Circulating Tumor DNA Clinical Application -...
36
Role of liquid biopsies and circulating tumor DNA Pierre Laurent-Puig European Georges Pompidou Hospital Paris Descartes University
Transcript of Circulating Tumor DNA Clinical Application -...
Role of liquid biopsies and circulating tumor DNA
Pierre Laurent-Puig
European Georges Pompidou Hospital
Paris Descartes University
DISCLOSURE
AMGEN
ASTRAZENECA
BIOCARTIS
BOERINGHER INGELHEIM
INTEGRAGEN
MERCK SERONO
RAINDANCE TECHNOLOGIES NOT yet BIORAD
ROCHE
SANOFI
Detection of circulating tumor DNA• By searching for the genetic or epigenetic alterations which
characterize the DNA coming from tumor cells
• Tumor specific mutations
• Tumor specific structural changes (i.e. rearrangement)
• Copy Number Variations
• MicroRNA
• Methylated DNA
Zonta et al. Advances in Clinical Chemistry, Volume 70, 2015, Pages 197-246
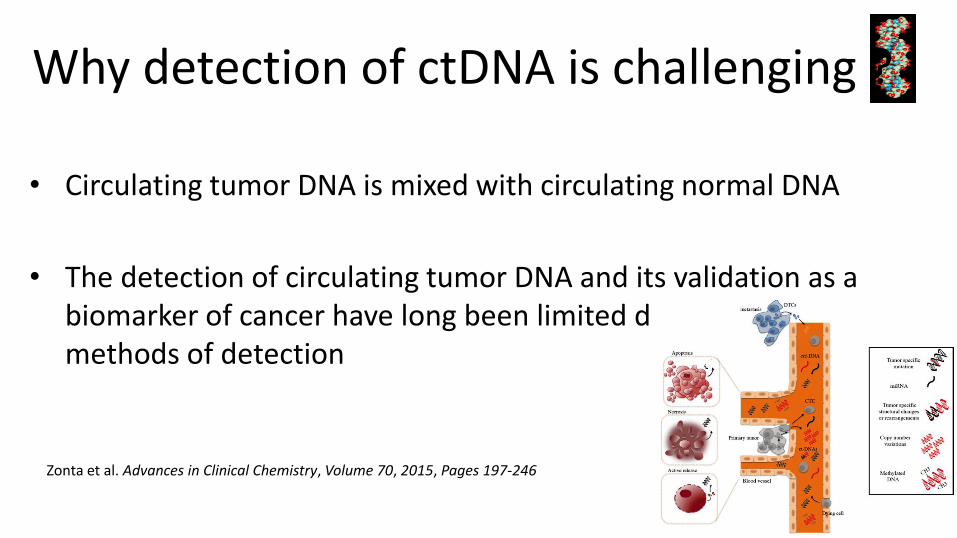
Why detection of ctDNA is challenging ?
• Circulating tumor DNA is mixed with circulating normal DNA
• The detection of circulating tumor DNA and its validation as a biomarker of cancer have long been limited due to inefficient methods of detection
Zonta et al. Advances in Clinical Chemistry, Volume 70, 2015, Pages 197-246
0.001
0.01
0.1
1
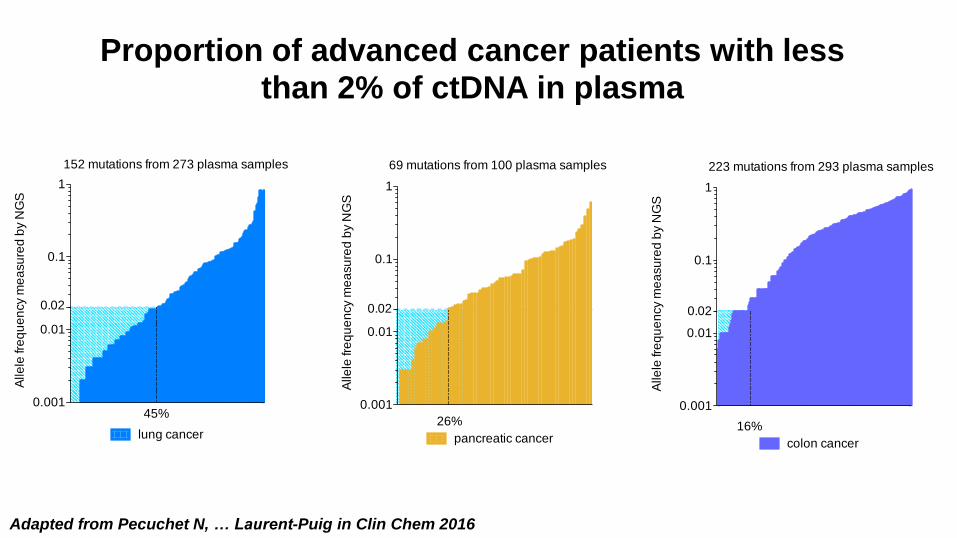
colon cancer
16%
0.02
Alle
le fr
eq
ue
ncy m
ea
su
red
by N
GS
223 mutations from 293 plasma samples
0.001
0.01
0.1
1
pancreatic cancer
69 mutations from 100 plasma samples
26%
0.02
Alle
le fr
eq
ue
ncy m
ea
su
red
by N
GS
0.001
0.01
0.1
1
lung cancer
152 mutations from 273 plasma samples
45%
0.02
Alle
le fr
eq
ue
ncy m
ea
su
red
by N
GS
Adapted from Pecuchet N, … Laurent-Puig in Clin Chem 2016
Proportion of advanced cancer patients with lessthan 2% of ctDNA in plasma
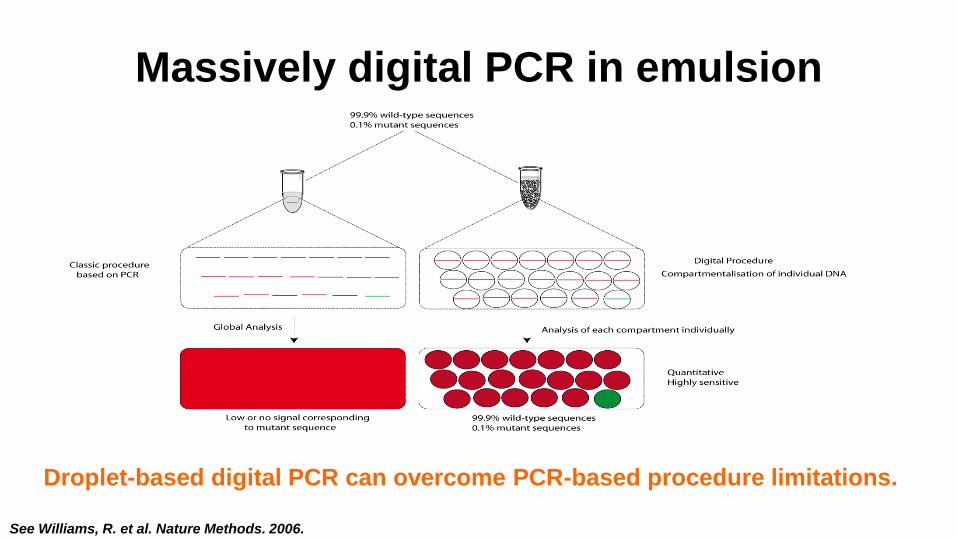
Massively digital PCR in emulsion
Droplet-based digital PCR can overcome PCR-based procedure limitations.
See Williams, R. et al. Nature Methods. 2006.
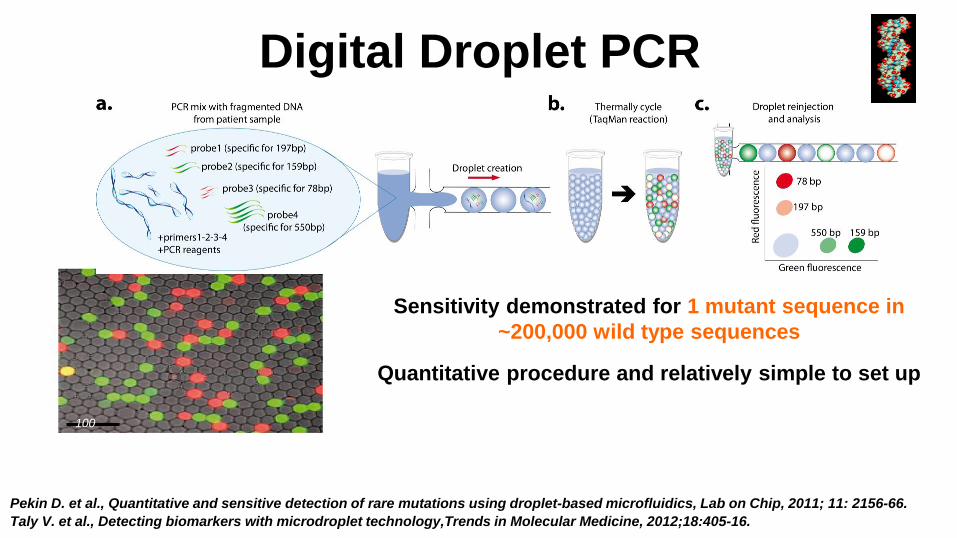
Digital Droplet PCR
100 µm
Pekin D. et al., Quantitative and sensitive detection of rare mutations using droplet-based microfluidics, Lab on Chip, 2011; 11: 2156-66.
Taly V. et al., Detecting biomarkers with microdroplet technology,Trends in Molecular Medicine, 2012;18:405-16.
Sensitivity demonstrated for 1 mutant sequence in
~200,000 wild type sequences
Quantitative procedure and relatively simple to set up
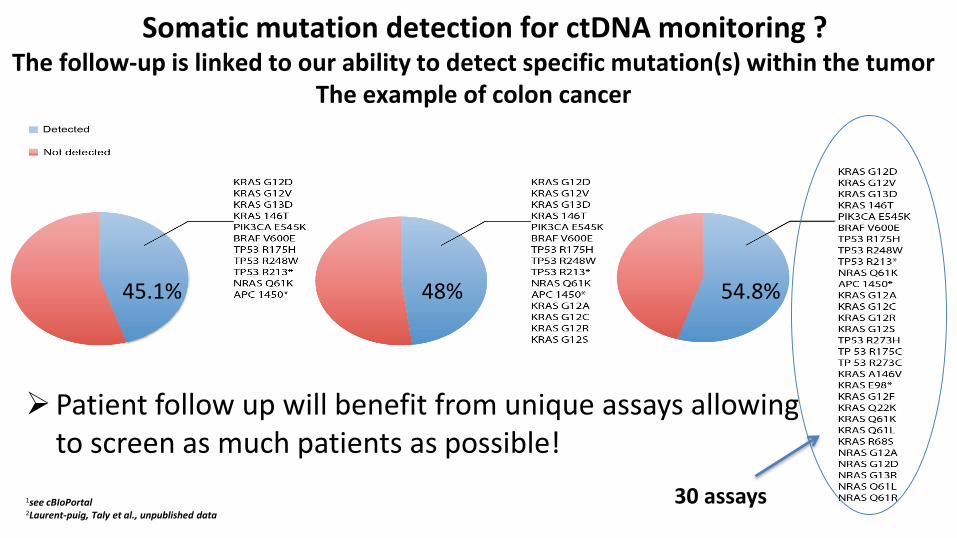
48%45.1% 54.8%
➢Patient follow up will benefit from unique assays allowing to screen as much patients as possible!
30 assays1see cBIoPortal2Laurent-puig, Taly et al., unpublished data
Somatic mutation detection for ctDNA monitoring ?The follow-up is linked to our ability to detect specific mutation(s) within the tumor
The example of colon cancer


Massively parallel sequencing Different methods have been used to improve sensitivity of NGS
CAPP seq, Safe SeqBPER methodCircle sequencing
All these methods tend to improve sensitivity of detection by differentiating true mutation to background noiseLess than 0.1%

First question : is liquid biopsy ready
for colorectal cancer screening ?
THE ANSWER IS NO BUT …..

Adapted from Garrigou S et al. Clin Chem 2016;62
Circulating Tumor DNA according to Tumor stage

SEPT9 methylation as a marker of circulating
tumor DNA 7941 asymptomatic individuals >50 years old
53 cases of colorectal cancers
Sensitivity of the SEPT9 test for CRC : 48.2% CI95% 32.4%-63.6%
Stage I 35%, Stage II 63%, Stage III 46%, Stage IV 77.4%
Specificity of the SEPT9 plasma detection 91.5% CI95% 89.7%-93.1%
Sensitivity for advanced adenoma was low 11.2%
Based on this study FDA approved the test in April 2016 with this labelling « The epi procolon test is
indicated to screen adults of either sex, 50 years or older, defined as average risk for crc, who have
been offered and have a history of not completing crc screening. The Epi proColon test is not
intended to replace colorectal cancer screening tests that are recommended by appropriate
guidelines »
Church TR et al. Gut 2014;63:315-325
Second question :
Is the liquid biopsy ready to search for the RAS
gene mutations?
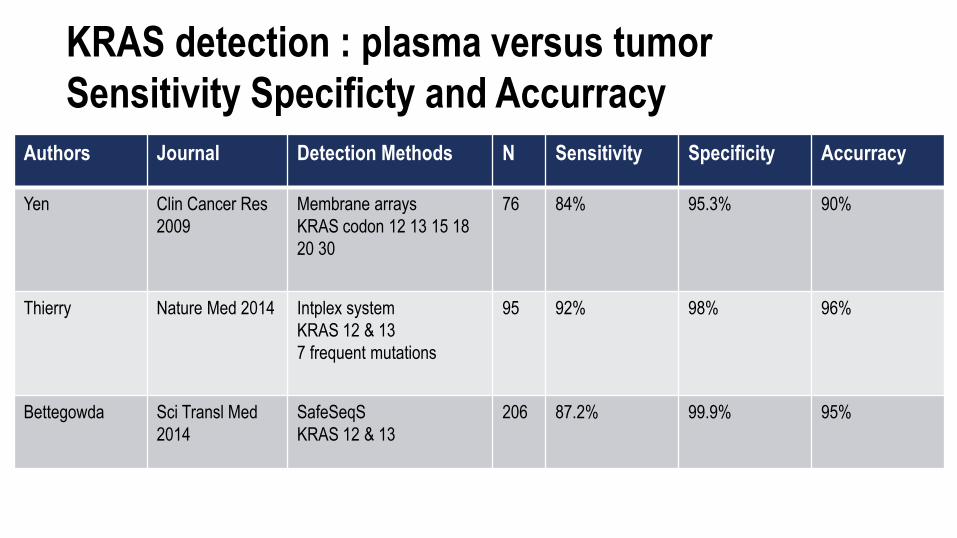
KRAS detection : plasma versus tumor
Sensitivity Specificty and Accurracy
Authors Journal Detection Methods N Sensitivity Specificity Accurracy
Yen Clin Cancer Res
2009
Membrane arrays
KRAS codon 12 13 15 18
20 30
76 84% 95.3% 90%
Thierry Nature Med 2014 Intplex system
KRAS 12 & 13
7 frequent mutations
95 92% 98% 96%
Bettegowda Sci Transl Med
2014
SafeSeqS
KRAS 12 & 13
206 87.2% 99.9% 95%
Second question :
Is the liquid biopsy ready to search for the RAS
gene mutations?
THE ANSWER IS PROBABLY YES waiting for
prospective series in all RAS mutation
Second question :
Is the liquid biopsy ready to search for the RAS
gene mutations?
THE ANSWER IS PROBABLY YES waiting for
prospective series in all RAS mutation
So we do it

RASANC study
• Prospective biospecimen collection study in previously untreated advanced mCRC(NCT02502656)
• AGEO French collaborative study
• Plasma collected in Streck tubes
• Plasma NGS performed using established panel
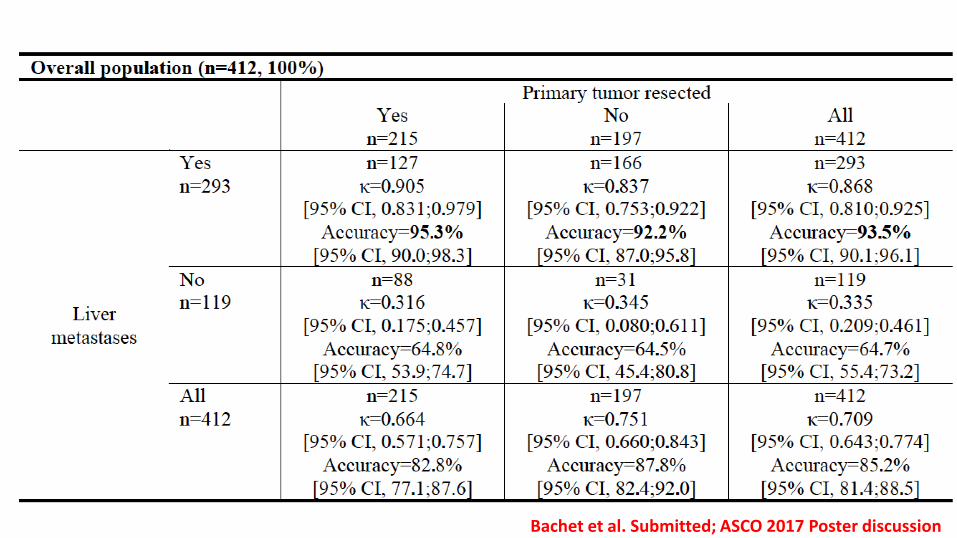
Bachet et al. Submitted; ASCO 2017 Poster discussion
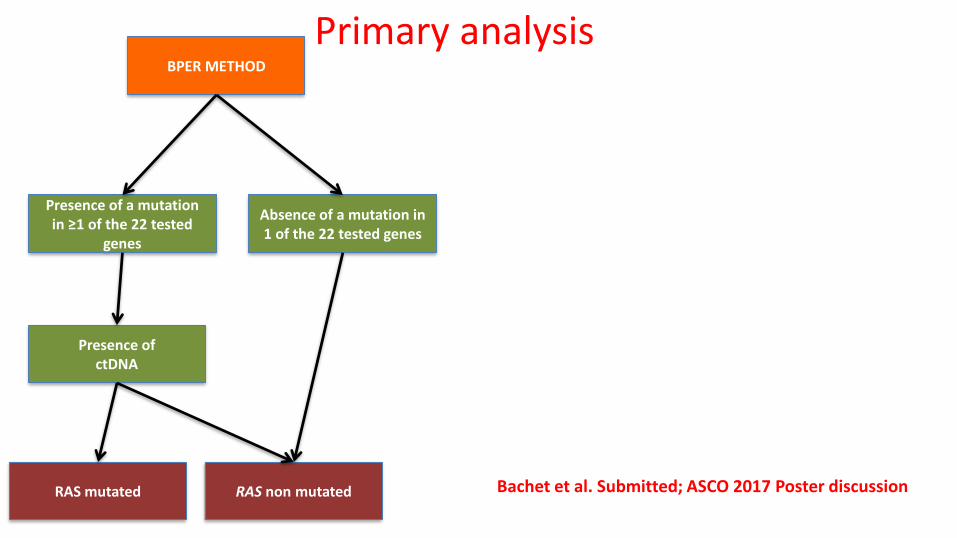
BPER METHOD
Presence of a mutation in ≥1 of the 22 tested
genes
Presence of ctDNA
RAS mutated RAS non mutated Bachet et al. Submitted; ASCO 2017 Poster discussion
Absence of a mutation in 1 of the 22 tested genes
Primary analysis

BPER METHOD
Presence of a mutation in ≥1 of the 22 tested
genes
Presence of ctDNA
RAS mutatedN=187 (45.4%)
RAS non mutatedN=225 (56.4%) Bachet et al. Submitted; ASCO 2017 Poster discussion
Absence of a mutation in 1 of the 22 tested genes
RAS mutation in plasma sample
Absence No.
Presence No.
Total No.
RA
Sm
utatio
n in
tu
mo
r
AbsenceNo.
167(41%)
3(1%)
170 (41%)
Presence No.
58 (14%)
184 (45%)
242 (59%)
Total No.225
(55%)187
(45%)412 (100%)
Primary analysis
BPER METHOD
Presence of a mutation in ≥1 of the 22 tested
genes
Presence of ctDNA
RAS mutatedN=187 (45.4%)
RAS non mutatedN=142(43%)
Bachet et al. Submitted; ASCO 2017 Poster discussion
Absence of a mutation in 1 of the 22 tested genes
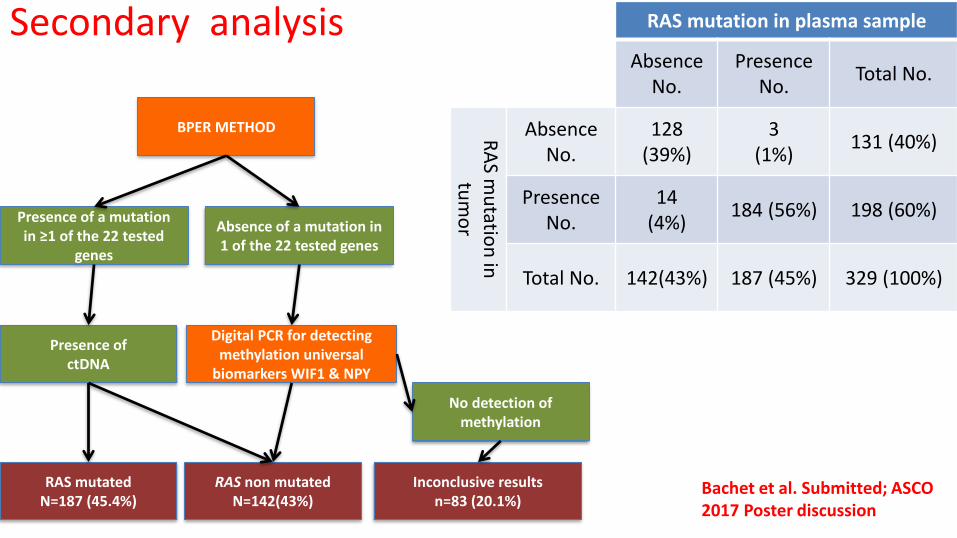
Secondary analysis
Digital PCR for detecting methylation universal
biomarkers WIF1 & NPY
No detection of methylation
Inconclusive resultsn=83 (20.1%)
RAS mutation in plasma sample
Absence No.
Presence No.
Total No.
RA
Sm
utatio
n in
tu
mo
r
AbsenceNo.
128(39%)
3(1%)
131 (40%)
Presence No.
14 (4%)
184 (56%) 198 (60%)
Total No. 142(43%) 187 (45%) 329 (100%)
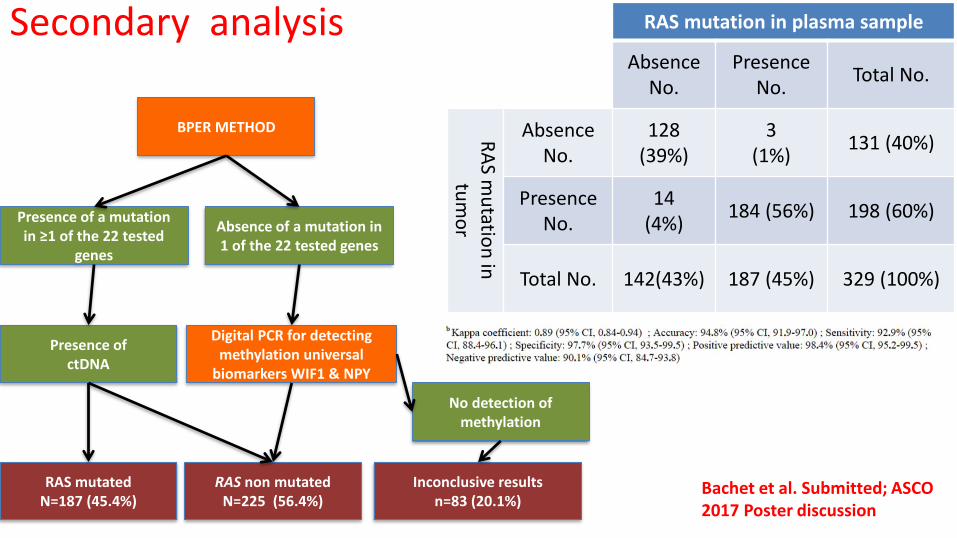
BPER METHOD
Presence of a mutation in ≥1 of the 22 tested
genes
Presence of ctDNA
RAS mutatedN=187 (45.4%)
RAS non mutatedN=225 (56.4%)
Bachet et al. Submitted; ASCO 2017 Poster discussion
Absence of a mutation in 1 of the 22 tested genes
Secondary analysis
Digital PCR for detecting methylation universal
biomarkers WIF1 & NPY
No detection of methylation
Inconclusive resultsn=83 (20.1%)
RAS mutation in plasma sample
Absence No.
Presence No.
Total No.
RA
Sm
utatio
n in
tu
mo
r
AbsenceNo.
128(39%)
3(1%)
131 (40%)
Presence No.
14 (4%)
184 (56%) 198 (60%)
Total No. 142(43%) 187 (45%) 329 (100%)
Bachet et al: RASANC study• Tumor DNA shed is
related to a range of clinical and biologic factors
• Thus, this is a tool that is most effective when used in the right patients
Bachet et al. Submitted; ASCO 2017 Poster discussion

Bachet et al: RASANC study• Tumor DNA shed is
related to a range of clinical and biologic factors
• Thus, this is a tool that is most effective when used in the right patients
Bachet et al. Submitted; ASCO 2017 Poster discussion
Third question: Is the liquid biopsy a
prognostic marker for colorectal cancer in early
and advanced stage?
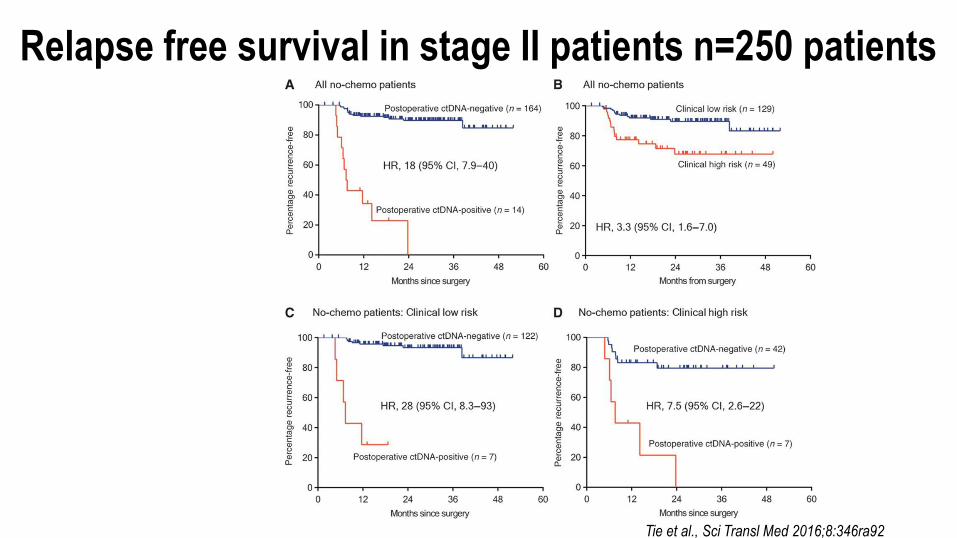
Tie et al., Sci Transl Med 2016;8:346ra92Published by AAAS
Relapse free survival in stage II patients n=250 patients
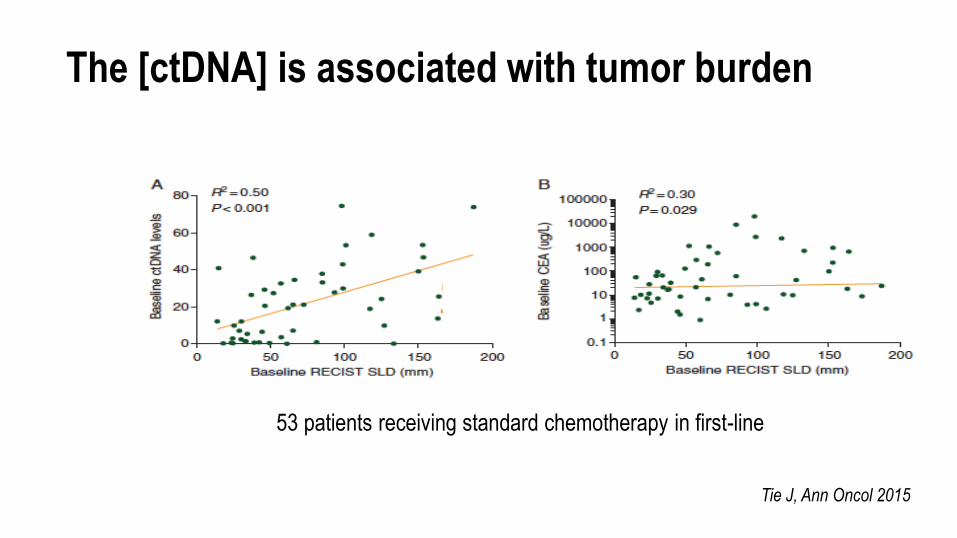
The [ctDNA] is associated with tumor burden
Tie J, Ann Oncol 2015
53 patients receiving standard chemotherapy in first-line
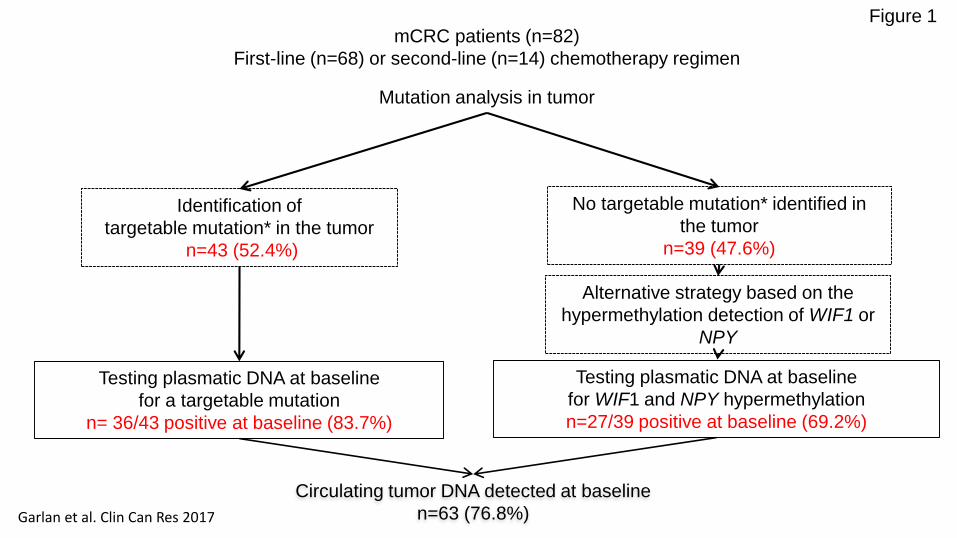
mCRC patients (n=82)
First-line (n=68) or second-line (n=14) chemotherapy regimen
Mutation analysis in tumor
Identification of
targetable mutation* in the tumor
n=43 (52.4%)
No targetable mutation* identified in
the tumor
n=39 (47.6%)
Circulating tumor DNA detected at baseline
n=63 (76.8%)
Testing plasmatic DNA at baseline
for WIF1 and NPY hypermethylation
n=27/39 positive at baseline (69.2%)
Testing plasmatic DNA at baseline
for a targetable mutation
n= 36/43 positive at baseline (83.7%)
Alternative strategy based on the
hypermethylation detection of WIF1 or
NPY
Figure 1
Garlan et al. Clin Can Res 2017
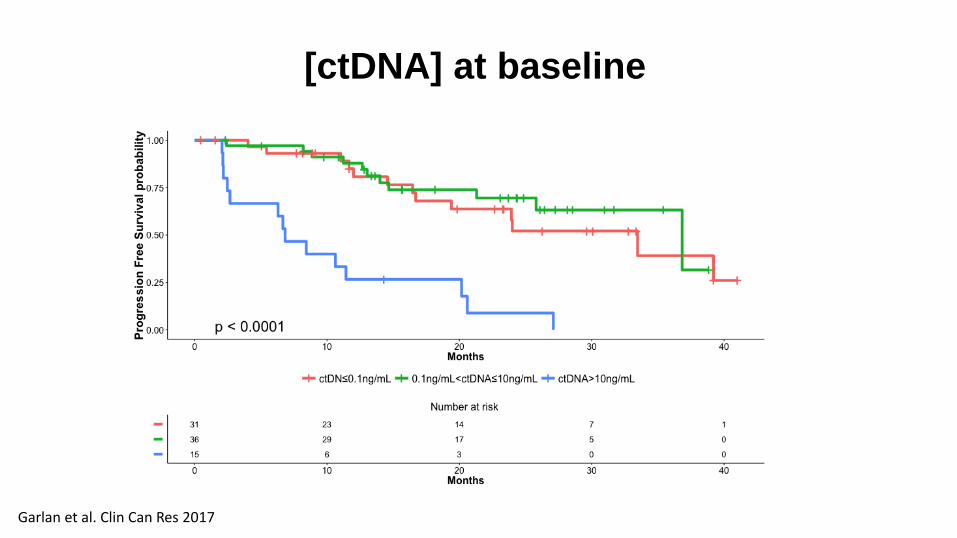
[ctDNA] at baseline
Garlan et al. Clin Can Res 2017
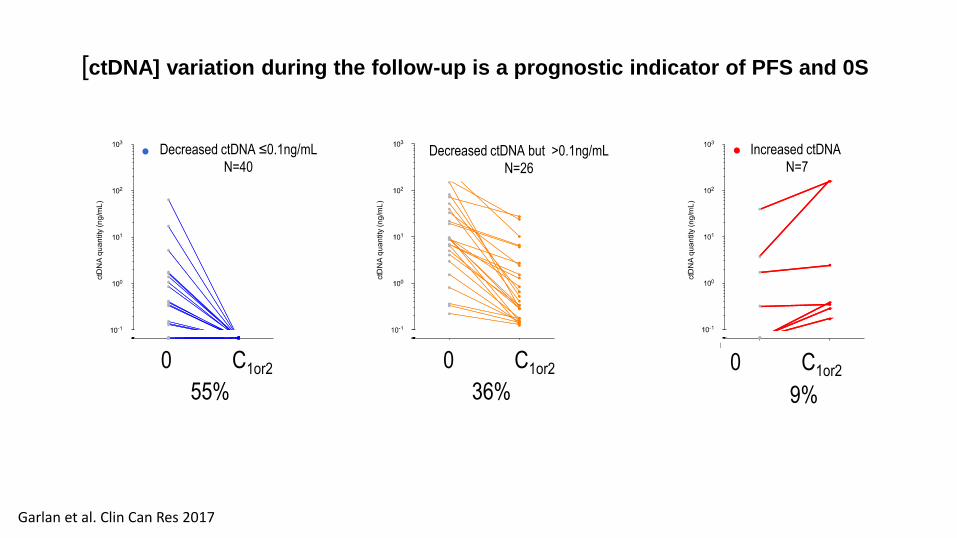
55% 36% 9%
Decreased ctDNA ≤0.1ng/mL
N=40Decreased ctDNA but >0.1ng/mL
N=26
Increased ctDNA
N=7
0 C1or20 C1or2 0 C1or2
[ctDNA] variation during the follow-up is a prognostic indicator of PFS and 0S
Garlan et al. Clin Can Res 2017

[ctDNA] variation during the follow-up is a prognostic indicator of PFS and 0S
Garlan et al. Clin Can Res 2017

55% 36% 9%
Decreased ctDNA ≤0.1ng/mL
N=40Decreased ctDNA but >0.1ng/mL
N=26
Increased ctDNA
N=7
0 C1or20 C1or2 0 C1or2
[ctDNA] variation during the follow-up is a prognostic indicator of PFS and 0S
Garlan et al. Clin Can Res 2017
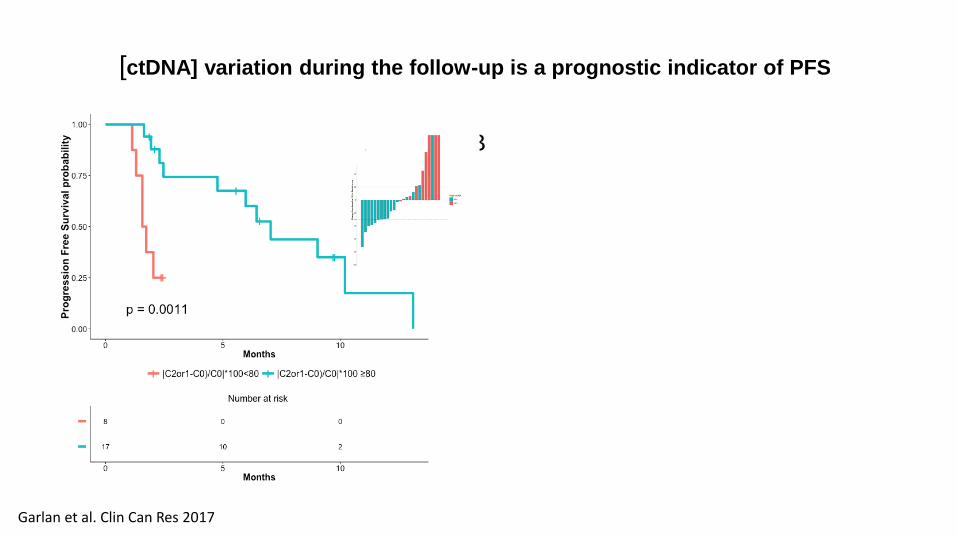
[ctDNA] variation during the follow-up is a prognostic indicator of PFS
A B
Garlan et al. Clin Can Res 2017
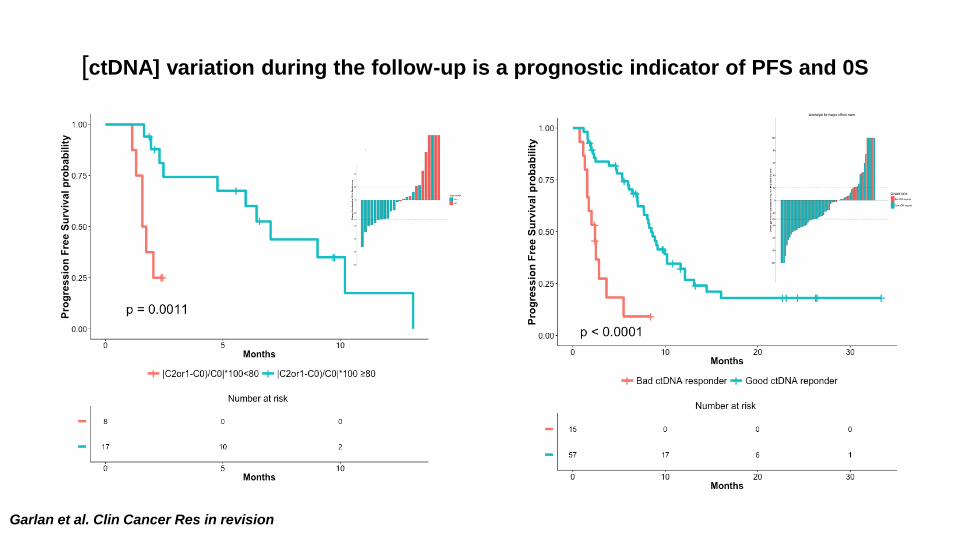
Garlan et al. Clin Cancer Res in revision
[ctDNA] variation during the follow-up is a prognostic indicator of PFS and 0S
A B
Conclusions Improvement of methods for detecting ctDNA allows them to be
used in a clinical setting
The presence of ctDNA in early stage cancer after surgery is an
indicator of early recurrence
Quantification of ctDNA is a probably a surrogate marker of tumor
burden and therefore a prognostic marker in advanced stage
Evolution of ctDNA concentration under treatment is likely an early
indicator of chemotherapy efficacy
Finally, ctDNA allows the identification of resistance mutation and
could be a decision-making tool
Oncologists, pathologists and biostaticians
Prof. O. BouchéDr. B. LandiProf. JF. EmileDr F. Bibaut
Thanks to...
Fundings- Supports
Institut National pour la recherche sur le Cancer (INCa)
Association pour la Recherche contre le Cancer (ARC)
Région Alsace
Université de Strasbourg
Centre National de la Recherche Scientifique (CNRS)
Institut National de la santé et la recherche médicale (INSERM)
Université Paris-Descartes
Hopital Européen Georges Pompidou (hEGP)
Agence Nationale de la recherche (ANR)
UMRS-1147/ UdS
V. TalyJB BachetL. BenhaimDr H. BlonsDr V. BoigeA. DidelotDr E. FabreF. GarlanS. GarrigouT. HorD. Le CorreDr P. NizardC. NormandDr N. Pecuchet
Dr D. PekinDr K. Perez TorallaDr Y. SkhiriDr A. ZaananDr E. Zonta
RainDance Technologies
Dr D. LinkDr B. HutchisonJ. OlsonS. KotsopoulosQ. ZhongI. Atochin
X. Li A. CornerC. MilburyM. Samuels
R. NiarraP. AucouturierG. ChatellierDr Y. Rozenholc