Clinical Approach to the Disruptive Physician: The Tennessee Experience Anderson Spickard Jr., MD...
52
Clinical Approach to the Clinical Approach to the Disruptive Physician: The Disruptive Physician: The Tennessee Experience Tennessee Experience Anderson Spickard Jr., MD Anderson Spickard Jr., MD Reid Finlayson, MD Reid Finlayson, MD Ron Neufeld, LADC Ron Neufeld, LADC Roland Gray, MD Roland Gray, MD Bill Swiggart, MS, LPC/MHSP Bill Swiggart, MS, LPC/MHSP Charles Samenow, MD, MPH Charles Samenow, MD, MPH
-
Upload
kory-blake -
Category
Documents
-
view
219 -
download
1
Transcript of Clinical Approach to the Disruptive Physician: The Tennessee Experience Anderson Spickard Jr., MD...

Clinical Approach to the Clinical Approach to the Disruptive Physician: The Disruptive Physician: The
Tennessee ExperienceTennessee Experience
Anderson Spickard Jr., MDAnderson Spickard Jr., MDReid Finlayson, MDReid Finlayson, MDRon Neufeld, LADCRon Neufeld, LADCRoland Gray, MDRoland Gray, MD
Bill Swiggart, MS, LPC/MHSPBill Swiggart, MS, LPC/MHSPCharles Samenow, MD, MPHCharles Samenow, MD, MPH

IntroductionIntroduction

Distressed Physician Distressed Physician TeamTeam
Vanderbilt Center for Professional Vanderbilt Center for Professional HealthHealth
Anderson Spickard, Jr MD -- Anderson Spickard, Jr MD -- DirectorDirector
William Swiggart, MS, LPC/MHSP William Swiggart, MS, LPC/MHSP -- Training Director-- Training Director
Charles Samenow, MD, MPH -- Charles Samenow, MD, MPH -- Research AssistantResearch Assistant
Ron Neufeld, LADC -- Clinical Ron Neufeld, LADC -- Clinical Assessment, TeachingAssessment, Teaching
Tobi Fischel-Ingram, PhD -- Tobi Fischel-Ingram, PhD -- Teaching, CurriculumTeaching, Curriculum
Jennifer Blackford, PhD -- Jennifer Blackford, PhD -- BiostatisticsBiostatistics
David Dodd, MD -- TeachingDavid Dodd, MD -- TeachingDianna Phillips -- AdministrativeDianna Phillips -- AdministrativeJan Cao -- AdministrativeJan Cao -- Administrative
Vanderbilt Vanderbilt Comprehensive Comprehensive Assessment ProgramAssessment Program
Reid Finlayson, MDReid Finlayson, MD
Ron Neufeld, LCSWRon Neufeld, LCSW
Tennessee Medical Tennessee Medical FoundationFoundation
Roland Gray, MDRoland Gray, MD
Vince ParishVince Parish

ResearchResearch
Education, Education, PreventionPreventionAdvocacy, Advocacy, OutreachOutreach
Assessment Assessment and and TreatmentTreatment

VANDERBILT VANDERBILT COMPREHENSIVE COMPREHENSIVE
ASSESSMENT ASSESSMENT PROGRAMPROGRAM
…for Professionals…for Professionals
www.mc.vanderbilt.edu/root/www.mc.vanderbilt.edu/root/vcapvcap
615 322-4567615 322-4567
Reid Finlayson, MDReid Finlayson, MDRon Neufeld, LADCRon Neufeld, LADC

V-CAP MISSIONV-CAP MISSION
Providing the highest quality Providing the highest quality behavioral health evaluation and behavioral health evaluation and treatment planning services to treatment planning services to professionals in crisis due to professionals in crisis due to addictions, mental health issues, addictions, mental health issues, sexual boundary related problems sexual boundary related problems and burnout.and burnout.

Assessment ComponentsAssessment Components
Psychological TestingPsychological Testing MMPI – II; SCT; TAT; PAI; COPE Coping MMPI – II; SCT; TAT; PAI; COPE Coping
Scale; State-Trait Anger Expression Scale; State-Trait Anger Expression Inventory; DSFI (sexual functioning); Inventory; DSFI (sexual functioning); GARS (stress)GARS (stress)
Psychiatric Evaluation and Addiction Psychiatric Evaluation and Addiction ScreeningScreening MAST; DAST; SAST; BVI; TSI; BDI; Mini-MAST; DAST; SAST; BVI; TSI; BDI; Mini-
Mental Status Exam; Flooding self-testMental Status Exam; Flooding self-test

Assessment Components, Assessment Components, cont’d.cont’d.
Psychosocial Assessment and GenogramPsychosocial Assessment and Genogram Nursing AssessmentNursing Assessment Lab work and urine drug screenLab work and urine drug screen Other components as needed, including H&P, Other components as needed, including H&P,
AASI, Neuropsych workupAASI, Neuropsych workup Collaborative information from family, peers, Collaborative information from family, peers,
administrators, coworkers, etc. with written administrators, coworkers, etc. with written permission by clientpermission by client
Written report and review session with client and Written report and review session with client and designated othersdesignated others

Reasons for ReferralReasons for Referral
0
10
20
30
40
50
60
70
BoundaryViolations
DisruptiveBehavior
AddictionScreening
Court Return towork/Fit to
practice
MentalHealth
Screening

Disruptive ReferralsDisruptive ReferralsAxis I DiagnosisAxis I Diagnosis
Intermittent Explosive DisorderIntermittent Explosive Disorder Adjustment DisorderAdjustment Disorder Impulse Control DisorderImpulse Control Disorder None (or rule out)None (or rule out) Substance Dependence Substance Dependence (either active or (either active or
in remission)in remission)

Disruptive ReferralsDisruptive ReferralsAxis II DiagnosisAxis II Diagnosis
Personality Disorder, NOSPersonality Disorder, NOS Narcissistic (and other) traitsNarcissistic (and other) traits Compulsive personality traitsCompulsive personality traits OthersOthers

Problematic Physicians:Problematic Physicians:A Comparison of Personality Profiles by A Comparison of Personality Profiles by
Offense Type*Offense Type*
88 Physicians evaluated for “Fitness for Duty” 88 Physicians evaluated for “Fitness for Duty” 82 male (M age 46.8 / SD=9.5) 6 female (47.5 / 12.2)82 male (M age 46.8 / SD=9.5) 6 female (47.5 / 12.2) 80% married; 13% divorced; 7% single80% married; 13% divorced; 7% single 89% White; 5% Black; 4% Hispanic; 1% Asian89% White; 5% Black; 4% Hispanic; 1% Asian
A – Behavior Disruptive (anger, demeaning others)A – Behavior Disruptive (anger, demeaning others)
B – Sexual Boundary ViolationsB – Sexual Boundary Violations
C – Others (SUD, emotional instability, etc.)C – Others (SUD, emotional instability, etc.) All 3 groups similar demographics: age, race, marital status (all ps All 3 groups similar demographics: age, race, marital status (all ps
>.05) >.05)
* Canadian Journal of Psychiatry 2007 – in press

Problematic PhysiciansProblematic Physicians
MMPI -2 PAI MMPI -2 PAI CATEGORIESCATEGORIES
0
20
40
60
Ds Ch Nl nV
DisruptSexualOther
020406080
D I AS N
DisruptSexualOther
A - DISRUPTIVE N = 39A - DISRUPTIVE N = 39
B – SEXUAL N = 25B – SEXUAL N = 25
C – OTHER N = 24C – OTHER N = 24
CATEGORY ANALYSISCATEGORY ANALYSIS
MMPI-2MMPI-2: Ds=distress, Ch=character, Nl=normal, : Ds=distress, Ch=character, Nl=normal, nV=invalidnV=invalid
PAIPAI: D=distress, I-interpersonal, AS=antisocial, : D=distress, I-interpersonal, AS=antisocial, N=normalN=normal

Problematic PhysiciansProblematic Physicians A (Disruptive)A (Disruptive)
Valid profiles, open, high interpersonal dysfunction, Valid profiles, open, high interpersonal dysfunction, admit and rationalize angeradmit and rationalize anger
B (Sexual) – FEWEST NORMAL PROFILESB (Sexual) – FEWEST NORMAL PROFILES - MOST CHARACTER PATHOLOGY- MOST CHARACTER PATHOLOGY
Impulsive, selfish, low empathy, irresponsibleImpulsive, selfish, low empathy, irresponsible Exaggerated positive light = Therapeutic Challenge Exaggerated positive light = Therapeutic Challenge
C (Other)C (Other)

Tennessee Medical Tennessee Medical Foundation’s Foundation’s
Physician Health Physician Health ProgramProgramRoland Gray, MDRoland Gray, MD
Medical DirectorMedical Director

Statistics for 2002-Statistics for 2002-20062006
2002-2006 YTD2002-2006 YTD
Identifications:Identifications:
ChemicalChemical 335335
BehavioralBehavioral 194194
PsychiatricPsychiatric 5858
Sexual Sexual BoundaryBoundary
5656
Over-Over-prescribingprescribing
2424
TOTALTOTAL 667667

““Distressed Physician” Distressed Physician” CME CourseCME Course
www.mc.vanderbilt.edu/cph
William Swiggart, MS, William Swiggart, MS, LPC/MHSPLPC/MHSP

Center for Center for Professional Professional
HealthHealthContinuing Medical Education Continuing Medical Education CoursesCourses
Prescribing Controlled Prescribing Controlled Drugs Drugs
Maintaining Proper Maintaining Proper Boundaries Boundaries
Disruptive/Distressed Disruptive/Distressed PhysicianPhysician

A Program for Distressed A Program for Distressed PhysiciansPhysicians
Physicians appropriate for referral:Physicians appropriate for referral: Physician is currently workingPhysician is currently working Physician does not require residential Physician does not require residential
treatmenttreatment Physician has some support for change Physician has some support for change
i.e., the State Physician Health Program i.e., the State Physician Health Program or institutional or group practice supportor institutional or group practice support

Differential DiagnosisDifferential Diagnosis
Substance abuse or dependenceSubstance abuse or dependence Medical illnessesMedical illnesses Stress (career choice, Stress (career choice,
personal/family, skills personal/family, skills issues,etc.)issues,etc.)
Psychiatric disorders Psychiatric disorders

When “a little chat” When “a little chat” doesn't workdoesn't work
Mr. Bangsiding felt (and wrongly so) that a littlechat would be enough to stop Bob’s disruptive
behavior.

A Program for Distressed A Program for Distressed PhysiciansPhysicians(Phase I)(Phase I)
Components:Components: Comprehensive EvaluationComprehensive Evaluation Screening with additional measuresScreening with additional measures
Trauma (Trauma Symptom Inventory™)Trauma (Trauma Symptom Inventory™) Flooding Flooding (Gottman)(Gottman)
Workplace assessment (PULSE)Workplace assessment (PULSE) Phone interviewPhone interview Collateral interviewCollateral interview

FloodingFlooding
1.1. After a conflict I want to keep away After a conflict I want to keep away or isolate for a while.or isolate for a while.
2.2. I can never seem to soothe myself I can never seem to soothe myself after a conflict.after a conflict.
3.3. When I get negative, stopping it is When I get negative, stopping it is like trying to stop an oncoming like trying to stop an oncoming truck.truck.
4.4. I can never tell when a blowup is I can never tell when a blowup is going to happen.going to happen.

FloodingFlooding
The average flooding score was The average flooding score was reduced by 50% from the pre-reduced by 50% from the pre-course test. course test.
Pre-course average = 8.29Pre-course average = 8.29
Post-course average = 4.06Post-course average = 4.06
Range 0-24Range 0-24

Components of the Components of the ProgramProgram(Phase II)(Phase II)
Three-day CME course up to 46.5 CMEThree-day CME course up to 46.5 CME Didactic lectures - e.g., shame reaction, Didactic lectures - e.g., shame reaction,
family of origin connections family of origin connections GenogramGenogram Teach Specific tools/skills – e.g., Teach Specific tools/skills – e.g.,
grounding skills, Alter sheet, grounding skills, Alter sheet, communication strategiescommunication strategies
Role-playingRole-playing HomeworkHomework

Role Play ExerciseRole Play Exercise
Describe an incident you are Describe an incident you are concerned about.concerned about.
Who was there?Who was there? Pick someone to play you.Pick someone to play you. A powerful cathartic exercise A powerful cathartic exercise
viewing their behavior from multiple viewing their behavior from multiple points of view.points of view.
Example.Example.

Components of the VUMC Components of the VUMC ProgramProgram
(Phase III)(Phase III) Three follow-up sessions with the core Three follow-up sessions with the core
group over the next six months; group over the next six months; importance of group processimportance of group process
Repeat workplace assessment (PULSE)Repeat workplace assessment (PULSE)
Workbook (Workbook (The Anger Book, The Anger Book, M McKay, M McKay, P Rogers, 2000)P Rogers, 2000)

Characteristics Characteristics and Behavioral and Behavioral Change in the Change in the
First 20 First 20 Disruptive Disruptive PhysiciansPhysiciansCharles P. Samenow, MD, Charles P. Samenow, MD,
MPHMPHDepartment of PsychiatryDepartment of PsychiatryVanderbilt University Vanderbilt University Medical CenterMedical Center

DemographicsDemographics
Total Physicians Studied = 20Total Physicians Studied = 20 Mean Age: 44.6 (compare to CPH mean Mean Age: 44.6 (compare to CPH mean
age 49)age 49) Age Range: 27 - 61Age Range: 27 - 61 Predominantly Male (90%) and Predominantly Male (90%) and
Caucasian (100%)Caucasian (100%) 60% Married, 30% Divorced (1/2 60% Married, 30% Divorced (1/2
multiple)multiple) States Represented: 11States Represented: 11

Specialty TypesSpecialty TypesEmergency Emergency MedicineMedicine
3 (5%)3 (5%)
Family MedicineFamily Medicine 2 (10%)2 (10%)
Internal Medicine Internal Medicine (Specialty)(Specialty)
6 (30%)6 (30%)
Ob/GynOb/Gyn 3 (15%)3 (15%)
PathologyPathology 1 (5%)1 (5%)
Pediatrics Pediatrics (General)(General)
1 (5%)1 (5%)
Pediatrics Pediatrics (Specialty)(Specialty)
1 (5%)1 (5%)
Surgery Surgery (General)(General)
2 (10%)2 (10%)
Surgery Surgery (Specialty)(Specialty)
2 (10%)2 (10%)

Referral SourcesReferral Sources
Employer (35%)Employer (35%) PHP (35%)PHP (35%) Board of Licensure (15%)Board of Licensure (15%) Treatment Center (10%)Treatment Center (10%) Self (5%)Self (5%) Other (5%)Other (5%)

AggressiveAggressive
Anger outburst, verbal threats, swearing (90%) Physical contact and throwing objects (20%)
Sexual Harassment (10%)
PassivePassiveAggressiveAggressive
Derogatory comments about institution, hospital, group, etc.
Refusing to do tasks (20%)
PassivePassive
Chronically late, not responding to call (15%)
Inappropriate/inadequate chart notes, not dictating (15%)
Categories of Reported Disruptive Categories of Reported Disruptive BehaviorsBehaviors

InterventionsInterventions
Confrontation by Practice (95%)Confrontation by Practice (95%) Required Assessment (35%)Required Assessment (35%) Involvement of PHP (35%)Involvement of PHP (35%) Formal Disciplinary Action (30%)Formal Disciplinary Action (30%) Board of Licensure Involvement Board of Licensure Involvement
(10%)(10%) Termination (10%)Termination (10%)

Physician Mental HealthPhysician Mental Health
Previous Psychotherapy (65%)Previous Psychotherapy (65%) Previous Psychotropic Medications Previous Psychotropic Medications
(25%)(25%)

Study DesignStudy Design
Retrospective, Cohort DesignRetrospective, Cohort Design Total Physicians: 20Total Physicians: 20 Behavior Measured By PULSEBehavior Measured By PULSE
Motivating BehaviorsMotivating Behaviors Disruptive BehaviorsDisruptive Behaviors Motivating Impact on OthersMotivating Impact on Others Disruptive Impact on OthersDisruptive Impact on Others Both Self and “Others” (Colleagues, Both Self and “Others” (Colleagues,
Staff, Supervisors)Staff, Supervisors)

Study DesignStudy Design
Pre-Course PULSE: 15Pre-Course PULSE: 15 3-month Follow-up PULSE: 143-month Follow-up PULSE: 14 6-month Follow-up PULSE: 56-month Follow-up PULSE: 5 Average # of “Others”: 20Average # of “Others”: 20

General TrendsGeneral Trends
At 3 months, significant changes in At 3 months, significant changes in all domainsall domains Increased motivating behaviors and Increased motivating behaviors and
motivating impactmotivating impact Decreased disruptive behaviors and Decreased disruptive behaviors and
disruptive impactdisruptive impact Changes in behavior reported by Changes in behavior reported by
“others” more significant than “others” more significant than changes reported by self.changes reported by self.

Mean Motivating Mean Motivating Behaviors As Measured Behaviors As Measured
by Self and Othersby Self and Others
1
1.5
2
2.5
3
3.5
4
4.5
5
Pre-Course Post-Course (3-months)
SelfOthers
Self p =.12 “Others” p < .001

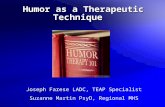
Mean Change in Mean Change in Disruptive Behaviors as Disruptive Behaviors as Measured by Self and Measured by Self and
OthersOthers
1
1.5
2
2.5
3
3.5
4
4.5
5
Pre-Course Post-Course (3-months)
SelfOthers
Self p = .14 “Others” p < .001

General Trends General Trends (Continued)(Continued)
Analysis of individual physicians Analysis of individual physicians demonstrates:demonstrates: Improvement in 12 of the 14 physiciansImprovement in 12 of the 14 physicians Although mean behaviors do not seem Although mean behaviors do not seem
severe, most physicians demonstrated severe, most physicians demonstrated severe behavioral problems in one or severe behavioral problems in one or more domains.more domains.
Reports of disruptive behavior was not Reports of disruptive behavior was not consistent across setting or those who consistent across setting or those who observed it. observed it.

Change in Motivating Change in Motivating Behaviors for Individual Behaviors for Individual Physicians as Measured Physicians as Measured
by Othersby Others
2.5
2.7
2.9
3.1
3.3
3.5
3.7
3.9
4.1
4.3
4.5
Pre-Course Post-Course

Mean % Change in Mean % Change in Disruptive Behaviors (by Disruptive Behaviors (by Severity) as Measured by Severity) as Measured by
OthersOthers
0
5
10
15
20
25
30
35
40
Pre-Course Post-Course
SevereBorderlineGood

OverheadsOverheads

Who is effected?Who is effected?
Colleagues 100%Colleagues 100% Staff (Hospital and/or Practice) 77%Staff (Hospital and/or Practice) 77% Supervisors 63%Supervisors 63% Direct effects on patients are rareDirect effects on patients are rare

General TrendsGeneral Trends
6-month data demonstrates potential 6-month data demonstrates potential for maintenance or improvement in for maintenance or improvement in behavioral changebehavioral change
Limited by small sample sizeLimited by small sample size

6-Month Trends for 6-Month Trends for Disruptive Behavior Disruptive Behavior
Change as Measured by Change as Measured by OthersOthers
0
0.5
1
1.5
2
2.5
3
Pre-Course Post (3 months) Post (6-months)

LimitationsLimitations
Most behaviorally severe physicians Most behaviorally severe physicians may not be includedmay not be included
Difficult to determine the role the Difficult to determine the role the CME course plays in causing CME course plays in causing behavioral changebehavioral change
Difficulty in measuring longitudinal Difficulty in measuring longitudinal changechange

Lessons Learned Lessons Learned Program for Program for Distressed Distressed PhysiciansPhysicians
Anderson Spickard Jr., MDAnderson Spickard Jr., MD

Lessons Learned Lessons Learned Physicians are referred by physician health Physicians are referred by physician health
programs, hospital or practiceprograms, hospital or practice Full psychiatric assessment not always Full psychiatric assessment not always
necessarynecessary Group process addressed the loneliness of Group process addressed the loneliness of
their professiontheir profession Participants were younger than other coursesParticipants were younger than other courses Collateral information was vitalCollateral information was vital Physicians with narcissistic traitsPhysicians with narcissistic traits

Lessons LearnedLessons Learned
A number of them already in outpatient A number of them already in outpatient therapy or open to that recommendation therapy or open to that recommendation by this team as another component to by this team as another component to their “recovery”their “recovery”
Some unhappy in their careerSome unhappy in their career Considered good physicians technicallyConsidered good physicians technically More open than expectedMore open than expected They liked the experiential aspects of They liked the experiential aspects of
the program especially group interactionthe program especially group interaction

Lessons LearnedLessons Learned PULSE indicates behavioral change for a PULSE indicates behavioral change for a
subset of physicians is not only possible, subset of physicians is not only possible, but can be maintained.but can be maintained.
Even when not statistically significant, Even when not statistically significant, large effect sizes and physician large effect sizes and physician testimonials point to a promising testimonials point to a promising interventionintervention
Future studies needed to identify which Future studies needed to identify which physicians are most likely to succeed and physicians are most likely to succeed and to understand role that system plays in to understand role that system plays in enabling/facilitating behaviors.enabling/facilitating behaviors.