Clin Infect Dis. 2011 Phyo 977 84

of 8
-
Upload
erlangga-perwira-negara -
Category
Documents
-
view
213 -
download
0
Transcript of Clin Infect Dis. 2011 Phyo 977 84
-
7/28/2019 Clin Infect Dis. 2011 Phyo 977 84
1/8
M A J O R A R T I C L E
Dihydroartemisinin-Piperaquine Versus
Chloroquine in the Treatment of Plasmodiumvivax Malaria in Thailand: A RandomizedControlled Trial
Aung Pyae Phyo,1 Khin Maung Lwin,1 Ric N. Price,4,5 Elizabeth A. Ashley,1,2,5 Bruce Russell,6 Kanlaya Sriprawat,1
Niklas Lindegardh,2,5 Pratap Singhasivanon,3 Nicholas J. White,2,3 and Francxois Nosten1,2,3
1Shoklo Malaria Research Unit, Mae Sod, 2Mahidol Oxford Research Unit, and 3Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand;4Global Health Division, Menzies School of Health Research, Charles Darwin University, Australia; 5Centre for Tropical Medicine, Nuffield Department
of Clinical Medicine, University of Oxford, United Kingdom; and 6Laboratory of Malaria Immunobiology, Singapore Immunology Network, Biopolis,
Agency for Science Technology and Research (A*STAR)
Background. Chloroquine (CQ) remains the treatment of choice for Plasmodium vivax malaria. Initiallyconfined to parts of Indonesia and Papua, resistance of P. vivax to CQ seems to be spreading, and alternative
treatments are required.
Methods. We conducted a randomized controlled study to compare the efficacy and the tolerability of CQ and
dihydroartemisinin-piperaquine (DP) in 500 adults and children with acute vivax malaria on the Northwestern
border of Thailand.
Results. Both drugs were well tolerated. Fever and parasite clearance times were slower in the CQ than in the DP
group (P, .001). By day 28, recurrent infections had emerged in 18 of 207 CQ recipients compared with 5 of 230
treated with DP (relative risk, 4.0; 95% confidence interval [CI], 1.5110.58; P5 .0046). The cumulative risk of
recurrence with P. vivaxat 9 weeks was 79.1% (95% CI, 73.5%84.8%) in patients treated with CQ compared with
54.9% (95% CI, 48.2%61.6%) in those receiving DP (hazard ratio [HR], 2.27; 95% CI, 1.82.9; P, .001). Children
,5 years old were at greater risk of recurrent P. vivax infection (74.4%; 95% CI, 63.2%85.6%) than older patients
(55.3% [95% CI, 50.2%60.4%]; HR, 1.58 [95% CI, 1.12.2]; P5 .005). In vitro susceptibility testing showed that
13% of the tested isolates had a CQ median inhibitory concentration .100 nmol/L, suggesting reduced susceptibility.
Conclusions. The efficacy of CQ in the treatment of P. vivax infections is declining on the Thai-Myanmar
border. DP is an effective alternative treatment.
Clinical Trials Registration. ISRCTN87827353.
Chloroquine (CQ) remains the drug of choice for
the prevention and treatment of infections caused by
Plasmodium vivax in most endemic regions, although
the decline in the efficacy of CQ may have been over-
looked [1, 2]. CQ-resistant P. vivaxwas first described
in 1989 in Papua New Guinea [3]. For several years,
reports of reduced CQ efficacy were limited to the
island of New Guinea [46]. The degree of CQ re-
sistance in Papua, Indonesia and Papua New Guineahas now become so severe that local antimalarial
treatment policies have been revised to adopt arte-
misinin combination therapy for both Plasmodium
falciparum and P. vivax infections. More recently,
CQ-resistant P. vivax has been documented across
the Indonesian archipelago [1] and in Myanmar [7, 8],
South Korea [9], Turkey [10], the Horn of Africa [11],
and South America [12].
Received 22 April 2011; accepted 16 August 2011.
Correspondence: Francxois Nosten, MD, Shoklo Malaria Research Unit, Mahidol
Oxford University Tropical Medicine Research Unit, 68/30 Baan Tung Rd, PO Box
46, Mae Sod, Tak Province 63110, Thailand ([email protected]).
Clinical Infectious Diseases 2011;53(10):977984
The Author 2011. Published by Oxford University Press on behalf of the Infectious
Diseases Society of America. All rights reserved. For Permissions, please email:
This is an Open Access article distributed under the terms of the Creative Commons
Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/
2.5/), which permits unrestricted non-commercial use, distribution, and reproduction
in any medium, provided the original work is properly cited.
1058-4838/2011/5310-0002$14.00
DOI: 10.1093/cid/cir631
Treatment of Plasmodium vivaxWith Dihydroartemisinin-Piperaquine d CID 2011:53 (15 November) d 977
-
7/28/2019 Clin Infect Dis. 2011 Phyo 977 84
2/8
In Thailand, malaria remains a problem along the borders
with Cambodia and Myanmar, where multidrug-resistant
P. falciparum is endemic. In 1996, in camps for displaced per-
sons of the Karen ethnic minority on the Northwestern border
of Thailand, we found that CQ was a highly effective treatment
for P. vivax malaria, with ,3% of patients having a recurrence
(relapse, reinfection or recrudescence) by day 28 [13]. However,
in a study conducted 7 years later in neighboring Myanmar,
almost 35% of treated patients had a parasite recurrence by day28, raising the possibility that resistance was spreading along the
Thai-Myanmar border [7]. In addition, in vitro sensitivity
testing on fresh parasite isolates collected between 2003 and
2007 in the same region indicated a decreased susceptibility to
CQ in some isolates [14]. Patients with CQ-resistant P. vivaxcan
be treated effectively with the dihydroartemisinin-piperaquine
combination (DP) as well as other artemisinin combination
therapies [2, 5, 15]. To reassess the efficacy of CQ in the treatment
of P. vivax infections on the Northwestern border of Thailand
and study the efficacy of DP, we conducted a randomized
controlled trial in patients with P. vivax monoinfections.
METHODS
Patients
The study took place in the Shoklo Malaria Research Unit clinics
on the Thailand-Myanmar border, an area of low (entomologic
inoculation rate, ,1) and seasonal malaria transmission[16].
Patients .1 year old and with a body weight of$5 kg were
eligible for enrollment if they had a microscopically confirmed
monoinfection of P. vivax (parasitemia, $5/500 white blood
cells), if they were febrile (axillary temperature,$37.5C) or hada history of fever, and if they or their guardians gave fully in-
formed consent. Patients were excluded if they had a known
hypersensitivity to the study drugs; had intercurrent illness or
were pregnant, lactating, or severely anemic (hematocrit,
,20%); or had received mefloquine treatment in the previous
60 days or DP in the previous 3 months.
Randomization
Patients were allocated to the treatment arms based on a pre-
generated randomization list in blocks of 20. The individual
allocations were concealed in sealed envelopes and opened onlyafter enrollment by the field team. Although patients and clinic
workers were not blinded to the treatment arm after allocation,
laboratory technicians were unaware of treatment allocation.
Drugs
Chloroquine (Government Pharmaceutical Organization,
Thailand) was given once a day for 3 days, with a target dose of
25 mg base/kg with a glass of water. DP (Duocotexin; Holley
Peoples Republic of China) was administered once a day for
3 days with milk, with a total target dose of 7 mg/kg for dihy-
droartemisinin and 55 mg/kg for piperaquine. All patients with
a normal G6PD test result were offered a course of 14 days of
primaquine (0.5 mg base/kg/d) at the end of the follow-up
period. This delay was instituted because primaquine itself is
active against asexual stages of P. vivax [17] and its adminis-
tration earlier would have compromised the analysis of the
efficacy of CQ and DP.
Enrollment Procedures
A case-record form was completed for all patients documenting
symptoms before clinic attendance, concomitant illness, drug
history and physical examination. Capillary blood was collected
formalaria thick andthin films, hematocrit, and G6PD deficiency
testing. Patients .1 year of age presenting with parasitemia of
.100 P. vivaxtrophozoites/500 white blood cells were asked to
provide 5 mL of venous blood for in vitro sensitivity testing.
Follow-up
Patients were seen daily from admission until they were afebrile
and aparasitemic and then weekly until day 63. At each visit,
temperature was measured and a symptom questionnaire was
completed. Capillary blood was taken for malaria blood smear
and hematocrit weekly. Any concomitant medication taken
during the study period was recorded. Patients presenting to the
clinic within the follow-up period with microscopically con-
firmed P. vivax had capillary blood sampling for measurement
of CQ and desethylchloroquine plasma concentrations. Patients
with P. falciparum infection diagnosed during the follow-up
period were withdrawn from the study and treated with the
standard 3-day treatment of mefloquine and artesunate.
Drug Measurements
CQ and desethylchloroquine plasma concentrations were mea-
sured in patients .10 years old at the time of recurrent malaria.
Plasma drug concentrations were quantified using solid-phase
extraction and high-performance liquid chromatography with UV
detection [18]. The limit of detection was 1 ng/mL for both drugs.
Laboratory Methods
Malaria blood films were stained with Giemsa, and parasite
counts were expressed as the number of parasites per 1000 red
blood cells or, if the parasitemia was ,1% packed red blood
cells, as the number of parasites per 500 white blood cells. G6PDdeficiency was assessed by the fluorescent spot test SQMMR500
(R&D Diagnostic). In vitro samples for drug susceptibility were
processed and analyzed as described elsewhere [14].
Study End Points
The analysis of efficacy was conducted using a modified
intention-to-treat analysis that included all patients who fulfilled
the enrollment criteria. The primary end point was the overall
risk of recurrence with P. vivax during the 63-day follow-up
978 d CID 2011:53 (15 November) d Phyo et al
-
7/28/2019 Clin Infect Dis. 2011 Phyo 977 84
3/8
period. Secondary end points included the risk of reappearance
ofP. falciparum, the parasite and fever clearance times, and the
adverse events reported by the patients.
Sample Size
The original sample size of 500 patients had 80% power and
95% confidence to detect a 15% difference in the primary end
point, assuming a 50% recurrence rate in the CQ group,
allowing for up to 15% loss to follow-up by day 63.
Statistical Analysis
Data were double entered into Microsoft Access software and
analysis was performed using SPSS for Windows (version 16;
SPSS). The MannWhitney U test was used for nonparametric
comparisons, and Student ttest or 1-way analysis of variance for
parametric comparisons. Proportions were examined using v2
with Yates correction or by Fishers exact test. Efficacy end
points were assessed by survival analysis, in which the cumulative
risk of failure was calculated by the KaplanMeier product limit
formula and compared by the MantelHaenszel log-rank test. In
addition, treatments were compared and the hazard ratio (HR)
calculated using a Cox proportional hazards model. Data were
censored for patients who were unavailable for follow-up or, in
the case of secondary end points, presented again with a different
outcome and not regarded as treatment failures. Those patients
with recurrent vomiting or adverse drug effects, which required
early termination of treatment and the administration of rescue
therapy, were regarded as therapeutic failures.
Ethical Approval
The study was approved by the Ethics Committee of the Faculty
of Tropical Medicine, Mahidol University (MUTM 2006-029),
and the Oxford Tropical Research Ethics Committee, Oxford
University (OXTREC 027-05). The trial was registered at
ClinicalTrials.gov (ISRCTN87827353).
RESULTS
Recruitment and Baseline Characteristics
Between January 2007 and December 2008, 500 patients were
enrolled in the study. Eight of these patients did not meet the
inclusion criteria and were excluded from further analysis
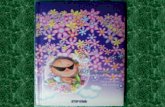
(Figure 1). The baseline characteristics of the 492 patients in the
evaluable population (modified intention-to-treat analysis) are
presented in Table 1; there were no differences in baseline
characteristics between treatment arms. Follow-up to day 63 or
day of failure (per-protocol analysis) was achieved in 86.7% of
Figure 1. Study profile.
Treatment of Plasmodium vivaxWith Dihydroartemisinin-Piperaquine d CID 2011:53 (15 November) d 979
-
7/28/2019 Clin Infect Dis. 2011 Phyo 977 84
4/8
patients (215/248) treated with DP and 87.3% (213/244) given
CQ (P5 .95). Nonadherence to follow-up was more likely in
adults (16%; 47/291) than in children (8.5%; 17/201; P5 .01),
but these patients otherwise had similar baseline characteristics
as those who were adherent to follow-up. With the exception of
a 3-year old boy who vomited CQ repeatedly, there were no
other early treatment failures. In patients receiving a complete
course of treatment, the median dose of CQ administered in the
CQ arm was 24.8 mg base/kg (range, 21.329.4), and patients in
the DP arm received median doses of 6.7 mg/kg (range, 510)
of dihydroartemisinin and 53.3 mg/kg (range, 4080) of
piperaquine.
Early Therapeutic Response
Within 24 hours after the start of treatment, 63.7% of patients
(156/245) receiving DP had clearance of asexual parasitemia
after, compared with only 21.1% (51/242) receiving CQ (odds
ratio, 6.6; 95% confidence interval [CI], 4.310.0; P, .001).
After 48 hours, these proportions had risen to 97.5% (237/243)
and 84.1% (201/239), respectively (P , .001). Five patients
treated with CQ were still parasitemic at 72 hours, and all but
1 had cleared by 96 hours. In the CQ but not in the DP group,
patients with schizont stages present at enrollment were more
likely to be parasitemic at 24 hours than were patients with
only trophozoite asexual stages present (93% [69/74] vs 72.6%
[122/168], respectively; odds ratio, 5.2; 95% CI, 1.915.7;
Table 1. Patient Characteristics at Baselinea
Characteristic DP treatment (n 5 248) CQ treatment (n 5 244)
Asexual parasitemia, geometric mean (95% CI), lL21 3776 (31114582) 4406 (36375339)
Gametocytemia, geometric mean (95% CI), lL21 214 (178257) 280 (236333)
Gametocytemia present 85 (210) 84 (205)
Schizonts present at enrollment 32 (79) 30 (74)
Male sex 70 (173) 64 (155)
G6PD deficiency 6.1 (15/247) 5.3 (13)
Weight, median (range), kg 45 (774) 45 (961)
Age, median (range), years 18 (157) 18 (163)
Age, years
,5 14 (34) 12 (30)
514 27 (67) 29 (70)
.14 59 (147) 59 (144)
Fever .38.0C 42 (94/225) 42 (97/229)
Duration of febrile illness, median (range), days 2 (08) 2 (05)
Hematocrit, mean (SD), % 37.2 (5.0) 37.6 (5.2)
Anemia (hematocrit ,30%) 4.5 (11/247) 5.8 (14/242)
Splenomegaly 14 (34/243) 12 (29/237)
Hepatomegaly 23 (57/247) 26 (63)
Abbreviations: CI, confidence interval; CQ, chloroquine; DP, dihydroartemisinin-piperaquine; SD, standard deviation.a
Unless otherwise indicated, data represent % (No.) of patients, with denominators where these were smaller than the full sample.
Table 2. Risk of Treatment Failure: Modified Intention-to-Treat Analysis
Cumulative risk of recurrencea (95% CI), %
Type of recurrence DP treatment (n 5 248) CQ treatment (n 5 244) Hazard ratiob (95% CI)
Plasmodium vivax
Day 63c 54.9 (48.261.6) 79.1 (73.484.8) 2.27 (1.82.9) (P, .001)
Day 28d 4.1 (1.66.6) 9.8 (5.913.7) 2.3 (1.14.9) (P5 .032)
Plasmodium falciparum
Day 63d 8.0 (4.511.5) 11.5 (6.616.4) 1.5 (0.82.9) (P5 .176)
Day 28d 2.4 (0.44.4) 7.8 (4.311.3) 3.1 (1.27.9) (P5. 015)
Abbreviations: CI, confidence interval; CQ, chloroquine; DP, dihydroartemisinin-piperaquine.a
Cumulative risk calculated by Kaplan-Meier method. Patients with an incomplete course of treatment were included in the analysis conservatively as treatment
failures; other patients with incomplete follow-up were censored on the last day of follow-up as nonfailures.b
Hazard ratios were calculated using a Cox proportional hazards model.c
Primary end point.d
Secondary end point.
980 d CID 2011:53 (15 November) d Phyo et al
-
7/28/2019 Clin Infect Dis. 2011 Phyo 977 84
5/8
P5 .0005). Overall 84.3% of patients (415/492) had P. vivax
gametocytemia evident on their admission blood film. By
48 hours, this proportion had fallen to 7.6% (18/238) in the CQ
group and 1.3% (3/239) in the DP group (P5 .001). Although
all patients had a history of fever (median duration, 2 days) on
admission to the study, only 42.1% (191/454) were febrile at
enrollment. Fever clearance was significantly faster in patients
receiving DP; 92.9% (183/197) were afebrile by day 2 compared
with 82.2% (171/208) of those receiving CQ (P5 .001).
Efficacy Analysis
In the modified intention-to-treat analysis, the cumulative risk
of recurrence with P. vivax at 9 weeks was 79.1% (95% CI,
73.5%84.8%) in patients treated with CQ compared with
54.9% (95% CI, 48.2%61.6%) in those receiving DP (HR, 2.27;
95% CI, 1.82.9; P, .001) (Table 2). This significant difference
had already emerged by day 28 of follow-up and was confirmedat both day 28 and day 63 in the per-protocol population (Table 3
and Figure 2). By day 28, recurrent infections had emerged in
8.7% CQ recipients (18/207) compared with 2.2% (5/230)
treated with DP (relative risk, 4.0; 95% CI, 1.5110.58; P5 .005).
The median time to recurrence ofP. vivaxinfection was 56 days
(interquartile range [IQR], 4256; range, 1465) in the DP
group compared with 42 days (IQR, 3549; range 1966) in the
CQ group (P , .001). Falciparum malaria was also more
A
B
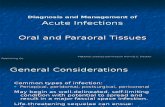
Figure 2. A, Cumulative risk of treatment failure in patients with Plasmodium vivax parasitemia (P. vivax alone or mixed infections). Diamondsrepresent chloroquine (CQ); circles, dihydroartemisinin-piperaquine (DP). The overall difference between treatment groups at day 63 was significant
(P, .001). B, Cumulative risk of treatment failure in patients with Plasmodium falciparumparasitemia (P. falciparuminfection alone or mixed infections).
The overall difference between treatment groups was significant at day 28 ( P5 .015) but not by day 63 (P5 .176).
Treatment of Plasmodium vivaxWith Dihydroartemisinin-Piperaquine d CID 2011:53 (15 November) d 981
-
7/28/2019 Clin Infect Dis. 2011 Phyo 977 84
6/8
common in the CQ group; by day 28, 1 patient in the DP group
and 15 in the CQ group were parasitemic with P. falciparum
(either alone or mixed with P. vivax) (HR, 3.1; 95% CI, 1.27.9;
P5 .015). These figures had increased to 13 and 21, respectively,
by day 63, although this difference was no longer significant in
the modified intention-to-treat analysis (Table 2). Recurrent
malaria within 28 days (both P. vivax and P. falciparum) was
therefore 6.11 (95% CI, 2.6114.29) times more frequent in CQ
recipients than in DP recipients.
Cox regression analysis (modified intention-to-treat pop-
ulation) revealed 2 independent baseline factors predicting
recurrent P. vivaxinfection: treatment with CQ (adjusted HR
[AHR], 2.3; 95% CI, 1.82.9; P , .001) and young age
(14 years) (AHR, 1.58; 95% CI, 1.12.2; P5 .005 for com-
parison with older children and adults). In addition, patients
treated with CQ who had delayed parasite clearance (still
parasitemic on day 2), were at significantly greater risk
of recurrent P. vivax infection by day 28 (23.5%; 95% CI,
9.2%37.8%) compared with 6.5% (95% CI, 2.4%10.6%) in
patients whose initial parasitemia had cleared within 48 hours
(P5 .004). This difference remained significant after age andbaseline parasitemia were controlled for (AHR, 4.2; 95% CI,
1.611.1; P5 .004).
The minimum effective plasma concentration (MEC) of
combined CQ plus desethylchloroquine considered effective
against CQ-susceptible parasites is 12 ng/mL [1, 19]. Of 156
recurrences of P. vivax infection in the CQ group, plasma
concentrations of CQ and desethylchloroquine were de-
termined in 85 patients (54%). In the 5 patients with
recurrence before day 28, these plasma concentrations at the
time of failure were 4.59, 5.00, 5.00, 7.50, and 15.5 ng/mL. The
patient with a plasma CQ-desethylchloroquine concentration
of 15.5 ng/mL (higher than the MEC of 12 ng/mL) had
treatment failure at day 21.
Symptoms and Tolerability
Early vomiting within the first hour of drug administration was
recorded in 7.9% of patients treated with DP (19/241) and 7.1%
of those treated with CQ (17/241) (P5 .86). With the exception
of the 3-year-old boy in the CQ group, all patients tolerated drug
readministration (Figure 3). The only significant difference be-
tween the 2 treatment arms in the development of symptoms
was a 4.0-fold (95% CI, 1.511.3-fold) increased risk of vomiting
on days 1 and 2 associated with CQ; 10.5% of patients receiving
CQ (22/209) vomited, compared with 2.8% (6/211) of those
receiving DP (P5 .003). The risk of diarrhea was 0.2% in both
treatment arms assessed at day 7. No serious adverse event
occurred during the study.
Parasite In Vitro Drug SusceptibilityCQ susceptibility was assessed in 50 isolates before administra-
tion of antimalarial medication, of which 43 had a majority of
ring stages present. Drug susceptibility could be assessed suc-
cessfully in 86% of these isolates (37/43). The median inhibitory
concentration (IC50) for CQ was 27.4 ng/mL (IQR, 11.846.1l;
range, 3.4124.8) and 51.7 ng/mL (IQR, 45.369.3; range, 12.5
121.7) for piperaquine (Figure 4). In total, 13.5% of isolates
(5/37) had CQ IC50 values .50 ng/mL (100 nmol/L).
Figure 3. Adverse events on day 1 or 2 in patients without symptoms at admission.
982 d CID 2011:53 (15 November) d Phyo et al
-
7/28/2019 Clin Infect Dis. 2011 Phyo 977 84
7/8
DISCUSSION
An estimated 2849 million persons are at risk ofP. vivaxinfection
[20], with between 76 and 391 million clinical cases per year. The
efficacy of CQ, the drug used to treat vivax malaria for.50 years,
has fallen in some areas, and resistance seems to be spreading. The
assessment of treatment efficacy in P. vivaxis more difficult than
in P. falciparum, because there are no genotyping methods that
reliably distinguish relapses from new infections, and long-term
cultures of P. vivax cannot be maintained, thereby confining in
vitro testing of drugs to assays on fresh isolates. This means that it
is difficult to document unequivocal cases of treatment failure in
areas where resistance is emerging, but anyP. vivaxinfection that
occurs within 28 days after the start of CQ treatment, whether
recrudescence, relapse, or new infection, has grown through re-
sidual CQ concentrations in blood. If these concentrations are
adequate, then the infection is resistant, by definition [21].
In this study we assessed the in vivo efficacy of CQ and
compared it with that of DP, an artemisinin combination
therapy with documented efficacy against CQ-resistant P. vivax
[5, 22, 23]. More than 8% of patients treated with CQ had
a recurrent infection within 28 days, and this rate rose to 22% in
young children. Parasite and fever clearance times were both
significantly faster after DP treatment. The artemisinin de-
rivatives are the most rapidly acting drugs against P. vivax[17],
so this difference is expected. The artemisinin component of DP
contributes significantly to the initial therapeutic response but
would not be expected to affect subsequent relapses or re-infections. Parasite clearance time was prolonged after CQ
treatment, with 16% of patients still parasitemic at 48 hours and
2% at 76 hours. Delayed parasite clearance, as defined by par-
asitemia on day 2, increased the subsequent risk of recurrent
P. vivax infection within 28 days by almost 4-fold after CQ
treatment. Interestingly, patients who had schizonts in the
peripheral blood on admission had significantly slower parasite
clearance after CQ treatment. This presumably reflects
uninterrupted schizogony and is consistent with in vitro ob-
servations showing marked reduction in activity of CQ against
these stages [24]. As expected, children who have less naturalimmunity against malaria were more at risk of parasite re-
currence independent of the above-mentioned risk factors.
During follow-up, the risk of recurrence ofP. vivaxinfection was
significantly greater after CQ than after DP treatment
(AHR, 2.3), a difference that was already apparent by day 28.
Recurrences can result from recrudescence, reinfection, or
relapses from dormant liver stages, although we were unable to
distinguish between these. Both CQ and DP have long elimi-
nation phases and therefore persistent blood concentrations,
delaying the time to the first relapse. In areas where CQ sensitive
parasites predominate, the prolonged posttreatment prophylaxis
of CQ usually affords a minimum of 28 days without recurrence.
In the current study the main difference in the parasitologic
response between CQ and DP was evident within this period,
with nearly 9% of patients treated with CQ having a recurrence
by day 28. This figure is 3 times higher than in our previous
study in 1996, but one-third of that reported from neighboring
Myanmar [7]. In addition, in 1 of these early recurrences
Figure 4. Ex vivo drug susceptibility to chloroquine and piperaquine.IC50, median inhibitory concentration.
Table 3. Risk of Treatment Failure: Per-Protocol Analysis
Patients with recurrence, % (no.)
Recurrence DP treatment CQ treatment Odds ratio (95% CI)Plasmodium vivax
Day 63a 55.1 (113/205) 80.3 (155/193) 3.3 (2.15.3) (P, .001)
Day 28a 2.2 (5/230) 8.7 (18/207) 4.3 (1.513.5) (P5 .005)
Plasmodium falciparum
Day 63b 10.1 (13/129) 29.6 (21/71) 3.8 (1.68.7) (P, .001)
Day 28b 0.4 (1/228) 7.0 (15/215) 17.0 (2.3349) (P, .001)
Abbreviations: CI, confidence interval; CQ, chloroquine; DP, dihydroartemisinin-piperaquine.a
Excludes all patients with protocol violations or incomplete follow-up due to P. falciparum parasitemia before day 61 (for day 63 risk) or 26 (for day 28 risk).b
Excludes all patients with protocol violations or incomplete follow-up due to recurrent P. vivax parasitemia before day 61 (for day 63 risk) or 26 (for day 28 risk).
Treatment of Plasmodium vivaxWith Dihydroartemisinin-Piperaquine d CID 2011:53 (15 November) d 983
-
7/28/2019 Clin Infect Dis. 2011 Phyo 977 84
8/8
(day 21) the combined CQ plus desethylchloroquine plasma
concentration (15.5 ng/mL) was higher than the MEC of 12 ng/
mL, demonstrating recurrence through drug levels that would
be expected to inhibit CQ-sensitive parasites [1, 19]. In the latest
published study in the same area, primaquine was administered
with CQ, which may have masked the emergence of recurrences
by day 28 [25]. In the present study, the confounding effect of
primaquine asexual stage activity was avoided by adminis-
tering the drug at the end of the follow-up period, to focussolely on evaluating the main schizontocidal drugs. Associated
in vitro results highlight the fact that whereas the IC50 values
for CQ were generally low (median, 27.4 ng/mL), some iso-
lates exhibited relatively high values. Drug susceptibility
testing was performed only in a small proportion of patients,
and hence our study was underpowered to assess the in vivo
ex vivo correlates. However, in the parasites that could be
tested, 13% of isolates had reduced susceptibility to CQ
(IC50 .100 nmol/L), in keeping with the overall 9% risk of
recurrence within 28 days.
In conclusion our results suggest that CQ efficacy on theNorthwestern border of Thailand is declining. DP is a suitable
alternative in the treatment of P. vivax infections in this area,
although further studies are needed to define how best to combine
this treatment with appropriate antirelapse therapy (primaquine).
Notes
Acknowledgments. We thank all the patients and staff at all the Shoklo
Malaria Research Unit (SMRU) clinics who participated in this study.
Financial support. Holley Pharm provided financial support for the
study and donated the dihydroartemisinin-piperaquine but had no role in
the planning, design, and conduct of the study, nor in the analysis and
interpretation of results or writing of the manuscript. The SMRU is attached tothe Faculty of Tropical Medicine, Mahidol University. This investigation was
part of the Wellcome Trust Mahidol University Oxford Tropical Medicine
Research Programme, supported by the Wellcome Trust of Great Britain.
Potential conflicts of interest. All authors: No reported conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to the
content of the manuscript have been disclosed.
Author contributions. A. P. P., K. M. L., E. A., and F. N. conducted the
trial; R. P. analyzed the data; B. R. and K. S., performed the in vitro tests;
N. L. measured the drug concentrations; P. S., E. A., N. J. W., and F. N.
conceived the protocol and supervised the study; all authors contributed to
the interpretation of data and writing of the manuscript.
References
1. Baird JK. Chloroquine resistance in Plasmodium vivax. Antimicrob
Agents Chemother 2004; 48:407583.
2. Douglas NM, Anstey NM, Angus BJ, Nosten F, Price RN. Artemisinin
combination therapy for vivax malaria. Lancet Infect Dis 2010; 10:40516.
3. Rieckmann KH, Davis DR, Hutton DC. Plasmodium vivaxresistance to
chloroquine? Lancet 1989; 2:11834.
4. Baird JK, Basri H, Purnomo , et al. Resistance to chloroquine by
Plasmodium vivaxin Irian Jaya, Indonesia. Am J Trop Med Hyg 1991;
44:54752.
5. Ratcliff A, Siswantoro H, Kenangalem E, et al. Two fixed-dose arte-
misinin combinations for drug-resistant falciparum and vivax malaria
in Papua, Indonesia: an open-label randomised comparison. Lancet
2007; 369:75765.
6. SumawinataIW, Bernadeta , Leksana B, et al. Very high risk of therapeutic
failure with chloroquine for uncomplicated Plasmodium falciparum and
P. vivax malaria in Indonesian Papua. Am J Trop Med Hyg 2003; 68:
41620.
7. Guthmann JP, Pittet A, Lesage A, et al. Plasmodium vivaxresistance to
chloroquine in Dawei, southern Myanmar. Trop Med Int Health 2008;
13:918.
8. Marlar T, Myat Phone K, Aye Yu S, Khaing Khaing G, Ma S, Myint O.
Development of resistance to chloroquine by Plasmodium vivax in
Myanmar. Trans R Soc Trop Med Hyg 1995; 89:3078.
9. Lee KS, Kim TH, Kim ES, et al. Short report: chloroquine-resistant
Plasmodium vivaxin the Republic of Korea. Am J Trop Med Hyg 2009;
80:2157.
10. Kurcer MA, Simsek Z, Zeyrek FY, et al. Efficacy of chloroquine in the
treatment of Plasmodium vivax malaria in Turkey. Ann Trop Med
Parasitol 2004; 98:44751.
11. Teka H, Petros B, Yamuah L, et al. Chloroquine-resistant Plasmodium
vivaxmalaria in Debre Zeit, Ethiopia. Malar J 2008; 7:220.
12. de Santana Filho FS, Arcanjo AR, Chehuan YM, et al. Chloroquine-
resistant Plasmodium vivax, Brazilian Amazon. Emerg Infect Dis 2007;
13:11256.
13. Luxemburger C, van Vugt M, Jonathan S, et al. Treatment of vivaxmalaria on the western border of Thailand. Trans R Soc Trop Med Hyg
1999; 93:4338.
14. Suwanarusk R, Russell B, Chavchich M, et al. Chloroquine resistant
Plasmodium vivax: in vitro characterisation and association with mo-
lecular polymorphisms. PLoS One 2007; 2:e1089.
15. Karunajeewa HA, Mueller I, Senn M, et al. A trial of combination
antimalarial therapies in children from Papua New Guinea. N Engl J
Med 2008; 359:25457.
16. Luxemburger C, Thwai KL, White NJ, et al. The epidemiology of
malaria in a Karen population on the western border of Thailand.
Trans R Soc Trop Med Hyg 1996; 90:10511.
17. Pukrittayakamee S, Chantra A, Simpson JA, et al. Therapeutic re-
sponses to different antimalarial drugs in vivax malaria. Antimicrob
Agents Chemother 2000; 44:16805.
18. Blessborn D, Neamin G, Bergqvist Y, Lindegardh N. A new approach toevaluate stability of amodiaquine and its metabolite in blood and
plasma. J Pharm Biomed Anal 2006; 41:20712.
19. Berliner RW, Earle DP, Taggart JV, et al. Studies on the chemotherapy
of the human malarias. Vi. The physiological disposition, antimalarial
activity, and toxicity of several derivatives of 4-aminoquinoline. J Clin
Invest 1948; 27:98107.
20. Guerra CA, Howes RE, Patil AP, et al. The international limits and
population at risk of Plasmodium vivax transmission in 2009. PLoS
Negl Trop Dis 2010; 4:e774.
21. White NJ. The assessment of antimalarial drug efficacy. Trends Para-
sitol 2002; 18:45864.
22. Hasugian AR, Purba HL, Kenangalem E, et al. Dihydroartemisinin-
piperaquine versus artesunate-amodiaquine: superior efficacy and
posttreatment prophylaxis against multidrug-resistant Plasmodium
falciparum and Plasmodium vivax malaria. Clin Infect Dis 2007; 44:106774.
23. Karunajeewa H, Lim C, Hung TY, et al. Safety evaluation of fixed com-
bination piperaquine plus dihydroartemisinin (Artekin) in Cambodian
children and adults with malaria. Br J Clin Pharmacol 2004; 57:939.
24. Sharrock WW, Suwanarusk R, Lek-Uthai U, et al. Plasmodium vivax
trophozoites insensitive to chloroquine. Malar J 2008; 7:94.
25. Muhamad P, Ruengweerayut R, Chacharoenkul W, Rungsihirunrat K,
Na-Bangchang K. Monitoring of clinical efficacy and in vitro sensitivity
of Plasmodium vivax to chloroquine in area along Thai Myanmar
border during 20092010. Malar J 2011; 10:44.
984 d CID 2011:53 (15 November) d Phyo et al