Clinical Handover - A Strategy Options Paper · PDF fileA STRATEGY OPTIONS PAPER ....
45
CLINICAL HANDOVER (CH) A STRATEGY OPTIONS PAPER Consultation Draft Queensland Health PATIENT SAFETY CENTRE CENTRE FOR HEALTHCARE IMPROVEMENT November 2009
Transcript of Clinical Handover - A Strategy Options Paper · PDF fileA STRATEGY OPTIONS PAPER ....

CLINICAL HANDOVER (CH)
A STRATEGY OPTIONS PAPER
Consultation Draft
Queensland Health PATIENT SAFETY CENTRE
CENTRE FOR HEALTHCARE
IMPROVEMENT
November 2009

Table of Contents
Table of Contents.......................................................................................................2 Acknowledgements....................................................................................................3 List of Figures ............................................................................................................3 List of Tables .............................................................................................................3 Recommendations for improvement in CH ...............................................................4 Principles and assumptions as the basis for recommendations..................................6 Glossary of terms .......................................................................................................7 Executive summary....................................................................................................8 1.0 Background to consultation draft CH strategy options paper............................10 2.0 Aims and objectives...........................................................................................10 2.1 Scope and purpose .............................................................................................10 3.0 Literature Review...............................................................................................10 3.1 Adverse events associated with communication and CH ..................................10 3.2 Consequences of ineffective CH:.......................................................................11 3.3 High risk scenarios in CH and causes................................................................11 3.3.1 Complexity of the health care system.............................................................12 3.3.2 Multiple health care encounters and transitions of care..................................12 3.3.3 Lack of policy, education and training in CH and teamwork .........................13 3.4 What is CH? – basic elements & functions .......................................................14 3.4.1 Communication of information, continuity and coordination of care ............14 3.4.2 Responsibility and accountability in CH ........................................................15 3.4.2.1 Responsibility for the conduct of effective CH ...........................................16 3.4.2.2 Accountability in CH ...................................................................................16 3.5 Patient transfers, discharges and CH .................................................................17 3.6 What is best practice in CH?..............................................................................20 3.7 Flexible standardisation of CH ..........................................................................21 3.8 Communication channels...................................................................................22 3.9 Lessons learned from human factors experts, HROs and some healthcare examples on best practice in CH..............................................................................22 ..................................................................................................................................23 3.9.1. Two-way, face-to-face interactive exchange of information.........................23 3.9.2 Face-to-face communication with written support .........................................23 3.9.2.1 Shift-to-shift handovers ...............................................................................23 3.9.2.2 Interdisciplinary team-based checklists, briefings and daily goals..............24 3.9.2.3 Whiteboards/journey boards ........................................................................27 3.9.2.4 Bedside handover.........................................................................................28 3.9.3 Multidisciplinary/interdisciplinary teamwork & communication ..................29 3.9.4 Process/structure redesign options..................................................................30 3.9.5 Verbal orders and repeat-back, read-backs.....................................................30 3.9.6 Team-based training strategies and solutions to promote resilience and enhance patient safety in CH ...................................................................................32 3.9.7 Simulation as an adjunct to team training.......................................................33 4.0 Conclusion .........................................................................................................33 Bibliography ............................................................................................................34
Front page
2
“The number of possible conversations increases combinatorially with the number of individuals who need to communicate….. Even small clinical teams have the capacity to generate large and complex communication spaces” (after Lang and Dickie, 1978 in Coiera, 2006).

Acknowledgements This consultation draft strategy options paper was developed with key stakeholders in Queensland Health and nationally. List of Figures Figure 1 Staff/practitioner contributing factors to SAC 1 clinical incidents reported in
PRIME-CI 2006-07, Queensland Health .............................................................11 Figure 2 Preconditions to accountability .....................................................................17 Figure 3 Richness of communication channels ...........................................................22 List of Tables Table 1 Responsibility in CH varies due to situational factors....................................15 Table 2 Key to good pretransfer assessment and preparation......................................19 Table 3 Differences between MDTs and IDTs ............................................................29 Table 4 Errors associated with verbal orders ...............................................................31
3

Recommendations for improvement in CH Recommendation 1 - Statewide, standardised, mandatory policy guidance on CH Queensland Health has an organisational responsibility to provide guidance for the effective conduct of CH. Subject to stakeholder consultation, elements of the policy and implementation standard could include the following: • Where possible, CH must be conducted face-to-face, verbally, with interactive
questioning and clarification to create shared mental models/understanding. • CH must be supported by a written or documented component such as a checklist,
computer-generated handover template, whiteboard, electronic means or similar. • A requirement that the handover occurs at the patient’s bedside and includes the
patient and their family, where possible. • Taped handovers, as a sole method of CH, be banned under this policy. • Ideally, handover should be incorporated into the work of interdisciplinary teams,
such as daily ward rounds, patient care and discharge planning. • A requirement that handover be lead and overseen by the most available senior
clinician of the team. Senior staff have a unique role to play in the supervision, education and modelling of desirable professional behaviours in CH and teamwork to junior staff.
• A requirement that sufficient time designated for handover is built into the rostering system.
• A requirement for environmental control during handover to limit interruptions and promote open communication, including adequate ward coverage.
• An outline of acceptable language and abbreviations is described in the policy. • Provision of policy guidance on the various tools and strategies available for
effective CH and when to use them. E.g. SBAR, read-back. • Provision of policy guidance for staff on the possible content, format and style of
handover communication is provided. This must include a revision of historical data, description of the patient’s current condition, a forward-looking, proactive plan of care, expected care trajectory and goals for patient care, including rationale, risks and possible deviations from the expected care plan and any contingency measures required.
• A clear description of the roles, responsibilities and accountability for staff during handover towards the organisation, one another and the patient.
• Clear guidance on the requirements for the provision and receipt of verbal orders, phone consults and telephone diagnostic test results reporting.
• Clear guidance on communication requirements, roles, responsibilities and accountabilities for patient transfers and discharges.
Recommendation 2 - Specific recommendation for Operating Theatres (OTs) Evidence for the effectiveness of the World Health Organisation (WHO) surgical checklist with team briefings is established. It is therefore recommended that the WHO surgical checklist, with team briefings and debriefings be the preferred model of team communication and CH to be used in the OTs throughout Queensland Health facilities. Recommendation 3 - Further consultation on CH content/minimum data set
4
Handover content will vary according to the clinical setting in which it is undertaken. It is recommended that extensive stakeholder consultation during policy development

be undertaken statewide to determine a possible minimum data set for clinical handover. Recommendation 4 - Policy guidance on transfer and discharge of patients Formal, standardised policy guidance is required for the conduct of patient transfers and discharges between Queensland Health units, facilities, other organisations and the community. Policy development and implementation should occur in tandem with new work being undertaken for the care of the deteriorating patient and risk management of patients who are outliers, and this work will require ongoing stakeholder consultation. Recommendation 5 - Interdisciplinary teamwork, communication and CH education and training Healthcare professionals are expected to work as members of interdisciplinary teams in order to provide high quality, safe care for their patients. Queensland Health has a responsibility to its staff to provide training and education in effective CH, teamwork and communication, in order to promote and build organisational learning, capacity and resilience for the prevention and mitigation of gaps, errors and patient harm associated with poor communication. Therefore, it is recommended that: • All new and existing Queensland Health (QH) clinical staff receive orientation,
education and training in how to conduct effective CH. • A TeamSTEPPS (Team Strategies and Tools to Enhance Performance and Patient
Safety) train-the-trainer training workshop was conducted in July in Brisbane, followed by piloting of this program in three sites within QH. If pilot testing is successful, a business case will be developed to evaluate feasibility of a phased-in approach to statewide implementation of TeamSTEPPS team training.
• In some dynamic, high risk clinical areas, such as the OT, Emergency Department (ED), Labour & Delivery Unit (L&D) and Intensive Care Unit (ICU) where time pressures and staffing levels might preclude long absences from the clinical setting for team training purposes, the introduction of situated learning in the form of checklists and interdisciplinary team briefings, based on the principles of team training, could be a more cost-effective approach.
• Interdisciplinary team training early in clinical education for health professionals is essential for ongoing practice in the healthcare setting. It is recommended that Queensland Health Patient Safety Centre liaise with universities, nursing and medical schools and the Skills Development Centre on teaching effective CH, teamwork and communication.
5

Principles and assumptions as the basis for recommendations
The following principles and assumptions form the basis for the recommendations made in this consultation draft CH strategy options paper:
1) A broad definition of CH is adopted and preferred, due to the embedded nature of
CH within teamwork interactions and communication processes. Handovers ‘permeate’ the healthcare system and encompass: shift-to-shift handovers, transfers and discharges, transitions of care between and within clinical areas, briefings, consults, verbal orders and telephone receipt of diagnostic test results.
2) CH, like all health care, should be patient and family-centred. 3) It is proposed that the principle of ‘shared responsibility and accountability’ in
CH, interdisciplinary teamwork and communication be the basis for promoting and driving a shift in patient safety culture in order to close the gaps and errors caused by ineffective teamwork and communication and to provide the best safety net for patients. Responsibility and accountability in CH and communication must extend across both role and physical boundaries during patient care transitions until that transfer or care transition is complete. This is based upon the observation that the highest risk for patients occurs at the edges and boundaries of care transitions and patient transfers where roles can become ambiguous and responsibility and accountability become diffused and less demarcated over time and space.
4) Roles, responsibility and accountability for ongoing patient care must be made
explicit during CH. Responsibility can be delegated or negotiated (accepted or rejected), depending on the situation and clinical setting (see preconditions to accountability, page17).
5) A comprehensive CH improvement framework must include both top-down
(policy guidance, clear roles, responsibilities and accountability) and bottom-up approaches (development of capacity and resilience among interdisciplinary teams through education and training in CH, teamwork and communication).
6

Glossary of terms High Reliability Organisations (HROs): organisations that have succeeded in avoiding catastrophes in an environment where normal accidents can be expected due to risk factors and complexity. HRO teams are comfortable and adept at quickly building creative responses to failure because they lean on their training and experience as a reliable means to recover from failure. Human factors: the study of all aspects of the way humans relate to the world around them, with the aim of improving operational performance, safety, through life costs and/or adoption through improvement in the experience of the end user. Mental model: the internal mental representation held by an individual. It involves accurate alignment of present and future perceived system states with actual system states. Mnemonic: a memory or learning aid, usually verbal—such as a very short poem or a special word used to help a person remember something—but may be visual, kinesthetic or auditory. Mnemonics rely on associations between easy-to-remember constructs which can be related back to the data that is to be remembered. This is based on the principle that the human mind much more easily remembers spatial, personal, surprising, humorous or otherwise meaningful information than arbitrary sequences. Resilience: the ability to adapt or absorb disturbance, disruption, and change and this may be increased by team processes in a complex, sociotechnical system. Building resilience is the process of aiding people who are under pressure from conflicting goals to cope with organisational complexity so they can actively adapt to create and sustain failure-sensitive strategies. Satisficing: Seeking or achieving a satisfactory outcome, rather than the best possible. SBAR: Situation-Background-Assessment-Recommendation. The SBAR mnemonic was first used in the military for nuclear submarines. It was introduced in 2004 as a tool to improve communication primarily between nurses and physicians in hospitals in the United States (US). It is an easy-to-remember mnemonic; useful for framing any conversation, but especially critical ones requiring a clinician’s immediate attention or action. Situational awareness: the perception of environmental elements within a volume of time and space, the comprehension of their meaning, and the projection of their status in the near future.
7

Executive summary
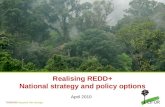
Communication failure is thought to account for up to 75% of root causes of adverse events in health care and up to 50% of those may be attributed to the handover period (Dunn et al, 2007; Joint Commission 2006). Australian data on contributing factors for reported sentinel events (2004-2005) indicated that communication failures contributed to almost 60% of all sentinel events reported in that period. Communication failures were the second most frequent contributing factor for wrong patient, wrong body part surgeries (34%) after issues associated with policies, rules and procedures (68%) (AIHW & ACSQHC, 2007). In Queensland, communication failure (26%) is also the leading contributing factor for SAC 1 clinical incidents reported in PRIME-CI (2006-07) for staff/practitioner-related contributing factors (DAT, 2009).
The consequences and effects of ineffective clinical handover (CH) are
numerous and far reaching. These include: patient complaints (Bark et al, 1994); increased health care expenditure (Zwarenstein & Bryant, 2002); delays in medical diagnosis (Pronovost et al, 2002); wrong treatment (Priest & Holmberg, 2000); increased hospital length of stay (Zwarenstein & Bryant, 2002); life threatening adverse events (Bulau, 1992) and a range of other potentially preventable adverse events (Petersen et al, 1994).
The causes of ineffective CH and communication are also numerous and are
typically embedded within the structure and processes of the healthcare system. These include: (1) the complex sociotechnical system of health care itself, including information asymmetry, organisational complexity involving both horizontal differentiation of labour as well as vertical divisions of hierarchy and power (Braithwaite et al, 2009); (2) increasing patient encounters across specialties, rapid turnover of staff and patients, increasing acuity of care, technological complexity and increasing casualisation of the workforce (Cohen & Hilligoss, 2009; UTS, 2008); (3) lack of education and training in CH, lack of policy guidance on CH, and lack of education and training in interdisciplinary teamwork among health care professionals (Leonard et al, 2004; Healey et al, 2008; Quin et al, 2009).
The basic elements of CH encompass: (1) communication of information to
facilitate continuity and coordination of patient care, (2) notions of responsibility and accountability for the effective conduct of CH and for patient care, (3) movement of the patient and equipment across care transitions, transfers and discharges, (4) many other functions, including the education and professionalisation of staff and promotion of teamwork (Strange, 1996).
The evidence-base for improvement in CH is growing but is at present incomplete and is complicated by the lack of a uniform and widely accepted definition (Wong et al, 2008). There is no convenient ‘one size fits all’ solution for CH (Botti et al, 2009) and it is evident that although there are some principles to guide best practice in CH, solutions and strategies will be context-specific and will need to be tailored locally (Johnson & Barach, 2009). Lessons learned from High Reliability Organisations (HROs) and some context-specific health services research point to some basic requirements for effective CH. These include:
8

(1) Two-way, face-to-face, verbal, interactive exchange of information (Lardner, 1996) with written/document support, such as structured communication tools, e.g. computer-generated pre-populated sheets, checklists, whiteboards/journey boards (Haynes et al, 2009; Parke & Mishkin, 2005; Lardner, 1999),
(2) Interdisciplinary team rounds and other process redesigns (Hall & Weaver, 2001; Jessup, 2007, Mudge et al, 2006), and,
(3) Bedside handover, patient and family centred CH (Chaboyer et al, 2008).
Efforts to standardise CH must be balanced with the need to retain other important functions of CH, such as the provision of social and professional support for all staff and the promotion of individual, team and organisational learning (Cohen & Hilligoss, 2009; Patterson, 2008; Patterson, 2007). Flexible standardisation is preferred rather than imposing a rigid standard for CH across all clinical settings (Lillrank & Liukko, 2004). Therefore, the key to improving patient safety in CH and improving communication between health care providers lies in viewing people (including teams) as the primary source of resilience in creating safety under increasing organisational complexity, resource and performance pressure. Building resilience could be described as the process of aiding people who are under pressure from conflicting goals to cope with organisational complexity so they can actively adapt to create and sustain failure-sensitive strategies (Patterson et al in Bognor, in press; Johnson & Barach, 2009). A system-wide strategy to improve CH should be comprehensive and provide multifaceted top-down and bottom-up strategies aimed at the level of the organisation, teams and individuals through:
(1) Policy guidance for the conduct of CH, including clear guidance on roles,
responsibility and accountability in CH, (2) Provision of tools and strategies for effective CH, and, (3) Education and training in effective CH, communication and interdisciplinary
teamwork.
The preferred options for a system-wide strategy to improve CH are outlined in the following table:
CH recommended strategy options Responsibility
1. Statewide CH policy & implementation standard (PSC develops policy, educational resources, tools and strategies, consultation and liaison with stakeholders on CH, interdisciplinary teamwork and communication)
Patient Safety Centre
2. Implementation of the WHO surgical checklist with briefings/debriefings in all QH Operating Theatres
Patient Safety Centre with HSDs
3. Implementation of bedside handover by interdisciplinary teams
Patient Safety Centre with HSDs
4. TeamSTEPPS training in communication, CH and teamwork skills including use of video-reflexive technique
Patient Safety Centre, Skills Development Centre & HSDs
9

1.0 Background to consultation draft CH strategy options paper CH has been identified as a high priority in patient safety. The Australian
Commission on Quality and Safety in Health Care (ACSQHC) has identified CH as one of its top priorities (Priority Area 5) for work in 2007-2008. This priority is in the context of Australia taking a lead role in producing a standard operating protocol for CH as part of its participation in the World Health Organisation’s ‘High Fives’ initiative (Wong et al, 2008). In the US, interest in improving handover has increased with The Joint Commission issuing a requirement that hospitals implement a standardised approach to handover communications, including an opportunity to ask and respond to questions (Joint Commission, 2006).
2.0 Aims and objectives • To describe and better understand the complex nature of CH • To examine patient safety risks in relation to CH • To define best practice in CH • To propose a comprehensive framework for statewide implementation of CH • To provide indicative costings for implementation 2.1 Scope and purpose
A broad definition of CH is preferred in order to firstly, fully understand its
complexity and secondly, to propose effective strategies for comprehensive improvement. Therefore, this draft consultation strategy options paper encompasses the different types of CH: shift-to-shift handovers (e.g. nurse-nurse, doctor-doctor), multi- and interdisciplinary care rounds, patient transfers within and between health care facilities, discharge to home or community setting, and care transitions, such as perioperative care. Other forms of communication are considered and discussed e.g. telephone consults and receipt of diagnostic test results in the context of CH. Case studies or vignettes of de-identified and modified Root Cause Analyses (RCAs) of adverse events reported in PRIME are included in text-boxes to illustrate problems associated with CH in QH. The purpose of this draft consultation strategy options paper is to propose strategies aimed at the organisation, team and individual level to build organisational resilience that will improve interdisciplinary teamwork, communication and approaches to CH. Resilience is defined as: “the ability to adapt or absorb disturbance, disruption, and change” and this “may be increased by team processes in a complex, sociotechnical system” (Patterson et al, 2007). Additional information on CH can be provided in a CH Discussion Paper, including an environmental scan of current and past CH initiatives in QH.
3.0 Literature Review 3.1 Adverse events associated with communication and CH
10
Based on sentinel events data from the US, communication failure is the leading source of adverse events in healthcare and is thought to account for up to 75% of root causes of adverse events in health care. Up to 50% of those may be attributed to the handover period (Dunn et al, 2007; Joint Commission 2006). Australian data on contributing factors for reported sentinel events (2004-2005) indicated that communication failures contributed to almost 60% of all sentinel events reported in

11
that period. Communication failures were the second most frequent contributing factor for wrong patient, wrong body part surgeries (34%) after issues associated with policies, rules and procedures (68%) (AIHW & ACSQHC, 2007). In Queensland, communication failure (26%) is also the leading contributing factor for SAC 1 clinical incidents reported in PRIME-CI (2006-07) for staff/practitioner-related contributing factors (DAT, 2009).
Figure 1 Staff/practitioner contributing factors to SAC 1 clinical incidents reported in PRIME-CI 2006-07, Queensland Health
Staff / Practitioner Contributing Factors
Communication - care / treatment
4426%
Instructions not follow ed or
misinterpreted18
11%
Distraction or inattention16
10%
Others36
22%
Know ledge / skill issues32
19%
Teamw ork / Supervision factors
2012%
3.2 Consequences of ineffective CH: The consequences and effects of ineffective CH are numerous and far
reaching. These impact on all levels of the health system, including the organisation, teams, individuals and patients and their families. A former Australian Safety & Quality Council (2005) literature review summarised the consequences of ineffective handover as follows:
• Patient complaints (Bark et al, 1994)
• Increased hospital length of stay (Zwarenstein & Bryant, 2002)
• Increased health care expenditure (Zwarenstein & Bryant, 2002)
• Delays in medical diagnosis (Pronovost et al, 2002)
• Wrong treatment (Priest & Holmberg, 2000)
• Life threatening adverse events (Bulau, 1992)
• A range of other potentially preventable adverse events (In the Petersen et al (1994) study these were due to gaps in communication and patient care between cross-covering medical teams).
3.3 High risk scenarios in CH and causes
CH is paradoxical. It represents both a high-risk period for patient safety
during the process of ‘handing over’ patient care information, responsibility and

accountability, and an opportunity to catch errors through ‘fresh eyes’ (Clancy, 2006). During CH, changes in shifts, patient transfers and transitions in patient care, ‘gaps’ in continuity of care, communication and responsibility may arise, creating potential for error and resultant patient harm. Characterising gaps in continuity of care, understanding how they develop, how they manifest themselves in the work world in particular contexts, and how they impact patient care and safety is essential to designing effective means for creating continuity of care (Patterson et al in Bognor, in press) and preventing error and patient harm. Gaps arise from a variety of sources:
• Lost information about current or past status, the history of care, or plans for
future care. • Organisational and institutional boundaries that mark changes in responsibility or
authority, different roles of professionals, or formal divisions of labor. • During transfers, whether physical transfer of patients from unit to unit within a
hospital or shift changes. In the complex environment with multiple actors engaged in care, roles may shift quickly and obviously or slowly and subtly.
3.3.1 Complexity of the health care system
Modern day health care is performed by teams of health care professionals working in a “complex sociotechnical system” (Braithwaite et al, 2009). Due to its complexity, the healthcare system has to some degree lacked the structure, systems and processes to support effective transfer of information (Plsek & Greenhalgh, 2001). Information asymmetry aggravates or worsens patient care coordination resulting in fragmentation of care and discontinuity of care that can compromise patient safety (Arora et al, 2008). Communication needs are therefore increased in the context of increasing specialisation of health care. One of the goals of communication is to coordinate the actions of individuals through mutual understanding and obligation (Weigand et al, 2003). Adding to the problem of information asymmetry, organisational complexity involves both horizontal differentiation of labour as well as vertical divisions of hierarchy and power. Significantly, relationships among and between team members are shaped and determined by these divisions. These structures and differences in status have a powerful influence on not only how health care teams relate to one another but can also determine whether and how vital information is effectively communicated (Sutcliffe et al, 2004). Seniority, experience and expertise of in-coming staff, as well as changes in the surrounding conditions, such as transition from day to night hospital coverage, can also contribute to adverse patient outcomes, even if all the required information is perfectly communicated (Petersen et al, 1994; Cohen & Hilligoss, 2009). 3.3.2 Multiple health care encounters and transitions of care
12
Two contemporary trends that characterise today’s complex health care organisations are increasing specialisation and increasing rates of personnel change (Cohen & Hilligoss, 2009). Increasing patient encounters across specialties, rapid turnover of staff and patients, increasing acuity of care, technological complexity and increasing casualisation of the workforce, are all factors that impact on the safety and quality of health care (UTS, 2008). Health care necessarily involves multiple

occasions where vital information must be effectively communicated and responsibility and accountability for patient care is transferred between or shared among caregivers. Health care providers are also faced with the inherent limitations of human performance from increased pressures due to time constraints, fatigue, multitasking and interruptions to their daily routines (Denham, 2008; Leonard et al, 2004). During an episode of care and between episodes of care, a patient can potentially be treated by a number of different healthcare individuals and teams in multiple different healthcare settings. Patients will often move between areas of care, diagnosis and treatment on a regular basis and encounter changing shifts of staff at each interval (WHO, 2007). Discontinuity of health care personnel and tasks during shift-to-shift handovers and fragmentation of care due to transitions in patient care across settings can lead to the risk of non-transmission or miscommunication of critical information (Lardner, 1999; Schultz et al, 2007). Variability in structure, type, extent and order of information exchanged between providers is thought to increase the potential for omissions of information and miscommunication as well as making it difficult to anticipate what information will be received in handover, leading to wasted effort in looking for this elsewhere. It also makes it less efficient because the rules for handover need to be negotiated each time anew (Borowitz et al, 2008). The movement of patients across the health care continuum and between phases of care must be accompanied by mechanisms to support the transfer of high quality information and be supported by clear lines of responsibility and accountability for patient care between members of the health care team (AMA, 2006; Sutcliffe et al, 2004). 3.3.3 Lack of policy, education and training in CH and teamwork
13
To date, in Australia, formal and comprehensive national and statewide healthcare policy guidance outlining information requirements, communication processes, and roles and responsibilities in CH, has been lacking (Quin et al, 2009). Coupled with this, few health care education and training programs formally teach health care providers how to perform effective CH (Horwitz et al, 2006), leading to poor quality CH among trainees and associated adverse events, mistakes and near misses (Jagsi et al, 2005). This has largely been learned informally, on-the-job and by observing senior colleagues giving CH (Sharit et al, 2005). Furthermore, health care providers receive little or no training in non-technical skills such as teamwork and communication within interdisciplinary teams, yet they are expected to work effectively in interdisciplinary teams in the healthcare setting (Singh et al, 2007). Education and training of health care providers such as doctors, nurses and allied health professionals has in the past typically focussed on communication with patients and individual technical skills for proficiency of specific tasks (Nestel & Kidd, 2006). Health care providers are also educated and trained within their respective professions. Effective communication and teamwork between disciplines have been assumed and formal training and assessment in these areas has been largely absent (Leonard et al, 2004; Healey et al, 2008). Failures of communication are not simply the result of faulty transmission and exchange of information between health care providers, but also arise from lack of role clarity, role conflict and ambiguity, and struggles with professional status and interpersonal power differentials between individuals and within disciplines (Sutcliffe et al, 2004). Teamwork is an important pre-determinant of successful CH and is influenced by many complex, system-based factors (CRE-PS & ACSQHC, 2007). Yet CH is highly variable within and across teams, disciplines and health care organisations and is often poorly performed (Arora

et al, 2008). Strategies aimed at improving communication and CH between members of health care teams must therefore clarify roles and responsibilities of team members and bridge these differences in status and power (Weller et al, 2008).
3.4 What is CH? – basic elements & functions Although CH has been researched for at least four decades, a comprehensive definition of CH has not been proposed or universally recognised (Wong et al, 2008). This has significant implications for establishing a common understanding of CH and determining how implementation of best practice in CH may be achieved. Additionally, CH has been studied and researched in particular clinical settings and so much of the evidence is context-specific (Cohen & Hilligoss, 2009). The term CH has typically been used to describe the process of ‘handing over’ patient care from one caregiver to another between shifts or on transfer of the patient from one health care setting to another. It involves the communication of patient care-related information and transfer, sharing and acceptance of responsibility and accountability for patient care among and between individuals and teams of health care providers across the health care continuum and between transitions of care (ACSQHC, 2008; Safety & Quality Council, 2005). Understanding the nature of CH is central to understanding its associated problems. It is also the necessary starting point to proposing any comprehensive solutions or strategies for improvement. The two main elements of CH comprise communication of information and ‘handing over’ of responsibility and accountability in addition to other covert and ritual functions. CH is complex, dynamic, multifaceted and difficult to define (CRE-PS, 2007; Turner et al, 2006).
3.4.1 Communication of information, continuity and coordination of care
In nursing circles CH has been described as a “process of passing complete
and accurate patient-specific information from one caregiver to another” (Mascioli et al, 2009). Its basic feature as a system for communicating the information needed to facilitate the patient care process has remained. Coiera (2006) describes a ‘communication space’ in health care that is formed by interpersonal interactions. Even small teams can generate a large and complex communication space and that most information is sought not from documentation sources but from other members of the health care team. According to Coiera (2006), “the biggest information repository in healthcare sits in the heads of the people working within it, and the biggest information network is the complex web of conversations that link the actions of these individuals”.
14
Authors have adopted the view that patient care continuity is central to any definition of handover and that it is its primary function (Sherlock, 1995; Thurgood, 1995). Continuity refers to coherent, connected, smoothly evolving care as the individual patient moves from location to location and from provider to provider. Discontinuity of tasks and personnel may result in non-transmission or miscommunication of information and poor coordination among caregivers. Shift handover, in particular, is a task-oriented interaction occurring between two or more individuals (Lardner, 1999). Continuity is accomplished by the person accepting responsibility for care having an accurate, complete mental model of the patient’s history and current status, being aware of significant data or events, being prepared to deal with impacts from previous events and anticipate future events, conducting

planned activities, and avoiding an unwarranted shift in goals, decisions, priorities, or plans (Patterson et al., 2004). Cohen & Hilligoss (2009) refer to CH as a proactive, forward-looking activity: to summarise the patient’s situation in order to significantly shape subsequent treatment and decision-making.
Practitioner risk factors for poor communication include: culture/ethnicity;
education, literacy, beliefs and behaviours; gender; and personality. The three most common areas of communication failure may be found at the levels of: (1) the individual (autonomy, lack of team training, hierarchy, and trust), (2) the environment (interruptions, time constraints and workloads, multiple conversations, lack of face-to-face interactions, noise) and at (3) the structural level (daily changes in patient condition, orders, lab results and treatment plans; lack of structured communication tools such as checklists, unclear or incomplete data and lack of clarification of information) (Haig, 2006). 3.4.2 Responsibility and accountability in CH
More recently, in medical circles, CH has been defined as: “the transfer of professional responsibility and accountability for some or all aspects of care for a patient, or group of patients, to another person or professional group on a temporary or permanent basis” (NPSA, 2006; AMA, 2006; ACSQHC, 2008). Definitions of CH that describe it as a transfer of responsibility or ‘passing of a baton’ are unnecessarily narrow and possibly misleading. Communication, responsibility and accountability are shaped and determined by the particular circumstances and setting and the process is non-linear and often coordinated amongst many individuals (Beach et al, 2003; Cameron, no date). Responsibility can be defined as “an action that acknowledges the requirement to complete/fulfil an action/decision, with a voluntary element”. The different types of responsibility are summarised below: Table 1 Responsibility in CH varies due to situational factors
Type of Responsibility
Context/setting
Clear, direct transfer (‘passing the baton’) or delegated
• Shift-to-shift where outgoing caregiver(s) hand over responsibility for patient care to incoming (s) and leave (Lardner, 1999)
• Patient care responsibility is delegated by a senior to a junior staff member (Smith et al, 2008)
• The patient is physically transferred or discharged from one location to another and responsibility for care passes from one individual, team or organisation to another (Horwitz et al, 2008)
Shared • Where responsibility for patient care is shared among members of an interdisciplinary team, e.g. in the OT (Jessup, 2007; Beach et al, 2003)
Negotiated or transitional and diffused
• Where responsibility for patient care is intended to be transferred but instability of the patient/process prevents this from occurring e.g. patient transferred from OT by anaesthetist to PACU and receiving recovery nurse requests anaesthetist to remain with the patient until the vital signs stabilise (Smith et al, 2008)
• Where a patient is in the ED awaiting transfer to an inpatient unit but the unit is not yet ready to receive them (Horwitz et al, 2008)
15
It is proposed in this consultation draft strategy options paper that, for CH to be truly effective in preventing and mitigating patient harm, roles and responsibilities should be: (1) made explicit during CH and (2) responsibility be viewed as being shared among and between members of the interdisciplinary team or when the patient

is undergoing transitions in care or during transfers. Most handover communication occurs within disciplines (doctor to doctor and nurse to nurse), rather than across groups. Whilst there may be effective communication and transfer of responsibility from doctor to doctor or nurse to nurse, the lack of structured interaction between disciplines and across care settings is a risk factor for communication gaps, errors and patient harm (Fairbanks et al, 2007; Reader et al; Weller et al, 2008; Thomas et al, 2003). 3.4.2.1 Responsibility for the conduct of effective CH
Responsibility for the effective conduct of CH rests both with the organisation
and its staff members. Analysis of accidents and incidents in the nuclear processing industry, space shuttle mission control and off-shore oil refinery maintenance operations by several researchers (Lardner, 1996; Lardner, 1999; Parke & Mishkin, 2005) has resulted in recommendations and advice for ensuring a systems approach to conducting effective CH and these have relevance for healthcare organisations:
1) Organisations are responsible for setting standards for effective communication in
CH by providing policy and procedural guidance on how effective CH should occur.
2) Organisations have a responsibility to their employees by developing the communication skills of their new and existing staff through education and training.
3) Staff share joint responsibility for ensuring accurate communication takes place. In particular, consideration of the specific information needs of others and capturing and communicating this information in a reliable and unambiguous manner. It therefore must be made explicit to staff that responsibility for ensuring effective handover communication rests with both incoming and outgoing staff.
3.4.2.2 Accountability in CH
16
Accountability refers to “the act of accepting, acknowledging and assuming the responsibility for action/decision, encompassing the obligation to report, explain and be answerable for resulting consequences” (Jorm & Iedema, 2008). Accountability in CH is very complex and is related to responsibility; but responsibility is only one aspect of accountability (Bergman, 1981). It is proposed that there are certain preconditions to accountability in CH and that these have increasing significance in today’s complex healthcare system in relation to matters such as the training, supervision and delegation of responsibility to junior staff, scope of practice and the staffing and resourcing of departments and healthcare facilities. For example, a person is held accountable when; firstly, one acquires the necessary knowledge, skills and abilities via education and training. Secondly, one is given formal authority in the form of a role description or a defined scope of practice and is adequately resourced to perform the role. Thirdly, one is provided adequate information in CH through effective communication. Finally; responsibility is explicitly given and accepted – one is thus accountable (Fig. 2). The model therefore implies that responsibility and accountability can be rejected or refused if the preceding preconditions are not satisfied. It is proposed that this point should be clearly stated in a CH policy and implementation standard in order to promote patient safety in cases where there is doubt about any of the preconditions. Accountability in CH is operationalised through collaboration and sharing of information and responsibility

with other healthcare professionals and includes the patient and their family (Bergman, 1981).
Figure 2 Preconditions to accountability
Person is accountable for patient’s care
Responsibility is delegated or negotiated (explicitly given and received)
Provision of information via effective communication of the patient’s care plan
Formal authority for patient care – role, scope of practice and capacity, resources
Knowledge, skills and abilities via education and training in healthcare
Adapted from Bergman (1981) Accountability: Definition and dimensions, International Nursing Review, 28(2), 53-59. 3.5 Patient transfers, discharges and CH
Patient transfers and discharges are care transitions or interfaces where patient
care-related information/documentation, responsibility and accountability ideally accompany movement of the patient, and sometimes equipment, between health care settings. These interfaces have been identified as a high-risk situation for patients due to a combination of factors and complex interactions required to coordinate patient movement between clinical settings and between teams (Catchpole et al, 2007). Such interfaces may contribute to errors or omissions of information or communication and result in diffusion of patient care responsibility (Horwitz et al, 2008). Where CH involves patient transfers or discharges from one location to another, these may be for:
17
(1) Patient-centred reasons (e.g. transfer from Emergency Department (ED) to Intensive Care Unit (ICU) for higher acuity ongoing care).

(2) Logistical reasons (e.g. access block in ED and need to move patients out to inpatient units). It is suggested that this represents a high-risk situation for patients because transfer reasons are not patient-centred and therefore may result in patients being sent to units in unstable conditions or be received by units that are not able to provide optimal care for the patient (Horn et al, 2004). Patients may be transferred to the unit of their covering doctor or may be transferred to another unit as an outlier. This situation represents an especially high-risk situation for patients due a diffusion of responsibility where the unit staff may be unsure of who is responsible for the care of the patient and when they should contact staff for assistance and advice.
In general, it is advisable that patients should not be transferred when their
condition is unstable, but this is not always possible (Dunn et al, 2007a; Patterson et al, 2004). Ideally, transfer of the patient should be accompanied by the required information that is communicated in the most efficient, effective and appropriate channel or medium and the receiver(s) would be adequately knowledgeable, skilled and have the resources to accept ongoing responsibility and accountability for care of the patient. Furthermore, CH for these patients should include guidelines for the care of the deteriorating patient: how to recognise this is the case (parameters for vital signs and other observations), who is the responsible treating doctor and what is their contact number, or contact name and number of covering doctor. Transfer of high-acuity care patients may further be complicated by the simultaneous transfer of equipment (Dunn et al, 2007 (a); Kripalani et al, 2007; Jack et al, 2009; Catchpole et al, 2007).
Catchpole et al (2007) demonstrated that the transfer and handover of patients
between high acuity units, such as from the OT to the ICU, requires both effective and structured communication as well as teamwork to coordinate activities and equipment during such transfers. The research team developed a simple transfer protocol (checklist) combined with a short training session for teams from the OT (transferring unit) to the ICU (receiving unit) for patients undergoing paediatric cardiac surgery based upon principles from formula 1 racing and aviation. The protocol or checklist served as an aide de memoire during handovers between staff from each unit. Handover involved pre-handover preparation of a patient transfer form, preparation of bed space and equipment, preparation and completion of all paperwork. During information handover a team leader maintained overall situational awareness and coordination of the transfer process whilst the sending anaesthetist and surgeon first gave their reports uninterrupted. This was followed by interactive questioning by the receiving team with reference to the information contained in the checklist. Finally, the receiving team discussed the case as a group, made plans, identified anticipated problems and expected recovery and accepted responsibility for ongoing care of the patient. Results showed significant reductions in technical errors (from 5.42 to 3.15, p<0.001), reduction of information omissions (from 2.09 to 1.07) and reduction in
18
Case study: A patient had been treated in the ED for asthma and respiratory infection and was experiencing respiratory distress. The patient was transferred out of the ED as an outlier to a distant unit due to increasing access block in the ED, despite ongoing respiratory distress. The handover process did not provide staff with reportable parameters for vital signs. Two hours later the patient suffered a cardiac arrest unattended by staff.

duration of handover (from 10.8 mins to 9.4 mins). The authors stated that this checklist/protocol could also be used in other clinical areas where there are limited opportunities for training. They were able to implement the protocol within 15-30 minutes of training and stated it could be introduced at staff induction. The teams in this study were quite likely already high performing teams, but the study authors suggested that the checklist protocol could actually change the impact of teamwork on the handover process, whilst emphasising the value of good teamwork in achieving low rates of error.
Transfers of critically ill patients between hospitals and units pose a risk to
patient safety because these transfers are often made out of normal working hours, and where junior staff may accompany the patient. The patient would ideally be stabilised pre-transfer, however, the reality is often that of striving for balance between achieving this aim, the need for urgent transport and the accepting team’s readiness. This in turn is influenced by the availability of the nature and severity of the patient’s condition, the availability of transfer personnel and equipment and availability of specialist investigations. Dunn et al (2007a) have provided guidelines for safe pretransfer assessment and preparation of critically ill patients and state that personnel involved in such transfers must be adequately trained and experienced in this work in order to reduce risk of serious injury to patients or staff.
Table 2 Key to good pretransfer assessment and preparation
Patient Familiarisation with current condition, investigation results, current treatment and further management plan
Transfer staff Suitably trained staff, appropriate clothing, adequate handover from referring team, return plans arranged and insurance
Equipment Suitable equipment and drugs, spare batteries and sufficient oxygen Organisation Patient notes and investigation results, transfer documentation,
coordination of transfer vehicle and personnel, relatives informed and compliance with relevant regulations
Destination Receiving doctor name, receiving unit address and telephone number, and directions to receiving unit
Pre-departure Receiving unit informed of estimated time of arrival, patient packaged and secured, equipment secured or stowed, electrical and oxygen supplies attached to vehicle outlets if appropriate, transfer staff seated and secured if appropriate
(Adapted from Dunn et al (2007a) Critical care in the emergency department: patient transfer, Emergency Medicine Journal. Emj.bmj.com).
As the specialisation of hospital care expands, transfers and discharges from
hospital-based care to community-based care are becoming increasingly common and are often characterised by delayed or inaccurate communication. There is an urgent need to improve communication and information transfer between hospital-based and community`–based care in order to improve continuity of care, patient safety, patient and provider satisfaction and optimise resource use. A systematic review of 55 observational studies conducted between 1970 and 2005 that investigated communication and information transfer at hospital discharge was performed by Kripalani et al (2007). This review revealed a number of problems associated with this process including:
19
• Infrequent direct communication between hospital and primary care physicians (3-20%).

• Low availability of discharge summaries at the first post discharge visit (12-34%), that remained relatively low at four weeks (51-77%) negatively affecting quality of care and physician satisfaction in 25% of cases.
• Discharge summaries commonly lacked: diagnostic test results (33-63%), treatment/hospital course (7-22%), discharge medications (2-40%), test results pending at discharge (65%), patient or family counselling (90-92%) and follow up plans (2-43%).
The adverse outcomes of these findings included: higher readmission rates,
adverse effects on follow up management plans, and late actioning of diagnostic test results leading to delayed or incorrect diagnoses. Of the interventions reported for 18 of the studies in the systematic review, three of these were randomised studies. In the first of those, hand delivery of the discharge letter by the patient to the General Practitioner (GP) decreased delays in receipt of this information. The second involved computer-generated summaries that resulted in a higher rate of completion than dictated summaries and also increased and improved content of important items such as diagnosis (from 65% to 100%), pertinent findings and test results (from 87% to 99%) and discharge medications (from 93% to 100%). The third involved a multimodal enhanced discharge planning intervention using a combination of telephone call to GP, scheduling a follow up appointment with the patient and provision of educational booklets for patients and GPs. This was associated with GPs reporting higher rates of their understanding of the patients’ hospital management, quality of communication and involvement in post hospital care. The QH Enterprise Discharge Summary with integration with GPs will include the development and rollout of a standards-compliant electronic discharge summary that can be delivered to GPs or be made available to GPs via an external portal facility.
Belfrage et al (2009) trialled use of the envelope between Residential Aged
Care Facilities (RACFs) and EDs in Victoria as part of the ACSQHC CH research program and concluded that it was useful, easy to use, valued by staff and that it improved CH processes. The most significant outcome of the project was that it also raised awareness of the need for improved handover between those settings. Prior to the initiative, staff did not recognise handover as being necessary. There was a perception among staff that once the patient was dispatched, the responsibility for care was discharged and that the receiver would take over the patient’s care without a formal handover of information.
Silvester & Carr (2009) reported on the trialled implementation of Health
Record eXchange (HRX) since 2005 to share summary patient information between multidisciplinary health care professionals in North Brisbane. Outcomes included benefits to patients from a multidisciplinary, multisector, team-based approach to the planning and provision of care, an average reduction in inpatient associated costs of 26% for intervention and the facilitation of the flow of information between care team members. They concluded that, despite difficulties in implementation, significant benefits are derived from the use of electronic tools which provide essential infrastructure to support delivery of high quality multidisciplinary care team management of patients with complex needs.
3.6 What is best practice in CH?
20
Several authors and researchers worldwide have concluded that there is no one best practice model in CH, nor is there a ‘silver bullet’ or a ‘one size fits all’ strategy

for improving CH (Cohen & Hilligoss, 2009; Wong et al, 2008). This may be partly explained by the fact that the effectiveness of handover communication can only be defined with reference to a particular context. That is, information content, format and communication channel used will be determined by the needs arising from that context, and so it will need to be peculiar to and adapted to that context. And so, in turn, handover practices will also necessarily be context or situation-specific (Lardner, 1999). This is evident in the great variety of strategies, solutions and different approaches to handover available within, across and between health care organisations. The answer to ‘what is best practice in CH?’ is, ‘it depends” (on the situation or context). Similarly, what works in one context may not work in another.
It is widely recognised that a major contributing factor to patient harm is the lack of standardised approaches. Variation and complexity in practices and processes increases risks to patient safety. Furthermore, reliance on vigilance and memory as a way of ensuring patient safety is becoming increasingly prone to failure as the complexity of healthcare increases. A consistent approach to the prevention of clinical incidents involving CH across QH facilities is considered the most effective protection of patient safety (AIHW & ACSQHC, 2007; Wakefield, 2008). The Joint Commission in the US has mandated a standardised approach to handover communications, including an opportunity to ask and respond to questions. The Joint Commission has further recommended that a particular mnemonic (SBAR) be used for organising content and structure of handover communication (Pillow, 2007).
Recommendations for improving CH generally come from two main sources:
lessons learned from HROs and health care context-specific research (Cohen & Hilligoss, 2009). Several authors have expressed concern that the urgency of protecting patient safety by standardising CH may in itself entail risk. Efforts to standardise CH across different clinical settings may in fact jeopardise the other important functions of CH outlined previously in this consultation paper, such as the provision of social and professional support for staff and the promotion of individual, team and organisational learning. It may also introduce other unintended consequences or result in the adoption of a ‘quick fix’, satisficing approach rather than waiting for more evidence to support recommended strategies (Cohen & Hilligoss, 2009; Patterson, 2008; Patterson, 2007). 3.7 Flexible standardisation of CH
Given the warnings on standardisation of CH by experts in human factors and
lessons learned from HROs, the key to improving CH lies in flexible standardisation. The method of standardisation that is chosen should be flexible enough to meet the particular needs of the patients and staff who are the participants in handover. That is, it should be customised to the clinical setting, as well as balancing the need for improved coordination and continuity of patient care. Key features of flexible standardisation according to the OSSIE Guide to Clinical Handover Improvement (ACSQHC, 2009) include the following and these could form the basis of a CH policy:
• All participants know the purpose of handover, including required information and
how it is communicated.
21
• All participants know what documentation is required.

22
• Senior staff provide leadership and monitoring to ensure the form of handover that has been agreed upon locally to be best for patient safety and unit efficiency.
• All participants are free to attend handover on time and communicate the relevant information required to transfer responsibility and accountability.
• Adequate vigilance and coverage by staff is provided to ensure safe patient care during handover.
The Commission Website (www.safetyandquality.gov.au) also provides information on implementation of CH strategies and a range of tools to assist in effective CH. Additional information about Commission-sponsored research into CH is available in the Medical Journal of Australia; 190 (11) 1 June Supplement. 3.8 Communication channels
Communication channels are categorised according to their richness (Lardner,
1999). The following figure shows the relationship between the effectiveness and the richness of the communication channel used. Figure 3 Richness of communication channels
(Adapted from a PowerPoint presentation by Dr Ian Scott, Director of Internal Medicine, Princess Alexandra Hospital, Queensland Health) 3.9 Lessons learned from human factors experts, HROs and some healthcare examples on best practice in CH
There is some evidence to support recommendations for improvement in CH.
Observational work by human factors experts and organisational psychologists in HROs, such as oil refineries and NASA space missions, has provided some general guidance on best practice handover in health care (Patterson et al, 2004; Patterson, 2008; Lardner, 1999; Parke & Mishkin, 2005). The following are some specific recommendations from observational work in HROs during shift change handovers:
Face- face at the
bedside

3.9.1. Two-way, face-to-face interactive exchange of information According to organisational psychology, shift handover communication is
thought to be problematic because of a misalignment or incompatibility of mental models. A mental model is the internal mental representation held by an individual. It involves accurate alignment of present and future perceived system states (mental model) with actual system states. In the health care context, this might be, for example, a mental model of the patient’s diagnosis and how that needs to be managed. Where mental models are aligned or compatible between sender and receiver, it is not necessary for the receiver to feedback their understanding because the sender’s meaning is implicitly understood. This may in part explain why high-performing teams do not need to communicate as much as low-performing teams (Patterson, 2008). Where these differ (due to expertise, for example), or where abnormal or unstable conditions exist or where there is discontinuity in care processes, feedback becomes vital for both sender and receiver: the receiver (explicitly) confirms they have received, correctly interpreted and understood the message, and the sender (explicitly) confirms the message was successfully transmitted and can clarify any misunderstandings. Thus, shared understanding is achieved by the alignment of mental models through the process of face-to-face interactive verbal communication (Lardner, 1999).
Face-to-face communication does not involve the transfer of meaning from
one person to another; rather, the listener creates meaning in his/her own mind. Therefore unintentional meaning is likely and potential miscommunication is the norm rather than the exception. It is not surprising then that up to 75% of adverse events are associated with miscommunication. Communication channels are categorised according to their richness (Figure 3). Face-to-face communication is the richest channel because it provides for immediate feedback, thus allowing understanding to be checked and corrected in order to align mental models. Feedback is associated with increased accuracy and confidence in communication. Face-to-face communication is the most effective for mitigating ambiguity and creating shared understanding. (Lardner, 1999). Achieving understanding or comprehension by communication relates to use of information from dialogue, in combination with existing knowledge, to arrive at a shared meaning. Effective communication is aided by qualitative aspects of speech, such as assessments of comprehension, confidence, competence, phrasing, hesitancy and fluency (Lardner, 1996). Furthermore, face-to-face communication enables gestures, eye contact, tones of voice, and other rich and redundant aspects of interpersonal communication that can be used in conveying mental models (Parke & Mishkin, 2005). Effective communication requires effort by both parties and repetition of some sort is required to ensure comprehension, either intra-message or extra-message, within the message itself or over more than one communication channel (Lardner, 1999). 3.9.2 Face-to-face communication with written support 3.9.2.1 Shift-to-shift handovers
23
Information should be repeated via more than one medium or communication channel in order to introduce redundancy to communication thereby reducing the risk of miscommunication (Lardner, 1996). Face-to-face communication is improved when supported by structured written material, such as a checklist of items to convey

and/or position log or computer-generated pre-populated handover sheet to review. According to Lardner (1996), this style of handover is standing operating procedure in nuclear power plants, air traffic control and mission control for shuttle and space station operations. Without structure, communication tends to be variable in style and content. Written materials and checklists introduce redundancy in the verbal handover, reducing the risk of erroneous communication. They also allow one to specify ahead of time those aspects of communication that are most important and those that should be left out (i.e. elimination of unnecessary information). These written materials could be mandatory or discretionary and will depend upon the context and the particular patient care setting.
Communication is also improved when the content of handover captures
intent. Rather than just listing what occurred, handover should capture problems, hypotheses and intent. This involves critical analysis and a predictive diagnosis of the situation. Structured written materials should not only contain historical data, but should contain proactive content such as safety risks, what should happen (current plan) and what might happen and what to do in this situation (contingency plan). Perception and memory are organised by hierarchical goal representations and these in turn drive narrative comprehension, memory and planning. The advantage of such written material lies in assisting memory; cutting down unnecessary detail to ensure relevant information is passed between shifts and the ability to see at a glance where specific information is on one page (Parke & Mishkin, 2005; Lardner, 1999).
An experimental study by Behara et al (2007) among medical officers in the
UK, compared retention of information across handover cycles between verbal-only handover, verbal handover with written notes and verbal handover with accompanying pre-printed handout populated with all relevant patient information. After five handover cycles, 2.5% of information was retained using a verbal-only handover, 85.5% of information was retained using the verbal with note taking method, and 99% of information was retained using verbal handover with accompanying pre-printed handout containing all relevant patient information. There was no difference in loss of important or less important information between cycles. The results demonstrated that verbal information must be supplemented by a written component. The authors recommended the written component needs regular updating to ensure accuracy and that the advent of IT-assisted documentation and personal digital assistants (PDAs) may improve handwritten documentation. 3.9.2.2 Interdisciplinary team-based checklists, briefings and daily goals
24
According to a systematic review of interdisciplinary education and teamwork conducted by Hall & Weaver (2001), healthcare professionals learn their roles through the educational processes of their respective disciplines. This role then becomes part of their ‘cognitive map’ (“the whole cognitive and perceptual approach embraced by the discipline” as defined by Petrie (1976)). Healthcare professionals bring this conceptual map to the healthcare team. These preconceived maps of their roles based upon learned culture, beliefs and cognitive approaches within the disciplines may result in a poor understanding of other discipline’s roles and maps. This is thought to lead to anxiety, conflict and ineffective teamwork because the respective team members may not appreciate or realise the potential of other team members, causing them to underutilise team members’ expertise, exclude them from

vital communication and sharing of information and further difficulties in establishing effective communication among the disciplines. This is typically seen in the conflict that arises between doctors and nurses (Thomas et al, 2003). According to Mariano (1999), for effective teamwork to succeed there needs to be a degree of ‘role blurring’: overlapping competencies and shared responsibility. Suggestions for improved teamwork and clarification of each other’s roles include:
a) Clarification of roles and expectations. b) Identification of one’s own professional competencies and those of other
team members. c) Exploration of overlapping responsibilities. d) A renegotiation of role assignments.
Team members can only realise and truly gain insight into the importance of
each other’s roles by working together with problems in the real world. The solution therefore lies in establishing interdisciplinary teamwork education and training, in which there is role blurring and shared responsibility for patient care, team communication skills training, including for CH, conflict resolution skills training and leadership. These can be achieved either through formal team training initiatives or the use of situated learning in the workplace using a variety of ‘communication bridges’ such as checklists, team briefings, debriefing and huddles, MDT rounding and daily care or goal setting and discharge planning, with the patient as the focus of the team’s attention (Hall & Weaver, 2001; Pronovost et al, 2003; Lingard et al, 2008).
A checklist serves three purposes: firstly, it ensures critical information is not
overlooked; secondly, it provides a consistent order in which information should be communicated; and thirdly, it serves to ‘plug’ the holes in individual and team situational awareness (Mistry et al, 2008; McIlvaine, 2007). A brief introduction of team members including their respective roles further promotes team cohesion by improving team members’ appreciation of one another’s roles. Several studies have shown that ambiguity about roles and responsibilities, lack of leadership, different communication styles, hierarchy and status, as well as a lack of appreciation of team members’ information needs, are barriers to effective communication in MDT settings that contribute to errors and patient harm (Greenberg et al, 2007; Weller et al, 2008; Reader et al, 2007). Furthermore, the briefing, as for handover, should capture problems, hypotheses and intent involving critical analysis and a predictive diagnosis of the situation. The checklist should therefore not only contain historical data, but should contain proactive content such as safety risks, what should happen (current plan including rationale), what might happen/possible complications, and what to do in this situation (contingency plan) (Lardner, 1999; Parke & Mishkin, 2005). The post-operative debriefing allows the team to review what went well, what could be improved next time and promotes important situated learning not only for junior staff but for the whole operative team (Roberts et al, 2009).
25
The healthcare literature contains some notable examples of the benefits of using structured written documentation in conjunction with face-to-face communication in the OT and ICU environment where team-based care is the norm. The first of these is a worldwide study by Haynes et al (2009) that involved a pre-/post assessment of the use of a 19 item surgical checklist developed by the World Health Organisation (WHO). The checklist consists of an oral confirmation by

surgical teams of the completion of the basic steps for ensuring safe delivery of anesthesia, prophylaxis against infection, effective teamwork, and other essential practices in surgery. It is used at three critical junctures in care: before anesthesia is administered, immediately before incision, and before the patient is taken out of the operating room. Implementation of the checklist resulted in improved teamwork among OT staff, and significant reduction in the rate of death from 1.5% before the checklist was introduced to 0.8% afterward (P = 0.003). Inpatient complications also reduced from a baseline of 11.0% of patients to 7.0% after introduction of the checklist (P<0.001). The authors stated that implementation of the checklist required routine performance of team introductions, briefings, and debriefings; but that the exact mechanism of improvement was less clear and most likely multifactorial. Use of the checklist involved both changes in systems and changes in the behavior of individual surgical teams. To implement the checklist, all sites had to introduce a formal pause in care during surgery for preoperative team introductions and briefings and postoperative debriefings, team practices that have previously been shown to be associated with improved safety processes and attitude.
Lingard et al (2004; 2005; 2006; 2008) have observed team processes in the
OT in numerous studies and have used pre-operative checklists and team briefings in the OT as interventions to improve team collaboration and communication. Several studies have demonstrated the benefits and outcomes of improved communication between teams (such as improved collaboration, understanding of clinical goals, teamwork and communication) but did not objectively assess how communication improved. Lingard et al (2004) reported a recurrent set of communication problems in the OT: communication that was too late, inconsistent and inaccurate content, issues left unresolved until the point of urgency and exclusion of key individuals from discussions and decisions. Lingard et al (2008) sought to describe the precise nature of improvement in communication associated with checklist and pre-operative briefings and found that:
1) The intervention resulted in a marked decrease by 64% of communication failures
that were associated with at least one error. 2) Almost half of the communication events identified a problem, ambiguity, or
critical knowledge gap, provoked a change in plan or prompted follow-up action, thus having a direct impact on patient care by changing decisions or actions during the course of the surgical procedure.
26
3) Surveys of participant perceptions about the intervention revealed that the briefing allowed team members to identify and solve problems and helped guard against mistakes.
Another study was a prospective cohort study by Pronovost et al (2003) in
collaboration with the Volunteer Hospital Association, the Institute for Healthcare Improvement, and Johns Hopkins Hospital's 16-bed surgical oncology ICU involved multidisciplinary development and use of an ICU Daily Goals Worksheet. The main outcome variables were ICU length of stay (LOS) and percent of ICU residents and nurses who understood the goals of care for patients in the ICU. Baseline measurements were compared with measurements of understanding after implementation of a daily goals form. At baseline, less than 10 percent of residents and nurses understood the goals of care for the day. After implementing the daily goals form, greater than 95 percent of nurses and residents understood the goals of care for the day. After implementation of the ICU Daily Goals Worksheet, ICU LOS

decreased from a mean of 2.2 days to 1.1 days. During daily rounds in the ICU, the ICU team visits each patient, develops a plan of care for the day and completes the ICU Daily Goals Worksheet. The fellow or attending physician signs the worksheet and hands it to the patient’s nurse before moving on to the next patient. All providers, physicians, nurses, respiratory therapists, and pharmacists review the goals for the day and initial the worksheet three times a day. The team updates the worksheet if the goals of care change. The goal of the ICU Daily Goals Worksheet is to reduce ICU length of stay and mortality while increasing the care team’s understanding of the daily goals for patients in the ICU, including what work needs to happen for the patient to leave the ICU; what is the greatest safety risk to the patient; what are the key processes for ventilator patients; what are the scheduled labs for the patient; catheter; and what can be done to assist in facilitating communication with the family.
A more recent study by Henrickson et al (2009) involved the development and
pilot testing of a preoperative briefing protocol for cardiovascular surgery by collaboration between all members of the cardiac surgery team. Implementation was preceded by training for all staff in the use of the briefing protocol. Following implementation of the briefing protocol, there was a significant reduction in total surgical flow disruptions (5.4 per case pre-implementation vs 2.8 post-implementation, p=0.004), reductions in procedural knowledge disruptions (4.1 vs 2.17, p=0.004), and miscommunication events (2.5 vs 1.7, p=0.03). Another significant outcome of the briefings was improved morale among team members in the operating theatres. The authors stated that the briefing went beyond use of a checklist in that it accounted for the unexpected as well as the routine, expected errors that can be revealed using a checklist. The key success factor in the briefing protocol, according to the authors, has been proactive team management of error through a shared mental model of the procedure, including engagement, mutual awareness and information sharing between team members from the beginning of the procedure. The value of briefings is two-fold: (1) informational and (2) functional. Informational benefits are explicit confirmation, reminders, education and facts surrounding a case and are complemented by functional benefits such as promotion of problem identification, prompting of decision-making, and provoking follow-up actions. Remaining challenges include cultural barriers between and across different operating theatre environments, determination of the most appropriate time to hold the briefing and ensuring all team members are able to participate in the briefing. 3.9.2.3 Whiteboards/journey boards
27
Whiteboards function as a dynamic, concurrent representation of the state of a unit and are commonly used in most inpatient units within hospitals such as medical and surgical wards, EDs, OTs and ICUs. According to Wears et al (2007), the importance of the whiteboard is evident in its function to enable both within-group and between-group communication, planning and coordination across health care organisational boundaries. Like the structured checklist used by Haynes et al (2009) and the daily goals form used by Pronovost et al (2003), the whiteboard bridges the communication and coordination gaps between multidisciplinary teams. Healthcare teams are typically lacking formal structure, have shifting memberships and amorphorous boundaries. Each group has its own bounded view of patient care and of organisational operations. This creates great problems for inter-group coordination since each group has its own perceptions and interpretations of different slices of an “organisation’s reality”. Therefore, tools such as whiteboards are vital for bridging

gaps in the large and complex communication space created within the healthcare system (Wears et al, 2007).
In shift handovers the whiteboard is used extensively in the preparation phase
of CH (Wears et al, 2007). Out-going staff can use the information on the whiteboard to update the ‘state of the unit’ in preparation of documentation for handover and both out-going and in-coming can refer to the whiteboard during handover communication. During handover, staff can triangulate whiteboard displays with verbal, face-to-face handover communication with structured written or computer generated handover sheets to further increase accuracy and reliability of information, clarity of understanding, shared mental models, patient care planning, risk assessment and goal setting. This comes with the proviso that all staff update the whiteboard regularly (Chaboyer et al, 2009). The whiteboard also provides an overview function noted by Patterson et al (2004) as being key to improving safety and care coordination among and between health care teams by making it clear at a glance who is responsible for which duties at a particular time. It can also promote mutual support and appropriate resource allocation through monitoring of tasks and responsibilities of team members. Communication of risk status such as falls risk, or infectious status can be conveyed on the whiteboard and the addition of the names and contact numbers of which staff are responsible for the patient can also be displayed on the whiteboard. Other functions of the whiteboard include tracking patient movements, bed management, promotion of team collaboration, facilitation of timely referrals and improved patient flow (Wears et al, 2007; Chaboyer et al, 2009).
The location or placement of the whiteboard could raise issues of privacy and
concerns about patient confidentiality; however, these should not override issues of patient safety and can be overcome by not writing patients’ names on the whiteboard or by placing them in areas where they are not accessible to the general public (Garling, 2008; Chaboyer et al, 2009).
3.9.2.4 Bedside handover
Face-to-face communication at the bedside offers the richest form of
communication with regard to patient safety because it combines the benefits of verbal face-to-face interactive communication exchanges with written support and includes the patient and their bedside environment, including a review of current patient care related documentation (Figure 3). Transforming care at the bedside, better known as TCAB, has recently emerged as a framework for improving safety on medical and surgical wards in acute care hospitals. Several QH hospitals have introduced TCAB for nursing shift handover. Traditionally, nursing handovers have taken place away from patients in a separate room such as the nurses’ station or office. Chaboyer et al (2008) implemented a quality improvement initiative at Ipswich Hospital to improve nursing shift handover. Drivers for the change to bedside
28
Case study: Handover information was that the patient had been complaining of pain and that the anaesthetic doctor had been notified, but had not yet attended to assess pain. Patient had been complaining of being in significant pain for several hours. Assessment of patient post handover found the PCA was not attached to the patient and the morphine had been dripping onto the floor.

handover among nurses included waste of time during handovers; inclusion of insufficient and irrelevant information and ‘gossip’ during handover; lack of congruence between information received at handover and actual patient status; inability of doctors to locate a nurse who knew anything about a particular patient; and delays between in-coming staff completing handover and seeing their patients (Chaboyer et al, 2008).
Bedside handover has the potential to improve effective teamwork. Three
factors that influenced team performance in this study included: (1) Effective teams successfully integrated individual actions into the team. Bedside handovers took place with a number of nurses from both the outgoing and incoming staff as well as occasional membership of doctors and other staff. (2) Because healthcare teams function in a complex, dynamic system, coordination through effective communication of patient care-related information is crucial. By bringing groups of nurses and other health care staff together, it is possible that bedside handover facilitates such coordination. (3) Team leadership is an important factor in team performance. In the case of bedside handover, nurses noted that bedside handover provided opportunities for them to gain support from shift coordinators and team leaders (Chaboyer et al, 2008; Manojlovich, 2005).
3.9.3 Multidisciplinary/interdisciplinary teamwork & communication
It is widely held that multidisciplinary team (MDT) and interdisciplinary team (IDT) work and communication are essential to patent safety. Communication failure among health care providers is one of the most frequently cited causes of preventable harm to patients (Wilson et al, 1995). Poorly functioning teams and systematically faulty exchange of information within and between treating teams is a major contributing factor to patient harm (Chassin & Becher, 2002). The complexity of patient care has made multidisciplinary teamwork and communication ever more critical to the safety and efficiency of care, as noted above. It is important first to distinguish between MDTs and IDTs (Jessup, 2007). Table 3 outlines these differences.
Table 3 Differences between MDTs and IDTs
Multidisciplinary teams Interdisciplinary teams Comprised of members from different disciplines
Comprised of members from different disciplines
Each discipline approaches the patient from their own perspective
Common understanding and holistic view of the patient’s care
Consultations may be conducted separately or together
Separate consultations integrated into a single consultation with the patient
Common to meet without the patient present Patient is part of the decision making process Responsibility and accountability for patient care resides within the disciplines
Shared responsibility and accountability to augment and support the others’ contributions
Interdisciplinary communication usually via physician in-charge
Frequent communication, problem solving and working closely together to optimise patient care
29
IDTs are therefore more efficient and effective than MDTs through lack of duplication of effort, are patient-centred and may even identify system gaps not

always evident in MDTs. It is suggested that IDT members have shared responsibility for patient care because they work together as an integrated whole. Hall & Weaver (2001) describe this as a “continuum of interactions and responsibilities”. The risk of IDTs, as for MDTs, is that traditional hierarchies may dominate and impede open communication among team members. The Garling (2008) report on Acute Care Services in NSW Public Hospitals has concluded that multidisciplinary team ward rounds are essential to patient-centred, safe care. Recommendations made with respect to handover in the report included implementation of daily multidisciplinary ward rounds to improve patient centred care, team communication, and discharge planning, including note taking and supervision of junior doctors by seniors during handover. Similarly, Beach et al (2003) proposed system changes to improve patient safety. Significant among these, the recommendation to “Foster a culture that encourages communication and joint accountability through team and leadership training”. 3.9.4 Process/structure redesign options
According to Patterson (2008), the process of standardisation provides a
window of opportunity to restructure how work is normatively conducted. Nonetheless, there is still a need for flexibility within the structure to tailor the plan to a specific context, support exception handling for non-routine cases and enable adaptation to feedback about priorities when making trade-offs. Patterson (2008) stated that redesigning handover processes could be a first step to improving interdisciplinary coordination. Improvement in interdisciplinary coordination, in turn, might be a key leverage point for radically improving health care delivery.
It is beyond the scope of this consultation paper to recommend any process or
structural re-design options to improve CH but they are certainly worth considering in the broader context of patient safety, and quality and efficiency of the healthcare system overall. New care coordination models being introduced in the US include: shared decision making with non-doctors, collaborative cross-checking to increase system resilience (including across authority gradients), using information technology to make work more observable to team members and increasing access to specialised off-site expertise via telemedicine. Another way to manage health care complexity and improve CH would be to re-arrange shift, team, departmental and other work structures that often dictate when, where and who must be involved in CH. Efforts to improve CH would therefore be complemented by process redesign and restructuring of work practices as noted above (Cohen & Hilligoss, 2009).
3.9.5 Verbal orders and repeat-back, read-backs
30
When information is conveyed verbally, miscommunication may occur in a variety of ways, especially when transmission may not occur clearly (e.g. by telephone or if communication occurs under stress). To address this possibility, the military, civil aviation, and many high-risk industries use protocols for mandatory repeat-back and read-back, in which the listener either verbally repeats what was said or reads back this information once it has been written, so that the transmitter can then confirm its correctness. In health care, traditionally, read-back has been mandatory only in the context of checking to ensure accurate identification of recipients of blood transfusions. However, there are many other circumstances in which health care teams could benefit from following such protocols, for example, when communicating key

lab results or patient orders over the phone, and even when exchanging information in person (e.g. in handovers) (AHRQ, 2009).
The use of verbal orders has been identified as a risk to patient safety. Two
types of verbal orders identified are: (1) face-to-face and (2) telephone orders. Although the use of verbal orders has not been studied in depth, Wakefield & Wakefield (2009) have described the available literature and have proposed a model to identify potential error trigger points to serve as a basis for future research into verbal orders and patient safety. These errors are summarised in the following table. Table 4 Errors associated with verbal orders
Sources of verbal errors Reason for non-use of read-back/clarification
Causes of verbal order errors
Misspeaking Similar sounding medications
Incorrect communication of patient’s status
Background noise, difficulty hearing
Fear of appearing incompetent
Making the wrong decision
Muffled voices, accents, mispronunciations
Negative response from provider
Failure to seek clarification
Unfamiliar with patient’s status/condition
Failure to recognise lack of understanding
Failure to understand/read-back verbal order
Failure to understand Inadequate staffing/workload Transcription error Confusion Previous experience between
prescriber and order receiver
Use of unapproved abbreviations/doses
There is little literature available to provide any evidence for the effectiveness
of read-backs as a form of closed loop communication. A study by Barenfanger et al (2004) in three microbiology laboratories in three different hospitals in the US revealed a surprisingly high rate of errors by physicians despite being the receivers of the fewest calls about laboratory results. Of a total 822 telephone contacts made for critical lab results, 29 errors were made (overall error rate 3.5%). The major categories of errors were incorrect name of the patient, incorrect test result, incorrect specimen or test repeated, and refusal of the recipient to repeat the message. The error rate for physicians was 5%, nurses 3.4%, other 3.5% and ward clerks 0%. The authors noted that lab staff were reluctant to ask physicians to read-back the lab results over the phone even though nurses and ward clerks are asked to comply with this requirement. The authors stressed the importance of ensuring that read-backs are consistently used across healthcare systems to reduce the rate of avoidable errors associated with telephone reporting of critical lab results. According to Barenfanger et al (2004), the Joint Commission’s patient safety goals require that any laboratory test result that is defined as requiring a telephone report (e.g. critical value reporting) will require a read-back from the recipient. Recommendations from Wakefield & Wakefield (2009) to improve verbal order communication include:
31
Case study: Patient was ordered antibiotic by medical resident, medical resident verbalized the order to the registered nurse in charge of patient's care, medication not available on ward, medication not given, registrar not notified. Close to handover time and patient taken to EEG - not handed over to afternoon staff.

1) Specification of when verbal orders should and should not be used. 2) Specification of who is allowed and who is not allowed to give and receive verbal
orders. 3) What constitutes verbal orders and the related verbal content that must be
documented. 4) Limitations and prohibitions on the use of verbal orders. 5) Authorisation and validation of the verbal orders. 6) Strategies, techniques and specific actions to increase the clarity and effectiveness
of verbal orders. 7) Requirements for periodic monitoring and evaluation of verbal order practices and
compliance with organisational policies and procedures.
3.9.6 Team-based training strategies and solutions to promote resilience and enhance patient safety in CH
The opportunity for clinical information to be consistently conveyed between and within teams of health care professionals during CH relies on individual knowledge, skills and attitudes of teamwork and communication. Teamwork is essential to the provision of safe, high quality healthcare; yet there is little formal training in teamwork skills development in undergraduate or postgraduate healthcare professional education programs. Teamwork skills are typically learned on the job. There is a need for better preparation of health care professionals in teamwork where patient outcomes are dependent upon effective IDT work (Leggat, 2007).
The benefits of improved teamwork are well documented in the literature. In
general, teamwork results in: • enhanced team effectiveness, reduction in clinical errors and adverse outcomes
(Morey et al, 2002; Mann et al, 2006); • shorter length of stay, clarification of admission criteria, discharge needs and
acuity/staffing needs (Pronovost et al, 2003; Neily et al, 2004); • improved communication, morale and job satisfaction, reduced staff turnover
(Awad et al, 2005; Leonard et al, 2004); • reduction in adverse drug events (Haig et al, 2006); • increased efficiency (cost and time savings), lower stress and use of sick leave
(Neily et al, 2004); and,
32
• improved patient satisfaction (AHRQ, 2005). Research into teamwork has matured over the past two decades, and HROs
such as the aviation industry, nuclear power, and the military have now embraced formal team training. TeamSTEPPS (Team Strategies and Tools to Enhance Performance and Patient Safety) has evolved from the culmination of this research and has been made available by the Agency for Healthcare Research and Quality (AHRQ) and Department of Defence (DoD) for use in health care (King et al, 2007). It is a comprehensive training program designed to improve the way health care professionals communicate and work together as a team and is currently being implemented nationally throughout the US in healthcare facilities and universities, and statewide in South Australia (SA) (Powell, 2008; Kumar et al, 2008). Powell (2008) has summarised TeamSTEPPS in a white paper. TeamSTEPPS focuses upon four evidence-based learnable, teachable skills to improve team performance. Together, these comprise the necessary skills for team members to become adaptable

and flexible (i.e. resilient) in their interactions with one another and the complex sociotechnical system in which they work (Alonso et al, 2006): • Leadership — the ability to direct and coordinate activities of team members,
assess team performance, assign tasks, develop team knowledge and skills, motivate team members, plan and organise, and establish a positive team atmosphere,
• Situation monitoring (or mutual performance monitoring) — the capacity to develop common understandings of the team environment and apply appropriate strategies to monitor team-mate performance accurately),
• Mutual support (or back-up behaviour) — the ability to anticipate other team members' needs and to shift workload among members to achieve balance,
• Communication — including the efficient exchange of information and consultation with other team members.
More information on TeamSTEPPS may be obtained from the Website: www.teamstepps.ahrq.gov/. 3.9.7 Simulation as an adjunct to team training
Team training programs can benefit from additional use of simulation-based
training (Baker et al, 2005; 2006; Cohen & Hilligoss, 2009). This is a rapidly evolving technology that has potential to provide trainees with practice in realistic case scenarios without the risk of patient harm. Combining the use of video-taped feedback of such training opportunities provides a powerful method of feedback and reflection by trainees (Iedema et al, 2009). Regular, targeted simulation-based training is a priority for patient safety under the Queensland Health Patient Safety and Quality Plan 2008-2012. Consideration of the use of simulation for future team training in communication and handover is highly recommended. 4.0 Conclusion
In summary, there is no one size fits all strategy for CH across all QH clinical settings (Cohen & Hilligoss, 2009). The coordination of multiple approaches is more effective than reliance on an elusive “silver bullet” (Patterson et al, in Bognor, in press) and this requires extensive stakeholder consultation and flexible standardisation (Lillrank & Liukko, 2004; ACSQHC, 2009). The best identified strategies to provide a comprehensive improvement framework for CH combine both top-down (policy and implementation standard with roles, responsibilities and accountability in CH) with bottom-up approaches (interdisciplinary team based training in CH, communication and teamwork) to build capacity and resilience among interdisciplinary teams.
33

Bibliography Agarwal, S., Frankel, L., Tourner, S. et al (2008) Improving communication in a pediatric intensive care unit using daily patient goal sheets, Journal of Critical Care; 23(2): 227-235. Agency for Healthcare Research and Quality (AHRQ) (2005) Medical teamwork and patient safety: the evidence-based relation. Available at: http://www.ahrq.gov/qual/medteam/medteam2.htm#training Agency for Healthcare Research and Quality (AHRQ) (2009) AHRQ Patient Safety Network, Glossary. Accessed at http://www.psnet.ahrq.gov/glossary.aspx on 08.07.09 Albarran, J. & Scholes, J. (2008) Editors Note, Nursing in Critical Care; 13(3): 123. Alonso, A., Baker, D.P., Holtzman, A., Day, R. et al (2006) Reducing medical error in the Military Health System: How can team training help? Human Resource Management Review; 16: 396-415. Australian Institute of Health and Welfare (AIHW) & Australian Commission on Safety and Quality in Health Care (ACSQHC) (2007) Sentinel Events in Australian Public Hospitals 2004-05, AIHW: Canberra Aronsky, D., Jones, I., Lanaghan, K. et al (2008) Supporting Patient Care in the Emergency Department with a Computerized Whiteboard System, Journal of the American Informatics Association; 15: 181-194. Australian Council for Safety and Quality in Health Care (ACSQHC) (2005) Clinical Handover. http://www.safetyandquality.gov.au/internet/safety/publishing.nsf/Content/PriorityProgram-05 Australian Commission on Safety and Quality in Health Care (ACSQHC) (2009) OSSIE Guide to Clinical Handover Improvement, For clinician-leaders and managers, Consultation Edition, Sydney: ACSQHC. Australian Medical Association (AMA) (2006) Safe Handover: Safe Patients, Guidance on clinical handover for clinicians and managers, Australian Medical Association Limited. Awad, S.S., Fagan, S.P. Bellows, C. (2005) Bridging the communication gap in the operating room with medical team training, American Journal of Surgery; 190(5): 770-774. Baker, D.P., Gustafson, S., Beaubien, J., Salas, E., Barach, P. (2005) A Literature Review, Medical Teamwork and Patient Safety: the Evidence-based Relation, AHRQ. http://www.ahrq.gov/qual/medteam/.
34
Baker, D.P., Day, R. & Salas, E. (2006) Teamwork as an Essential Component of High-Reliability Organizations, Health Research and Educational Trust; 41(4): Part II (August 2006).

Barenfanger, J., Sautter, R.L. Lang, D.L. et al (2004) Improving Patient Safety by Repeating (Read-Back) Telephone Reports of Critical Information, American Journal of Clinical Pathology; 121: 801-803. Bark, P., et al. (1994) Clinical complaints: a means of improving quality of care, Quality in Health Care; 3(3): 123-32. Beach, C., Croskerry, P., Shapiro, M. (2003) Profiles in Patient Safety: Emergency Care Transitions, Academic Emergency Medicine; 10(4): 364-367. Bergman, R. (1981) Accountability: Definition and dimensions, International Nursing Review, 28(2), 53-59. Belfrage, M.K., Chiminello, C., Cooper, D., Douglas, S. (2009) Pushing the envelope: clinical handover from the aged-care home to the emergency department, MJA; 190(11): (Suppl) S117-120. Borowitz, S.M., Waggoner-Fountain, L.A., Bass, E., Sledd, R.M. (2008) Adequacy of information transferred at resident sign-out (inhospital handover of care): a prospective survey, Quality and Safety in Health Care; 17: 6-10. Botti, M., Bucknall, T., Cameron, P., et al (2009) Examining communication and team performance during clinical handover in a complex environment: the private sector post-anaesthetic care unit, MJA; 190(11): S157-160. Braithwaite, J., Runciman, W.B., & Merry, A.F. (2009) Towards safer, better healthcare: harnessing the natural properties of complex sociotechnical systems, Quality and Safety in Health Care; 18: 37-41. Bulau, J.M. (1992) Alleged failure to treat a technology-dependent infant in the home health care setting: a risk management case study, Journal of Home Health Care Practice; 5(1): 47-54. Cameron, P. (no date) Is there a framework for improving Patient Handover? Centre of Research Excellence in Patient Safety, PowerPoint presentation www.crepatientsafety.org.au/seminars/...handover/petercameron.pdf accessed 29.06.09 Carroll T. (2006) SBAR and Nurse-Physician Communication: Pilot testing an Educational Intervention, Nursing Administration Quarterly; 30(3): 295–299. Catchpole, K.R., De Leval, M.R., McEwan, A., Pigott, N., et al (2007) Patient handover from surgery to intensive care: using Formula 1 pit-stop and aviation models to improve safety and quality, Pediatric Anesthesia; 17: 470-478. Centre for Research Excellence in Patient Safety (CRE-PS) & ACSQHC (2007) Workshop Report, Developing a research framework and agenda for clinical handover, 24 February 2007, Mercure Hotel, Brisbane, QLD.
35

Chaboyer, W., McMurray, A., Johnson, J., Hardy, L., Wallis, M., Chu, S. (2008) Bedside Handover: Quality Improvement Strategy to “Transform Care at the Bedside”, Journal of Nursing Care Quality; 24(2): 136-142. Chaboyer, W., Wallen, K., Wallis, M., McMurray, A. (2009) Whiteboards: one tool to improve patient flow, MJA; 190(11): S137-140.
Chassin, M.R. & Becher, E.C. (2002) The Wrong Patient, Annals of Internal Medicine; 136(11): 826-833.
CHSRF (Canadian Health Services Research Foundation) (2008) HOW CAN WE IMPROVE COMMUNICATION BETWEEN HEALTHCARE PROVIDERS? LESSONS FROM THE SBAR (SITUATION, BACKGROUND, ASSESSMENT, RECOMMENDATION) TECHNIQUE, Insight and Action, Issue 47, November 2008. http://www.chsrf.ca/other_documents/insight_action/html/ia47_e.php Accessed 26.05.09
Clair, L. & Trussell, P.M. (1969) The change of shift report – study shows weakness, how it can be improved, Hospital; 43: 91-95. Clancy, C.M. (2006) Care transitions: a threat and an opportunity for patient safety, American Journal of Medicine and Quality; 21:415-417. Clancy, C & Tornberg, D. (2008) TeamSTEPPS: Integrating Teamwork Principles into Healthcare Practice, Agency for Healthcare Research and Quality. Clark, E., Squire, S., Heyme, A., Mickle, M-E., Petrie, E. (2009) The PACT Project: improving communication at handover; MJA; 190(11): S125-127. Cohen, M.D. & Hilligoss, P.B. (2009) Handoffs in Hospitals: a review of the literature on information exchange while transferring patient responsibility. Available at: http://deepblue.lib.umich.edu/bitstream/2027.42/61522/1/Handoffs_in_Hospitals_Draft_2009_01_28.pdf. Accessed 09.06.09 Coiera, E. (2006) Communication Systems in Healthcare, The Clinical Biochemist – Reviews; 27(2): 89-98. DAT (Data Analysis Team) (2009), SAC 1 Clinical Incidents Reported in PRIME-CI 2006-2007, Patient Safety Centre, Queensland Health, Brisbane. Dayton, K. & Henriksen, E. (2007) Teamwork and Communication, Communication Failure: Basic Components, Contributing Factors & the Call for Structure, Joint Commission Journal on Quality and Patient Safety; 33(1): 34-47. Denham, C.R. (2008) SBAR for Patients, Journal of Patient Safety; 4(1): 38-48. Dunn, E.J., Mills, P.D., Neily, J., et al (2007) Medical Team Training: Applying Crew Resource Management in the Veterans Health Administration, The Joint Commission Journal on Quality and Patient Safety; 33(6): 317-325.
36

Dunn, M.J.G., Gwinnutt, C.L., Gray, A.J. (2007a) Critical care in the emergency department: patient transfer, Emergency Medicine Journal. Emj.bmj.com accessed 22.06.09. Ekman, I. & Segesten, K. (1995) Deputed power of medical control: the hidden message in the ritual of oral shift reports, Journal of Advanced Nursing; 22: 1006-1011. ECRIInstitute (2006) Healthcare Risk Control, Risk Analysis, Risk and Quality Management Strategies 17, Communication, Supplement A, July 2006, pp.1-21. Fairbanks, R.J., Bisantz, A.M., Sunm, M. (2007) Emergency Department Communication Links and Patterns, Annals of Emergency Medicine; 50(4): 396-406. Finn, R. & Waring, J. (2006) Organisational Barriers to Architectural Knowledge and Teamwork in Operating Theatres, Public Money & Management, April 2006, pp117-124. Frost Gorder, P. (2004) Strategies Could Make for Safer Shift Changes at Hospitals, Press Release, Institute for Ergonomics, The Ohio State University, April 16 2004. Garling, P. (2008) Final Report of the Special Commission of Inquiry, Acute Care Services in NSW Public Hospitals, State of NSW through the Special Commission of Inquiry: Acute Care Services in New South Wales Public Hospitals. http:www.lawlink.nsw.gov.au/acsinquiry. Accessed 20/05/09. GPpartners (2009) Presentation of audit results for 93 RCAFs in Metro North HSD at Australian College of Health Services Executives (ACHSE) breakfast meeting held at Royal on the Park, Brisbane, March 2009. Guerlain, S., Adams, R.B., Turrentine, F.B., et al (2005) Assessing Team Performance in the Operating Room: Development and Use of a “Black-Box” Recorder and Other Tools for the Intraoperative Environment, American College of Surgeons; 200: 29-37. Haig, K. M., Sutton, S., & Whittington, J. (2006) National Patient Safety Goals. SBAR: A Shared Mental Model for Improving Communication Between Clinicians, Joint Commission Journal on Quality & Patient Safety, 32(3), 167-175. Haig, K. (2006) Eighth Annual NPSF Congress presentation, cited in Hospitals and Health Networks, Critical Communication and Patient Safety. Available at www.hhnmag.com/ accessed 22.05.09. Hall, P. & Weaver, L. (2001) Interdisciplinary education and teamwork, Medical Education; 35: 867-875. Hatten-Masterson, S.J. & Griffiths, M.L. (2009) SHARED maternity care: enhancing clinical communication in a private maternity hospital setting, MJA; 190(11): S150-151.
37

Haynes, A.B., Weiser, T.G., Berry, W.R., et al (2009) A Surgical Safety Checklist to Reduce Morbidity and Mortality in a Global Population, New England Journal of Medicine; 360: 491-499. Healey, A.N., Catchpole, K., Yule, S. (2008) Enhancing surgical systems, Cognition and Technology in Work; 10:251–254. Hohenhaus S. (2006) Enhancing patient safety during hands-off, American Journal of Nursing; 106: 72A–72C. Hollnagel, E., Woods, D. D., & Leveson, N. (2005). Resilience engineering. Concepts and precepts. Aldershot. UK: Ashgate, in bin Abd Hamid, H.S. (2007 Extended Situational Awareness and Resilience in Healthcare Systems. The 4th International Postgraduate Research Colloquium IPRC Proceedings, Thailand. Horn, J., Bell, M.D., Moss, E. (2004) Handover of responsibility for the anaesthetised patient – opinion and practice, Anaesthesia; 59: 658-663. Henrickson, S.E., Wadhera, R.K., ElBardisi, A.W., Wiegmann, A., Sundt, T.M. (2009) Development and Pilot Evaluation of a Preoperative Briefing Protocol for Cardiovascular Surgery, Journal of the American College of Surgeons; 208(6): 1115-1123. Iedema, R., Merrick, E.T., Kerridge, R., et al (2009) Handover – Enabling learning in Communication for Safety (HELiCS): a report on achievements at two hospital sites, MJA 190(11): (Suppl): S133-136. Jack, B.W., Chetty, V.K., Anthony, D. et al (2009) A Reengineered Hospital Discharge Program to Decrease Rehospitalisation, American College of Physicians; 150(3): 178-187. Jessup, R.L. (2007) Interdisciplinary versus multidisciplinary care teams: do we understand the difference? Australian Health Review; 31(3): 330-331. Johnson, J.K. & Barach, P. (2009) Patient care handovers: what will it take to ensure quality and safety during times of transition? MJA; 190(11):(Suppl) S110. Joint Commission, National Patient Safety Goals: 2006 Critical Access Hospital and Hospital National Patient Safety Goals, 2006. Jordan, P. (1991) Psychiatric ward handovers, Nursing Times; 87: 40-42. Jorm, C, & Iedema, R. (2008) Innovative Approaches to Enhancing Clinical Handover, Australian Commission on Safety and Quality in Health Care and University of Technology, Sydney. Kerr, M.P. (2002) A qualitative study of nursing shift handover practice and function from a socio-technical perspective, Journal of Advanced Nursing; 37(2): 125-134.
38

King, H.B., Battles, J., Baker, D.P., Alonso, A., Salas, E., Webster, J., Toomey, L., Salisbury, M. (2007) TeamSTEPPS: Team Strategies and Tools to Enhance Performance and Patient Safety. www.ahrq.gov/downloads/pub/advances2/vol3/Advances-King-1.pdf. Kripalani, S., LeFevre, F., Phillips, C.O. et al (2007) Deficits in Communication and Information Transfer Between Hospital-Based and Primary Care Physicians: Implications for Patient Safety and Continuity of Care, JAMA; 297(8): 831-841. Kumar, S., Schultz, T., Adams, R., Pirone, C., Wareham, C. Stead, K. (2008) Improving communication and teamwork in health care settings: processes and outcomes from implementing the TeamSTEPPS programme in South Australia. Poster presentation. Lardner, R. (1996) Offshore Technology Report – Effective Shift Handover, The Keil Centre, Edinburgh, Scotland. Lardner, R. (1999) Safe Communication at Shift Handover: Setting Implementation Standards, The Keil Centre, Edinburgh, Scotland. http://www.hse.gov.uk/humanfactors/comah/standards.pdf. Accessed 12.06.09 Lawrence, R.H., Tomolo, A.M., Garlisi, A. P., Aron, D.C. (2008) Conceptualising handover strategies at change of shift in the emergency department: a grounded theory study, BMC Health Services Research; 8: 256. doi:10.1186/1472-6963-8-256. Leggat, S.G. (2007) Effective healthcare teams require effective team members: defining teamwork competencies, BMC Health Services Research; 7:17. doi:10.1186/1472-6963-7-17. Lelean, S.R. (1973) Ready for Report Nurse? RCN Publications, London. Leonard, M., Graham, S., Bonacum, D. (2004) The human factor: the critical importance of effective teamwork and communication in providing safe care, Quality and Safety in Health Care: i85-i90. Lewin, K. (1947) Frontiers of Group Dynamics, Human Relations; 1: 5-41 Lillrank, P. & Liukko, M. (2004) Standard, routine and non-routine processes in health care, International Journal of Health Care Quality Assurance; 17(1): 39-46. Lingard, L., Espin, S., Whyte, S. et al (2004) Communication failures in the OR: an observational classification of types and outcomes, Quality and Safety in Health Care; 13: 330-334. Lingard, L., Espin, S., Rubin, B. et al (2005) Getting teams to talk: development and pilot implementation of a checklist to promote Interprofessional communication in the OR, Quality and Safety in Health Care; 14(5): 340-346.
39
Lingard, L., Regehr, G., Espin, S., Whyte, S. et al (2006) A theory-based instrument to evaluate team communication in the operating room: balancing measurement authenticity and reliability, Quality and Safety in Health Care; 14(6): 422-426.

Lingard, L., Regehr, G., Orser, B., Reznick, R., Baker, R., Doran, D., Espin, S., Whyte, S. et al (2008) Evaluation of Preoperative Checklist and Team Briefing Among Surgeons, Nurses, and Anesthesiologists to Reduce Failures in Communication, Archives of Surgery; 143(1): 12-17. LiveData (2009) Press release, 16 March 2009, The Johns Hopkins Hospital to Install LiveData OR-Dashboard, Driving Universal Protocol and SCIP Compliance. http://www.earthtimes.org/articles/show/the-johns-hopkins-hospital-to,750717.shtml# Maher, L. (2007) Sustainability, Australasian teleconference, Facilitated by Dr Duncan Stuart, Dr Lynne Maher, Head of Innovation Practice, NHS Institute for Innovation and Improvement, PowerPoint presentation. Manchester Patient Safety Framework (MaPSaF) (2006) NHS National Patient Safety Agency, The University of Manchester, United Kingdom. Mann, S., Marcus, R., Sachs, B. (2006) Lessons learned from the cockpit: How team training can reduce errors on L & D (Grand Rounds), Contemporary Ob/Gyn; 5(1): 34-42. Manojlovich M. (2005) The effect of nursing leadership on hospital nurses' professional practice behaviours, Journal of Nursing Administration; (7/8): 366–37. Mariano, C. (1999) The case for interdisciplinary collaboration, Nursing Outlook; 37(6): 285-288. Mascioli, S., Laskowski-Jones, L., Urban, S. et al (2009) Improving Handoff Communication; Nursing2009; February, pp. 52-55. McIlvaine, W.B. (2007) Situational awareness in the operating room: a primer for the anesthesiologist, Seminars in Anesthesia, Perioperative Medicine and Pain; 26: 167-172. Mistry, K.P., Jaggers, J., Lodge, A.J. et al (2008) Using Six Sigma Methodology to Improve Handoff Communication in High-Risk Patients. Accessed at http://www.ahrq.gov/downloads/pub/advances2/vol3/advances-mistry_114.pdf. On 13.07.09. Monroe, M. (2006) SBAR: A Structured Human Factors Communication Technique, http://www.asse.org/practicespecialties/Healthcare/docs/HealthBeat_Newsletter_Spring2006%20for%20Web.pdf. Accessed 26.05.09. Morey, J.C., Simon, R., Jay, G.D. et al (2002) Error reduction and performance improvement in the emergency department through formal teamwork training: Evaluation results of the MedTeams project, Health Services Research; 37: 1553-1581. Mudge, A., Laracy, S., Richter, K., Denaro, C. (2006) Controlled trial of multidisciplinary care teams for acutely ill medical inpatients: enhanced multidisciplinary care, Internal Medicine Journal; 36: 558-563.
40

National Patient Safety Association (NPSA) www.npsa.nhs.uk/ Neily, J., Dunn, E., Mills, P. (2004) Medical Team Training – An Overview, TIPS, VA National Centre for Patient Safety, 4(5): 1-4. Nestel, D. & Kidd, J. (2006) Nurses’ perceptions and experiences of communication in the operating theatre: a focus group interview, BMC Nursing; 5(1). Doi:10.1186/1472-6955-5-1. Parke, B. & Mishkin, A. (2005) Best Practices in Shift Handover Communications: Mars Exploration Rover Surface Operations, Proceedings of the International Association for the Advancement of Space Safety Conference, Nice, France, 25-27 October, 2005. Patient Safety Centre (PSC) (2008) Patient Safety: Clinical Handover, Final Report on Queensland Health Clinical Handover Pilot Program, October 2008. Patterson, E.S., Roth, E.M., Woods, D.D., et al (2004) Handoff strategies in settings with high consequences for failure: lessons for health care operations, Journal for Quality in Health Care; 16(2): 125-132 Patterson, E.S., Roth, E.M., Render, M.L. (2005) Handoffs during nursing shift changes in acute care, Proceedings of the Human Factors and Ergonomics Society Meeting; 1057-1061. Patterson, E.S. (2007) Communication Strategies From High-reliability Organisations. Translation is Hard Work, Annals of Surgery; 245(2): 170-172. Patterson, E.S., Woods, D.D., Cook, R.I., Render, M.L. (2007) Collaborative cross-checking to enhance resilience, Cognition and Technology in Work; 9: 155-162. Patterson, E.S. (2008) Commentary. Structuring flexibility: the good, bad and ugly in standardisation of handovers, Quality and Safety in Health Care, 17(1): 4-5.
Patterson, E.S., Cook, R.I., and Woods, D.D. Gaps and Resilience. In M. S. Bogner (ed.) Human Error in Medicine, second edition. Erlbaum, in press.
Petersen, L.A., et al. (1994) Does housestaff discontinuity of care increase the risk for preventable adverse events? Annals of Internal Medicine; 121(11): 866-872. Petrie, H.G. (1976) Do you see what I see? The epistemology of interdisciplinary inquiry, Journal of Aesthetic Education; 10: 29-43. Pillow, M. (2007) Ed. Improving Hand-Off Communication, Joint Commission Resources: Oakbrook Terrace, Illinois, US, in Cohen, M.D. & Hilligoss, P.B. (2009) Handoffs in Hospitals: a review of the literature on information exchange while transferring patient responsibility. Available at: http://deepblue.lib.umich.edu/bitstream/2027.42/61522/1/Handoffs_in_Hospitals_Draft_2009_01_28.pdf. Accessed 09.06.09
41

Plsek, P.E. & Greenhalgh, T. (2001) The challenge of complexity in health care, British Medical Journal; 323: 625-628. Pope, B.B., Rodzen, L. & Spross, G. (2008) Raising the SBAR: How better communication improves patient outcomes, Nursing; 38(3): 41-3. Porteus, J.M., Stewart-Wynne, E.G., Connolly, M., Crommelin, P.F. (2009) isobar – a concept and handover checklist: the National Clinical Handover Initiative, MJA; 190(11): S152-156. Powell, S.M. (2008) White Paper. TeamSTEPPS™- Strategies and Tools to Enhance Performance and Patient Safety: A Collaborative Initiative for Improving Communication and Teamwork in Healthcare. Priest, C.S. and Holmberg, S.K. (2000) A new model for the mental health nursing change of shift report, Journal of Psychosocial Nursing &Mental Health Services; 38(8): 36-43. Pronovost, P., et al. (2002) Building safety into ICU care, Journal of Critical Care; 17(2): 78-85. Pronovost, P., Berenholtz, S., Dorman, T., Lipsett, P.A., Simmonds, T., Haraden, C. (2003) Improving Communication in the ICU using daily goals, Journal of Critical Care; 18(2): 71-75. Queensland Government (2009) Queensland Health Patient Safety and Quality Plan 2008-2012, Queensland Government, Brisbane. Quin, D.M., Moulden. A.L., Fraser, S.H. et al (2009) Evaluation of the acceptability of standardised clinical handover tools at four Victorian health services, MJA; 190(11): S141-143. Reason, J. (2000) Human error: models and management, BMJ; 320: 768-770. Riesenberg, L.A., Leitzsch, J., Little, B.W. (2009) Systematic Review of Handoff Mnemonics Literature, American Journal of Medical Quality Online. DOI: 10.1177/1062860609332512. Accessed 25.05.09. Roberts, N.K., Williams, R.G., Kim, M.J., Dunnington, G.L. (2009) The Briefing, Intraoperative Teaching, Debriefing Model for Teaching in the Operating Room, American College of Surgeons; 208(2): 299-303. Rycroft-Malone, J., Fontenla, M., Seers, K. & Bick, D. (2009) Protocol-based care: the standardisation of decision-making? Journal of Clinical Nursing; 18(10): 1490-1500. Safety and Quality Council (2005) ‘Passing the baton of care – the patient relay’, Workshop Report 19 April 2005, Sydney, NSW.
42
Safety & Quality Council (2005) Clinical Handover and Patient Safety, Literature Review Report, March 2005.

Schein, E. H. (1995). Kurt Lewin’s change theory in the field and in the classroom: Notes toward a model of managed learning. http://www.sol-ne.org/res/wp/10006.html Senge, P. (1990) The Fifth Discipline. New York: Doubleday, 1990. Schultz, K., Carayon, P., Schoofs Hundt, A., Springman, S.R. (2007) Care transitions in the outpatient preoperative process: facilitators and obstacles to information flow and their consequences, Cognition and Technology in Work; 9: 219-231. Sharit, J., McCane, I., Thevenin, D.M., et al (2005) Examining issues in communicating patient care information across shifts in a critical care setting, Proceedings of the Human Factors and Ergonomics Society Meeting; 1062-1066. Sherlock, C. (1995) The patient handover: a study of its form, function and efficiency. Nursing Standard; 9: 33-36. Silvester, B.V. & Carr (2009) A shared electronic record: lessons from the coalface, MJA; 190(11): (Suppl) S113-116. Sims, D.E., Salas, E., Burke, S.C. (2004) Is there a “big five” in teamwork? 19th Annual Meeting of the Society for Industrial and Organisational Psychology, Chicago, IL. Smith, A.F., Pope, C., Goodwin, D., & Mort, M. (2008) Interprofessional handover and patient safety in anaesthesia: observational study of handovers in the recovery room, British Journal of Anaesthesia; 101(3): 332-337. Strange, F. (1996) Handover: an ethnographic study of ritual in nursing practice, Intensive and Critical Care Nursing; 12: 106-112 in Kerr, M.P. (2002) A qualitative study of nursing shift handover practice and function from a socio-technical perspective, Journal of Advanced Nursing; 37(2): 125-134. Stead, K., Kumar, S., Schultz, T., et al (2009) Teams communicating through STEPPS, MJA; 190(11): S128-132. TeamSTEPPS Implementation Guide, (2006). Available at: http://dodpatientsafety.usuhs.mil/index.php?name=Downloads&req=getit&lid=737. The Joint Commission (2006) Improving handoff communications: Meeting National Patient Safety Goal 2E, Joint Perspective Patient Safety, 6: 9-15 Thomas, E.J., Sexton, B.J., Helmreich, R.L. (2003) Discrepant attitudes about teamwork among critical care nurses and physicians, Critical Care Medicine; 31(3): 956-959. Thurgood, G. (1995) Verbal handover reports: what skills are needed? British Journal of Nursing; 4: 720-722.
43
Turner, P., Wong, M.C., Yee, K.C. (2006) Understanding interactions and factors influencing clinical handover: insights for information technology. Proceedings of the

15th Annual Health Informatics Conference, Health Informatics Society of Australia, Sydney. Volpp, K.G.M. & Grande, D. (2003) Residents’ suggestions for reducing errors in teaching hospitals, New England Journal of Medicine; 348: 851-855. University of Technology Sydney (UTS) Centre for Health Communication (2008) The National Clinical Handover Project: A Reflexive Tool for the Redesign of Clinical Handover. http://www.communication.uts.edu.au/centres/health/projects/clinical-handover/index.html Velji K, Baker GR, Fancott C, Andreoli A, Boaro N, Tardif G, Aimone E & Sinclair L (2008) Effectiveness of an adapted SBAR communication tool for a rehabilitation setting, Healthcare Quarterly; 11 (3 Spec No.): 72-79. Veltman, L. & Larison, K. (2007) PURE conversations: Enhancing communication and teamwork, Journal of Healthcare Risk Management; 27(2): 41-44. Wakefield, J. (2008) Patient Safety: From Learning to Action, Second Report on Clinical Incidents in the Queensland Public Health System 2006-07, Queensland Health, Brisbane. Wakefield, D.S. & Wakefield, B.J. (2009) Are verbal orders a threat to patient safety? Quality and Safety in Health Care; 18: 165-168. Wears, R.L., Perry, S.J., Wilson, S., Galliers, J., Fone, J. (2007) Emergency department status boards: user-evolved artifacts for inter- and intra-group coordination, Cognition and Technology in Work; 9: 163-170. Whyte, S., Lingard, L., Espin, S. (2008) Paradoxical effects of interprofessional briefings on OR team performance, Cognition, Technology and Work; 10: 287-294. Wilson, R.M., Runciman, W.B., Gibberd, R.W., Harrison, B.T., Newby, L., Hamilton, J.D. (1995) The Quality in Australian Health Care study, Medical Journal of Australia; 163: 458–71. Wong, M.C., Yee, K.C., and Turner, P. (2008) Clinical Handover Literature Review, eHealth Services Research Group, University of Tasmania. Woodhall, L.J, Vertacnik, L. & McLaughlin, M. (2008) Implementation of the SBAR communication technique in a tertiary center, Journal of Emergency Nursing; 34(4): 314-317. World Health Organisation (WHO) (2007) Communication During Patient Hand-Overs, Patient Safety Solutions; volume 1, solution 3. Yee, K.C., Wong, M.C., Turner, P. (2009) ‘HAND ME AN ISOBAR’: a pilot study of an evidence-based approach to improving shift-to-shift clinical handover, MJA; 190(11): S121-127.
44

Zimmerman, P.G. (2006) Cutting-edge Discussions of Management, Policy and Program Issues in Emergency Care, SBAR technique for patient handoffs, Journal of Emergency Nursing; 32:267-73. Zwarenstein, M. and Bryant, W. (2002) Interventions to promote collaboration between nurses and doctors (Cochrane Review), in Cochrane Database of Systematic Reviews; p.16.
45