Clinical and Subclinical Eating Disorders in Counseling Center Clients
18
This article was downloaded by: [University of Connecticut] On: 06 October 2014, At: 19:58 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of College Student Psychotherapy Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/wcsp20 Clinical and Subclinical Eating Disorders in Counseling Center Clients Wendy D. Hoyt MS a & Steve D. Ross Psyd a a Colorado State University , USA Published online: 03 Oct 2008. To cite this article: Wendy D. Hoyt MS & Steve D. Ross Psyd (2003) Clinical and Subclinical Eating Disorders in Counseling Center Clients, Journal of College Student Psychotherapy, 17:4, 39-54, DOI: 10.1300/J035v17n04_06 To link to this article: http://dx.doi.org/10.1300/J035v17n04_06 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan,
Transcript of Clinical and Subclinical Eating Disorders in Counseling Center Clients

This article was downloaded by: [University of Connecticut]On: 06 October 2014, At: 19:58Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH,UK
Journal of College StudentPsychotherapyPublication details, including instructions forauthors and subscription information:http://www.tandfonline.com/loi/wcsp20
Clinical and Subclinical EatingDisorders in Counseling CenterClientsWendy D. Hoyt MS a & Steve D. Ross Psyd aa Colorado State University , USAPublished online: 03 Oct 2008.
To cite this article: Wendy D. Hoyt MS & Steve D. Ross Psyd (2003) Clinical andSubclinical Eating Disorders in Counseling Center Clients, Journal of College StudentPsychotherapy, 17:4, 39-54, DOI: 10.1300/J035v17n04_06
To link to this article: http://dx.doi.org/10.1300/J035v17n04_06
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all theinformation (the “Content”) contained in the publications on our platform.However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness,or suitability for any purpose of the Content. Any opinions and viewsexpressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of theContent should not be relied upon and should be independently verified withprimary sources of information. Taylor and Francis shall not be liable for anylosses, actions, claims, proceedings, demands, costs, expenses, damages,and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of theContent.
This article may be used for research, teaching, and private study purposes.Any substantial or systematic reproduction, redistribution, reselling, loan,

sub-licensing, systematic supply, or distribution in any form to anyone isexpressly forbidden. Terms & Conditions of access and use can be found athttp://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

Clinical and Subclinical Eating Disordersin Counseling Center Clients:
A Prevalence Study
Wendy D. HoytSteve D. Ross
ABSTRACT. Eating disorders on college campuses comprise a serious,yet understudied mental health issue. Specifically, prevalence studies ofeating disorders among college counseling center populations are lack-ing in the current literature. Attempting to quantify the seriousness ofthis issue becomes an important first step in adapting counseling and out-reach services for the larger campus community. Accordingly, this studyutilized the Eating Attitudes Test-26 (EAT-26) and Body Mass Index(BMI) to assess clients accessing counseling services at the universitycounseling center of a large state university. The study revealed a signifi-cant increase in the number of clients diagnosed with an eating disorderduring the course of the survey. These results are discussed in terms ofthe need for a specific eating disorders protocol to increase client disclo-sure and counselor awareness. [Article copies available for a fee from TheHaworth Document Delivery Service: 1-800-HAWORTH. E-mail address:<[email protected]> Website: <http://www.HaworthPress.com> © 2003by The Haworth Press, Inc. All rights reserved.]
Wendy D. Hoyt, MS, and Steve D. Ross, PsyD, are both affiliated with ColoradoState University.
Address correspondence to: Wendy D. Hoyt, MS, Counseling and Consultation,P. O.Box 871012,Arizona State University, Tempe, AZ 85287-1012 (E-mail: [email protected]).
The authors would like to recognize the assistance provided by Stacey Huss andJulie Hewson in data collection and analysis. They also would like to thank SusanMacQuiddy and Lori Kogan for reviewing early editions of this manuscript.
Journal of College Student Psychotherapy, Vol. 17(4) 2003http://www.haworthpress.com/store/product.asp?sku=J035 2003 by The Haworth Press, Inc. All rights reserved.
10.1300/J035v17n04_06 39
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

KEYWORDS. Prevalence, college counseling centers, eating disorders
At least one major longitudinal incidence study of eating disordershas shown a continuing linear increase in eating disorder pathology for15- to 24-year-old females (Lucas, Crowson, O’Fallon, & Melton, 1999).However, eating disorder prevalence studies on college campuses havebeen sparse, despite the fact that this is an at-risk environment with re-spect to age, developmental factors, and environmental stressors. Thelimited available data collected over the past 10 years have consistentlyrevealed a high prevalence of eating disorders among women enrolledin colleges and universities throughout the United States. In addition tothe estimated 1-4% of female college students meeting the full DSM-IV(APA, 1994) criteria for anorexia nervosa or bulimia nervosa, an addi-tional 35-70% report such direct and indirect symptoms of disorderedeating as: loss of appetitive control; periodic use of laxatives, purging orexcessive exercise to inhibit weight gain; body image dissatisfactionand distortion; obsessive monitoring of caloric and fat content; un-healthy weight fluctuations; excessive weight monitoring; moderate de-pression; and low self-esteem (Edwards-Hewitt & Gray, 1993; Heather-ton, Nichols, Mahamedi, & Keel, 1995; Kurth, Krahn, Nairn, & Drewn-owski, 1995; Nelson, Hughes, Katz, & Searight, 1999; Schwitzer,Bergholz, Dore, & Salimi, 1998; Winzelberg et al., 1998). These indi-viduals who do not meet the full DSM-IV diagnostic criteria but displayproblematic behaviors can be classified as having subclinical eatingdisorders, disorders which clearly account for most of the eating pathol-ogy seen on college campuses.
There are also subgroups within the college environment that are atan even greater risk for the development of an eating disorder. Collegeathletes frequently experience pressures to remain thin and lean, partic-ularly those who participate in sports in which having a smaller bodysize correlates with perceptions of improved performance and/or greaterconformity to aesthetic standards (Beals & Manore, 1994). However, inaddition to sponsoring college athletes, many campuses have a largenumber of students participating in intramural or recreational sportingactivities. Although the fact that individuals with subclinical and clini-cal eating disorders tend to participate in high levels of exercise iswell-known (Davis et al., 1994; Davis et al., 1997; Long et al., 1993;Szymanski & Chrisler, 1991; Wolf & Akamatsu, 1994), there is again apaucity of research addressing levels of eating disorder symptoms incollege students engaged in lower levels of sporting activities. Accord-
40 JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

ingly, we were interested in looking at athletic endeavor as a possiblerisk factor within a college group.
As stated, while there have been many studies looking at eating dis-ordered behaviors on college campuses, there has been much less re-search focusing on specific groups. Therefore, the focus of the presentstudy is on a group that, to this date, no previous research has ad-dressed–university counseling center clients. Many universities havecounselors, nutritionists, and medical professionals that devote a largeamount of their time to the treatment of students with eating disorders.However, on many campuses it is unclear how many students these pro-fessionals are serving. It is clear that the number of students sufferingfrom disordered eating on college campuses is alarmingly high, and dueto the size of most campuses, it is difficult to reach many individualsthrough campus wide prevention and intervention strategies. Coun-seling centers are one campus agency where, if the campus is aware ofhow many students with disordered eating are seeking treatment, addi-tional resources can be effectively employed. However, many profes-sionals who work in this field recognize that the eating pathology inmany clients is not addressed due to the secretive nature of the disorder,thus making it difficult to determine the importance of professionalsspecializing in eating disorder treatment. Therefore, in this study, themain purpose was to determine the frequency of eating pathology instudents who seek treatment at a university counseling center.
We were also interested in examining the data in relation to a hypoth-esized “priming effect,” which we anticipated would occur over the du-ration of the research. It should be noted that our semantic notion ofpriming within the context of this research lies outside of the parametersof purer scientific measures of learning, memory and cognition. For ourpurposes, we were interested in the combined effect on therapists andcounseling center clients of having the Eating Attitudes Test-26(EAT-26) included in the demographic packet given to clients. Al-though we are unaware of prior use of the EAT-26, or related eating dis-order specific assessment instruments, to assess the impact of such apriming effect, Cowan and Morewitz (1995) found that students pre-senting to a student health center were indeed more likely to discusspsychosocial issues and problems if they completed a questionnaire ad-dressing such issues prior to meeting with a health professional. In addi-tion, they found that the health professionals themselves were more likelyto question students about these issues when presented with the com-pleted questionnaire. Therefore, we anticipated that including the EAT-26with the typical paperwork completed by incoming clients would prime
Wendy D. Hoyt and Steve D. Ross 41
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

the subsequent psychological assessments made by therapists, increas-ing the likelihood therapists would inquire about eating disorder issuesthat may otherwise not have been explored. Our hypothesis anticipatedincreases in primary and secondary diagnoses of eating disorderpsychopathology and increases in reports of subclinical eating disorderissues, primarily diagnoses of Eating Disorder Not Otherwise Spec-ified.
METHOD
Participants
A total of 555 participants for this study were recruited from the cli-entele of the University Counseling Center at a large university in theRocky Mountain Region of the United States. All students requestingservices at the University Counseling Center during the Spring 2000 se-mester received the survey materials. The self-reported ethnicity of cli-ents seen at the University Counseling Center during this time periodwas as follows: 82.2% Caucasian, 6.88% Hispanic, 3.18% Asian/Pa-cific American, 1.26% African American, and 0.87% Native American.These percentages are similar to those in the overall student population.
Measures
Eating Attitudes Test-26 (EAT-26). The EAT-26 is arguably the mostwidely utilized self-report instrument for measuring eating disordersymptoms (Garner, 1993; Garner, 1997). In addition, the EAT-26 is oneof the most efficient questionnaires available as it can be completed in5-10 minutes. Therefore, this questionnaire was used to assess the level ofeating disorder symptomatology in all participants. The EAT-26 con-sists of 26 items regarding eating attitudes, and participants are asked toindicate their responses using a six-point Likert scale ranging from “Al-ways” to “Never.” In addition, this measure includes demographicquestions addressing height, weight, year in school, and level of athleticparticipation (intramural, intermural, or collegiate) and five questionsrelated to binge/purge frequency, previous treatment for an eating dis-order, and suicidal ideation. The five additional items were added by theoriginal author for use as part of the nationwide Eating Disorder Aware-ness Week screenings. This version of the EAT-26 was chosen due toits wide use for screenings in counseling centers throughout the United
42 JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

States and due to its recent validation as “a screening tool for identify-ing nonclinical women who are likely suffering from an undifferenti-ated DSM-IV eating disorder” (Mintz & O’Halloran, 2000). A totalscore of 20 or above on the EAT-26 has been used to identify individu-als who might be at risk for the development of, or currently have, aneating disorder. In addition, anyone who answers yes to any of the fivequestions regarding binge/purge behaviors, previous treatment, or sui-cidal ideology is considered to be at risk. Mintz and O’Halloran (2000)report that the EAT-26 has an accuracy rate of approximately 90%when used with nonclinical women.
Body Mass Index (BMI). Self-reported current height and weightwere used to calculate participant’s BMI. Prior research has demon-strated that self-report of these parameters correlates highly (r = .98)with objective height and weight measures in individuals with and with-out eating disorders (Burckes-Miller & Black, 1988). As a standardmeasure of participant’s body size, BMI was calculated using the fol-lowing formula: weight in kilograms divided by height in squared me-ters. Individuals who have a BMI of 18 or below are considered to bebelow average weight and at risk for anorexia nervosa. BMI is not an ef-fective measure for identifying individuals with bulimia nervosa orbinge eating disorder, as the majority of these individuals are of normalweight or above.
Procedure
This project was approved by the Human Research Committee inFall 1999 with the condition that all surveys would remain confidentialand would not be tracked (i.e., using any type of identification code thatcould result in a survey being traced to the specific participant). Thiscondition was included due to the fact that participants were clients in acounseling center and as a result of the sensitive nature of the behaviorsbeing studied. Because it was expected that there would be a small per-centage of the sample that would meet criteria for an eating disorder andsimilar demographic information was collected as part of both the EAT-26and the counseling center paperwork, it was determined that the possi-bility, however small, that paperwork could be connected to the specificparticipant was too significant a risk to confidentiality.
All students requesting treatment at the University Counseling Cen-ter received the study materials and a consent letter explaining that thepurpose of the study was “to assess the attitudes University CounselingCenter clients have towards eating.” All interested new and returning
Wendy D. Hoyt and Steve D. Ross 43
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

clients completed the survey prior to their first appointment for the se-mester. Surveys were collected from all clients regardless of whether ornot they chose to complete the survey. No identifying information wasattached to any of the surveys, and once clients returned the surveys, thesurveys were stored in a separate file and collected weekly by the re-searchers. Although the surveys were anonymous and confidential, allclients were given the option to have the counselor they would be seeingreview their survey. If clients chose to do this, the counselor reviewedthe survey with the client, and then returned the survey to the separatefile without adding any identifying information.
RESULTS
A total of 555 surveys were distributed. Of those administered, 448(80.7%) were returned to the researchers completed. Incomplete sur-veys were not used in the rest of the analyses.
Of the participants who completed the survey, 338 (75.6%) were fe-male, and 109 (24.4%) were male. Ages ranged from 18 to 54 years,with a mean of 24.09 years (SD = 6.35). For males, the average heightand weight was 1.78 meters (SD = .06) and 80.66 kilograms (SD =12.29), respectively. The average EAT score for males was 5.06 (SD =6.13). For females, the average height and weight was 1.65 meters (SD =.06) and 61.67 kilograms (SD = 10.75), respectively. The average EATscore for females was 10.13 (SD = 12.34).
Level of participation in sporting activities (intramural, intermural,or collegiate) and eating disorder symptomology are presented in Table 1.Number of incidences in the past six months for those who indicated en-gaging in binge/purge behavior is presented in Table 2. As expected, theresults indicated that more females than males have engaged in eatingdisordered behaviors. In addition, a much larger percentage of femaleshad EAT scores of 20 or above, and BMI’s of 18 or below. However,more men than women reported engaging in sporting activities.
In order to more closely examine the level of eating disorder pathol-ogy in clients at risk for an eating disorder, participants with an EATscore of 20 or above were examined separately (n = 58), and comparedto individuals with a score below 20 (see Tables 3 and 4). Of the indi-viduals with an EAT-26 score of 20 or above, 87.9% were female, 3.5%had a BMI of 18 or below, 40% had engaged in binges, 53% had usedvomiting to control their weight, and 50% had used laxatives to control
44 JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4
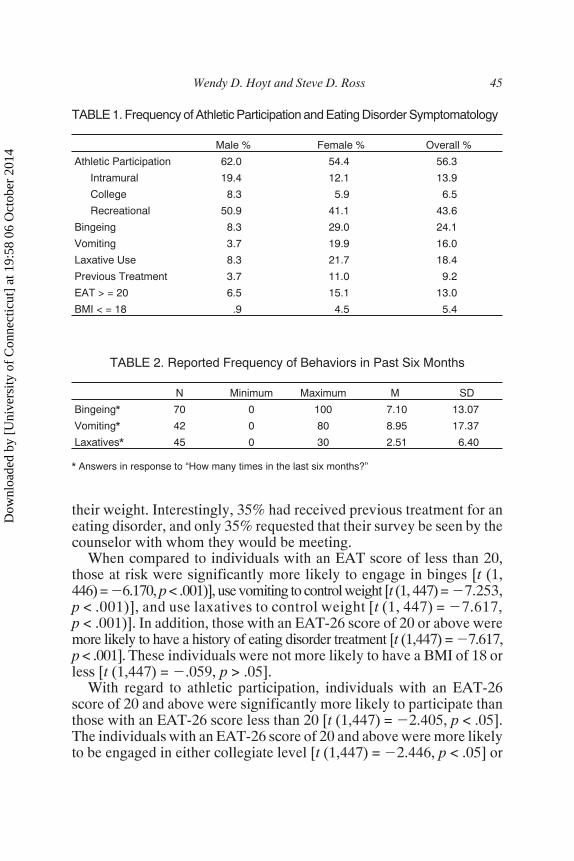
their weight. Interestingly, 35% had received previous treatment for aneating disorder, and only 35% requested that their survey be seen by thecounselor with whom they would be meeting.
When compared to individuals with an EAT score of less than 20,those at risk were significantly more likely to engage in binges [t (1,446) = �6.170, p < .001)], use vomiting to control weight [t (1, 447) = �7.253,p < .001)], and use laxatives to control weight [t (1, 447) = �7.617,p < .001)]. In addition, those with an EAT-26 score of 20 or above weremore likely to have a history of eating disorder treatment [t (1,447) = �7.617,p < .001]. These individuals were not more likely to have a BMI of 18 orless [t (1,447) = �.059, p > .05].
With regard to athletic participation, individuals with an EAT-26score of 20 and above were significantly more likely to participate thanthose with an EAT-26 score less than 20 [t (1,447) = �2.405, p < .05].The individuals with an EAT-26 score of 20 and above were more likelyto be engaged in either collegiate level [t (1,447) = �2.446, p < .05] or
Wendy D. Hoyt and Steve D. Ross 45
TABLE 1. Frequency of Athletic Participation and Eating Disorder Symptomatology
Male % Female % Overall %
Athletic Participation 62.0 54.4 56.3
Intramural 19.4 12.1 13.9
College 8.3 5.9 6.5
Recreational 50.9 41.1 43.6
Bingeing 8.3 29.0 24.1
Vomiting 3.7 19.9 16.0
Laxative Use 8.3 21.7 18.4
Previous Treatment 3.7 11.0 9.2
EAT > = 20 6.5 15.1 13.0
BMI < = 18 .9 4.5 5.4
TABLE 2. Reported Frequency of Behaviors in Past Six Months
N Minimum Maximum M SD
Bingeing* 70 0 100 7.10 13.07
Vomiting* 42 0 80 8.95 17.37
Laxatives* 45 0 30 2.51 6.40
* Answers in response to “How many times in the last six months?”
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

intramural sports [t (1,447) = �2.454, p < .05], but were no more likelyto be engaged in recreational athletics [t (1,447) = �.834, p > .05].
Those participants with a BMI of 18 and below were also examinedseparately (n = 16). As stated previously, individuals with a BMI of 18and below are at greater risk for the development or existence of an-orexia nervosa. However, it should also be noted that these individualsmight be of naturally thin build and not suffering from an eating disor-der. Of the individuals with a BMI of 18 or below, 93.8% were female,
46 JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
TABLE 3. Frequencies Related to EAT-26 Score
EAT-26 � 20 EAT-26 < 20
(n = 58) (n = 387)
Gender
Male 12.1 26.1
Female 87.9 73.9
Athletic Participation
Any Participation 70.7 54.0
College 13.8 5.4
Intramural 24.0 12.1
Recreational 48.3 42.5
Eating Behaviors
Bingeing 60.3 18.7
Vomiting 46.6 11.3
Laxative Use 50.0 13.7
BMI � 18 3.4 3.7
History of ED Treatment 34.5 5.4
TABLE 4. Descriptive Statistics Related to EAT-26 Score
EAT-26 � 20 EAT-26 < 20
M SD M SD
Age 22.3 5.9 24.4 6.4
BMI 22.6 3.7 23.4 4.1
Binges* 5.6 15.6 0.7 3.0
Vomiting* 5.8 16.2 0.3 2.5
Laxative* 2.0 6.6 0.1 0.6
* Answers in response to “How many times in the last six months?”
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

6.3% had engaged in binges, 18.8% had used vomiting to control theirweight, and none had used laxatives to control their weight. A total of18.8% had received previous treatment for an eating disorder, and 25%requested that their survey be reviewed by the counselor with whomthey would be meeting (see Table 5). There were no significant differ-ences on the frequency data between those with and without a BMIscore � 18.
Table 6 presents descriptive statistics related to BMI. There were nosignificant differences between the two groups with regard to age orEAT-26 score. In addition, there was not a significant difference interms of mean episodes of vomiting in the past 6 months. However, thegroup with a BMI score � 18 reported a significantly larger number ofbingeing episodes [t (1,386) = �4.107, p < .001] and laxative use [t (1,385) = �2.49, p < .05].
Finally, only 2 individuals had EAT-26 scores of 20 or above in com-bination with a BMI of 18 or below. However, both of these individualsindicated being involved in athletics and had a history of using vomitingas a means for controlling weight. In addition, both of these individualshad received prior treatment for an eating disorder.
In order to examine the relationship between sports participation andeating disorder symptomatology, individuals who indicated any level of
Wendy D. Hoyt and Steve D. Ross 47
TABLE 5. Frequencies Related to BMI
BMI � 18 BMI > 18
(n = 16) (n = 423)
Gender
Male 6.2 25.3
Female 93.8 74.7
Athletic Participation
Any Participation 37.5 57.1
College 6.3 14.2
Intramural 12.5 6.2
Recreational 18.8 44.5
Eating Behaviors
Bingeing 6.3 24.6
Vomiting 18.8 16.2
Laxative Use 0.0 19.3
History of ED Treatment 18.8 9.0
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

sports participation (n = 252) were examined separately and comparedto participants who did not report sports participation. Of these partici-pants, 11.5% were collegiate level of athletes, 24.6 reported participa-tion in intramural athletics, and 77.4% in recreational athletics. Of theparticipants who participated in sporting activities, 16.4% had an EAT-26score of 20 or above, and 2.4% had a BMI of 18 or below. The sportsparticipants reported high rates of binge/purge activity, with 24.5%having engaged in binges, 17.6% having used vomiting to controlweight and 18.8% having used laxatives to control weight. A total of 29(11.6%) had previously received treatment for an eating disorder. Par-ticipants who reported engaging in sporting activities had higherEAT-26 scores [t (1, 447) = �2.109, p < .05], were more likely to fallwithin the at-risk range on the EAT-26 [t (1, 447) = �2.405, p < .05],and report histories of eating disorder treatment [t (1, 447) = �1.965, p =.05] than did the participants who did not report sport participation.
Due to the fact that female athletes are at a greater risk than male ath-letes, female participants who reported sporting activities were com-pared to females who did not. As expected, the differences between thegroups were even greater; female sports participants had significantlyhigher EAT-26 scores [t (1,335) = �2.570, p < .001], and they weremore likely to fall within the at-risk range on the EAT-26 [t (1, 335) =�3.182, p < .001).
The final stage of this study involved comparing survey results withsubsequent diagnoses given to clients seen during the Spring 2000 se-mester. Formal assessment instruments designed to identify eating dis-orders have never been normal practice in this counseling center setting.Statistics from the two semesters previous, Summer-Fall 1999, showedthat typically 5-15 (depending on the semester) clients were diagnosed
48 JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
TABLE 6. Descriptive Statistics Related to BMI
BMI � 18 BMI > 18
M SD M SD
Age 21.2 2.1 24.2 6.4
EAT-26 12.8 17.4 8.8 11.1
Binges* 0.0 0.0 1.3 6.2
Vomiting* 0.6 2.1 0.9 6.3
Laxative* 0.0 0.0 0.3 2.3
*Answers in response to “How many times in the last six months?”
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

with anorexia nervosa, bulimia nervosa or eating disorder not otherwisespecified. During the time of this study, a total of 55 clients received aneating disorder diagnosis as either a primary or secondary diagnosis.The specific diagnoses received are presented in Table 7. This repre-sents a 320% increase in eating disorder diagnoses from the Fall 1999semester to the Spring 2000 semester. Interviews with one counselor re-vealed the following thoughts as to why this increase occurred:
I suspect I learned more about the full extent of clients’ ED behav-iors and concerns because of the survey; I suspect they might haveminimized those behaviors and concerns upon my queries if thiswasn’t their presenting concern.
DISCUSSION
Some limitations of the present study should be recognized. The factthat all participants had to remain anonymous reduced our ability to de-termine which individuals requested that their counselor review the sur-vey, and which individuals eventually received eating disorder diagno-ses. We cannot definitively determine the causal relationship betweenusing this survey and increased diagnoses. However, trends from previ-ous semesters and comments from current counselors can be used tohelp determine the effects of the EAT-26. In addition, we must recog-nize that there is a high likelihood that the percentages reported in thisstudy are actually lower than the actual prevalence of eating disorder
Wendy D. Hoyt and Steve D. Ross 49
TABLE 7. Eating Disorder Diagnoses Given During the Spring 2000 Term
Diagnosis Number of Clients Percent*
Primary 46 83.6
Anorexia Nervosa 5 9.1
Bulimia Nervosa 11 20.0
Eating Disorder NOS 30 54.5
Secondary 9 16.4
Anorexia Nervosa 2 3.6
Bulimia Nervosa 3 5.5
Eating Disorder NOS 4 7.3
* Percent of eating disorder diagnoses
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

symptomatology, due to the secretive nature of these disorders and theface validity of the EAT-26 instrument. Previous researchers havefound that as many as 38.5% of women who refuse to participate in sur-veys related to eating disorders actually have symptoms of an eatingdisorder (Beglin & Fairburn, 1992). The EAT-26 is a face valid instru-ment; thus, most participants were probably aware of the purpose of thestudy and some clients who actually had eating disorder symptoms mayhave refused to complete the survey.
It has long been known that college students are at an increased riskfor the development of an eating disorder. Typically, the college envi-ronment is one that emphasizes physical attractiveness, which is cur-rently socially defined as thin and/or physically fit. The ideal appearancefor both men and women almost demands careful attention to diet andexercise routines. In this study, a total of 72, or 12.9%, of the 555 menand women had an EAT-26 of 20 or above or had a BMI of 18 or less,both of which are indicative of an individual at-risk for the developmentof an eating disorder. Of these clients, 90% were female. These data areconsistent with previous studies indicating that 90-95% of individualswith disordered eating are female. It is important to note that only twowomen had both a high EAT-26 score and a low BMI. This supports thediagnostic reality that many of the individuals at-risk for an eating dis-order are not easily recognizable from their body size.
Over 50% of the clients within the at-risk range engaged in binge/purgebehavior. In addition, clients who participated in sports activities re-ported relatively high levels of binge/purge behavior. Approximately12% of the sports participants had previously received treatment for aneating disorder. These are numbers one might expect in elite athletics,but it is important to note that the majority of the participants indicatedbeing involved in recreational, non-competitive sporting events. Only6.5% of the participants were involved in college athletics. Therefore,college counselors need to be aware that the clients they see who are en-gaging in sports, college or recreational, may be at an increased risk forthe development of an eating disorder.
To our knowledge, prior to this study, the prevalence of eating disor-dered behavior in counseling center clients has never been assessed.Additionally, eating disorders, by their very nature, have significant el-ements of secrecy and shame–elements that lead to underreporting. As aresult, many individuals with eating disturbances frequently present atcounseling centers with co-occurring symptoms of depression, anxiety,low self-esteem, and relationship difficulties. An underlying eating dis-order is often discovered later in treatment as a result of either the client
50 JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

withholding information and/or the intake counselor being less awareof questions important for effective eating disorder assessment.
It was hypothesized that both clients and counselors would be “primed”to disclose or recognize eating disturbances if clients completed theEAT-26 prior to an assessment. As expected, the number of eating dis-order diagnoses did increase. What was surprising was the rate of in-crease. Over three times as many individuals received eating disorderdiagnoses as in previous semesters. Although it is impossible to identifythe specific cause of the increase in diagnoses, perhaps providing an ini-tial assessment instrument made it easier for clients to talk about theirstruggles. However, it is also fair to speculate that using the EAT-26heightened counselor awareness around eating disorder signs andsymptoms, leading to a greater depth of questioning regarding eating is-sues. Both of these effects are consistent with those reported by Cowanand Morewitz (1995).
Increasing counselor awareness of eating disturbances is a vital keyto effective diagnosis and treatment. In this study, only 35% of clientswith an EAT-26 of 20 or above, and only 25% of clients with a BMI of18 or below requested that their survey be reviewed by the counselorthey would be seeing. Therefore, it is likely that 65-75% of the clientswith eating disorder symptoms did not openly disclose eating relatedproblems to the counselor. Although it is possible that some clients dis-closed to their counselor without showing him/her their EAT-26, thisdoes not seem likely. However, the fact that the counselors were moreaware of eating disorder signs and symptoms likely contributed to in-creased detection.
Also important are the diagnoses actually given by the individualcounselors. An eating disorder diagnosis was given as a primary diag-nosis in 84% of the cases in which an eating disorder diagnosis wasgiven. However, the most common eating disorder diagnosis given wasEating Disorder Not Otherwise Specified. Counselors in a college set-ting are frequently trained to recognize symptoms of anorexia nervosaand bulimia nervosa, but detecting more subtle cases can often be muchmore difficult. Use of instruments such as the EAT-26 may make as-sessing the level of symptomatology in clients easier. In addition, in-creasing counselor awareness is fundamental in recognizing less “cutand dried” or “textbook” eating disorder cases.
In conclusion, the data presented here clearly show that eating disor-ders are a major issue for college counseling centers. In addition, the in-crease in diagnoses from previous semesters to the Spring 2000 semesterindicates that symptoms of eating disorders, and particularly those in in-
Wendy D. Hoyt and Steve D. Ross 51
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

dividuals with less specific types of eating disorders (i.e., Eating Disor-der Not Otherwise Specified), are frequently not addressed. Thus, itseems that administering a short questionnaire such as the EAT-26 dur-ing an extended assessment or the beginning stages of therapy could in-crease therapeutic awareness of the more subtle signs of eating disorderpsychopathology.
Recommendations
The results of the current study are consistent with the notion thatmany college students suffering from disordered eating are hesitant toshare their behaviors with counselors. This is evident in the fact thatonly 35% of the students with scores of 20 or above on the EAT-26chose to share their survey with their counselor. Researchers and clini-cians working with individuals with eating disorders frequently see therelationship between shame and guilt clients have about eating disorderbehaviors and secrecy about these behaviors. As mentioned, this some-times can lead to intake counselors, and even individual counselors, be-ing unaware of eating disorder behaviors until later in treatment. Thus,we present the following recommendations:
1. Based on the notion of a priming effect, it is recommended thatcounseling centers include in their initial paperwork some ques-tions related to eating disorder behaviors. Counseling centerscould utilize instruments such as the EAT-26, or simply include ashorter set of questions assessing eating disorder behaviors alongwith other demographic information. This sets a tone indicatingthat it is acceptable to address these behaviors.
2. Due to the high prevalence of disordered eating on college cam-puses, counseling centers would benefit from participating inyearly staff development presentations related to effective initialassessment of eating disorder symptoms and appropriate diagnosis.
3. Some counseling centers may benefit from designating particularstaff to conduct eating disorder assessments. These staff may beselected based on level of clinical expertise, level of assessmentknowledge/skill or other related factors. Counseling centers shouldbe cautious to not limit eating disorder assessment/treatment to fe-male counselors, as this can unintentionally reinforce the notionthat eating disorders are “female disorders,” thus possibly in-creasing shame for males with disordered eating.
4. In order to reduce clients’ sense of shame, counselors should striveto ask specific eating disorder related questions in a straightfor-
52 JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

ward and accepting manner, thus “normalizing” the behaviors andhopefully reducing clients’ fear that the counselor will view themnegatively for engaging in such behaviors.
5. Counselors should be prepared to ask about specific behaviors, in-cluding any incidence of fasting/starving, binge eating, purging(by vomiting, laxative use, use of diet pills and other products,and/or exercise), compulsive overeating, weight loss or gain. Coun-selors should also question whether the individual has any historyand/or treatment of these behaviors.
6. Counselors should be careful to ask these questions of all clients,regardless of gender, ethnicity, sexual orientation, SES or otherdiversity characteristics, and should be specially aware of groupsat higher risk for the development of eating disorders (i.e., ath-letes, sorority members, students in certain majors, etc.).
REFERENCES
American Psychiatric Association. (1994). Diagnostic and statistical manual of men-tal disorders: DSM-IV. Washington, DC: Author.
Beals, K. A., & Manore, M. M. (1994). The prevalence and consequences of subclinicaleating disorders in female athletes. International Journal of Sports Nutrition, 4,175-195.
Beglin, S. J., & Fairburn, C. G. (1992). Women who choose not to participate in sur-veys on eating disorders. International Journal of Eating Disorders, 12, 113-116.
Burckes-Miller, M. E., & Black, D. R. (1988). Male and female college athletes: Preva-lence of anorexia nervosa and bulimia nervosa. Athletic Training, 22, 137-140.
Cowan, P. F., & Morewitz, S. J. (1995). Encouraging discussion of psychosocial issuesat student health visits. Journal of American College Health, 43, 197-199.
Davis, C., Katzman, D. K., Kapstein, S., Dirsh, C., Brewer, H., Kalmback, K., Olmstead,M. P., Woodside, D. B., & Kaplan, A. S. (1997). The prevalence of high-level exer-cise in the eating disorders: Etiological implications. Comprehensive Psychiatry,38, 321-326.
Davis, C., Kennedy, S. H., Ravelski, E., & Dionne, M. (1994). The role of physical ac-tivity in the development and maintenance of eating disorders. Psychological Medi-cine, 24, 957-967.
Edwards-Hewitt, T., & Gray, J.J. (1993). The prevalence of disordered eating attitudesand behaviours in Black-American and White-American college women: Ethnic,regional, class and media differences. Eating Disorders Review, 1, 41-54.
Garner, D. M. (1993). Self-report measures for eating disorders. Current Contents, So-cial and Behavioral Sciences, 25, 8.
Garner, D. M. (1997). Psychoeducational principles in treatment. In: D.M. Garner & P. E.Garfinkel (Eds.), Handbook of Treatment for Eating Disorders (pp. 145-177) NewYork: Guilford Press.
Wendy D. Hoyt and Steve D. Ross 53
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4

Garner, D. M., Olmsted, M. P, Bohr, Y., & Garfinkel, P. E. (1982). The eating attitudestest: Psychometric features and clinical correlates. Psychological Medicine, 12,871-878.
Heatherton, T. F., Nichols, P., Mahamedi, A. M., & Keel, P. (1995). Body weight, diet-ing, and eating disorder symptoms among college students, 1982 to 1992. AmericanJournal of Psychiatry, 152, 1623-1629.
Kurth, C., Krahn, D., Nairn, K., & Drewnowski, A. (1995). The severity of dieting andbingeing behavior in college women: Interview validation of survey data. Journalof Psychiatric Research, 29, 211-225.
Long, C. G., Smith, J., Midgley, M., & Cassidy, T. (1993). Over-exercising in anorexicand normal samples: Behavior and attitudes. Journal of Mental Health, 2, 321-327.
Lucas, A. R., Crowson, C. S., O’Fallon, W. M., & Melton, L. J. (1999). The ups anddowns of anorexia nervosa. International Journal of Eating Disorders, 26,397-405.
Mintz, L. B., & O’Halloran, M. S. (2000). The eating attitudes test: Validation withDSM-IV eating disorder criteria. Journal of Personality Assessment, 74, 489-503.
Nelson, W. L., Hughes, H. M., Katz, B., & Searight, H. R. (1999). Anorexic eating atti-tudes and behaviors of male and female college students. Adolescence, 34, 621-633.
Pederson, M. M., Crosby, R. D., Crow, S. J., Knopke, A. J., Peterson, C. B.,Wonderlich, S. A., & Mitchell, J. E. (2000). Utilization of empirically supportedpsychotherapy treatments for individuals with eating disorders: A survey of psy-chologists. International Journal of Eating Disorders, 27, 230-237.
Schwitzer, A. M., Bergholz, K., Dore, T., & Salimi, L. (1998). Eating disorders amongcollege women: Prevention, education, and treatment responses. Journal of Ameri-can College Health, 46, 199-207.
Sundgot-Borgen, J. (1994). Risk and trigger factors for the development of eating dis-orders in female elite athletes. Medicine and Science in Sports and Exercise, 2,414-419.
Szymanski, L. A., & Chrisler, J. C. (1991). Eating disorders, gender role and athleticactivity. Psychology–A Quarterly Journal of Human Behavior, 28, 20-29.
Winzelberg, A. J., Taylor, C. B., Sharpe, T., Eldredge, K. L., Dev, P., & Constantinou,P. S. (1998). Evaluation of a computer-medicated eating disorder intervention pro-gram. International Journal of Eating Disorders, 24, 339-349.
Wolf, E. M., & Akamatsu, T. J. (1994). Exercise involvement and eating-disorderedcharacteristics in college students. Eating Disorders, 2, 308-318.
RECEIVED: 10/03/01REVISED/ACCEPTED: 03/09/02
54 JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
Dow
nloa
ded
by [
Uni
vers
ity o
f C
onne
ctic
ut]
at 1
9:58
06
Oct
ober
201
4