CLABSI Definition with Case Studies - cdc.gov · CLABSI Definition with Case Studies NHSN...
74
National Center for Emerging and Zoonotic Infectious Diseases CLABSI Definition with Case Studies NHSN Bloodstream Infection Surveillance in 2017 NHSN Annual Training March 22, 2017 Kyle Puckett, BS, RRT, RCP, CIC Infection Prevention Consultant
Transcript of CLABSI Definition with Case Studies - cdc.gov · CLABSI Definition with Case Studies NHSN...

National Center for Emerging and Zoonotic Infectious Diseases
CLABSI Definit ion with Case Studies
NHSN Bloodstream Infect ion Surveillance in 2017
NHSN Annual Training March 22, 2017Kyle Puckett, BS, RRT, RCP, CICInfection Prevention Consultant

Object ives / Outline
Locate the training resources, protocol and supporting materials
Define key terms for device-associated infections specifically CLABSI
Discuss device-associated infection surveillance changes for 2017
Identify Case Studies correctly
Describe data collection process for key NHSN locations (Numerator & Denominator)

3
Reality that is CLABSI~30,000 CLABSI Events annually
~46% Reduction Mortality Rate 12-25% Cost ~ $70,696
Estimates of infections and deaths prevented and excess costs averted among participating adult ICUs using all data (“reported”) and data after missing value imputation (“estimated”) using CDC estimates
Health Research and Education Trust.(October 2012), Eliminating CLABSI, A National Patient Safety Imperative – AHRQ. Retrieved from https://www.ahrq.gov/sites/default/files/publications/file/clabsicompanion.pdf

4
NHSN Resources cdc.gov/NHSN

5
BSI Training Resources

6
Surveillance Protocols

7
Frequently Asked Quest ions
8
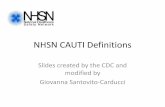
Support ing Material

Acronyms & Key Terms Defined
Organism cultured from the blood was seeded from another primary site specific infection source such as UTI, SSI, PNEU, or one from Chapter 17
Secondary BSI’s do not create a BSI RIT,
Primary BSI
Secondary BSI
Organism cultured from the blood that is notrelated to an infection at another site. LCBI 1, LCBI 2, LCBI 3
Primary BSI’s create a 14 day RIT

Acronyms & Key Terms Defined continued…
An intravascular catheter that terminates at or close to the heart or in one of the great vessels which is used for infusion, withdrawal of
blood, or hemodynamic monitoring. Central Line
• Aorta• Pulmonary artery• Superior vena cava• Inferior vena cava• Brachiocephalic veins• Internal jugular veins
• Subclavian veins• External iliac veins• Common iliac veins• Femoral veins• Umbilical artery/vein
(neonate)
Once a Central Line it stays a Central Line until removed
Great Vessels for CLABSI Reporting

11
Acronyms & Key Terms Defined continued…
Temporary: A non-tunneled, non-implanted catheter Permanent: A Tunneled (including certain dialysis)
catheters or implanted port Umbilical catheter: Inserted through the umbilical artery
or vein in a neonate
Arterial Catheters Arteriovenous fistula Arteriovenous graft Extracorporeal membrane
oxygenation (ECMO) Hemodialysis reliable outflow
(HERO) dialysis catheters
Intra-aortic balloon pump (IABP) devices
Ventricular Assist Devices(VAD) Non-accessed central line (not
accessed nor inserted) Peripheral IV’s Any device without a lumen
Devices that are NOT considered central lines for NHSN reporting
Introducer may or may not be a central line
Types of Central Lines

Acronyms & Key Terms Defined cont inued…
An exclusion is in place specifically for IVDA’s who have documentation within the IWPof observed or suspected inject ion into their vascular access.
This is considered an LCBI but not a CLABSI
Line placement, insertion of a needle into the port, infusion or withdrawal through the line.
Access = an eligible line for CLABSI eventsInfusion- administering a solution into a blood vessel via a
catheter lumen
Central Line Access
Patient Access of Central Line
If reporting into NHSN event field: Central line? = NODoes create a 14 day BSI RIT

Acronyms & Key Terms Defined continued…
LCBI 1, 2, or 3 with a qualifying CL in place for >2calendar days on the DOE AND the line was in place
on the DOEor the day before = CLABSI.
CL placed-CL day 1
“Accessed” X
CL Day 2
X
CL Day 3
*Eligible for CLABSI
CL removed CL Day 4
*Eligible for CLABSI
No CL
*Eligible for CLABSI
No CL
X
CL placed CL Day 1
“Accessed”X
CL outCL Day 2
X
Implanted port
ø accessed or placed
X
Implanted
port
ø accessed
X
Implanted port
accessed-CL Day 1
X
Implanted port
accessed-CL Day 2
X
Implanted port de-accessed-CL Day 3
*Eligible for CLABSI
Implanted port
ø accessed-CL Day 4
*Eligible for CLABSI
Implanted port
ø accessed-CL Day 5
*Eligible for CLABSI
Implanted port
ø accessed-CL Day 6
*Eligible for CLABSI
YES
Jan 1 Jan 2 Jan 3 Jan 4 Jan 5 Jan 6 Jan 7 Jan 8
Table Representation of Central Line Count & CLABSI Event Eligibility
Central Line Associated BSI
CLABSI

IWP: Infect ion Window
Period
The 7-day period: in which all site-specific infection criterion must be met. It includes the date of collect ion of the first blood specimen which identifies an organism in the blood, 3 calendar days before and 3 calendar days after
DOE: Date of Event
LCBI 1:DOEwill always be the date of the blood specimen collection which identifies an organism in the blood (will always be a recognized pathogen) No symptom requiredLCBI 2 or 3:DOEwill always be the first date an element that is used to meet the LCBI 2 or 3 criteria (symptom or the first of 2 cultures with matching CC) occurs within the BSI IWP
Acronyms & Key Terms Defined cont inued…

15
Mr. Price 6/1: Mr. Price is admitted to CCU after
having a heart attack. A central line was placed on admission
6/3 Developed a fever 39C.
6/4: : Pt confused, hypotensive, Blood culture drawn, grew CNS (common commensal).
6/5 BC repeated, grew S. epidermidis (matching common commensal)
6/8: Central line discontinued
Hosp day / date
First Diagnostic
Test IWP DOE RIT Notes
6/1 Admit, CL placed
6/2
6/3 Fever 39⁰C
6/4 BC+ CNS ↓BP
6/5 BC + S. epi
6/6
6/7
6/8 CL discontinued
6/9
6/10
6/11
6/12
6/13
6/14
6/15
6/16
6/17
BC + CNS DOE
3 Day Before
DOE
3 Day After DOE
DOEDOE=HAI
RIT= 14 Days
with DOE = Day 1
Adm CCU -CL placed
HAI CLABSI with S. epidermidis DOE 6/3
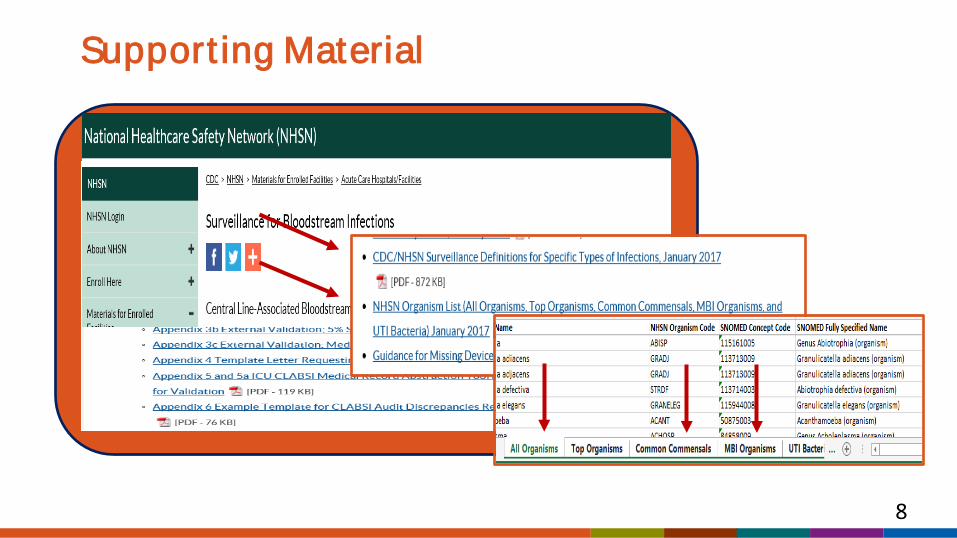
New 2017 Excluded BSI Organisms Campylobcter spp. C. difficile Enteropathogenic E. coli Salmonella spp. Shigella spp. Listeria spp. Yersinia spp.
Group B Strep: Excluded for the first 6 days of lifeIs considered an LCBI that creates an RIT but is NOT a CLABSI
Excluded from ALL NHSN Definitions Blastomyces Histoplasma Coccidioides Paracocidioides Cryptococcus Pneumocystis

17
What is a matching organism?
If the organism is less definit ively ident ified in one culture than the other, the ident ificat ions must be complementary.
Ex: A blood culture growing CNS and a blood culture growing S. epidermidis are
considered a match because S. epidermidis is a CNS
Ex: A blood culture growing CNS and a blood culture growing Staphylococcusare
NOT considered matching because Staphylococcus can be either CNS or CPS
How to Report Speciated & Un-Speciated
ResultsTable found on page 4-17 of the BSI protocol

18
Surveillance Definit ions ≠ Clinical Diagnosis
Surveillance Definit ions Clinical Diagnosis
Purpose Identify trends within a populat ion for prevention efforts
and research
Identify disease in, and treatment needs for, individual pat ients
Components Limited to objective data All diagnostic information available
Clinical judgment Excluded if possible Valued

19
Laboratory Confirmed Bloodstream Infection
LCBI
LCBI 1
MBI-LCBI 1
LCBI 2
MBI-LCBI 2
LCBI 3
MBI-LCBI 3

20
LCBI
LCBI 1
Any age patient1 specimen
Recognized pathogenNo symptom
LCBI 2
Any age patient2 specimens
Matching CCsPlus one symptom
LCBI 3
< 1 year old2 specimens
Matching CCsPlus one symptom
If LCBI 1 and LCBI 2 are met, report as LCBI 1with pathogen first

21
Invest igat ing a + Blood Specimen as Possible CLABSI
Primary BSI’s do NOT have a secondary BSI attribution Period
Infect ion is suspected based on + blood specimen1. Determine the IWP √2. Determine elements present in IWP √3. Consider the organism & determine DOE √4. Determine if POA or HAI √
if POA-stop, nothing to report 5. If HAI determine device association & location of attribution √6. Determine RIT √7. Determine if another site specific source of infection present
If secondary, stop-no LCBI to report-go to secondary BSI8. If not secondary: determine LCBI 1, LCBI 2 or LCBI 3 based on organism & symptom if required √
LCBI Criterion 1
Patient of any age has a recognized pathogen identified from one or more blood specimens by a culture or non-culture based microbiologic testing method
AND Organism(s) identified in blood is not related
to an infection at another site
Primary BSI’s do NOT have a secondary BSI attribution Period

Mr. Smith
Jan. 1st Mr. Smith was admitted to CCU after having a heart attack.
Jan. 2nd A central line was placed in the cath lab. Jan. 4th A blood culture was collected because he
became confused and was having chills. Culture resulted E. faecalis (a recognized pathogen) No other source of infection was identified.

24
Mr. SmithIs this an LCBI?
A. YesB. No

25
Mr. Smith Is it Central Line Associated?
A. YesB. No

26
Mr. Smith Rationale Test IWP DOE RIT
BC + E. faecalis
No o
Hosp day / date
First Diagnostic
Notes1-Jan Adm CCU2-Jan CL placed
3-Jan
4-Jan chills5-Jan
6-Janther source of infection
7-Jan8-Jan9-Jan
10-Jan11-Jan12-Jan13-Jan14-Jan15-Jan16-Jan17-Jan18-Jan19-Jan
Mr. Smith has a primary HAI ; LCBI 1 that is central
line associated, IWP 1/1 - 1/7,
DOE 1/4, RIT /1/4 - 1/17
with E. faecalis attributed to CCU
CL placed
27
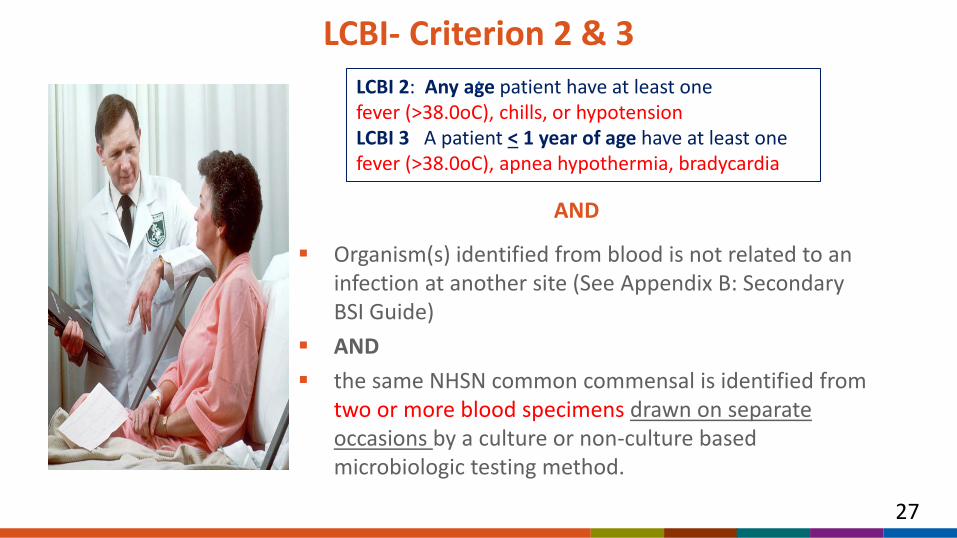
LCBI- Criterion 2 & 3
Organism(s) identified from blood is not related to an infection at another site (See Appendix B: Secondary BSI Guide)
AND the same NHSN common commensal is identified from
two or more blood specimens drawn on separate occasions by a culture or non-culture based microbiologic testing method.
LCBI 2: Any age patient have at least onefever (>38.0oC), chills, or hypotensionLCBI 3 A patient < 1 year of age have at least onefever (>38.0oC), apnea hypothermia, bradycardia
:
AND

28
Mrs. Jones
Mrs. Jones was admitted to the Oncology ward on Jan 1 and a central line was placed for enteral nutrition.
Jan 2 She developed a fever (102.F) Blood cultures were collected on
Jan 4th which grew CNS. Repeat blood cultures collected on
Jan 5th grew S. epidermidis. No other source of infection was
identified.
Hosp day / date
First Diagnostic
Test IWP DOE RIT
Fe
BC + CNS
BC+ S. epiNo o
of
POADOE
BC CNS
Notes
1-Jan Adm 4W
2-Jan ver 102⁰F
3-Jan
4-Jan
5-Janther source infection
6-Jan
7-Jan
8-Jan
9-Jan
10-Jan
11-Jan
12-Jan
13-Jan
14-Jan
15-Jan
16-Jan
17-Jan
18-Jan
19-Jan

• 2 mo. old Baby Grace was admitted on Jan 1st
• Afebrile with no symptoms of an infection. • On Jan 2nd she developed a fever and periods
of apnea, 2 sets of blood culture were collected.
• One specimen grew S. epidermidis.
Baby Grace does not meet either LCBI 2 or LCBI 3 criteria
POA LCBI 2 or 3 using fever or LCBI 3 using apnea
Baby Grace Scenario

Baby Boy Ben Scenario
Baby boy Ben was admitted to NICU on 1/15 after being born 1 mo. premature. On 1/18 he had new onset bradycardia. A central line was placed.1-19 He developed a low grade fever of 100⁰F and 2 sets of blood cultures were drawn separately both growing S. capitis. No other source of infection identified.

Baby Boy Ben Scenario
A
C
Bradyca S.
HAI
meets HAI LCBI Crite
Hosp day / date
First Diagnostic test IWP DOE RIT Notes
1/15/2017 dmit NICU
1/16/20171/17/2017 L placed
1/18/2017 rdia Fever 100F1/19/2017 BC capitis x 21/20/20171/21/2017
1/22/20171/23/2017
1/24/2017
1/25/2017
1/26/2017
1/27/2017
1/28/2017
1/29/2017
1/30/2017
1/31/2017
2/1/2017
2/2/2017
Yes, Baby Boy Ben rion 3, w/ S. capitis, DOE 1/18, not associated with the central line, attributed to NICU

32
Mucosal Barrier Injury-LCBI (MBI-LCBI)

Mucosal Barrier Injury - LCBI Criterion 1
Patient of any age meets criterion 1 for LCBI with at least one blood specimen identified by a culture or non-culture based microbiologic testing method, with ONLY intestinal organisms from the MBI Organism List AND Patient meets at least one of the following:1. Is an allogeneic hematopoietic stem cell transplant recipient within the past year with
one of the following documented during same hospitalization as positive blood culture:a. Grade III or IV gastrointestinal graft versus host disease (GI GVHD)b. ≥1 liter diarrhea in a 24 hour period (or ≥20 mL/kg in a 24 hour period for patients
<18 years of age) with onset on or within 7 calendar days before the date the positive blood culture is collected.
2. Is neutropenic, defined as at least 2 separate days with values of absolute neutrophil count (ANC) or total white blood cell count (WBC) <500 cells/mm3 within a 7 day period which includes the date the positive blood culture was collected (Day 1), the 3 calendar days before and the 3 calendar days after.

34
MBI-LCBI Neutropenia Criteria
Qualifying ANC/WBC timeframe (7 days) includes the Day of the + blood specimen, 3 days before and 3 days after

35
Example: Edith Parker
• Sept 3rd Edith Parker had a central line inserted on admission
• Sept. 6th she had an ANC level of 320 cells/mmᶾ
• Sept 7th two BC’s drawn + E. coli. • Sept 9th WBC level 410 cells/mmᶾ• No other source of infection was
identified.

36
Hosp day / date
First Diagnostic
test IWP DOE RIT Notes
9/3/2017Admit, CL placed
9/4/2017
9/5/20179/6/2017 ANC 320
9/7/2017BC x 2E. coli
no other source of infection
9/8/20179/9/2017 WBC 4109/10/20179/11/20179/12/20179/13/20179/14/20179/15/20179/16/20179/17/20179/18/20179/19/20179/20/2017
Edith Parker
Edith has an HAI CLABSI MBI-LCBI Criterion 1:2
(neutropenia) with E. coli on 9/7
Hosp day / date
First Diagnostic
test IWP DOE RIT Notes
9/3/2017Admit, CL placed
9/4/2017
9/5/20179/6/2017 ANC 320
9/7/2017BC x 2E. coli DOE = HAI
no other source of infection
9/8/20179/9/2017 WBC 4109/10/20179/11/20179/12/20179/13/20179/14/20179/15/20179/16/20179/17/20179/18/20179/19/20179/20/2017

Mucosal Barrier Injury - LCBI 2 & 3
with at least two blood specimens identified by a culture or non-culture based microbiologic testing method, with ONLY viridans group strep and no other organisms AND Patient meets at least one of the following:1. Is an allogeneic hematopoietic stem cell transplant recipient within the past year with one of the following documented during same hospitalization as positive blood culture:
a. Grade III or IV gastrointestinal graft versus host disease (GI GVHD)b. ≥1 liter diarrhea in a 24 hour period (or ≥20 mL/kg in a 24 hour period for
patients <18 years of age) with onset on or within 7 calendar days before the date the positive blood culture is collected.
2. Is neutropenic, defined as at least 2 separate days with values of absolute neutrophil count (ANC) or total white blood cell count (WBC) <500 cells/mm3 within a 7 day period which includes the date the positive blood culture was collected (Day 1), the 3 calendar days before and the 3 calendar days after.
Any age - fever, hypotension, chills < 1 yr - fever, hypothermia, apnea, bradycardia
MBI-LCBI 2 Patient of any age meets criterion 2 for LCBI MBI-LCBI 3 Patient < 1 year of age meets criterion 3 for LCBI

38
MBI-LCBI Criteria- Examples
Day # -7 -6 -5 -4 -3 -2 -1 1 2 3 4
ANC Not tested
410 130 Not tested
Not tested
120 110 Not tested;+ BC* w/viridansgroup strep X2 and fever 38.1°C
110 300 320
MBI-LCBI 2

39
Example: MBI-LCBI 1
HAI CLABSI MBI-LCBI 1 w/ Neutropenia
DOE= 2/13E. faecium
2/18 Must edit 2/13 MBI-LCBI to LCBI 1
and add S. aureus
Hosp day / date
First Diagnostic
test IWP DOE RIT Notes
2/10/2017 Admit-CL placed
2/11/2017
2/12/2017 ANC 300
2/13/2017
BC+ E. faecium, S. epi x 1
IWP=2/10 –2/16
DOE= 2/13HAI
RIT 2/13 – 2/26
2/14/2017
2/15/2017 ANC 210
2/16/2017
2/17/2017
2/18/2017 BC+S. aureus
2/19/2017
2/20/2017
2/21/2017
2/22/2017
2/23/2017
2/24/2017
2/25/2017
2/26/2017
2/27/2017
S. aureus not an
MBI

40
Mrs. Jones
12/20 Ms. Jones who is S/P allogeneic SCT 3 mos. ago was admitted to 4E with diarrhea (>1L in 24hrs) & abdominal pain. 12/21 She had a CL placed12/23 She became hypotensive and BC’s x 2 were collected, both grew VGS.

41
Example: Mrs. Jones Hosp day / date
First Diagnost i
c test IWP DOE RIT Notes
12/20/2016 Admit
Diarrhea > 1L/24hrs, abd pain
12/21/2016 CL placed
12/22/2016
12/23/2016BC+VGS X 2 BC x 2 VGS,
hypotension
12/24/2016
no other source of infection
12/25/2016
12/26/2016
12/27/201612/28/201612/29/201612/30/201612/31/2016
1/1/20171/2/20171/3/20171/4/20171/5/2017
Mrs. Jones meets HAI CLABSI MBI-LCBI 2-b
Allogeneic SCT w/ diarrhea
DOE 12/23 Viridans Group Strep
DOE= HAI
RITIWP√
42
Diarrhea must occur within the IWP to meet MBI-LCBI 1, 2 or 3 criteria?
a. Trueb. False
False: > 1 L diarrhea in 24 hrs. with onset on or within 7 calendar days before the date of the + blood specimen

43
Identifying BSI Events

44
Mrs. Kennedy
Feb 5th Mrs. Kennedy was discharged from the ED with antibiotics for an infected wound. Feb 10th She returns to ED with fever, generalized pain, nausea and hypotension. A central line is inserted and blood cultures are drawn, which are negative. She is admitted to ICU. Feb 13th repeat blood cultures grow E. coli.*No other source of infection identified

45
Case Determinat ion for Kennedy
a. HAI LCBI 1, E. coli that is CL associated, attributed to ICU
b. POA LCBI 1, E. coli that is not central line associated, attributed to ED
c. HAI LCBI 2, E. coli that is central line associated, attributed to ED
d. POA LCBI 2, E. coli that is not central line associated, attributed to ICU
.Feb 10th admitted-CL placed, fever, pain, nausea, hypotensionFeb 13th BC + E.coli

46
Mrs. Kennedy RationaleHosp day / date
First Diagnostic
test IWP DOE RIT Notes
2/7
2/8
2/9
2/10
Admit to ICU w/ CL. BC neg, fever, pain,
hypotension
2/11
2/12
2/13 BC+ E.coli
2/14
2/15
2/16
2/17
2/18
2/19
2/20
2/21
2/22
2/23
2/24
2/25
2/26
BC +E. coli
Day 4-HAI
Fever, Hypoten
sion
RIT
1. First diagnostic test 2/132. IWP 2/10-2/16. 3. E.coli is a recognized
pathogen 4. DOE 2/135. POA or HAI? Day 4=HAI6. RIT 2/13-26

Mrs. Kennedy cont.
On February 20th, a repeat blood culture is
collected and is growing S. aureus. No
other source of infection is identified.
Hosp day / date
First Diagnostic
test IWP DOE RIT Notes2/7
2/8
2/9
2/10
Admit to ICU w/ CL. BC neg, fever, pain,
hypotension2/11
2/12
2/13 BC+ E.coli HAI LCBI 1 BC+ E.coli
2/14
2/15
2/16
2/17
2/18
2/19
2/20
BC + S. aureus
No other source of infection
2/21
2/22
2/23
2/24
2/25
2/26
S. Aureus added to CLABSI with DOE 2/13 with
E.coli

48
Mrs. Fitzgerald
April 6: Mrs. F., who is 50, has been in your oncology ICU for a week with a central line which has been in use since admission. 4 months ago she received an allogeneic stem cell transplant for acute myeloid leukemia. Her central line is discontinued today. WBCs= 100 cells/mm3.
April 7: She becomes disoriented and hypotensive. Blood cultures x 2 and urine cultures are collected.
1 blood culture is positive for Streptococcus mutans and the other is reported as Enterococcus faecium. Urine culture is negative.
Yes, This is a primary BSI that is healthcare associated
49
Which Criteria?
a. MBI-LCBI 1b. MBI-LCBI 2c. LCBI 1d. LCBI 2
One or more blood cultures with a recognized pathogen Enterococcus faecium. Not an MBI-LCBI with only one qualifying WBC –neutropenia not demonstrated.
The single S. mutans, is a CC that is a contaminant

50
Mrs. Fitzgerald Variat ion
Would the case determination change if Grade III GI-GVHD was documented during the Mrs. Kennedy’s admission?
Case: April 6th: Allogeneic-SCT 4 mo. Ago. Admit to ICU with a CL in use for a week CL was removed. On April 7: patient became hypotensive; BC x 2 and urine cultures;
1 BC+ Strep mutans and 1 BC+ Enterococcus faecium.
HAI LCBI Criterion 1, E. faecium, CL associated, attributed to ICU

51
Mr. Morgan 8/11: Mr. Morgan presented to the ED on for pelvic fracture after a slip and
fall while playing in the Alumni Basketball Games :
8/11: Admitted to Trauma ICU. CL inserted and IV fluids began. Foley catheter inserted.
8/12: To OR for closed reduction and traction placement. Returned to Trauma ICU postoperatively.
8/13: Temp 38.5° C.
8/14: Trauma unit. Temp 38.5° C. 1 set blood culture collected - + S. epidermidis.
8/15: Trauma unit. Temp 37.9° C. 1 set of blood cultures collected - + S. epidermidis.

52
Is the S. epidermidis a contaminant in this case?a. Yesb. No
No, by requiring 2 matching common commensals from 2 separate blood draws using 2 decontamination steps, the likelihood of getting 2 specimens with a true contaminant is greatly diminished.

53
What is the Determinat ion in this Scenario?
a. This is a POA BSI
b. This is an HAI BSI
c. This is not a BSI
d. I don’t know
8/11 Admitted TICU, CL & Foley inserted, 8/12 to OR, 8/13 Fever 38.5C 8/14 Fever 38.5C BC S. epi 8/15 Fever 37.9C BC S. epi
54
Which BSI Criteria & Device Associat ion are Met?
a. LCBI 1, CL associatedb. LCBI 2, not CL associatedc. LCBI 2, CL associatedd. LCBI 3, not CL associated

55
Mrs. Morgan Rationale
HAI CLABSI LCBI 2
DOE = 8/13, Fever
Hosp day / date
First Diagnostic
test IWP DOE RIT Notes
8/11/2016 IWP=Admit ED / TICU
CL placed
8/12/20168/11-8/17
8/13/2016DOE= HAI
RIT=8/13-8/26 Tmax = 38.5
8/14/2016BC+S. epi x
1 Tmax = 38.5
8/15/2016BC+S. epi x
1 Tmax = 37.9
8/16/2016
8/17/2016
8/18/2016
8/19/2016
8/20/2016
8/21/2016
8/22/2016
8/23/2016
8/24/2016
8/25/2016
8/26/2016
8/27/2016

56
Lit t le Johnny Example
Little Johnny, who is 10 years old, has been in PICU for a week with a new diagnosis of leukemia. He’s had a central line in use for TPN since admission. He currently weighs 25kg.
April 4: ANC 325 April 6: Pt became hypotensive & new onset confusion- pulled the CL out April 7: Blood cultures x 2 and urine cultures are collected. April 8: ANC 485 1 blood culture is positive for Streptococcus mutans which is a Viridans group strep from
the MBI organism list and the other is Viridans Group Strep. Not related to an infection at another site.
Yes

57
Lit t le Johnny RationaleHosp day /
date
First Diagnostic
test IWP DOE RIT Notes
4/2/2017CL since
adm, PICU4/3/20174/4/2017 ANC 3254/5/2017
4/6/2017 Hypotension
4/7/2017
BC+ x S. mutans BC+VGS
4/8/2017 WBC 4854/9/20174/10/20174/11/20174/12/20174/13/20174/14/20174/15/20174/16/20174/17/20174/18/20174/19/20174/20/2017
+ BC S. mutans +BC VGS
IWP 4/4 –4/10
DOE-HAI
RIT 4/6 – 4/19
HAI MBI-LCBI Criterion 2

58
Little Johnny VariationWhat if a subsequent BC is collected within the RIT growingS. aureus that is not related to an infection at another site?
a. Don’t report another BSI. Just add S. aureus to the original MBI-LCBI.
b. Change the original MBI-LCBI to an LCBI 2 , adding S. aureus.
c. Report a second CLABSI. d. Change the original MBI-LCBI
to LCBI 1 and add the S. aureus as pathogen #1.

59
Little Johnny-Rationale
The subsequent blood culture falls within the RIT of the primary MBI-LCBI 2 event but the pathogen is a non-MBI organism therefore, MBI-LCBI criteria is no longer met. The original event must be edited to an LCBI 1 with S. aureus added as pathogen #1.
Hosp day / date
First Diagnostic
test IWP DOE RIT Notes
2/5/2017
2/6/2017
2/7/2017
2/8/2017
2/9/2017
2/10/2017 BC+ E. coli
no other source of infection
2/11/2017
2/12/2017
2/13/2017
2/14/2017
2/15/2017
2/16/2017
2/17/2017
2/18/2017
2/19/2017
2/20/2017
2/21/2017
2/22/2017
2/23/2017
Hosp day / date
First Diagnostic
test IWP DOE RIT Notes
2/5/2017 Admit, CL
2/6/2017
2/7/2017
2/8/2017
2/9/2017
2/10/2017
BC+ S. mutans BC+ VGS
IWPDOE-HAI RIT
2/11/2017
2/12/2017
2/13/2017
2/14/2017
2/15/2017
2/16/2017
2/17/2017
BC+ S. aureus
2/18/2017
2/19/2017
2/20/2017
2/21/2017
2/22/2017
2/23/2017

60
CLABSI Data Accuracy
The accuracy of NHSN data is dependent on the accuracy of surveillance determinations, data collection and entry– Accurate numerators
• Strict Adherence to the Definitions & Reporting Instructions
– Accurate denominators• Mapping Accuracy (see NHSN online training)• Collection Accuracy
• Specific Requirements by Location Type• Validation of Electronic Collection

61
BSI Event Data Collect ion Form
http://www.cdc.gov/nhsn/forms/57.108_PrimaryBSI_BLANK.pdf

62
Denominator Requirements by Location & DeviceLocation All
LocationsSCA-Oncology, dialysis NICU
All pts with > 1 CL = 1 CL Day
CL Days CL Days by:PermanentTemporary
If both a permanent & a temporary line
present- report temporary
CL Days by: Central line
Umbilical line
All patients in an inpatient
location = 1 Pt Day
All In-Pt Days
All In-Pt Days All In-Pt Days by:Birth Weight
< 750gms751-1000gms
1001-1500gms1501-2500gms
>2501gms

63
Check Your Denominator Data Ensure your denominator data is correct. Examples of potential problems:
– Counting a patient with 2 CLs as 2 rather than 1 CL day– Electronic data import happening twice a day rather than once
CL days 3000
CL days 5400

64
Collecting Denominator & Entering Summary Data for ICU/Wards
For all locations, count at the same t ime each dayNumber of patients on the unitNumber of patients with a central line

65
Collecting Denominator & Entering Summary Data for SCA Oncology
Central Lines strat ified by Device TypeNumber of patients on the unit
Number of patients with a permanent central lineNumber of patients with a Temporary central line
For patients with both a temporary & permanent line: count as Temporary

66
Collecting Denominator & Entering Summary Data for NICU
Patient Days & CL strat ified by Birth Weight# of patients on the unit by birth weight:
# of patients with a central line by birth weight:< 750gms
751-1000gms1001-1500gms1501-2500gms
>2501gms

67
Electronic Collection of Summary Data
Electronic capture of summary data is acceptable:
Following validation of the electronic method against the manual method
3 months concurrent data collection with both methods
Difference between methods must be within +/- 5% of each other
If difference > 5 % address issues, and revalidate for 3 months; repeat cycle until difference ≤5%

68
Once Weekly Denominator Collection
Reduces NHSN Data Collection Burden
Eligible ICU and ward location types may use– Must have 75 or more CL days per month
Patient days – Collected daily
– Recorded both:
• Total of weekly samples (e.g., every Tuesday)
• Monthly total (every day in month)
Central line days – Collected on a single day, once a week e.g. Every
Tuesday

69
Entering Summary Data (ICU/Wards)

70
In Summary
CLABSIs result in significant morbidity and mortality in U.S. hospitals.
– Much progress has been made but the journey continues
Clinical and surveillance definitions will sometimes differ– Intention is the same but the methods differ– Surveillance definitions must be adhered to strictly and
consistently
Located the protocols & training materials on NHSN.com Reviewed the forms & data collection & entry
requirements for BSI events Reviewed the 2017 Protocol with changes

71
Organism List Updated:“include but not limited to” added to list of exclusions which was expanded to include Campylobacter spp., C. difficile, Enteropathogenic E. coli. Shigella spp., Listeria spp., and Yersinia spp.Group B streptococcus will not be a CLABSI for first 6 days of lifeDefined Recognized pathogen-not on CC listAdded additional guidance for determining “matching” organisms
Clarified list off devices that are considered central lines:Femoral changed to ArterialImpella changed to Ventricular Assist Device
Defined “Access” & added examplePatient access clarified to accession to “Injection”
Deleted: “which is performed by culture or non-culture based microbiologic testing method which is performed for diagnostic or treatment”
Reporting Instructions:LCBI 1 & LCBI 2 simultaneously…Report LCBI 1 with pathogen then CCMBI-LCBI 1 added “only” intestinal organismsMBI-LCBI 2 clarified 2 culture requirement with VGSMBI-LCBI 1 & MBI-LCBI 2 simultaneously…Report organism as MBI-LCBI 1
2017 NHSN BSI Protocol Changes Summary

72
Resources for BSI Reporting CLABSI protocols, forms, etc:
– http://www.cdc.gov/nhsn/acute-care-hospital/clabsi/index.html– http://www.cdc.gov/nhsn/newsletters.html
Operational guidance for CMS reporting:– http://www.cdc.gov/nhsn/cms/index.html– http://www.cdc.gov/nhsn/acute-care-hospital/clabsi/index.html
Contact list for QIO/QINs: http://www.qualitynet.org/dcs/ContentServer?c=Page&pagename=QnetPublic%2FPage
%2FQnetTier2&cid=1144767874793
NHSN training:– http://www.cdc.gov/nhsn/training/– http://www.cdc.gov/nhsn/newsletters.html

American Journal of Infection ControlNHSN Case-Study Series Additional educational tool
• Perfect for reliability testing of ICP teams, APIC chapters, etc. Target: quarterly publication Address common surveillance scenarios
• CLABSI, CAUTI, VAE, SSI, MDRO/CDI Test your knowledge Quiz and answers via web link Pursuing other access opportunities