Classification of Hand Eczema Clinical and Aetiological Types
10
Contact Dermatitis • Original Article COD Contact Dermatitis Classification of hand eczema: clinical and aetiological types. Based on the guideline of the Danish Contact Dermatitis Group Jeanne Duus Johansen 1 , Marianne Hald 1 , Bo Lasthein Andersen 2 , Grete Laurberg 3 , Anne Danielsen 4 , Christian Avnstorp 5 , Berit Kristensen 6 , Ove Kristensen 6 , Knud Kaaber 7 , Jens Thormann 8 , Torkil Menn ´ e 9 and Niels Veien 3 1 Department of Dermato-Allergology, National Allergy Research Centre, Copenhagen University Gentofte Hospital, 2900 Hellerup, Denmark, 2 Dermatology Clinic, Havnepladsen 3A, 5700 Svendborg, Denmark, 3 Dermatology Clinic, Vesterbro 99, 9000 Aalborg, Denmark, 4 Dermatology Clinic, Baneg ˚ ardspladsen 1, 1570 Copenhagen V, Denmark, 5 Dermatology Clinic, Roskildevej 264, 2610 Rødovre, Denmark, 6 Dermatology Clinic, Bredgade 50, 4400 Kalundborg, Denmark, 7 Dermatology Clinic, Bredgade 30, 7400 Herning, Denmark, 8 Dermatology Clinic, Skovgade 23 C, 7100 Vejle, Denmark, and 9 Department of Dermato-Allergology, Copenhagen University Gentofte Hospital, 2900 Denmark doi:10.1111/j.1600-0536.2011.01911.x Summary Background. No generally accepted classification scheme for hand eczema exists. The Danish Contact Dermatitis Group recently developed a guideline defining common clinical types and providing criteria for aetiological types. Objectives. To test the concepts of this guideline in a group of hand eczema patients. Methods. Seven hundred and ten hand eczema patients were included from seven dermatology clinics in Denmark. The hand eczema was classified into one of five clinical types, with standard photographs as reference. The severity was scored by the physician, who also made a final aetiological diagnosis. Results. Irritant contact dermatitis was most frequent in chronic, dry fissured hand eczema (44.3%), pulpitis (41.7%), and nummular hand eczema (40.9%), whereas allergic contact dermatitis dominated in vesicular types of hand eczema, with recurrent (35%) and few (24.2%) eruptions. Hyperkeratotic palmar hand eczema was the only clinical type that constituted a distinct subgroup; it was found most frequently in older men and had the strongest relationship, although not significant, with non-specific dermatitis. Conclusions. The relationship between clinical type of hand eczema and aetiological diagnosis fitted with general experience, but no simple relationship was found. This emphasizes that patch testing and exposure analysis are mandatory. Hyperkeratotic palmar hand eczema was identified as a distinct clinical subtype. Key words: disease classification; hand eczema severity index; non-specific dermatitis; quality of life. The Danish Contact Dermatitis Group (DCDG) recently published its guideline for classification of hand eczema (1). In parallel, the group has conducted a Correspondence: Jeanne Duus Johansen, Department of Dermato- Allergology, National Allergy Research Centre, Copenhagen University Gentofte Hospital, Niels Andersens vej 65, 2900 Hellerup, Denmark. Tel: +45 39777301; Fax: +45 39777118. E-mail: [email protected] Conflicts of interest: No conflicts of interests to be declared. Accepted for publication 19 February 2011 prospective study of clinical and aetiological types of hand eczema, risk factors, and other characteristics of hand eczema patients, based on the concept of this guideline. Attempts have previously been made to characterize hand eczema in clinical types, for example by Cronin (2) and Wilkinson (3). The development and course of hand eczema is a dynamic process, and is closely linked to the environment. This means that the clinical expression of a disease may depend on changes in living conditions, the time period and the nature of exposure, and interactions with genes. © 2011 John Wiley & Sons A/S • Contact Dermatitis, 65, 13–21 13
-
Upload
apiffaulia -
Category
Documents
-
view
218 -
download
0
description
zxv
Transcript of Classification of Hand Eczema Clinical and Aetiological Types
-
Contact Dermatitis Original Article CODContact Dermatitis
Classification of hand eczema: clinical and aetiological types. Basedon the guideline of the Danish Contact Dermatitis Group
Jeanne Duus Johansen1, Marianne Hald1, Bo Lasthein Andersen2, Grete Laurberg3,Anne Danielsen4, Christian Avnstorp5, Berit Kristensen6, Ove Kristensen6, Knud Kaaber7,Jens Thormann8, Torkil Menne9 and Niels Veien31Department of Dermato-Allergology, National Allergy Research Centre, Copenhagen University Gentofte Hospital, 2900 Hellerup, Denmark, 2DermatologyClinic, Havnepladsen 3A, 5700 Svendborg, Denmark, 3Dermatology Clinic, Vesterbro 99, 9000 Aalborg, Denmark, 4Dermatology Clinic, Banegardspladsen 1,1570 Copenhagen V, Denmark, 5Dermatology Clinic, Roskildevej 264, 2610 Rdovre, Denmark, 6Dermatology Clinic, Bredgade 50, 4400 Kalundborg,Denmark, 7Dermatology Clinic, Bredgade 30, 7400 Herning, Denmark, 8Dermatology Clinic, Skovgade 23 C, 7100 Vejle, Denmark, and 9Department ofDermato-Allergology, Copenhagen University Gentofte Hospital, 2900 Denmark
doi:10.1111/j.1600-0536.2011.01911.x
Summary Background. No generally accepted classification scheme for hand eczema exists.The Danish Contact Dermatitis Group recently developed a guideline defining commonclinical types and providing criteria for aetiological types.Objectives. To test the concepts of this guideline in a group of hand eczema patients.Methods. Seven hundred and ten hand eczema patients were included from sevendermatology clinics in Denmark. The hand eczema was classified into one of five clinicaltypes, with standard photographs as reference. The severity was scored by the physician,who also made a final aetiological diagnosis.Results. Irritant contact dermatitis was most frequent in chronic, dry fissured handeczema (44.3%), pulpitis (41.7%), andnummularhandeczema (40.9%),whereasallergiccontact dermatitis dominated in vesicular types of hand eczema, with recurrent (35%)and few (24.2%) eruptions. Hyperkeratotic palmar hand eczema was the only clinicaltype that constituted a distinct subgroup; it was found most frequently in older men andhad the strongest relationship, although not significant, with non-specific dermatitis.Conclusions. The relationship between clinical type of hand eczema and aetiologicaldiagnosis fitted with general experience, but no simple relationship was found. Thisemphasizes that patch testing and exposure analysis are mandatory. Hyperkeratoticpalmar hand eczema was identified as a distinct clinical subtype.
Key words: disease classification; hand eczema severity index; non-specific dermatitis;quality of life.
The Danish Contact Dermatitis Group (DCDG) recentlypublished its guideline for classification of handeczema (1). In parallel, the group has conducted a
Correspondence: Jeanne Duus Johansen, Department of Dermato-Allergology, National Allergy Research Centre, Copenhagen UniversityGentofte Hospital, Niels Andersens vej 65, 2900 Hellerup, Denmark. Tel:+45 39777301; Fax: +45 39777118. E-mail: [email protected]
Conflicts of interest: No conflicts of interests to be declared.
Accepted for publication 19 February 2011
prospective study of clinical and aetiological types of handeczema, risk factors, and other characteristics of handeczema patients, based on the concept of this guideline.
Attempts have previously been made to characterizehand eczema in clinical types, for example by Cronin (2)and Wilkinson (3). The development and course of handeczema is a dynamic process, and is closely linked to theenvironment. This means that the clinical expression of adisease may depend on changes in living conditions, thetime period and the nature of exposure, and interactionswith genes.
2011 John Wiley & Sons A/S Contact Dermatitis, 65, 1321 13
-
CLASSIFICATION OF HAND ECZEMA DUUS JOHANSEN ET AL.
Even though the clinical descriptions are still in focus,disease classification for hand eczema has moved frommorphology to aetiology, as for many other diseases (4).Anaetiological diagnosis offers the advantage of targetingpreventionand, insomecases,alsoprovidingmorespecifictreatment.
In the current study, consecutivehandeczemapatientswere studied to give an update of clearly defined clinicaltypes and their relationshipswith aetiology. In particular,an attempt was made to characterize patients who endupwith the diagnosis of non-specific dermatitis, a sort ofnomans land, where no targeted prevention is possible.
Materials and Methods
The study was designed as a cross-sectional multicentrestudy performed fromNovember 2008 to February 2010by dermatologists from seven private practices thatare members of the DCDG. Consecutive patients withhand eczema, referred to one of the seven participatingclinics with 17 dermatologists across Denmark, wereincluded prospectively. The medical history of thepatient was recorded by the treating physician withregard to the MOAHLFA index, which includes sex,occupational relationship, history of atopic dermatitis,hand eczema, stasis eczema/ulcer, facial eczema, and ageabove 40 years.
The clinical examination of the hands at the timeof patch testing included a severity score obtained bythe physician with the Hand Eczema Severity Index(HECSI) (5) and an evaluation of the clinical type ofhand eczema. This was based on photographs anddescriptions as in the guideline of the DCDG for handeczema classification (1) in a slightly modified version, asinterdigital eczema was not included in the preliminaryversions of the guideline at the time when this study wasinitiated.Thosepatientswhocouldnotbeclassifiedwithinone of these categories were termed non-classifiable.
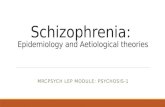
Thus, the clinical types consisted of five defined typesof hand eczema: vesicular hand eczema, chronic dryfissured hand eczema, palmar hyperkeratotic handeczema, nummular hand eczema, and pulpitis. Palmarhyperkeratotic hand eczema is shown in Fig. 1, as anexample; the other photographs can be seen in theguideline (1). In addition, the dynamics of the handeczemawererecordedaseither rareeruptions, recurrenteruptions, or constant activity. As vesicular handeczema, in particular, is known for its dynamic activity,which also may indicate different subtypes (6, 7), theresults for vesicular hand eczema with rare eruptionsand with recurrent eruptions are given separately in thefollowing.
Fig. 1. Palmar hyperkeratotic hand eczema characterized byhyperkeratotic changes in the palms, possibly extending to thevolar side of the fingers. There may be fissures, but there are novesicles at any time.
All patients were patch tested as a minimum with theEuropean baseline series of contact allergens and, whenrequired, with additional substances. Finally, the treatingphysician recorded the aetiological diagnosis as allergiccontact dermatitis, irritant contact dermatitis atopicdermatitis, non-specific dermatitis, or combinations ofthese, according to the disease classification codes (WorldHealthOrganization, ICD-10)DL23x,DL24x,DL209,andDL309.
Patients filled in a questionnaire at inclusion regardingduration of hand eczema, hand eczema in childhood,triggers of eczema, current occupation, use of gloves atwork, type of gloves used, hand washing, occupationalrelationship, and sick leave. On the basis of thequestionnaire, avariablewas constructed forwetwork forthosewhohad repeated handwashings (20 times/day),or wet hands or use of occlusive gloves for at least 2 hrduring the working day.
In addition, the patients answered questions aboutquality of life using the Dermatology Life Quality Index(DLQI) (8). The DLQI score was calculated as the sum ofscores of each question, with a maximum score of 30 anda minimum score of 0. The higher the score, the greaterthe impairment of quality of life (QoL).
Patients also rated the severity of their hand eczemacurrently and during the past year by use of avisual analogue scale (VAS) from 0 (no eczema) to10 (very severe eczema) and a photographic guideshowing photographs of different severity (9) Patientswere followed for a year with questionnaires and anadditional clinical examination. This article concerns theresults at the time of inclusion of the patients. The HESCIwas performed and the questionnaires filled in at the firstconsultation and/or at the time of patch testing.
14 2011 John Wiley & Sons A/S Contact Dermatitis, 65, 1321
-
CLASSIFICATION OF HAND ECZEMA DUUS JOHANSEN ET AL.
Statistics
Data are presented as proportions in percentages for cate-gorical variables and as median values and interquartilerange for continuous variables. The 2-test was usedfor comparison between groups. The MannWhitneyU -test and KruskalWallis test were used for comparisonof continuous measurements.
A logistic regression analysis was performed, with thediagnosis of non-specific hand eczema (DL309) as thedependent variable versus the remaining types, and withthe clinical types as explanatory variables. In a separatestep, the risk factors wet work (yes/no), occupationalrelationship (yes/no) and one or more positive patch testreactions were examined, and in a third step differentmeasures of severity were analysed as the explanatoryvariables: long duration (over 5 years, yes/no), severelyimpaired QoL ( 15), severe HECSI (>17), severe VAS atpresent (>4), severe VAS previously (>5), and constantactivity (yes/no). Associations were expressed as oddsratios (ORs) with 95% confidence intervals. The cut-point of the most severely affected patients was basedon the 25th percentile for each of the variables HECSIand VAS, and the choice of QoL 15 was based on therecommendations from the National Institute for Healthand Clinical Excellence in the UK and their guideline fortreatment of severe chronichandeczemawithalitretinoin(http://www.nice.org.uk).
Data analyses were performed with SPSS (SPSS,Chicago, IL, USA) for Windows (release 18.0).
Results
A total of 710 hand eczema patients were included, 463women and 247 men (ratio 1.87). The seven clinicseach contributed 30174 patients. The median agewas 39 years (range 1883 years), with women beingstatistically significantly younger than men (Table 1).A personal history of atopic dermatitis was present in21.7%, with no difference between sexes. A duration ofhand eczema of >5 years was seen in 28.1%. The QoL(DLQI) was more affected in women than in men, aswas the self-evaluated severity (on a VAS) in the past12 months, whereas the HECSI scored by the treatingdermatologist at inclusion showedno differences betweensexes (Table 2). In 44% of cases, the eczema was eithercaused or aggravated by the work, with no differencebetween sexes (Table 1).
In508cases, handeczemawas classified intooneof thefive defined clinical types, whereas in 49 (8.8%), the handeczema could not be classified in one of the clinical types(Table 2). This informationwasmissing for the remaining153 cases; in 35 of these, the hand eczema had cleared at
the timeof inclusion.Chronic, dryfissuredeczemawas themost frequent (36.1%), followedbyvesicular eczemawithrecurrent eruptions (31.8%), nummular eczema (7.9%),hyperkeratotic palmar eczema (7.4%), vesicular eczema(rare eruptions) (5.9%), and pulpitis (2.2%). Both pulpitisandhyperkeratotic palmarhandeczemawere statisticallysignificantly more frequent in men than in women; forthe remainder, there were no sex differences. A tendencywas found for patients with hyperkeratotic palmar handeczema or nummular or pulpitis to be older than patientswithout these clinical types, with median ages of 45, 47and 55 years, respectively, in comparison with 39 yearsfor the whole group (Table 3).
Regarding the dynamics, dry fissured hand eczema,hyperkeratotic palmar eczema and pulpitis showed atendency to have constant activity. Vesicular handeczema with rare eruptions was of a shorter durationthan the rest p = 0.04), had significantly lower HESCI(p < 0.001) and DLQI (p < 0.05) scores, and lowercurrent self-evaluated severity on the VAS (p < 0.001).
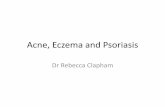
The distribution of HECSI and DLQI scores accordingto clinical type is presented in Figs. 2 and 3.
The relationship between aetiological diagnosis andthe different clinical types was analysed (Table 4). Norelationship between a history of atopic dermatitis orcurrent atopic hand eczema and any clinical type wasseen. Irritant contact dermatitis was most frequent inchronic, dry fissured hand eczema (44.3%), pulpitis(41.7%), and nummular hand eczema (40.9%), whereasallergic contact dermatitis dominated in vesicular typesof hand eczema, with recurrent (35%) and few (24.2%)eruptions. A diagnosis of non-specific dermatitis (DL309)was most frequent among patients with hyperkeratoticpalmar hand eczema (43.9%) and vesicular hand eczemawith few eruptions (33.3%) (Table 4).
The characteristics of patients with a diagnosis ofnon-specific dermatitis (DL309) were analysed by use ofmultivariate analysis. No significant relationshipwith sexwas found, and the group, in general, was younger thanother hand eczema patients (p = 0.02). No clinical typewassignificantly related tonon-specificdermatitis, but theOR for hyperkeratotic palmar eczema was the highest, at4.3 (0.822.4),p = 0.09. Severehandeczemameasuredwith theHECSI,DLQIandVASat two timepoints andwithlongdurationshowednosignificantoverrepresentation innon-specificdermatitis. The results fromthephotographicguide of severity gave the same result (data not shown).
Discussion
One major advance in this study was the use of cleardefinitions of the clinical types of hand eczema supported
2011 John Wiley & Sons A/S Contact Dermatitis, 65, 1321 15
-
CLASSIFICATION OF HAND ECZEMA DUUS JOHANSEN ET AL.
Table 1. Data collected in consecutive hand eczema patients in dermatology clinics in Denmark. Basic characteristics (MOAHLFA) andpatients own assessment
n/total (%) or median values (percentiles)
Men n = 247 Women n = 463Whole population
n = 710 p-value
Occupational relationshipa 88/221 (39.8) 193/417 (46.3) 281/638 (44.0) 0.14c
Atopic dermatitisb 36/247 (14.6) 118/463 (25.5) 154/710 (21.7) 0.001Leg (ulcer/stasis eczema) 2/247 (0.8) 0 2/710 (0.3) 0.2Face 11/247 (4.5) 15/463 (3.2) 26/710 (3.7) 0.5
Age (years) median (25th to 75th percentile) 44 (3158) 37 (2851) 39.0 (2953) 0.0001d
OR (CI)e
1830 years 58 (23.5) 149 (32.2) 207 (29.2) 0.3 (0.180.52)3160 years 142 (57.5) 277 (59.8) 419 (59.0) 0.4 (0.250.64)>60 years 47 (19.0) 37 (8.0) 84 (11.8) 1
Duration of hand eczema n = 240 n = 453 n = 693OR (CI)e
5 years to 10 years 24 (10.0) 39 (8.6) 63 (9.1) 1.8 (0.93.4)>10 years 32 (13.3) 100 (22.1) 132 (19.0) 1
Long duration, >5 years 56 (23.3) 139 (30.7) 195 (28.1) 0.05c
Hand eczema in childhood 27/232 (11.6) 64/427 (15.0) 91/659 (13.8) 0.3c
Hand eczema eruptions n = 226 n = 433 n = 659 0.7cPresent all the time 112 (49.6) 206 (47.6) 318 (48.3)More than half of the time 70 (31.0) 147 (33.9%) 217 (32.9)Less than half of the time 44 (19.5) 80 (18.5) 124 (18.8)
DLQI score n = 239 n = 450 n = 689 0.001dMedian (25th to 75th percentiles) 3.0 (1.05.7) 4.0 (2.08.0) 3.0 (2.07.0)VAS present eczema n = 240 n = 447 n = 687 0.2dMedian (25th to 75th percentiles) 3.0 (1.55.0) 3.5 (1.55.5) 3.0 (1.55.0)VAS past 12 months n = 236 n = 443 n = 669 0.004dMedian (25th to 75th percentiles) 5.5 (4.07.5) 6.5 (4.58.0) 6.0 (4.08.0)
CI, confidence interval; DLQI, dermatology life quality index; OR, odds ratio; VAS, visual analogue scale.aPatients own assessment.bPhysicians assessment.Analysed by c2- test (two-sided).dMannWhitney U-test.elogistic regression. The OR quantifies the risk; for example, the OR of 2.4fshows the risk of being male in patients with a short duration ascompared with patients with a duration of hand eczema over 10 years. In other words, males are significantly overrepresented in patientswith short duration of hand eczema.
by a photoguide with typical photographs, as previouslypublished (1).
Chronic, dry fissured eczema was the most frequent(36.1%), followed by vesicular eczema with recurrenteruptions (31.8%). Each of the clinical types nummulareczema, hyperkeratotic palmar eczema, vesicular eczemawith rare eruptions, and pulpitis was seen in fewer than10% of the patients. Both pulpitis and hyperkeratoticpalmar hand eczema were statistically significantly morefrequent in men than in women, whereas for theremainder there were no sex differences. A tendencywas found for patients with hyperkeratotic palmar handeczema, nummular eczema or pulpitis to be older than
patients without these clinical types. This is in agreementwith previous studies (3, 10).
Vesicular hand eczemawith few eruptions had a lowerseverity score, both as assessed by the physician and incurrent self-assessment. This may be attributable to theshorter duration and the low number of eruptions, withnormal skin in between. This is supported by the findingthat self-assessment of severity for the past 12 monthswas as severe as for the other types of hand eczema.
It is the rule rather than the exception that diseases,in spite of having similar aetiologies, may show greatvariations clinically (4). This also applies to hand eczema.This study shows that there is no simple relationship
16 2011 John Wiley & Sons A/S Contact Dermatitis, 65, 1321
-
CLASSIFICATION OF HAND ECZEMA DUUS JOHANSEN ET AL.
Table 2. Data collected in consecutive hand eczema patients in dermatology clinics in Denmark; evaluation of hand eczema (physiciansassessment) was performed on the basis of the guideline of the Danish Contact Dermatitis Group
n/total (%) or median values (percentiles)
Men n = 247 Women n = 463Whole population
n = 710 p-value
Clinical classification n = 193 n = 364 n = 557Vesicular, rare eruptions 8 (4.1) 25 (6.9) 33 (5.9) 0.3a
Vesicular, repeated eruptions 58 (30.1) 119 (32.7) 177 (31.8) 0.6a
Dry fissured 67 (34.7) 134 (36.8) 201 (36.1) 0.7a
Hyperkeratotic palmar 22 (11.4) 19 (5.2) 41 (7.4) 0.01a
Nummular 16 (8.3) 28 (7.7) 44 (7.9) 0.8a
Pulpitis 8 (4.1) 4 (1.1) 12 (2.2) 0.04a
Non-classifiable 14 (7.3) 35 (9.6) 49 (8.8) 0.4a
Dynamics (past 6 months)Permanent activity 86 (38.9) 123 (29.5) 209 (32.8) 0.02a
Recurrent 76 (34.4) 184 (44.1) 260 (40.8) 0.02a
Rare eruptions 31 (14.0) 52 (12.5) 83 (13.0) 0.5a
SeverityHECSI median n = 209 n = 409 n = 618 0.4b
(25th to 75th percentiles) 7.5 (2.020.0) 6.0 (3.016.0) 6.5 (2.7518.0)
HECSI, Hand Eczema Severity Index.a2-test (two-sided).bMannWhitney U-test.
Fig. 2. Hand Eczema Severity Index (HESCI) score in consecutivehand eczema patients from dermatology clinics in Denmark. Datawere collected at the time of patch testing and are presentedaccording to clinical type of hand eczema, based on photographsgiven in the guideline of the Danish Contact Dermatitis Group (1).The boxes shows the quartiles, the line in the middle the median,and the whiskers the range. There is a significant differencebetween groups (p = 0.006) by KruskalWallis test.
between clinical type of hand eczema and aetiology, anobservation that was also made by Cronin, who studiedfour clinical patterns of hand eczema palms and fingers,dorsa and fingers, fingers only, and the entire hands inwomen (2). She found that all patterns of eczema wereequallyprone to sensitization,andalthough irritantswereof greater importance in eczema of the fingers and dorsaof the hands, they were nevertheless to be consideredsignificant in half (42%) of the palmar group (2).
Diepgen et al. recently investigated six different mor-phological features, such as erythema, infiltration, andvesicles, in 416 hand eczema patients, and found no clearrelationshipwith aetiological group (11). They suggesteda classification system of five aetiological groups andtwo clinical types (vesicular and hyperkeratotic handeczema) (11); however, no definitions were provided,which affects its applicability and reproducibility. Wilkin-son, in his chapter on classification of hand eczema in1994, gave a description of different clinical types of handeczema, which he suggested as a starting point and areference frame within which the relevant factors andbehaviour of similar patterns could be studied (3). Thecurrent study is based on this concept (1), and providesa classification of hand eczema both at the clinical leveland at the aetiological level in all cases. Some usefulobservationsweremade. Therewas no statistically signif-icant relationship between the diagnosis of current atopiceczema and any of the clinical types. This also appliedif a history of atopic eczema was used in the analysis
2011 John Wiley & Sons A/S Contact Dermatitis, 65, 1321 17
-
CLASSIFICATION OF HAND ECZEMA DUUS JOHANSEN ET AL.
Table3.
Charac
teristicsof
thediffe
rentc
linical
type
sof
han
deczemain
consecu
tive
han
deczemapa
tien
tsin
term
sof
dynam
icsan
dseve
rity
mea
suredby
aseve
rity
score[H
andEc
zema
Seve
rity
Inde
x(H
ECSI)],q
ualityof
life[D
ermatolog
yLifeQualityInde
x(D
LQI)]a
ndself-assessmen
tson
avisu
alan
alog
uescale(V
AS)
forthepresen
tandpa
stye
ar
n/total(%
)ormed
ianvalues
(percentiles)
Vesicular,rare
erup
tions
n=
33
Vesicular,recurrent
erup
tions
n=
177
Dry
fissured
n=
201
Hyp
erke
ratotic
palm
arn
=41
Num
mular
n=
44Pu
lpitis
n=
12Alln
=50
8p-valuea
Men
8(24.2)
58(32.8)
67(33.3)
22(53.7)
16(36.4)
8(66.7)
179(35.2)
Wom
en25
(75.8)
119(67.2)
134(66.7)
19(46.3)
28(63.6)
4(33.3)
329(64.8)
Age
(yea
rs)m
edian
38(2655
.5)
38(2949
)37
.0(2952
)45
(3258
.5)
47(30.059
.75)
55
(4061
.3)
39(2953
)0.00
7Dyn
amicsb
Con
stan
tactiv
ity10
8(53.7)
31
(75.6)
10
(22.7)
8(66.7)
15
7(55.1)