Class III–IV Proliferative Lupus Nephritis and Pregnancy: A Study of 42 Cases
7
Class III–IV Proliferative Lupus Nephritis and Pregnancy: A Study of 42 Cases INTRODUCTION Systemic lupus erythematosus (SLE) is the autoim- mune disease that most frequently compromises preg- nancy. 1,2 The coexistence of SLE and pregnancy is by no means a rare event, as SLE has a predilection for women of childbearing age. Maternal morbidity may be severe during an SLE exacerbation, and treatment itself is limited by pregnancy. On the contrary, active SLE places the embryo, fetus and neonate at enormous risk. 1,3 Studies published in the 1960s underlined the increased fetal and maternal risk and recommended protection against pregnancy in lupus patients. More recently, however, it has been reported that pregnancy in patients with SLE should not be regarded as an unacceptable high-risk condition for the mother or her baby provided that conception is accurately planned and patients are managed according to a careful multidisciplinary treatment schedule. 4–6 The above notwithstanding, renal disease was the only significant predictor of fetal loss in a recent multivariate analysis. 7 A number of studies have evaluated the reciprocal impact of pregnancy and lupus nephritis. However, available data often provi- ded conflicting results and pregnancy outcome accord- ing to the severity of lupus nephritis was not considered in previous reports. 6,8–10 The present study summarizes maternal and fetal outcome in 42 pregnancies in 35 SLE patients with the prolifera- tive forms (class III or IV) of lupus nephritis which are considered to represent the whole spectrum of the same pathogenetic group, generally follow a progressive course, share a similar clinical pattern and natural history, and are the most severe forms in terms of American Journal of Reproductive Immunology AJRI 2005; 53: 182–188 Copyright Ó Blackwell Munksgaard, 2005 Carmona F, Font J, Moga I, La`zaro I, Cervera R, Pac V, Balasch J. Class III–IV proliferative lupus nephritis and pregnancy: a study of 42 cases. AJRI 2005; 53:182–188 Ó Blackwell Munksgaard, 2005 PROBLEM: A growing number of women with lupus nephritis wish pregnancy. Our aim was to analyze maternal and fetal outcome in pregnancies with the most severe forms (proliferative or class III–IV) of lupus nephritis. METHOD OF STUDY: Forty-two pregnancies in 35 women with class III or IV lupus nephritis confirmed by renal biopsy (group 1); 12 pregnancies in 10 patients having histologically proven lupus nephritis class II or V (group 2); and 54 pregnant women randomly selected among our cohort of pregnant lupus patients without nephropathy who were matched for age, parity and duration of lupus to patients with class III or IV lupus nephritis (group 3) were studied. RESULTS: Pregnancy outcome and mean gestational age of neonates were similar in the three groups studied with hypertension and preeclampsia, being significantly more prevalent in patients in group 1 (37.1%) than among patients in groups 2 (11.1%) and 3 (11.6%) (P < 0.05). Mean birthweight (S.D.) was significantly lower in group 1 (2214 802 g) than in groups 2 (2783 721 g) and 3 (2870 835 g) (P < 0.05). CONCLUSION: Lupus nephritis class III–IV is a risk factor for hypertensive disease during pregnancy, but it does not contraindicate gestation. Francisco Carmona 1 , Josep Font 2 , Isabel Moga 3 , Isabel LȤzaro 1 , Ricard Cervera 2 , VisitaciɃn Pac 3 , Juan Balasch 1 1 Institut Clȷnic of Gynecology, Obstetrics, and Neonatology, Barcelona, Spain; 2 Department of Autoimmune Diseases, Faculty of Medicine, University of Barcelona, Hospital Clȷnic, Institut d'Investigacions Biomŕdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain; 3 Department of Internal Medicine, Hospital de Bellvitge-Prȷnceps d'Espanya, L'Hospitalet de Llobregat, Spain Key words: Hypertensive disorders, lupus nephritis, pregnancy, SLE Address reprint requests to J. Balasch, MD, Institut Clȷnic of Gynecology, Obstetrics, and Neonatology, Hospital Clȷnic, C/Casanova 143, 08036 Barcelona, Spain. E-mail: [email protected] Submitted October 29, 2004; revised January 14, 2005; accepted January 21, 2005. Ó BLACKWELL MUNKSGAARD, 2005
-
Upload
francisco-carmona -
Category
Documents
-
view
212 -
download
0
Transcript of Class III–IV Proliferative Lupus Nephritis and Pregnancy: A Study of 42 Cases

Class III–IV Proliferative Lupus Nephritisand Pregnancy: A Study of 42 Cases
INTRODUCTION
Systemic lupus erythematosus (SLE) is the autoim-mune disease that most frequently compromises preg-nancy.1,2 The coexistence of SLE and pregnancy is byno means a rare event, as SLE has a predilection forwomen of childbearing age. Maternal morbidity maybe severe during an SLE exacerbation, and treatmentitself is limited by pregnancy. On the contrary, activeSLE places the embryo, fetus and neonate at enormousrisk.1,3 Studies published in the 1960s underlined theincreased fetal and maternal risk and recommendedprotection against pregnancy in lupus patients. Morerecently, however, it has been reported that pregnancyin patients with SLE should not be regarded as anunacceptable high-risk condition for the mother or herbaby provided that conception is accurately planned
and patients are managed according to a carefulmultidisciplinary treatment schedule.4–6
The above notwithstanding, renal disease was theonly significant predictor of fetal loss in a recentmultivariate analysis.7 A number of studies haveevaluated the reciprocal impact of pregnancy andlupus nephritis. However, available data often provi-ded conflicting results and pregnancy outcome accord-ing to the severity of lupus nephritis was notconsidered in previous reports.6,8–10 The presentstudy summarizes maternal and fetal outcome in42 pregnancies in 35 SLE patients with the prolifera-tive forms (class III or IV) of lupus nephritis which areconsidered to represent the whole spectrum of the samepathogenetic group, generally follow a progressivecourse, share a similar clinical pattern and naturalhistory, and are the most severe forms in terms of
American Journal of Reproductive ImmunologyAJRI 2005; 53: 182–188Copyright � Blackwell Munksgaard, 2005
Carmona F, Font J, Moga I, Lazaro I, Cervera R, Pac V, Balasch J.Class III–IV proliferative lupus nephritis and pregnancy: a study of42 cases. AJRI 2005; 53:182–188 � Blackwell Munksgaard, 2005
PROBLEM: A growing number of women with lupus nephritis wishpregnancy. Our aim was to analyze maternal and fetal outcome inpregnancies with the most severe forms (proliferative or class III–IV)of lupus nephritis.METHOD OF STUDY: Forty-two pregnancies in 35 women withclass III or IV lupus nephritis confirmed by renal biopsy (group 1); 12pregnancies in 10 patients having histologically proven lupus nephritisclass II or V (group 2); and 54 pregnant women randomly selectedamong our cohort of pregnant lupus patients without nephropathywho were matched for age, parity and duration of lupus to patientswith class III or IV lupus nephritis (group 3) were studied.RESULTS: Pregnancy outcome and mean gestational age of neonateswere similar in the three groups studied with hypertension andpreeclampsia, being significantly more prevalent in patients in group 1(37.1%) than among patients in groups 2 (11.1%) and 3 (11.6%)(P < 0.05). Mean birthweight (�S.D.) was significantly lower in group1 (2214 � 802 g) than in groups 2 (2783 � 721 g) and 3 (2870 � 835 g)(P < 0.05).CONCLUSION: Lupus nephritis class III–IV is a risk factor forhypertensive disease during pregnancy, but it does not contraindicategestation.
Francisco Carmona1, Josep Font2,Isabel Moga3, Isabel L�zaro1,Ricard Cervera2, Visitaci�n Pac3,Juan Balasch11Institut Cl�nic of Gynecology, Obstetrics, andNeonatology, Barcelona, Spain; 2Department ofAutoimmune Diseases, Faculty of Medicine, University ofBarcelona, Hospital Cl�nic, Institut d'InvestigacionsBiom�diques August Pi i Sunyer (IDIBAPS), Barcelona,Spain; 3Department of Internal Medicine, Hospital deBellvitge-Pr�nceps d'Espanya, L'Hospitalet de Llobregat,Spain
Key words: Hypertensive disorders, lupus nephritis,pregnancy, SLE
Address reprint requests to J. Balasch, MD, Institut Cl�nicof Gynecology, Obstetrics, and Neonatology, HospitalCl�nic, C/Casanova 143, 08036 Barcelona, Spain.E-mail: [email protected]
Submitted October 29, 2004;revised January 14, 2005;accepted January 21, 2005.
� BLACKWELL MUNKSGAARD, 2005

prognosis. In contrast, class I and II represent minimalhistologic damage with very good prognosis and classV is a distinct group with rather good prognosis interms of renal function.11
MATERIAL AND METHODS
PatientsBetween January 1995 and December 2001, a total of42 pregnancies occurred in 35 women with previouslydiagnosed class III or IV lupus nephritis confirmed byrenal biopsy. These patients constituted the studygroup (group 1). Pregnancies occurring before thediagnosis of lupus nephropathy or nephropathy occur-ring after delivery were not taken into account.Histological patterns of SLE nephritis were assessedaccording to the 1995 WHO criteria.12 All patientsfulfilled the 1997 American College of Rheumatologycriteria for SLE.13 Antiphospholipid syndrome wasdiagnosed according to accepted criteria.14
For comparative purposes, two control groups wereused. Group 2 included 12 pregnancies in 10 SLEpatients previously diagnosed as having histologicallyproven lupus nephritis class II or V during the samestudy period. Finally, group 3 comprised 54 pregnantwomen randomly selected among our cohort of preg-nant SLE patients without lupus nephropathy whowere matched for age, parity and duration of SLE topatients in group 1.
All the SLE patients from three groups wereattending the two tertiary Department of AutoimmuneDiseases/Internal Medicine referral centers in Barce-lona and were followed up during pregnancy in a singleInstitute of Gynecology, Obstetrics and Neonatologyby a multidisciplinary team composed of obstetricians,autoimmunologists/internists, neonatologists andnephrologists. Institutional review board approvalwas not required because there were no interventionsother than those for the standard care of these patients.
Medical ManagementAt the time of pregnancy diagnosis, a completephysical examination was performed and visits werescheduled every 2 or 3 weeks (or more often whennecessary) until the 26th week; from 27th to 35thweeks, patients were scheduled fortnightly and then,weekly until delivery. After delivery, patients were seenevery 3 weeks until the second postpartum month.
The following laboratory tests were performedwithin 3 months before attempting conception and atthe first pregnancy visit and then, repeated monthly:hematological parameters (including hemoglobin, redand white cell and platelet counts and erythrocytesedimentation rate), serum levels of creatinine, uric
acid, proteins, sodium, alanine and aspartate amino-transpherases, urine microscopy and 24-hr urine col-lection for measurement of creatinine clearance, totalproteinuria and sodium and calcium excretion. Immu-nological evaluation was performed within 3 monthsbefore attempting conception and at the first preg-nancy visit and then, repeated every 10–12 weeksduring pregnancy and included: lupus anticoagulant(LA) and anticardiolipin antibodies (aCL) usingmethods previously described,15–18 antinuclear anti-bodies (ANA) (indirect immunofluorescence usingmouse liver as substrate), antidouble-stranded DNAantibodies (Farr’s technique), C3, C4 (radial immuno-diffusion) and CH50 (Lachmann’s hemolytic tech-nique) complement components as well as Coombs�test for autoimmune hemolysis and determination ofthe rheumatoid factor activity (latex fixation andWaaler-Rose tests). Precipitating antibodies to extract-able nuclear antigens (ENA) including Ro (SS-A) andLa (SS-B), RNP, and Sm (counter immunoelectropho-resis) were determined performed within 3 monthsbefore attempting conception and at the first preg-nancy visit.
Disease activity was determined according to thelupus activity criteria count,19 an overall and clinicallyuseful method of disease activity evaluation,20 that hasbeen used in many clinical studies.4,21–23 A flare wasconsidered when a clinical manifestation attributableto disease activity appeared during the course of thestudy period.
Patients were advised to become pregnant when SLE(including lupus nephropathy) was inactive for at least6 months and they were taking no cytotoxic drugs inthe previous 12 months (except azathioprine, whichwas given to 12 patients in group 1 at daily dosesof 50–100 mg). Hydroxycloroquine, 200 mg/day(15 patients in groups 1 and 2, and nine patients ingroup 3) and prednisone (5–20 mg/day) (all patients ingroups 1 and 2, and 24 patients in group 3) weremaintained in those patients who were previouslytaking these drugs. Lupus flare was treated withprednisone (0.25–1 mg/kg/day, depending on severity);after remission, prednisone was continued at a dose aslow as possible. In patients testing positive for LA and/or aCL, aspirin (100 mg/day) was added from 1 monthbefore attempting conception and throughout preg-nancy, as previously reported.24–26 Heparin was alsoadded if previous thrombotic events were present orwhen there were previous pregnancy losses undertreatment with aspirin alone.
Obstetrical ManagementObstetrical visits were scheduled as for medical man-agement. As SLE pregnancies are high-risk pregnan-cies, in addition to routine pregnancy management,
LUPUS NEPHRITIS AND PREGNANCY / 183
AMERICAN JOURNAL OF REPRODUCTIVE IMMUNOLOGY VOL. 53, 2005
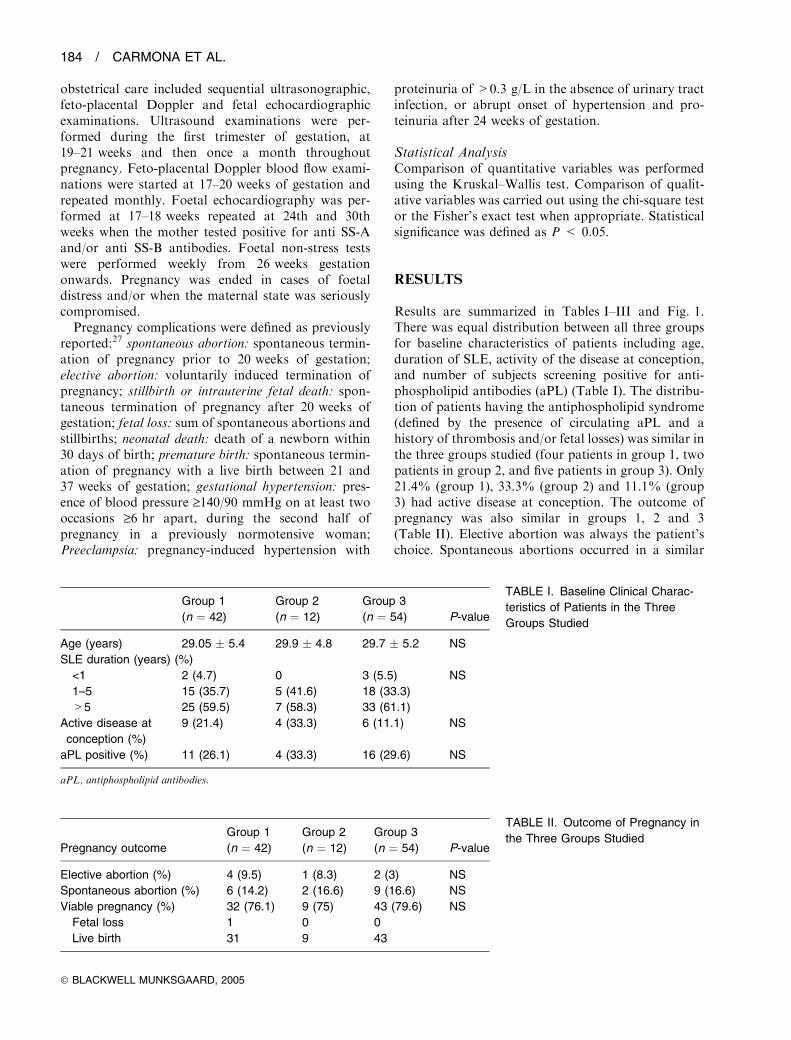
obstetrical care included sequential ultrasonographic,feto-placental Doppler and fetal echocardiographicexaminations. Ultrasound examinations were per-formed during the first trimester of gestation, at19–21 weeks and then once a month throughoutpregnancy. Feto-placental Doppler blood flow exami-nations were started at 17–20 weeks of gestation andrepeated monthly. Foetal echocardiography was per-formed at 17–18 weeks repeated at 24th and 30thweeks when the mother tested positive for anti SS-Aand/or anti SS-B antibodies. Foetal non-stress testswere performed weekly from 26 weeks gestationonwards. Pregnancy was ended in cases of foetaldistress and/or when the maternal state was seriouslycompromised.Pregnancy complications were defined as previously
reported:27 spontaneous abortion: spontaneous termin-ation of pregnancy prior to 20 weeks of gestation;elective abortion: voluntarily induced termination ofpregnancy; stillbirth or intrauterine fetal death: spon-taneous termination of pregnancy after 20 weeks ofgestation; fetal loss: sum of spontaneous abortions andstillbirths; neonatal death: death of a newborn within30 days of birth; premature birth: spontaneous termin-ation of pregnancy with a live birth between 21 and37 weeks of gestation; gestational hypertension: pres-ence of blood pressure ‡140/90 mmHg on at least twooccasions ‡6 hr apart, during the second half ofpregnancy in a previously normotensive woman;Preeclampsia: pregnancy-induced hypertension with
proteinuria of >0.3 g/L in the absence of urinary tractinfection, or abrupt onset of hypertension and pro-teinuria after 24 weeks of gestation.
Statistical AnalysisComparison of quantitative variables was performedusing the Kruskal–Wallis test. Comparison of qualit-ative variables was carried out using the chi-square testor the Fisher’s exact test when appropriate. Statisticalsignificance was defined as P < 0.05.
RESULTS
Results are summarized in Tables I–III and Fig. 1.There was equal distribution between all three groupsfor baseline characteristics of patients including age,duration of SLE, activity of the disease at conception,and number of subjects screening positive for anti-phospholipid antibodies (aPL) (Table I). The distribu-tion of patients having the antiphospholipid syndrome(defined by the presence of circulating aPL and ahistory of thrombosis and/or fetal losses) was similar inthe three groups studied (four patients in group 1, twopatients in group 2, and five patients in group 3). Only21.4% (group 1), 33.3% (group 2) and 11.1% (group3) had active disease at conception. The outcome ofpregnancy was also similar in groups 1, 2 and 3(Table II). Elective abortion was always the patient’schoice. Spontaneous abortions occurred in a similar
TABLE I. Baseline Clinical Charac-
teristics of Patients in the Three
Groups Studied
Group 1
(n ¼ 42)
Group 2
(n ¼ 12)
Group 3
(n ¼ 54) P-value
Age (years) 29.05 � 5.4 29.9 � 4.8 29.7 � 5.2 NS
SLE duration (years) (%)
<1 2 (4.7) 0 3 (5.5) NS
1–5 15 (35.7) 5 (41.6) 18 (33.3)
>5 25 (59.5) 7 (58.3) 33 (61.1)
Active disease at
conception (%)
9 (21.4) 4 (33.3) 6 (11.1) NS
aPL positive (%) 11 (26.1) 4 (33.3) 16 (29.6) NS
aPL, antiphospholipid antibodies.
TABLE II. Outcome of Pregnancy in
the Three Groups StudiedPregnancy outcome
Group 1
(n ¼ 42)
Group 2
(n ¼ 12)
Group 3
(n ¼ 54) P-value
Elective abortion (%) 4 (9.5) 1 (8.3) 2 (3) NS
Spontaneous abortion (%) 6 (14.2) 2 (16.6) 9 (16.6) NS
Viable pregnancy (%) 32 (76.1) 9 (75) 43 (79.6) NS
Fetal loss 1 0 0
Live birth 31 9 43
184 / CARMONA ET AL.
� BLACKWELL MUNKSGAARD, 2005

percentage in all three groups and they were associatedwith the presence of aPL (10.3% in patients withoutaPL and 29% in patients with aPL; P < 0.05).
Medical and obstetrical complications in potentiallyviable pregnancies are presented in Table III. Themost striking difference between study groups was thathypertension and preeclampsia were more prevalentamong patients in group 1. Cesarean rate tended to behigher in group 1 when compared with groups 2and 3, although this was not statistically significant(P ¼ 0.06). Birth weight of neonates was lesser ingroup 1 when compared with groups 2 and 3 (P ¼0.02). However, the mean gestational age of neonateswas not significantly different in the three groupsstudied. As reported in Tables I and III there was notstatistically significant difference in disease activity atconception or during pregnancy among patients in thethree groups studied when stratified by active andinactive disease or flare rate. Flare rates were similarin the three groups of patients. Four patients in group1 and one in group 2 presented renal flare, mainlycharacterized by increased proteinuria and renalfunction impairment. They were treated by increasingthe dose of prednisone (0.25 to 1 mg/kg/day) andadding azathioprine (100 mg/day). All patientsimproved after delivery. The clinical manifestationsof flares in the remaining patients in groups 1, 2 and 3,included mainly cutaneous (n ¼ 2 in group 1; n ¼ 2 ingroup 2; n ¼ 7 in group 3) or articular (n ¼ 1 in group1; n ¼ 1 in group 2; n ¼ 5 in group 3) symptoms orboth.
Fig. 1 shows sequential renal function evaluationduring pregnancy and at 6–8 weeks postpartum. Pro-teinuria was significantly increased on the thirdtrimester of pregnancy with respect to baseline valuesobserved before conception in groups 1 and 2 but notin non-nephropathy controls. The percentage changein proteinuria from baseline values was significantlyhigher in group 1 when compared with patients ingroup 2 (Fig. 1). Plasma creatinine levels showed no
significant changes throughout pregnancy in the threegroups studied (Fig. 1).
DISCUSSION
As many women with SLE are of childbearing age andhave normal fertility, the clinician often faces manyproblems relating to pregnancy in patients with lupus
TABLE III. Obstetrical and Medical
Complications of Viable Pregnancies
in the Three Groups Studied
Group 1
(n ¼ 32)
Group 2
(n ¼ 9)
Group 3
(n ¼ 43) P-value
Hypertension (%) 12 (37.5) 1 (11.1) 5 (11.6) 0.01
Preeclampsia (%) 9 (28.1) 0 2 (4.6) 0.005
Gestational age (weeks) 35.6 � 2.6 36.8 � 3.3 37.2 � 4.2 NS
Preterm delivery (%) 10 (34.6) 3 (26.6) 8 (18.6) NS
Cesarean (%) 14 (43.7) 3 (33.3) 8 (18.6) 0.06
Birthweight (g) 2214 � 802 2783 � 721 2870 � 835 0.02
Flare* (%) 8 (19) 4 (33.3) 15 (27.7) NS
Renal flare 4 1 0
*Including flares in non-viable pregnancies.
Figures are mean � S.E.M.
Fig. 1. Proteinuria and creatinine plasma levels throughout preg-
nancy in patients with class III–IV lupus nephritis (open bars), class
II and V lupus nephritis (black bars) and SLE patients without lupus
nephritis (dashed bars).
LUPUS NEPHRITIS AND PREGNANCY / 185
AMERICAN JOURNAL OF REPRODUCTIVE IMMUNOLOGY VOL. 53, 2005

nephritis. These include the influence of lupus nephritison fetal outcome, obstetric complications, and theinfluence of pregnancy on lupus nephropathy. Thissubject has been thoroughly reviewed in a recent reportincluding retrospective and prospective nephrologicaland obstetrical studies conducted with at least15 patients published between 1980 and 2001.6
Reports on lupus pregnancy from the 1950s and1960s mention patients with nephritis, usually in thecontext of severe flare, increasing proteinuria, azote-mia or acute anuric renal failure, hypertension,preeclampsia, onset of nephritis during pregnancy,and even maternal deaths.27 On the contrary, in the1970s and 1980s, several papers reported on uneventfulcourse of pregnancy, or a better prognosis, when renalfunction is normal, and lupus nephritis has beeninactive for 3–6 months before conception. This trendhas continued through the 1990s.10,27
At present, it is accepted that most lupus pregnan-cies do well, but there is an increased incidence ofadverse fetal outcome.28 Theoretically, several factorscan account for the increased frequency of fetal loss inSLE patients, but in a recent multivariate analysis,maternal renal disease was the only statistically signi-ficant predictor for fetal loss and hypertension for poorfetal outcome.7 The risk of fetal loss in lupus nephritispatients has been established as between 12 and 38%.6
Miscarriage accounted for 8–24% of fetal loss, whilestillbirths or neonatal deaths accounted for 4–24%.6
On the contrary, preeclampsia is more likely to occurin women with renal disease, arterial hypertension andaPL.10,27,29,30 Remarkably, a recent study30 has shownthat aPL are associated with an increased risk forchronic renal insufficiency in patients with lupusnephritis.The above result is in agreement with those in the
present study when: (i) both medical and obstetricalcomplications were associated mainly with the pres-ence of circulating aPL; and (ii) hypertensive disorderswere significantly more prevalent in group 1 than incontrol groups. The relative low incidence of obstet-rical and medical complications related to aPL may beexplained by the fact that all our patients receivedappropriate treatment25 which was started beforeconception. In lupus pregnancy, up to 25% of patientsdevelop significant proteinuria and hypertension in thesecond half of pregnancy.27 Opinions have variedwidely as to whether this represents preeclampsia oractive lupus nephritis. However, it is accepted thatinvestigation of serum complement levels (C3), anti-DNA antibodies, and urinary sediment, as done in thepresent study, can help to differentiate between activelupus nephritis and preeclampsia. A lupus flare isfrequently associated with hypocomplementenemia,high titers of anti-DNA antibodies, and an active
urinary sediment (red and white blood cells andcellular casts).6,27 Thus, according to our results,hypertensive disease but not lupus flare in pregnancyis significantly associated with advanced classes oflupus nephritis.
In pregnancy with maternal renal disease other thanlupus nephritis, hypertension develops in 41% of thesewomen, with a higher risk for severe hypertension inwomen with diffuse proliferative nephritis or withnephrosclerosis.27 This is in agreement with results inthe present investigation when showing that hyperten-sive disease was significantly more prevalent amongpatients in group 1 having class III or IV nephritis. Inthese women too, hypertension occurs most oftenduring the third trimester. Women with prior chronichypertension may develop preeclampsia in pregnancy,and the term �superimposed preeclampsia� is used.27
Superimposed preeclampsia occurred in 44% of ourpreeclamptic patients in group 1.
Preeclampsia is caused by shallow placentation,insufficient development of the spiral arteries in theuteroplacental vasculature, which results in placentalischemia, oxidative stress, destruction of trophoblastictissue, and infarction. It results in increased resistanceof the uteroplacental circulation, atherosis of theplacental vessels, systemic endothelial dysfunction,and ischemia with intrauterine growth restriction inthe fetus and hypertension in the mother.27 This mayexplain both the increased rate of cesarean section andlow-birth-weight neonates observed in group 1 in ourstudy. Remarkably, however, fetal loss rate was notsignificantly increased in patients in group 1 whencompared with groups 2 and 3.
The potential impact of pregnancy on lupus activityhas been debated for decades without a consensus.Data on the potential impact of pregnancy in patientswith lupus nephritis are scanty. Thus, Moroni et al.31
reported that the incidence of renal flares observed inthe period from the diagnosis of lupus nephritis to thebeginning of pregnancy was similar to that observedduring pregnancy and 6 months after delivery. This isin agreement with results in our study where the lupusflare and renal flare rates during pregnancy andpuerperium were similar in patients with SLE withoutnephropathy and lupus nephritis patients irrespectiveof the lupus nephritis class. In this regard, it has beenrecently stressed9 that in a nephrological seriesincluding only women with SLE nephritis diagnosedbefore pregnancy, flares rates of 0 and 9% werefound in the most recent studies, probably becausemost pregnancies had begun when SLE was inremission. On the contrary, in the older studiesincluding women with SLE nephritis diagnosedduring pregnancy, higher flare rates, up to 81%,were seen.
186 / CARMONA ET AL.
� BLACKWELL MUNKSGAARD, 2005

There was a potential limitation to this study.Patients were classified on the basis of renal histologyat time of renal biopsy but not at time of start ofpregnancy. Thus, several years could have passedbetween these two times for a number of patients.Considering that lupus nephritis is a treatable condi-tion with possibility, under treatment, of completeremission or change of class of renal histology, wecannot be entirely sure that initial histological class ofnephropathy could be responsible of the pregnancyoutcome. However, this is a common feature in studiesreporting on pregnancy outcome in women with long-standing SLE nephritis and what seems clear from thecurrent investigation and previous reports6,8–10 is thatthe risk of obstetrical and medical complications inpatients with lupus nephritis continues to be higherthan in pregnancies in healthy women and SLE patientswithout lupus nephritis. This is to be noted consideringthat, as recently stressed,9 a growing number of womenwith nephritis in the past wish to be pregnant.
In conclusion, in our experience, pre-existing renalinvolvement in the form of lupus nephritis class III–IVis clearly a risk factor for hypertensive disease duringpregnancy, but it does not contraindicate gestationprovided that careful planning of conception andmultidisciplinary monitoring and treatment are carriedout.
AcknowledgementsThis work was supported in part by grants from theInstituto de Salud Carlos III (RCMN C03/08), and theComissionat per a Universitat i Recerca-Generalitat deCatalunya (2001SGR 00372).
REFERENCES
1. Del Junco DJ. Association of autoimmune conditionswith recurrent intrauterine death. Clin Obstet Gynecol1986; 29:959–975.
2. Gimovsky ML, Montoro M. Systemic lupus erythema-tosus and other connective tissue diseases in pregnancy.Clin Obstet Gynecol 1991; 34:35–50.
3. Lockshin MD. Overview of lupus pregnancies. Am JReprod Immunol 1992; 28:181–182.
4. Carmona F, Font J, Cervera R, Munoz F, Cararach V,Balasch J. Obstetrical outcome of pregnancy inpatients with systemic lupus erythematosus. A study of60 cases. Eur J Obstet Gynecol Reprod Biol 1999;83:137–142.
5. Derksen RHWM, Bruinse HW, Groot PG, Kater L.Pregnancy in systemic lupus erythematosus: a prospectivestudy. Lupus 1994; 3:149–155.
6. Moroni G, Ponticelli C. The risk of pregnancy in patientswith lupus nephritis. J Nephrol 2003; 16:161–167.
7. Rahman P, Gladman DD, Urowitz MB. Clinical pre-dictors of fetal outcome in systemic lupus erythematosus.J Rheumatol 1998; 25:1526–1530.
8. Julkunen H. Pregnancy and lupus nephritis. Scand J UrolNephrol 3001; 35:319–327.
9. Huong DLT, Wechsler B, Vauthier-Brouzes D, BeaufilsH, Lefebvre G, Piette JC. Pregnancy in past or presentlupus nephritis: a study of 32 pregnancies from a singlecentre. Ann Rheum Dis 2001; 60:599–604.
10. Rahman FZ, Rahman J, Al-Suleiman SA, Rahman MS.Pregnancy outcome in lupus nephropathy. Arch GynecolObstet 2004; Mar 30 (Epub ahead of print).
11. Contreras G, Roth D, Pardo V, Striker LG, Schultz DR.Lupus nephritis: a clinical review for practicing nephrol-ogists. Clin Nephrol 2002; 57:95–107.
12. Kashgarian M. Lupus nephritis: pathology, pathogenesis,clinical correlations, and prognosis. In Dubois� LupusErythematosus, DJWallace, BHHahn (eds). Philadelphia,PA, Lippincot Williams & Wilkins, 2002, pp 1062–1076.
13. Grossman JM, Kalunian KC. Definition, classification,activity, and damage indices. In Dubois� Lupus Erythe-matosus, DJ Wallace, BH Hahn (eds). Philadelphia, PA,Lippincot Williams & Wilkins, 2002, pp 19–31.
14. Coulam CB, Branch DW, Clark DA, Gleicher N, KuttehW, Lockshin MD, Rote NS: American Society forReproductive Immunology. Report of the Committee forEstablishing Criteria for Diagnosis of ReproductiveAutoimmune Syndrome. Am J Reprod Immunol 1999;41:121–132.
15. Balasch J, Font J, Lopez-Soto A, Cervera R, Jove I,Casals FJ, Vanrell JA. Antiphospholipid antibodies inunselected patients with repeated abortion. Hum Reprod1990; 5:43–46.
16. Balasch J, Carmona F, Lopez-Soto A, Font J, Creus M,Fabregues F, Ingelmo M, Vanrell JA. Low-dose aspirinfor prevention of pregnancy losses in women with pri-mary antiphospholipid syndrome. Hum Reprod 1993;8:2234–2239.
17. Font J, Lopez-Soto A, Cervera R, Balasch J, Pallares L,Navarro M, Bosch X, Ingelmo M. The �primary� anti-phospholipid syndrome: antibody pattern and clinicalfeatures of a series of 23 patients. Autoimmunity 1991;9:69–75.
18. Font J, Cervera R, Navarro M, Pallares L, Lopez-SotoA, Vivancos J, Ingelmo M. Systemic lupus erythematosusin men: clinical and immunological characteristics. AnnRheum Dis 1992; 51:1050–1052.
19. Urowitz MB, Gladman DD, Tozman ECS, GoldsmithCH. The lupus activity criteria count (LACC). J Rheu-matol 1984; 11:783–787.
20. Grossman JM, Kalunian KC. Definition, classification,activity, and damage indices. In Dubois� Lupus Erythe-matosus, DJ Wallace, BH Hahn (eds). Philadelphia, PA,Lippincot Williams & Wilkins, 2002, pp 19–31.
21. Pacilio M, Migliaresi S, Meli R, Ambrosone L, BigliardoB, Di Carlo R. Elevated bioactive prolactin levels insystemic lupus erytheamtosus – association with diseaseactivity. J Rheumatol 2001; 28:2216–2221.
22. Arce-Salinas A, Cardiel MH, Guzman J, Alcocer-VarelaJ. Validity of retrospective assessment in systemic lupuserythematosus. J Rheumatol 1996; 23:846–849.
23. Esdaile JM, Abrahamowicz M, MacKenzie T, HayslettJP, Kashgarian M. The time-dependence of long-termprediction in lupus nephritis. Arthritis Rheum 1994;37:359–368.
24. Balasch J, Carmona F, Creus M, Font J, Cervera R.Management of reproductive autoimmune failure in the
LUPUS NEPHRITIS AND PREGNANCY / 187
AMERICAN JOURNAL OF REPRODUCTIVE IMMUNOLOGY VOL. 53, 2005

antiphospholipid syndrome. In The AntiphospholipidSyndrome II, RA Ashershon, R Cervera, JC Piette, YShoenfeld (eds). Amsterdam, Elsevier, 2002: pp 375–394.
25. Carmona F, Font J, Azulay M, Creus M, Fabregues F,Cervera R, Puerto B, Balasch J. Risk factors associatedwith fetal losses in treated antiphospholipid syndromepregnancies: a multivariate analysis. Am J ReprodImmunol 2001; 46:274–279.
26. Farquharson RG, Quenby S, Greaves M. Antiphosp-holipid syndrome in pregnancy: a randomized, controlledtrial of treatment. Obstet Gynecol 2002; 100:408–413.
27. Kitridou RC. The mother in systemic lupus erythemato-sus. In Dubois� Lupus Erythematosus, DJ Wallace, BHHahn (eds). Philadelphia, PA, Lippincot Williams &Wilkins, 2002: pp 988–1021.
28. Cervera R, Font J, Carmona F, Balasch J. Pregnancyoutcome in systemic lupus erythematosus: good news forthe new millennium. Autoimmunity Rev 2002; 1:354–359.
29. Branch DW, Andres R, Digre KB, Rote NS, Scott JR.The association of antiphospholipid antibodies withsevere preeclampsia. Obstet Gynecol 1989; 73:541–545.
30. Moroni G, Ventura D, Riva P, Panzeri P, Quaglini S,Banfi G, Simonini P, Bader R, Meroni PL, Ponticelli C.Antiphospholipid antibodies are associated with anincreased risk for chronic renal insufficiency in patientswith lupus nephritis. Am J Kidney Dis 2004; 43:28–36.
31. Moroni G, Quaglini S, Banfi G, Caloni M, Finazzi S,Ambroso G, Como G, Ponticelli C. Pregnancy in lupusnephritis. Am J Kidney Dis 2002; 40:713–720.
188 / CARMONA ET AL.
� BLACKWELL MUNKSGAARD, 2005