
Clinical Analysis of 3160 Patients with Epidemic non-A and ...
7
105 Clinical Analysis of 3160 Patients with Epidemic non-A and non-B Hepatitis in Xinjiang of China Chao SHU-YAN Department of Infections Disease, Xinjiang Regional People's Hospital Urumqi, CHINA Key words: ENANB• H, Clinical analysis, Xinjiang, China Summary In this paper, the patients were from in-patient in epidemic area. The diagnosis was made by exeluding other type of virus hepatitis, and has been proved that it is Epidemic non-A and non-B Hepatitis (ENANB •H) and it was spreaded by gastrointestinal tract. The mode of transmission was similar to hepatitis A. The clinical manifestations and abnormality liver functions were mild than hepatitis A or B. Most of them were young and middle-aged people. The pregant women were nore susceotible to this type of hepatitis and the mortatity was higher. The hemorrhage may be primary factor of the death of ENANB • H. The histological findings were inflammation in the portal area, Cholestasis and Sportt-patchy necrosis. On transmission electron microscope (TEM), the virus particle, 26-30 nm, presented in cytoplasm. The patients wer followed up during the convalescence, which tend to chronization. It is reported that ENANB • H has been epidemic in neibouing countries-India, Burma, Nepal, Soviet and Parkistan etc1>-11) for ten years. Since 1980, the spordic epidemic has presented in south Xinjiang. The outbreak epidemic was presented from Sep. 1986 to May 1988, in this paper the clinical manifestations were reported. Materials and Methods 1 Patients with ENANB• H were diagnosed, and Choiced by random sampling from population at different stage of disease from the local hospitals. 2 The diagnostic standard and different types were in according to Nan-nine meeting of China in 1984, and excluding other types of virus hepatitis. 3 Serological test: Labe-HBV and anti-HBV-IgM were determined by means of RPHA and ELISA respectively. The reagents were provided by Beijing Biological Producted Institute, Beijing Biochemical Immune Center and Tan Shan Prevented Station. 4 Examined liver function and amine acid were determined by Biochemical Laboratory of our hospital and Certer Laboratory of Xinjiang Agriculture Institute. Result General materials: 3160 cases in which 1484 of male and 1676 of female were found. The youngest was 1.5, the oldest was 102 and the mean was 27 + 0.6 years old, 19-49 years old was 85.4 per cent. So, most of them were young people. The distribution of rations were similar to the proportion of national 別刷請求先: Xinjiang Vighur Auto mous Region, China the Department of Infection Disease People's Hospital, Urumqi. Chao Shu-Yan 平成2年1月20日
Transcript of Clinical Analysis of 3160 Patients with Epidemic non-A and ...

105
Clinical Analysis of 3160 Patients with Epidemic non-A and non-BHepatitis in Xinjiang of China
Chao SHU-YAN
Department of Infections Disease, Xinjiang Regional People's Hospital Urumqi, CHINA
Key words: ENANB• H, Clinical analysis, Xinjiang, China
Summary
In this paper, the patients were from in-patient in epidemic area. The diagnosis was made by exeluding
other type of virus hepatitis, and has been proved that it is Epidemic non-A and non-B Hepatitis
(ENANB • H) and it was spreaded by gastrointestinal tract. The mode of transmission was similar tohepatitis A. The clinical manifestations and abnormality liver functions were mild than hepatitis A or B.
Most of them were young and middle-aged people. The pregant women were nore susceotible to this type of
hepatitis and the mortatity was higher. The hemorrhage may be primary factor of the death of ENANB • H.
The histological findings were inflammation in the portal area, Cholestasis and Sportt-patchy necrosis. On
transmission electron microscope (TEM), the virus particle, 26-30 nm, presented in cytoplasm. The
patients wer followed up during the convalescence, which tend to chronization.It is reported that ENANB • H has been epidemic in neibouing countries-India, Burma, Nepal, Soviet
and Parkistan etc1>-11) for ten years. Since 1980, the spordic epidemic has presented in south Xinjiang. The
outbreak epidemic was presented from Sep. 1986 to May 1988, in this paper the clinical manifestations
were reported.
Materials and Methods
1 Patients with ENANB• H were diagnosed, and Choiced by random sampling from population at
different stage of disease from the local hospitals.2 The diagnostic standard and different types were in according to Nan-nine meeting of China in
1984, and excluding other types of virus hepatitis.
3 Serological test: Labe-HBV and anti-HBV-IgM were determined by means of RPHA and ELISA
respectively. The reagents were provided by Beijing Biological Producted Institute, Beijing Biochemical
Immune Center and Tan Shan Prevented Station.
4 Examined liver function and amine acid were determined by Biochemical Laboratory of our
hospital and Certer Laboratory of Xinjiang Agriculture Institute.
Result
General materials: 3160 cases in which 1484 of male and 1676 of female were found. The youngestwas 1.5, the oldest was 102 and the mean was 27 + 0.6 years old, 19-49 years old was 85.4 per cent. So,
most of them were young people. The distribution of rations were similar to the proportion of national
別刷 請求先: Xinjiang Vighur Auto mous Region,
China
the Department of Infection Disease
People's Hospital, Urumqi.
Chao Shu-Yan
平成2年1月20日
106 Chao SHU-YAN
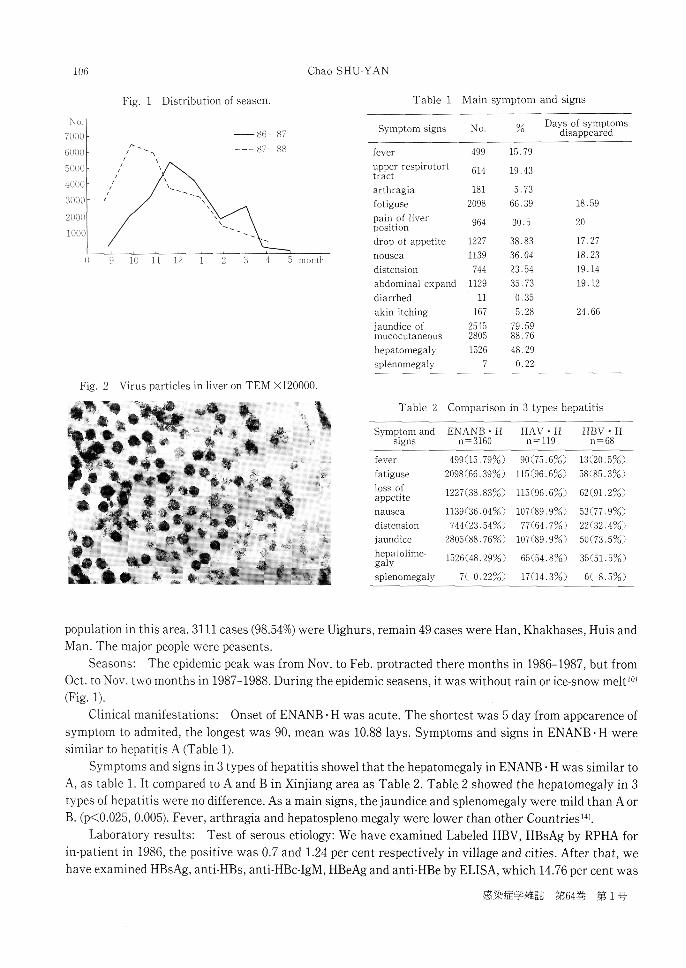
Fig. 1 Distribution of seasen.
Fig. 2 Virus particles in liver on TEM X120000.
Table 1 Main symptom and signs
Table 2 Comparison in 3 types hepatitis
population in this area. 3111 cases (98.54%) were Uighurs, remain 49 cases were Han, Khakhases, Huis andMan. The major people were peasents.
Seasons: The epidemic peak was from Nov. to Feb. protracted there months in 1986-1987, but from
Oct. to Nov. two months in 1987-1988. During the epidemic seasens, it was without rain or ice-snow melt10
(Fig. 1).Clinical manifestations: Onset of ENANB • H was acute. The shortest was 5 day from appearence of
symptom to admited, the longest was 90, mean was 10.88 lays. Symptoms and signs in ENANB • H were
similar to hepatitis A (Table 1).
Symptoms and signs in 3 types of hepatitis showel that the hepatomegaly in ENANB H was similar to
A, as table 1. It compared to A and B in Xinjiang area as Table 2. Table 2 showed the hepatomegaly in 3
types of hepatitis were no difference. As a main signs, the jaundice and splenomegaly were mild than A or
B. (p<0.025, 0.005). Fever, arthragia and hepatospleno megaly were lower than other Countries14Laboratory results: Test of serous etiology: We have examined Labeled HBV, HBsAg by RPHA for
in-patient in 1986, the positive was 0.7 and 1.24 per cent respectively in village and cities. After that , wehave examined HBsAg, anti-HBs, anti-HBc-IgM, HBeAg and anti-HBe by ELISA, which 14.76 per cent was
感染症学雑誌 第64巻 第1号

Anaysis of Patients with non-A non-B Hepatitis 107
Table 3 Test of liver functions
Table 4 Comparal 3-types of hepatitis test of
liver functions
Table 5 Results of partial biolochemistry
Table 6 Result of coagulant factors test
ab. = abnomal
positive. Anti-HAVIgM ELISA was 3.67 per cent of positive. 3160 cases in this paper have been exeluded
above-mentional cases.
Tests of liver functions (Table 3, 4, 5, 6): In Table 3 and 4, the bilirubin and glutamic-pyruvic
transaminase (GPT) were changed more prominent in ENANB•EH. Three types compared to each other,
bilirubi in ENANB•EH increased than A or B markedly (p<0.001). Table 5 showed the pregnant and severe
平成2年1月20日

108 Chao SHU-YAN
Table 7 Clinical features of each type of hepatitis
cases do not dissociated jaundice with enzyme. The bilirubin was mean 6.16 mg% in severe case, but AKP,
Cholesterin and HDL-c were more decreased. Therefore, this three parameter can be predict the severity
and prognosis. The thrombin time in these two types were prolonged markedly (Table 6). It showed that
the factor II was abnormal in ordinary type, in other two types were the abnormal markedly. The factor V
and thrombocyto (TBC) decreased in pregnant type. The factor V, VII decreased some time with factor VIII,
but the thrombocytopenia was mild than pregnant. Therefore, the score of the hemorrhage is because of
liver dysfunctions. In several cases developed DIC.
The amino acid was analysed for 10 cases of ordinary type and 10 cases severe types , the ratio of
BCAA/AAA is small than one, It's cause is unclear.
Biopsy of liver: The specimens of hepatic tissues of 22 patents showed inflammation in portal area,
degeneration in varying degree, chlolestasis, sport or patchy necrosis, bile pigment deposit, bile thrombus
and cholangiectasis on light microscope. On TEM, mitochondrial swelling, dilated endoplasmic reticulum,
degranulation, increasing glycogen granule, cell organ necrosis and nucleole hyperfunction were found. On
the basis we divided it into 4 types: mild, chlolestasis necrosis and mixed. 26-30 nm virus partiles was
found in two speciment. It's size and shape were similar to find virus partiles in stool .
Clinical classification and characters: 3160 cases can be divide into acute ieterie form being 75.98 per
cent (2401/3160), acute unicteric form being 15.28 per cent (483/3160), severe form being 8.67 per cent
(273/3160). In severe type included acute form of 258 cases and subacute form of 15 cases. Chlolestasis form
was 0.09 per cent (3/3160). Therefore, most of ENANB•EH were acute form, being 91.23 per cent, and
similar to hepatitis A.
The Table 7 showed the characters of ENANB•EH in pregnant, severe, aged and infant. ENANB•EH was
similar to hepatitis B in middle-aged. In infant ENANB•EH, middle-school-ages was 76.19 per cent (144
cases) and higher than under three years old cases which was 23.8 per cent (45 cases). Their 58 patients
were followed up, which clinical features disapper and liver function was normal. Pregnant ENANB•EH
was 23.6 per cent and more than hepatitis B which was 1.9 per cent (3/157 p<0.001) at the sametime in this
local. Severe form was 24.4 per cent (182/746). Among which pregnant was 66.1 per cent (182/273) and 15.6
per cent of mortlity which was higher than hepatitis B which three patients complicated pregnant to not be
感染症学雑誌 第64巻 第1号

Anaysis of Patients with non-A non-B Hepatitis 109
sovere form or death. So, pregnent with ENANB•EH was severe and death easily.
Treatment, course and prognosis: ENANB•EH is an auto-limited disease which they tend to disappear
spontaneously and the severe cases are using combined treatment. There are to speak of:
1 It was comsidered using steroid for severe cases at early stage. In this type, most of patients were
pregnant, who presental a hypercoagulability in perinatal period. Whether or not eflected for steriod which
may be two groups for analysis, the mortality with sterid was 71.4 per cent (20/25), but without sterid was
51 per cent (27/53), there was no diference between two groups (p>0.05). It would be further observed and
comfirmed.
2 Pregnant hepatitis was "upgrod theraly" in tranditional ideas. The hemorrhage due to death is
much more in this type. Therefore, Monitering coagulant factors and corecting in time, the nursing was
strengthened in the puerperium and stages of labor, which may be incresing survival rate. We have been to
take combined therapy at ante partum for 98 cases of postpartum. ENANB•EH, which mother and infant
were sare and sound.
Course of disease: The hospitalization averaged 25 days, the clinical remission averaged 14.5 days,
the jaundice diseppear an average of 17.8 days but personal may be come of 120 days. There are 30 per cent
of case which SGPT returned to normal but still preseated mild jaundice and hepatomegaly disappeared an
average of 26.59 days.
Prognosis: In 3160 patients with ENANB•EH, the cure rate was 94.8 per cent and the mortality was
5.3 per cent, which was lower than other country14). Severe patient's mortality was 61.5 per cent, pregnant
and parturient were 15.5 per cent. The patients of death all have hepatic coma. The pure coma led up to
death that was 21.87 per cent, coma IV-V grad and complicated cerebra edema. Coma with hemorrhage was
67.84 per cent, in which third two developed postpertum hemorrhage and secondary coma. Coma with
assciation hemorrhage and renal failure was 9.3 per cent of mortality. Infection and operation were one per
cent of mortality in coma cases. In these patients are 24 male and 144 female. The mortality in pregnant
and parturient were four times than without one's. During the period of pregnancy protracted more than
three months, the mortality was 81.9 per cent.
Discharged three months later, the patient was without other infection and presental typical symptom
of hepatitis, which admited again to be 6.88 per cent, 500 cases convalescence were follow up at 1, 3, 6, 12
months, examined clinic, liver function and ultrasonography. In one year the resuld showed liver pein was
36.4 per cent (182/500), abdomen distension was 2 per cent (10/500), liver dysfunction was 27.2 per cent,
one year later, hepatomegaly was 12.8 per cent (64/500), splenomegaly was 0.6 per cent (3/500), increasing
GPT was one per cent, increasing y globulin was 28 per cent (28/100). It is suggested that ENANB•EH may
tend to chroniation, whith this condition differ from other countries").
Comment
In last ten years, ENANB•EH was pay closed attention to day by day in Asia and Northwest Africa. It is
known that ENANB•EH was similar to hepatitis A in epidemic and clinic. The virus granule have been fund
in patients stool in China.
1980-1986, ENANB•EH developed from spordic to outbreak in Xinjiang of China. The patients in this
paper, ENANB•EH was diagnosed by excluding hepatitis A and B, overloping and mixed infection so that get
a clear understanding of it. It is showed that the clinical features were mild than hepatitis A and than
ENANB•EH in other countries too. On liver function, the increasing bilirubin was prominent; bilirubin in
severe cases was mean 6.16 mg%, do not dissociated jaundice with enzyme. Before death, biopsy of liver
found out the degeneration and edema in hepatic cells, which suggested the characters of clinic and
pathology which provided a suprot for emergency treatment to a patient. Virus serous type and it's
平成2年1月20日

110 Chao SHU-YAN
classification must be further a study. Because of the type tend to one type in other countrios.
The mortality of ENANB•EH was higher. It is reported that the mortality was 12 per cent, in pregnancy
andpuerperant were 20-39 per cent14). This paper reported the mortality was 5.3 per cent, pregnancy and
pureperant were 15.5 per cent, which is lower than reporting of tother countries. Today, the cause of death
do not reported in literature. We have observed that the cause of death is hemorrhage. For monitering
coagulant, the abnormal coagulant is prominent dysfunction of liver. The abnormal factor II was in
ordinary form, defect of factor V was presented in pregnant ENANB•EH, but the puerperant can be salf-
regulation and compensation. It developed to a severe form, which the factor VII and/or factor VIII was
decreased, who all died. Therefore, most of the patient can be rescued for complement coagulant factors. It
is important that perfomed the monitoring coagulant factors for severe and pregnatn form. The decreasing
factor II-V-VII, HDL-C and cholesterol were a dangerous mark. Nest, in some patients prolonged
prothrombin time (PT) and thromocytopenia suggest a developing DIC. DIC was appeared easily in
perinatal period. This two conditions all lend to hemorrhage, worsehed, hypoxia and damage liver, result in
coma finally. After coma, worsened hemorrhage, appeared renal failure, multiple organs failure and death.
Certainly these factors were presented at same time.
It is known that the pregnant and puerperant with ENANB•EH appeared infection, worsening and
death easily1)-14). Pregnant and pureperant in severe cases in this paper were 66.1 per cent. At this time, it
developed premature birth, abortion, dead fetus and dead infant. Theae complications have a injury to
fetus, which the virus of ENANB•EH whether directed to placenta and embryo or indirected, perhaps
dysfunction of detoxification, unclear. We observed 58 infant without features of hepatitis, in the absence
of diagnostic serum, the infectious infant could not excluded.
Chronization of ENANB•EH was not reportedlo in other countries, we followed up for one year, in some
patients, who the clinical features and liver function do not return normal, remains to be comfirmed on
pathology.
Reference
1) Khuroo et al.: Study of an epidemic of non-A, non-B hepatitis possibility of another human hepatitis virus distinct
from post-transfusion non-A non-B type. Am. J. Med., V80, P818, 1980.
2) Tandon, B. N., et al.: An epidemic of non-A non-B hepatitis in North India. Indian J. Med. Res., May V75, P739-744,
1982.
3) Belabbes, H., et al.: non-A, non-B epidemic viral hepatitis in Algeria strong evidence for its water Spread in: vyas
GN, Dienstag J. C., Hoafnagle J. H. (Eds): viral hepatitis and liver diseases . New York, G. rune and Stratton Inc.,
P637, 1984.
4) Glynn, M J., et al.: Inported Epidemic non-A, non-B Hepatitis in Qater. J. Med. Viral., 17 (4): 375, 1985.
5) Myint Hla, et al.: A clinical and epidemiological Study of an epidemic non-A, non-B hepatitis in Rangoon . AM. J. Trop
Med. Hyg., 34 (6): 1183-1189, 1985.
6) Kane, M.A., et al.: Epidemic non-A non-B hepatitis in Nepal: Receovery of a possible etiologic agent and transmission
Studies in marmosets. JAMA., 252 (22): 3140-3145, 1984.
7) Furuta, S., et al.: Epidemiological clinical aspect of non-A, non-B, hepatitis Igaku no ayumi 136: 1052, 1986.
8) Molini, et al.: Acute apidemic non-A non-B hepatitis: Clinical study of 38 cases seen in chad, Gas Clin Biol 10(6-7):
475-9, 1986.
9) T. K. 3AHPOB: 3JIEKTPCHHO MHKPOCKOHHLIECKHE HCCJIE)1 OB AHHSI IIPH BHPYCHOM TEIIATI4TE
1III A HHB C„U „UEKAJIPHO-OPAJIPHbIM MEXAHH3MOM 11EPEgA„XH HH„UEK LAHH . BOIIPOCbI
BHPYCOJIOTH H. No. 2 172-175, 1986.
10) Liu Yu-Zhang et al.: Chnese Journal of preventive medicine. 20 (4): 209, 1986.
11) Ji Xing-Sheng et al.: Chinese Journal of public health. 5157: 27-29, 1986.
12) Doris, C. Wong et al.: Epidenmic and endemic Hepatitis in India: Evidence for a non-A non-B heptitis vitus
Aetiology. Iancet V(8200): 876-878, 1980.
13) VI. B. I.IIAXTIIJIE„^5IH: „^III4 EMHOJIOFI4 ECKHE OCObEHHOCTI4 BI4PY CHOTO I,EJIATHTA HI4 A H1 B
感染症学雑誌 第64巻 第1号

Anaysis of Patients with non-A non-B Hepatitis 111
CeEKAJIEHOOPAHEHMM MEXAHH3MOM HEPE,IIALIH. BOJIPOCEI BHPYCOJIOF HI4 No.2, P175-179,1986.
14) Zhuang Hui: Chinese journal of epidemiology. 8(1): 58-91, 1978. External medicine (epidemic, infectious volume),1986, 2, P67.
15) Tian Geng-Shan: External medicine (epidemic, infectous volume), 5, 193-196, 1987.16) Song Guo-Pei: Chinese Journal of clinical hepatology: 3, 179-185, 1987.17) Balatan, M. S., et al.: Evidence for a cirus in non-A non-B hepatitis transmitted Via the Fecal-oral Route. Interviology
V2, P23-31, 1983.18) Joshi, Y. K., et al.: Immunoprophylaxis of epidemic non-A non-B hepatitis. Indian J. Med. Res., V81, January,
P18-19, 1985.19) Zhang Tai-He: Chinese journal of internal medicine. 1985, Supplement P11-13.20) Shen Gebg-Rong, et al.: External medicine (internal volume), 8, P347-352, 1987.21) Re Zhong-Lin: Xinjiang hygiene and prevention, 1-2, P56-64, 1987.
中国新彊 における流行性非A非B型 肝炎3,160例 の臨床的検討
新彊維吾尓自治区人民医院
趙 素 元
(平成1年1月10日 受付)
(平成1年6月6日 受理)
要 旨
本論文においては非A非B型 肝炎流行地域患
者を対象 とした.非A非B型 肝炎の診断は他 の
原因による肝炎が否定 され流行性である事により
下 した.感 染の形式は経 口感染であった.本 症の
臨床症状及び検査値異常 はA型 及びB型 肝炎 よ
り軽度であった.年 齢分布では青壮年層に多 く,
また妊婦は感染 しやす く致命率も高かった.
本症の主たる死因は出血であった.病 理組織学
的所見では門脈域の炎症所見及び胆汁欝帯並びに
巣状壊死巣が認められた.透 過型電子顕微鏡にお
いて細胞質内に26~30nmの ウイルス粒子を認め
た.
回復期患者の経過を観察 したが慢性化す る傾向
を認めた.
(付記):本 文は著者の同意を得て英文要旨を編
集委員会において和訳 した.
平成2年1月20日


















