Clinical and topographic magnetic resonance imaging characteristics of suspected thalamic infarcts...
5
Clinical and topographic magnetic resonance imaging characteristics of suspected thalamic infarcts in 16 dogs Rita Gonçalves a, * , Inés Carrera b , Laurent Garosi c , Peter M. Smith a , J. Fraser McConnell a , Jacques Penderis b a Department of Veterinary Science, Small Animal Teaching Hospital, University of Liverpool, Leahurst, Chester High Road, Neston CH64 7TE, UK b Institute of Comparative Medicine, Faculty of Veterinary Medicine, University of Glasgow, Glasgow G61 1QH, UK c Davies Veterinary Specialists, Manor Farm Business Park, Higham Gobion, Hertfordshire SG5 3HR, UK article info Article history: Accepted 30 March 2010 Keywords: Thalamus Cerebrovascular Stroke Anatomy Dog abstract Sixteen dogs with acute-onset, non-progressive signs of brain dysfunction and magnetic resonance imag- ing (MRI) characteristics compatible with thalamic infarction are described. Topographically the MRI lesions could be grouped in three thalamic regions, namely, paramedian (8/16), extensive dorsal (5/16) and ventrolateral (3/16). Paramedian lesions resulted in signs typical of vestibular dysfunction. Extensive dorsal lesions were associated with vestibular ataxia, circling and contralateral menace response deficits. Ventrolateral lesions resulted in circling and contralateral proprioceptive deficits. In several dogs, regions other than the thalamus were also affected: four extended into the midbrain; six extended to the internal capsule, and two dogs had a second lesion in the cerebellum. Three clinical syndromes were identified in association with thalamic infarction. These signs varied somewhat, most likely because lesions were not confined to specific nuclear boundaries and involved different combinations of thalamic nuclei. Ó 2010 Elsevier Ltd. All rights reserved. Introduction Cerebrovascular disease is increasingly recognised in dogs. It represents an abnormality of the brain caused by a disturbance in blood supply (Kalimo et al., 2002) and its clinical manifestation, also known as cerebrovascular accident or stroke, can be broadly divided into ischemic (resulting from arterial or venous obstruc- tion) or haemorrhagic (resulting from rupture of blood vessels). The term infarction describes the area of necrotic tissue resulting from ischemia and the subsequent neuronal and glial cell death (Adams and Victor, 1997). With the advent of advanced imaging techniques in veterinary practice our understanding of brain infarction in dogs is increasing. Recent studies have described the magnetic resonance imaging (MRI) characteristics, topographic distribution of lesions and sus- pected underlying causes of brain infarction in dogs (Garosi et al., 2005, 2006). MRI findings include well-defined, sharply demar- cated lesions with minimal to no mass effect that are limited to the vascular territory of a main cerebral or perforating artery and that are hyperintense on T2-weighted images (T2WI) and/or fluid attenuated inversion recovery (FLAIR) images. Concurrent medical conditions have been reported in approximately half of the cases and most commonly include chronic kidney disease and hyperadrenocorticism. In humans, a correlation between clinical syndromes, imaging findings and location of the infarction, stroke mechanism (embolic or thrombotic) and possible concurrent medical conditions has been found. This has not been feasible in dogs (Garosi et al., 2005). Cerebellar infarcts within the vascular territory of the ros- tral cerebellar artery have been most commonly identified, fol- lowed by similar numbers of telencephalic infarcts within the regions of the rostral and middle cerebral arteries and striate arter- ies and thalamic/midbrain infarcts within the territory of the cau- dal perforating arteries (Garosi et al., 2006). In humans, four distinct clinical syndromes associated with thalamic infarctions are recognised (Schmahmann, 2003): anterior, paramedian, infero- lateral and posterior infarcts, representing obstruction of the tuberothalamic, paramedian, inferolateral and posterior choroidal vessels, respectively (Schmahmann, 2003; Saez de Ocariz et al., 1996; Wang et al., 2008). Three variant types (anteromedian, cen- tral and posterolateral infarcts) have also been described and their existence is thought to be related to either variations of the terri- tories supplied by the thalamic arteries or to the occurrence of hemodynamic (borderzone) mechanisms (Carrera et al., 2004). In the dog, the blood supply of the thalamus differs from that of humans (Inoue et al., 1985; Brenowitz and Yonas, 1990; Garosi et al., 2006) and derives predominantly from three blood vessels (Table 1). Although thalamic infarcts accounted for only 15% of sus- pected brain infarctions in the dog in one recent study (Garosi et al., 2006), our clinical experience is that thalamic infarction is more common and that it could result in different clinical 1090-0233/$ - see front matter Ó 2010 Elsevier Ltd. All rights reserved. doi:10.1016/j.tvjl.2010.03.024 * Corresponding author. Tel.: +44 151 795 6100; fax: +44 151 795 6101. E-mail address: [email protected] (R. Gonçalves). The Veterinary Journal 188 (2011) 39–43 Contents lists available at ScienceDirect The Veterinary Journal journal homepage: www.elsevier.com/locate/tvjl
-
Upload
rita-goncalves -
Category
Documents
-
view
213 -
download
0
Transcript of Clinical and topographic magnetic resonance imaging characteristics of suspected thalamic infarcts...

The Veterinary Journal 188 (2011) 39–43
Contents lists available at ScienceDirect
The Veterinary Journal
journal homepage: www.elsevier .com/ locate/ tv j l
Clinical and topographic magnetic resonance imaging characteristicsof suspected thalamic infarcts in 16 dogs
Rita Gonçalves a,*, Inés Carrera b, Laurent Garosi c, Peter M. Smith a, J. Fraser McConnell a, Jacques Penderis b
a Department of Veterinary Science, Small Animal Teaching Hospital, University of Liverpool, Leahurst, Chester High Road, Neston CH64 7TE, UKb Institute of Comparative Medicine, Faculty of Veterinary Medicine, University of Glasgow, Glasgow G61 1QH, UKc Davies Veterinary Specialists, Manor Farm Business Park, Higham Gobion, Hertfordshire SG5 3HR, UK
a r t i c l e i n f o a b s t r a c t
Article history:Accepted 30 March 2010
Keywords:ThalamusCerebrovascularStrokeAnatomyDog
1090-0233/$ - see front matter � 2010 Elsevier Ltd. Adoi:10.1016/j.tvjl.2010.03.024
* Corresponding author. Tel.: +44 151 795 6100; faE-mail address: [email protected] (R. Gonçalve
Sixteen dogs with acute-onset, non-progressive signs of brain dysfunction and magnetic resonance imag-ing (MRI) characteristics compatible with thalamic infarction are described. Topographically the MRIlesions could be grouped in three thalamic regions, namely, paramedian (8/16), extensive dorsal (5/16)and ventrolateral (3/16). Paramedian lesions resulted in signs typical of vestibular dysfunction. Extensivedorsal lesions were associated with vestibular ataxia, circling and contralateral menace response deficits.Ventrolateral lesions resulted in circling and contralateral proprioceptive deficits. In several dogs, regionsother than the thalamus were also affected: four extended into the midbrain; six extended to the internalcapsule, and two dogs had a second lesion in the cerebellum. Three clinical syndromes were identified inassociation with thalamic infarction. These signs varied somewhat, most likely because lesions were notconfined to specific nuclear boundaries and involved different combinations of thalamic nuclei.
� 2010 Elsevier Ltd. All rights reserved.
Introduction
Cerebrovascular disease is increasingly recognised in dogs. Itrepresents an abnormality of the brain caused by a disturbancein blood supply (Kalimo et al., 2002) and its clinical manifestation,also known as cerebrovascular accident or stroke, can be broadlydivided into ischemic (resulting from arterial or venous obstruc-tion) or haemorrhagic (resulting from rupture of blood vessels).The term infarction describes the area of necrotic tissue resultingfrom ischemia and the subsequent neuronal and glial cell death(Adams and Victor, 1997).
With the advent of advanced imaging techniques in veterinarypractice our understanding of brain infarction in dogs is increasing.Recent studies have described the magnetic resonance imaging(MRI) characteristics, topographic distribution of lesions and sus-pected underlying causes of brain infarction in dogs (Garosi etal., 2005, 2006). MRI findings include well-defined, sharply demar-cated lesions with minimal to no mass effect that are limited to thevascular territory of a main cerebral or perforating artery and thatare hyperintense on T2-weighted images (T2WI) and/or fluidattenuated inversion recovery (FLAIR) images. Concurrent medicalconditions have been reported in approximately half of the casesand most commonly include chronic kidney disease andhyperadrenocorticism.
ll rights reserved.
x: +44 151 795 6101.s).
In humans, a correlation between clinical syndromes, imagingfindings and location of the infarction, stroke mechanism (embolicor thrombotic) and possible concurrent medical conditions hasbeen found. This has not been feasible in dogs (Garosi et al.,2005). Cerebellar infarcts within the vascular territory of the ros-tral cerebellar artery have been most commonly identified, fol-lowed by similar numbers of telencephalic infarcts within theregions of the rostral and middle cerebral arteries and striate arter-ies and thalamic/midbrain infarcts within the territory of the cau-dal perforating arteries (Garosi et al., 2006). In humans, fourdistinct clinical syndromes associated with thalamic infarctionsare recognised (Schmahmann, 2003): anterior, paramedian, infero-lateral and posterior infarcts, representing obstruction of thetuberothalamic, paramedian, inferolateral and posterior choroidalvessels, respectively (Schmahmann, 2003; Saez de Ocariz et al.,1996; Wang et al., 2008). Three variant types (anteromedian, cen-tral and posterolateral infarcts) have also been described and theirexistence is thought to be related to either variations of the terri-tories supplied by the thalamic arteries or to the occurrence ofhemodynamic (borderzone) mechanisms (Carrera et al., 2004).
In the dog, the blood supply of the thalamus differs from that ofhumans (Inoue et al., 1985; Brenowitz and Yonas, 1990; Garosiet al., 2006) and derives predominantly from three blood vessels(Table 1). Although thalamic infarcts accounted for only 15% of sus-pected brain infarctions in the dog in one recent study (Garosiet al., 2006), our clinical experience is that thalamic infarction ismore common and that it could result in different clinical

Table 1Thalamic arterial blood supply and its distribution in the dog.
Arterial supply Distribution
Proximal perforating artery arising fromthe caudal communicating artery
Rostromedial aspect of thethalamus
Distal perforating artery arising fromthe caudal communicating artery
Caudolateral aspect of thethalamus and subthalamus
Caudal perforating artery arising fromthe basilar bifurcation andparamedian branches arising fromthe proximal portion of the caudalcerebral artery
Median and paramedian aspect ofthe thalamus, pons and midbrain
40 R. Gonçalves et al. / The Veterinary Journal 188 (2011) 39–43
presentations. The aims of this study were therefore to describe (1)the clinical syndromes seen with thalamic infarction, (2) the tha-lamic regions (nuclei) affected, and (3) the outcome associatedwith the lesions identified.
Materials and methods
The medical records from the Neurology and Neurosurgery Units of the Univer-sities of Glasgow and Liverpool and from Davies Veterinary Specialists were re-viewed to identify dogs in which a diagnosis of thalamic infarction had beenmade. These patients had been presented for investigation of acute-onset, non-pro-gressive (after the initial 24 h) signs of neurological dysfunction affecting the brain.Dogs were included in this study if intracranial MRI examination revealed a lesionthat was hyperintense on T2WI and FLAIR images, in the vascular territory of one ofthe arteries supplying the thalamus and causing minimal to no mass effect.
All dogs had normal cerebrospinal fluid analysis results. Signalment, findings ofthe neurological examination and concurrent medical conditions were recorded.Information regarding the outcome was collected from the records or by telephoneconversation with the owners and/or referring veterinary surgeons. The outcomewas defined as good if there was improvement of the clinical signs without signif-icant permanent neurological deficits or poor if the suspected infarction resulted indeath, lack of improvement or recurrent neurological deficits.
MRI examinations were performed using either a 1.5 T (Gyroscan NT, PhilipsMedical System), 1 T (Siemens Magnetom) or a 0.4 T (Aperto, Hitachi) magnet. Pulsesequences varied but included transverse, sagittal and dorsal T2WI (TR, 2500–4400;TE, 100–125), transverse FLAIR (TR, 5900–10,895; TE, 100–120; TI, 2000–2100) andtransverse pre- and post-contrast (intravenous injection of 0.1 mmol/kg of gado-pentetate dimeglumine) T1-weighted images (T1WI; TR, 520–750; TE, 11.5–14.5).The slice thickness used was 3 mm and the interslice gap was 0.5 mm.
The thalamic infarctions were classified according to the suspected arterial ter-ritory involved: proximal, distal and caudal perforating arteries. The locations of thelesions within the thalamus and the most affected thalamic nuclei were identifiedand recorded, using the nomenclature proposed by previous descriptive studies ofthe canine diencephalon (Rioch, 1929; Sakai et al., 1983).
Results
Sixteen cases met the criteria for inclusion. The median age atpresentation was 8.1 years (11 months to 13 years) and no breedpredisposition was noted. There were 3 Cavalier King Charles span-
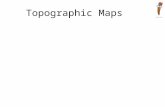
Fig. 1. MRI images illustrating presumed infarcts in the four topographic thalamic regiparamedian infarct. (B) Transverse plane T2WI of the brain of a 7-year old CKCS with a dwith a ventrolateral infarct.
iels (CKCS) and 3 Greyhounds, 2 mixed breed dogs, 2 Weimaraners,2 Labradors, 1 Beagle, 1 Dalmatian, 1 Staffordshire bull terrier, and1 Pug. Twelve dogs were male (three were neutered) and four wereneutered females.
The lesions were divided into three groups based on the tha-lamic regions affected: paramedian (affecting the mediodorsalnucleus and other midline nuclei to a variable extent; Fig. 1a),dorsal extensive (large infarcts mostly located in the rostral thal-amus and affecting mainly the areas of the mediodorsal, centrallateral, ventral lateral, anterior ventral and lateral geniculate nu-clei; Fig. 1b); and ventrolateral (mainly affecting the ventral lat-eral, ventral posterior lateral and ventral anterior nuclei;Fig. 1c). The neurological deficits associated with lesions in thesedifferent regions are documented in Table 2. Clinical signs weresomewhat variable but three main clinical syndromes wererecognised. Paramedian lesions resulted in signs typical of vestib-ular dysfunction (contralateral head tilt, vestibular ataxia andnystagmus) in 6/8 dogs. The more extensive dorsal lesions alsocaused vestibular ataxia, with falling and leaning to the sideopposite the lesion, but nystagmus and head tilt were not seen;these lesions also caused circling, contralateral menace responsedeficits and hemiparesis. Ventrolateral lesions resulted in circlingand contralateral proprioceptive deficits.
In several dogs, the area of T2W hyperintensity seen in the thal-amus extended into an adjacent region of the brain. In four dogswith paramedian lesions, the lesion extended caudally into themidbrain (Fig. 2a) and in four dogs with extensive lesions andtwo with ventrolateral lesions, the lesion extended laterally to in-volve the internal capsule (Fig. 2b). In two other dogs with parame-dian lesions, a second lesion (Fig. 2c) was identified in theipsilateral cerebellum. Both of these lesions were hyperintenseon T2WI, hypointense on T1WI and did not enhance following con-trast injection; these were considered to likely be older infarcts.
In 10/16 dogs, no concurrent medical condition was identified.Two dogs were hypoalbuminemic and were diagnosed with pro-tein losing diseases (inflammatory bowel disease and protein los-ing nephropathy, respectively) and one dog was diagnosed withboth hyperadrenocorticism and neoplasia (transitional cell carci-noma). In all three CKCS, Chiari-like malformation was identified.
Long-term follow-up information ranged from 4 to 60 months.Four dogs had a poor outcome (two dogs with a dorsal extensivelesion and one each of the other regions). One dog was euthanased1 week following diagnosis of the suspected infarction due to theconcurrent neoplasia. The dog in which seizures were part of theinitial presentation developed symptomatic epilepsy. Two otherdogs suffered subsequent episodes of neurological dysfunction (de-scribed as similar episodes by the referring veterinary surgeon).Ten dogs made a full recovery according to the owners and had
ons described. (A) Transverse plane T2WI of the brain of a 9-year old CKCS with aorsal extensive infarct. (C) Dorsal plane T2WI of the brain of a 9-year old Labrador

Table 2Neurological deficits associated with the three thalamic syndromes.
Clinical signs Paramedian(n = 8)
Dorsalextensive(n = 5)
Ventrolateral(n = 3)
Total(n = 16)
Ataxia 8 4 1 13Circlinga 2 5 2 9Contralateral PD 2 5 2 9Disorientation 2 2 2 6Contralateral head
tilt6 0 0 6
Nystagmus 6 0 0 6Contralateral
menace deficit1 4b 0 5
Contralateralhemiparesis
0 4 0 4
Pleurothotonus 0 1 2 3Bilateral pelvic
limb PD2 0 1 3
Positionalstrabismus
1 1 1 3
Hypermetria 1 1 0 2Contralateral
facialhypalgesia
0 2 0 2
Seizures 1 0 0 1Abnormal
ipsilateral PLR1 0 0 1
Ipsilateral headtilt
0 0 1 1
Obtundation 0 1 0 1Anisocoria 1 0 0 1Horner’s
syndrome1 0 0 1
PD, proprioceptive deficits; PLR, pupillary light reflex.a In two cases (one paramedian and one dorsal extensive lesion), the direction of
the circling was not recorded but in all other cases it was ipsilateral to the lesionidentified on MRI.
b One dog with a dorsal lesion had previous enucleation of the eye contralateralto the thalamic lesion, so the menace response could not be assessed.
R. Gonçalves et al. / The Veterinary Journal 188 (2011) 39–43 41
no further episodes of neurological dysfunction. Two dogs werelost to follow-up.
Discussion
In the current study, we identified a variety of clinical signs indogs showing presumptive thalamic infarction. By dividing dogsinto three categories based on the site of the infarct, we were able
Fig. 2. MRI images illustrating the intracranial regions beside the thalamus also affectedPug with a presumed paramedian infarct extending caudally to the midbrain. (B) Dorsal pinfarct simultaneously affecting the internal capsule. (C) Transverse plane T2WI of thpresumed second infarct in the ipsilateral cerebellum.
to characterise the neurological deficits associated with lesions atthese different sites. Thus, dogs with paramedian infarcts showedmainly vestibular dysfunction, those with ventrolateral lesionstended to circle and had contralateral proprioceptive deficits, andthose with dorsal extensive lesions presented with ataxia, circlingand contralateral menace deficits.
All infarcts described in this study were thought to have arisenthrough occlusion of the perforating arteries and were thereforeclassified as lacunar infarcts. Eleven dogs had small localised le-sions whilst five presented with more extensive lesions, suggestingpossible occlusion of more than one perforating artery. Most (8/16)lesions were located in the caudomedial thalamus (paramedian le-sions), an area supplied by the caudal perforating arteries and par-amedian branches of the caudal cerebral artery. These arteries alsosupply the pons and midbrain, which might explain why lesionsextended into the midbrain in some cases. With three lesions(two ventrolateral and one dorsal extensive infarct), the caudolat-eral thalamus was affected, suggesting occlusion of a distal perfo-rating artery. Six dogs had thalamic infarcts primarily involving therostral aspect of the thalamus; five of these were dorsal extensivelesions and one was ventrolateral. This region is supplied by theproximal perforating arteries, which irrigate mainly the rostrome-dial thalamus. The presence of a rostrolateral lesion raises the pos-sibility of a variation of the thalamic arterial supply, a phenomenoncommonly recognised in humans (Carrera et al., 2004).
Many of the presenting clinical signs encountered in the currentstudy reflect the well established role of the thalamus as a relaycentre between brainstem structures and the cerebral cortex. Thus,contralateral proprioceptive deficits were found in animals with le-sions affecting the ventral lateral nucleus or the thalamocorticalprojection fibres from this region, which comprise part of the path-way for conscious proprioception. The menace response was im-paired in animals with dorsal extensive lesions in which thelateral geniculate nucleus, a component of the visual pathway,was affected. Hemiparesis, seen in four dogs with dorsal extensivelesions, was most likely caused by damage to the internal capsule(Helgason and Wilbur, 1990). Although a less powerful influenceon limb movement in domestic animals than in people, this findingsuggests that acute damage to the pyramidal tracts may have a sig-nificant impact on clinical presentation.
Our study sheds some interesting light on the similarities anddifferences between the thalamus in humans and domestic ani-mals. Vestibular ataxia was the most commonly reported neuro-logical deficit in the current series and occurred with lesions in
by the suspected thalamic infarcts. (A) Dorsal plane T2WI of the brain of a 7-year oldlane T2WI of the brain of a 7-year old Greyhound with a presumed dorsal extensive
e brain of an 8-year old Weimaraner with a presumed paramedian infarct and a

42 R. Gonçalves et al. / The Veterinary Journal 188 (2011) 39–43
all regions of the thalamus. This is different from humans, in whichthe caudal lateral thalamus is the region mostly associated withvestibular ataxia. Several possible reasons have been proposedfor this: firstly, the ventrolateral nucleus is thought to be the mainafferent thalamic relay station for multiple multisensory vestibularcortex areas (Sans et al., 1970; Shiroyama et al., 1999); secondly, aphenomenon of contralateral hemi-ataxia termed crossed cerebel-lar diaschisis is described in patients when there is functionaldepression of the contralateral cerebellar hemisphere followingdamage to the ventrolateral region of the thalamus (Tanakaet al., 1992); thirdly, the ventrolateral thalamic region receivesafferents from the dentatorubrothalamic pathway and it is thoughtthat damage to these fibres can cause ataxic hemiparesis throughdisrupted cerebellocortical feedback (Helgason and Wilbur,1990). We identified ataxia associated with lesions in all regionsbut in only 1/3 dogs with caudolateral lesions, indicating that theseexplanations do not apply to dogs.
Six of eight dogs with paramedian infarcts showed vestibulardysfunction, including nystagmus and head tilt. In humans, themedial portion of the thalamus is considered devoid of vestibularfunction and patients presenting with paramedian infarction andsigns typical of vestibular disease are considered to have simulta-neous involvement of the paramedian rostral midbrain (Brandt andDieterich, 1994), including the interstitial nucleus of Cajal (INC). Inseveral of our dogs with paramedian infarcts, the lesion extendedcaudally into the midbrain, including the region of the INC andthe adjacent medial longitudinal fasciculus (MLF). Experimentalstudies in several species have shown that stimulation or destruc-tion of the INC and/or MLF causes contralateral abnormal head andneck postures as well as nystagmus and strabismus (Mabuchi,1970; Hassler, 1972; Anderson, 1981) and it seems likely that dam-age to these regions contributed to the clinical syndrome observedin the current study. Moreover, the mediodorsal nucleus, the larg-est and most severely affected nucleus in the paramedian infarcts,has direct connections with the cerebellum (Sakai et al., 1983) andwith several brainstem structures including the INC (Irle et al.,1984).
Circling was frequently identified and was seen with lesionsaffecting all three regions, although it was less common with par-amedian lesions. Various neuroanatomical structures have beenassociated with circling behaviour but this feature most often oc-curs with lesions affecting the basal nuclei and substantia nigra(Pycock, 1980). In experimental studies, the thalamic regions mostcommonly associated with circling are the ventromedial area(Starr and Summerhayes, 1982; Garcia-Munoz et al., 1983) andthe centromedian–parafascicular complex (Dalsass and Krauth-amer, 1981; Henderson et al., 2005), both of which are connectedto the nigrostriatal system. In most dogs in our study that pre-sented with circling, there were MRI changes in the ventromedialregion, suggesting similar connectivity to the basal nuclei in dogs.In some dogs the centromedian–parafascicular complex was alsoaffected; however, this area was affected in several other dogs withparamedian lesions that did not circle. Ipsiversive head and neckturn (pleurothotonus) has also been described in association withlesions in the ventromedial thalamus and often occurs simulta-neously with ipsiversive circling (Di Chiara et al., 1979; Welzlet al., 1984).
One case in the current series had seizures at presentation.Seizures are not reported in humans (Berges et al., 2000) or dogs(Garosi et al., 2006) with ischemic thalamic infarction and occuronly rarely with thalamic haemorrhagic stroke (Sung and Chu,1989). However, experimental studies have demonstrated that sei-zure activity can result from electrical stimulation of the thalamus,mainly in the region of the midline nuclei (Hunter and Jasper,1949), and it is possible that our case developed seizures as a resultof thalamic infarction.
We found a number of features, such as age, were similar tothose previously reported in dogs. Because of the small numberof cases, a breed predisposition could not be identified, althoughboth CKCS and Greyhounds were most commonly represented,similar to a previous report (Garosi et al., 2005). There was anapparent male predisposition but because of the small number ofcases and the lack of previous reports, the significance of this find-ing is uncertain. Approximately two-thirds of the animals had agood prognosis, a higher number than that reported for all braininfarctions in dogs (Garosi et al., 2005). This is similar to humansfor whom the prognosis of thalamic infarction is good comparedwith lesions affecting the cerebral cortex or other subcortical struc-tures (Saez de Ocariz et al., 1996).
A significant limitation to the present study is the lack of MRIangiographic data or histopathological confirmation of the infarc-tion, with the presumptive diagnosis being based on appropriatehistorical, clinical and imaging findings.
Conclusions
Three clinical syndromes associated with presumed thalamicinfarction of different regions (paramedian, extensive dorsal andventrolateral) were identified. These observations shed light onthe differences in anatomy between the canine and human thala-mus and should help clinicians to understand the potentially con-fusing array of clinical signs associated with vascular lesions in thisregion.
Conflict of interest statement
None of the authors of this paper has a financial or personalrelationship with other people or organisations that could inappro-priately influence or bias the content of the paper.
References
Adams, R., Victor, M., 1997. Cerebrovascular diseases. In: Adams, R., Victor, M.(Eds.), Principles of Neurology, sixth ed. McGraw-Hill Inc., New York, NY, USA,pp. 777–873.
Anderson, J., 1981. Ocular torsion in the cat after lesions of the interstitial nucleus ofCajal. Annals of the New York Academy of Sciences 374, 865–871.
Berges, S., Moulin, T., Berger, E., Tatu, L., Sablot, D., Challier, B., Rumbach, L., 2000.Seizures and epilepsy following strokes: recurrence factors. EuropeanNeurology 43, 3–8.
Brandt, T., Dieterich, M., 1994. Vestibular syndromes in the roll plane: topographicdiagnosis from brainstem to cortex. Annals of Neurology 36, 337–347.
Brenowitz, G., Yonas, H., 1990. Selective occlusion of blood supply to the anteriorperforated substance of the dog: a highly reproducible stroke model. SurgicalNeurology 33, 247–252.
Carrera, E., Nichel, P., Bogousslavsky, J., 2004. Anteromedian, central andposterolateral infarcts of the thalamus. Three variant types. Stroke 35, 2826–2831.
Dalsass, M., Krauthamer, G., 1981. Behavioral alterations and loss of caudatemodulation in the centrum medianum–parafascicular complex of the catfollowing electrolytic lesions of the substantia nigra. Brain Research 208, 67–79.
Di Chiara, G., Morelli, M., Porceddu, M., Gessa, G., 1979. Role of the thalamic c-aminobutyrate in motor functions: catalepsy and ipsiversive turning afterintrathalamic muscinol. Neuroscience 4, 1453–1465.
Garcia-Munoz, M., Patino, P., Wright, A., Arbuthnott, G., 1983. The anatomicalsubstrate of the turning behaviour seen after lesions in the nigrostriataldopamine system. Neuroscience 8, 87–95.
Garosi, L., McConnell, J.F., Platt, S.R., Barone, G., Baron, J.C., de Lahunta, A.,Schatzberg, S.J., 2005. Results of diagnostic investigations and long-termoutcome of 33 dogs with brain infraction (2000–2004). Journal of VeterinaryInternal Medicine 19, 725–731.
Garosi, L., McConnell, J.F., Platt, S.R., Barone, G., Baron, J.C., de Lahunta, A.,Schatzberg, S.J., 2006. Clinical and topographic magnetic resonancecharacteristics of suspected brain infarction in 40 dogs. Journal of VeterinaryInternal Medicine 20, 311–321.
Hassler, R., 1972. Supranuclear structures regulating binocular eye and headmovements. Bibliotheca Ophthalmologica 82, 207–219.
Helgason, C., Wilbur, A., 1990. Capsular hypesthetic ataxic hemiparesis. Stroke 21,24–33.

R. Gonçalves et al. / The Veterinary Journal 188 (2011) 39–43 43
Henderson, J., Schleimer, S., Allbutt, H., Dabholkar, V., Abela, D., Jovic, J., Quinlivan,M., 2005. Behavioural effects of parafascicular thalamic lesions in an animalmodel of parkinsonism. Behavioural Brain Research 162, 222–232.
Hunter, J., Jasper, H., 1949. Effects of thalamic stimulation in unanesthetisedanimals. Electroencephalography and Clinical Neurophysiology 1, 305–324.
Inoue, T., Kobayashi, S., Sugita, K., 1985. Dye injection method for thedemonstration of territories supplied by individual perforating arteries of theposterior communicating artery in the dog. Stroke 16, 684–686.
Irle, E., Markowitsch, H., Streicher, M., 1984. Cortical and subcortical, includingsensory-related, afferents to the thalamic mediodorsal nucleus of the cat.Journal für Hirnforschung 25, 29–50.
Kalimo, H., Kaste, M., Haltia, M., 2002. Vascular diseases. In: Graham, D., Lantos, P.(Eds.), Greenfield’s Neuropathology, seventh ed. Arnold, London, UK, pp. 233–280.
Mabuchi, M., 1970. Rotatory head response evoked by stimulating and destroyingthe interstitial nucleus and surrounding region. Experimental Neurology 27,175–193.
Pycock, C., 1980. Turning behaviour in animals. Neuroscience 5, 461–514.Rioch, D., 1929. Studies on the diencephalon of Carnivora. Part I. The nuclear
configuration of the thalamus, epithalamus and hypothalamus of the dog andcat. The Journal of Comparative Neurology 49, 1–119.
Saez de Ocariz, M.M., Nader, J.A., Santos, J.A., Bautista, M., 1996. Thalamic vascularlesions. Risk factors and clinical course for infarcts and hemorrhages. Stroke 27,1530–1536.
Sakai, S., Stanton, G., Tanaka, D., 1983. The ventral lateral thalamic nucleus in thedog: cytoarchitecture, acetylthiocholinesterase histochemistry, and cerebellarafferents. Brain Research 271, 1–9.
Sans, A., Raymond, J., Marty, R., 1970. Response thalamiques et corticales a lastimulation electrique du nerf vestibulaire chez le chat. Experimental BrainResearch 10, 265–275.
Schmahmann, J., 2003. Vascular syndromes of the thalamus. Stroke 34, 2264–2278.Shiroyama, T., Kayahara, T., Yasui, Y., Nomura, J., Nakano, K., 1999. Projections of the
vestibular nuclei to the thalamus in the rat: a Phaseolus vulgaris leucoagglutininstudy. The Journal of Comparative Neurology 407, 318–332.
Starr, M., Summerhayes, M., 1982. Multifocal brain sites for apomorphine-inducedcircling and other stereotyped motor behaviour in the 6-hydroxydopamine-lesioned rat. Neuroscience Letters 34, 277–282.
Sung, C.Y., Chu, N.S., 1989. Epileptic seizures in intracerebral haemorrhage. Journalof Neurology, Neurosurgery, and Psychiatry 52, 1273–1276.
Tanaka, M., Kondo, S., Hirai, S., Ishiguro, K., Ishihara, T., Morimatsu, M., 1992.Crossed cerebellar diachisis accompanied by hemiataxia: a PET study. Journal ofNeurology, Neurosurgery, and Psychiatry 55, 121–125.
Wang, X., Fan, Y.H., Lam, W.W., Leung, T.W., Wong, K.S., 2008. Clinical features,topographic patterns on DWI and etiology of thalamic infarcts. Journal of theNeurological Sciences 267, 147–153.
Welzl, H., Schwarting, R., Kulajta, J., Huston, J., 1984. Perioral biting reflex and turningafter intranigral injection of a GABA- or metenkephalin-agonist: role of thethalamus and superior colliculus. Experimental Brain Research 55, 438–444.