Cisternal segments of the glossopharyngeal, vagus, and ...combined use of 3D CISS and 3D TOF...
16
J Neurosurg 110:1026–1041, 2009 1026 J. Neurosurg. / Volume 110 / May 2009 T HE glossopharyngeal and vagus nerves and the cra- nial component of the accessory nerve are together designated the lower CN complex. The nuclei of these nerves are located in the medulla oblongata. The dorsal vagal nuclei form the bulging vagal trigone on the floor of the fourth ventricle. 6 Cranial nerves IX, X, and XI arise from the medulla oblongata as a line of rootlets distributed along the pos- terior edge of the inferior olive in the postolivary sulcus. These rootlets coalesce to form nerve root bundles, which then traverse the lateral cerebellomedullary cistern. The bundles enter the jugular foramen close to each other through dural openings designated the glossopharyn- geal meatus (for CN IX) and the vagal meatus (for CNs X and XI). 27 A permanent dural septum separates the glossopharyngeal from the vagal meatus. Cranial nerve XI is traditionally considered to have both a cranial com- ponent (crCN XI) and a spinal root (spCN XI); however, the existence of a crCN XI is disputed, with different au- thors assigning the “traditional” crCXI rootlets to either CN X or XI. 17,40 Magnetic resonance imaging has been used success- fully to visualize CNs and associated lesions within the basal cisterns. 2,3,41,42,44–46 To our knowledge, however, only 1 imaging study has revealed the anatomy of the lower CN complex in detail. 35 Pathological entities such as schwan- nomas 1,4 and meningiomas 13 can affect the cisternal por- tions of the lower CN complex. Compression of the REZ Cisternal segments of the glossopharyngeal, vagus, and accessory nerves: detailed magnetic resonance imaging– demonstrated anatomy and neurovascular relationships Clinical article JENNIFER LINN, M.D., 1 BERNHARD MORIGGL, M.D., 2 FRIEDERIKE SCHWARZ, 1 THOMAS P. NAIDICH, M.D., PH.D., 3 URS D. SCHMID, M.D., 4 MARTIN WIESMANN, M.D., 1 HARTMUT BRUCKMANN, M.D., 1 AND INDRA Y OUSRY , M.D. 1 1 Department of Neuroradiology, University Hospital Munich, Germany; 2 Institute of Anatomy, Histology, and Embryology, Medical University Innsbruck, Austria; 3 Department of Radiology, Section of Neuroradiology, Mount Sinai Medical Center, New York; and 4 Neurosurgical Unit, Klinik Im Park, Zurich, Switzerland Object. The aim of this study was to determine whether high-resolution MR imaging is suitable for identifying and differentiating among the nerve root bundles of the glossopharyngeal (cranial nerve [CN] IX), vagus (CN X), and accessory nerves (CN XI) as well as any adjacent vessels. Methods. Twenty-five patients (50 sides) underwent MR imaging using the 3D constructive interference in steady-state (CISS) sequence, as well as noncontrast and contrast-enhanced 3D time-of-flight (TOF) MR angiogra- phy. Two individuals scored these studies by consensus to determine how well these sequences displayed the neu- rovascular contacts and nerve root bundles of CNs IX and X and the cranial and spinal roots of CN XI. Landmarks useful for identifying each lower CN were specifically sought. Results. The 3D CISS sequence successfully depicted CNs IX and X in 100% of the sides. Nerve root bundles of the cranial segment of CN XI were identified in 88% of the sides and those of the spinal segment of CN XI were noted in 93% of the sides. Landmarks useful in identifying the lower CNs included the vagal trigone, the choroid plexus of the lateral recess, the glossopharyngeal and vagal meatus, the inferior petrosal sinus, and the vertebral artery. The combined use of 3D CISS and 3D TOF sequences demonstrated neurovascular contacts at the nerve root entry or exit zones in 19% of all nerves visualized. Conclusions. The combined use of 3D CISS MR imaging and 3D TOF MR angiography (with or without con- trast) successfully displays the detailed anatomy of the lower CNs and adjacent structures in vivo. These imaging sequences have the potential to aid the preoperative diagnosis of and the presurgical planning for pathology in this anatomical area. (DOI: 10.3171/2008.3.17472) KEY WORDS • accessory nerve • glossopharyngeal nerve • magnetic resonance imaging • neurovascular relationship • vagus nerve Abbreviations used in this paper: AICA = anterior inferior cer- ebellar artery; CISS = constructive interference in steady state; CN = cranial nerve; crCN XI = cranial component of CN XI; DTPA = diethylenetriamine pentaacetic acid; FOV = field of view; IAM = internal acoustic meatus; PE = point of entry or exit; PICA = poste- rior inferior cerebellar artery; REZ = nerve root entry zone; RExZ = nerve root exit zone; spCN XI = spinal root of CN XI; TOF = time- of-flight; VA = vertebral artery.
Transcript of Cisternal segments of the glossopharyngeal, vagus, and ...combined use of 3D CISS and 3D TOF...
J Neurosurg 110:1026–1041, 2009
1026 J. Neurosurg. / Volume 110 / May 2009
The glossopharyngeal and vagus nerves and the cra-nial component of the accessory nerve are together designated the lower CN complex. The nuclei of
these nerves are located in the medulla oblongata. The dorsal vagal nuclei form the bulging vagal trigone on the floor of the fourth ventricle.6
Cranial nerves IX, X, and XI arise from the medulla oblongata as a line of rootlets distributed along the pos-terior edge of the inferior olive in the postolivary sulcus. These rootlets coalesce to form nerve root bundles, which
then traverse the lateral cerebellomedullary cistern. The bundles enter the jugular foramen close to each other through dural openings designated the glossopharyn-geal meatus (for CN IX) and the vagal meatus (for CNs X and XI).27 A permanent dural septum separates the glossopharyngeal from the vagal meatus. Cranial nerve XI is traditionally considered to have both a cranial com-ponent (crCN XI) and a spinal root (spCN XI); however, the existence of a crCN XI is disputed, with different au-thors assigning the “traditional” crCXI rootlets to either CN X or XI.17,40
Magnetic resonance imaging has been used success-fully to visualize CNs and associated lesions within the basal cisterns.2,3,41,42,44–46 To our knowledge, however, only 1 imaging study has revealed the anatomy of the lower CN complex in detail.35 Pathological entities such as schwan-nomas1,4 and meningiomas13 can affect the cisternal por-tions of the lower CN complex. Compression of the REZ
Cisternal segments of the glossopharyngeal, vagus, and accessory nerves: detailed magnetic resonance imaging–demonstrated anatomy and neurovascular relationships
Clinical articleJennifer Linn, M.D.,1 BernharD MoriggL, M.D.,2 frieDerike Schwarz,1 ThoMaS P. naiDich, M.D., Ph.D.,3 UrS D. SchMiD, M.D.,4 MarTin wieSMann, M.D.,1 harTMUT BrUckMann, M.D.,1 anD inDra YoUSrY, M.D.1 1Department of Neuroradiology, University Hospital Munich, Germany; 2Institute of Anatomy, Histology, and Embryology, Medical University Innsbruck, Austria; 3Department of Radiology, Section of Neuroradiology, Mount Sinai Medical Center, New York; and 4Neurosurgical Unit, Klinik Im Park, Zurich, Switzerland
Object. The aim of this study was to determine whether high-resolution MR imaging is suitable for identifying and differentiating among the nerve root bundles of the glossopharyngeal (cranial nerve [CN] IX), vagus (CN X), and accessory nerves (CN XI) as well as any adjacent vessels.
Methods. Twenty-five patients (50 sides) underwent MR imaging using the 3D constructive interference in steady-state (CISS) sequence, as well as noncontrast and contrast-enhanced 3D time-of-flight (TOF) MR angiogra-phy. Two individuals scored these studies by consensus to determine how well these sequences displayed the neu-rovascular contacts and nerve root bundles of CNs IX and X and the cranial and spinal roots of CN XI. Landmarks useful for identifying each lower CN were specifically sought.
Results. The 3D CISS sequence successfully depicted CNs IX and X in 100% of the sides. Nerve root bundles of the cranial segment of CN XI were identified in 88% of the sides and those of the spinal segment of CN XI were noted in 93% of the sides. Landmarks useful in identifying the lower CNs included the vagal trigone, the choroid plexus of the lateral recess, the glossopharyngeal and vagal meatus, the inferior petrosal sinus, and the vertebral artery. The combined use of 3D CISS and 3D TOF sequences demonstrated neurovascular contacts at the nerve root entry or exit zones in 19% of all nerves visualized.
Conclusions. The combined use of 3D CISS MR imaging and 3D TOF MR angiography (with or without con-trast) successfully displays the detailed anatomy of the lower CNs and adjacent structures in vivo. These imaging sequences have the potential to aid the preoperative diagnosis of and the presurgical planning for pathology in this anatomical area. (DOI: 10.3171/2008.3.17472)
keY worDS • accessory nerve • glossopharyngeal nerve • magnetic resonance imaging • neurovascular relationship • vagus nerve
Abbreviations used in this paper: AICA = anterior inferior cer-ebellar artery; CISS = constructive interference in steady state; CN = cranial nerve; crCN XI = cranial component of CN XI; DTPA = diethylenetriamine pentaacetic acid; FOV = field of view; IAM = internal acoustic meatus; PE = point of entry or exit; PICA = poste-rior inferior cerebellar artery; REZ = nerve root entry zone; RExZ = nerve root exit zone; spCN XI = spinal root of CN XI; TOF = time-of-flight; VA = vertebral artery.

J. Neurosurg. / Volume 110 / May 2009
Magnetic resonance imaging–demonstrated anatomy of the cranial nerves
1027
or RExZ by vessels or tumors can cause glossopharyngeal neuralgia.15,18,25 Surgically treating these lesions can cause iatrogenic lower CN pathology.27 Therefore, successfully displaying the anatomy of the caudal CN complex in vivo should help physicians to identify pathology, assess the extent of disease, formulate short differential diagnoses, and plan for successful surgical therapy for the pathology displayed.
Our specific aims in this study were to 1) determine whether high-resolution MR imaging of the lateral med-ullary cistern could reliably visualize and differentiate among the root bundles of CN IX, CN X, crCN XI, and spCN XI; 2) discover the exact relationships among the nerve root bundles, neighboring CNs, and adjacent ves-sels; and 3) establish anatomical landmarks useful for identifying the cisternal segments of CNs IX, X, and XI individually.
MethodsPatient Characteristics
The study group included 25 patients (11 men and 14 women, with a mean age of 58.3 years [range 29–81 years]) who had undergone contrast-enhanced MR imag-ing for reasons unrelated to the infratentorial compart-ment and who agreed to undergo additional 3D CISS MR imaging, noncontrast 3D TOF MR angiography, and con-trast-enhanced 3D TOF MR angiography pulse sequences. None of these patients had clinical abnormalities known to affect the lower CN complex or any other pathology affecting the infratentorial compartment. Imaging studies from 3 additional patients were also included to illustrate the clinical relevance of the MR imaging pulse sequences in evaluating the pathology of the lower CNs.
The study was approved by the review board of the department and conformed to the Declaration of Helsin-ki. Before beginning the study, all patients gave written informed consent to participate.
Magnetic Resonance Imaging ProceduresData were obtained on a 1.5-T unit (Magnetom Vi-
sion [17 patients] or Symphony [8 patients], Siemens) with a standard quadrature head coil by using 3D CISS MR imaging, noncontrast 3D TOF MR angiography, and contrast-enhanced 3D TOF MR angiography (start-ing 3 minutes after contrast administration) to display fine anatomical detail. The following pulse sequence was used in the 3D CISS MR imaging: TR = 12.25 msec, TE = 5.90 msec, flip angle = 70°, FOV = 180 × 180 mm (read × phase encode), slab thickness = 70.0 mm, ma- trix = 512 × 262, number of 3D partitions = 106, number of slabs = 1, pixel size = 0.35 × 0.69 mm, effective slice thickness = 0.66 mm, number of acquisitions = 1, and scan time = 11.4 minutes. The following pulse sequence was used in the 3D TOF MR angiography studies before and 3 minutes after the administration of Gd-DTPA (0.1 mmol/kg): TR = 31 msec, TE = 7 msec, flip angle = 20°, FOV = 200 × 200 mm, slab thickness = 50 mm, ma- trix = 512 × 224, number of 3D partitions = 50, number of slabs = 1, pixel size = 0.78 × 0.39, effective slice thick-
ness = 1 mm, number of acquisitions = 1, and scan time = 5 minutes 49 seconds.
Image Analysis ProceduresThe 3D data sets were analyzed using the multipla-
nar reconstruction function of the standard PACS work-station (Magic View VE42, Siemens Medical Solutions) to identify and display the CNs in 3 planes: 1) a trans-verse plane, parallel to the cisternal courses of CNs IX, X, and XI; 2) a sagittal-oblique plane, precisely aligned from posteromedial to anterolateral along the anatomical course of each nerve root bundle identified (referred to as the “sagittal plane” in the following text); and 3) a coronal plane, parallel to the dorsal edge of the brainstem.
Two experienced neuroradiologists collaboratively analyzed the data sets from each sequence, and the re-sults were decided by consensus. The left and right sides of each patient were evaluated independently.
Anatomical Assessment of the Cisternal Segments of CNs IX, X, and XI: 3D CISS Sequence. For each of the 3 planes used, we recorded whether the nerve root bundles of CNs IX and X, the crCN XI, and the spCN XI could be identified and differentiated with certainty (score of 2), most probably (score of 1), or not at all (score of 0). The number of nerve root bundles identified was recorded for each CN separately. Specific attention was directed toward identifying and distinguishing between the nerve root bundles of CN X and the traditional crCN XI. Root bundles were classified as crCN XI when MR imaging showed that the roots exited the brainstem caudal to the superior third of the olive and did not join the main vagal trunks. Because the spinal portion of CN XI is the only nerve to pass through the foramen magnum,30 nerve root bundles here were classified as belonging to the spinal component of CN XI root bundles when MR imaging showed that they entered the posterior fossa through the foramen magnum and passed into the same dural meatus as CN X.31
For each nerve root bundle identified, the length of the bundle’s cisternal segment was measured in the trans-verse and sagittal planes from its PE from the brainstem to the point at which the nerve root bundle entered the corresponding dural meatus. The PE of the nerve was de-fined as the point at which the specific root bundle was first separable from the brainstem.
The distance from CN IX to the vestibulocochlear (CN VIII) and facial nerves (CN VII) was determined at 2 sites. At the PE, the interneural distances were deter-mined by extending perpendicular lines from the PE of CN VII and the PE of CN VIII to CN IX (Fig. 1). At the dural meatus, the interneural distances were determined by tracing a perpendicular line from CN IX to VII and to VIII at the points at which they entered the IAM.
The distance from CN IX to X was similarly deter-mined in the sagittal plane at the nerves’ PEs by extend-ing a perpendicular line from the PE of CN IX to the uppermost nerve root bundle of CN X (Fig. 1) and at the dural meatus by tracing a perpendicular line from CN IX to X at the entrance of CN IX into the glossopharyngeal meatus.

J. Linn et al.
1028 J. Neurosurg. / Volume 110 / May 2009
Neurovascular Relationships: Combined Use of 3D CISS MR Imaging and 3D TOF MR Angiography. Neuro-vascular contact was defined as the absence of any detect-able layer of CSF between the CN and the adjacent vessel. If the 3D CISS MR images showed a vessel in contact with the CN, we identified the vessel by tracing it backward to its parent vessel and comparing it with corresponding structures depicted on the 3D TOF MR angiograms. Ves-sels could be identified as arteries by tracing them back to their parent artery. Vessels were defined as veins if 1) they appeared hyperintense on contrast-enhanced, and not hy-perintense on noncontrast, 3D TOF MR angiograms, and/or 2) they could be traced forward to a larger vein. If there was direct contact between the nerve and vessel, we mea-sured the distance between the PE of the nerve from the brainstem and the point of contact with the vessel.
The precise neurovascular relationship was recorded at 3 sites: contact at the PE of the respective nerve root bundle, contact along the REZ and/or RExZ, and contact along the cisternal segment of the nerve distal to the REZ or RExZ.
The definitions of the REZ or RExZ of CNs vary in the literature.5,19,21,28,39 In the context of the present study,
we defined the REZ and RExZ, respectively, as the length of the nerve segment between the PE of the nerve from the brainstem and the point of transition from central to peripheral myelin. Histologically, the mean length of the central (glial) segment of the CN is 1.1 mm for the sen-sory root of CN IX, < 1 mm for the motor root of CN IX, ≤ 2 mm for CN X, and ≤ 0.1 mm for CN XI.19
Landmarks for Identifying CNs IX, X, and XI. We determined whether the vagal trigone, the choroid plexus of the lateral recess of the fourth ventricle, the dural en-trances into the jugular foramen (glossopharyngeal and vagal meatus), and the inferior petrosal sinus could be used as landmarks for identifying the cisternal segments of CNs IX and X and the crCN XI. We also considered whether the VA could be used as a landmark for identify-ing the cisternal segment of the spCN XI. In each case, the certainty with which these structures could be identi-fied by these landmarks was scored with the previously described system (Scores 0, 1, and 2) used to grade the nerve bundles themselves.
The dimensions of the glossopharyngeal and vagal meatus were measured in the transverse and coronal planes. The distance between the cranial margin of the
Fig. 1. Schematic illustrating measurements performed to determine distances between the CNs at their PEs and dural entrances. Distances between the respective nerves at their PEs were calculated by dropping perpendiculars from CN VII to IX (yellow arrow), from CN VIII to IX (blue arrow), and from CN IX to the uppermost CN X root bundle (white arrow). At their dural entrances distances were determined by drawing perpendiculars from CN IX to VII (light green arrow), from CN IX to VIII (dark green arrow), and from CN IX to the uppermost CN X root bundle (black arrow). Red line marks the entrance level into the glossopharyngeal meatus. 1 = CN IX; 2 = CN VII; 3 = CN VIII; 4 = CN X root bundles; 5 = crCN XI nerve root bundles; 6 = spCN XI; 7 = vagal meatus; 8 = glossopharyngeal meatus; 9 = IAM.
J. Neurosurg. / Volume 110 / May 2009
Magnetic resonance imaging–demonstrated anatomy of the cranial nerves
1029
glossopharyngeal meatus and the caudal margin of the IAM was recorded. The certainty with which a dural sep-tum could be identified between the glossopharyngeal meatus and the vagal meatus was also noted.
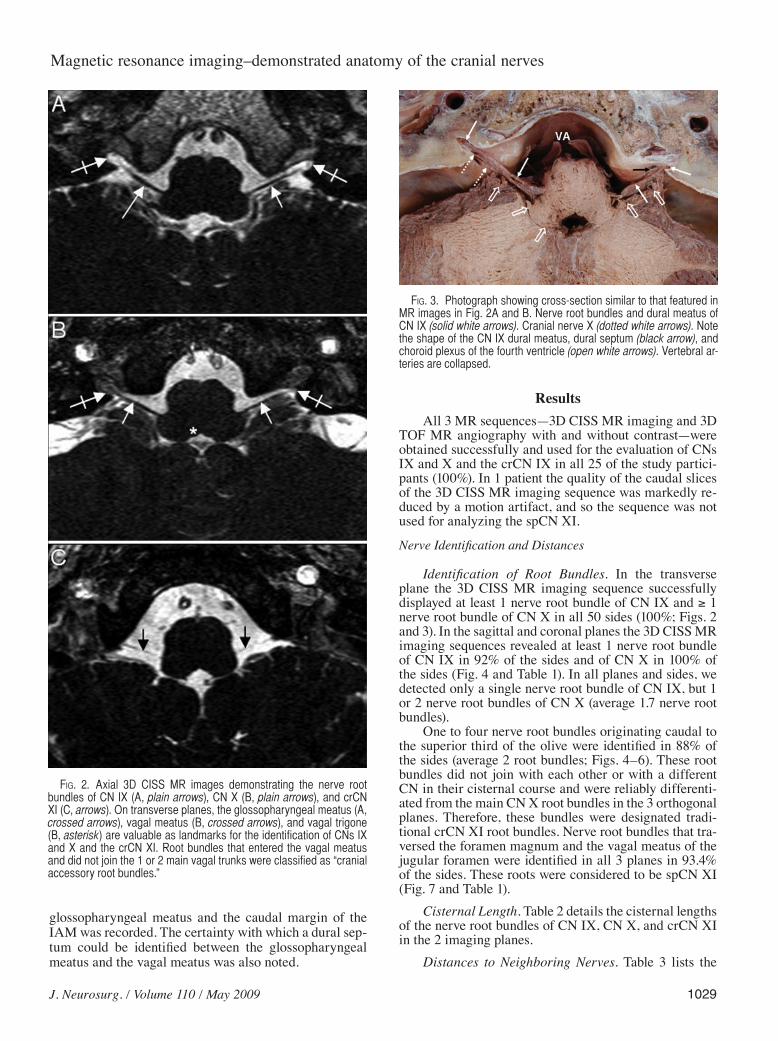
ResultsAll 3 MR sequences—3D CISS MR imaging and 3D
TOF MR angiography with and without contrast—were obtained successfully and used for the evaluation of CNs IX and X and the crCN IX in all 25 of the study partici-pants (100%). In 1 patient the quality of the caudal slices of the 3D CISS MR imaging sequence was markedly re-duced by a motion artifact, and so the sequence was not used for analyzing the spCN XI.
Nerve Identification and Distances
Identification of Root Bundles. In the transverse plane the 3D CISS MR imaging sequence successfully displayed at least 1 nerve root bundle of CN IX and ≥ 1 nerve root bundle of CN X in all 50 sides (100%; Figs. 2 and 3). In the sagittal and coronal planes the 3D CISS MR imaging sequences revealed at least 1 nerve root bundle of CN IX in 92% of the sides and of CN X in 100% of the sides (Fig. 4 and Table 1). In all planes and sides, we detected only a single nerve root bundle of CN IX, but 1 or 2 nerve root bundles of CN X (average 1.7 nerve root bundles).
One to four nerve root bundles originating caudal to the superior third of the olive were identified in 88% of the sides (average 2 root bundles; Figs. 4–6). These root bundles did not join with each other or with a different CN in their cisternal course and were reliably differenti-ated from the main CN X root bundles in the 3 orthogonal planes. Therefore, these bundles were designated tradi-tional crCN XI root bundles. Nerve root bundles that tra-versed the foramen magnum and the vagal meatus of the jugular foramen were identified in all 3 planes in 93.4% of the sides. These roots were considered to be spCN XI (Fig. 7 and Table 1).
Cisternal Length. Table 2 details the cisternal lengths of the nerve root bundles of CN IX, CN X, and crCN XI in the 2 imaging planes.
Distances to Neighboring Nerves. Table 3 lists the
Fig. 2. Axial 3D CISS MR images demonstrating the nerve root bundles of CN IX (A, plain arrows), CN X (B, plain arrows), and crCN XI (C, arrows). On transverse planes, the glossopharyngeal meatus (A, crossed arrows), vagal meatus (B, crossed arrows), and vagal trigone (B, asterisk) are valuable as landmarks for the identification of CNs IX and X and the crCN XI. Root bundles that entered the vagal meatus and did not join the 1 or 2 main vagal trunks were classified as “cranial accessory root bundles.”
Fig. 3. Photograph showing cross-section similar to that featured in MR images in Fig. 2A and B. Nerve root bundles and dural meatus of CN IX (solid white arrows). Cranial nerve X (dotted white arrows). Note the shape of the CN IX dural meatus, dural septum (black arrow), and choroid plexus of the fourth ventricle (open white arrows). Vertebral ar-teries are collapsed.

J. Linn et al.
1030 J. Neurosurg. / Volume 110 / May 2009
Fig. 4. Sagittal (A and B) and coronal (C) 3D CISS MR images clearly depicting the nerve root bundles of CN IX (crossed white arrows), CN X (plain white arrows), and the crCN XI (black arrows).
TABLE 1: Identification of nerve root bundles of CNs IX and X, the crCN XI, and the spCN XI in their cisternal course*
Transverse Sagittal Coronal
Region 2 1 0 2 1 0 2 1 0
CN IX 39 (78) 11 (22) 0 (0) 38 (76) 8 (16) 4 (8) 35 (70) 11 (22) 4 (8)CN X 49 (98) 1 (2) 0 (0) 44 (88) 6 (12) 0 (0) 38 (76) 12 (24) 0 (0)crCN XI 29 (58) 14 (28) 7 (14) 32 (64) 11 (22) 7 (14) 11 (22) 32 (64) 7 (14)spCN XI† 42 (87.5) 3 (6.25) 3 (6.25) 42 (87.5) 3 (6.25) 3 (6.25)
* Values represent the number of sides (%). With regard to CNs IX and X and the crCN XI, 50 sides were analyzed; with regard to the spCN XI, only 48 sides were analyzed because of severe motion artifacts in the caudal slices in 1 patient. Scores: 2 = positive identification, 1 = highly probable identification, 0 = no identification.† Sagittal plane was not evaluated.
J. Neurosurg. / Volume 110 / May 2009
Magnetic resonance imaging–demonstrated anatomy of the cranial nerves
1031
distances between the nerve root bundles of CNs IX and X as well as the distances between the nerve bundles of CNs VII and IX, and VIII and IX at their PEs and their entrances into the dural meatus.
Anatomical Landmarks
Vagal Trigone. The vagal trigone was successfully identified at the floor of the fourth ventricle in all study participants (score of 2 on all sides; Fig. 8A).
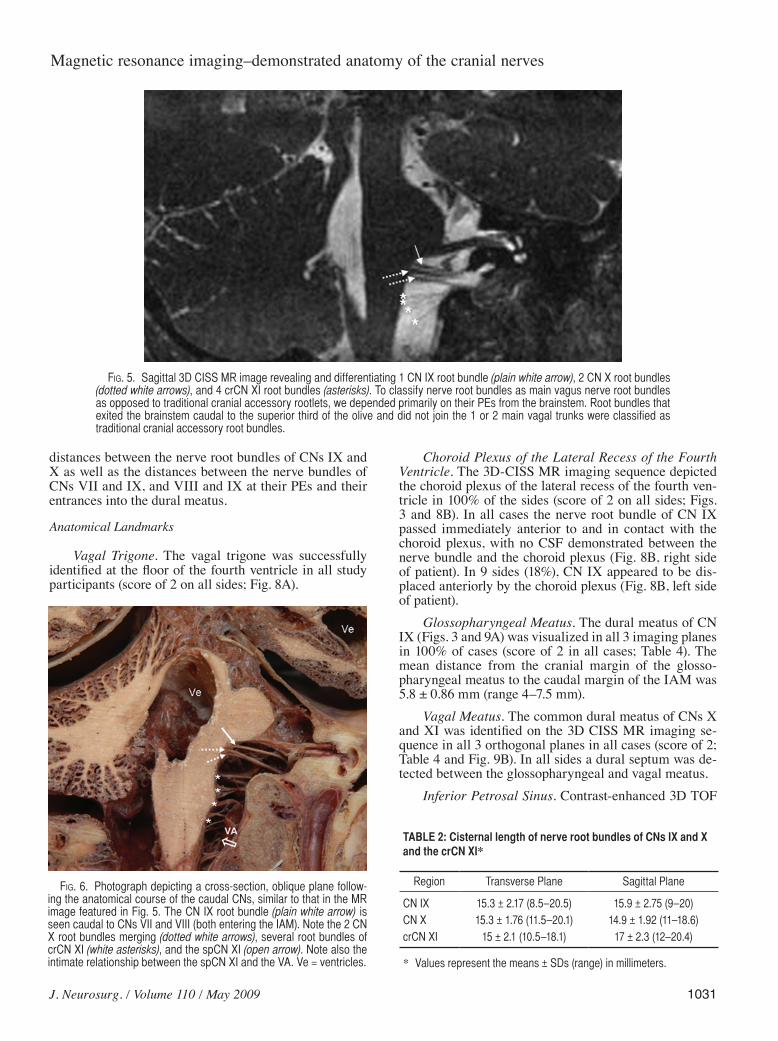
Choroid Plexus of the Lateral Recess of the Fourth Ventricle. The 3D-CISS MR imaging sequence depicted the choroid plexus of the lateral recess of the fourth ven-tricle in 100% of the sides (score of 2 on all sides; Figs. 3 and 8B). In all cases the nerve root bundle of CN IX passed immediately anterior to and in contact with the choroid plexus, with no CSF demonstrated between the nerve bundle and the choroid plexus (Fig. 8B, right side of patient). In 9 sides (18%), CN IX appeared to be dis-placed anteriorly by the choroid plexus (Fig. 8B, left side of patient).
Glossopharyngeal Meatus. The dural meatus of CN IX (Figs. 3 and 9A) was visualized in all 3 imaging planes in 100% of cases (score of 2 in all cases; Table 4). The mean distance from the cranial margin of the glosso- pharyngeal meatus to the caudal margin of the IAM was 5.8 ± 0.86 mm (range 4–7.5 mm).
Vagal Meatus. The common dural meatus of CNs X and XI was identified on the 3D CISS MR imaging se-quence in all 3 orthogonal planes in all cases (score of 2; Table 4 and Fig. 9B). In all sides a dural septum was de-tected between the glossopharyngeal and vagal meatus.
Inferior Petrosal Sinus. Contrast-enhanced 3D TOF
Fig. 5. Sagittal 3D CISS MR image revealing and differentiating 1 CN IX root bundle (plain white arrow), 2 CN X root bundles (dotted white arrows), and 4 crCN XI root bundles (asterisks). To classify nerve root bundles as main vagus nerve root bundles as opposed to traditional cranial accessory rootlets, we depended primarily on their PEs from the brainstem. Root bundles that exited the brainstem caudal to the superior third of the olive and did not join the 1 or 2 main vagal trunks were classified as traditional cranial accessory root bundles.
Fig. 6. Photograph depicting a cross-section, oblique plane follow-ing the anatomical course of the caudal CNs, similar to that in the MR image featured in Fig. 5. The CN IX root bundle (plain white arrow) is seen caudal to CNs VII and VIII (both entering the IAM). Note the 2 CN X root bundles merging (dotted white arrows), several root bundles of crCN XI (white asterisks), and the spCN XI (open arrow). Note also the intimate relationship between the spCN XI and the VA. Ve = ventricles.
TABLE 2: Cisternal length of nerve root bundles of CNs IX and X and the crCN XI*
Region Transverse Plane Sagittal Plane
CN IX 15.3 ± 2.17 (8.5–20.5) 15.9 ± 2.75 (9–20)CN X 15.3 ± 1.76 (11.5–20.1) 14.9 ± 1.92 (11–18.6)crCN XI 15 ± 2.1 (10.5–18.1) 17 ± 2.3 (12–20.4)
* Values represent the means ± SDs (range) in millimeters.

J. Linn et al.
1032 J. Neurosurg. / Volume 110 / May 2009
MR angiograms revealed the entrance of the inferior pet-rosal sinus into the jugular foramen at the level of the en-trance of CN IX into its meatus in all 3 orthogonal planes in all cases (Fig. 9C).
Vertebral Artery. The imaging studies always dis-
played a close relationship between the spCN XI and the point of entry of the VA into the dura mater at the level of the atlas (100% of cases; Figs. 10 and 11). The spCN XI always crossed the VA dorsomedially (see Neurovascular Relationships below).
Fig. 7. Sagittal (A–D and F) and coronal (E) 3D CISS MR images showing the spCN XI (arrowheads), always passing imme-diately dorsomedial to the VA (arrows) at the dural entrance of the vessel.
TABLE 3: Distances between the CNs at their PEs and dural entrances*
CN VII–IX CN VIII–IX CN IX–X
at PE† 2.98 ± 0.3 (2.6–3.6) 3.1 ± 0.5 (1.4–3.8) 2.5 ± 0.6 (1.4–4.6)at dural entrance‡ 5.5 ± 0.7 (4.5–6.9) 5.7 ± 0.9 (4.7–7) NM
* Values represent the means ± SD (range) in millimeters. Abbreviation: NM = not measured.† Measured by extending perpendicular lines from CN VII to IX, from CN VIII to IX, and from CN IX to the uppermost nerve root bundle of CN X at the PEs.‡ Measured by extending perpendicular lines from CN IX to VII, from CN IX to VIII, and from CN IX to the uppermost nerve root bundle of CN X at the entrance into their dural meatus.

J. Neurosurg. / Volume 110 / May 2009
Magnetic resonance imaging–demonstrated anatomy of the cranial nerves
1033
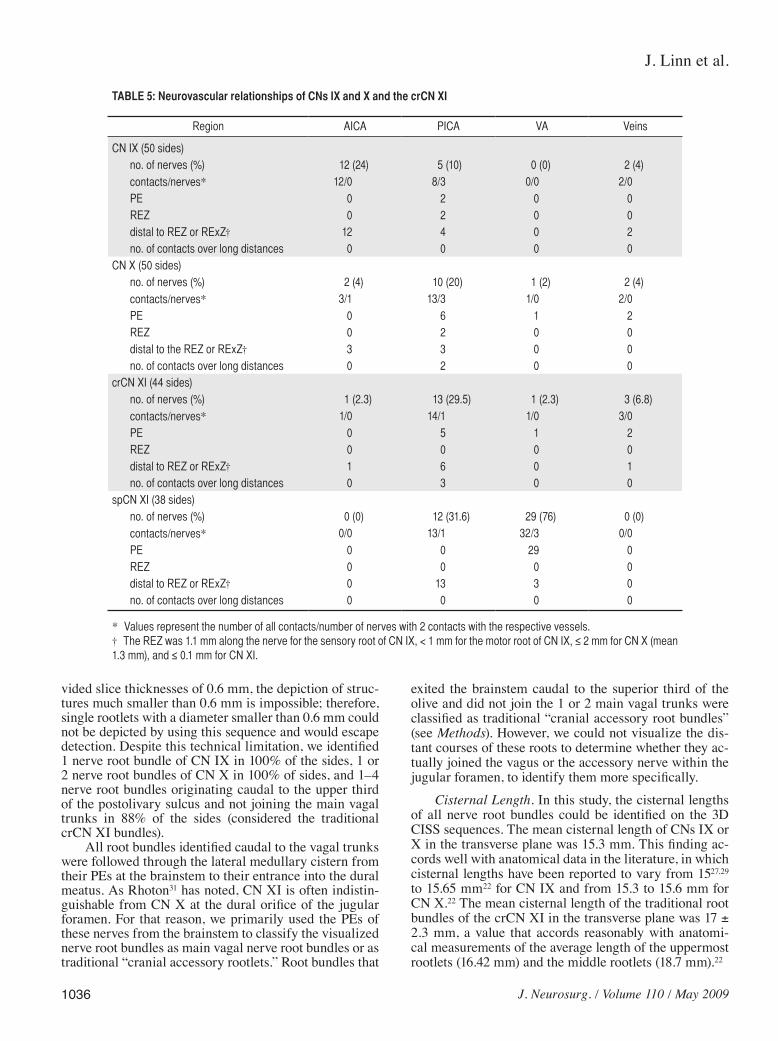
Neurovascular RelationshipsThe vessels identified as having a relationship to the
cisternal segments of CNs IX and X and the crCN XI included branches of the AICA, PICA (Fig. 12), VA, and diverse veins (Table 5). The spCN XI showed neurovas-cular contacts with the VA and PICA. Direct contact of the VA with the spCN XI occurred at the PE of the VA into the dura at the atlas in 76% of cases; proximity of the artery and nerve was observed in the remaining 24% of cases. In all of these cases, the spCN XI passed imme-diately dorsomedial to the VA at the level of the vessel’s entry into the dura (Figs. 7, 8, and 10). Direct contact be-tween the PICA and the spCN XI was identified in 31.6% of the sides. No neurovascular contact was found between CN IX, X, or XI and the basilar artery in this series.
Pathological Cases
Glossopharyngeal Neuralgia: Neurovascular Con-tact. In a 46-year-old woman with severe glossopharyn-geal neuralgia, imaging studies demonstrated neurovas-cular compression of the left CN IX by the left VA (Fig. 13A and B). The patient became symptom free after inter-position of a Teflon pad between the nerve and the vessel. Control imaging after surgery revealed a correct location of the Teflon spacer (Fig. 13C).
Fig. 8. A: Axial 3D CISS MR image depicting the vagal trigone (black arrows) formed by the dorsal motor vagal nucleus. Cranial nerve X leaves the brainstem at this level, so the vagal trigone serves as a land-mark for CN X on transverse MR images. B: Three-dimensional CISS MR image revealing the choroid plexus of the lateral recess of the fourth ventricle (white arrows). Cranial nerve IX (short black arrows) always passes immediately anterior to the choroid plexus with no intervening CSF. The left CN IX is displaced anteriorly by the plexus.
TABLE 4: Dimensions of the glossopharyngeal and vagal meatus in 50 sides*
Meatus Width† Height‡
glossopharyngeal 3.4 ± 0.9 (2–5.4) 2.4 ± 0.6 (1.2–4.1)vagal 4.4 ± 0.9 (2.4–6.5) 3.6 ± 0.9 (1.9–6)
* Values represent the means ± SD (range) in millimeters. † Assessed in the transverse planes.‡ Assessed in the coronal planes.
Fig. 9. The glossopharyngeal meatus, vagal meatus, and inferior petrosal sinus as landmarks for CNs IX and X. Axial 3D CISS images clearly depicting the entrance meatus of CNs IX and X into the jugular foramen. A: The glossopharyngeal meatus is funnel-shaped, becoming narrower as the nerve passes distally, resembling a small internal auditory canal. B: The vagal me-atus is approximately twice as wide as the glossopharyngeal meatus and varies in shape from elliptical to round. C: The inferior petrosal sinus (arrowheads) enters the jugular foramen at the same level that CN IX (crossed arrow) enters the glossopharyngeal meatus (white arrow). Asterisk indicates the choroid plexus of the lateral recess of the fourth ventricle.

J. Linn et al.
1034 J. Neurosurg. / Volume 110 / May 2009
Schwannoma of the spCN XI: Neurotumoral Con-tact. In a 30-year-old woman with known neurofibroma-tosis Type II, contrast-enhanced MR imaging demon-strated a tumor of the right CN XI at the craniocervical junction and a second small lesion in the right perimedul-lary cistern (Fig. 14). Three-dimensional CISS MR im-aging showed neurotumoral contact between the large right craniocervical junction tumor and the right spCN XI. The smaller tumor originated from the right CN IX. Surgery revealed 2 schwannomas. A right-sided acoustic schwannoma, bilateral trigeminal schwannomas, and a right frontal convexity meningioma were also present.
Agenesis of CNs IX and X. A 6-month-old child pre-sented with severe dysphagia and velopharyngeal insuf-ficiency. Three-dimensional CISS MR imaging revealed bilateral agenesis of CNs IX and X (Fig. 15).
DiscussionThe combined use of 3D CISS MR imaging and 3D
TOF MR angiography (with or without contrast) permits reliable identification of the individual nerves and neuro-vascular relationships of the lower CN complex. These sequences depicted CNs IX and X in 100% of the sides in 25 patients, and the crCN XI and spCN XI in 88 and 93.4% of the sides, respectively. Neurovascular contacts were identified at the REZ or RExZ in 8 (CN XI), 22 (CN X), and 18% (crCN XI) of the sides.
Emergence and Course of the Lower CNsThe nuclei of the caudal CNs are located in the me-
dulla oblongata. The dorsal vagal nuclei form the vagal trigone6 on the floor of the fourth ventricle. The rootlets
Fig. 10. The VA as a landmark for the spCN XI. Axial (A and B) and coronal (C and D) 3D CISS MR images demonstrating a very close relationship between spCN XI (arrowheads) and the VA (arrows) at its entrance through the dura. The spCN XI always passes dorsomedial to the VA at this point.
Fig. 11. Photograph showing cross-section similar to that featured in the MR image in Fig. 10A. Vertebral arteries (long arrows) at their dural entrance. Cranial nerve IX (short arrows) crosses immediately dorso-medial to them.

J. Neurosurg. / Volume 110 / May 2009
Magnetic resonance imaging–demonstrated anatomy of the cranial nerves
1035
of CNs IX and X and the crCN XI arise from the brain-stem in the postolivary sulcus.31 Cranial nerve IX emerg-es from the medulla oblongata as 10–20 rootlets22,27 dis-tributed along the upper third of the postolivary sulcus. These rootlets coalesce to form the cisternal segment of CN IX, with a nerve root diameter of 0.4–1.1 mm.32
The rootlets of CN X also arise in the upper third of the postolivary sulcus but slightly caudal to CN IX.19,29 These rootlets emerge along a length of 2–5.5 mm, have diameters of 0.1–1.5 mm, and typically coalesce into 2 (upper and lower) nerve root bundles.22 The most rostral vagal fibers usually arise immediately adjacent to the rootlets of CN IX but can be separated from CN IX by as much as 2.0 mm.32
Just caudal to the vagal bundle at the level of the in-ferior third of the olive, 6–16 additional delicate rootlets (diameter 0.1–1.0 mm) emerge from the medulla oblonga-ta and coalesce into 4–5 nerve root bundles.20,32,40 These rootlets have traditionally been regarded as the crCN XI, because they are considered to join the spCN XI and travel with it briefly before they become part of CN X (the so-called pars vagalis) within the jugular foramen.17,22
The spCN XI arises as 6–7 rootlets emerging from the cervical spinal cord segments C1–6 in line with the paraolivary sulcus of the medulla.19,21 The spCN XI as-cends vertically into the spinal canal, traverses the fo-ramen magnum, and passes to the jugular foramen.12,19 The final spinal nerve root has a mean diameter of ~ 1.0 mm.31
It is unclear whether the cranial rootlets of CN XI are best considered to be rootlets of the vagus or accessory nerve. Lang has pointed out that the cranial rootlets of CN XI cannot be securely separated from rootlets of the vagus nerve.21 He has shown that these rootlets have their origin in the caudal part of the nucleus ambiguus and the dorsal nucleus of the vagus nerve, and therefore are func-tionally vagal rootlets.6,12 Lachmann et al.17 have found no connection between “the cranial CN XI rootlets” and the spCN XI, so they considered these rootlets to be the “caudal posterior medullary rootlets of the vagus nerve.” However, other authors have shown that these caudal rootlets do intermingle with the spCN XI.30 Working in embalmed human cadavers, Wiles et al.40 have shown that distinct rootlets emerge from the postolivary sulcus cau-dal to, and separate from, the main trunk of the vagus nerve and then join the spCN XI.2 They considered these rootlets to be cranial CN XI rootlets.
Magnetic Resonance Imaging of CNs IX, X, and XI
Nerve Identification. The small distances between the origins of CNs IX, X, and XI at the brainstem and the small diameters of these rootlets make it particularly dif-ficult to identify and separate them on MR imaging. The diameters of the glossopharyngeal, vagal, and cranial ac-cessory rootlets vary from 0.1 to 1.5 mm. These thin root-lets then coalesce into the thicker nerve root bundles and roots. Given that the 3D CISS sequence in our study pro-
Fig. 12. Neurovascular contact in a symptom-free patient. Axial (A) and coronal (C) 3D CISS MR image revealing broad-based contact between the right CN X (black arrows) and the right PICA (white arrows). Neurovascular contact is also present at the PE (asterisk) of CNX. Noncontrast TOF MR angiograms (B and D) showing a flow void within the vessel, identifying it as an artery (white arrows).
J. Linn et al.
1036 J. Neurosurg. / Volume 110 / May 2009
vided slice thicknesses of 0.6 mm, the depiction of struc-tures much smaller than 0.6 mm is impossible; therefore, single rootlets with a diameter smaller than 0.6 mm could not be depicted by using this sequence and would escape detection. Despite this technical limitation, we identified 1 nerve root bundle of CN IX in 100% of the sides, 1 or 2 nerve root bundles of CN X in 100% of sides, and 1–4 nerve root bundles originating caudal to the upper third of the postolivary sulcus and not joining the main vagal trunks in 88% of the sides (considered the traditional crCN XI bundles).
All root bundles identified caudal to the vagal trunks were followed through the lateral medullary cistern from their PEs at the brainstem to their entrance into the dural meatus. As Rhoton31 has noted, CN XI is often indistin-guishable from CN X at the dural orifice of the jugular foramen. For that reason, we primarily used the PEs of these nerves from the brainstem to classify the visualized nerve root bundles as main vagal nerve root bundles or as traditional “cranial accessory rootlets.” Root bundles that
exited the brainstem caudal to the superior third of the olive and did not join the 1 or 2 main vagal trunks were classified as traditional “cranial accessory root bundles” (see Methods). However, we could not visualize the dis-tant courses of these roots to determine whether they ac-tually joined the vagus or the accessory nerve within the jugular foramen, to identify them more specifically.
Cisternal Length. In this study, the cisternal lengths of all nerve root bundles could be identified on the 3D CISS sequences. The mean cisternal length of CNs IX or X in the transverse plane was 15.3 mm. This finding ac-cords well with anatomical data in the literature, in which cisternal lengths have been reported to vary from 1527,29 to 15.65 mm22 for CN IX and from 15.3 to 15.6 mm for CN X.22 The mean cisternal length of the traditional root bundles of the crCN XI in the transverse plane was 17 ± 2.3 mm, a value that accords reasonably with anatomi-cal measurements of the average length of the uppermost rootlets (16.42 mm) and the middle rootlets (18.7 mm).22
TABLE 5: Neurovascular relationships of CNs IX and X and the crCN XI
Region AICA PICA VA Veins
CN IX (50 sides) no. of nerves (%) 12 (24) 5 (10) 0 (0) 2 (4) contacts/nerves* 12/0 8/3 0/0 2/0 PE 0 2 0 0 REZ 0 2 0 0 distal to REZ or RExZ† 12 4 0 2 no. of contacts over long distances 0 0 0 0CN X (50 sides) no. of nerves (%) 2 (4) 10 (20) 1 (2) 2 (4) contacts/nerves* 3/1 13/3 1/0 2/0 PE 0 6 1 2 REZ 0 2 0 0 distal to the REZ or RExZ† 3 3 0 0 no. of contacts over long distances 0 2 0 0crCN XI (44 sides) no. of nerves (%) 1 (2.3) 13 (29.5) 1 (2.3) 3 (6.8) contacts/nerves* 1/0 14/1 1/0 3/0 PE 0 5 1 2 REZ 0 0 0 0 distal to REZ or RExZ† 1 6 0 1 no. of contacts over long distances 0 3 0 0spCN XI (38 sides) no. of nerves (%) 0 (0) 12 (31.6) 29 (76) 0 (0) contacts/nerves* 0/0 13/1 32/3 0/0 PE 0 0 29 0 REZ 0 0 0 0 distal to REZ or RExZ† 0 13 3 0 no. of contacts over long distances 0 0 0 0
* Values represent the number of all contacts/number of nerves with 2 contacts with the respective vessels.† The REZ was 1.1 mm along the nerve for the sensory root of CN IX, < 1 mm for the motor root of CN IX, ≤ 2 mm for CN X (mean 1.3 mm), and ≤ 0.1 mm for CN XI.

J. Neurosurg. / Volume 110 / May 2009
Magnetic resonance imaging–demonstrated anatomy of the cranial nerves
1037
Distances. Cranial nerve IX arises between CN VIII cranially and CN X caudally. Systematic evaluation of the distance between these nerves and CN IX showed that the mean distance between CNs IX and VIII at their PEs was 3.1 mm, and the mean distance between CNs IX and X at their PEs was 2.5 mm. These measurements accord well
with anatomical dissection data.29 The mean distance be-tween CNs VII and IX, and VIII and IX at their dural entrances measured 5.5–5.7 mm. We could find no refer-ence values for these meatal measurements in anatomical cadaver studies.
Because CN VII consistently arises from the brain-stem 2–3 mm from CN IX, knowledge of the constancy of these relationships may assist the neurosurgeon in preoperative planning and intraoperative decision mak-ing with regard to the facial nerve or lower cranial nerve complex.29,48
Anatomical Landmarks Structural relationships and landmarks identified in
this study may assist with imaging and intraoperative identification of the lower CN roots. These landmarks in-clude the vagal trigone (Fig. 8A), the choroid plexus of the lateral recess of the fourth ventricle (Fig. 8B), the me-atus of the glossopharyngeal and vagus nerves, the infe-rior petrosal sinus (Fig. 9), and the vertebral artery at the point at which it pierces the dura at C-1 (Fig. 10).
Vagal Trigone. In 3D CISS images, the vagal trigo-ne is consistently (100% of cases) displayed as a distinct bulge formed in the caudal portion of the floor of the fourth ventricle by the dorsal motor nucleus of the vagus nerve. Given that CN X exits the brainstem at this level,1 the vagal trigone may serve as an imaging landmark for CN X (Fig. 8A).
Choroid Plexus. Anatomical studies have shown that the choroid plexus of the fourth ventricle’s lateral recess may help to identify the cisternal segment of CN IX.10,28 In the present study we noted that CN IX always courses anterior to the choroid plexus of the lateral recess and always has direct contact with the plexus in vivo; thus, the choroid plexus serves as a valuable landmark for the depiction and identification of CN IX. In 18% of the sides in this study we even noted anterior displacement of the nerve by the plexus. Although we confirmed that contact between CN IX and the choroid plexus is a normal find-ing and that anterior displacement of CN IX by the plexus may also be a typical finding, glossopharyngeal neuralgia has been reported to result from a compromised cisternal segment of CN IX by an exuberant choroid plexus.25
Glossopharyngeal and Vagal Meatus. The dural cover of the neural portion of the jugular foramen has 2 characteristic perforations: the glossopharyngeal me-atus cranially and the vagal meatus caudally, separated by a fibrous crest (dural septum).26,27,31 Cranial nerve IX enters the jugular foramen through the glossopharyngeal meatus, whereas CN X, the crCN XI and the spCN XI enter the jugular foramen via the vagal meatus. Anatomi-cal cadaver studies have shown that the glossopharyngeal meatus may serve as a landmark for identifying CN IX in the subarachnoid space.26,27 Rhoton31 has noted that the correct identification of the specific nerves may be easiest in the area just proximal to the dural septum, because the close origin of these nerves from the brainstem and the arachnoidal adhesions between them in the lateral medul-lary cistern make it difficult to identify them elsewhere.
Fig. 13. Three-dimensional CISS MR images obtained in a 46-year-old woman with severe left-sided glossopharyngeal neuralgia. Preop-erative images (A and B) demonstrating neurovascular compression of the left CN IX (solid white arrows) by the VA (arrowheads) at 4.5 mm from the nerve’s exit from the brainstem (and therefore distal to the REZ or RExZ of CN IX). The patient became symptom free after interposition of a Teflon pad between the nerve and the vessel. Postoperative image (C) revealing correct location of the interposed pad (dotted white arrow). Symptomatic patients with compression can benefit from surgery even if the site of compression is distal to REZ or RExZ.

J. Linn et al.
1038 J. Neurosurg. / Volume 110 / May 2009
Fig. 14. Three-dimensional CISS MR images demonstrating schwannomas of CN IX and the spCN XI in a 30-year-old woman with neurofibromatosis Type II and a right frontal convexity meningioma (not shown). A and B: A small tumor at the right cran-iocervical junction (open arrow), which contacts the right spCN XI (arrowheads). At surgery, this lesion proved to be schwannoma deriving from the spCN XI. C and D: The smaller tumor arising from the right CN IX (black arrow) proved to be a schwannoma at surgery. E: Thin white arrow (also in panel C) indicates CN X. The patient also had an additional right acoustic schwannoma (thick solid white arrow) easily distinguishable from CN IX (D) and CN X.
Fig. 15. Three-dimensional CISS MR images obtained in a 6-month-old child who had presented with severe dysphagia and velopharyngeal insufficiency, revealing bilateral agenesis of the CNs IX and X. Arrows mark the glossopharyngeal meatus (A) and vagal meatus (B). Cranial nerves IX and X are not discernible in their respective meatus, whereas CN VIII can easily be identified within the IAM (C, arrows).

J. Neurosurg. / Volume 110 / May 2009
Magnetic resonance imaging–demonstrated anatomy of the cranial nerves
1039
In the present study, 3D CISS MR images consistently revealed the glossopharyngeal and vagal meatus and the intervening dural septum in all 3 orthogonal planes. Thus, MR imaging has proved to be a valuable tool for identi-fying and distinguishing these structures and the related nerves in vivo.
In accord with anatomical studies we found that the glossopharyngeal meatus is funnel-shaped, narrows distally, and resembles a “small internal auditory canal” (Figs. 3 and 9), whereas the vagal meatus is round to ellip-tical and approximately twice as wide as the glossopha-ryngeal meatus.32 We also found that the mean width of the glossopharyngeal meatus was 3.4 ± 0.9 mm (height 2.4 ± 0.6 mm), whereas the mean width of the vagal me-atus was 4.4 ± 0.9 mm (height 3.6 ± 0.9 mm). The differ-ences in size and shape help to distinguish the glossopha-ryngeal meatus from the vagal meatus, and therefore CN IX from CN X and CN XI.
In this study the mean distance from the glossopha-ryngeal meatus to the inferior lip of the internal auditory canal was 5.8 ± 0.9 mm. This finding accords well with the distance of 2.5–6.5 mm reported in anatomical dis-section studies.19 This intermeatal distance could help to identify the glossopharyngeal meatus in the coronal and sagittal planes.
Inferior Petrosal Sinus. The inferior petrosal sinus courses on the intracranial surface of the petroclival fis-sure before it enters the petrosal part of the jugular fo-ramen. Anatomical cadaver studies have shown that the inferior petrosal sinus empties into the medial aspect of the jugular bulb between the glossopharyngeal nerve anteriorly and the vagus nerve posteriorly.31 On MR im-aging, we reliably identified the entrance of the inferior petrosal sinus into the jugular foramen at the level of the glossopharyngeal meatus. Thus, we propose this venous structure as a valuable landmark for the identification of CN IX.
Vertebral Artery. We consistently observed a close relationship between the dural entrance of the VA and the spCN XI, with the spCN XI passing immediately dor-somedial to the VA. A general relationship between the vessel and the nerve root has been described in several anatomical cadaver studies19,22,25 and in an imaging study by Edal et al.7 To our knowledge, the present study is the first in which this constant relationship has been analyzed in detail and the VA at its dural entrance has been pro-posed as an explicit landmark for the identification of the spCN XI on cranial MR imaging.
Neurovascular RelationshipsVascular compression can occur at any point along a
CN; however, only compression at vulnerable sites along the cisternal segment of the nerve is widely believed to cause neurovascular compression syndromes.5,9,21,24 The precise locations of and nomenclature for these vulner-able sites has been debated in the literature.5,9,21,24 For the purposes of this study, we designated the central portion of the cisternal segment of the nerve, where the myelin is derived from oligodendroglial cells, as the REZ or RExZ and considered it to be the portion of the nerve vulner-
able to neurovascular compression. As defined, the REZ or RExZ extends from the nerve’s point of entry into or exit from the brainstem to the point of transition from central (derived from oligodendroglia) to peripheral my-elin (derived from Schwann cells).
The length of the REZ or RExZ varies from nerve to nerve. Histologically, the mean length of the central (glial) segment of the CN is 1.1 mm for the sensory root of CN IX, < 1 mm for the motor root of CN IX, up to 2 mm for CN X (average 1.3 mm), and up to 0.1 mm for CN XI.5,9,19 Thus, for this study and in accordance with the literature, we considered the REZ or RExZ to be within 1 mm of the PEs for CNs IX and XI but within 2 mm of the PE for CN X.21
Based on this definition, we identified neurovascu-lar contacts at the REZ or RExZ of CNs IX, X, and XI in 19% of all nerves investigated (Fig. 12). Specifically, we identified neurovascular contacts at the REZ/RExZ of CN IX in 8% of all sides, of CN X in 22% of all sides, and of the crCN XI in 18% of all sides. In accordance with an-atomical reports, vessels noted to have contact with CNs IX, X, and XI were the PICA, AICA, VA, and various veins.19,20,23 We did not detect contact between the REZ or RExZ of the CNs and the basilar artery.19,20,23
Clinical RelevanceA number of syndromes are thought to result from
the contact of vessels with the REZ or RExZ of specific CNs.8,10,11,14,16,24,33,38,43 It is suggested that at least some cas-es of glossopharyngeal neuralgia are caused by vessels compressing the sensory root of the CN IX. The vessel most frequently implicated in glossopharyngeal neuralgia has been the PICA.8,11,38 However, Jannetta10 has reported on 2 cases of glossopharyngeal neuralgia caused by com-pression of the nerve by the VA (Fig. 13). Neurovascular contact has also been proposed to cause essential hyper-tension (CN X)14,33,34 and spasmodic torticollis (CN XI).37
None of the study participants manifested any symp-toms of CN abnormality. This high incidence of clinically normal neurovascular contacts accords well with studies on essential hypertension that show neurovascular contact in 12–53% of healthy control groups.33,34 Neurovascular contacts at the lower CNs, therefore, have low specificity for predicting clinical symptomatology, as is the case for neurovascular contacts at CN V.46
Figures 13–15 illustrate the clinical application of MR imaging studies for the diagnosis and surgical manage-ment of lower CN pathology, such as neural compression by intrinsic and extrinsic neurinomas and neurovascular contact.36,47 Interestingly, in the case of glossopharyngeal neuralgia presented in Fig. 13, the contact between nerve and vessel was considerably distal to the REZ or RExZ. Nonetheless, the patient did benefit from decompression surgery. These observations confirm the widely held clin-ical conviction that physicians should not rely on imaging alone for making therapeutic decisions about neurovascu-lar compression syndromes. The presence and localiza-tion of neurovascular contacts should be evaluated only in the context of a specific clinical presentation.

J. Linn et al.
1040 J. Neurosurg. / Volume 110 / May 2009
ConclusionsThis study demonstrates that in vivo MR imaging
with 3D CISS and 3D TOF sequences (with or without contrast) successfully visualizes and reveals differentia-tion among the cisternal segments of CNs IX and X and the cranial and spinal roots of CN XI. Our data provide detailed information regarding the lengths of the cisternal segments of the lower CNs, the distances between nerve root bundles, the distances between their dural meatus, and the neurovascular relationships of the lower CN com-plex. We also showed landmarks useful for identifying the specific CNs with the aid of preoperative imaging and intraoperative inspection. A detailed depiction of patient anatomy—and individual anatomical variation—should assist the surgeon in proper preoperative planning and in-traoperative decision making, potentially leading to im-proved outcome with decreased perioperative morbidity and death.48
Disclaimer
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
References
1. Aydin K, Maya MM, Lo WW, Brackmann DE, Kesser B: Ja-cobson’s nerve schwannoma presenting as middle ear mass. AJNR Am J Neuroradiol 21:1331–1333, 2000
2. Casselman JW, Dehaene I: Imaging of the IIIrd, IVth, and VIth cranial nerves. Neuroophthalmology 19:63–68, 1998
3. Casselman JW, Kuhweide R, Deimling M, Ampe W, Dehaene I, Meeus L: Constructive interference in steady state-3DFT MR imaging of the inner ear and cerebellopontine angle. AJNR Am J Neuroradiol 14:47–57, 1993
4. Clairmont AA, Conley JJ: Malignant schwannoma of the parapharyngeal space. J Otolaryngol 6:28–30, 1977
5. De Ridder D, Møller A, Verlooy J, Cornelissen M, De Ridder L: Is the root entry/ exit zone important in microvascular com-pression syndromes? Neurosurgery 51:427–434, 2002
6. Duvernoy HM: Structure and functions of the brain stem, in Duvernoy HM (ed): The Human Brain Stem and Cerebel-lum. New York: Springer-Verlag, 1995, pp 41–89
7. Edal A, Balériaux D, Metens T, David P, Yang P, Thierry R, et al: Three-dimensional turbo spin echo cervical magnetic resonance myleography. Normal appearance, anatomic land-marks, and early clinical results. Int J Neuroradiol 3:130–135, 1997
8. Fischbach F, Lehmann TN, Ricke J, Bruhn H: Vascular com-pression in glossopharyngeal neuralgia: demonstration by high-resolution MRI at 3 tesla. Neuroradiology 45:810–811, 2003
9. Hohenbleicher H, Schmitz SA, Koennecke HC, Offermann R, Offermann J, Zeytountchian H, et al: Neurovascular contact of cranial nerve IX and X root-entry zone in hypertensive pa-tients. Hypertension 37:176–181, 2001
10. Jannetta PJ: Observations on the etiology of trigeminal neu-ralgia, hemifacial spasm, acoustic nerve dysfunction and glossopharyngeal neuralgia: definitive microsurgical treat-ment and results in 177 patients. Neurochirurgia (Stuttg) 20:145–154, 1977
11. Karibe H, Shirane R, Yoshimoto T: Preoperative visualiza-tion of microvascular compression of crainal nerve IX using constructive interference in steady state magnetic resonance imaging in glossopharyngeal neuralgia. J Clin Neurosci 11:679–681, 2004
12. Katsuta T, Rhoton AL Jr, Matsushima T: The jugular foramen: Microsurgical anatomy and operative approaches. Neurosur-gery 41:149–201, 1997
13. Kawahara N, Sasaki T, Nibu K, Sugasawa M, Ichimura K, Na-katsuka T, et al: Dumbbell type jugular foramen meningioma extending both into the posterior cranial fossa and into the parapharyngeal space: report of 2 cases with vascular recon-struction. Acta Neurochir (Wien) 140:330–331, 1998
14. Kleineberg B, Becker H, Gaab MR, Naraghi R: Essential hy-pertension associated with neurovascular compression: angio-graphic findings. Neurosurgery 30:834–841, 1992
15. Kondo A: Follow-up results of using microvascular decom-pression for treatment of glossopharyngeal neuralgia. J Neu-rosurg 88:221–225, 1998
16. Korogi Y, Nagahiro S, Du C, Sakamoto Y, Takada A, Ushio Y, et al: Evaluation of vascular compression in trigeminal neu-ralgia by 3D time-of-flight MRA. J Comput Assist Tomogr 19:879–884, 1995
17. Lachman N, Acland RD, Rosse C: Anatomical evidence for the absence of a morphologically distinct cranial root of the accessory nerve in man. Clin Anat 15:4–10, 2002
18. Laha RK, Jannetta PJ: Glossopharyngeal neuralgia. J Neuro-surg 47:316–320, 1977
19. Lang J: [Anatomy, length and blood vessel relations of “cen-tral” and “peripheral” paths of intracisternal cranial nerves.] Zentralbl Neurochir 43:217–258, 1982 (Ger)
20. Lang J: Clinical Anatomy of the Head: Neurocranium, Or-bit, Craniocervical Region. Berlin: Springer-Verlag, 1983
21. Lang J: [Neuroanatomy of the optic, trigeminal, facial, glosso-pharyngeal, vagus, accessory and hypoglossal nerves (author’s transl).] Arch Otorhinolaryngol 231:1–69, 1981 (Ger)
22. Lang J, Reiter U: [Intracisternal length of cranial nerves 7-12.] Neurochirurgia (Stuttg) 28:153–157, 1985 (Ger)
23. Murali R, Chandy MJ, Rajshekhar V: Neurovascular relation-ships of the root entry zone of lower cranial nerves: a micro-surgical anatomic study in fresh cadavers. Br J Neurosurg 5: 349–356, 1991
24. Naraghi R, Hastreiter P, Tomandl B, Bonk A, Huk W, Fahl-busch R: Three-dimensional visualization of neurovascular relationships in the posterior fossa: technique and clinical ap-plication. J Neurosurg 100:1025–1035, 2004
25. Occhiogrosso M, De Tommasi A, Vailati G: Glossopharyn-geal neuralgia due to exuberant choroid plexus. Surg Neurol 13:459–461, 1980
26. Özveren MF, Türe U: The microsurgical anatomy of the glos-so pharyngeal nerve with respect to the jugular foramen le-sions. Neurosurg Focus 17(2):E3, 2004
27. Özveren MF, Türe U, Özek MM, Pamir MN: Anatomic land-marks of the glossopharyngeal nerve: A microsurgical ana-tomic study. Neurosurgery 52:1400–1410, 2003
28. Peker S, Kurtkaya O, Uzün I, Pamir MN: Microanatomy of the central myelin-peripheral myelin transition zone of the trigeminal nerve. Neurosurgery 59:354–359, 2006
29. Rhoton AL Jr: The cerebellopontine angle and posterior fossa cranial nerves by the retrosigmoid approach. Neurosurgery 47 (3 Suppl):93–129, 2000
30. Rhoton AL Jr: The foramen magnum. Neurosurgery 47 (3 Sup pl):S155–S193, 2000
31. Rhoton AL Jr: Jugular foramen. Neurosurgery 47 (3 Suppl):S267–S285, 2000
32. Rhoton AL Jr, Buza R: Microsurgical anatomy of the jugular foramen. Neurosurgery 42:541–550, 1975
33. Säglitz SA, Gaab MR: Investigations using magnetic reso-nance imaging: is neurovascular compression present in pa-tients with essential hypertension? J Neurosurg 96:1006–1012, 2002
34. Schmitz SA, Hohenbleicher H, Koennecke H-C, Offermann R, Offermann J, Branding G, et al: Neurogenic hypertension: a new MRI protocol for the evaluation of neurovascular com-

J. Neurosurg. / Volume 110 / May 2009
Magnetic resonance imaging–demonstrated anatomy of the cranial nerves
1041
pression of the cranial nerves IX and X root-entry zone. In-vest Radiol 34:774–780, 1999
35. Seitz J, Held P, Fründ R, Strotzer M, Nitz WR, Völk M, et al: Visualization of the IXth to XIIth cranial nerves using 3-di-mensional constructive interference in steady state, 3-dimen-sional magnetization-prepared rapid gradient echo and T2-weighted 2-dimensional turbo spin echo magnetic resonance imaging sequences. J Neuroimaging 11:160–164, 2001
36. Shigematsu Y, Korogi Y, Hirai T, Okuda T, Ikushima I, Suga-hara T, et al: Contrast-enhanced CISS MRI of vestibular schwannomas: phantom and clinical studies. J Comput As-sist Tomogr 23:224–231, 1999
37. Shima F, Fukui M, Kitamura K, Kuromatsu C, Okamura T: Diagnosis and surgical treatment of spasmodic torticollis of 11th nerve origin. Neurosurgery 22:358–363, 1988
38. Sindou M, Mertens P: Microsurgical vascular decompression (MVD) in trigeminal and glosso-vago-pharyngeal neuralgias. A twenty year experience. Acta Neurochir Suppl (Wien) 58:168–170, 1993
39. Tomii M, Onoue H, Yasue M, Tokudome S, Abe T: Micro-scopic measurement of the facial nerve root exit zone from glial myelin to peripheral Schwann cell myelin. J Neurosurg 99:121–124, 2003
40. Wiles CCR, Wrigley B, Greene JRT: Re-examination of the medullary rootlets of the accessory and vagus nerves. Clin Anat 20:19–22, 2007
41. Yousry I, Camelio S, Schmid UD, Horsfield MA, Wiesmann M, Bruckmann H, et al: Visualization of cranial nerves I-XII: value of 3D-CISS and T2-weighted FSE sequences. Eur Ra-diol 10:1061–1067, 2000
42. Yousry I, Camelio S, Wiesmann M, Moriggl B, Bruckmann H, Yousry TA: Detailed magnetic resonance imaging anatomy of the cisternal segment of the abducent nerve: Dorello’s ca-nal, neurovascular relationships and landmarks. J Neurosurg 91:276–283, 1999
43. Yousry I, Dieterich M, Naidich TP, Schmid UD, Yousry TA:
Superior oblique myokymia: magnetic resonance imaging support for the neurovascular compression hypothesis. Ann Neurol 51:361–368, 2002
44. Yousry I, Moriggl B, Dieterich M, Naidich TP, Schmid UD, Yousry TA: MR anatomy of the proximal cisternal segment of the trochlear nerve: neurovascular relationships and land-marks. Radiology 223:31–38, 2002
45. Yousry I, Moriggl B, Schmid UD, Naidich TP, Yousry TA: De-tailed anatomy of the intracranial segment of the hypoglossal nerve: neurovascular relationships and landmarks on magnet-ic resonance imaging sequences. J Neurosurg 96:1113–1122, 2002
46. Yousry I, Moriggl B, Schmid UD, Naidich TP, Yousry TA: De-tailed anatomy of the motor and sensory roots of the trigemi-nal nerve and their neurovascular relationships. J Neurosurg 101:427–434, 2004
47. Yousry I, Muacevic A, Olteanu-Nerbe V, Naidich TP, Yousry TA: Exophytic pilocytic astrocytoma of the brain stem in an adult with encasement of the caudal cranial nerve complex (IX–XII): presurgical anatomical neuroimaging using MRI. Eur Radiol 14:1169–1173, 2004
48. Zausinger S, Yousry I, Bruckmann H, Schmid-Elsaesser R, Tonn JC: Cavernous malformations of the brain stem: three-dimensional-constructive interference in steady-state magnet-ic resonance imaging for improvement of surgical approach and clinical results. Neurosurgery 58:322–330, 2006
Manuscript submitted October 26, 2007.Accepted March 25, 2008.Please include this information when citing this paper: published
online January 30, 2009; DOI: 10.3171/2008.3.JNS17472.Address correspondence to: Jennifer Linn, M.D., Department
of Neuroradiology, Klinikum Grosshadern, Marchioninistrasse 15, D-81377 Munich, Germany. email: [email protected].