) of 0.91 with a 95% confidence interval of 0.90 to 0.93 (p<0.001).21
Further studies show increasing concentrations of BNP correlate with the New York Heart Association’s classifica-tion system for the progression of CHF.13,20 In this system, Class I patients (with median BNP levels of 95.4 pg/mL) show no signs or symptoms of CHF with normal activity, Class II patients (221.5 pg/mL) display slight symptom of the disease with physical activity, Class III patients (459.1 pg/mL) have marked signs and limitations due to CHF, and Class IV patients (1006.3 pg/mL) are unable to perform any physical activity without distress. Additionally, elevated levels of BNP show a relationship with other physical signs of CHF including raised pulmonary wedge pressure, reduced ventricular systolic and diastolic function, myocardial infarc-tion, and left ventricular hypertrophy.22 In a separate study of 1286 people without CHF, the Triage assay demonstrated negative predictive value of 98% with BNP levels of less than or equal to 100 pg/mL.20
Calibration of the meter is accomplished via a coded chip that corresponds to the reagent lot in use. Low and high liquid controls are run as if they are patients with each new shipment or lot change of the BNP devices. A special quality control device, similar in appearance to the test device, is used at the initial meter setup, prior to daily testing and whenever the integrity of the test results is in question. Furthermore, each device has a set of built-in controls that ensure enough sample was added; that unbound antibodies were washed away; and that the device was correctly inserted to, and read by, the meter. The recovery of BNP is not interfered with by hemoglobin (up to 10,000 mg/dL), lipids (up to 1000 mg/dL), bilirubin (up to 20 mg/dL), all pharmaceuticals tested, and related proteins and peptides. However, grossly hemolyzed specimens should be avoided.20 Samples should be well mixed and at room temperature before testing. If the specimen cannot be tested within four hours of collection then the plasma must be separated and stored at -20 °C until testing can be performed.
CONCLUSIONThe incidence of CHF will continue to increase as the size of the elderly population grows. It is likely, however, that the many other causes of dyspnea will rise as well. With a finite number of emergency room beds and healthcare dollars, the ability to quickly distinguish heart failure from pulmonary etiologies will save money as well as patients. Modern BNP POCT analyzers such as the Biosite Triage assay offer a fast and accurate method to differentiate those patients suffering from cardiac insufficiency from those that are not in heart failure. A BNP level of greater than 100 pg/ml is indicative

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 217
of CHF; and, this level will increase with the severity of the disease. In addition, it appears that increased amounts of BNP may be a predictor of mortality among coronary heart disease patients.23 Conversely, BNP levels of less than or equal to100 pg/ml have a negative predictive value of 98%; therefore, this test can be used to rule out cardiac causes of dyspnea. This means that inappropriate treatment and expensive follow-up testing (e.g., echocardiography) can be avoided. Although BNP alone cannot be used to solely diagnose CHF, it has become the most important marker of heart failure. This assay, along with echocardiography, chest x-rays, and ECG, has removed much of the guess work in the determination of CHF.
REFERENCES 1. Maisel A, Clopton P, Krishnaswamy P, and others. Impact of age, race,
and sex on the ability of B-type natriuretic peptide to aid in the emer-gency diagnosis of heart failure: results from the breathing not properly (BNP) multinational study. Am Heart J 2004;147(6):1078-84.
2. Cowie M and Mendez G. BNP and congestive heart failure. Prog in Cardio Dis 2002;44(4):293-321.
3. American Association for Clinical Chemistry – Lab Tests On-line. 2005 September 2. BNP and NT-proBNP. Available from http://www.labtestsonline.org/understanding/ analytes/ bnp/test.html. Accessed 2006 Feb 23.
4. Mueller C, Scholer A, Laule-Kilian B, and others. Use of B-type natriuretic peptide in the evaluation and management of acute dyspnea. New Eng J Med 2004;350(7):647-54.
5. American Heart Association. 2005 Heart Disease and Stroke Sta-tistics — 2005 Update. Available from http://www.americanheart.org/downloadable/heart/1105390918119HDSStats2005Update.pdf. Accessed 2005 Oct 8.
6. Vinson J, Rich M, Sperry J, and others. Early readmission of elderly patients with heart failure. J Amer Geriatr Soc, 1990;38:1290-1295
7. National Institute on Aging, Bureau of the Census. Aging in the Americas into the XXI Century. 2002 June 18. US Census Bureau. Available from http://www.census.gov/ipc/prod /ageame.pdf. Ac-cessed 2005 Oct 8.
8. Sutter, M and Diercks D. New insights into decompensated heart
failure. Emer Med 2005; 37(6):18-25. 9. Zevitz, M. 2005 July 7. Heart Failure. E –Medicine. Available from
http://www.emedicine. com/med/topic3552.htm. Accessed 2005 Oct 10.
10. Gheorghiade M, Bonow R, Goldman L, and others. Use of beta-blocker therapy for mild-to-moderate chronic heart failure. Amer J Med 2001; 110 (Suppl 7A).
11. Steg P, Joubin L, McCord J, and others. B-type natriuretic peptide and echocardiographic determinations of ejection fraction in the diagnosis of congestive heart patients with acute dyspnea. Chest 2005;128:21-9.
12. Dao Q, Krishnaswamy P, Kazanegra R, and others. Utility of B-type natriuretic peptide in the diagnosis of congestive heart failure in an urgent-care setting. J Amer Coll Cardio 2001;37(2):379-385.
13. Henry JP, Pearce JW. The possible role of cardiac stretch receptors in the induction of changes in urine flow. J Physiol 1956;131:572-94.
14. de Bold AJ, Borenstein HB, Veress AT, and others. A rapid and potent natriuretic response to intravenous injection of atrial myocardial extract in rats. Life Sci 1981;28:89-94.
15. Sudoh T, Kangawa K, Minamino N, and others. A new natriuretic peptide in porcine brain. Nature 1988;332:78-81.
16. Mueller T, Gegenhuber A, Poelz W, and others. Head-to-head comparison of the diagnostic utility of BNP and NT-proBNP in the symptomatic and asymptomatic structural heart disease. Clin Chem Acta 2004;341:41-8.
17. Wilkins MR, Redondo J, and Brown L. The natriuretic-peptide family. Lancet 1997;349:1307-10.
18. Bhalla V, Maisel S. B-type natriuretic peptide in the neurohormonal hierarchy in heart failure. Cardiovasc Rev Rep 2004;25(3):100-4.
19. Young J, Francis G, Maisel A, and others. Testing for B-type natri-uretic peptide in the diagnosis and assessment of heart failure: what are the nuances? Cleveland Clin J Med 2004;71(Suppl.5):S1-S17.
20. Biosite. Triage BNP test (Product Insert): BNP test for rapid quan-tification of B-type natriuretic peptide. Biosite Inc. 1999.
21. Maisel A, Krishnaswamy P, Nowak R, and others. Rapid measure-ment of B-type natriuretic peptide in the emergency diagnosis of heart failure. New Eng J Med 2002;347(3):161-7.
22. Sagnella G. Measurement and significance of circulating natriuretic peptides in cardiovascular disease. Clin Sci 1998;95:519-29.
23. Kragelund C, Gronning B, Kober L, and others. N-Terminal Pro-B-type natriuretic peptide and long-term mortality in stable coronary heart disease. New Eng J Med 2005;352(7):666-75.
CLINICAL PRACTICE

CLINICAL PRACTICE
Factor V Leiden: An Overview
DONNA M SHAW
The peer-reviewed Clinical Practice Section seeks to publish case stud-ies, reports, and articles that are immediately useful, are of a practical nature, or contain information that could lead to improvement in the quality of the clinical laboratory’s contribution to patient care, includ-ing brief reviews of books, computer programs, audiovisual materials, or other materials of interest to readers. Direct all inquiries to Berna-dette Rodak MS CLS(NCA), Clin Lab Sci Clinical Practice Editor, Clinical Laboratory Science Program, Indiana University, Clarian Pathology Laboratory, 350 West 11th Street, 6002F, Indianapolis IN 46202. [email protected]
This paper provides an update and an overview of factor V Leiden, an inherited condition, which predisposes affected in-dividuals to thrombosis. Factor V Leiden occurs due to a single point mutation on chromosome one. Tests for factor V Leiden include screening for activated protein C (APC) resistance, and if positive, testing for the Factor V Leiden mutation.
ABBREVIATIONS: APC = activated protein C; APTT = ac-tivated partial thromboplastin time; DVT = deep vein throm-bosis; INR = international normalized ratio; LMWH = low molecular weight heparin; MI = myocardial infarction; PCR = polymerase chain reaction; PE = pulmonary embolism.
INDEX TERMS: activated protein C resistance; factor V Leiden; thrombosis.
Clin Lab Sci 2006;19(4):218
Donna M Shaw MT(ASCP) is a teaching assistant in the Department of Medical and Research Technology, University of Maryland School of Medicine, Baltimore MD.
Address for correspondence: Donna M Shaw MT(ASCP), 3216 Hooper Road, New Windsor MD 21776. (410) 875-1336, (410) 875-0998 (fax). [email protected].
The human body maintains a delicate balance of procoagu-lant and anticoagulant processes by using a complex system of cofactors and inhibitors. The system uses a feedback mechanism to maintain the equilibrium.1 When this balance is disrupted, there may be an episode of bleeding or a clotting event such as deep vein thrombosis (DVT) or pulmonary embolism (PE). Thrombophilia is used to describe the ten-
dency of some people to form abnormal blood clots.2 The consequences are usually DVTs of the legs, and PE, which can both cause considerable suffering and even death.1 Each year, approximately 201,000 new cases of venous thrombosis are diagnosed in the United States. Of these, 107,000 individu-als develop DVTs and 94,000 develop PE.3 Approximately 60,000 deaths in the United States each year are due to venous thromboembolism.3
Thrombophilia may be due to either an inherited condition or a condition that develops during life. Some examples of causes for development of non-hereditary thrombophilia are cancer, obesity, diabetes, and surgery.2 Hereditary thrombosis, due to genetic mutations, is the cause of about half of the cases.1 Causes for hereditary thrombophilia result from single gene mutations, and include protein C deficiency, protein S deficiency, antithrombin deficiency, prothrombin mutation, and factor V Leiden.4,5,6 Other causes of thrombosis include antiphospholipid syndrome and elevated levels of factor VIII or homocysteine.6 A study done by Bertina and others in 1994 showed that factor V Leiden is found in about 50% of the cases of familial thrombosis.7
It is important to note the difference between factor V defi-ciency and factor V Leiden. Factor V deficiency is an inher-ited disorder in which the clotting factor V is low, resulting in bleeding problems.8 Factor V Leiden is also inherited, with normal factor levels but an abnormal form of factor V, which results in a tendency for thrombosis.8 Factor V Leiden is an autosomal co-dominantly inherited disease, present in approximately three to seven percent of the Caucasian population, making it the most common cause of inherited thrombophilia.7,9 It is most common in Northern European and Middle Eastern populations, while less common in Hispanic, Asian, African, and Native American populations.2 Factor V Leiden is due to a single mutation on chromosome one, where guanine is replaced with adenine, causing the conversion of agrinine 506 of factor V to glutamine.10 This is the position where activated protein C (APC) must bind to the factor V molecule for normal anticoagulant response.10
When there is a vascular injury, thrombin is generated. The thrombin activates platelets, clots fibrinogen, and binds to
VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 218

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 219
CLINICAL PRACTICE
the endothelial membrane protein thrombomodulin. This promotes the conversion of thrombin from a procoagulant to an anticoagulant protease, which activates protein C.1 Protein C is a naturally occurring anticoagulant, and along with its cofactors protein S and antithrombin III, prevents ongoing thrombin production.10 The factor V genetic muta-tion causes the synthesis of a factor V molecule that is not properly activated by APC, due to the binding site being altered from the mutation.7 Factor V must be inactivated to prevent ongoing thrombin production. Since APC cannot properly bind, it leads to continued thrombin generation, and a state of hypercoagulation.10
The risk of thrombosis in individuals with factor V Leiden is increased five- to seven-fold for heterozygous persons, and increased 80-fold for homozygous individuals.11 These patients usually experience their first thrombosis at a much earlier age (31 years versus 44 years) than persons without the mutation.12 A study conducted by Rosendall and others suggested that factor V Leiden individuals who are homozy-gous will experience at least one event of thrombosis during their lifetime.12
Women affected by factor V Leiden have additional risks for thrombosis. Hormone use increases the risk of DVT and PE in women. Healthy women taking oral contraceptives have a three- to four-fold increased risk of DVT or PE.2 Further, women with factor V Leiden who are taking oral contraceptives, have an increased risk of about 35 fold when compared to factor V Leiden women who do not take oral contraceptives.2 Factor V Leiden post-menopausal women using hormone replacements therapy have a 15 fold increased risk of developing an event of thrombosis.2
Djordjevic and others studied the prevalence of factor V Leiden in a group of 45 women with first episode of DVT during pregnancy or puerperium (the period of state of confinement during and just after childbirth).13 The results showed that 44.4% of the women were heterozygous for fac-tor V Leiden, and 2.2 % of the women were homozygous. This study suggests that testing for factor V Leiden is recom-mended in women with a history of DVT during pregnancy and puerperium.13
Another study conducted by Prochazka and others examined whether being a carrier of the factor V Leiden gene was as-sociated with an increased risk of premature separation of the palcenta.14 They studied 135 women with confirmed diag-nosis of abruptio placentae, and compared them to a control
group of 198 pregnant women who completed delivery. The results showed women with abruptio placentae were carriers of factor V Leiden in 15.5 % of the cases, compared to 5.1 % of the control group. Their conclusion was that factor V Leiden is a risk factor for premature placental separation.14
Middendorf and others performed a study on factor V Leiden and its role in patients with myocardial infarction (MI).15 The study included 507 patients with documented MIs. The prevalence of factor V Leiden in patients with MI was 8.7%, compared to the control group’s prevalence of 3.7%. They concluded that their study showed a significant increase in the prevalence of the factor V Leiden mutation, leading them to the conclusion that patients with factor V Leiden mutation have a predisposition for MI.15 Their study also showed factor V Leiden patients had a lower prevalence of hyperlipidemia and hypertension and rate of smoking than the total population of patients with MI. They propose this may show that traditional risk factors for MI may be less important in patients with factor V Leiden mutations.15 Hille (as cited by Middendorf, 2004) observed a nine fold increase in mortality from coronary heart disease in patients under age 45, who were the parents of factor V Leiden children.15
LABORATORY TESTINGIndividuals who have a history of venous thrombosis or a fam-ily history of a high incidence of venous thrombosis should be screened for hereditary causes of thrombophilia.16 Tests ordered should include Factor V Leiden (APC resistance), protein S deficiency, protein C deficiency, antithrombin as-say, Prothrombin G20210A mutation, factor VIII activity, homocysteine level, and Lupus anticoagulant.5,6,17 Studies have shown that up to one-third of families affected with a hereditary form of thrombosis have two genetic defects, one of which is factor V Leiden.5
When testing for factor V Leiden, a screening test is done to determine APC resistance. This test was first described in 1993 by Dahlback and others.18 The activated partial throm-boplastin time (APTT) was measured both in the presence and absence of exogenous APC. The normal response was a prolonged APTT in presence of APC, because of the inactiva-tion of factors Va and VIIIa. Abnormal response was a failure of prolongation of APTT due to a resistance of added APC.18 The limitations of the assay include that it can not be used for patients who are on heparin or warfarin therapy, due to a preexisting prolonged APTT results.16 Other coagulation defects such as a lupus inhibitor, haemostatic changes dur-ing pregnancy, or acute thrombosis could also affect the test

220 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
CLINICAL PRACTICE
result.16 Due to these interferences, the assay has a sensitivity and specificity of 85%-90 % for factor V Leiden.16
A modified or second generation method was developed that shows sensitivity and specificity values for factor V Leiden that are near 100%.16 The modified assay requires that the plasma is first diluted 1:4 with factor V deficient plasma that also contains a heparin neutralizer.16 This step corrects for inac-curacies due to other deficient factors, neutralizes therapeutic concentrations of heparin, and eliminates the effects of some lupus inhibitors.16 The modified assay can be used for patients undergoing warfarin or heparin therapy, and in cases of acute thrombosis, pregnancy, or inflammation.16 Since lupus anti-coagulant may be a potential interferent in the modified assay, patients with lupus anticoagulant should be evaluated for the factor V Leiden mutation by genetic testing.19
Bertina and others (as cited by Major, 2000) reported that the factor V Leiden mutation is present in more than 95% of the individuals studied with APC resistance.20 All patients testing positive for APC resistance should be tested for the factor V Leiden mutation. Polymerase chain reaction is the “gold standard” for testing for the mutation of factor V Leiden.19 However, other DNA-based methods are commercially avail-able, including an invasive signal amplification reaction assay called the Invader assay, by Third Wave Technologies, Inc., Madison, Wisconsin.19 This test uses florescent probes, one for the wild-type, and one for factor V Leiden.18 In several studies conducted, this assay correctly identified 95.8%-100% of the individuals, when compared with PCR.19
Testing of asymptomatic family members for factor V Leiden is controversial. The testing could facilitate counseling on reducing risk factors and informing the patients of symptoms of DVT and PE.2 The detrimental effects of the testing are anxiety, withholding certain treatments, such as oral contra-ceptives, and the possibility of the individual’s being denied insurance or employment.2 Thus, a positive test could cause unwanted consequences, while a negative test could cause a false sense of security and cause family members to ignore other risks. It is recommended that individuals discuss the implications of testing with their physicians.2
There are some additional risk factors that, when in combina-tion with factor V Leiden, increase the risk of thrombosis. These include age, obesity, cancer, immobility, hospitaliza-tion, surgery, trauma, pregnancy, taking oral contraceptives or hormone replacement therapy, chronic medical conditions, and air travel.2 Some risk factors such as genetics and age are
not alterable, but other factors can be controlled by lifestyle modifications or medications.2
TREATMENTTreatment after a first event of thrombosis with a revers-ible risk factor is usually three months of anticoagulant therapy.21 The anticoagulant therapy of choice is usually a course of IV unfractionated heparin or subcutaneous low mo-lecular weight heparin (LMWH), followed by oral warfarin therapy.16 The target international normalized ratio (INR) is 2.5, with a therapeutic range of 2.0 to 3.0.16 After recur-rent events, anticoagulant therapy is usually continued for 12 months or indefinitely.21 If a factor V Leiden individual has never had a clot, no routine treatment is recommended; however, the patient should be counseled about eliminating other risk factors. Temporary treatment may be necessary during high risk periods, such as surgery.2 It is recommended that homozygous and heterozygous patients with another prothrombotic genetic defect take anticoagulant therapy in all risk situations, and lifelong anticoagulant therapy is considered even after a single thrombotic event.11
SUMMARYIn summary, factor V Leiden contributes to a large number of individuals experiencing a state of hypercoagulation, which may lead to DVT, PE, and MI. Factor V Leiden occurs due to a single point mutation on chromosome one, and leads to the synthesis of a factor V molecule that is not properly activated by APC.7,10 Factor V Leiden is an autosomal co-dominantly inherited disease, present in approximately three percent to seven percent of the Caucasian population, mak-ing it the most common cause of inherited thrombophilia.7,9 Women with factor V Leiden who are taking hormones are at a significantly higher risk for developing a thrombotic event. Women with factor V Leiden are at a higher risk for DVT during pregnancy or puerperium, and at a higher risk for abruption placentae.
Testing symptomatic individuals begins with a test for activated protein C resistance, and then if positive, genetic testing is performed. Testing asymptomatic individuals for factor V Leiden is controversial. It is important for individu-als to be aware of their family history, and to report any familial history of thrombosis to their physician, so they can be screened for factor V Leiden if the physician deems it necessary. Positive lifestyle changes, and treatment when deemed necessary, can prevent blood clots in a significant number of these individuals.

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 221
REFERENCES 1. Majerus PW. Human genetics. Bad blood by mutation. Nature
1994;369(6475):14-5. 2. Ornstein DL, Cushman M. Cardiology patient page. Factor V Leiden.
Circulation 2003;107(15):e94-7. 3. National Alliance for Thrombosis and Thrombophilia (2005).Avail-
able from www.nattinfo.org. Accessed 2005 Sep 18. 4. Loscalzo J, Schafer AI, editors. Thrombosis and Hemorrhage. 3rd edi-
tion. Philadelphia: Lippincott Williams & Williams; 2003. p 330. 5. Taylor AK. Venous thrombosis and the factor V (Leiden) mutation.
Genetic Drift [online] 1997; 14. Available from from http://www.mostgene.org/gd/gdvol14b.htm. Accessed 2005 Oct 18.
6. Fritsma GA, Marques, MB. Thrombosis risk testing in the clinical laboratory. Lab Med 2005;32(2):115-8.
7. Bertina RM, Koeleman BP, Koster T, and others. Mutation in blood coagulation factor V associated with resistance to activated protein C. Nature 1994; 369(6475):64-7.
8. Moll, S. (2005) FVL thrombophilia support page. Available from http://www.fvleiden.org/ask/07.html. Accessed 2005 Oct 18.
9. Gardner J. Factor V Leiden with deep venous thrombosis. Clin Lab Sci 2003; 16(1):6-9.
10. Harmening, Denise M. Clinical hematology and fundamentals of hemostasis . 4th edition. Philadelphia: FA Davis; 2003. p 499-500.
11. Nicolaes GA, Dahlback B. Activated protein C resistance (FV Leiden) and thrombosis: factor V mutations causing hypercoagulable states. Hematol Oncol Clin N Am 2003; 17(1):37-61.
12. Rosendaal FR, Koster T, Vanderroucke, JP, and others. High risk of thrombosis in patients homozygous for factor V Leiden (activated protein C resistance). Blood 1995; 85: 1504-8.
13. Djordjevic V, Rakicevic L, Miljic P, and others. Factor V Leiden, FII G20210A, MTHFR C677T mutations and first venous thrombosis during pregnancy and puerperium [abstract]. Pathophysiol Haemost Thromb 2003; 33(suppl2).
14. Prochazka M, Slavik L, Proxhazkova J, and others. Factor V Leiden, prothrombin G20210A and MTHFR C667T mutations in women with abruption placentae [abstract]. Pathophysiol Haemost Thromb 2003; 33(suppl2).
15. Middendorf K, Gohring P, Huehns TY, and others. Prevalence of resistance against activated protein C resulting from factor V Leiden is significantly increased in myocardial infarction: investigation of 507 pa-tients with myocardial infarction. Am Heart J 2004; 147(5):897-904.
16. Kujovich, JL (2004). Factor V Leiden thrombophilia. Available from http://www.geneclinics.org/profiles/factor-v-leiden/details.html. Ac-cessed 2005 Oct 18.
17. Lab tests online (2004). Factor V Leiden and PT 20210. Available from http://www.labtestsonline.org/understanding/analytes/fac-tor_v_and_pt20210/test.html. Accessed 2005 Oct 18.
18. Dahlback B, Carlsson M, Sevensson PJ. Familial thrombophilia due to a previously unrecognized mechanism characterized by poor anticoagulant response to activated protein C: prediction of a cofactor to activated protein C. Proc Natl Acad Sci USA 1993; 90: 1004-8.
19. Van Cott EM, Soderberg BL, Laposata M. Activated protein C resistance, the factor V Leiden mutation, and a laboratory testing algorithm. Arch Path Lab Med 2002; 126(5):577-82.
20. Major DA, Sane DC, Herrington DM. Cardiovascular implications of the factor V Leiden mutation. Am Heart J 2000;140:189-95.
21. Juul K, Tybjaerg-Hansen A, Schnohr P, and others. Factor V Leiden and the risk for venous thrombolism in the adult Danish population. Ann Intern Med 2004;140:330-7.
INSTRUCTIONS TO AUTHORS
Detailed Instructions to Authors can be found on the ASCLS website (http://www.ascls.org) by following the Pub-lications links, or by going directly to http://www.ascls.org/leadership/cls/index.asp. Questions may be addressed to Managing Editor Margaret LeMay-Lewis at the Clinical Laboratory Science editorial office, IC Ink, 858 Saint Anne’s Drive, Iowa City IA 52245. (319) 354-3861, fax (319) 338-1016. [email protected]
CLINICAL PRACTICE

CLINICAL PRACTICE
Two Non-invasive Diagnostic Tools for Invasive Aspergilosis:(1-3)-β-D-Glucan and the Galactomannan Assay
AMY KELAHER
The peer-reviewed Clinical Practice Section seeks to publish case stud-ies, reports, and articles that are immediately useful, are of a practical nature, or contain information that could lead to improvement in the quality of the clinical laboratory’s contribution to patient care, includ-ing brief reviews of books, computer programs, audiovisual materials, or other materials of interest to readers. Direct all inquiries to Berna-dette Rodak MS CLS(NCA), Clin Lab Sci Clinical Practice Editor, Clinical Laboratory Science Program, Indiana University, Clarian Pathology Laboratory, 350 West 11th Street, 6002F, Indianapolis IN 46202. [email protected]
Invasive aspergillosis (IA) is a serious cause of morbidity and mortality among immunocompromised patients. Prompt and non-invasive methods for diagnosing IA are needed to improve the management of this life-threatening infection in patients with hematological disorders. In summary, this retrospective review of studies performed on the two assays finds that both assays have high sensitivity and specificity but are more useful when used together as a diagnostic strategy for patients with invasive aspergillosis.
ABBREVIATIONS: BDG = beta-D-glucan; GM = galacto-mannan; IA = invasive aspergillosis; IFI = invasive fungal infections; ODI= optical density index.
INDEX TERMS: aspergillosis; galactomannan; glucan.
Clin Lab Sci 2006;19(4):222
Amy Kelaher is a graduate student in the Department of Medi-cal Research and Technology, University of Maryland School of Medicine, Baltimore MD.
Address for correspondence: Amy Kelaher, Department of Medical and Research Technology, University of Maryland School of Medicine, 100 Penn Street-AHB Room #435, Bal-timore MD 21201.(301) 496-3049, (410) 706-0073 (fax). [email protected].
Invasive aspergillosis (IA) is one of the most serious causes of morbidity and mortality among immunocompromised patients. Among several factors that contribute to the high mortality rate, difficulties in establishing a reliable diagnosis early enough for successful intervention have been reported.1
The crude mortality rate of IA is very high despite appropriate antifungal treatment, since the difficulty in obtaining an early di-agnosis results in a delay in establishing treatment. The diagnosis of IA is frequently established postmortem. The establishment of a prompt and optimal noninvasive method for diagnosing IA is needed to improve the management of this life-threatening infection in patients with hematological disorders.2,3
Current conventional diagnostic methods such as histological examination and cultures of deep tissues are not only insensi-tive, but require an aggressive approach. This often precludes their use due to profound thrombocytopenia, hypoxemia, and the critical condition of these patients. As a result, many physicians begin empiric or prophylactic amphotericin B therapy before making a definitive diagnosis. Initiation of empiric or prophylactic therapy with amphotericin B may lead to treatment failure of a full systemic infection or risk of nephrotoxicity.4
Over the past decade there have been many advances made to further the options of both diagnostics and therapeutics. Diagnostic options have widened with the addition of di-agnostic imaging, histopathology, and several non-invasive laboratory tests for IA. These tests include a double-sandwich enzyme-linked immunosorbent assay (ELISA) for galacto-mannan (GM) antigen (Platellia Aspergillus), tests for (1→3)-β-D-glucan (BDG) (Glucatell or FungiTec G test), and a number of PCR-based assay systems for Aspergillus DNA.5
The GM and BDG test monitors Aspergillus GM by detecting the polysaccharide cell wall component based on the use of a rat monoclonal antibody (Mab), EB-A2, that recognizes the 1→5-β-galactofuranoside side chains of the GM molecule. GM is a polysaccharide that is attached to and released from Aspergillus hyphae during growth. As little as 0.5 ng to 1.0 ng of circulating GM per ml may be detected with this double-sandwich enzyme-linked immunosorbent assay.6 The excellent sensitivity and specificity of this assay have been repeatedly demonstrated and validated in tests of patients with hematological disorders.7
The assay for (1→3)-β-D-glucan detects (BDG) glucans produced by fungi. BDG is a ubiquitous component of
222 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE

CLINICAL PRACTICE
diverse fungal species. The assay system is currently available for the sensitive detection of circulating BDG, based on the Limulus reaction, crab coagulation cascade through Factor G. The activation events result in clot formation when co-agulogen is cleaved to coagulin by the clotting enzyme. The introduction of a chromogenic peptide substrate permits spectrophotometric quantitation of the activated proclot-ting enzyme.8
RESULTSIn a study performed by Odabasi and others, the (1→3)-β-D-glucan detection kit by Glucatell was examined. The results of this study showed that the Glucatell and the Fungitec-G assays were found to be specific for polysaccharides com-posed of, or containing, BDG sequences. Both assays were non-reactive with two other types of polysaccharides, (1→4)-β-D-glucan and (1→6)-β-D-glucan, as well as non-glu-cans containing (1→3)-β-D-glucan linkages. The determined BDG cutoff for the Glucatell assay was 60 pg/mL and was chosen as the positive cut-off for the diagnosis of invasive fungal infections (IFI). Testing was performed with serial se-rum samples from 283 subjects with acute myeloid leukemia or myelodysplastic syndrome who were receiving antifungal prophylaxis. The absence of a positive BDG finding had a 100% negative predictive value, and the specificity of the test was 90% for a single positive test result and >96% for more than two sequential positive results. This study demonstrated that the Glucatell serum BDG detection assay is highly sensi-tive and specific as a diagnostic for IFI.9
A multi-center clinical evaluation of the (1→3)-β-D-glu-can assay, Glucatell, was described in a study completed by Ostrosky-Zeichner and others as an aid to diagnose fungal infections in humans. In this study, patients at six clinical sites in the United States were enrolled as either fungal infection negative or with proven or probable IFI. Using a cutoff of 60 pg/mL, the sensitivity and specificity of the assay were 69.9% and 87.1%, respectively. The positive and negative predictive values were 83.8% and 75.1%. Additionally, a cutoff value of 80 pg/mL, the sensitivity and specificity were 64.4% and 92.4%, respectively, with a positive and negative predictive value of 89% and 73%. Of the ten patients with aspergil-losis, 80% had positive results at cutoff values of 60 pg/mL and 80 pg/mL. The study concluded that the reproducible assay results with high specificity and high positive predic-tive values in a multi-center setting demonstrate that use of the assay to detect serum BDG levels is a useful diagnostic adjunct for IFI.8
In 2005 Pazos and others completed a study on the contri-bution of (1→3)-β-D-glucan for diagnosis and therapeutic monitoring of IA in neutropenic adults in comparison with serial screening for circulating galactomannan. The two tests (Glucatell, and Platelia Aspergillus) were used retrospectively in a twice-weekly screening for IA in 40 neutropenic adult patients. The cutoff used for GM assay and BDG assay were optical density index (ODI) of 1.0 and 60 pg/mL, respec-tively. Out of 11 cases there were five proven cases of invasive aspergillosis, three probable cases, and three possible cases. In both assays BDG and GM were detected in 100% of patients with proven IA and in 66% of patients with probable IA. The sensitivity, specificity, and the positive and negative predic-tive values for GM and BDG were identical: 87.5%, 89.6%, 70%, and 96.3%, respectively. False/positive reactions did occur at a rate of 10.3% in both tests. Although both tests anticipated clinical diagnosis, initiation of antifungal therapy, and computed tomography abnormalities, BDG showed positive results earlier than GM. This study concluded that joint use of both tests is very useful to identify false-positive reactions by each. Joint use improves each individual test’s specificity and positive predictive value to 100%, without affecting the sensitivity and negative predictive values.10
In a study performed by Kawazu and others, 149 treatment episodes in 96 consecutive patients, including nine proven IA, two probable IA, 13 possible invasive fungal infections (IFI), and 125 no-IA episodes were studied. Overall, 1,233 samples were analyzed using the ELISA for GM detection and 1,243 samples were examined using the BDG test. The GM and BDG levels in a cohort of patients at high risk for IA were measured weekly. The two different tests were ex-amined using receiver-operating characteristic analysis. The area under the receiver-operating characteristic curve was the greatest for ELISA, using two consecutive positive results (0.97; p = 0.055 for ELISA versus BDG). The cutoff for ELISA could be reduced to an optical density index (ODI) of 0.6. With the use of this cutoff for ELISA and the cutoff for BDG, 60 pg/mL, that give a comparable level of specific-ity, the sensitivity, specificity, positive predictive value, and negative predictive value of the ELISA and BDG tests were 1.00/0.93/0.55/1.00 and 0.55/0.93/0.40/0.96, respectively. The conclusion of this study was that the double sandwich ELISA test was the most sensitive at predicting the diagnosis of IA in high-risk patients with hematological disorders, using a reduced cutoff of 0.6 ODI.11
A series of allogeneic stem cell transplant recipients were examined in a paper written by Maertens and others. The
VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 223

224 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
CLINICAL PRACTICE
study analyzed the relationship between antigenemia and other diagnostic triggers for initiation of antifungal therapy. The sensitivity and specificity of GM detection were 94.4%, and 98.8%, respectively. The positive and negative predictive values were also 94.4% and 98.8%. This method of detec-tion, with a cutoff value of 1.0 ODI, was found to be better statistically than other triggers, such as unexplained fever, new pulmonary infiltrates, isolation of Aspergillus species, and computed tomography imaging. The results of the study were that antigenemia preceded diagnosis on the basis of radio-logic examination or Aspergillus isolation by eight and nine days in 80% and 88.8% of patients. Antigenemia detection preceded therapy in 83.3% of patients. The conclusion of the study was that detection of GM allows earlier diagnosis of aspergillosis than conventional diagnostic criteria.12
DISCUSSIONDiagnosis of invasive pulmonary aspergillosis still remains a challenge, mainly because of atypical clinical presentations, coexistence with other infectious and noninfectious diseases, and a relative inability to culture these organisms by standard microbiological techniques. Non-culture based techniques for diagnosing IA have improved steadily in recent years but improvements are still needed.
The development of GM antigen ELISA (Platelia Aspergillus, Bio-Rad Laboratories) tests significantly improved the quality of non-invasive diagnostics. The Bio-Rad GM assay is one such test that may be applied for these purposes; however, reported diagnostic performance has been controversial. Although specificity of the test has been high (i.e., >90%) in most studies performed, reported sensitivities have varied.
The reviewed articles discussed above also demonstrate that the (1→3)-β-D-glucan assay may be useful to measure serum BDG in clinical specimens with a high specificity and posi-tive predictive values for patients with proven or probable IFI. A cutoff value of 60 pg/mL or 80 pg/mL appears to be appropriate for this test. Although the performance of this assay does not appear to be affected by the presence of an-tifungal therapy, it is very sensitive to glucans that naturally reside in the environment.
In summary, this large retrospective review of studies per-formed on both assays has demonstrated that GM and β-glu-can detection assays do have high sensitivity and specificity, but have variable cutoffs that affect the use of these assays as
tools for clinical diagnosis of invasive aspergillosis. Although tissue culture and radiologic examination remain the “gold standard” indicators of invasive disease, the low cost, rapid results, and non-invasive methods of the two assays make them more appealing to physicians and patients. The two assays used in combination may provide physicians and patients with a stronger diagnostic strategy for diagnosing invasive aspergillosis.
REFERENCES: 1. Patterson TF, Kirkpatrick WR, White M, Hiemenz JW, and oth-
ers. Invasive aspergillosis. Disease spectrum, treatment practices, and outcomes. I3 Aspergillus Study Group. Medicine (Baltimore) 2000;79(4):250-60.
2. Latge JP. Aspergillus fumigatus and aspergillosis. Clin Microbiol Rev 1999;12(2):310-50.
3. Singh N. Invasive aspergillosis in organ transplant recipients: new issues in epidemiologic characteristics, diagnosis, and management. Med Mycol 2005;43 Suppl 1:S267-70.
4. Hope WW, Walsh TJ, Denning DW. Laboratory diagnosis of invasive aspergillosis. Lancet Infect Dis 2005;5(10):609-22.
5. Dupont B, Richardson M, Verweij PE, Meis JF. Invasive aspergillosis. Med Mycol 2000;38 Suppl 1:215-24.
6. Stynen D, Goris A, Sarfati J, Latge JP. A new sensitive sandwich en-zyme-linked immunosorbent assay to detect galactofuran in patients with invasive aspergillosis. J Clin Microbiol 1995;33(2):497-500.
7. Bart-Delabesse E, Basile M, Al Jijakli A, Souville D, and others. Detection of Aspergillus galactomannan antigenemia to determine biological and clinical implications of Beta-lactam treatments. J Clin Microbiol 2005;43(10):5214-20.
8. Ostrosky-Zeichner L, Alexander BD, Kett DH, Vazquez J, and others. Multicenter clinical evaluation of the (1→3) beta-D-glucan assay as an aid to diagnosis of fungal infections in humans. Clin Infect Dis 2005;41(5):654-9.
9. Odabasi Z, Mattiuzzi G, Estey E, Kantarjian H, Saeki F, and others. Beta-D-glucan as a diagnostic adjunct for invasive fungal infections: validation, cutoff development, and performance in patients with acute myelogenous leukemia and myelodysplastic syndrome. Clin Infect Dis 2004;39(2):199-205.
10. Pazos C, Ponton J, Del Palacio A. Contribution of (1→3)-beta-D-glucan chromogenic assay to diagnosis and therapeutic monitoring of invasive aspergillosis in neutropenic adult patients: a comparison with serial screening for circulating galactomannan. J Clin Microbiol 2005;43(1):299-305.
11. Kawazu M, Kanda Y, Nannya Y, Aoki K, Kurokawa M, and others. Prospective comparison of the diagnostic potential of real-time PCR, double-sandwich enzyme-linked immunosorbent assay for galacto-mannan, and a (1→3)-beta-D-glucan test in weekly screening for invasive aspergillosis in patients with hematological disorders. J Clin Microbiol 2004;42(6):2733-41.
12. Maertens J, Van Eldere J, Verhaegen J, Verbeken E, Verschakelen J, Boogaerts M. Use of circulating galactomannan screening for early diagnosis of invasive aspergillosis in allogeneic stem cell transplant recipients. J Infect Dis 2002;186(9):1297-306.

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 225
RESEARCH AND REPORTS
Cessation of Menstruation Improves the Correlation of FPG to Hemoglobin A1c in Caucasian Women
KRISTINA JACKSON BEHAN
BACKGROUND: Anemia is known to cause spurious he-moglobin A1c (HbA1c) results. The effect of menstruation on HbA1c was tested by correlating it to FPG in non-anemic premenopausal and in menopausal women.
METHOD: Non-diabetic, non-obese middle-aged Cauca-sian women were classified as premenopausal or menopausal. Hemogram, FPG, and A1c results were obtained.
RESULTS: Hemoglobin concentrations were lower in the premenopausal group. FPG showed a poor correlation to A1c value overall (r = 0.251, p = 0.001) which was improved by multiplying the A1c % by the total hemoglobin concentra-tion to create an absolute A1c value (r = 0.362, p = 0.000). When the data was sorted by menopause status, the correla-tion of FPG to Absolute A1c improved (r = 0.463, p = 0.000) in the menopausal women, but remained low (r = 0.283, p = 0.005) in the premenopausal women.
CONCLUSIONS: Menstruation may be a significant factor affecting the accuracy of A1c concentrations.
ABBREVIATIONS: A1c = hemoglobin A1c; BMI = body mass index; CI = confidence interval, FPG = fasting plasma glucose; HbA1c = hemoglobin A1c; MBG = mean blood glucose; MCV: mean corpuscular volume; NGSP = National Glycohemoglobin Standardization Program; RDW = red blood cell distribution width.
INDEX TERMS: Absolute A1c; A1c; glucose; menopause; menstruation.
Clin Lab Sci 2006;19(4):225
Kristina Jackson Behan is Associate Professor, University of West Florida, Department of Biology, Division of Life and Health Sciences.
Address for correspondence: Kristina Jackson Behan PhD MT(ASCP), Program in Clinical Laboratory Sciences, De-partment of Biology, Division of Life and Health Sciences, University of West Florida, 11000 University of West Florida, Pensacola FL 32514. (850) 474-3060, (850) 474-2749 (fax). [email protected].
In the past 24 years, the prevalence of diagnosed diabetes has increased 59% for American women. In 2004, 7.8% of white females between the ages of 45 and 64 had diagnosed diabe-tes, with an average age at diagnosis of 46.4 years.1 Chronic complications of diabetes include retinopathy, kidney disease, neuropathy, and cardiovascular disease, and can be delayed and diminished by tight glycemic control for both type 1 and type 2 diabetics.2-5 Fasting plasma glucose (FPG) is the preferred screening tool for diabetes mellitus, and a FPG > 126 mg/dL (7.0 mmol/L) that is reproduced on a separate occasion is diagnostic for diabetes.6 Hemoglobin A1c has long been recognized as the best test of long term glycemic status for both type 1 and type 2 diabetics, and elevations in A1c are linked to higher incidence of chronic complications.2-4,7 Glycation is a continuous process, and the long life of red blood cells gives the A1c test a look back capability over the lifetime of those cells.8
Technical problems with A1c measurement that cause a spuri-ous result have been discussed in depth, and encompass the inclusion of labile A1c in the total A1c, the inability to distin-guish glycated hemoglobin from carbamylated hemoglobin, and the positive and negative effects of variant hemoglobins on A1c concentration.8,9 The National Glycohemoglobin Standardization Program was established to certify methods as traceable to the Diabetes Control and Complications Trial Reference Method.10,11
Nathan and colleagues7 determined a linear relationship between mean blood glucose (MBG) and A1c in 21 diabet-ics, showing MBG (mg/dL) = 33.3*HbA1c – 86, r = 0.958.
The peer-reviewed Research and Reports Section seeks to publish reports of original research related to the clinical laboratory or one or more subspecialties, as well as information on important clinical laboratory-related topics such as technological, clinical, and experimental advances and innovations. Literature reviews are also included. Direct all inquiries to David G Fowler PhD CLS(NCA), Clin Lab Sci Research and Reports Editor, Dept of Clinical Laboratory Sciences, University of Mississippi Medical Center, 2500 North State St, Jackson MS 39216. (601) 984-6309, (601) 815-1717 (fax). [email protected]

226 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
RESEARCH AND REPORTS
Recently Rohlfing and colleagues12 examined 1439 patients and refined the relationship to mean plasma glucose MPG (mg/dL) = 35.6*A1c – 77.3, r = 0.82. When they examined fasting glucose alone, the correlation to A1c was lower, r = 0.69. Pathologic conditions can cause discrepant A1c values, invalidating the correlation to plasma glucose. A1c values are lower in hemolytic disease and hemoglobinopathies with decreased red blood cell survival.13 Iron deficiency anemia causes increased A1c values in diabetics14,15 and non-diabet-ics.16 Spuriously low values of A1c were found in diabetic subjects with anemia, and correction of the anemia raised the A1c.17 Subtler differences remain to be discovered. Kilpatrick and coworkers reported an intra-individual vari-ance of six percent for glycated hemoglobin, but an 85% inter-individual variance.18 Rates of glycation differ among individuals, and A1c concentration is also affected by the duration of the diabetic status.19
Menstruation has not been investigated as a significant cause of A1c inaccuracy, even though it is a leading cause of iron deficiency anemia. The average age of menopause in American women is 51, close to the average age of diagnosis for diabetes. Many women experience significant blood loss during perimenopause, a several year span of time prior to menopause. This work looks at middle-aged, non-obese, non-diabetic Caucasian women, distinguishing them as pre-menopausal or menopausal, and compares the hemoglobin values between the groups. It correlates A1c to FPG, and Hemoglobin to FPG in both groups. It introduces a param-eter called “Absolute A1c”, the product of total hemoglobin* A1c and tests its correlation to FPG in both groups.
MATERIALS AND METHODSPopulationTwo hundred women between the ages of 40 and 54 were recruited by newspaper, television, and radio announcement in the Pensacola, Florida area between November 2004 and May 2005. Participants were interviewed to determine their health status, race, age, and menopause status. Some women had a previous hysterectomy and were not aware of their menopause status; these women were grouped with the menopausal women. Participants were weighed and height measured, and BMI was calculated as weight in kg/height in m2. Participants were excluded if they were outside the speci-fied age range, obese (BMI > 30), were known diabetics or had a fasting plasma glucose (FPG) > 126 mg/dL (7.0 mmol/L), or if they took medication to lower their cholesterol. Since race other than Caucasian is a risk for diabetes, and only 7.8% of the enrollees were not Caucasian, these women were
excluded from this analysis. 169 subjects remained. For the correlation with FPG and A1c, women with hemoglobin < 11.0 g/dL or MCV < 80 fL were disqualified (n = 5). All of the subjects were in good health. This study was approved by the Institutional Review Board at the University of West Florida; all subjects provided informed consent.
Laboratory analysisSubjects were instructed to fast between ten and 12 hours, and blood was collected in the morning. Blood for glucose analysis was collected in serum separator tubes, and centrifuged within 60 minutes of collection. Glucose was performed on a Dade RXL using the Hexokinase G-6-PD method. Hemoglobin A1c was collected in EDTA and was performed on a Tosoh A1c 2.2+. This instrument is an ion exchange HPLC method approved by the NGSP, it is not affected by carbamylation or HbAS, it separates labile A1c from stable A1c, and printouts alert the operator when the instrument is unable to identify unusual elution peaks. Hemoglobin concentrations were per-formed by the Cyanmethemoglobin method and MCV and RDW by electrical impedance on a Beckman Coulter HMX. All assays were performed at West Florida Hospital, Pensacola, Florida within one day of collection by a qualified technical staff. The between run imprecision (CV) for glucose, A1c, hemoglobin, MCV and RDW were 1.7%, 2.9%, 0.9%, 0.7%, and 1.2%, respectively. Absolute A1c value was calculated as the A1c %* total hemoglobin in g/L.
Data analysisDescriptive statistical analysis was performed using Microsoft Excel. Student’s t-test of unequal variances was performed for age, FPG, hemoglobin. Student’s t-test of equal variance was performed for A1c, Absolute A1c, and MCV. Confidence intervals are 95%. Correlations and box plots were generated with SPSS v.12. Pearson correlation coefficients (r) represent two tailed significance.
RESULTSAll of the women were between 40 and 54 years old, Cauca-sian, non-diabetic, and normal to overweight. The women were grouped as premenopausal (n = 100) or postmenopausal (n = 69). None of the women reported anemia in their health history. One woman had a hemoglobin concentration of 5.9 g/dL; as an extreme outlier she was excluded. The premeno-pausal women had a mean hemoglobin of 13.6 g/dL (95% Confidence interval 13.5 – 13.8). The menopausal women had a mean hemoglobin of 13.9 g/L (95% Confidence inter-val 13.7 – 14.1), p = 0.003. Median hemoglobins were 13.6 g/dL for the premenopausal women and 13.8 g/dL for the

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 227
RESEARCH AND REPORTS
menopausal women. Boxplot analysis showed that the pre-menopausal women had lower hemoglobin concentrations in general, ranging from 9.8 g/dL to 15.4 g/dL compared to the menopausal women with 12.6 g/dL to 15.9 g/dL (Figure 1). Since iron deficiency anemia is known to prolong red cell survival and increase A1c results, four additional premeno-pausal women were excluded from the following analysis based on low hemoglobin or MCV.
The two sets of women were similar with respect to BMI, FPG, A1c, MCV, and RDW; they differed in age (p < 0.001) and Hemoglobin concentration (p = 0.009). Comparison of the two groups is shown in Table 1. FPG showed a weak correlation to A1c value overall (r = 0.251, p = 0.001). FPG showed a better correlation to A1c % in the menopausal group (r = 0.218, p = 0.034 for the premenopausal group, r = 0.296, p = 0.013 for the menopausal group), shown in Figure 2, A and B.
Total hemoglobin correlated with FPG in the menopausal women (r = 0.385, p = 0.001), but not with the premeno-pausal women (r = 0.130, p = 0.209). Absolute A1c values were generated in g/L (A1c %* total hemoglobin) shown in Table 1; the two groups of women were significantly different (p = 0.008). Absolute A1c correlated significantly to FPG (r = 0.362, p = 0.000). The correlation between Absolute A1c was stronger in the postmenopausal women (r = 0.463, p = 0.000) than the premenopausal women (r = 0.283, p = 0.005), and is shown in Figure 2, C and D.
DISCUSSIONPrevious studies have found a less than perfect correlation between A1c and FPG even in non-diabetics. As manu-facturers correct the technical factors affecting accuracy of those assays, pre-analytical factors come more into focus. Hemoglobin is glycated in a glucose-dose dependent fashion to form A1c. Total hemoglobin concentration has not been considered in this equation except in the instances where turnover of red cell mass is noticeably altered. Menstrual blood loss is an innocuous factor here, in that most of the premenopausal women would not be classified as anemic. Comparing the hemoglobin ranges of premenopausal to menopausal women shows the effect of that menstrual loss (Figure 1).
This study showed a positive correlation between total he-moglobin and FPG in the menopausal women (r = 0.385, p = 0.001). This is not unexpected. Serum hematocrit and serum ferritin levels have been shown to be positively as-sociated with plasma glucose levels in both diabetics and in subjects with insulin resistance syndrome.20-25 In a study of nondiabetic non-obese Caucasian women in a Pennsylvania population,26 hemoglobin correlated significantly with FPG in women aged 54 to 70 years (r = 0.344, p = 0.000, n = 119, unpublished results). Incorporating the total hemoglobin and A1c into Absolute A1c in the present study improved its correlation to FPG from 0.296 to 0.463. This suggests that both the glucose and the hemoglobin concentrations are relevant in the glycation process.
Table 1. Descriptive statistics of non-anemic subjects
Premenopausal Menopausal Mean (95% CI) Mean (95% CI) p value
Age 46.1 (45.3 – 47.0) 50.0 (49.3 – 50.7) <0.001**BMI 23.2 (22.6 – 23.8) 23.6 (22.8 – 24.3) 0.190FPG mg/dL 88.0 (88 – 90) 88.0 (86 – 90) 0.500A1c % 5.4 (5.3 – 5.4) 5.4 (5.3 – 5.5) 0.081Hemoglobin g/dL 13.6 (13.5 – 13.8) 13.9 (13.7 – 14.1) 0.009**MCV fL 90.5 (89.8 – 91.2) 90.1 (89.2 – 91.0) 0.311RDW 12.3 (12.2 – 12.5) 12.2 (12.1 – 12.4) 0.189Absolute A1c g/L 7.29 (7.18 – 7.41) 7.55 (7.39 – 7.71) 0.008**
n 95 69
*indicates significance at <0.05; **indicates significance at <0.01

228 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
Total hemoglobin did not correlate to glucose in the premeno-pausal women (r = 0.130, p = 0.209). This data is also consis-tent with findings from the Pennsylvania study: hemoglobin did not correlate to FPG in women aged 40 to 50 years (r = 0.208, p = 0.103, n = 63, unpublished data). Incorporating the total hemoglobin and A1c into Absolute A1c improved its cor-relation to FPG, but to a lesser extent than in the menopausal women (from 0.218 to 0.283). This finding suggests that menstrual blood loss has a pre-analytical effect on A1c. Since menstruation is not a pathologic process it has been overlooked as a source of variation in A1c accuracy. Women with heavy periods can become iron deficient; in fact 20% of women will become iron deficient sometime during their reproductive years.27 The paradox is this: While the iron deficiency should make the A1c concentration higher, the blood loss and replace-ment with younger cells should make the A1c concentration lower. In this study, five percent of the premenopausal women were suspected to have iron deficiency and therefore inaccurate A1c results. Even after they were excluded from the analysis the premenopausal group still had a poor correlation to FPG when compared to the non-menstruating group, consistent with a variable pattern of red blood cell turnover.
This study suggests that menstruation during middle age can have a significant effect on the accuracy on A1c, and that effect goes away at menopause. This is a significant finding, because half of the women who develop type 2 diabetes do so in perimenopause.28 The average age for diagnosis of diabetes in white American women is about 46 years,1 the average age for her menopause is 51, with perimenopause occurring as early as 35 or as late as 55.28 Women in perimenopause suffer from irregular menstruation. In a study of 500 perimenopausal women 18% reported more frequent and/or heavier periods with irregular bleeding between periods.29 Clearly the accuracy of the A1c result is dependent upon consistent hemoglobin concentration. This study showed a significant difference in hemoglobin concentration between premenopausal and menopausal women with similar MCV and RDW.
This work introduces the parameter “Absolute A1c”, derived as the product of total hemoglobin and %A1c. It is intriguing that this parameter showed a superior correlation to FPG. It is logi-cal that A1c formation is dependent upon the concentration of both glucose and hemoglobin. This parameter is very appealing, given the association of insulin resistance with increased iron stores,23-25 and after thorough study may prove to be a valuable diagnostic tool. It is important to interpret these results within the specifications of this study. The subjects were not diabetic, so the range of glucose and A1c was limited. Furthermore, only 169 subjects were tested. Mean blood glucose would be a stronger tester than FPG, but that data was not collected. Sub-jects with hemoglobinopathies may have different results. This study uses Absolute A1c as a tool to examine the differences between premenopausal and menopausal Caucasian women, and it is clear that these groups are different from each other. It will be important to test the validity of Absolute A1c and the effect of menstruation on A1c in non-Caucasian women, as these women represent a significant at-risk population. The prevalence of diabetes in African Americans is 1.8 times that of whites, the prevalence in Hispanics is 1.7 times that of whites, and American Indians are 2.2 times as likely to have diabetes as whites of a similar age.30
It will be interesting to test Absolute A1c in other groups, includ-ing those with iron deficiency, men, and older women. Coban and colleagues16 have already speculated that iron deficient indi-viduals may have increased A1c in part due to a higher glucose to hemoglobin ratio. One study restricted to men showed a low variation in Glycohemoglobin,31 which is consistent with the expectation of stable hemoglobin levels. Older women of all races have an increased prevalence of diabetes30 and will benefit from improvements in the indicators of glycemic control.
Figure 1. Hemoglobin ranges for premenopausal and menopausal women
The hemoglobin range is wider and the concentrations are lower for premenopausal compared to menopausal women. Ranges are depicted in quartiles. Error bars represent the extremes. The box represents quartile two and quartile three. The line represents the median. Open circles represent weak outliers.
RESEARCH AND REPORTS

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 229
Strengths of this study lie in its limitation of variables: the subjects are non-diabetics so overall glucose variation was limited, none of the subjects were obese so that blood volume was comparable in the subjects, and they all were the same sex and similar in age. It is unlikely that any participants had a hemoglobinopathy based on race and the ability of the HPLC analyzer to flag unexpected eluate peaks. One weakness of this study is that each set of data – FPG and A1c – was obtained only once from each participant. Women were dichotomized as premenopausal or menopausal based on patient reporting. Since this study revolved around blood loss from menstruation, women who had hysterectomies were included with the menopausal women. There was no method to determine which non-menopausal women were in peri-menopause, therefore all of the menstruating women were analyzed as one group. Hormonal changes may have some effect on glucose and A1c; this was not explored.
A1c results are valuable in long term maintenance and as-sessment of diabetes, and both the American Diabetes As-sociation6 and the American Heart Association recommend
a target goal A1c < 7% to reduce the risk for micro and macrovascular disease in women.32 The Standards of Medi-cal Care in Diabetes6 do not include an assessment of total hemoglobin in diabetes management, and men and women have the same target A1c goal. Clinicians and researchers should be aware that perimenopausal patterns of bleeding may cause inconsistent A1c values, and incorporate patient history of menstrual and other bleeding, self monitoring blood glucose results, and hemogram results (including hemoglobin, MCV and RDW) with A1c for a thorough assessment of glycemic control.
ACKNOWLEDGEMENTSThe author would like to thank Jorge Salgado, Mary Gi-menez, and Frances Connolly Forrest for help with data collection; Sherman Bonomelli and Swarna Krothapalli of the Medical Technology Program at the University of West Florida; and Joan Simmons, Stephanie Risinger, Marsha Dumas, Rita Casey and the laboratory staff at West Florida Hospital. This project was funded by a grant by the American Society for Clinical Laboratory Sciences.
RESEARCH AND REPORTS
Figure 2. Correlation of FPG with A1c in premenopausal and menopausal women
Correlation of A1c % is stronger in menopausal women than premenopausal women (compare B to A). Absolute A1c correlates better than A1c % to FPG in premenopausal women (compare C to A) and menopausal women (compare D to B).
*indicates significance at <0.05; **indicates significance at <0.01

230 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
REFERENCES 1. National Center for Chronic Disease Prevention and Health Promo-
tion, Diabetes Public Health Resource. Available from http://www.cdc.gov/diabetes/index.htm. Accessed 2005 Dec.
2. Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long term complications in insulin-dependent diabetes mellitus. N Eng J Med 1993;329:977-86.
3. UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patient with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-53.
4. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Intensive diabetes therapy and carotid intima-media thickness in type 1 diabetes mel-litus. N Engl J Med 2003;348:2294-303.
5. Gaede P, Vedel P, Larsen N, Jensen GVH, Parving H-H, Pederson O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med 2003;348:383-93.
6. American Diabetes Association. Standards of medical care in diabetes mellitus. Diabetes Care 2005;28(Suppl 1):S4-S36.
7. Nathan DM, Singer DE, Hurxthal K, Goodson JD. The clinical information value of the glycosylated hemoglobin assay. New Engl J Med. 1984;310:341-6.
8. Sacks DB, Bruns DE, Goldstein DE, Maclaren NK, McDonald JM, Parrott M. Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus. Clin Chem 2002;48:436-72.
9. Bry L, Chen PC, Sacks DB. Effects of hemoglobin variants and chemically modified derivatives on assays for glycohemoglobin. Clin Chem 2001;47:153-63.
10. Little RR, Rohlfing CL, Wiedmeyer HM, Myers GL, Sacks DB, Goldstein DE. The national glycohemoglobin standardization pro-gram: a five-year progress report. Clin Chem 2001;47:1985-1992.
11. National Glycohemoglobin Standardization Program. Available from http://www.ngsp.org. Accessed 2005 Dec.
12. Rohlfing CL, Wiedmeyer H-M, Little RR, England JD, Tennill A, D Goldstein. Defining the relationship between plasma glucose and HbA1c. Diabetes Care 2002; 25:275-8.
13. Winter WE, Signorino MR. Diabetes mellitus: pathophysiology, etiologies, complications, management, and laboratory evaluation. Washington, DC: AACC Press. 2002;137pp.
14. Tarim O, Kucukerdogan A, Gunay U, Eralp O, Ercan I. Effects of iron deficiency anemia on hemoglobin A1c in type 1 diabetes mel-litus. Pediatr Int 1999;41:357-62.
RESEARCH AND REPORTS
15. El-Agouza I, Abu Shahla A, Sirdah M. The effect of iron deficiency anaemia on the levels of haemoglobin subtypes: possible consequences for clinical diagnosis. Clin Lab Haematol 2002;24:285-289.
16. Coban E, Ozdogan M, Timuragaoglu A. Effect of iron deficiency anemia on the levels of hemoglobin A1c in non-diabetic patients. Acta Haematologica 2004;112:126-8.
17. Camargo JL, Gross JL. Conditions associated with very low values of glycohaemoglobin measured by an HPLC method. J Clin Pathol 2004;57:346-9.
18. Kilpatrick ES, Maylor PW, Keevil BG. Biological variation of glycated hemoglobin. Implications for diabetes screening and monitoring. Diabetes Care 1998;21:261-4.
19. Hudson PR, Child DF, Jones H, Williams CP. Differences in rates of glycation (glycation index) may significantly affect individual HbA1c results in type 1 diabetes. Ann Clin Biochem 1999;36:451-9.
20. McCarty MF. Hyperinsulinemia may boost both hematocrit and iron absorption by up-regulating activity of hypoxia-inducible fac-tor-1alpha. Med Hypothesis 2003;61:567-73.
21. Ford ES, Cogswell ME. Diabetes and serum ferritin concentration among US adults. Diabetes Care 1999;22:1978-83.
22. Fernandez-Real JM, Lopez-Mermejo AL, Ricart W. Perspectives in diabetes: cross-talk between iron metabolism and diabetes. Diabetes 2002;51:2348-54.
23. Haap M, Fritsche A, Mensing HJ, Haring, H-U, Stumvoll, M. Associa-tion of high serum ferritin concentration with glucose intolerance and insulin resistance in health people. Ann Int Med 2003;139:869-71.
24. Jehn M, Clark JM, Guallar E. Serum ferritin and risk of the metabolic syndrome in US adults. Diabetes Care 2004;27:2422-28.
25. Bozzini C, Girelli D, Olivieri O, Martinelli N, Bassi A, DeMatteis G, and others. Diabetes Care 2005;28:2061-3.
26. Behan KJ, Amin RW. Normoglycemia may encompass two subpopu-lations with respect to vascular risk in non-obese Caucasian women. Lab Med 2005; 36:2-7.
27. Schreiber W. Iron, porphyrin, and bilirubin metabolism. In: Kaplan LA, Pesce AJ , Kazmierczak SC eds. Clinical Chemistry Theory, Analysis, Correlation 4th edition. St. Louis: Mosby 2003;657-674.
28. Corio LE, Kahn LG. 2000. The change before the change. New York: Bantam Books. 2000;434pp.
29. Seltzer VL, Benjamin F, Deutsch S. Perimenopausal bleeding patterns and pathologic findings. JAMWA 1990;45:132-134.
30. National Diabetes Statistics. Available from http://diabetes.niddk.nih.gov/dm/pubs/statistics/index.htm#10. Accessed 2006 Apr 29.
31. Rohlfing C, Wiedmeyer H-M, Little RR, Grotz VL, Tennill A, England J, Madsen R, Goldstein D. Biological variation of glycohe-moglobin. Clin Chem 2002;48:116-8.
32. Mosca L. Heart disease prevention in women. Circulation 2004;109:e158-60.

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 231
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
An Overview of the Human Immunodeficiency Virus Featuring Laboratory Testing for Drug Resistance
EMIL SCOSYREV
The Focus section seeks to publish relevant and timely continuing education for clinical laboratory practitioners. Section editors, topics, and authors are selected in advance to cover current areas of interest in each discipline. Readers can obtain continuing education credit (CE) through P.A.C.E.® by completing the tearout form/examination ques-tions included in each issue of Clin Lab Sci and mailing it with the appropriate fee to the address designated on the form. Suggestions for future Focus topics and authors, and manuscripts appropriate for CE credit are encouraged. Direct all inquiries to the Clin Lab Sci Editorial Office, IC Ink, 858 Saint Annes Drive, Iowa City IA 52245. (319) 354-3861, (319) 338-1016 (fax). [email protected]
The human immunodeficiency virus (HIV) pandemic is unique in human history in its rapid spread, its persistence, and the depth of its impact. The Joint United Nations Programme on HIV/AIDS (UNAIDS) estimates that ap-proximately 65 million people have been infected with HIV since the beginning of the epidemic. During this time, approximately 25 million people have died from acquired immune deficiency syndrome AIDS.1
HIV-associated morbidity and mortality was substantially reduced during the last decade following the introduction of highly active antiretroviral therapy (HAART). In spite of the striking success of HAART in treating HIV infection, many patients experience treatment failure as genetic changes emerge in the virus leading to drug resistance.2
Laboratory testing for drug resistance in HIV strains is now used in combination with other methods to guide antiret-roviral therapy. The purpose of this report is to review the background information on HIV with the focus on the problem of drug resistance and to describe the laboratory methods of testing for drug resistance in HIV strains.
ABBREVIATIONS: ABC = abacavir; AIDS = acquired immune deficiency syndrome; AZT = zidovudine; ddC = zalcitabine; ddI = didanosine; dNTP = deoxynucleotide tri-phosphate; ddNTP = dideoxynucleotide triphosphate chain terminator; d4T = stavudine; FDA = Food and Drug Admin-istration; FTC = emtricitabine; HIV = human immunodefi-ciency virus; HAART = highly active antiretroviral therapy; LTR = long terminal repeats; NNRTI = non-nucleoside
reverse transcriptase inhibitor; NRTI = nucleoside analogue reverse transcriptase inhibitor; PI = protease inhibitor; PR = protease; RT = reverse transcriptase; TAM = thymidine analogue mutations; TDF = tenofovir; 3TC = lamivudine.
INDEX TERMS: genotypic resistance testing; HIV drug resistance; phenotypic resistance testing
Clin Lab Sci 2006;19(4):231
Emil Scosyrev MS is a PhD student in the Epidemiology Program in the Department of Community and Preventive Medicine, School of Medicine and Dentistry, University of Rochester, Rochester NY.
Address for correspondence: Emil Scosyrev MS, Epidemiol-ogy Program, Department of Community and Preventive Medicine, University of Rochester, 601 Elmwood Avenue, Box 644, Rochester NY 14642. (256) 736-4454. [email protected].
Emil Scosyrev MS is the Focus: Human Immunodeficiency Virus guest editor.
Focus Continuing Education Credit: see pages 246-249 for test questions and application form.
LEARNING OBJECTIVES 1. Describe the main genetic properties of the human im-
munodeficiency virus (HIV). 2. Describe the major events in the life cycle of HIV. 3. Identify the primary functions of each of the following
viral proteins: gp120, gp41, reverse transcriptase, inte-grase, protease.
4. List the three major stages in the natural course of the HIV infection.
5. Describe the changes in the viral loads and the CD4 counts during the natural course of the HIV disease.
6. List the four FDA-approved classes of antiretroviral drugs and identify the molecular targets of therapy for each class.
7. Describe benefits and limitations of antiretroviral therapy.

232 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
8. Describe the mechanisms of resistance in each of the four FDA-approved classes of antiretroviral drugs.
9. List the two fundamental approaches to HIV drug re-sistance testing.
10. Describe the principles of phenotypic resistance testing and list the main steps of the testing process.
11. Define IC50 and calculate the X-fold reduction in sus-ceptibility using the IC50 values.
12. Describe the principles of sequencing-based genotypic resistance testing and list the main steps of the testing process.
13. Describe the principles of dideoxynucleotide sequencing.14. Describe the principles and the limitations of hybridiza-
tion-based resistance assays.15. Discuss the clinical utility of HIV drug resistance testing.
BIOLOGICAL CHARACTERISTICS OF HIVOverviewThis section contains information on biological characteristics of HIV such as taxonomy, genetic properties, structural com-ponents, life cycle, pathogenesis, and the virulence factors.
TaxonomyHuman immunodeficiency virus type 1 (HIV-1) is assigned to genus Lentivirus, subfamily Orthoretrovirinae, family Ret-roviridae.3 Other human pathogens included in this family are HIV-2 (genus Lentivirus), HTLV-1, and HTLV-2 (genus Deltaretrovirus). Most cases of HIV infection worldwide are caused by HIV-1. The HIV-2 is endemic in West Africa, but cases are also reported in other parts of the world.4
Three major groups of HIV-1 are M (main), N (new), and O (outlier). Among M group viruses, which account for the overwhelming majority of HIV infections worldwide, there are several subtypes (clades), designated by the letters A-H, J and K, as well as many recombinant forms. Clade B, the most prevalent subtype in the United States (US) and western Europe, differs considerably from the subtypes found in Africa and Asia, where the majority of HIV infected individuals reside.5
Genetic properties and structural components of HIV-1The genetic material of HIV-1 is linear, single-stranded, positive-sense RNA, 9.2 kilobases in length. The genome is dimeric (two identical strands of RNA), the 5’-end has a methylated nucleotide cap, the 3’-end has a poly(A) tail, and both ends are flanked by long terminal repeats (LTR).3
The genome includes nine genes that encode various func-tional proteins of HIV.6 The HIV-1 genes and gene products
are summarized in Table 1. The main structural components of HIV virions are shown in Figure 1.
The virions are spherical, icosahedral, and enveloped particles, approximately 100 nm in diameter.3 The envelope is composed of glycoproteins embedded in a lipid membrane, which is de-rived from the host cells. The two viral envelope proteins, gp120 and gp41, form 72 trimeric functional units each consisting of three molecules of gp120 exposed on the virion surface and associated with three molecules of gp41 inserted into the viral lipid membrane.7,8 These functional units appear as knob-like structures on the surface of viral particles.
The inner surface of the lipid membrane is covered by the matrix protein (p17). Viral capsid, located beneath the matrix protein layer, contains two copies of HIV RNA associated
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
Table 1. HIV-1 genes and gene products
Genes Gene products
Gag p55 precursor is cleaved to form p17 (matrix protein), p24 (capsid protein), and p15 precursor which is further processed into p7 (nucleocapsid pro-tein), p6 (accessory protein), p1 and p2
Pol p11 (protease, also referred to as p10), p32 (integrase, also referred to as p31), p51/p66 (reverse transcriptase)
Env gp160 precursor is cleaved to form gp120 (envelope protein) and gp41 (transmembrane protein)
Tat p14 (transcriptional transactivator)
Rev p19 (regulator of viral gene expression)
Vif p23 (viral infectivity factor)
Nef p27 (negative effector)
Vpr p15 (viral protein R)
Vpu p16 (viral protein U)

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 233
with nucleocapsid protein (p7), reverse transcriptase (p66/51), protease (p11) and integrase (p32). The outer layer of the capsid is formed by p24 (the capsid protein).6
The HIV is characterized by extreme genetic variability. Retroviral replica-tion is a very unstable process with a high error rate (approximately 0.0001 per base per replication cycle) and rapid turnover of the virus.9,12 As a result of extensive viral replication with high mutation rates, each HIV-infected individual accumulates a large number of viral variants referred to as “quasispecies”. Genetic mutations occurring in HIV over time result in the production of altered antigens to which prior immune responses are ineffective. This property of HIV complicates the process of vaccine development. Genetic variability of HIV also results in the emergence of drug resistant strains.13
Life cycle and pathogenesisThe first step in the reproductive cycle of HIV is attachment of the virus to a
the viral RNA. This cDNA is inte-grated into the host’s genome by the ac-tion of integrase. The insertion of viral DNA (provirus) into the host genome may be followed by a period of tran-scriptional latency, which explains the inability of potent antiviral therapies to eradicate the virus from the body. The period of transcriptional latency also makes it difficult for the immune system to recognize and eliminate the HIV infected cells.13,17
After the provirus is integrated into the host genome, the transcription of HIV genes and the formation of new viral particles may begin. The HIV transcription process is initiated by the host proteins. Certain sequences in HIV’s 5’LTR region provide the bind-ing sites for transcription activators that are normally present in the host cells. The 5’ LTR is similar to eukary-otic transcriptional units. It contains downstream and upstream promoter elements, which include the initiator (Inr), TATA-box, and three Sp1 sites.18 These regions help position the RNA polymerase II at the site of initiation of transcription. Slightly upstream of the promoter is the enhancer domain with binding sites for nuclear factor kappa-B, nuclear factor of activated T cells, and Ets family members. These proteins activate the transcription of HIV genes.13,18,19
The initial transcription results in the synthesis of the regulatory proteins tat and rev. These proteins regulate the for-mation of other HIV gene products.13
Some of these products are translated as large precursor molecules that are later cleaved by the protease (p10) to form functional HIV subunits. The virions are assembled and released from the cell with the help of vif, nef, and vpu.13,20,21
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
Figure 1. Structural components of the HIV virions
susceptible CD4 positive host cell. The CD4 antigen serves as a receptor for the virus by binding the gp120 molecule on the outer surface of the HIV envelope. The T helper lymphocytes are the main target for HIV infection because they express high numbers of CD4 antigens. Other CD4 positive cells (macrophages, monocytes, dendritic cells, Langerhans cells, and microglial cells of the brain) may also be infected.14
Entry of HIV into the host cells re-quires an additional binding step in-volving a specific subset of chemokine receptors on the cell surface (CCR5 or CXCR4). Binding of the chemokine receptors allows for entry of HIV by inducing a conformational change in the gp41 glycoprotein, which medi-ates fusion of the virus to the cell membrane.14-16
Following membrane fusion, the viral particle is taken into the cell, and un-coating of the particle exposes the viral genome. Action of reverse transcriptase produces complementary DNA from

234 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
The pathogenesis of HIV infection is primarily associated with the de-struction of T helper lymphocytes. These cells play a central role in the immune system by regulating the activities of B and T lymphocytes and their destruction results in decreased effectiveness of both antibody- and cell-mediated immune responses.14
Severe immunosuppression leads to opportunistic infections, malignancies, and other complications of advanced HIV disease.
The exact mechanism of T helper lym-phocyte destruction in HIV infected individuals remains unclear.22 Various factors, such as direct cytopathic ef-fect of HIV, defects in the process of lymphocyte proliferation and replace-ment, chronic immune activation with high lymphocyte turnover, and the role of HIV induced apoptosis were investigated.22-27
SummaryThe HIV is a retrovirus with high af-finity for CD4 positive (T-helper) lym-phocytes. The destruction of these cells leads to severe immunosuppression with emerging opportunistic infec-tions, malignancies, and other compli-cations of advanced HIV disease.
Once the infection is established, HIV cannot be eliminated by natural or vaccine induced immune responses, drugs, or any other forms of therapy.
The persistence of infection results from a number of unique biological properties of HIV, such as its extreme genetic variability with short genera-tion time and high mutation rate, the phenomenon of transcriptional laten-cy, and the incompletely understood mechanism of CD4 cell depletion.
NATURAL HISTORY OF HIV INFECTION OverviewThe course of HIV infection has been observed to progress through three clinical stages, which coincide with the level of viral replication and the amount of immune destruction: pri-mary infection, clinical latency, and acquired immune deficiency syndrome (AIDS).14
Primary HIV infectionThe primary stage, also known as acute HIV infection, is characterized by a rapid burst of viral replication prior to the development of HIV-specific immune responses. During this stage plasma viral load often reaches very high levels in the range of millions of RNA copies/mL and HIV begins to dissemi-nate to lymphoid organs.14,28,29
Over the following weeks, viremia de-clines before reaching a viral setpoint.
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
Figure 2. Viral loads and CD4 counts during the natural course of the HIV disease
The magnitude of this setpoint is a strong predictor of long term disease progression rates. The initial reduction of viremia is associated with massive, oligoclonal expansion of HIV-specific cytotoxic T lymphocytes.30
The CD4 counts and CD4 function may decline during acute HIV infec-tion, occasionally to levels that allow opportunistic infections to develop. Even though the CD4 count rebounds with the resolution of the primary infection, it rarely returns to the pre-infection levels in the absence of antiviral therapy.30
Approximately 50 percent to 70 percent of patients with acute HIV infection develop flu-like symptoms, such as fever, sore throat, arthralgia, myalgia, fatigue, and lymphodenopathy. These symptoms, collectively known as acute retroviral syn-drome usually appear three to six weeks after initial infection and resolve within a few days to a few weeks.14

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 235
Clinical latencyAs HIV-specific immune responses develop, they begin to suppress the replication of the virus, and patients enter the period of clinical latency. This stage is characterized by a decrease in viremia and the absence of clinical symptoms.14
Despite the lack of clinical symptoms at this stage, viral replication and CD4 cell turnover remain active.10 The CD4 cell counts are gradually decreasing at an estimated rate of 50-90 cells/ microliter per year.31 The length of clinical latency can vary widely in individual patients, but typically lasts for several years.
AIDSMost untreated individuals will ultimately progress to AIDS, which is characterized by extremely low CD4 counts, re-surgence of viremia and severe immunosuppression. The relationship between viral load and CD4 counts during the natural course of HIV disease is summarized in Figure 2.
According to the Centers for Disease Control and Prevention criteria, AIDS is diagnosed when the CD4+ T-lymphocyte count drops below 200 cells/microliter, or below 14 percent of total lymphocyte count, or when the patient develops one of the AIDS-defining conditions.32 Most complications of advanced HIV disease are associated with opportunistic infections and malignancies. Individuals with AIDS are susceptible to a variety of bacterial, viral, parasitic, and fun-gal infections, including Pneumocystis jiroveci pneumonia, cerebral toxoplasmosis, CMV retinitis, and infections with Mycobacterium avium complex. Most of these conditions do not occur in immunocompetent individuals at all or cause mild self-limiting illness. Malignancies commonly seen in AIDS patients are Kaposi’s sarcoma, non-Hodgkin’s lym-phomas, and invasive cervical cancer. These conditions are included in the list of AIDS-defining illnesses.33
SummaryThe course of the HIV infection has been observed to progress through three clinical stages which coincide with the level of viral replication and the amount of immune destruction: acute infection, clinical latency, and AIDS. The acute stage is characterized by a rapid burst of viral replication prior to the development of HIV-specific immune responses. The stage of clinical latency is marked by decrease in viremia as the virus is cleared from the circulation, and the absence of clinical symp-toms. The AIDS stage is characterized by extremely low CD4 counts, resurgence of viremia and severe immunosuppression with emerging opportunistic infections and malignancies.
ANTIRETROVIRAL THERAPYOverviewThe HIV-associated morbidity and mortality has been substantially reduced during the last decade following the introduction of effective antiretroviral therapy.
There are currently four Food and Drug Administration (FDA)-approved classes of antiretroviral drugs in general use: nucleoside analogue reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), protease inhibitors (PIs), and fusion inhibitors.
Treatment with multiple drugs is more effective than treat-ment with a single drug. Multidrug regimens involving drugs from two or three of the classes mentioned above are now a standard of treatment known as highly active antiretroviral therapy or HAART.34
NRTIsNRTIs are false building blocks competing with physiological nucleosides. The incorporation of a nucleoside analog into a growing DNA chain aborts DNA synthesis, as phospho-diester bridges can no longer be built to stabilize the double strand.34 The FDA has approved seven nucleoside and one nucleotide analog.35 Tenofovir (TDF) is the nucleotide (adenosine monophosphate) analog. Zidovudine (AZT) and stavudine (d4T) are thymidine analogs. Lamivudine (3TC), zalcitabine (ddC), and emtricitabine (FTC) are cytidine analogs. Abacavir (ABC) is a guanosine analog. Didanosine (ddI) is an inosine analog, which is converted to dideoxyadenosine.34
NNRTIs The NNRTIs inhibit viral replication by binding directly to reverse transcriptase at a position in close proximity to the substrate binding site.34 There are three FDA approved NNRTIs: nevirapine, delavirdine, and efavirenz.35
Protease inhibitorsProtease inhibitors interfere with the post-translational modi-fication of viral proteins by directly binding to the active site of the HIV protease. Drug levels achieved during PI therapy can vary greatly among individuals, often dropping below the optimal therapeutic range. This has led to the practice of administering small doses of ritonavir, a P450 enzyme inhibitor, in combination with other PIs to increase drug concentrations by decreasing the clearance rate – a practice known as PI boosting.34,36 There are nine FDA-approved PIs: ritonavir, amprenavir, fosamprenavir, indinavir, lopinavir
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS

236 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
(manufactured in combination with ritonavir), nelfinavir, saquinavir, atazanavir, and tipranavir.35
Fusion inhibitors In 2003 T-20, the first drug of this class, was approved by the FDA. The T-20, also known as the Fuzeon, is a relatively large peptide composed of 36 amino acids. Unlike other antiret-roviral agents, it needs to be administered by subcutaneous injection. Fuzeon inhibits fusion by binding to gp41.34
Recommended combinationsCommon initial regimens consist of two nucleoside analogs, combined with either a PI, possibly boosted with ritonavir, or an NNRTI. Virological treatment success is usually un-derstood as the suppression of viral load to below the level of detection (< 50 copies/ml). The best time for initiation of therapy remains the subject of controversial debate. The risk of AIDS must be weighed against the risks of long-term toxicity and viral resistance.34
Benefits and limitations of HAARTAntiretroviral therapy reduces HIV-associated morbidity and mortality by reversing the natural course of the HIV disease. Patients receiving HAART usually have lower viral loads (virologic response), higher CD4 counts (immunologic re-sponse), and remain free of opportunistic infections and other AIDS-related conditions (clinical response). The progression to AIDS may be reversed or delayed by many years.
Nevertheless, HAART has limitations that may eventually lead to treatment failure. The following factors limit the ef-ficacy of antiretroviral therapy in HIV patients:
• HAART does not result in cure. HIV infection, there-fore, must be managed as a chronic condition with the problem of poor patient adherence to therapy, high cost of treatment, and limited availability of HAART in resource-poor settings.
• Antiretroviral therapy is associated with serious side effects, including hepatotoxicity, myelotoxicity, CNS problems, pancreatitis, lactic acidosis, nephrotoxicity and other complications.37
• HIV may become resistant to all currently available antiretroviral agents, including those used in salvage regimens. The problem of drug resistance is discussed separately in the next section.
SummaryDuring the last decade, with the introduction of HAART, AIDS was transformed from a rapidly fatal illness to a man-ageable chronic condition. However, HAART does not result in cure, it produces serious side effects, and viral resistance is recognized quickly following the introduction of new drugs. There are currently four FDA-approved classes of antiretro-viral drugs in general use: NRTIs, NNRTIs, PIs, and fusion inhibitors. Treatment with multiple drugs is more effective than treatment with a single drug. Multidrug regimens involving drugs from two or three of the classes mentioned above are now a standard of treatment.
THE PROBLEM OF DRUG RESISTANCEOverviewThis section will review the prevalence of drug resistant strains of HIV in the US, the origins and the mechanisms of resistance, and the relationship between drug resistance and clinical progression.
Prevalence and origins of resistanceIn the US, as many as 50% of patients receiving antiretroviral therapy are infected with viruses resistant to at least one of the available antiretroviral drugs.12 The average prevalence of resis-tance in treatment-naïve patients is approximately 14 percent, and may be as high as 23 percent in some areas.38-40
The origins of HIV drug resistance are strongly associated with the high mutation rate in the HIV genome, which is one of the key biological characteristics of the virus. Most antiretroviral drugs target viral proteins. The inhibitory ef-fect of the drug may be reduced when the structure of the target protein is altered in a certain way. These structural changes result from alterations in the corresponding HIV genes. The rate of resistance-conferring structural changes in target proteins is proportional to the mutation rate in the HIV genome.12
The genomic mutation rate is determined by two factors: 1) the number of mistakes per genome per replication cycle, which is very high in HIV because reverse transcriptase has no proof reading ability, and 2) by the number of replication cycles per unit of time.12,41 The magnitude of the second fac-tor is reflected in the viral loads. High viral loads are markers of active replication. It is clear that incomplete suppression of viral replication during HAART (VL > 50 copies/mL) is a risk factor for the emergence of drug resistance. This risk is proportional to the viral load.42
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 237
Incomplete suppression of replication with emerging drug resistance may result from the pharmacokinetic factors that decrease the drug levels and from treatment interruptions due to the dose-limiting side effects, poor patient adherence to therapy, or limited availability of HAART in resource-poor settings. The emergence of resistance in patients with stable virologic response to HAART (VL < 50 copies/mL) is less likely. However, as was stated earlier, resistant strains may be transmitted between individuals and appear in treatment-naïve patients.
Mechanisms of resistanceAntiviral drug resistance may be defined as the reduction in the susceptibility of mutated viruses to specific antiviral drugs. Fully susceptible viral strains not exposed to the selective pressure of antiviral drugs are known as the wild-type strains. Antiretroviral resistance is usually mediated by changes in the molecular target of therapy as a result of point mutations in the HIV genome.12
There is a standard numbering system for HIV-1 protease, reverse transcriptase, and gp41 which is based on the amino acid sequences of these peptides. Mutations are described using a shorthand notation in which a letter indicating the wild-type amino acid is followed by the amino acid position number and a letter indicating the mutation. For example, PR: I54V means that isoleucine (I) has been replaced by valine (V) in position 54 of the protease. If there is a mix-ture of more than one amino acid at a certain position, the components of the mixture are written after the position, separated by a slash.36 For example, RT: M184M/V means that the sequence has a mixture of the wild-type residue me-thionine (M) and the mutant residue valine (V) at position 184 of reverse transcriptase.
It has become customary to label some drug resistance muta-tions as “primary” and other mutations as “secondary”. Primary mutations are those that reduce drug susceptibility by them-selves whereas secondary mutations reduce drug susceptibil-ity in combination with primary mutations.36 The following discussion will focus on the main mechanisms of resistance in the four FDA-approved classes of antiretroviral drugs.
NRTIsThe NRTIs are chain terminators that block the extension of proviral DNA during reverse transcription. Reverse tran-scriptase is a heterodimer consisting of p66 and p51 subunits. The p51 peptide is composed of the first 440 amino acids translated from the pol gene. This subunit has no enzymatic
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
activity and functions as a supporting structure for the enzy-matically active p66 subunit. The p66 peptide is composed of all 560 amino acids of the pol gene. This subunit contains the DNA-binding groove and the active polymerization site. The polymerase domain of p66 subunit has sub-domains referred to as “fingers”, “palm”, and “thumb”. The remainder of the p66 subunit contains an RNaseH sub-domain and a connection sub-domain. Most RT inhibitor resistance muta-tions are in the 5’ polymerase coding regions, particularly in the “fingers” and “palm” subdomains.36 There are two main biochemical mechanisms that lead to NRTI resistance: steri-cal inhibition and primer unblocking.
Sterical inhibition is caused by mutations enabling the reverse transcriptase to recognize structural differences between NRTIs and the naturally occurring dNTPs. Incorporation of NRTIs is then prevented in favor of dNTPs. Examples of mutations associated with this mechanism are: M184V, Q151M, L74V, and K65R.39
Primer unblocking is caused by phosphorylysis via ATP or pyrophosphate leading to the removal of the NRTIs already incorporated in the growing DNA chain. This is the case with the following mutations: M41L, D67N, K70R, L210W, T215Y and K219Q. These substitutions are historically known as thymidine analog mutations (TAMs) because they were initially observed with zidovudine therapy.39 Mu-tations associated with primer unblocking mechanism are also referred to as NEMs (nucleotide excision mutations).36 Individual mutations and their effects on susceptibility to different antiretroviral agents are summarized in Table 2.
NNRTIsThe NNRTIs inhibit reverse transcriptase by binding to a hydrophobic pocket in the p66 subunit.43 Unfortunately, a single point mutation (most often K103N) can lead to a 20 to 30-fold resistance to all available NNRTIs.39
Residue 103 is located on the outer rim of the NNRTI-bind-ing pocket. Structural studies of HIV-1 RT with K103N have shown that this mutation creates a network of hydrogen bonds which is not present in the wild-type enzyme. These changes appear to stabilize the closed pocket form of reverse transcriptase and interfere with the ability of inhibitors to bind to the enzyme.43
HIV-1 group O and HIV-2 are intrinsically resistant to most NNRTIs.36 Other mutations associated with NNRTI resistance are listed in Table 2.

238 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
Protease inhibitorsThe HIV-1 protease is a homodimeric protein composed of two chemically identical subunits each consisting of 99 amino acids. The enzyme contains a hydrophobic sub-
strate cleft which recognizes and cleaves different peptide sequences to produce functional HIV proteins and a flex-ible flap region that closes down on the active site upon substrate binding.36,44
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
Table 2. FDA-approved antiretroviral drugs and selected resistance mutations
FDA-approved Examples of mutations associated with drug resistanceantiretroviral drugs
NRTIsZidovudine M41L, D67N, K70R, Q151M, L210W, T215Y, K219Q, T69SSXStavudine M41L, D67N, K70R, Q151M, L210W, T215Y, K219Q, T69SSX Didanosine K65R, L74V, Q151M, T69SSXZalcitabine K65R, L74V, Q151M, M184V, T69SSXEmtricitabine K65R, M184V/I, T69SSXLamivudine K65R, M184V/I, T69SSXAbacavir K65R, L74V, Y115F, Q151M, M184V, T69SSXTenofovir K65R, T69SSX
NNRTIsEfavirenz L100I, K101E, K103N, V106M, V108I, Y181C/I, G190S/ANevirapine L100I, K101E, K103N, V106M, V108I, Y181C/I, G190ADelavirdine L100I, K101E, K103N, V106M, Y181C, P236L
PIsIndinavir M46I/L, I54V, V82A, I84V, L90M, L10I/V, K20M/R, L24IRitonavir M46I/L, I54V, V82A, I84V, L90M, L10I/V, K20M/R, L24INelfinavir D30N, M46I/L, V82A, I84V, L90M, L10I/VSaquinavir >3 of the following: L10I, G48V, I54V/L, A71V/T, V77I, L90MTipranavir >2 of the following: L10I/V, M46I, I54V, V82A, I84V, L90M
Lopinavir >7 of the following: L10F/I/R/V, K20M/R, L24I, V32I, L33F, M46I/L,(with ritonavir) I47V/A, I50V, F53L, I54V/T/L, L63P, A71V/T, G73S, V82A/F/T, I84V, L90M
Amprenavir >5 of the following: L10F/I/V, V32I, E35D, G73S, I54/V/L/M, I84V, L90M(with ritonavir) orFosamprenavir(with ritonavir)
Atazanavir >5 of the following: L10I/V/F, K20R, L24I, L33I, M36I/L, M46I/L, I50L, L71V, (with ritonavir) G73C/S/T/A, V82A/F, I84V, L90M
Fusion inhibitorsT-20 G36D/E/S/V, N42T/D/S, N43D/K/H/S

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 239
Resistance to protease inhibitors is mediated by the appear-ance of protease amino acid substitutions, at positions either in direct contact with the inhibitor or at distant sites. These substitutions reduce the binding affinity between the inhibitor and the mutant protease enzyme.45 Primary resistance muta-tions are frequently seen in the substrate cleft (V82A/T/F/S, I84V, D30N) and in the flap (I54V) regions. Protease muta-tions may also occur at other conserved residues, for example, L90M contributes to the development of resistance to each of the nine approved PIs.36,39,46 It is interesting that some prote-ase inhibitors, especially when boosted with ritonavir, have a high genetic barrier to resistance meaning that several muta-tions must first accumulate before the resistance can develop. Resistance to boosted Lopinavir, for example requires the accumulation of at least eight different mutations.39 Protease resistance mutations are summarized in Table 2.
Fusion inhibitorsIn the process of fusion, two heptad repeat domains (HR1 and HR2) of gp41 form a helical bundle containing trimers of each domain. The first FDA-approved inhibitor of viral entry (T-20) is a synthetic peptide designed to inhibit the interaction of HR1 and HR2 by mimicking part of HR2, residues 127 to 162.12,36,39
The entire gp41 coding region consists of 351 codons. The T-20 resistance is generally accompanied by the appearance of mutations at positions 36 to 45 in the HR1 (e.g., G36/D/E/S, N42T/D/S).39 See Table 2 for a list of mutations associated with T-20 resistance.
Drug resistance and response to therapyThe relationship between resistance mutations and response to therapy is very complex. Each resistance mutation may be characterized by two factors: 1) level of associated phenotypic resistance, measured as an X-fold reduction in susceptibility compared to the wild-type virus, and 2) specificity of resis-tance mutation to one or more drugs. For example, D30N is a protease substrate cleft mutation that confers five to 20 fold resistance to nelfinavir, but not to other PIs.36,39 This mutation is relatively specific for one drug. On the other hand, K103N is an RT mutation that causes 20 to 30-fold resistance to all available NNRTIs (cross-resistance).39
Specificity and the X-fold reduction in susceptibility as-sociated with individual mutations may be influenced by the presence of other mutations. For example, resistance to zidovudine increases with increasing number of TAMs. Two TAMs result in a 5-fold reduction in susceptibility, three
TAMs confer approximately 30-fold resistance, and four or more TAMs result in 100-fold resistance.39
The complexity of relationship between genotypic resistance and phenotypic response may be demonstrated in the fol-lowing example. M184V is a common RT mutation confer-ring resistance to certain NRTIs by the sterical inhibition mechanism. M184V by itself causes high-level (>100-fold) resistance to lamivudine and emtricitabine. In the presence of TAMs, M184V also decreases susceptibility to didanosine, zalcitabine, and abacavir, but increases susceptibility to zid-ovudine, stavudine, and tenofovir (increasing susceptibility is only possible if no more than three TAMs are present).34,36,39 Another interesting feature of M184V mutation is that it impairs viral fitness. For this reason, lamivudine may some-times be included in the combination ARV therapy despite proven resistance in order to conserve the M184V mutation and thus reduce the replicative capacity of HIV.34
Because antiretroviral resistance depends on specific com-binations of primary and secondary mutations and the relationship between individual mutations is very complex, special algorithms were developed for interpretation of drug resistance data. These algorithms will be reviewed in the next section.
SummaryDrug resistance is one of the main limitations of HAART. The prevalence of drug resistant strains of HIV in the US is at least 50% in patients receiving ARV therapy, and may be as high as 23% in treatment-naïve patients. The origins of resistance are very diverse and include biological and epidemiological factors, such as extreme genetic variability of HIV with high mutation rate and short generation time, incomplete suppression of replication during treatment due to pharmacokinetic factors, poor patient adherence to therapy, dose-limiting side effects, and limited availability of HAART in resource-poor settings. The mechanisms of resistance include various structural changes in the target proteins as a result of point mutations in the HIV genome. The relationship between individual mutations and response to therapy is very complex. The interpretation of drug resis-tance data requires special rules and guidelines.
LABORATORY TESTING FOR DRUG RESISTANCE IN HIV STRAINSOverviewHIV drug resistance can be measured using either genotypic or phenotypic assays. Two genotypic assays, TruGene and
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS

240 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
ViroSeq, have been approved by the FDA. Clinical utility of resistance testing has been demonstrated in a number of randomized prospective studies. HIV-resistance testing is now recommended by various national and international treatment guidelines.36,39
Principles of phenotypic resistance testingPhenotypic resistance testing is based on the quantitative as-sessment of viral replication in cell cultures under the selective pressure of increasing concentrations of specific antiretroviral drugs. Drug concentration that results in 50% inhibition of viral growth is termed IC50. Phenotypic resistance is reported as an X-fold reduction in susceptibility, which is calculated by dividing the IC50 of the patient’s isolate by the IC50 of the wild-type virus. For example, if the wild-type virus requires 0.5 mg of zid-ovudine to reduce viral growth by 50% and the patient’s isolate requires five mg, then the phenotypic resistance to zidovudine will be reported as ten-fold reduction in susceptibility.2
To interpret the phenotypic resistance data (an X-fold reduction in susceptibility), it is important to know the re-producibility of the assay for a given drug (technical cutoff), the variation in IC50 required to inhibit wild-type viruses (biological cutoff), and the clinical significance associated with different levels of reduced drug susceptibility (clinical cutoff). The clinical cutoffs indicate up to which levels of reduced drug suscepibility virological success can still be ex-pected. For example, if a phenotypic assay reported a 15-fold resistance for a particular drug and the clinical cutoff for this drug/assay combination is 10-fold resistance, then the patient will probably no longer benefit from the drug. For protease inhibitors, one has to know whether the respective clinical cutoffs have been determined for unboosted or boosted PIs. Higher drug concentrations achieved with ritonavir boosting may overcome certain levels of resistance.39
Commercially available phenotypic assays include: Antivi-rogram (Virco), PhenoSense (Monogram), and Phenoscript (Viralliance). All phenotypic assays follow the same steps with minor variations in the testing process. The testing procedure begins with extraction of HIV RNA from patient’s plasma followed by reverse transcription and amplification of reverse transcriptase (RT) and protease (PR) sequences by PCR. The amplified sequences are then inserted into an RT-PR deficient vector. A second recombinant vector is prepared with RT-PR sequences from the wild-type virus. The replication of both recombinant forms in cell culture is measured under differ-ent concentrations of antiretroviral drugs. The results are displayed as percent inhibition of viral growth versus log10
drug concentration. Fold resistance values are calculated by dividing IC50 for the recombinant virus from the patient by the IC50 for the recombinant wild-type virus.47-48
Different commercial assays follow the same procedural steps but use different methods and reagents for RNA extraction, reverse transcription, amplification, recombinant vector preparation, and viral replication assessment. Both negative and positive controls are included for each step of the test-ing procedure. Negative controls for susceptibility testing are represented by the wild-type susceptible strain. Positive controls are derived from mutated viruses that are chosen to represent different resistance patterns for each drug class.
The performance characteristics of commercially available phenotypic assays were evaluated by the manufacturers and by independent research groups in recently published stud-ies.49-52 The agreement between the assays varied with drug classes and was highest for protease inhibitors and lowest for NRTIs.49-50 One recently published study concluded that the PhenoSense assay is more precise than the Antivirogram assay and superior at detecting resistance to certain NRTIs (abacavir, didanosine, and stavudine).50 Another study reported poor correlation between PhenoSense and Antivi-rogram for samples with lower resistance values (values near the cutoffs) that affected the interpretation of results. Using drug-specific cutoff values for viruses classified as resistant by the Antivirogram or PhenoSense assays, respectively, only 71.4% (95% CI: 58.7%-82.1%) and 57.0% (95% CI: 45.3%-68.1%) of the samples were classified as resistant using the other assay.51
Phenotypic resistance testing is used less frequently than geno-typic resistance testing due to the higher cost, greater complexity of the assays and longer turnaround times.36,39,53 The clinical utility of genotypic resistance testing has been demonstrated in a larger number of clinical trials, the evidence for clinical utility of phenotypic assays was less convincing.36,54-55
Principles of genotypic resistance testingGenotypic testing is based on identification of mutations associated with resistance to specific antiretroviral drugs. These mutations may be detected by the sequencing of the amplified segments of HIV genome or by specific hybridiza-tion techniques.39
Commercially available genotypic assays are sequencing-based methods: HIV-1 TruGene (Visible Genetics/Bayer Diagnostics), ViroSeq (Celera Diagnostics/Applied Biosys-
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 241
tems), VircoType HIV-1 (Virco), GeneSeq (Monogram), and GenoSure Plus (LabCorp).39 Some laboratories use “home-brew” methods with reagents obtained from separate vendors. TruGene and ViroSeq have been approved by the FDA in 2002 and 2003 respectively.56 This section reviews the general principles of genotypic resistance testing.
All sequencing-based genotypic assays follow the same steps with minor variations in the testing procedure. The testing process begins with HIV RNA extraction from patient’s plasma, followed by reverse transcription and amplification of the RT and PR segments by PCR. The amplification products are then sequenced by dideoxynucleotide sequenc-ing procedure.36 Dideoxynucleotide sequencing is based on the synthesis of new DNA strands (complementary to the target sequence of interest) in the presence of primers, de-oxynucleotide triphosphates (dNTPs) and dideoxynucleotide triphosphate chain terminators (ddNTPs). The synthesis of each new strand starts with the primer and continues until a chain terminator is incorporated in place of the appropriate dNTP. This process creates a mixture of DNA strands each differing from one another by the length of one nucleotide. The strands are arranged in the order of increasing length by polyacrylamide gel electrophoresis, and the final nucleotide on each strand is read by an automated sequencer using fluo-rometric methods that depend upon labeling of the primer or the terminators. This process is illustrated in Figure 3. The resulting sequence is compared to the wild-type reference sequence and examined for mutations associated with drug resistance. Known sequences of HIV-1 are processed with patients’ specimens for quality control.
Because a separate fluorescent marker is used for each of the four bases of DNA, a typical sequencing electrophoretogram appears as a series of colored peaks. Each peak corresponds to a specific nucleotide position in the target segment of DNA. If a mixture of two nucleotides is present at a specific position, a double peak will be generated for this position on the electrophoretogram. In the sequencing-based geno-typic assays, a nucleotide mixture can be detected when the least common nucleotide is present in at least 20% of the total virus population.36,39 Once the nucleotide sequence is determined, it may be converted to the amino acid sequence and aligned with the reference wild-type sequence as shown in Figure 4.
Hybridization techniques, as an alternative to complete sequencing, may be used to detect specific mutations asso-ciated with drug resistance. However, resistance testing by hybridization is challenging because HIV genome is very polymorphic. A recent study compared a hybridization-based method (LiPA reverse hybridization assay) to conventional sequencing-based methods (TruGene and home-brew se-quencing assays). LiPA HIV-1 RT and PR resistance assays use reverse hybridization to detect wild-type and mutant codons at specific positions in the RT and PR segments. Codon-specific oligonucleotide probes are applied as discrete lines on a nitrocellulose membrane in a strip format. After de-naturation, the amplified biotinylated DNA material hybrid-izes with the specific probes. A streptavidin conjugate labeled with alkaline phosphatase is then added to the mixture. The labeled conjugate attaches to the biotinylated DNA-probe hybridization products and a purple-brown color is formed after incubation with BCIP/NBT chromogen.57
The study reported the following concordance rates for LiPA versus conventional sequencing: for PR, 91.3% of the codon results were concordant, 3.0% were partially concordant, 4.5% were indeterminate by LiPA, and 1.3% were discor-dant. For RT, 88.0% of the codon results were concordant, 5.9% were partially concordant, 5.2% were indeterminate by LiPA, and 0.9% were discordant (partial concordance is reported if one method detected a mixture, while the other method detected one of the mixture’s components). The authors concluded that the clinical utility of LiPA is limited by the high rate of indeterminate results.57 Similar conclu-sions were made in the previous studies.58
Sequencing concordance as a measure of agreement between various sequencing-based methods was evaluated in a number of studies published between 2001 and 2006.59-74 The two
Figure 3. DNA strands arranged in the order of increas-ing length by polyacrylamide gel electrophoresis
DNA strands Detected sequence
Primer-A APrimer-AC CPrimer-ACT TPrimer-ACTG GPrimer-ACTGA APrimer-ACTGAT TPrimer-ACTGATC C
The last nucleotide on each strand is a chain terminator.
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS

242 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
FDA-approved assays were evaluated for reproducibility and compared to each other and to the reference sequences gener-ated by other sequencing methods. The average sequencing concordance with B-subtype isolates ranged from 97.6% to 99.9%.59,65-67,72-74 The performance of sequencing-based assays with non-B subtypes was less clear because multiple amplification and sequencing failures were reported in some studies, while other studies reported improved per-formance.60-61,70
The final step in the process of genotypic resistance testing is the analysis of generated sequences. The RT-PR sequences obtained from the patient are compared to the RT-PR se-quences of the wild-type virus and examined for mutations at resistance sites. The sequences may be aligned using dif-ferent software programs such as Bayer’s OpenGene software (included in the TruGene kit), Applied Biosystems Sequenc-ing Analysis Software (a component of the ViroSeq system), MegAlign program of Lasergene Navigator (DNASTAR), and others.67,71
When specific resistance-associated mutations are identified, an additional software program is used to generate the resis-tance report that relates phenotypic resistance to genotypic data. Both TruGene and ViroSeq include such programs.
The primary sequencing data may also be analyzed by an independent software program. The Stanford HIV data base (http://hivdb.stanford.edu) contains two programs: HIVseq and HIValg. The HIVseq program accepts user- submitted RT and PR sequences and compares them to a reference wild-type sequence. The HIValg program accepts user submitted RT and PR sequences or specific mutations and returns in-ferred levels of resistance to the FDA approved antiretroviral
drugs using three different algorithms: HIVDB, ANRS, and Rega v6.4. A similar program called “Geno2Pheno” is located at http://www.geno2pheno.org/cgi-bin/geno2pheno.pl. The HIV sequence database is located at http://www.hiv.lanl.gov/content/index. A simulated genotypic resistance report is shown in Figure 5.
Clinical utility of HIV resistance testingThe clinical utility of HIV resistance testing has been evalu-ated in a number of studies. Most studies have demonstrated that patients with treatment failure, whose physicians had access to genotypic resistance data before the therapy was changed, usually had more significant decreases in the viral load than patients for whom treatment was changed without knowledge of the resistance profile.36,75-78 Similar data was obtained for phenotypic testing. Some studies showed “no significant difference” in viral load reduction between resis-tance testing and physician guided therapy.36,79 The benefit of phenotypic resistance testing was also questioned in some re-cently published reports.54-55 Nevertheless, the clinical utility of resistance testing is now widely recognized, and resistance testing in patients with treatment failure is recommended by various expert panels, including the US Department of Health and Human Services.36,39
Several recently published reports also recommend resis-tance testing for treatment-naïve patients newly infected with HIV.40,80-81 As was previously stated, the prevalence of primary resistance mutations in treatment naïve patients in the US may be as high as 23%. Resistance testing prior to the initiation of ARV therapy is cost effective and may improve the clinical outcomes.80
Summary
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
Figure 4. Simulated amino acid sequence of patient’s isolate aligned with the reference wild-type sequence
Note that the patient’s isolate has three mutations (deviations from the reference sequence) in this segment: L10I, K20M, and V32I. These mutations are associated with resistance to protease inhibitors (see Table 2). This diagram shows only one segment of protease, positions 1-40. Sequencing-based methods of HIV drug resistance testing usu-ally sequence the entire protease (positions 1-99) and approximately 300 codons of reverse transcriptase.
Amino acid position: 1 10 20 32 40
Reference sequence: PQVTLWQRPL VTIKIGGQLK EALLDTGADD TVLEEMSLPG
Patient’s sequence: ………………I………………..M………………………I……………

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 243
the ability of the virus to grow in cell cultures with different concentrations of antiretroviral drugs. Genotypic testing is used more frequently than phenotypic testing because of lower cost, wider availability, shorter turnaround time, and more reliable evidence of clinical utility. The HIV drug resistance testing is now recommended by various national and international treatment guidelines.36-39
REFERENCES 1. UNAIDS data: AIDS epidemic update, December 2005. Available
from http://www.unaids.org/epi/2005/doc/report_pdf.asp. Accessed 2006 Jun15.
2. Constantine N, Zhao R. Molecular-based laboratory testing and monitoring for human immunodeficiency virus infections. Clin Lab Sci 2005;18:263-70
3. NIH data: Büchen-Osmond, C. (Ed) (2004). 00.061.1.06.009. Hu-man immunodeficiency virus 1. In: ICTVdB - The Universal Virus Database, version 3. ICTVdB Management, New York: Columbia University. Available from http://www.ncbi.nlm.nih.gov/ICTVdb/ICTVdB/00.061.1.06.009.htm. Accessed 2005 Nov 3.
4. CDC data: Human immunodeficiency virus type 2. Available from http://www.cdc.gov/hiv/pubs/facts/hiv2.htm. Accessed 2006 Jan 3.
5. Spira J, Wainberg MA, Loemba H. Impact of clade diversity on HIV-1 virulence, antiretroviral drug sensitivity and drug resistance. J Antimicrob Chemother 2003;51:229-40.
6. Cherry E, Weinberg M. The Structure and Biology of HIV-1. In: Emini E, ed. The human immunodeficiency virus. Princeton: Princ-eton University Press; 2002:1-44.
7. Forsell MN, Li Y, Sundback M, and others. Biochemical and im-munogenic characterization of soluble human immunodeficiency virus type 1 envelope glycoprotein trimers expressed by semliki forest virus. J Virol 2005;79:10902-14.
8. Kwong PD, Wyatt R, Robinson J, and others. Structure of an HIV gp120 envelope glycoprotein in complex with the CD4 receptor and a neutralizing human antibody. Nature 1998;393:648-59.
9. Boyer PL, Hughes SH. Effects of amino acid substitutions at position 115 on the fidelity of human immunodeficiency virus type 1 reverse transcriptase. J Virol 2000;74:6494-500.
10. Ho DD, Neumann AU, Perelson AS. Rapid turnover of plasma virions and CD4 lymphocytes in HIV-1 infection. Nature 1995;373:123-6.
11. Wei X, Ghosh SK, Taylor ME, and others. Viral dynamics in human immunodeficiency virus type 1 infection. Nature 1995;373:117-22.
12. Clavel F, Hance AJ. HIV drug resistance. N Engl J Med 2004;350:1023-35.
13. Rubbert R, Ostrowski M. Pathogenesis of HIV infection. In: Hoff-mann C, Rockstroh JK, Kamps BS, eds. HIV Medicine 2005. Flying Publisher; 2005:59-84.
14. Miller L. HIV serology. In: Stevens CD. Clinical immunology and serology, 2nd ed. Philadelphia, PA: FA Davis Company; 2003:346-69.
15. Deng H, Liu R, Ellmeier W, and others. Identification of a major co-receptor for primary isolates of HIV-1. Nature 1996;381:661-6.
16. Tamamura H, Otaka A, Fujii N. Development of anti-HIV agents targeting dynamic supramolecular mechanism: entry and fusion inhibitors based on CXCR4/CCR5 antagonists and gp41-C34-remodeling peptides. Curr HIV Res 2005;3:289-301.
17. Bisgrove D, Lewinski M, Bushman F, and others. Molecular mechanisms of HIV-1 proviral latency. Expert Rev Anti Infect Ther 2005;3:805-14.
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
Figure 5. Simulated genotypic resistance report
Most algorithms report resistance data in three basic categories: “susceptible” (no evidence of resistance), “intermediate” (possible or emerging resistance), and “resistant”.
Resistance Report
Patient ID: Patient Name:Sample ID: Date Drawn:
Relevant RT mutations: M41L, K65R, L74V, D67N, K70R, Q151M, M184V, L210W, T215Y, K219Q, K103N, Y181C
NRTIsZidovudine resistantStavudine resistantDidanosine resistantZalcitabine resistantEmtricitabine resistantLamivudine resistantAbacavir resistantTenofovir resistant
NNRTIsNevirapine resistantDelavirdine resistantEfavirenz resistant
Relevant PR mutations: D30N
PIsIndinavir susceptibleRitonavir susceptibleSaquinavir susceptibleNelfinavir resistantTipranavir susceptibleLopinavir/r susceptibleAmprenavir/r susceptibleFosamprenavir/r susceptibleAtazanavir susceptible
Drug resistance of HIV can be measured using either geno-typic or phenotypic assays. Genotypic assays detect muta-tions that cause drug resistance. Phenotypic assays measure

244 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
18. Bentley K, Deacon N, Sonza S, and others. Mutational analysis of the HIV-1 LTR as a promoter of negative sense transcription. Arch Virol 2004;149:2277-94.
19. Karin M, Ben-Neriah Y. Phosphorylation meets ubiquitina-tion: the control of NF-[kappa]B activity. Annu Rev Immunol 2000;18:621-663.
20. Adekale MA, Cane PA, McCrae MA. Changes in the Vif protein of HIV-1 associated with the development of resistance to inhibitors of viral protease. J Med Virol. 2005;75:195-201.
21. Binette J, Cohen EA. Recent advances in the understanding of HIV-1 Vpu accessory protein functions. Curr Drug Targets Immune Endocr Metabol Disord 2004;4:297-307.
22. Herbeuval JP, Grivel JC, Boasso A, and others.CD4+ T-cell death induced by infectious and noninfectious HIV-1: role of type 1 interferon-dependent, TRAIL/DR5-mediated apoptosis. Blood 2005;106:3524-31.
23. Pantaleo G. Unraveling the strands of HIV’s web. Nat Med 1999;5:27-8.
24. Silvestri G, Feinberg MB. Turnover of lymphocytes and conceptual paradigms in HIV infection. J Clin Invest 2003;112:821-4.
25. Stocker H, Scheller C, Jassoy C. Destruction of primary CD4(+) T cells by cell-cell interaction in human immunodeficiency virus type 1 infection in vitro. J Gen Virol 2000;81(Pt 8):1907-11.
26. Andreau K, Perfettini JL, Castedo M, and others. Contagious apoptosis facilitated by the HIV-1 envelope: fusion-induced cell-to-cell transmis-sion of a lethal signal. J Cell Sci 2004;117(Pt 23):5643-53.
27. Ahr B, Robert-Hebmann V, Devaux C, Biard-Piechaczyk M. Apop-tosis of uninfected cells induced by HIV envelope glycoproteins. Retrovirology 2004;1:12.
28. Piatak M, Saag MS, Yang LC, and others. High levels of HIV-1 in plasma during all stages of infection determined by competitive PCR. Science 1993;259:1749-54.
29. Daar ES, Moudgil T, Meyer RD, and others. Transient high levels of viremia in patients with primary human immunodeficiency virus type 1 infection. N Engl J Med 1991;324:961-4.
30. Altfeld M, Walker B. Acute HIV-1 Infection. In: Hoffmann C, Rockstroh JK, Kamps BS, eds. HIV Medicine 2005. Flying Pub-lisher:2005;33-41.
31. Phillips AN. CD4 lymphocyte depletion prior to the development of AIDS. AIDS 1992;6:735-6.
32. CDC data: HIV and AIDS case definitions. Available from http://www.cdc.gov/epo/dphsi/casedef/case_definitions.htm. Accessed 2006 Jan 16.
33. CDC data. 1993 Revised classification system for HIV infection and expanded surveillance case definitions for AIDS among adolescents and adults. Available from http://www.cdc.gov./mmwr/preview/mmwrhtml/00018871.htm. Accessed 2005 Nov 5.
34. Hoffmann C, Mulcahy F. ART 2005. In: Hoffmann C, Rockstroh JK, Kamps BS, eds. HIV Medicine 2005. Flying Publisher; 2005:85-263.
35. FDA data: drugs used in the treatment of HIV infection. Available from http://www.fda.gov/oashi/aids/virals.html. Accessed 2006 Jun 4.
36. Shafer RW. Genotypic testing for human immunodeficiency virus type 1 drug resistance. Clin Microbiol Rev 2002;15:247-77.
37. Schieferstein C, Buhk T. Management of side effects. In: Hoffmann C, Rockstroh JK, Kamps BS, eds. HIV Medicine 2005. Flying Publisher; 2005:263-82.
38. Ross L, Lim M, Liao Q, and others. Prevalence of antiretroviral drug resistance and resistance mutations in antiretroviral therapy (ART)
naïve HIV infected individuals. Abstract H-173, ICAAC 2004, Washington, DC, USA. Available at: http://www.natap.org/2004/ICAAC/icaac_10.htm. Accessed 2006 Jan 8.
39. Wolf E. HIV Resistance Testing. In: Hoffmann C, Rockstroh JK, Kamps BS, eds. HIV Medicine 2005. Flying Publisher; 2005:311-30.
40. Gallant JE. Antiretroviral drug resistance and resistance testing. Top HIV Med 2005 2006;13:138-42.
41. Mansky LM. Retrovirus mutation rates and their role in genetic variation. J Gen Virol 1998:79;1337-45.
42. Napravnik S, Edwards D, Stewart P, and others. HIV-1 drug resis-tance evolution among patients on potent combination antiretroviral therapy with detectable viremia. J Acquir Immune Defic Syndr 2005;40:34-40.
43. Hsiou Y, Ding J, Das K, and others. The Lys103Asn mutation of HIV-1 RT: a novel mechanism of drug resistance. J Mol Biol 2001:309;437-45.
44. Sluis-Cremer N, Tachedjian G. Modulation of the oligomeric struc-tures of HIV-1 retroviral enzymes by synthetic peptides and small molecules. Eur J Biochem 2002;269:5103-11.
45. Svicher V, Ceccherini-Silberstein F, Erba F, and others. Novel hu-man immunodeficiency virus type 1 protease mutations potentially involved in resistance to protease inhibitors. Antimicrob Agents Chemother 2005;49:2015-25.
46. Johnson VA, Brun-Vezinet F, Clotet B, and others. Update of the drug resistance mutations in HIV-1: 2004. Top HIV Med 2004;12:119-24.
47. Petropoulos CJ, Parkin NT, Limoli KL, and others. A novel pheno-typic drug susceptibility assay for human immunodeficiency virus type 1. Antimicrob Agents Chemother 2000;44:920-8.
48. Hertogs K, de Bethune MP, Miller V, and others. A rapid method for simultaneous detection of phenotypic resistance to inhibitors of protease and reverse transcriptase in recombinant human immunode-ficiency virus type 1 isolates from patients treated with antiretroviral drugs. Antimicrob Agents Chemother 1998;42:269-76.
49. Ross L, Boulme R, Fisher R, and others. A direct comparison of drug susceptibility to HIV type 1 from antiretroviral experienced subjects as assessed by the antivirogram and PhenoSense assays and by seven resistance algorithms. AIDS Res Hum Retroviruses 2005;21:933-9.
50. Zhang J, Rhee SY, Taylor J, and others. Comparison of the precision and sensitivity of the antivirogram and phenosense HIV drug sus-ceptibility assays. J Acquir Immune Defic Syndr 2005;38:439-44.
51. Wang K, Samudrala R, Mittler JE. Antivirogram or phenosense: a comparison of their reproducibility and an analysis of their correla-tion. Antivir Ther 2004;9:703-12.
52. Wang K, Samudrala R, Mittler J. Weak agreement between Antivi-rogram and Phenosense assays in predicting reduced susceptibility to antiretroviral drugs. J Clin Microbiol 2004;42:2353-4.
53. Richman DD. Benefits and limitations of testing for resistance to HIV drugs. J Antimicrob Chemother 2004;53:555-7.
54. Panidou ET, Trikalinos TA, Ioannidis JP. Limited benefit of an-tiretroviral resistance testing in treatment-experienced patients: a meta-analysis. AIDS. 2004;18:2153-61.
55. Dunn DT, Green H, Loveday C, and others. Evaluation of resistance assays (ERA) trial investigators. A randomized controlled trial of the value of phenotypic testing in addition to genotypic testing for HIV drug resistance: evaluation of resistance assays (ERA) trial investiga-tors. J Acquir Immune Defic Syndr 2005;38:553-9.
56. FDA data: Licensed/approved HIV, HTLV, and hepatitis tests. Centers
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 245
1 protease and reverse transcriptase sequencing of plasma samples from heavily treated patients. J Clin Microbiol 2001;39:1522-9.
69. Fontaine E, Riva C, Peeters M, and others. Evaluation of two com-mercial kits for the detection of genotypic drug resistance on a panel of HIV type 1 subtypes A through J. J Acquir Immune Defic Syndr 2001;28:254-8.
70. Beddows S, Galpin S, Kazmi SH, and others. Performance of two commercially available sequence-based HIV-1 genotyping systems for the detection of drug resistance against HIV type 1 group M subtypes. J Med Virol 2003;70:337-42.
71. Jagodzinski LL, Cooley JD, Weber M, and others. Performance characteristics of human immunodeficiency virus type 1 (HIV-1) genotyping systems in sequence-based analysis of subtypes other than HIV-1 subtype B. J Clin Microbiol. 2003;41:998-1003.
72. Galli R, Wynhoven B, Harrigan P, and others. Results from the first Canadian national HIV resistance testing external quality assessment panel. Abstract 114, CAHR 2003, Halifax, Canada. Available from http://www.cahr-acrv.ca/english/resources/abstracts_2003/abs/abs114.htm. Accessed 2006 Feb 3.
73. Huang D, Brambilla D, Ouma A, and others. Variability in quality assessment data from replicate genotyping of clinical samples. Abstract 584. 10th CROI; 2003; Boston, MA. Available from http://www.retro-conference.org/2003/cd/Abstract/584.htm.Accessed 2006 Feb 3.
74. Gale HB, Kan VL, Shinol RC. Performance of the TruGene human immunodeficiency virus type 1 genotyping kit and OpenGene DNA sequencing system on clinical samples diluted to approximately 100 Copies per milliliter. Clin Vaccine Immunol 2006;13:235-8.
75. Tural C, Ruiz L, Holtzer C, and others. Havana Study Group. Clini-cal utility of HIV-1 genotyping and expert advice: the Havana trial. AIDS 2002;16:209-18.
76. Baxter JD, Mayers DL, Wentworth DN, and others. A randomized study of antiretroviral management based on plasma genotypic an-tiretroviral resistance testing in patients failing therapy. CPCRA 046 study team for the Terry Beirn Community Programs for Clinical Research on AIDS. AIDS. 2000;14(9):F83-93.
77. Durant J, Clevenbergh P, Halfon P, and others. Drug-resistance ge-notyping in HIV-1 therapy: the VIRADAPT randomised controlled trial. Lancet. 1999;353:2195-9.
78. Hirsch HH, Drechsler H, Holbro A, and others. Genotypic and phenotypic resistance testing of HIV-1 in routine clinical care. Eur J Clin Microbiol Infect Dis 2005;24:733-8.
79. Evaluation of Resistance Assays (ERA) Trial Investigators. A random-ized controlled trial of the clinical utility of genotypic resistance testing in patients with limited prior exposure to antiretroviral drugs. HIV Clin Trials 2005;6:183-6.
80. Sax PE, Islam R, Walensky RP, and others. Should resistance testing be performed for treatment-naive HIV-infected patients? A cost-ef-fectiveness analysis. Clin Infect Dis 2005;41:1316-23.
81. Hecht FM, Grant RM. Resistance testing in drug-naive HIV-infected patients: is it time? Clin Infect Dis 2005;41:1324-5.
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
for Biological Evaluation and Research. Available from http://www.fda.gov/cber/products/testkits.htm. Accessed 2006 Jan 3.
57. Tsongalis GJ, Gleeson T, Rodina M, and others. Comparative performance evaluation of the HIV-1 LiPA protease and reverse transcriptase resistance assay on clinical isolates. J Clin Virol 2005;34:268-71.
58. Servais J, Lambert C, Fontaine E, and others. Comparison of DNA sequencing and a line probe assay for detection of human immunode-ficiency virus type 1 drug resistance mutations in patients failing highly active antiretroviral therapy. J Clin Microbiol 2001;39:454-9.
59. Erali M, Page S, Reimer LG, Hillyard DR. Human immunodeficiency virus type 1 drug resistance testing: a comparison of three sequence-based methods. J Clin Microbiol 2001;39:2157-65.
60. Eshleman SH, Hackett J Jr, Swanson P, and others. Performance of the Celera Diagnostics ViroSeq HIV-1 genotyping system for sequence-based analysis of diverse human immunodeficiency virus type 1 strains. J Clin Microbiol 2004;42:2711-7.
61. Maes B, Schrooten Y, Snoeck J, and others. Performance of ViroSeq HIV-1 genotyping system in routine practice at a Belgian clinical laboratory. J Virol Methods 2004;119:45-9.
62. Sturmer M, Berger A, Doerr HW. Modifications and substitutions of the RNA extraction module in the ViroSeq HIV-1 genotyping system version 2: effects on sensitivity and complexity of the assay. J Med Virol 2003;71:475-9.
63. Mracna M, Becker-Pergola G, Dileanis J, and others. Performance of Applied Biosystems ViroSeq HIV-1 genotyping system for sequence-based analysis of non-subtype B human immunodeficiency virus type 1 from Uganda. J Clin Microbiol 2001;39:4323-7.
64. Cunningham S, Ank B, Lewis D, and others. Performance of the Applied Biosystems ViroSeq human immunodeficiency virus type 1 (HIV-1) genotyping system for sequence-based analysis of HIV-1 in pediatric plasma samples. J Clin Microbiol 2001;39:1254-7.
65. Kuritzkes DR, Grant RM, Feorino P, and others. Performance charac-teristics of the TRUGENE HIV-1 Genotyping Kit and the Opengene DNA Sequencing System. J Clin Microbiol 2003;41:1594-9.
66. Grant RM, Kuritzkes DR, Johnson VA, and others. Accuracy of the TRUGENE HIV-1 genotyping kit. J Clin Microbiol 2003;41:1586-93.
67. Eshleman SH, Crutcher G, Petrauskene O, and others. Sensitivity and specificity of the ViroSeq human immunodeficiency virus type 1 (HIV-1) genotyping system for detection of HIV-1 drug resistance mutations by use of an ABI PRISM 3100 genetic analyzer. J Clin Microbiol 2005;43:813-7.
68. Shafer RW, Hertogs K, Zolopa AR, and others. High degree of in-terlaboratory reproducibility of human immunodeficiency virus type

246 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
Continuing Education Questions
FALL 2006
To receive 2.0 contact hours of intermediate level P.A.C.E.® credit for the Focus: Human Immunodeficiency Virus ques-tions, insert your answers in the appropriate spots on the continuing education registration form that follows, then mail a photocopy of the form as directed.
LEARNING OBJECTIVES 1. Describe the main genetic properties of the human im-
munodeficiency virus (HIV). 2. Describe the major events in the life cycle of HIV. 3. Identify the primary functions of each of the following
viral proteins: gp120, gp41, reverse transcriptase, inte-grase, protease.
4. List the three major stages in the natural course of the HIV infection.
5. Describe the changes in the viral loads and the CD4 counts during the natural course of the HIV disease.
6. List the four FDA-approved classes of antiretroviral drugs and identify the molecular targets of therapy for each class.
7. Describe benefits and limitations of antiretroviral therapy. 8. Describe the mechanisms of resistance in each of the
four FDA-approved classes of antiretroviral drugs. 9. List the two fundamental approaches to HIV drug re-
sistance testing.10. Describe the principles of phenotypic resistance testing
and list the main steps of the testing process.11. Define IC50 and calculate the X-fold reduction in sus-
ceptibility using the IC50 values.12. Describe the principles of sequencing-based genotypic resis-
tance testing and list the main steps of the testing process.13. Describe the principles of dideoxynucleotide sequencing.14. Describe the principles and the limitations of hybridiza-
tion-based resistance assays.15. Discuss the clinical utility of HIV drug resistance testing.
CONTINUING EDUCATION QUESTIONS 1. Which of the following is an accurate description of the
genetic properties of HIV?a. HIV is an RNA virus capable of converting its
genetic material to DNA.b. HIV is a DNA virus with high affinity for endothe-
lial cells and B-lymphocytes.
c. HIV is an RNA virus with extremely stable and conserved genome of 500 kilobases.
d. HIV is a DNA virus replicating with an error rate of 0.1 mistake per base per replication cycle.
2. Viral enzymes reverse transcriptase, protease, and integrase are transcribed from which of the following genes?a. Gagb. Polc. Envd. Rev
3. During the life cycle of HIV, the gp160 precursor protein is cleaved to form:a. p24, p17, gp118.b. gp60 and p100.c. gp90 and p70.d. gp120 and gp41.
4. The primary role of the protease in the life cycle of HIV is to:a. integrate the provirus into the host genome.b. interact with the CD4 receptor initiating the mem-
brane fusion.c. form the functional proteins of HIV by cleaving the
inactive precursors.d. regulate the transcription of the HIV genes.
5. The three main stages in the natural course of the HIV disease are:a. reverse transcription, clinical latency, AIDS.b. reverse transcription, transcriptional latency, AIDS.c. acute infection, clinical latency, AIDS.d. acute infection, membrane fusion, AIDS.
6. Which of the following laboratory findings would lead to the diagnosis of AIDS according to the CDC criteria?a. CD4 count 150 cells/μL, viral load 5,000,000
copies/mLb. CD4 count 280 cells/μL, viral load 10,000,000
copies/mLc. CD4 count 350 cells/μL, viral load 500,000 copies/mLd. CD4 count 800 cells/μL, viral load 100 copies/mL

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 247
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
7. The four FDA-approved classes of antiretroviral drugs are:a. nucleoside analogue reverse transcriptase inhibi-
tors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), RNA polymerase inhibitors, integrase inhibitors.
b. nucleoside analogue reverse transcriptase inhibi-tors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), protease inhibitors, fusion inhibitors.
c. nucleoside analogue reverse transcriptase inhibitors (NRTIs), gp120 inhibitors, protease inhibitors, acetylcholinesterase inhibitors.
d. nucleoside analogue reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhib-itors (NNRTIs), protease inhibitors, neuraminidase inhibitors.
8. Which of the following viral proteins is the primary target for the cytidine analogues, lamivudine, zalcitabine, and emtricitabine?a. Reverse transcriptaseb. Proteasec. Integrased. Gp41
9. All of the following are benefits of highly active antiret-roviral therapy (HAART), EXCEPT:a. lower viral loads.b. higher CD4 counts.c. reversed or delayed progression to AIDS.d. absence of serious side effects and long term toxicities.
10. The two main biochemical mechanisms leading to NRTI (nucleoside analogue reverse transcriptase inhibitor) resistance are:a. sterical inhibition and primer unblocking.b. sterical inhibition and ritonavir boosting.c. primer unblocking and substitutions in the HR1
domain of gp41.d. substrate cleft and flap region substitutions in the
protease.
11. K103N mutation is primarily associated with resistance to: a. nucleoside analogue reverse transcriptase inhibitors.b. non-nucleoside reverse transcriptase inhibitors.c. protease inhibitors.d. integrase inhibitors.
12. The two fundamental approaches to HIV drug resistance testing are:a. genotypic testing and Western Blot.b. genotypic testing and karyotyping.c. genotypic testing and phenotypic testing.d. phenotypic testing and Western Blot.
13. HIV RNA extraction, reverse transcription, amplification, recombinant vector preparation, and quantitative assess-ment of viral replication in cell culture are steps of:a. genotypic resistance testing.b. phenotypic resistance testing.c. resistance testing by reverse hybridization.d. resistance testing by karyotyping.
14. IC50 may be defined as:a. the concentration of the drug that results in a 50% inhibition of viral growth.b. the concentration of the drug that results in a 50% increase in the CD4 counts.c. the concentration of the drug that reduces the chance
of progression to AIDS within one year by 50%.d. the concentration of the drug that reduces the inci-
dence of primary resistance mutations by 50%.
15. If the IC50 of the wild-type virus is 2 mg/mL and the IC50 of the patient’s isolate is 6 mg/mL, then the X-fold reduction in susceptibility will be reported as:a. 3-fold resistance.b. 4-fold resistance.c. 8-fold resistance.d. 12-fold resistance.
16. HIV RNA extraction, reverse transcription, amplifica-tion, dideoxynucleotide sequencing, and algorithmic interpretation of the sequencing data are steps of: a. phenotypic resistance testing.b. genotypic resistance testing.c. resistance testing by karyotyping.d. resistance testing by Western Blot.
17. A double peak appears on the electrophoretogram during the process of dideoxynucleotide sequencing when:a. a mixture of two nucleotides is detected at a specific
position.b. a single wild-type nucleotide is detected at position
103 of reverse transcriptase.c. the M184V mutation is detected in the patient’s isolate.

248 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
d. a single nucleotide substitution is detected at a resistance-associated position in the protease.
18. During the process of dideoxynucleotide sequencing, which of the following procedures is used to arrange the DNA strands in the order of increasing length?a. Radial immunodiffusionb. Polyacrylamide gel electrophoresisc. Reverse transcriptase polymerase chain reaction
(RT-PCR)d. Western Blot
19. Resistance testing by reverse hybridization involves:a. synthesis of new DNA strands complementary to
the target sequence of interest in the presence of labeled chain terminators.
b. determination of IC50 for the patient’s isolate and the wild-type virus.
FOCUS: HUMAN IMMUNODEFICIENCY VIRUS
c. binding of the amplified biotinylated DNA material to codon-specific oligonucleotide probes.
d. preparation of RT-PR deficient vectors.
20. The clinical utility of HIV drug resistance testing has been evaluated in a number of studies with the following results (select the correct answer).a. All studies demonstrated the benefit of resistance
testing.b. All studies failed to demonstrate the benefit of re-
sistance testing.c. Some studies demonstrated the benefit of resistance
testing while other studies failed to demonstrate the benefit of resistance testing.
d. All studies demonstrated the benefit of phenotypic resistance testing but failed to demonstrate the ben-efit of genotypic resistance testing.
Clinical Laboratory ScienceAnnounces 2005 Distinguished Author Award Recipients
Recipients of the Clinical Laboratory Science Distinguished Author Awards are chosen by Clinical Laboratory Science editorial board members. Nominations are based upon based on originality and quality of writing, relevance to the laboratory science profession, and integration of theory and application. The editorial board of Clinical Laboratory
Science is pleased to announce the following recipients of the 2005 Distinguished Author Awards.
Clinical PracticeBobbi Dock, for her article Improving the Accuracy of Specimen Labeling,
published in the Fall 2005 issue of Clinical Laboratory Science.
Research and Reports Heidi Andersen, for her article Children on the Frontline against E.coli: Typical Hemolytic-Uremic Syndrome,
published in the Spring 2005 issue of Clinical Laboratory Science.
FocusTim R Randolph, for his article Chronic Myelocytic Leukemia - Part I: History, Clinical Presentation,
and Molecular Biology, published in the Winter 2005 issue of Clinical Laboratory Science.

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 249
To earn continuing education (PACE) credit, (1) complete the form below, (2) record your answers, and (3) mail a photocopy with a check or money order ($18 for ASCLS members, $28 for non-members) to:
American Society for Clinical Laboratory ScienceP.O. Box 79154, Baltimore MD 21279-0154
A certificate of completion will be awarded to participants who achieve a passing grade of 70% or better. Participants should allow eight weeks for notification of scores and receipt of certificates.
Focus: Human Immunodeficiency Virus carries 2.0 hours of intermediate level P.A.C.E.® credit. This form can be submitted for credit for up to one year from the date of issue.
Print or type carefully.
(01) NAME ______________________________________________________________________________________________ irst M.I.
ASCLS membership number __________________________________ Licensure number ______________________________
(02) ADDRESS __________________________________________________________________________________________
(03) CITY________________________(04) STATE/COUNTRY _____________(05) ZIP/POSTAL CODE_________________
(06) DAYTIME PHONE ( ______ )__________________________(07) E-MAIL:______________________________________
(08) CREDIT CARD # _____________________________ TYPE (CIRCLE) AE MC VIS EXP. DATE_____________
Continuing Education Registration Form
Check all that apply
❑ Send my certificate of completion via email❑ I would like to receive ASCLS membership information❑ I would like information on other continuing education sources
AnswersCircle correct answer.
Participant Information Please circle the most appropriate answers.
1. Is this program used to meet your CE requirements for: (a) state license (b) NCA (c) employment (d) other
2. Did these articles achieve their stated objectives? (a) yes (b) no
3. How long did it take you to complete both the reading and the quiz? ___________minutes
4. What subjects would you like to see addressed in future Focus articles?
1. a b c d2. a b c d3. a b c d4. a b c d5. a b c d6. a b c d7. a b c d8. a b c d9. a b c d10. a b c d
11. a b c d12. a b c d13. a b c d14. a b c d15. a b c d16. a b c d17. a b c d18. a b c d19. a b c d20. a b c d

250 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
Electronic Media Review
JAMES T GRIFFITH
Image Atlas SeriesinQUIZator SeriesIndiana Pathology Images; 2004, 2005http://www.ipimages.com
INDEX TERMS: clinical microbiology; electronic images; learning tools; review.
Each of the following five CD-ROMs is described to be for the express use of: educators (PowerPoint lectures, color im-ages for examinations, student laboratory manuals, intranet website postings); undergraduate, graduate, and medical students, residents, and fellows (intranet postings for review of lecture material, at-home review, printed ‘flash cards’ for national certification examination review); and practitioners (reference material, review material for continuing educa-tion credit, training and retraining of employees, images for laboratory procedure manuals).
IMAGE ATLAS SERIESBacteriology Image AtlasThis CD-ROM contains nearly 700 quality photomi-crographs. Each is clear and accessible. “Alphabetical”, “Grouping”, and “Tests” tabs allow the seamless movement from one way of searching to another. This reviewer ran the software through a Macintosh (Mac) SX environment and a Windows XP environment. While the Mac access was a bit more intuitive, both worked well. Indiana Pathology Images (IP) suggests that the CD has been designed to operate in MAC OSX v. 10.2-10.3 and Windows 95, 98, NT, 2000, and XP. There is also an Internet Explorer (5.0 and up) and Netscape operation. The operational modes are “RUN from CD-ROM”, simple for both environments, and “Internet RUN” which is optimal from PC environments only. It is not clear why this limitation exists.
The content is superb! Images exist for over 125 different or-ganisms ranging from Achromobacter xylosoxidans to Yersinia enterocolitica. Commonly identified organisms such as the En-terobacteriaceae are balanced with views of less frequently seen organisms such as Finegoldia magna and Mycobacterium phlei.
When you go to an organism, there are usually crystal-clear macroscopic and microscopic levels of images of that organ-ism to see. In addition, depending on the organism there
are likely to be 100mm petri dish views of the organism on appropriately different media. Close-up and/or stereoscopic views are included for many isolates. Stereoscopic examina-tion of anaerobic organisms is most useful in this level of visual recognition and the authors appear to have chosen this magnification as the opening image for viewing all anaerobe isolates. The photographed isolates all appear to have been incubated until colony morphology was well established.
When the organisms are grouped, they end up in these cate-gories: aerobes: Gram negative cocci (GNC), four subcatego-ries of Gram negative rods (GNR); anaerobes: GNC, GNR, GPC, GPR, and GPR, spore-forming; and mycobacteria. The term “rods”, which while common, is still not correct and this reviewer hopes that in the later versions (Bacteriology II, etc.) this will be corrected to “B” (bacilli).
There is also a category for tests in the following categories: biochemical and other tests, aerobes, anaerobes, mycobac-teria, and susceptibilities. There are over 80 tests in the aerobes category alone, ranging from Bacitracin susceptibil-ity to XV factor requirement(s). There are four versions of motility testing. Each has an appropriately photographed representation of POS and (in many cases) NEG versions of the test at hand.
Parasitology Image AtlasThis CD-ROM contains over 600 quality photomicrographs. Each is clear and accessible. “Classification” and “Grouping” tabs allow the seamless movement from one way of searching to another. This reviewer ran the software through a Mac OSX environment and a Windows XP environment. While the Mac access was a bit more intuitive, both worked well. IP suggests that the CD has been designed to operate in Mac OSX v. 10.2-10.3 and Windows 95, 98, NT, 2000, and XP. There is also an Internet Explorer (5.0 and up) operation. The operational modes are “RUN from CD-ROM”, simple for both environments, and “Internet RUN” which is op-timal from PC environments only. It is not clear why this limitation exists.
Again the content is superb!! Images exist for over sixty organisms ranging from Acanthamoeba species to Wuchereria bancrofti. The images can be searched in categories entitled arthropods, ces-todes, nematodes, protozoa, pseudoparasites, and trematodes

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 251
Each image typically has various magnifications (x 100, 500, 1,000, etc.) as appropriate, as well as the organism viewed in various stains (Giemsa, Trichrome, wet prep, H&E, etc.) as appropriate and various stages (ovum, trophozoite, adult, microfilaria) as appropriate.
Mycology Image AtlasThis CD-ROM contains over 600 quality photomicrographs. Each is clear and accessible. “Classification” and “Grouping” tabs allow the seamless movement from one way of searching to another. This reviewer ran the software through a Mac OSX environment and a Windows XP environment. While the Mac access was a bit more intuitive, both worked well. IP suggests that the CD has been designed to operate in MAC OSX v. 10.2-10.3 and Windows 95, 98, NT, 2000 and XP. There is also an Internet Explorer (5.0 and up) operation. The operational modes are “RUN from CD-ROM”, simple for both environments, and “Internet RUN” which is op-timal from PC environments only. It is not clear why this limitation exists.
The content is the same quality as the other sections. Images exist for over 75 organisms ranging from Absidia species to Ulocladium species. The images can be searched in the following categories: algae, dematiaceous fungi, derma-tophytes, dimorphic fungi, filamentous bacteria, hyaline fungi, pneumocystis, yeast and yeast-like organisms, and the zygomycetes. Each image typically has various magnifications (x 100, 400, 1,000, etc.) as appropriate, as well as the organ-ism viewed after various stains (LPCB, GMS, H&E, etc.) as appropriate. The images also typically include various views (obverse, reverse) as appropriate and as grown on various media (SDA, PDA, BHI, CMA, etc.) as appropriate.
INQUIZATOR SERIESinQUIZator: Mycology Containing a review bank, self-test, and laboratory compe-tency test, this CD-ROM does not operate in a Mac environ-ment at all. No explanation for this shortfall is available.
Choices can be made for classification, chapter headings (lab procedures, identification, habitat, etc.), or alphabetical listing by organism name. The review module also offers a randomized self-test. The competency test module allows the
user to take a randomized test selected from a bank of ques-tions with images that will assess the user’s ability to identify parasites. After completion of the self-test or competency test, a certificate can be printed that includes the user’s name, date, and test results. This certificate can be used to docu-ment competency for laboratory personnel or students (and presumably other health care professionals as well).
inQUIZator: ParasitologyContaining a review bank, self-test, and Laboratory Compe-tency test, this CD-ROM does not operate in a MAC environ-ment at all. No explanation for this shortfall is available.
Choices can be made for Classification, Chapter headings (lab procedures, identification, habitat, etc.), or Alphabetical listing by organism name. The review module also offers a randomized self-test. The competency test module allows the user to take a randomized test selected from a bank of ques-tions with images that will assess the user’s ability to identify parasites. After completion of the self-test or competency test, a certificate can be printed that includes the user’s name, date, and test results. This certificate can be used to docu-ment competency for laboratory personnel or students (and presumably other health care professionals as well).
SUMMARYAll in all, these products represent by scope, quality, and with the exception of the inQUIZator items, ease of use major resources for clinical laboratory professionals needing to il-lustrate microorganisms. The Indiana Pathology Images web site (www.ipimages.com) suggests future titles will include the following.
Image Atlas Series: Anaerobe Morphology; Cytology; Hematol-ogy; Histology; Infectious Disease Pathology; Renal Pathology; Virology.
inQuizator Series: Bacteriology; Cytology; Histology.
James T Griffith PhD CLS(NCA), Chancellor Professor and Chairperson, Department of Medical Laboratory Science, Uni-versity of Massachusetts, 285 Old Westport Road, Dartmouth MA 02747-2300. (508) 999-8328, (508) 999-8418 (fax). [email protected].
MEDIA REVIEW

252 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
2006 INDEX
Annual Index
INDEX TO VOLUME 19, NUMBERS 1 THROUGH 4
The index to volume 19 of Clinical Laboratory Science is composed of two parts: an Author Index and a Subject Index (p 256).
Issue PagesJanuary – March 1 – 64April – June 65 – 128July – September 129 – 192October – December 193 – 256Abbreviations:AB = AbstractBR = Book ReviewCP = Clinical PracticeDD = Dialogue and DiscussionFO = FocusRR = Research and ReportsWB = Washington Beat
AUTHOR INDEX
Accurso, Charity Einhaus The Incorporation of Student Support in
Distance Learning Course Structure. 92. ABAdams, Cynthia A Comparison of Learning Styles of Allied
Health Students. 90. ABAl Qaddoumi, Ayman A Co-inheritance of α and β-Thalassemia in a
Jordanian Family. 165. RRArenson, Wendy L Conversion of Existing Clinical Chemistry
Web-based Materials into Sharable Learning Objects. 97. AB
Ashley, Stephanie Interdisciplinary Healthcare Training: Bridg-
ing Clinical Laboratory Science, Genetic Counseling, and Physical Therapy. 97. AB
Overcoming Obstacles to Incorporate In-terdisciplinary Curriculum into a Graduate Laboratory Science Program. 159. AB
Aziz, Hassan Health Professions Workforce Partnership
Can Be the Answer. 154. AB Baldwin, Tamara Methicillin-resistant Staphylococcus aureus in
a Texas County Jail. 154. AB
Beason, Kevin β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Beck, Linda C A “Proficiency Assessment Process” for Clini-
cal Hematologists. 159. ABBehan, Kristina Jackson Cessation of Menstruation Improves the
Correlation of FPG to Hemoglobin A1c in Caucasian Women. 225. RR
Behm, Kylie J Breezing Up – An Interdisciplinary Health
Professions Course for High School Juniors and Seniors and College Freshman. 112. FO
Black, Angelica Antiphospholipid Syndrome: An Overview.
144. CPBrickell, Jean Student Information Management for Dum-
mies. 98. AB Learning Objects: Resources for Instruction.
184. FO Bright, Cynthia β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Britton, Lynda Investigation of Knowledge and Attitudes
of African American High School Students toward Clinical Laboratory Science. 159. AB
Brodeur, Lynne Teaching Techniques to Increase First Year
Success. 95. ABBruce, A Wayne Breezing Up – An Interdisciplinary Health
Professions Course for High School Juniors and Seniors and College Freshman. 112. FO
Bryant, Sabrina β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Cagle, Henry Hepatitis A Prevalence among Injection
Drug Users. 12. RRCarreiro-Lewandowski, Eileen Nutritional Assessment of Alzheimer’s
Patients Using Homocysteine, Folate, and Transthyretin Levels: Laboratory Identifica-tion of Alzheimer’s Disease. 155. AB
Caskey, Cheryl R The Rule of Law and Bioterrorism. 196. DDChang, G Andy Are Quality Laboratory Services Related to
Personnel Credentials? 153. ABChen, Michael Are Different Tests of Platelet Function Com-
parable When Taking Aspirin? 156. AB Urinary 11-dehydrothromboxane B2 Levels
in Healthy Individuals Following a Single Dose Response to Two Concentrations of Aspirin. 160. AB
Cheung, SW Improved Rapid Fluorescent In Situ Hybrid-
ization Protocol for Testing of Newborns for Possible Chromosomal Aneuploidy. 158. AB
Childs, Cherry Twelve Month, Second Degree Track in
Medical Technology. 95. ABClinton, Shawn β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Coleman, Faye E Evaluation of an On-campus Blood Bank
Clinical Practicum Course. 91. ABCooksey, Wileen β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Correiro, Elizabeth Teaching Techniques to Increase First Year
Success. 95. ABCrowell, Rasheeda β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Davis, Judy United States Government Accountability
Office (GAO) Targets Laboratory Quality. 194. WB
DeLany, Shannon Interdisciplinary Healthcare Training: Bridg-
ing Clinical Laboratory Science, Genetic Counseling, and Physical Therapy. 97. AB
Overcoming Obstacles to Incorporate In-terdisciplinary Curriculum into a Graduate Laboratory Science Program. 159. AB
Delost, Maria D Are Quality Laboratory Services Related to
Personnel Credentials? 153. AB

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 253
Dobbs M Are Different Tests of Platelet Function Com-
parable When Taking Aspirin? 156. AB Urinary 11-dehydrothromboxane B2 Levels
in Healthy Individuals Following a Single Dose Response to Two Concentrations of Aspirin. 160. AB
Doucette, Lorraine Interdisciplinary Healthcare Training: Bridg-
ing Clinical Laboratory Science, Genetic Counseling, and Physical Therapy. 97. AB
Overcoming Obstacles to Incorporate In-terdisciplinary Curriculum into a Graduate Laboratory Science Program. 159. AB
Eckert, Barry Health Professions Workforce Partnership
Can Be the Answer. 154. ABEsparza, Yvette Transfusion-related Bacterial Sepsis. 155. ABFelkner, Marilyn Methicillin-resistant Staphylococcus aureus in
a Texas County Jail. 154. ABFenaughty, Andrea Hepatitis A Prevalence among Injection
Drug Users. 12. RRFincher, Emily Validating the Assessment of Glucose-6-Phos-
phate Dehydrogenase (G6PD). 134. CPFinley, Jane B Student Information Management for Dum-
mies. 98. ABFisher, Dennis Hepatitis A Prevalence among Injection
Drug Users. 12. RRFlaws, Maribeth National Tuberculosis Curriculum Consor-
tium. 94. ABFlowers, Heather W Antibiotic Surveillance of Streptococcus pneu-
moniae in Mississippi. 5. CPFortenberry, Debbie β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Fortwendel, Jarrod The Incorporation of Student Support in Dis-
tance Learning Course Structure. 92. ABFranklin, Rosalind A Comparison of Learning Styles of Allied
Health Students. 90. ABFreeman, Vicki Conversion of Existing Clinical Chemistry
Web-based Materials into Sharable Learning Objects. 97. AB
Learning Objects: Resources for Instruction. 184. FO
Fritsma, George A NCA and BOR Consider New Credentialing
Agency. 132. DDGade, Wayne A Brief Survey of Aquaporins and Their
Implications for Renal Physiology. 70. CP CLS Meets the Aquaporin Family: Clinical
Cases Involving Aquaporin Systems. 80. CPGebert, Mark A Interpretation of Statistics in Clinical Labo-
ratory Studies 18. RRGideon, H Labiner The Incorporation of Student Support in Dis-
tance Learning Course Structure. 92. ABGocke, Christopher D Molecular Diagnostics of Hematological
Malignancies. 32. FOGolekboski, Karen A Implementation of an Integrated, Case-based
Course in Cell and Molecular Biology for Pre-clinical Laboratory Science and Pre-cytotechnology Students. 92. AB
Gordes, Karen Interdisciplinary Healthcare Training: Bridg-
ing Clinical Laboratory Science, Genetic Counseling, and Physical Therapy. 97. AB
Overcoming Obstacles to Incorporate In-terdisciplinary Curriculum into a Graduate Laboratory Science Program. 159. AB
Graeter, Linda J The Incorporation of Student Support in Dis-
tance Learning Course Structure. 92. ABGray, Jeffery R The Use of B-type Natriuretic Peptide to
Diagnose Congestive Heart Failure. 214. CPGriffin, Christine G Young Adults’ Perceptions of an Ideal Career
and a Career in Medical Laboratory Science. 160. AB
Griffith, James T Government 101: How an Idea Becomes
Law. 50. FO Government 103: What Happened to the
Great Idea? 54. FO Electronic Media Review. 250. BRGuiles, H Jesse Learning and Utilization of Generic Skills by
Practitioners in the Field of Clinical Labora-tory Science/Medical Technology. 104. RR
Guo, Mary β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Hall, Jeffrey M The Effect of Ozone on Common Environ-
mental Fungi. 157. ABHall, Margot β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
2006 INDEX
Hammami, Nasser Breezing Up – An Interdisciplinary Health
Professions Course for High School Juniors and Seniors and College Freshman. 112. FO
Hansen, Kathy Competitive Bidding. 2. WB Reimbursement Concerns. 66. WB Trends in Healthcare Payment. 130. WBHansen-Suchy, Kara Online Orientation: A Tool to Increase
Student Success. 97. ABHenderson, Ric Down Syndrome with Myelodysplasia of
Megakaryoblastic Lineage. 161. RRHendrix, Ericka Training Technologies for the Genomic Age.
148. CPHighsmith, Jr., W Edward Introduction to Molecular Cystic Fibrosis
Testing 24. FOHollifield, Kay β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Honeycutt, Karen Blended Learning in the Practice, Wet Labo-
ratory Learning Environment. 96. ABHovis, Karrie Investigation of Knowledge and Attitudes
of African American High School Students toward Clinical Laboratory Science. 159. AB
Hu, P Improved Rapid Fluorescent In Situ Hybrid-
ization Protocol for Testing of Newborns for Possible Chromosomal Aneuploidy. 158. AB
Hua, Helen β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Hubbard, Joel D Clinical Laboratory Science: A Profession
with Honors. 139. CP Introducing Clinical Laboratory Science: CLS
Students Help Shape the Future. 206. CPHuber, Fran Interdisciplinary Healthcare Training: Bridg-
ing Clinical Laboratory Science, Genetic Counseling, and Physical Therapy. 97. AB
Overcoming Obstacles to Incorporate In-terdisciplinary Curriculum into a Graduate Laboratory Science Program. 159. AB
Hudson, M Jane Managing a Clinical Laboratory Science Pro-
gram prior to, during, and after a Disaster. 93. AB
Irwin, David Investigation of Knowledge and Attitudes
of African American High School Students

254 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
toward Clinical Laboratory Science. 159. ABJackson, Margaret β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Jaffe, Adi Hepatitis A Prevalence among Injection
Drug Users. 12. RRJohnson James T β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Johnson, Sharae β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Josko, Deborah Diagnosis of Invasive Pulmonary Aspergil-
losis: Molecular vs. Culture. 157. ABKanuth, Michelle S Student Information Management for Dum-
mies. 98. AB Student Laboratories as a Component of a
Web-based Curriculum. 117. FO Learning Objects: Resources for Instruction.
184. FO Kasper, LM A Model for Educational Enrichment and
Employment Recruitment for Clinical Laboratory Science Students. 169. RR
Kay, Lisa W Interpretation of Statistics in Clinical Labo-
ratory Studies. 18. RRKelaher, Amy Two Non-invasive Diagnostic Tools for In-
vasive Aspergillosis: (1-3)-B-D-Glucan and the Galactomannan Assay. 222. CP
Khanna, Niharika Interdisciplinary Healthcare Training: Bridg-
ing Clinical Laboratory Science, Genetic Counseling, and Physical Therapy. 97. AB
Kirby, Beverly A An Introductory Pathology Course in a
Medical Technology Curriculum. 158. ABKnight, Z Are Different Tests of Platelet Function Com-
parable When Taking Aspirin? 156. AB Urinary 11-dehydrothromboxane B2 Levels
in Healthy Individuals Following a Single Dose Response to Two Concentrations of Aspirin. 160. AB
Korzun, William J Are Quality Laboratory Services Related to
Personnel Credentials? 153. AB The Effect of Ozone on Common Environ-
mental Fungi. 157. ABKoziatek, Vernon Validating the Assessment of Glucose-6-Phos-
phate Dehydrogenase (G6PD). 134. CPKraj, Barbara Status of Molecular Diagnostics Incorpora-
tion into Clinical Laboratory Science Curri-cula: Results of a National Survey. 94. AB
Larson, Carol Learning Objects: Resources for Instruction.
184. FOLatshaw, Sandra National Tuberculosis Curriculum Consor-
tium. 94. AB Learning Objects: Resources for Instruction.
184. FOLaudicina, Rebecca J Searching for Hereditary Hemochromatosis.
174. RRLavanty, Don Competitive Bidding. 2. WB Reimbursement Concerns. 66. WB Trends in Healthcare Payment. 130. WB United States Government Accountability
Office (GAO) Targets Laboratory Quality. 194. WB
Lawrence, Louann Managing a Clinical Laboratory Science Pro-
gram prior to, during, and after a Disaster. 93. AB
Investigation of Knowledge and Attitudes of African American High School Students toward Clinical Laboratory Science. 159. AB
Leclair, Susan “History is the Present”. 4. DD Federal Government Impact in the Clinical
Laboratory. 42. FOLehman, Sue Career Advancement for the Working Profes-
sional. 90. AB Industry and Education: The Categorical
Model of Learning. 93. ABLennon, PA Improved Rapid Fluorescent In Situ Hybrid-
ization Protocol for Testing of Newborns for Possible Chromosomal Aneuploidy. 158. AB
Levy, Howard Interdisciplinary Healthcare Training: Bridg-
ing Clinical Laboratory Science, Genetic Counseling, and Physical Therapy. 97. AB
Major, Charles Asowata Validating the Assessment of Glucose-6-Phos-
phate Dehydrogenase (G6PD). 134. CPManaceva, Slobodanka D β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
McCoy, Carol Writing Clinical Research Protocols: Ethical
Considerations. 60. BRMcGlasson, David L
2006 INDEX
Are Different Tests of Platelet Function Com-parable When Taking Aspirin? 156. AB
Urinary 11-dehydrothromboxane B2 Levels in Healthy Individuals Following a Single Dose Response to Two Concentrations of Aspirin. 160. AB
McGough, Ryan D The Incorporation of Student Support in Dis-
tance Learning Course Structure. 92. AB Diagnosis of Invasive Pulmonary Aspergil-
losis: Molecular vs. Culture. 157. ABMcKenzie, Shirlyn B Grade Inflation in Clinical Laboratory Sci-
ence. 153. ABMiller, W Greg Are Quality Laboratory Services Related to
Personnel Credentials? 153. ABMontoya, Isaac D Bioterrorism Defense and Its Impact on the
Clinical Laboratory. 68. DDMugan, Kathleen National Tuberculosis Curriculum Consor-
tium. 94. AB Twelve Month, Second Degree Track in
Medical Technology. 95. ABMundt, Lillian A Comparison of Learning Styles of Allied
Health Students. 90. AB Clinical Laboratory Sciences Curriculum
Re-development: An Application of Change Theories. 157. AB
Nadder, Teresa S Are Quality Laboratory Services Related to
Personnel Credentials? 153. ABNewsome, LP (Sky) Methicillin-resistant Staphylococcus aureus in
a Texas County Jail. 154. ABNielsen, Leonard Gary Teaching and Assessing New Method Verifi-
cation Skills Using Interactive Simulations. 188. FO
Palumbo, Mary Val Young Adults’ Perceptions of an Ideal Career
and a Career in Medical Laboratory Science. 160. AB
Parra, Kimberly Rainbow A “Proficiency Assessment Process” for Clini-
cal Hematologists. 159. ABPassiment, Elissa Regulatory Agencies Involved with the Clini-
cal Laboratory. 43. FOPatel, A Improved Rapid Fluorescent In Situ Hybrid-
ization Protocol for Testing of Newborns for Possible Chromosomal Aneuploidy. 158. AB
Paur, Ruth Career Advancement for the Working Profes-
sional. 90. AB

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 255
Industry and Education: The Categorical Model of Learning. 93. AB
Western College Alliance for Clinical Labo-ratory Science Education. 95. AB
Peterson, Karen Growth and Evolution of a Distance Educa-
tion Clinical Laboratory Science Program: One University’s Perspective. 91. AB
Western College Alliance for Clinical Labo-ratory Science Education. 95. AB
Porter, Robert Career Advancement for the Working Profes-
sional. 90. AB Industry and Education: The Categorical
Model of Learning. 93. ABPorter, Robert Growth and Evolution of a Distance Educa-
tion Clinical Laboratory Science Program: One University’s Perspective. 91. AB
Pretlow, Lester G Validating the Assessment of Glucose-6-
Phosphate Dehydrogenase (G6PD). 134. CP
Integrated Metabolism and Low Carbohy-drate Dieting. 158. AB
Randolph, Tim R Understanding of and Opinions about
Licensure for Laboratory Personnel among Laboratory Professionals in the United States. 155. AB
Ranne, Anne Future Challenges for Clinical Laboratory
Science Education. 91. ABRice-Spearman, Lori Clinical Laboratory Science: A Profession
with Honors. 139. CP Introducing Clinical Laboratory Science: CLS
Students Help Shape the Future. 206. CPRobinson, Brooke A Brief Survey of Aquaporins and Their
Implications for Renal Physiology. 70. CP CLS Meets the Aquaporin Family: Clinical
Cases Involving Aquaporin Systems. 80. CPRohde, Rodney E Methicillin-resistant Staphylococcus aureus in
a Texas County Jail. 154. ABSan Diego, Leticia J Medical Errors and Patient Safety: State Leg-
islation and Recommendations. 154. ABSato, Brendon LEAN: One Laboratory’s Solution. 93. ABSauer, Ronald L The Effect of Ozone on Common Environ-
mental Fungi. 157. ABSawyer, Barbara Clinical Laboratory Science: A Profession
with Honors. 139. CP Introducing Clinical Laboratory Science: CLS
Students Help Shape the Future. 206. CPSchill, Janna Growth and Evolution of a Distance Educa-
tion Clinical Laboratory Science Program: One University’s Perspective. 91. AB
Western College Alliance for Clinical Labo-ratory Science Education. 95. AB
Schultze, AE A Model for Educational Enrichment and
Employment Recruitment for Clinical Laboratory Science Students. 169. RR
Schultze, Harold β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Scosyrev, Emil An Overview of the Human Immunodefi-
ciency Virus Featuring Laboratory Testing for Drug Resistance. 231. FO
Shaw, Donna M Factor V Leiden: An Overview. 218. CPSimonian, Yasmen Advances and Innovations. 111. FOSims-Davis, Tammy β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Smith, Linda A Grade Inflation in Clinical Laboratory Sci-
ence. 153. AB Transfusion-related Bacterial Sepsis. 155. ABSmith, Toby L Student Information Management for Dum-
mies. 98. ABSolomon, Kathleen Understanding of and Opinions about
Licensure for Laboratory Personnel among Laboratory Professionals in the United States. 155. AB
Spence, Libby Down Syndrome with Myelodysplasia of
Megakaryoblastic Lineage. 161. RRSt John, E Camellia Student Laboratories as a Component of a
Web-based Curriculum. 117. FOStalewski, Susan Classroom Clicking for Enhanced Student
Learning. 96. ABSteinberg, Lisa Interdisciplinary Healthcare Training: Bridg-
ing Clinical Laboratory Science, Genetic Counseling, and Physical Therapy. 97. AB
Overcoming Obstacles to Incorporate In-terdisciplinary Curriculum into a Graduate Laboratory Science Program. 159. AB
Sullivan, Donna C Antibiotic Surveillance of Streptococcus pneu-
moniae in Mississippi. 5. CP
2006 INDEX
Sykes, Paul β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Szuflad, Paula M An Atypical Antibody Event. 156. ABTatum, Tootie Training Technologies for the Genomic Age.
148. CPThompson, Christina Importance of Patient History in Case with
Antibody to High Frequency Antigen. 155. AB
Diegoa Antigen Frequency and Anti-Diegoa
Frequency in a South Texas Community. 203. CP
Tompkins, Janice Career Advancement through Distance
Education Technology. 90. ABUphoff, Timothy S Introduction to Molecular Cystic Fibrosis
Testing 24. FOValle, Ana Marie Methicillin-resistant Staphylococcus aureus in
a Texas County Jail. 154. ABVan Asselt, Darla LEAN: One Laboratory’s Solution. 93. ABVanik, Janet A Comparison of Learning Styles of Allied
Health Students. 90. AB Clinical Laboratory Sciences Curriculum
Re-development: An Application of Change Theories. 157. AB
Vincent, Charles β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Ward-Cook, Kory Learning and Utilization of Generic Skills by
Practitioners in the Field of Clinical Labora-tory Science/Medical Technology. 104. RR
Weiner, Alan An Atypical Antibody Event. 156. ABWells, Rebecca Hepatitis A Prevalence among Injection
Drug Users. 12. RRWhitehurst, Anne Antibiotic Surveillance of Streptococcus pneu-
moniae in Mississippi. 5. CPWiggers, Thomas B Antibiotic Surveillance of Streptococcus pneu-
moniae in Mississippi. 5. CPWilson, Cynthia β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Wright, Scott PCR Laboratory Exercises for Clinical Mi-

256 VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE
crobiology Students. 94. ABYing, Jiarong β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Zundel, William B Bringing the Classroom Online: How to Set
Up and Maintain the Discussion Board Tool in Online CLS Courses. 96. AB
Interactivity: Key to CLS Online Instruction. 122. FO
SUBJECT INDEX
Accelerated degree Twelve Month, Second Degree Track in
Medical Technology. 95. ABα and β-thalassemia Co-inheritance of α and β-Thalassemia in a
Jordanian Family. 165. RRAlzheimer's Disease Nutritional Assessment of Alzheimer’s
Patients Using Homocysteine, Folate, and Transthyretin Levels: Laboratory Identifica-tion of Alzheimer’s Disease. 155. AB
Antibodies An Atypical Antibody Event. 156. AB Importance of Patient History in Case with
Antibody to High Frequency Antigen. 155. AB
Antigens Diegoa Antigen Frequency and Anti-Diegoa
Frequency in a South Texas Community. 203. CP
Antiphospholipid syndrome Antiphospholipid Syndrome: An Overview.
144. CPAquaporins A Brief Survey of Aquaporins and Their
Implications for Renal Physiology. 70. CP CLS Meets the Aquaporin Family: Clinical
Cases Involving Aquaporin Systems. 80. CPAspergillosis Two Non-invasive Diagnostic Tools for In-
vasive Aspergillosis: (1-3)-B-D-Glucan and the Galactomannan Assay. 222. CP
Aspirin (ASA) Are Different Tests of Platelet Function Com-
parable When Taking Aspirin? 156. AB Urinary 11-dehydrothromboxane B2 Levels
in Healthy Individuals Following a Single Dose Response to Two Concentrations of Aspirin. 160. AB
β-2-microglobulin β-2-Microglobulin Compared with Thirteen
Other Tumor Antigens for the Serodiagnosis of Pancreatic Cancer. 156. AB
Bioterrorism
Bioterrorism Defense and Its Impact on the Clinical Laboratory. 68. DD
The Rule of Law and Bioterrorism. 196. DDB-type natriuretic peptide The Use of B-type Natriuretic Peptide to
Diagnose Congestive Heart Failure. 214. CPCareer advancement Career Advancement for the Working Profes-
sional. 90. AB Career Advancement through Distance
Education Technology. 90. ABCareer patterns Learning and Utilization of Generic Skills by
Practitioners in the Field of Clinical Labora-tory Science/Medical Technology. 104. RR
Chromosomal aneuploidy testing Improved Rapid Fluorescent In Situ
Hybridization Protocol for Testing of Newborns for Possible Chromosomal An-euploidy. 158. AB
Cost reduction LEAN: One Laboratory’s Solution. 93. ABCourse evaluation Evaluation of an On-campus Blood Bank
Clinical Practicum Course. 91. ABCredentialing NCA and BOR Consider New Credentialing
Agency. 132. DDCurriculum – development Clinical Laboratory Sciences Curriculum
Re-development: An Application of Change Theories. 157. AB
Future Challenges for Clinical Laboratory Science Education. 91. AB
Implementation of an Integrated, Case-based Course in Cell and Molecular Biology for Pre-clinical Laboratory Science and Pre-cytotechnology Students. 92. AB
Curriculum – honors Clinical Laboratory Science: A Profession
with Honors. 139. CPCurriculum – interdisciplinary Overcoming Obstacles to Incorporate In-
terdisciplinary Curriculum into a Graduate Laboratory Science Program. 159. AB
Cystic fibrosis Introduction to Molecular Cystic Fibrosis
Testing 24. FODisaster management Managing a Clinical Laboratory Science Pro-
gram prior to, during, and after a Disaster. 93. AB
Distance education Growth and Evolution of a Distance Educa-
tion Clinical Laboratory Science Program: One University’s Perspective. 91. AB
The Incorporation of Student Support in Dis-tance Learning Course Structure. 92. AB
2006 INDEX
Online Orientation: A Tool to Increase Student Success. 97. AB
Student Laboratories as a Component of a Web-based Curriculum. 117. FO
Down syndrome Down Syndrome with Myelodysplasia of
Megakaryoblastic Lineage. 161. RREducation administration Student Information Management for Dum-
mies. 98. ABEducational collaboration Western College Alliance for Clinical Labo-
ratory Science Education. 95. AB Health Professions Workforce Partnership
Can Be the Answer. 154. ABEducational technology Advances and Innovations. 111. FO Blended Learning in the Practice, Wet Labo-
ratory Learning Environment. 96. AB Bringing the Classroom Online: How to Set
Up and Maintain the Discussion Board Tool in Online CLS Courses. 96. AB
Classroom Clicking for Enhanced Student Learning. 96. AB
Interactivity: Key to CLS Online Instruction. 122. FO
Factor V Leiden Factor V Leiden: An Overview. 218. CPFederal government Federal Government Impact in the Clinical
Laboratory. 42. FO Government 101: How an Idea Becomes
Law. 50. FO Government 103: What Happened to the
Great Idea? 54. FO Regulatory Agencies Involved with the Clini-
cal Laboratory. 43. FO Government Accountability Office (GAO) United States Government Accountability
Office (GAO) Targets Laboratory Quality. 194. WB
Glucose-6-phosphate dehydrogenase (G6PD)
Validating the Assessment of Glucose-6-Phos-phate Dehydrogenase (G6PD). 134. CP
Grade inflation Grade Inflation in Clinical Laboratory Sci-
ence. 153. ABHemochromatosis Searching for Hereditary Hemochromatosis.
174. RRHemoglobin A1c Cessation of Menstruation Improves the
Correlation of FPG to Hemoglobin A1c in Caucasian Women. 225. RR
Hepatitis A Hepatitis A Prevalence among Injection
Drug Users. 12. RR

VOL 19, NO 4 FALL 2006 CLINICAL LABORATORY SCIENCE 257
HIV drug resistance An Overview of the Human Immunodefi-
ciency Virus Featuring Laboratory Testing for Drug Resistance. 231 . FO
Interdisciplinary training Industry and Education: The Categorical
Model of Learning. 93. AB Interdisciplinary Healthcare Training: Bridg-
ing Clinical Laboratory Science, Genetic Counseling, and Physical Therapy. 97. AB
Learning objects Conversion of Existing Clinical Chemistry
Web-based Materials into Sharable Learning Objects. 97. AB
Learning Objects: Resources for Instruction. 184. FO
Learning styles A Comparison of Learning Styles of Allied
Health Students. 90. ABLeukemia Molecular Diagnostics of Hematological
Malignancies. 32. FOLicensure Understanding of and Opinions about
Licensure for Laboratory Personnel among Laboratory Professionals in the United States. 155. AB
Low carbohydrate dieting Integrated Metabolism and Low Carbohy-
drate Dieting. 158. ABMedical errors Medical Errors and Patient Safety: State Leg-
islation and Recommendations. 154. ABMedicare Competitive Bidding. 2. WB
2006 INDEX
Reimbursement Concerns. 66. WB Trends in Healthcare Payment. 130. WBMicrobiology Electronic Media Review. 250. BRMolecular diagnostic training Status of Molecular Diagnostics Incorpora-
tion into Clinical Laboratory Science Curri-cula: Results of a National Survey. 94. AB
Training Technologies for the Genomic Age. 148. CP
Ozone The Effect of Ozone on Common Environ-
mental Fungi. 157. ABPathology An Introductory Pathology Course in a
Medical Technology Curriculum. 158. ABPCR PCR Laboratory Exercises for Clinical Mi-
crobiology Students. 94. ABProficiency assessment A “Proficiency Assessment Process” for Clini-
cal Hematologists. 159. AB Are Quality Laboratory Services Related to
Personnel Credentials? 153. ABPulmonary aspergillosis Diagnosis of Invasive Pulmonary Aspergil-
losis: Molecular vs. Culture. 157. ABRecruitment Breezing Up – An Interdisciplinary Health
Professions Course for High School Juniors and Seniors and College Freshman. 112. FO
Investigation of Knowledge and Attitudes of African American High School Students toward Clinical Laboratory Science. 159. AB
A Model for Educational Enrichment and
Employment Recruitment for Clinical Laboratory Science Students. 169. RR
Young Adults’ Perceptions of an Ideal Career and a Career in Medical Laboratory Science. 160. AB
Introducing Clinical Laboratory Science: CLS Students Help Shape the Future. 206. CP
Research protocols Writing Clinical Research Protocols: Ethical
Considerations. 60. BRRetention Teaching Techniques to Increase First Year
Success. 95. ABStaphylococcus aureus Methicillin-resistant Staphylococcus aureus in
a Texas County Jail. 154. ABStatistics Interpretation of Statistics in Clinical Labo-
ratory Studies 18. RRStreptococcus pneumoniae Antibiotic Surveillance of Streptococcus pneu-
moniae in Mississippi. 5. CPTransfusion Transfusion-related Bacterial Sepsis. 155. ABTuberculosis Curriculum National Tuberculosis Curricu-
lum Consortium. 94. ABUS history “History is the Present”. 4. DD Verification, new method Teaching and Assessing New Method Verifi-
cation Skills Using Interactive Simulations. 188. FO
CLINICAL LABORATORY SCIENCE SEEKS MANUSCRIPTS
Clinical Laboratory Science invites all readers to submit manuscripts for possible publication. We particularly encourage submissions to the Research and Reports section.
If you have an idea for an article but aren’t sure how to begin, Clinical Laboratory Science editors can put you in touch with a mentor to help you prepare the manuscript. Their contact information, as well as full contact information for the editorial office, can be found on the inside front cover of this issue.
Submission guidelines may be found at http://www.ascls.org/leadership/cls/index.asp. Please contact Margaret LeMay-Lewis, Managing Editor, at [email protected] with any questions.