
CKD-RELATED ANEMIA KDIGO · Clinical Practice Guidelines on the Treatment of CKD-related Anemia...
67
CKD-RELATED ANEMIA CONCLUSION FROM KDIGO CONTROVERSIES CONFERENCE Dr. Gregorio T. Obrador Vera, M.P.H. Dean and Professor of Nephrology, Faculty of Health Sciences and School of Medicine, Universidad Panamericana (México, CDMX) Adjunct Assistant Professor of Medicine, Tufts University School of Medicine & Tufts Medical Center (Boston, MA) KDIGO
Transcript of CKD-RELATED ANEMIA KDIGO · Clinical Practice Guidelines on the Treatment of CKD-related Anemia...
CKD-RELATED ANEMIA CONCLUSION FROM KDIGO
CONTROVERSIES CONFERENCE Dr. Gregorio T. Obrador Vera, M.P.H.
Dean and Professor of Nephrology, Faculty of Health Sciences and School of Medicine, Universidad Panamericana (México, CDMX)
Adjunct Assistant Professor of Medicine, Tufts University School of Medicine & Tufts Medical Center (Boston, MA)
KDIGO
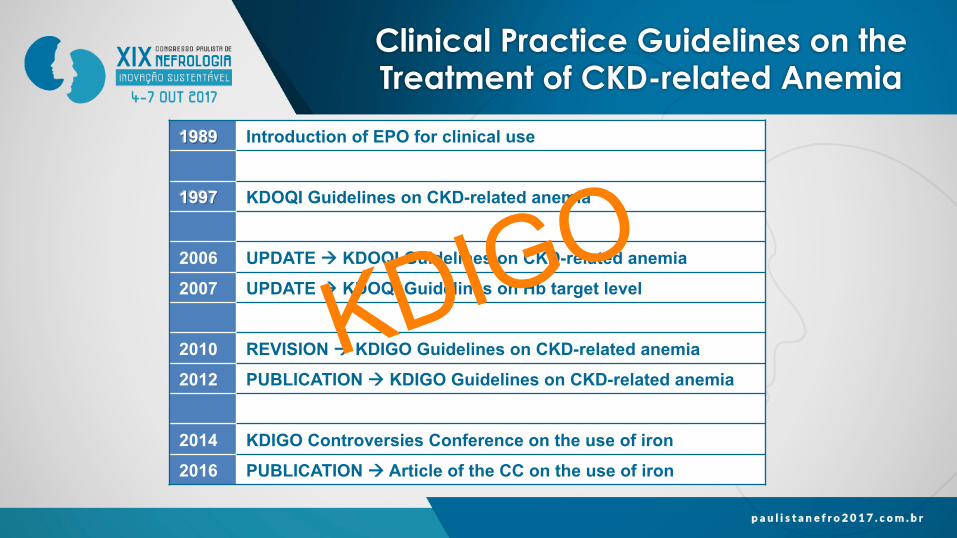
Clinical Practice Guidelines on the Treatment of CKD-related Anemia
1989 Introduction of EPO for clinical use
1997 KDOQI Guidelines on CKD-related anemia
2006 UPDATE à KDOQI Guidelines on CKD-related anemia
2007 UPDATE à KDOQI Guidelines on Hb target level
2010 REVISION à KDIGO Guidelines on CKD-related anemia
2012 PUBLICATION à KDIGO Guidelines on CKD-related anemia
2014 KDIGO Controversies Conference on the use of iron
2016 PUBLICATION à Article of the CC on the use of iron
KDIGO
KDIGO
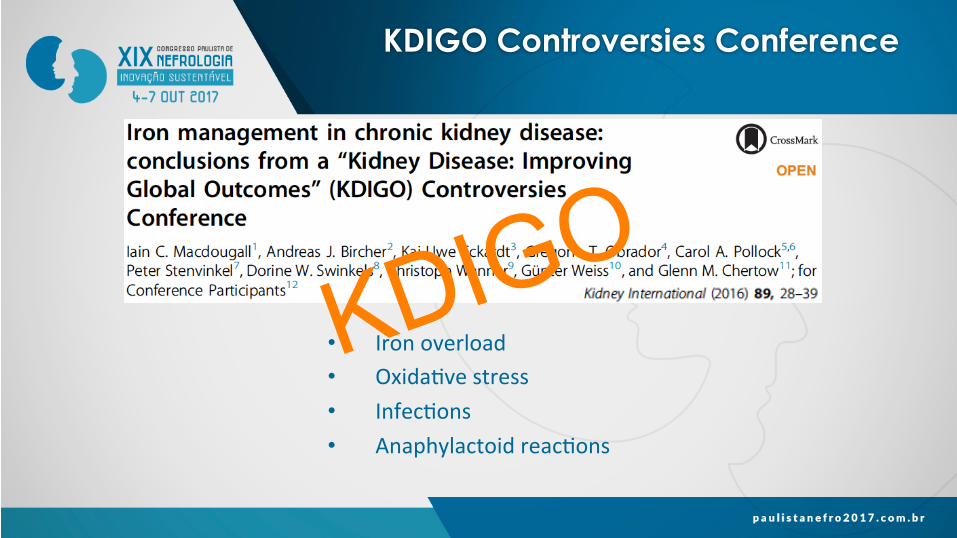
KDIGO Controversies Conference
• Ironoverload• Oxida.vestress• Infec.ons• Anaphylactoidreac.ons
KDIGO
2012 KDIGO Guidelines Anemia in CKD
ü Iden%fica%on,diagnosisandevalua%onofthecause
• RoleofirontotreatCKD-relatedanemia
• RoleofESAsandotherdrugstotreatCKD-relatedanemia
• RoleofbloodtransfusionstotreatCKD-relatedanemia
KDIGO
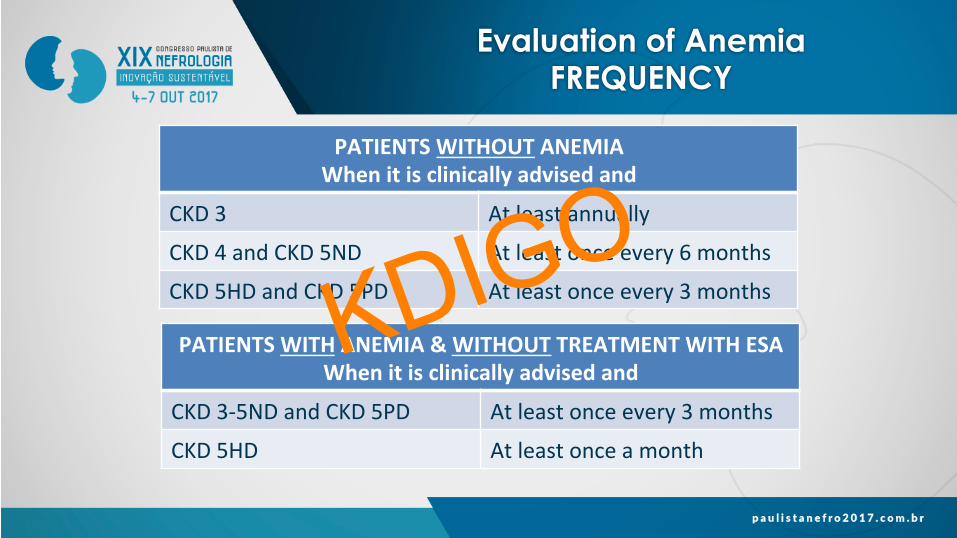
Evaluation of Anemia FREQUENCY
PATIENTSWITHOUTANEMIAWhenitisclinicallyadvisedand
CKD3 Atleastannually
CKD4andCKD5ND Atleastonceevery6months
CKD5HDandCKD5PD Atleastonceevery3months
PATIENTSWITHANEMIA&WITHOUTTREATMENTWITHESAWhenitisclinicallyadvisedand
CKD3-5NDandCKD5PD Atleastonceevery3months
CKD5HD Atleastonceamonth
KDIGO
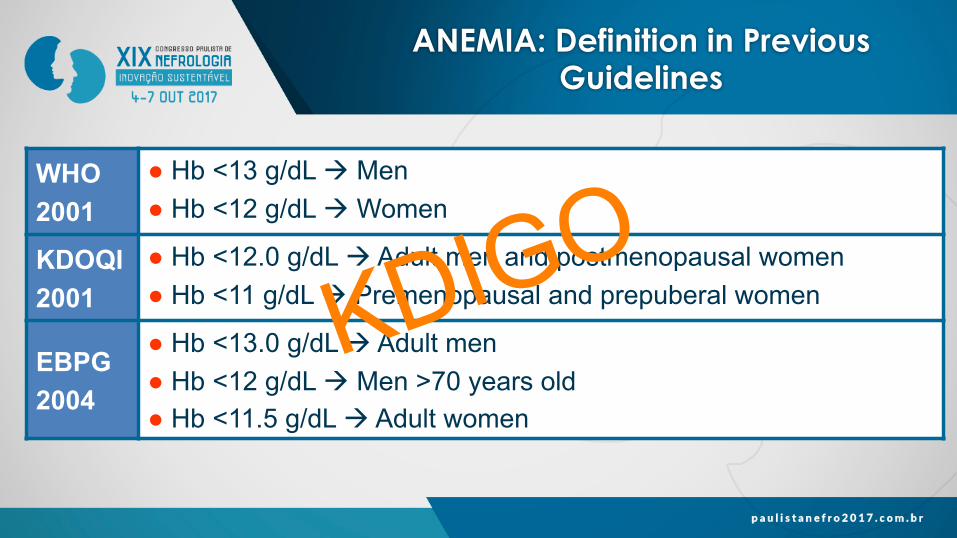
ANEMIA: Definition in Previous Guidelines
WHO 2001
● Hb <13 g/dL à Men ● Hb <12 g/dL à Women
KDOQI 2001
● Hb <12.0 g/dL à Adult men and postmenopausal women ● Hb <11 g/dL à Premenopausal and prepuberal women
EBPG 2004
● Hb <13.0 g/dL à Adult men ● Hb <12 g/dL à Men >70 years old ● Hb <11.5 g/dL à Adult women
KDIGO
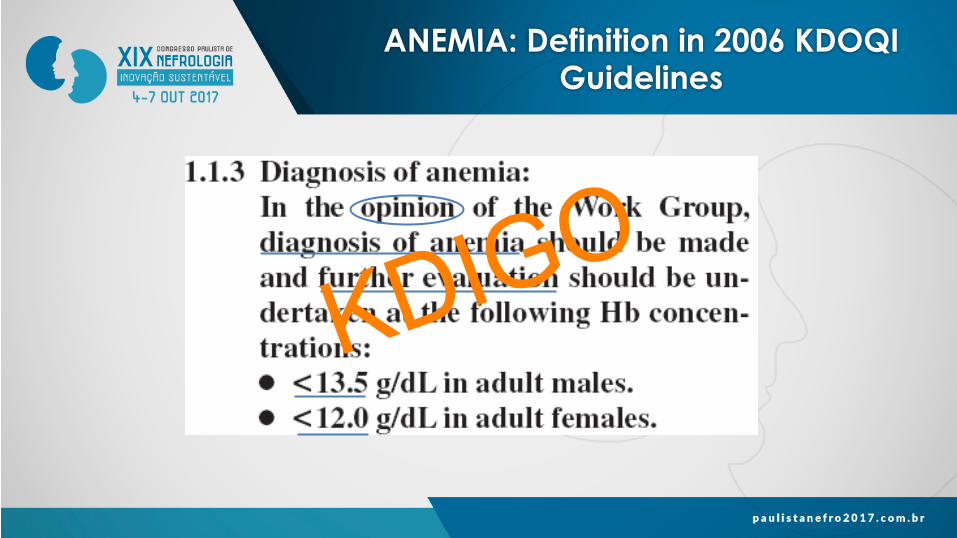
ANEMIA: Definition in 2006 KDOQI Guidelines
KDIGO
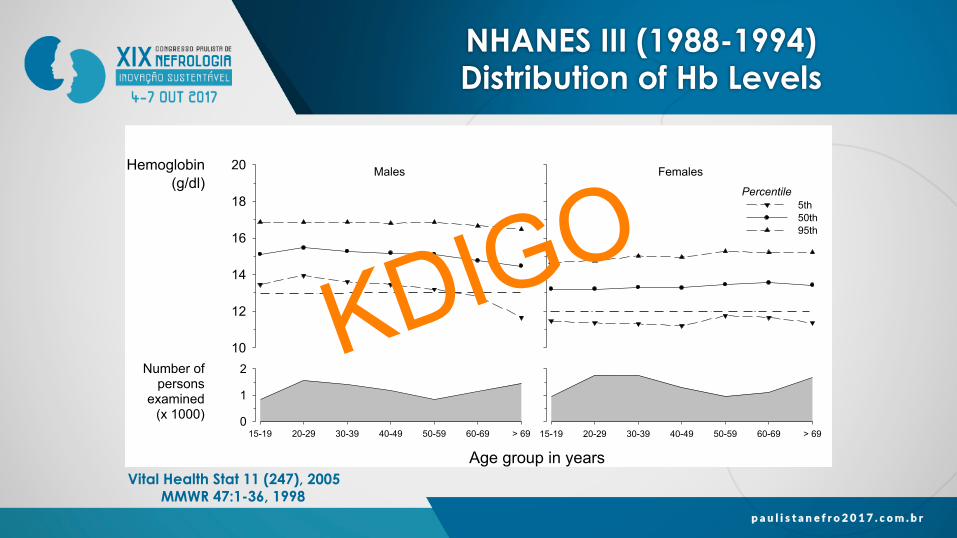
NHANES III (1988-1994) Distribution of Hb Levels
Hemoglobin(g/dl)
10
12
14
16
18
20
5th 50th 95th
15-19 20-29 30-39 40-49 50-59 60-69 > 69
Percentile
Females
Age group in years15-19 20-29 30-39 40-49 50-59 60-69 > 69
Number ofpersons
examined(x 1000) 0
1
2
Males
Vital Health Stat 11 (247), 2005 MMWR 47:1-36, 1998
KDIGO
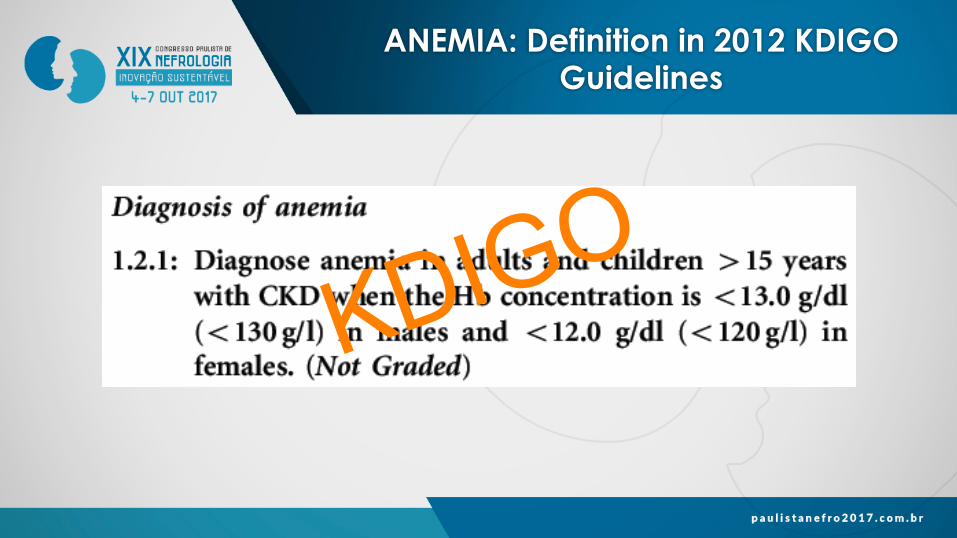
ANEMIA: Definition in 2012 KDIGO Guidelines
KDIGO
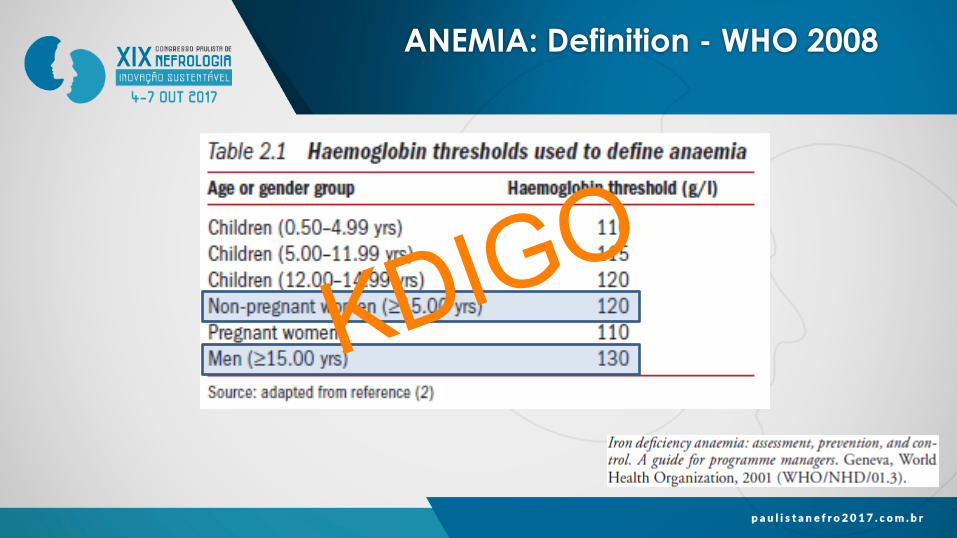
ANEMIA: Definition - WHO 2008
KDIGO
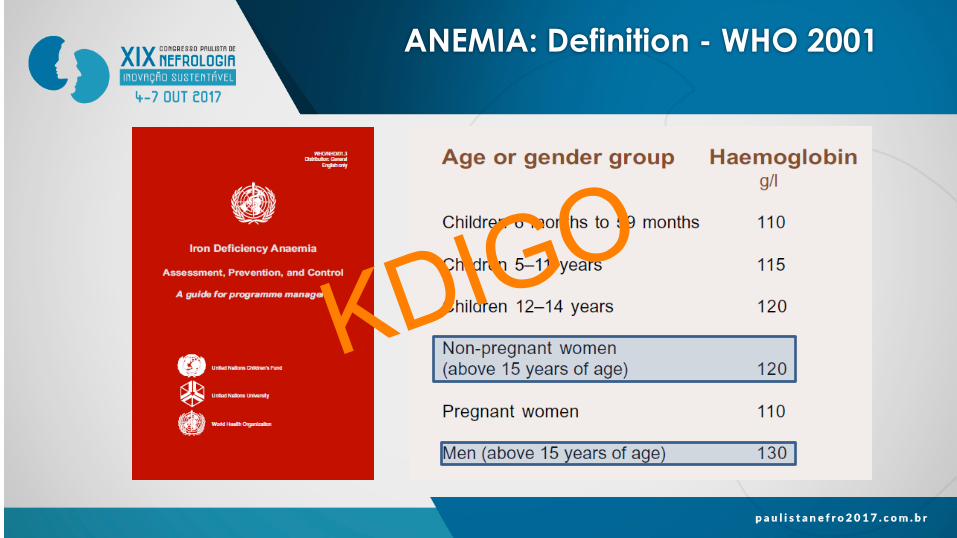
ANEMIA: Definition - WHO 2001
KDIGO
ANEMIA: Definition
KDIGO
ANEMIA: Definition Challenges
• WHO’sanemiadefini.onisques%onable;itcouldbeincludedasaresearchrecommenda.onintheguidelines
• IdeallyaHbdistribu%onshouldbeobtainedtodefineappropriatecut-offlevelsforeachpopula.on
• ItisnecessarytocorrecttheHblevelaccordingtoal%tude,smoking,andrace
KDIGO
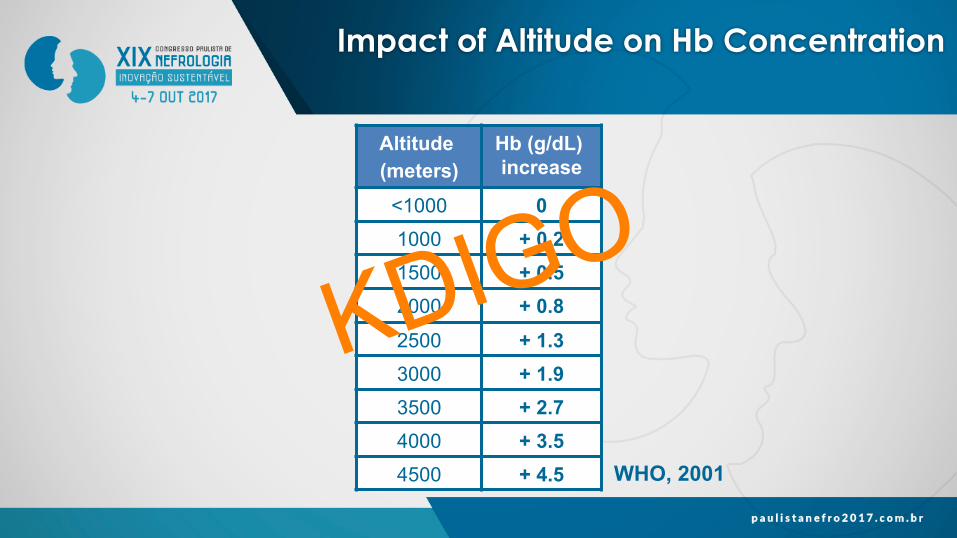
Impact of Altitude on Hb Concentration
Altitude (meters)
Hb (g/dL) increase
<1000 0 1000 + 0.2 1500 + 0.5 2000 + 0.8 2500 + 1.3 3000 + 1.9 3500 + 2.7 4000 + 3.5 4500 + 4.5 WHO, 2001
KDIGO
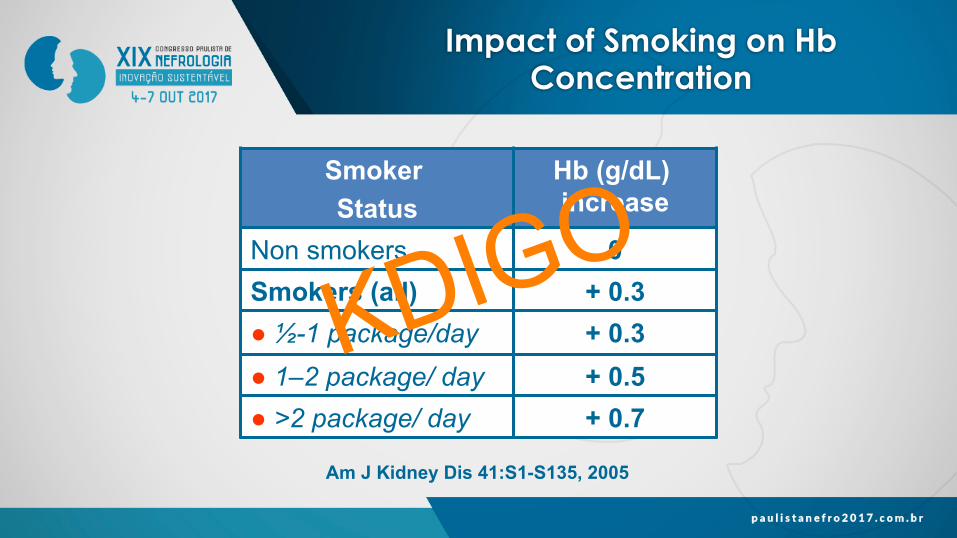
Impact of Smoking on Hb Concentration
Smoker Status
Hb (g/dL) increase
Non smokers 0 Smokers (all) + 0.3 ● ½-1 package/day + 0.3 ● 1–2 package/ day + 0.5 ● >2 package/ day + 0.7
Am J Kidney Dis 41:S1-S135, 2005
KDIGO
Impact of Race on Hb Concentration
• Hbconcetra.onlevelsvaryamongindividualsofdifferentraces
• African-AmericanindividualshaveHblevelsthatare0.5-0.9g/dllowerthanthoseofnonAfrican-Americanindividuals
• SincethecauseofthedifferenceinHblevelsamongracesisunknownandcouldreflectdifferentdegreesofcomorbidity,theguidelinedidnotincludespecificcut-offlevelsfordefininganemiaamongdifferentraces
KDIGO
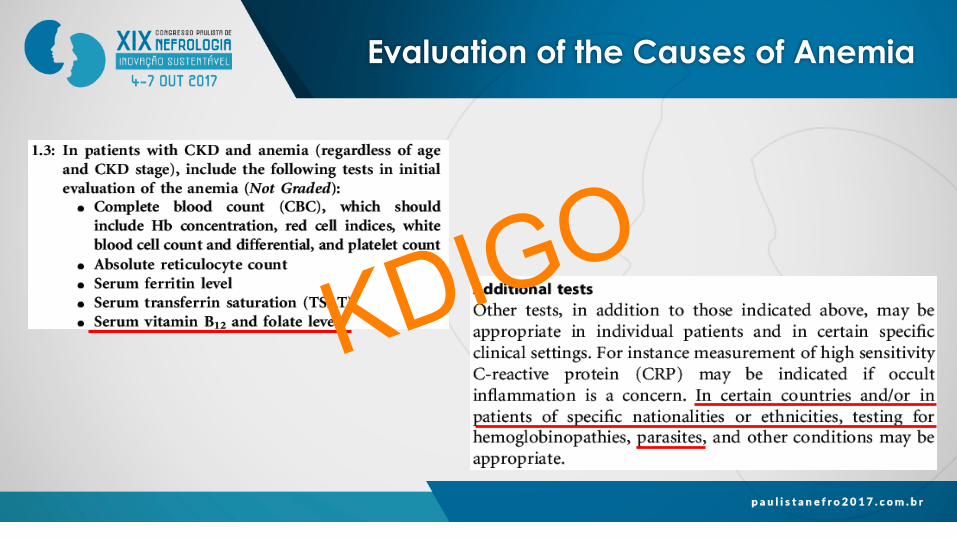
Evaluation of the Causes of Anemia
KDIGO
2012 KDIGO Guidelines Anemia in CKD
ü Iden%fica%on,diagnosisandevalua%onofthecause
ü RoleofirontotreatCKD-relatedanemia
• RoleofESAsandotherdrugstotreatCKD-relatedanemia
• RoleofbloodtransfusionstotreatCKD-relatedanemia
KDIGO
Treatment with Iron BENEFITS VS RISKS
Benefits Avoid or minimize • Transfusions • ESAs • Symptoms
Risks • Anaphylactoid and other acute reactions • Unknown long-term risks
KDIGO Guidelines 2012
KDIGO
Treatment with Iron OBJECTIVES AND INDICATIONS
IVIron(ororalironx1-3monthsifCKD-ND)
↑ Hb without initiating ESA, and TSAT ≤30% and ferritin ≤500 ng/ml (2C)
NoIronorESA IVIron(ororal
ironx1-3monthsifCKD-ND)↑Hbor↓doseofESA,andTSAT≤30%yferri.n≤500ng/ml(2C)
ESA
KDIGO Guidelines 2012
KDIGO
Treatment with Iron OBJECTIVES AND INDICATIONS
Ini%a%ngTreatmentTSAT ≤20%
SerumFerri%n
≤100 ng/ml in CKD-ND and CKD-5PD
≤200 ng/ml in CKD-5HD
Do not exceed 500 ng/ml
KDOQI Guidelines 2006
KDIGO
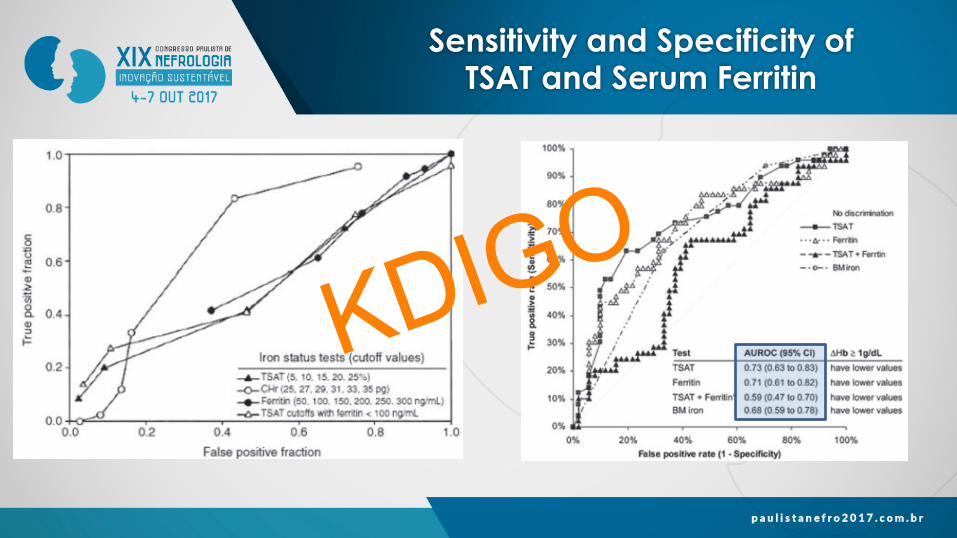
Sensitivity and Specificity of TSAT and Serum Ferritin
KDIGO
TSAT≤30%
• AlevelofTSAT<30%usuallyindicatesirondeficiency
• Pa.entswithanemiaandTSAT>20%tendtorespondtotreatmentwithironeitherbyincreasingtheHblevelorbydecreasingtheESAdose
• WithotherlevelsofTSAT,thesensi.vityandspecificityarelimitedtopredictirondeficiencyorHbincreasea`ertreatmentwithiron
Treatment with Iron OBJECTIVES AND INDICATIONS
KDIGO Guidelines 2012
KDIGO
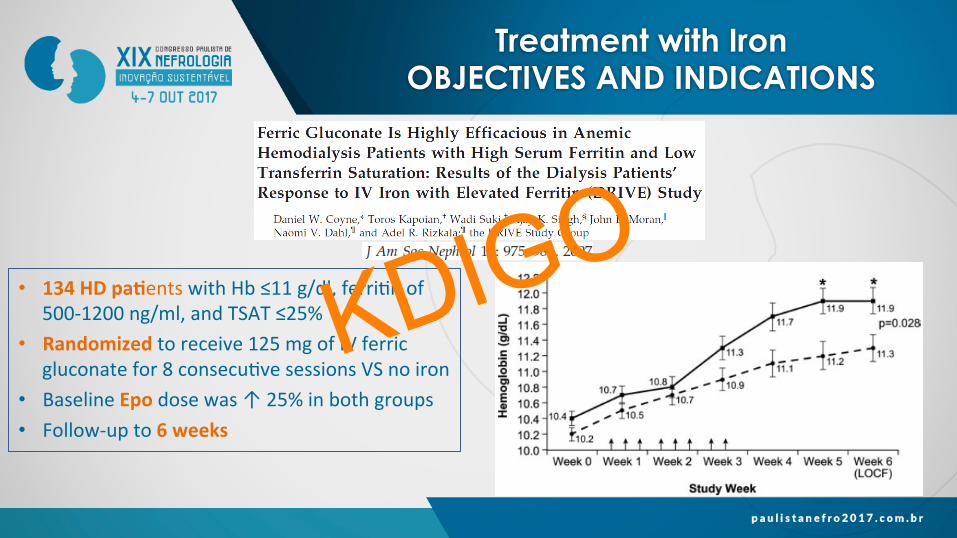
• 134HDpa%entswithHb≤11g/dl,ferri.nof500-1200ng/ml,andTSAT≤25%
• Randomizedtoreceive125mgofIVferricgluconatefor8consecu.vesessionsVSnoiron
• BaselineEpodosewas↑25%inbothgroups• Follow-upto6weeks
Treatment with Iron OBJECTIVES AND INDICATIONS
KDIGO
Treatment with Iron OBJECTIVES AND INDICATIONS
SerumFerri%n≤500ng/dl
• Althoughmostpa.entswithserumferri.n>100ng/dlhavenormalironstoresinthebonemarrow,theytendtorespondtotreatmentwithironbyincreasingtheHbconcentra.onordecreasingtheESAdose
• Thereisnotenoughevidencetodeterminethebenefitsandtherisksofadministeringaddi.onalirontopa.entswithserumferri.n>500ng/dlKDOQI2006andothersourcesrecommendNOTtoadministerirontopa.entswithserumferri.nlevelsbetween500-800ng/dl,becausetheincreaseinHblevelandthedecreaseinESAdoseislimitedandpoten.aladverseeffects
KDIGO Guidelines 2012
KDIGO
Treatment with Iron OBJECTIVES AND INDICATIONS
• ItdoesnotdefinethelowerlimitofTSATandofferri.ndue
toinsufficientevidence
• ItdefinestheupperlimitofTSATandferri.n
• Itemphasizestheimportanceofindividualizingtreatment
KDIGO Guidelines 2012
KDIGO
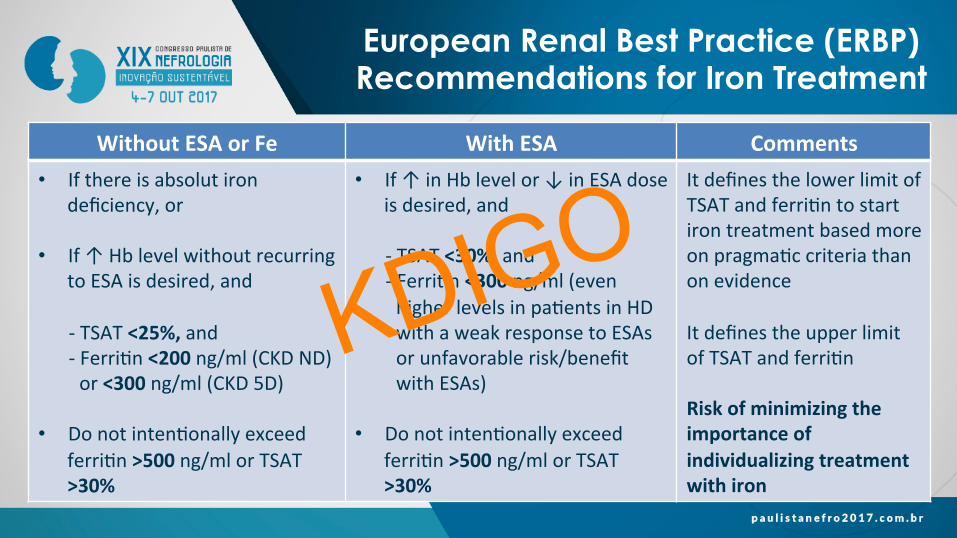
European Renal Best Practice (ERBP) Recommendations for Iron Treatment
WithoutESAorFe WithESA Comments• Ifthereisabsolutiron
deficiency,or
• If↑HblevelwithoutrecurringtoESAisdesired,and
-TSAT<25%,and-Ferri.n<200ng/ml(CKDND)or<300ng/ml(CKD5D)
• Donotinten.onallyexceedferri.n>500ng/mlorTSAT>30%
• If↑inHblevelor↓inESAdoseisdesired,and
-TSAT<30%,and-Ferri.n<300ng/ml(evenhigherlevelsinpa.entsinHDwithaweakresponsetoESAsorunfavorablerisk/benefitwithESAs)
• Donotinten.onallyexceedferri.n>500ng/mlorTSAT>30%
ItdefinesthelowerlimitofTSATandferri.ntostartirontreatmentbasedmoreonpragma.ccriteriathanonevidenceItdefinestheupperlimitofTSATandferri.nRiskofminimizingtheimportanceofindividualizingtreatmentwithiron
KDIGO
• Inpa.entswithCKD-ND,selecttherouteofadministra%onbasedon
• Severityofirondeficiency• IVaccessavailability• PreviousresponsetooralorIViron• Treatmentcompliance• Costs
Treatment with Iron ROUTE OF ADMINISTRATION
KDIGO Guidelines 2012
KDIGO
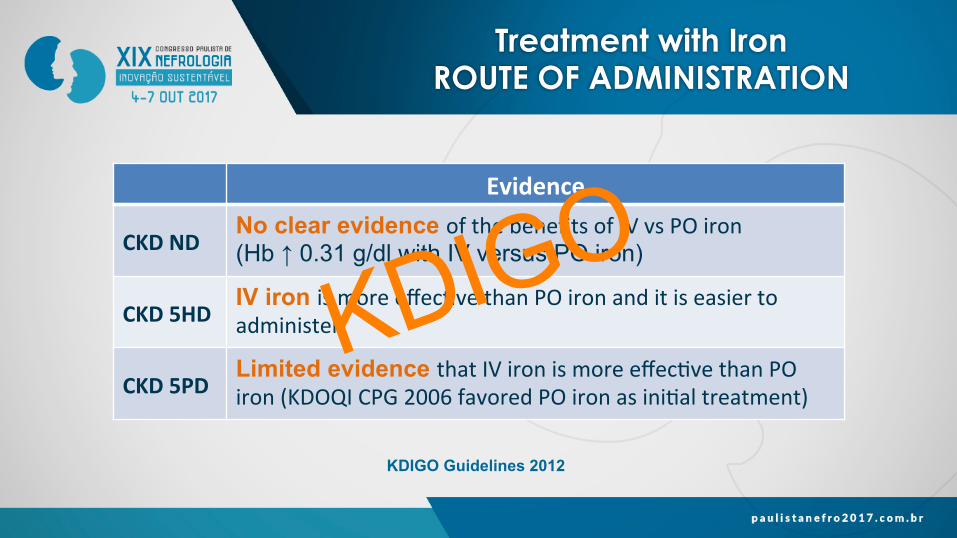
Treatment with Iron ROUTE OF ADMINISTRATION
Evidence
CKDNDNo clear evidence ofthebenefitsofIVvsPOiron(Hb ↑ 0.31 g/dl with IV versus PO iron)
CKD5HDIV iron ismoreeffec.vethanPOironanditiseasiertoadminister
CKD5PDLimited evidence thatIVironismoreeffec.vethanPOiron(KDOQICPG2006favoredPOironasini.altreatment)
KDIGO Guidelines 2012
KDIGO
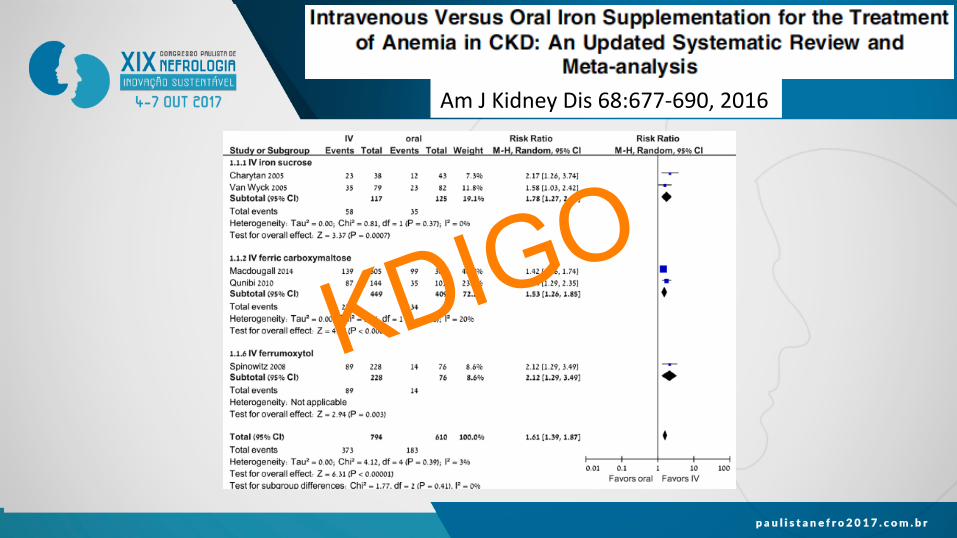
Treatment with Iron ROUTE OF ADMINISTRATION AmJKidneyDis68:677-690,2016
KDIGO
• Ini%alDose• Administeredasasingledoseorasrepeatlowerdosesthataddupto
1gram
• MaintenanceDose• Periodicdoseswhenneeded• Lowdosesatregularintervals
Treatment with Iron DOSAGE
KDIGO
KDIGO Controversies Conference
• Ironoverload• Oxida.vestress• Infec.ons• Anaphylactoidreac.ons
KDIGO
• Anelevatedleveloftotalbodyironcouldbeassociatedwithagreaterriskoforgandamageover.me
• Limleisknownaboutthecircumstancesinwhichtheexcessofironcausesdamagetotheorganswhereitaccumulatesandtheconsequencesoftheoverload
• Inpa.entswithCKD,organdysfunc.oncausedbyironoverloadisrare;however,itcouldtakelongertoaccumulateforbeingclinicallyrelevant
Iron Overload
KDIGO
• Administra.onofIVirontopa.entswithCKD• Oxida%vedamagetoDNAandperipheralbloodlymphocytes• Proteinoxida.onandlipidsperoxida.on• Celularapoptosis,endothelialdysfunc.on,andmonocyteadhesion
• Currentmethodstomeasureoxida.vestressandassessriskorprognosisareinconsistent
Oxidative Stress I
KDIGO
• Evidencethattheadministra.onofironpromotesatherosclerosisandvascularremodelingisalsoinconsistent
• Theeffectofan%oxidantsinpa.entswithCKDisunclear
Oxidative Stress II
KDIGO
• Ironisimportantfor• Prolifera.onandpathogenicityofmutlipleorganisms• Regual.onoftheimmuneresponse(i.e.,modulatescellprolifera.onanddiferen.a.on,cytokineproduc.on,andotherac.onsoftheimmunesystemagainstinfec.ons)
• Homeosta.cimbalanceofironcanaffectnotonlytheriskbutalsotheconsequencesofinfec.ons
Infections BASIC SCIENCE EVIDENCE
KDIGO
Clinicalevidenceisinsufficienttodetermineiftheadministra.onofironisassociatedwithanincreasedriskofinfec.on
• Mostoftheevidencederivesfromobserva.onalstudiesinHDpa.ents• Fewcontrolledclinicaltrialswithfewpa.entsandshortfollow-up• VerylimitedevidenceinpredialysisandPDpa.ents• Severalmeta-analysisandsystema.creviewshavebeeninconclusive
Infections CLINICAL EVIDENCE
KDIGO
Infections ELEMENTAL EVIDENCE
KDIGO
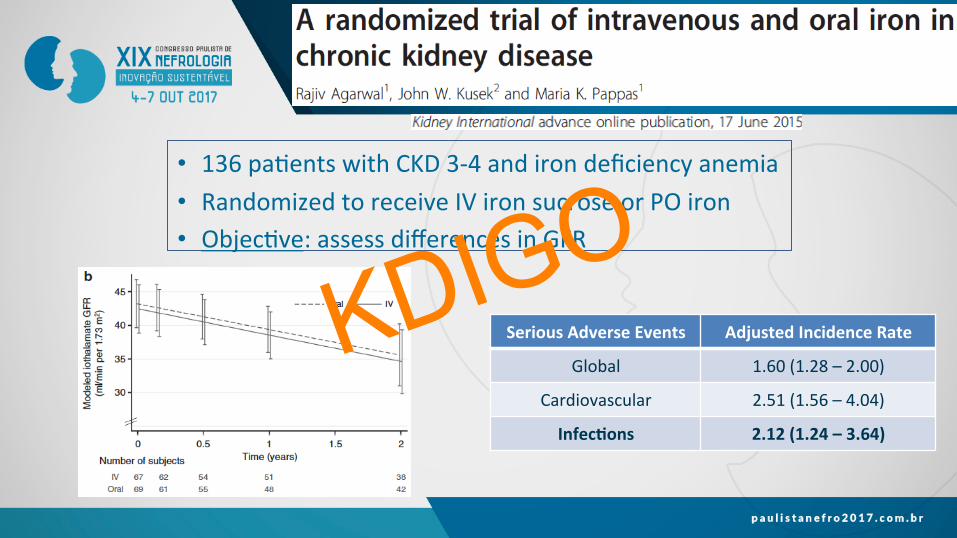
• 136pa.entswithCKD3-4andirondeficiencyanemia• RandomizedtoreceiveIVironsucroseorPOiron• Objec.ve:assessdifferencesinGFR
Infections CLINICAL EVIDENCE
SeriousAdverseEvents AdjustedIncidenceRate
Global 1.60(1.28–2.00)
Cardiovascular 2.51(1.56–4.04)
Infec%ons 2.12(1.24–3.64)
KDIGO
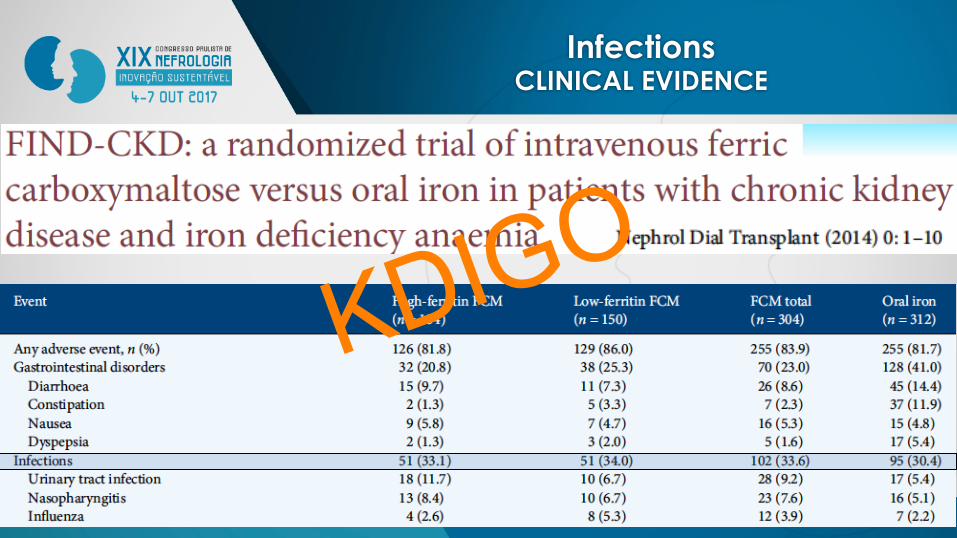
Infections CLINICAL EVIDENCE
KDIGO
• Therearesignificantmethodologicaldifferencesbetweenthetwostudes(REVOKEandFIND-CKD),sotheyarenotfullycomparable
• ThereisanurgentneedforacontrolledclinicaltrialtoassessthesafetyofthetreatmentwithIVironinpa.entswithCKD
• KDIGO’srecommenda.ontoavoiduseofIVironinthepresenceofsystemicbacterialinfec.onsisreasonable(NotGraded)
Infections
KDIGO
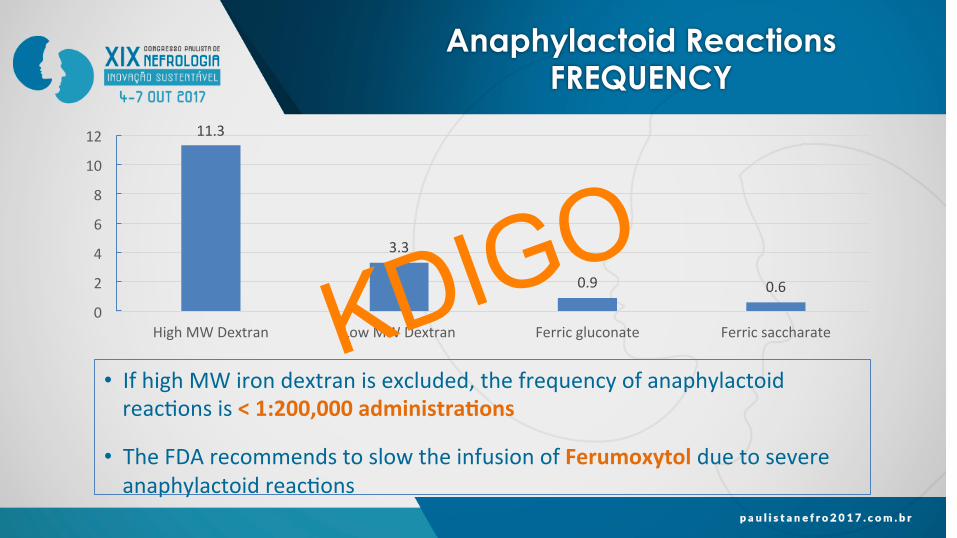
• IfhighMWirondextranisexcluded,thefrequencyofanaphylactoidreac.onsis<1:200,000administra%ons
• TheFDArecommendstoslowtheinfusionofFerumoxytolduetosevereanaphylactoidreac.ons
Anaphylactoid Reactions FREQUENCY
11.3
3.3
0.9 0.6
0
2
4
6
8
10
12
HighMWDextran LowMWDextran Ferricgluconate FerricsaccharateKDIGO
• Iftheini.aldoseofIVironisdextran(1B)ornotdextran(2C),werecommend/suggest
• Tomonitorthepa.entfor60minutesa`ertheinfusion• Havecardiopulmonaryresuscita%onequipmentathand
(includingdrugs)andtrainedpersonneltopoten.allytreatseriousadverseevents
KDIGO Recommendation
KDIGO Guidelines 2012
KDIGO
2012 KDIGO Guidelines Anemia in CKD
ü Iden%fica%on,diagnosisandevalua%onofthecause
ü RoleofirontotreatCKD-relatedanemia
ü RoleofESAsandotherdrugstotreatCKD-relatedanemia
• RoleofbloodtransfusionstotreatCKD-relatedanemia
KDIGO
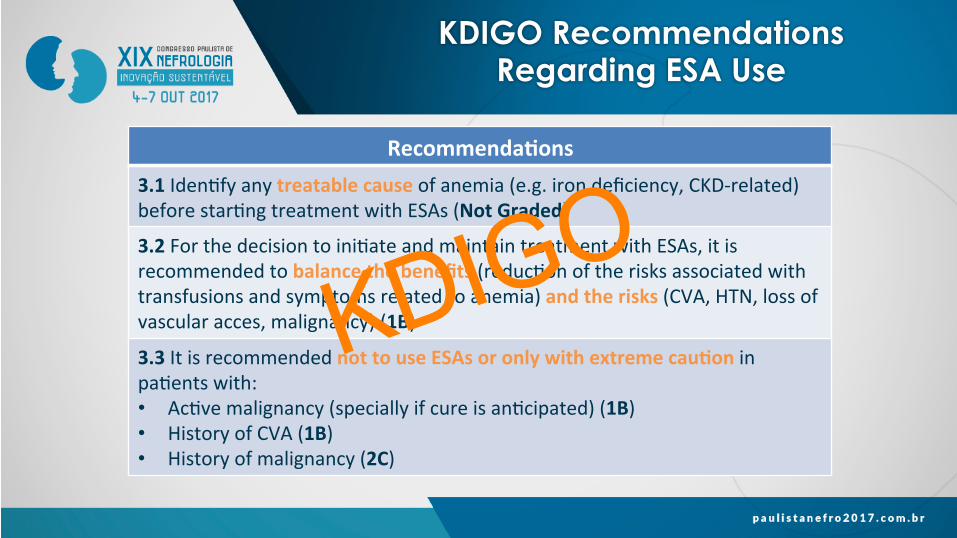
KDIGO Recommendations Regarding ESA Use
Recommenda%ons3.1Iden.fyanytreatablecauseofanemia(e.g.irondeficiency,CKD-related)beforestar.ngtreatmentwithESAs(NotGraded)
3.2Forthedecisiontoini.ateandmaintaintreatmentwithESAs,itisrecommendedtobalancethebenefits(reduc.onoftherisksassociatedwithtransfusionsandsymptomsrelatedtoanemia)andtherisks(CVA,HTN,lossofvascularacces,malignancy)(1B)
3.3ItisrecommendednottouseESAsoronlywithextremecau%oninpa.entswith:• Ac.vemalignancy(speciallyifcureisan.cipated)(1B)• HistoryofCVA(1B)• Historyofmalignancy(2C)
KDIGO
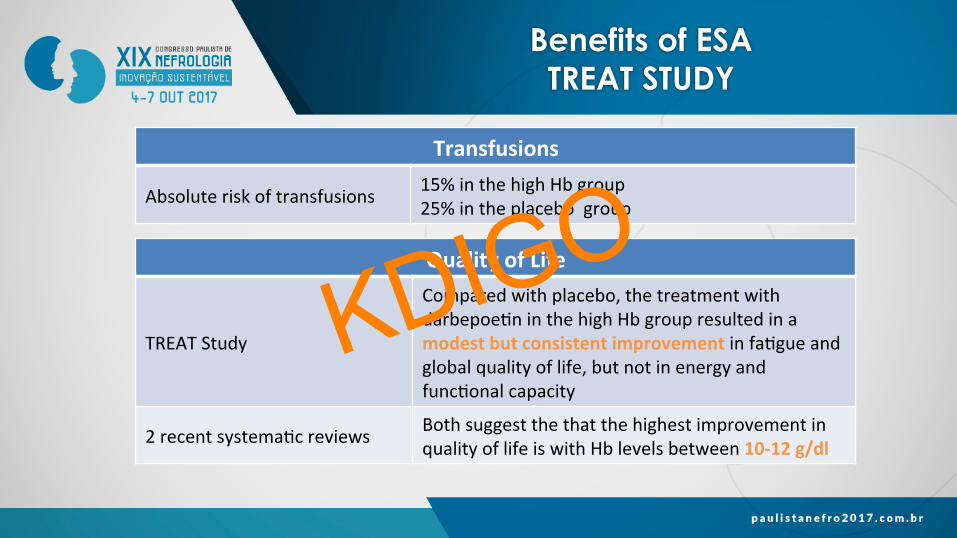
Benefits of ESA TREAT STUDY
Transfusions
Absoluteriskoftransfusions 15%inthehighHbgroup25%intheplacebogroup
QualityofLife
TREATStudy
Comparedwithplacebo,thetreatmentwithdarbepoe.ninthehighHbgroupresultedinamodestbutconsistentimprovementinfa.gueandglobalqualityoflife,butnotinenergyandfunc.onalcapacity
2recentsystema.creviews BothsuggestthethatthehighestimprovementinqualityoflifeiswithHblevelsbetween10-12g/dl
KDIGO
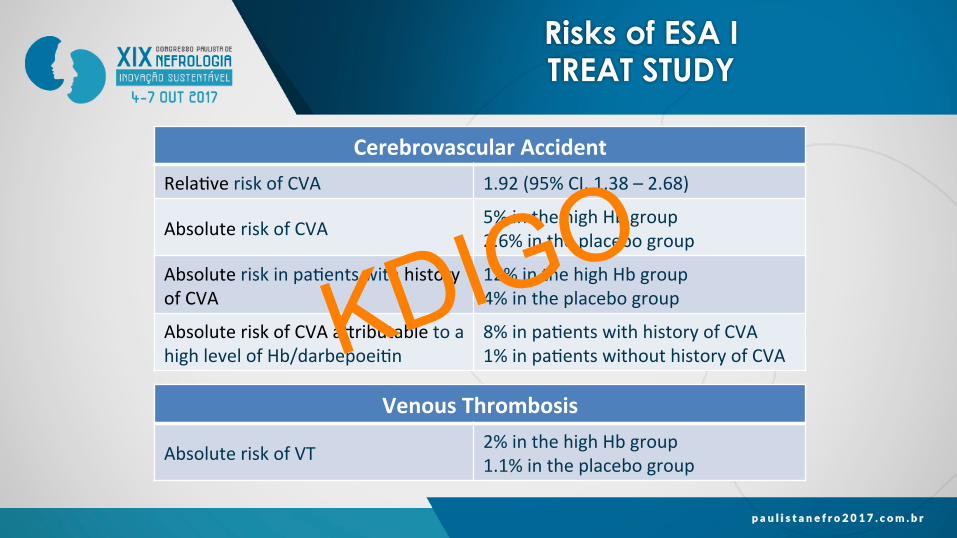
Risks of ESA I TREAT STUDY
CerebrovascularAccidentRela.veriskofCVA 1.92(95%CI,1.38–2.68)
AbsoluteriskofCVA 5%inthehighHbgroup2.6%intheplacebogroup
Absoluteriskinpa.entswithhistoryofCVA
12%inthehighHbgroup4%intheplacebogroup
AbsoluteriskofCVAamributabletoahighlevelofHb/darbepoei.n
8%inpa.entswithhistoryofCVA1%inpa.entswithouthistoryofCVA
VenousThrombosis
AbsoluteriskofVT 2%inthehighHbgroup1.1%intheplacebogroup
KDIGO
Risks of ESA II TREAT STUDY
MalignantNeoplasmInpa.entswithhistoryofmalignantneoplasmatthebegginingofthestudy
Mortalityof7.4%inthehighHbgroupMortalityof0.6%intheplacebogroupKDIGO
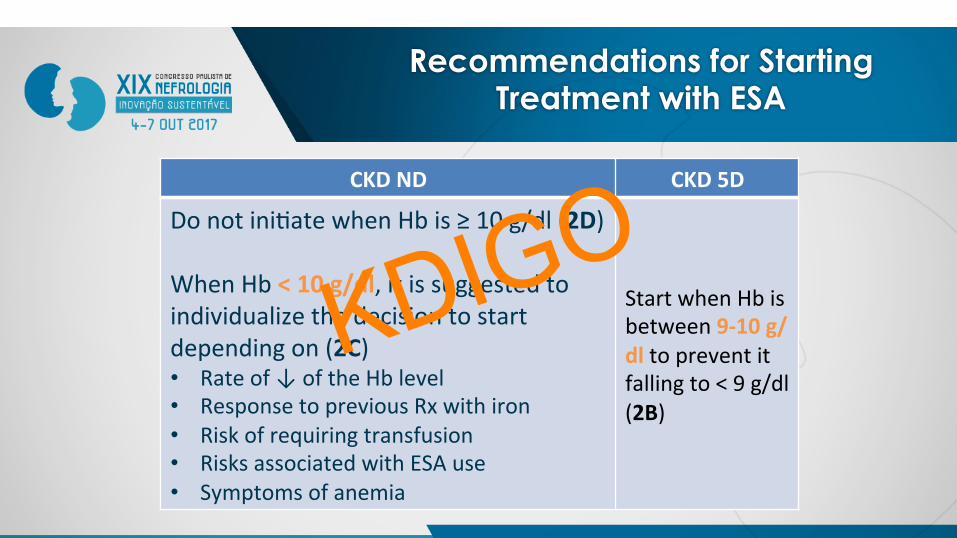
Recommendations for Starting Treatment with ESA
CKDND CKD5D
Donotini.atewhenHbis≥10g/dl(2D)WhenHb<10g/dl,itissuggestedtoindividualizethedecisiontostartdependingon(2C)• Rateof↓oftheHblevel• ResponsetopreviousRxwithiron• Riskofrequiringtransfusion• RisksassociatedwithESAuse• Symptomsofanemia
StartwhenHbisbetween9-10g/dltopreventitfallingto<9g/dl(2B)
KDIGO
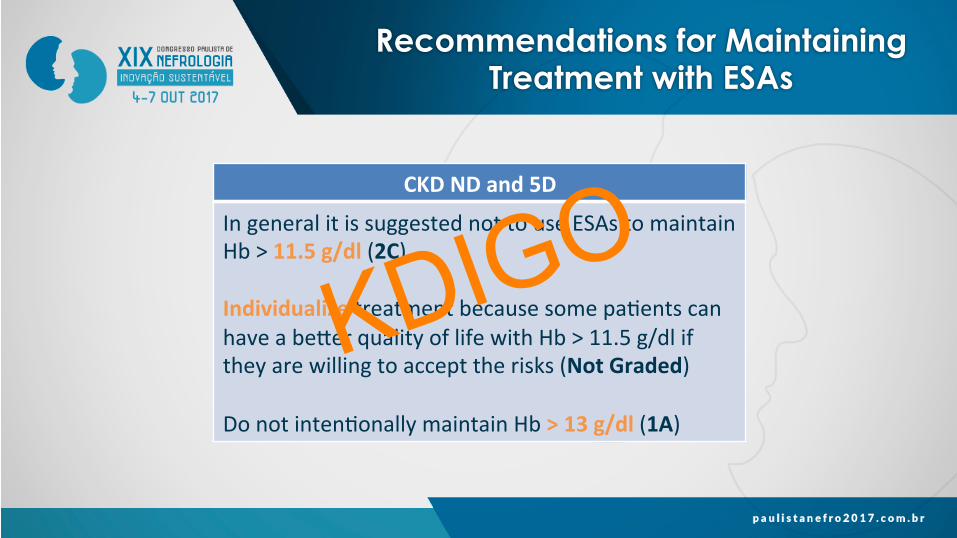
Recommendations for Maintaining Treatment with ESAs
CKDNDand5D
IngeneralitissuggestednottouseESAstomaintainHb>11.5g/dl(2C)Individualizetreatmentbecausesomepa.entscanhaveabemerqualityoflifewithHb>11.5g/dliftheyarewillingtoaccepttherisks(NotGraded)Donotinten.onallymaintainHb>13g/dl(1A)
KDIGO

Reasons for the Lower Limit of the Hb Target
• IntheTREATstudy,pa.entsrandomizedtoplacebohadameanHblevelof10.6g/dldespitethattheydidnotreceiveoronlyreceivedsmalldosesofdarbepoie.niftheHbwas<9g/dl
• Thereisnoevidencetosupportthatallpa.entswithHblevelsbetween9-10g/dlshouldreceivetreatmentwithESAs-INDIVIDUALIZE
• Inpa.entswithCKD5HD,Hbtendstodropfasterandreachlevelsof8g/dl;riskoftransfusionissignificantlyreducedifHbdoesnotfallto<9g/dl
KDIGO
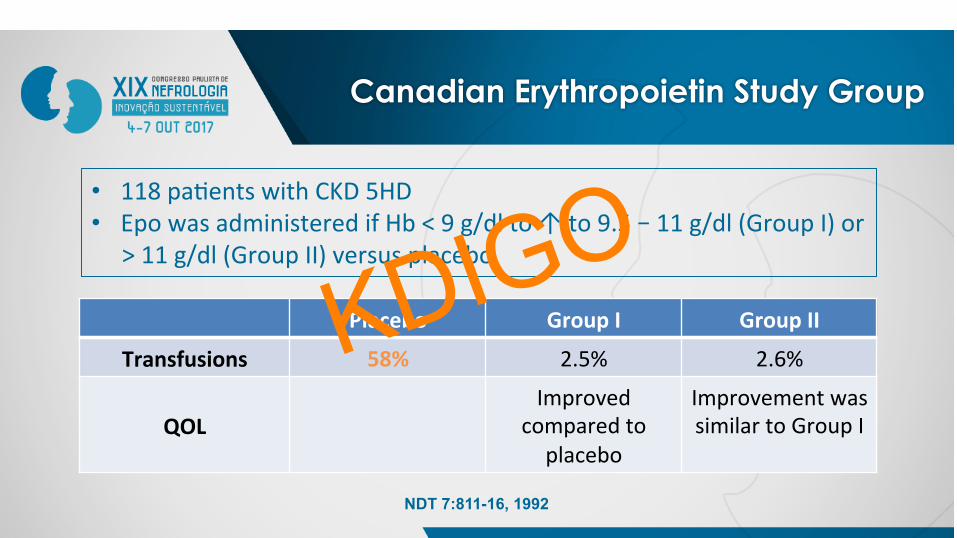
Canadian Erythropoietin Study Group
• 118pa.entswithCKD5HD• EpowasadministeredifHb<9g/dlto↑to9.5–11g/dl(GroupI)or
>11g/dl(GroupII)versusplacebo
Placebo GroupI GroupII
Transfusions 58% 2.5% 2.6%
QOLImproved
comparedtoplacebo
ImprovementwassimilartoGroupI
NDT 7:811-16, 1992
KDIGO
Reasons for the Upper Limit of the Hb Target
• Itisbasedupontheinterpreta.onthatthemaximumHblevelreachedinthecontrolgroupoftherecentECCswas<11.5g/dl
• Thereisnoenoughevidenceregardingthepoten.albenefitofincreasingtheHblevelbetween11.5-13g/dl• CREATEshowedbenefitsinqualityoflifebutCHOIRdidn’t
• AHblevel>13g/dlisassociatedwithahigherriskofcomplica.ons
KDIGO
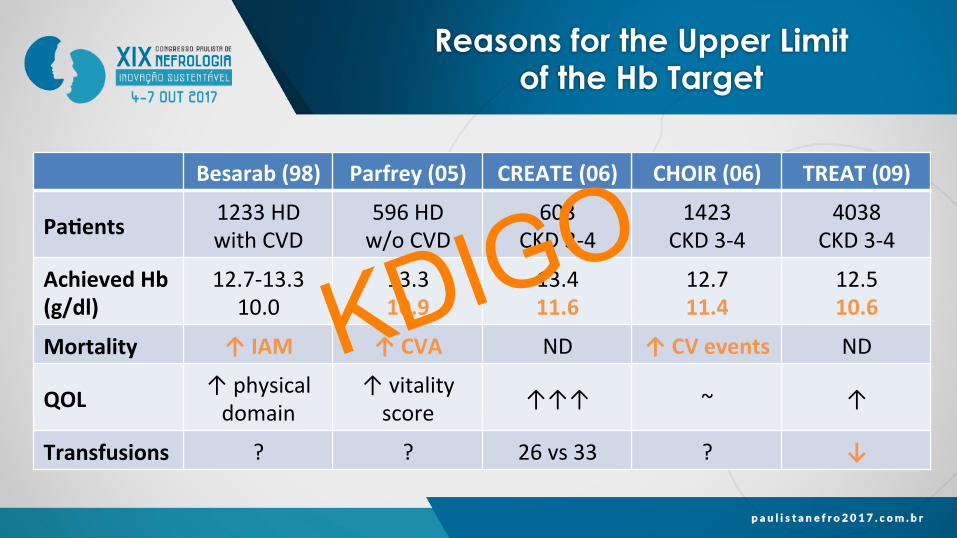
Reasons for the Upper Limit of the Hb Target
Besarab(98) Parfrey(05) CREATE(06) CHOIR(06) TREAT(09)
Pa%ents 1233HDwithCVD
596HDw/oCVD
603CKD3-4
1423CKD3-4
4038CKD3-4
AchievedHb(g/dl)
12.7-13.310.0
13.310.9
13.411.6
12.711.4
12.510.6
Mortality ↑IAM ↑CVA ND ↑CVevents ND
QOL ↑physicaldomain
↑vitalityscore ↑↑↑ ~ ↑
Transfusions ? ? 26vs33 ? ↓
KDIGO
2012 KDIGO Guidelines Anemia in CKD
ü Iden%fica%on,diagnosisandevalua%onofthecause
ü RoleofirontotreatCKD-relatedanemia
ü RoleofESAsandotherdrugstotreatCKD-relatedanemia
ü RoleofbloodtransfusionstotreatCKD-relatedanemia
KDIGO
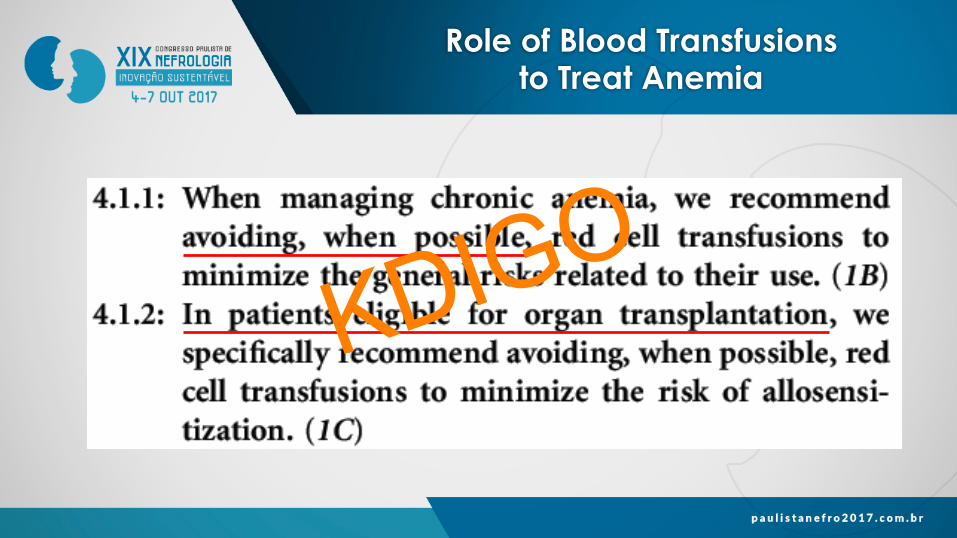
Role of Blood Transfusions to Treat Anemia
KDIGO
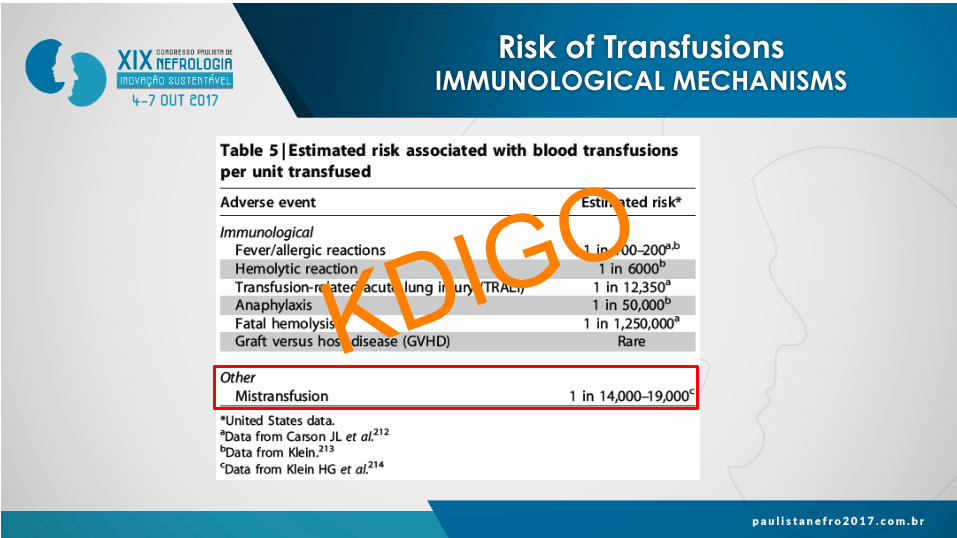
Risk of Transfusions IMMUNOLOGICAL MECHANISMS
KDIGO
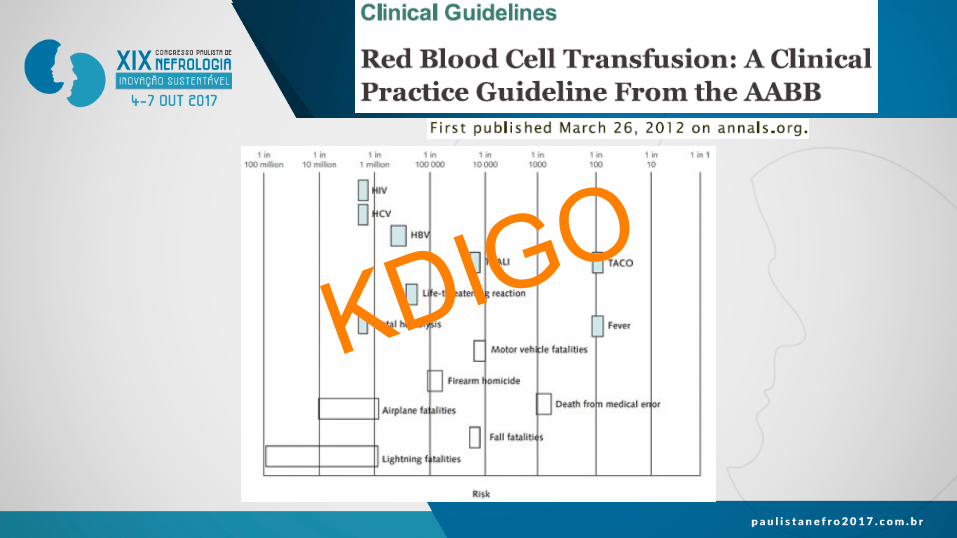
Risk of Transfusions IMMUNOLOGICAL MECHANISMS
KDIGO
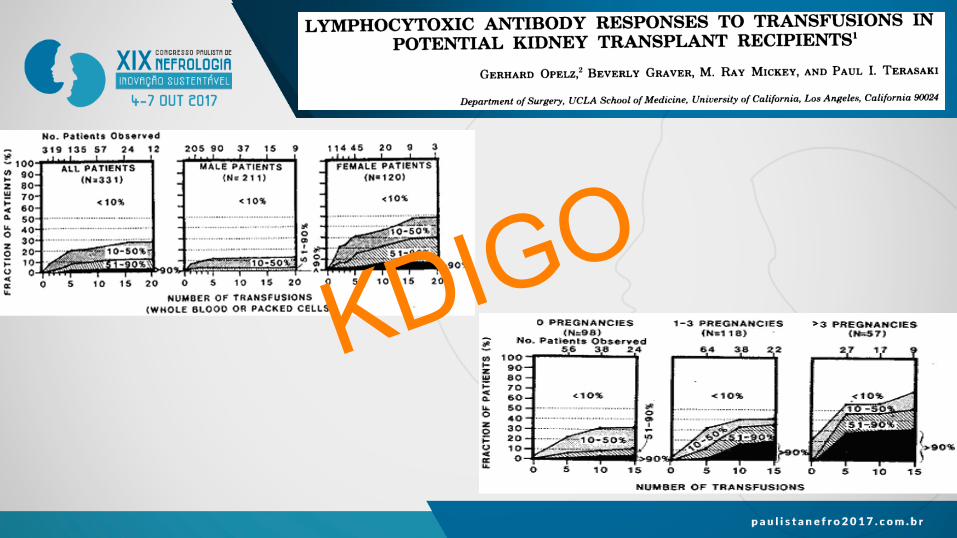
Risk of Transfusions IMMUNOLOGICAL MECHANISMS
KDIGO
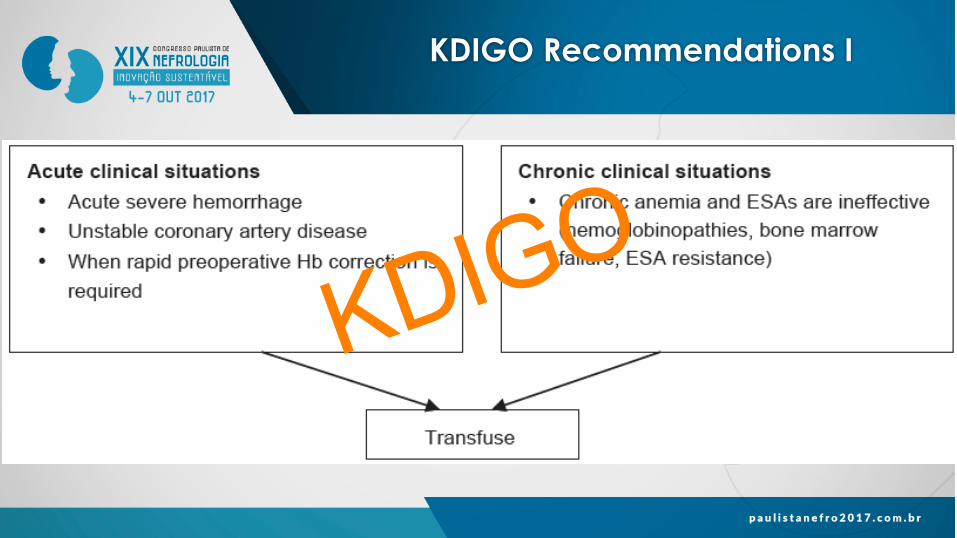
KDIGO Recommendations I
KDIGO

KDIGO Recommendations II
KDIGO

New Therapies HIF STABILIZERS New Therapies
HIF STABILIZERS
KDIGO
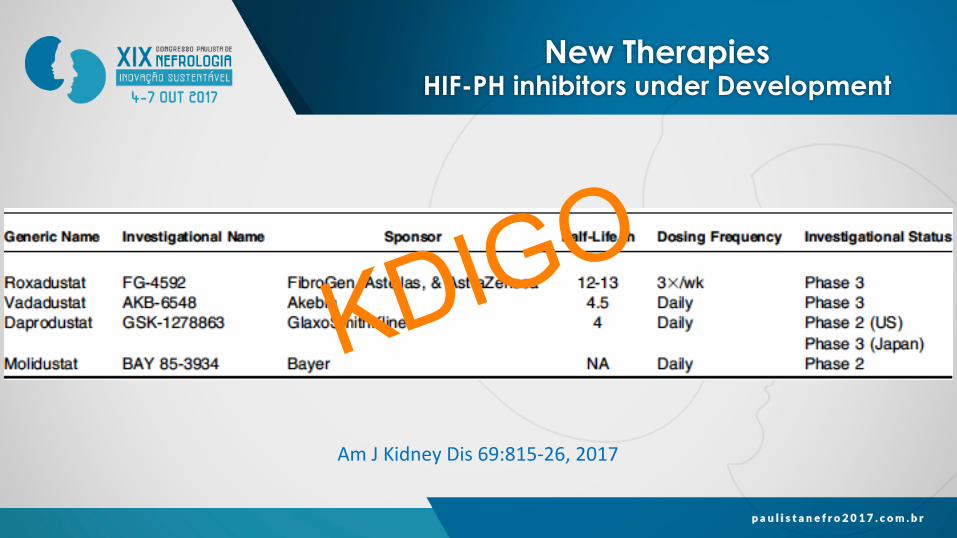
New Therapies HIF STABILIZERS New Therapies
HIF-PH inhibitors under Development
AmJKidneyDis69:815-26,2017
KDIGO
Potential Advantages of HIF Stabilizers
• Consistentalthoughnotcon.nuousandmorephysiologicaldosesofendogenousEpo
• Increasedavailabilityofironforerythropoiesis
• Oraladministra.on
KDIGO
Unanswered Questions
• Effectoncardiovascularhealth
• ImpactofnormalizingHbwiththeseagents
• Risksassociatedwithac.va.onofVEGF(progressivere.nopathy,tumorgrowth…)
KDIGO
Conclusions
• KDIGOguidelinerecommenda.onsforthemanagementofanemiaofCKDarebasedoncurrentlimitedevidence
• Therearegapsofknowledgethatrequirefurtherinves.ga.on
• CurrenttreatmentofanemiaofCKDisnotop.mal
• NewtherapiessuchasHIFstabilizersarepromising
KDIGO


















