Clinical Evaluation of Breast Diseases Joy Dorscher MD Department of Family Medicine and Community...
75
Clinical Evaluation of Breast Diseases Joy Dorscher MD Department of Family Medicine and Community Health [email protected]
-
Upload
madison-maxwell -
Category
Documents
-
view
219 -
download
0
Transcript of Clinical Evaluation of Breast Diseases Joy Dorscher MD Department of Family Medicine and Community...

Clinical Evaluation of Breast Diseases
Joy Dorscher MDDepartment of Family Medicine and Community [email protected]

Learning Objectives
Be able to identify:• Basic breast evaluation
• Basic breast imaging modalities
• Means of obtaining fluid/tissue for testing
• Tanner staging
• Breast disorders by age and gender

Embryologic Breast Development
• 5-7 weeks gestation
• Bilateral thickening of ectoderm
• Involutes except near the pectoral region
• Glandular development is dependant on placental hormones

Breast Self Examination

Clinical Breast Examination


Clinical Breast Examination
Lump or contour change
Skin tethering Nipple inversion Dilated vessels Ulceration Nipple scaling Edema or Peau
d’orange

Clinical Breast Examination
Lump or contour change
Skin tethering Nipple inversion Dilated vessels Ulceration Nipple scaling Edema or Peau
d’orange

Clinical Breast Examination
Lump or contour change
Skin tethering Nipple inversion Dilated vessels Ulceration Nipple scaling Edema or Peau
d’orange

Clinical Breast Examination
Lump or contour change
Skin tethering Nipple inversion Dilated vessels Ulceration Nipple scaling Edema or Peau
d’orange

Nature of Palpable Lesions
Firmness Irregularity of borders Focal Nodularity Fixation to skin or underlying
muscle Location-quadrant, distance from
nipple Size

Mammography Controversy
Annually (?) When to start (?) When to stop (?) False Positives (?)
Bottom lineMammography is not
the complete answer to breast cancer screening.

Mammography
Positioning Experience
Technologist Radiologist
X ray exposure

BI-RADSBreast Imaging Reporting and Data System
Category 0-6 Discuss results Assess risk Establish plan
Additional filmsRoutine intervalShort term F/UBiopsy

BI-RADS
Category 0- Incomplete
Category 1- Negative-Routine follow up, 5/10000
Category 2- Benign finding-Routine follow up,<2%
Category 3-Probably benign-short interval f/u, <2%
Category 4- Suspicious abnormality-Bx, 23-34%
Category 5- Highly Suggestive->Biopsy, 95%
Category 6- Known Malignancy-follow progress

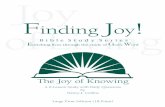
Malignant Breast Disease
6
10 7
T ime i n Y ea rs
No .O fC e lls
10 1 0
9
V isib le onM am mog raphy
P a lpab leL es ion
1 mm le si on
1 cm le si on
B a sed on an ave rage doub li ng tim e o f 100 day s
T aken fr o m Ob st e tric s a nd Gyne c ology 4 th Ed iti on 2002 ,L ipp inco tt, W illi am s, W ilk in s
M a mm o g ra p h ic a n d C li n ic al D et e ct io n o f B re a st Ma ss

BI RADS Category 0
Spot Compression Mammography is one of the methods that is used to further identify lesions on mammography
Ultrasound

Ultrasound
Analyzing cystic structures
Diagnosis with dense breasts
Not much value as a screening tool
3D ultrasound

Magnetic Resonance Mammography
Positives Breast implants and ruptures Highly sensitive to small
abnormalities Used effectively in dense
breasts Evaluate the extent of breast
cancer Can help determine type of
surgery needed May detect breast cancer
recurrences and residual tumors
Locate primary tumor in women with axillary lymph nodes
Useful in screening women at high risk for breast cancer
Equivocal mammogram
Negatives Time consuming Expensive Contrast agent (allergy or preg) Tolerate any claustrophobia MRI can be non-specific-2X bx Minimally invasive breast biopsy
techniques need to be further developed
Cannot image calcifications MRI centers cannot always
produce results cited in research studies
Inability to lie prone Extremely large breasts

Scintimammography
Uses Tc99m Sestamibi which concentrates in the mitochondria
Differences in uptake between normal and abnormal cells
Best when used for palpable lesions
May provide more functional information (drug resistance)
Has no value as a screening test

PET Scan
Metabolic activity Vascularization Oxygen
consumption Tumor receptor
sites Most helpful Least available Most expensive

eMed Aug 25,2008
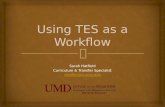
Imaging Modalities
Modality Sensitivity Specificity PPV Indications
Mammography 63-95%
(>90% palp
50% nonpalp
35% dense)
14-90%
(90% palp)
10-50%
(94% palp)
Asymptomatic, >35 screening, micro-calcifications
US 68-97% (palpable)
74-94% (palpable)
92% (palpable) Women < 35yo, cystic structures.
MRI 86-100% 21-97%
(<40% primary cancer)
52% Scar, implants, multiple lesions, borderline
Scintography 76-95% (palp)
52-91% (nonpalp)
62-94%
(94% nonpalpable)
70-83%
(83% palpable, 79% non palp)
>1cm axilla asses., predict drug resis.
PET 96%
(90% axillary metastasis)
100% Axilla assessment, scar, multifocal

Obtaining Tissue/Biopsy
Fine Needle Aspiration Core Needle Biopsy Excisional Biopsy Incisional Biopsy

Fine Needle Aspiration (FNA)
Palpable lesionCystic
structuresSolid masses
Malignant cells are loosely cohesive
Used less often

FNA
Positive Quick Painless Inexpensive No incision Minimal chance of
infection or bruising Immediate results Office procedure
Negative Less accurate Palpable lesion In situ vs. invasiveIn situ vs. invasive Cytotechnologist,
cytospin and slides Can’t use with
implants or lesions near chest wall

Core Needle Biopsy
Positive Quick Painless Inexpensive Small incision Minimal chance of
bruising/infection Can distinguish in situ vs.
invasive May avoid surgery If palpable> office
procedure Histologic assessment
ER, PR, Her2Neu
Negative Slightly less accurate May not provide
complete description of the tumor
If not palpable> hospital and possibly may still need surgery
Can not be used with breast implants or coumadin therapy or near chest wall

Incisional Biopsy
As for excisional biopsy with added complication of possibly needing more surgery.

Excisional Biopsy
Positive Accurate Provide complete
information about tumor
Rare false negative May be treatment
Negative Expensive Invasive/painful Time to heal Greater chance of
infection/bruising Change feel/look of
the breast Hospital procedure

Localization of Nonpalpable Lesions
Needle Localization Stereotactic Biopsy

Needle Localization
A wire is placed by radiologist for the surgeon to know what section of breast is abnormal
Can remove the tissue with the needle tip intact

Stereotactic Biopsy


Tanner staging-Female Breast
Preadolescent nipple is elevated with no underlying glandular tissue or increased pigmentation of the areola
(~11 yo)- glandular tissue in the subareaola is obvious. Nipple and breast are single mound off of the breast wall
(~12 yo) there is increase in the among of palpable glandular tissue with increased diameter and pigmentation of the areola breast and nipple in single plane.
(~13 yo) the areola further enlarges in a single plane, The nipple and areola form a separate mound above the level of the breast
(15 yo) there is a final development of a smooth contour with projection with nipple and areola

Tanner Staging-Female Genitalia
Prepubertal; no pubic hair Straight hair is extending
along and between the labia Pubic hair is increased in
quantity, darker and present in the typical female triangle
Pubic hair is more dense, curled and adult in distribution but less abundant
Abundant, adult type pattern hair may extend onto the medial aspect of the thigh

Tanner Staging -Male Preubertal, no pubic hair, genitalia
unchanged from early childhood Light colored hair develops laterally
and later becomes darker, penis and testes may be slightly larger, scrotal skin becomes more textured
Pubic hair is extended across the top of the penis; testes and scrotum are further enlarged; penis is larger especially in length
More abundant pubic hair with curling, genitalia resemble that of an adult, glans has become larger and broader
Quantity and pattern of pubic hair with hair present along the inner borders of the thighs. Testes and scrotum are adult in size.
1
4

Pediatric Breast Examination
Breast Buds Newborn Gynecomastia Mastitis Neonatorum

Pediatric Breast Congenital Anomalies
Polythelia Polymastia Athelia Amastia Amasia

Pediatric Breast Congenital Anomalies
Polytheliao Nipples
Polymastiao Breast
Athelia Amastia Amasia
Supernummary tissue
Failure of mammary ridge to regress in utero

Pediatric Breast Congenital Anomalies
Polythelia Polymastia Athelia
Absence of nipple/areola complex Amastia Amasia

Pediatric Breast Congenital Anomalies Polythelia Polymastia Athelia Amastia
o Absence of breast and nipple
o Pectoralis Muscle Amasia

Pediatric Breast Congenital Anomalies
Polythelia Polymastia Athelia Amastia Amasia
o Absence of breast tissueo Usually iatrogenic

Adolescent Female Breast Abnormalities Masses
FibroadenomaCystosarcoma phylloidesAbscessCystTrauma
DischargeMammary Duct Ectasia
All ages/both genders

Adolescent Female Breast Masses
FibroadenomaFibroadenoma Characteristics
Benign Proliferating epithelium and supporting fibrous
tissue Smooth, mobile, round (usually 1-3 cm) May be affected by menses
Treatment Monitor for 1-3 months
Considerations Removal may lead to iatrogenic amasia

Adolescent Female Breast MassesCystosarcoma phylloides Charactoristics
Cellular stroma with nuclear atypia and mitotic figures
May:o Have thinning increased vascularity of overlaying skino acutely enlarge
Painless Treatment
Excise with wide margins Considerations
Requires histologic differentiationo up to 25% are malignant

Adolescent Female Breast Masses
Abscess Characteristics
Behaves as an infection-because it iso Usually Staph or Strep
TreatmentRequires I & D +/- Abx

Adolescent Female Breast Masses
Cyst Characteristics
Mobile, round, nontender Treatment
Watch for 2-3 months Aspiration
o Diagnostic o May be curative

Adolescent Female Breast MassesTrauma Characteristics
May not recall insighting incidentMay cause a palpable mass
o peripheral calcificationso fibrotic scar o echogenic internal bands on ultrasound,
mammogram or MRM Treatment
Watchful waiting unless infected hematoma
ConsiderationsFuture abnormal imaging studies

Adolescent Female Breast DischargeMammary Duct Ectasia Charactorisitcs
Nipple discharge &/or breast mass in subaereolar region
All ages/both genders Benign lesion Self-limiting Usually unilateral Periductal fibrosis and inflammation with nipple
discharge +/- bloody discharge Treatment
Surgical removal Considerations
Dx on US

Normal Adolescent Breast Development Breast asymmetry at thelarche A homogenous enlargement of one
breast No distinct mass or discharge May or may not be breast tenderness May need ultrasound to make certain
diagnosis Treated with assurance and follow up
•Kleinfelter’s•Testicular feminization•Hormone secreting tumor•Hyper or hypo thryroidism•Cirrhosis•Drug use (cimetidine or marijuana)•Familial predisposition•Obesity
Gynecomastia in boysNormal (70%) to floridly abnormal

Genetic Breast Disorders in Adolescence
BRCA1 and BRCA2 Li-Fraumani Syndrome Cowden Syndrome Ataxia-telangectasia Syndrome Colon Cancer Gene mutations HBOC-Hereditary Breast and Ovarian
Cancer


Adult Benign Breast Disease
Fibrocystic Changes Fibroadenoma Lipoma Fat Necrosis Intraductal Papilloma Mammary Duct Ectasia Galactocele

Adult Benign Breast Disease
Fibrocystic Changes Characteristics
Fairly common Mastadynia Usually discrete masses Usually bilateral Increase in size and tenderness
just prior to menses +/- nipple discharge
Treatment controversial
Considerations Really is 32 different processes Nonproliferative changes Proliferative changes without
atypia Proliferative changes with atypia
May be a single cyst

Adult Benign Breast Disease
Fibroadenoma Characteristics
Solid round rubbery Freely moving Painless
Treatment 10% disappear
spontaneously Considerations
Hyperplastic process in single duct
Usually 20-30 year olds

Adult Benign Breast Disease
Lipoma Characteristics
Harmless fatty tumor Well defined Semi-firm Nontender
Treatment Surgical
Considerations Can occur anywhere on
the body

Adult Benign Breast Disease
Fat Necrosis Characteristics
due to trauma, surgery or radiation
Firm fixed hardIrregular borders
TreatmentInfected hematoma
ConsiderationsConsider abuse

Adult Benign Breast Disease
Intraductal Papilloma Characteristics
Wart-like growths in the lining of the mammary duct near the nipple
Typically not palpable +/- bloody discharge Usually 45-50 year old
Treatment Surgical removal

Adult Benign Breast Disease
Mammary Duct Ectasia Characteristics
Dilation of the mammary ducts Periductal fibrosis and
inflammation Nipple retraction is common
Treatment Surgical removal
Considerations Any age group

Adult Benign Breast Disease
Galactocele Warm Tender Associated with post
partum and/or breast feeding
Mastitis Infection
• Endemic• Epidemic
Chiari-Frommel Syndrome

Malignant Diseases of the Breast The average American woman has
a12% lifetime risk of developing cancer With a first degree relative the risk
increase 2-3 fold This increase to 9 fold if the disease was
bilateral in a premenopausal relative But only 5% of the breast cancers are
truly hereditary in nature

Risk Factors-Numerous
3 of 4 who get breast cancer do not have clearly identifiable risk factors
Possibly related to lifetime Estrogen exposure

Risks-vast and varied
Bone Mineral Density Weight gain in post menopausal
women ETOH OCPs (>10 years) EVIDENCE IS NOT STRONG TAKE HOME MESSAGE->STAY
TUNED

Epidemiology of Breast CancerWomen’s Health Initiative
Overall the breast cancer rates have increased 1.7% per year since 1990
Then in 1999 the rates began to decrease by 1% each year
Breast cancer incidence decreased in US women by 7-8% from 2002 to 2003.
The largest decrease was seen in ER positive breast cancers where they saw a decrease of 12% (ER negative decreased by 4%)
Hormone therapy dropped by 68% between 2001 and 2003

RR Factors related to increased risk
>4 Advanced age, No. Am or No. Europ. Descent, high perimenopausal IGF-1 and/or [E], h/o mother & sister with breast cancer
2-4 High SES, >30 yo at first FT preg., h/o cancer in 1 breast, 10 relative with Breast Cancer, h/o benign dysplastic lesion, mammo changes, or high dose ionizing radiation to the chest
1.1-1.9
Nulliparity, early menarche, late menopause, post menopausal obesity, high fat diet/sat fat-rich diet, suburban or no. US, white race >45 yo, black race, h/o endometrial or ovarian cancer
<1 Late menarche, BF > 1 year, monounsat fat-rich diet, phy. act, premenopausal obesity

One Theory of Breast CancerEarly Life Events
Mammary Gland Mass Seen in Caucasian with higher birth weights and
taller stature Growth enhancement
All growth enhancing factors are hormones and are involved in the underlying process that leads to breast cancer
Initiated cells Full term pregnancy after 35 yo has a slight transient
increase in risk (initiated clones are responding to the higher hormonal levels but there is protection later because of terminal differentiation of immature mammary cells)

Modified Gail Risk Factor Assessment Medical History of DCIS or LCIS Current age Age at menarche Age at first live birth Number of 10 relatives with breast
cancer Previous breast biopsy +/- atypia Race/ethnicity

Gail Risk Factor Assessment
Assess risk for five years and life time Under predicts:
Personal h/o lobular neoplasia over 60 multiple more distant relatives FH ovarian cancer or bilateral disease
Over predicts young women with first birth before 20 years of age
Does not take into account relatives unless first degree Does not look at other cancers such as ovarian Does not take into account age of diagnosis (pre vs. post menopause) or bilateral disease Does not take into account ethnicity ie. Ashkenazi Jews Doesn’t take into account bilateral disease or age of diagnosis therefore would underestimate BRCA

Paget’s Disease
Characteristics Long standing eczematous appearing rash of
nipple and areola complex Itching Tenderness Burning Occ. Bloody discharge Skin dimpling Peau d’orange
Treatment As eczema then biopsy

In Situ Cancer
LCIS From a terminal lobular apparatus Diffuse throughout the breast Non palpable 90-100% multicentricity 10-37% develop invasive carcinoma (bilateral)
DCIS Originates in ductal luminal cells Invasive cancer develops in 30-50% over a 10
years-usually in same location as original biopsy