
CIRCULAT in Chronic Ischemic Heart Disease - 20 Pat, Diabetic Foot and Gene Expression
95
CIRCULAT IN CIRCULAT IN CHRONIC ISCHEMIC CHRONIC ISCHEMIC HEART DISEASE HEART DISEASE
-
Upload
ischemic-cardiopathy -
Category
Health & Medicine
-
view
481 -
download
1
Transcript of CIRCULAT in Chronic Ischemic Heart Disease - 20 Pat, Diabetic Foot and Gene Expression
CIRCULAT IN CIRCULAT IN CHRONIC ISCHEMIC CHRONIC ISCHEMIC
HEART DISEASEHEART DISEASE

Centro Médico Docente AdaptógenoWho are we ?
• Most widespread private medical network (Vzla);
• Application of a proprietary therapeutic solution
(Systemic Medicine);
• 150 orthodox medical doctors;
• 45 Medical Centers and Units (Vzla); and Puerto Rico (3);
• Overseen > 1 mill. patients (2002-10).
Puerto Rico
Venezuela

Genetic Modulator

• CIRCULAT as a Gene expression modulator
• CIRCULAT in Diabetic Foot Management
• CIRCULAT in Chronic Ischemic Heart Disease
CIRCULAT Background Studies

Pennsylvania State University, 2007
Faculty of Medicine
187 modulated genes
with Circulat
August, 2007
STUDY

Evaluation of the changes in the Evaluation of the changes in the genetic expression after genetic expression after
CIRCULATCIRCULAT
Objective: Objective: To reveal the underlying molecular mechanisms to the To reveal the underlying molecular mechanisms to the
biological activity of the Circulatbiological activity of the Circulat. .

Gene Expression
HIGHLIGHTSModulation of Genes Associated
with the origin of Diabetes
• IL6: inflammatory mediator, glucose regulator in pancreatic beta cells
• HMGA1: Counters insulin resistance• SLC19A2: Associated with Diabetes
pathogenesis• C4A: Associated with diabetes origin

HIGHLIGHTSModulation of Genes Associated
with the origin of Cardiopathy
• TRPM2: Atherosclerosis• ATP5F1: ATP Sinthesys • CYP3A4: Oxidative Phosphorilation• NMNAT2: Anaerobic Glycolysis

Modulation of 24 Pathological Genes• PGK1 Hemolytic anemia due to PGK deficiency Myoglobinuria/hemolysis due to PGK deficiency• MYO1A Deafness, autosomal dominant no nsyndromic sensorineural• PRKAR1A Adrenocortical tumor, somatic Carney complex, type 1 Myxoma, intracardiac Pigmented
adrenocortical disease, primary isolated Thyroid carcinoma, papillary• AHI1 Joubert syndrome-3• SYN2 Schizophrenia, susceptibility to C4A• UROD Porphyria cutanea tarda Porphyria, hepatoerythropoietic• WNK1 Pseudo-hypo-aldosteronism, type II• NR4A3 Chondrosarcoma, extraskeletal myxoid • RAB7 Charcot-Marie-Tooth disease, type 2B • IL6 Diabetes type 1 and 2 Osteopenia, osteoporosis, Kaposi sarcoma, susceptibility to • SAT Keratosis follicularis spinulosa decalvans• SOCS3 Dermatitis, atopic, 4 • PDE4D Stroke, susceptibility to, 1 • SLC19A2 Diabetes type 2 Thiamine-responsive megaloblastic anemia syndrome • RAB3GAP1 Warburg micro syndrome 1 • ENTH Schizophrenia, susceptibility to• CD55 Blood group Cromer • ALDOB Fructose intolerance • LHX4 Short stature, pituitary and cerebellar defects, and small sella turcica\ Amyotrophic lateral
sclerosis 8Spinal muscular atrophy• VAPB Spinal muscular atrophy, late-onset, Finkel type LPPLeukemia, acute myeloid Lipoma• HMGA1 Diabetes type 2Lipoma• FANCB Fanconi anemia, complementation group B Breast cancer, early onset• BRIP1 Fanconi anemia, complementation group J• C4A Diabetes type 1

CIRCULAT: Gene expression modulator

CIRCULAT in Diabetic Foot Management
• CIRCULAT has been used very successfully in the CMA Network for the treatment of circulatory disorders.
• CIRCULAT achievements in circulatory disorders was also replicated in the treatment of diabetic foot (and varicose ulcers). This warranted a clinical study.
• Thus, a retrospective study was carried out in 174 diabetic foot patients treated between 2004 – 2007.

Publication: 2008
Diabetic Foot Results with Circulat174 patients; 88.5% Efectivety
STUDY

Results Stable Angina Pectoris Estudio realizado en 83 pacientes
Mejoría significativa 85%

Male, 64 years: evolution ‘years’
After 6 month treatment
Clinical Outcomes of Diabetic Foot Management with Circulat(Example of Study’s photographic evidence)

Female, 61 years, evolution ‘months’
After 6 months treatment
Diabetic Foot

Male, 58 years, evolution 6 months
Diabetic Foot
After 4 months’ treatment

After 2 1/2 months of treatment
Male, 56 years, evolution “years”
Diabetic Foot

After 9 months of treatment
Female, 65 years, evolution 15 days
Diabetic Foot

After 3 months of treatment
Female, 59 years, evolution 7 months
Diabetic Foot

Female, 67 years, evolution 2 years. After 7 months of treatment
Diabetic Foot

Female, 61 years, evolution “months”
After 6 months of treatment
Diabetic Foot

After 2 months of treatmentFemale, 49 years, evolution 1 year
Diabetic Foot

After 9 months of treatmentMale, 44 years, evolution 1 month
Diabetic Foot

After 2 months of treatment
Male, 46 years, evolution 4 months.
Diabetic Foot

Male, 62 years. Evolution“years”
After 1 months of treatment
Diabetic Foot

Female, 47 years. Evolution “months”
After 4 months of treatment
Diabetic Foot

Female, 79 years: evolution 2 years
After 6 year treatment
Photographic Evidence Varicose Ulcer

Female, 42 years: evolution 14 months
After 5 month treatment
Photographic Evidence Varicose Ulcer
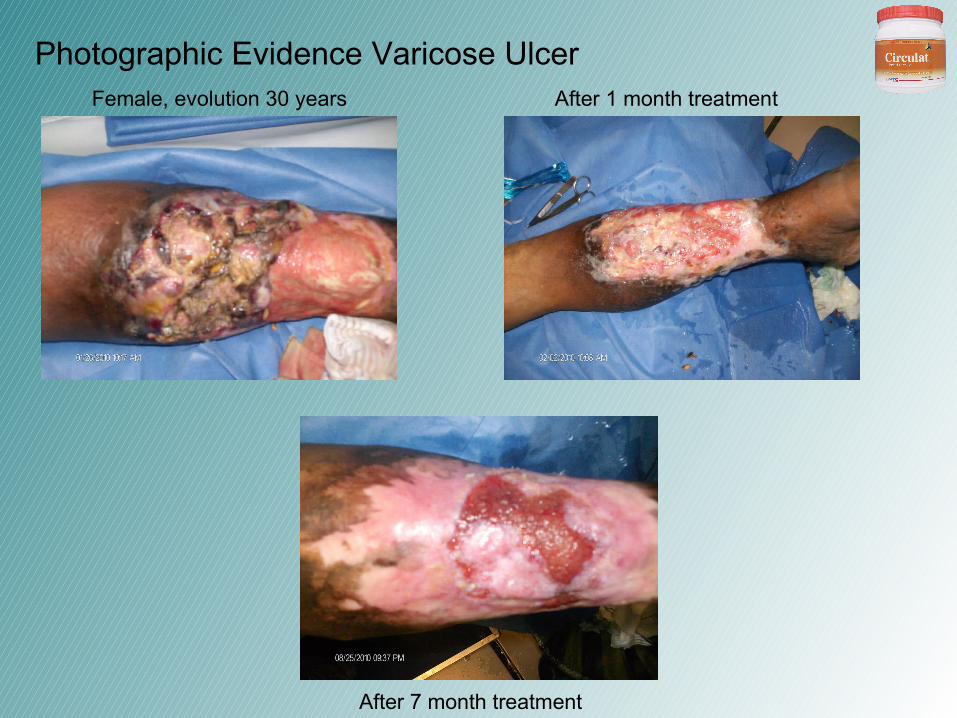
Female, evolution 30 years
Photographic Evidence Varicose Ulcer
After 7 month treatment
After 1 month treatment

Male, evolution 1 years
Photographic Evidence Varicose Ulcer
After 2 month’s treatment

Photographic Evidence Varicose Ulcer
Before After
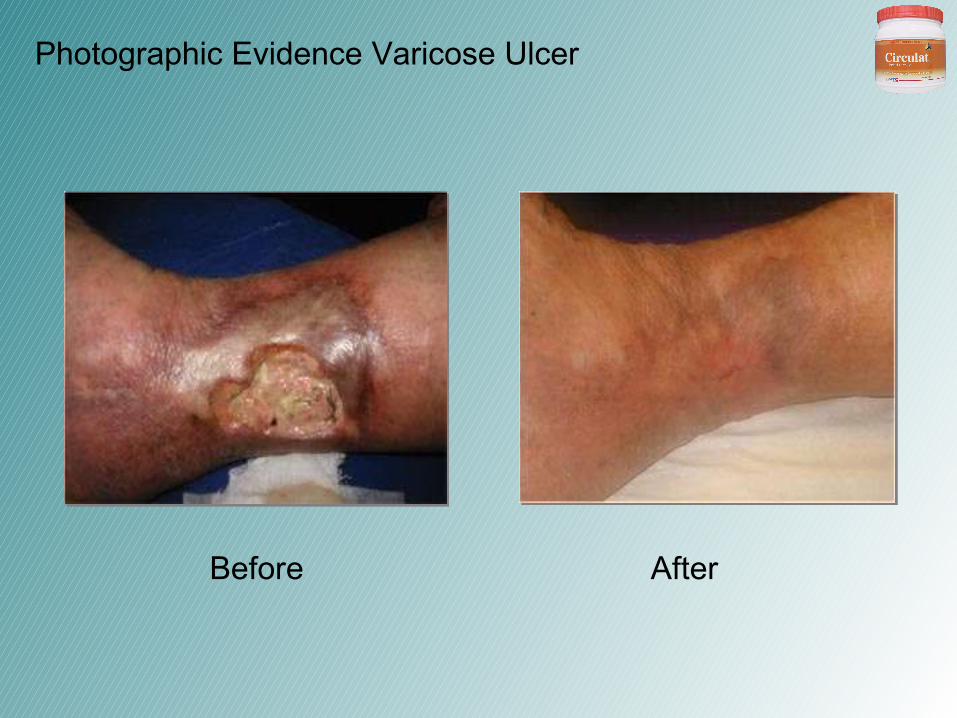
Photographic Evidence Varicose Ulcer
Before After

CMA Lecherías
H.C. 22728
Dra. Luz Méndez
Photographic Evidence Arterial Ulcer
Before After
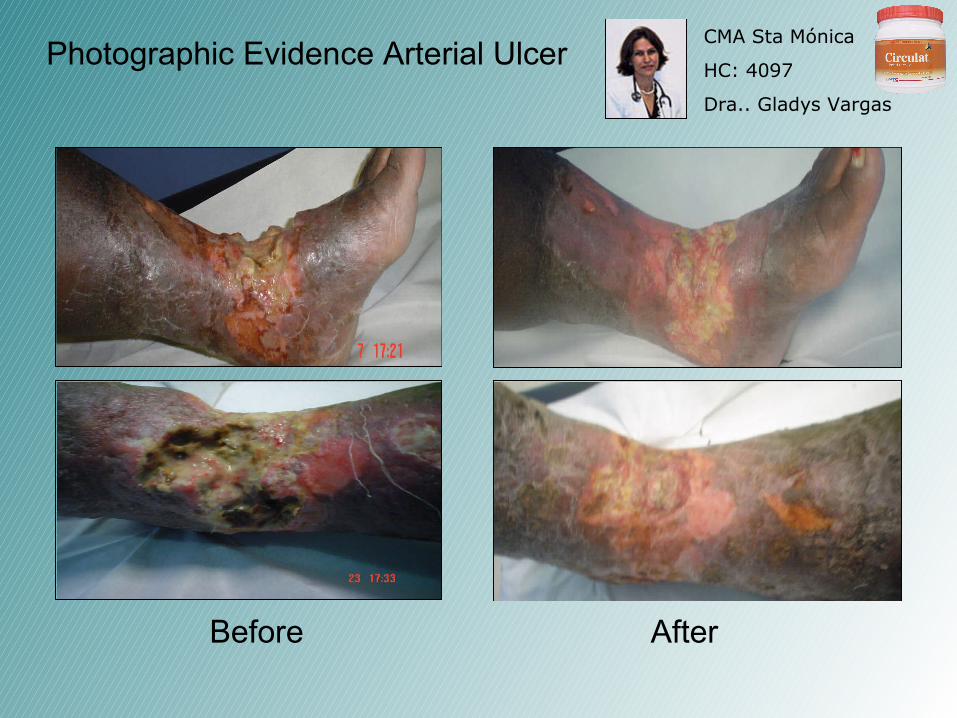
CMA Sta Mónica
HC: 4097
Dra.. Gladys Vargas
Photographic Evidence Arterial Ulcer
Before After

CMA Lechería
H.C. 22.970
Dra.. Luz Méndez
Photographic Evidence Arterial Ulcer
Before After
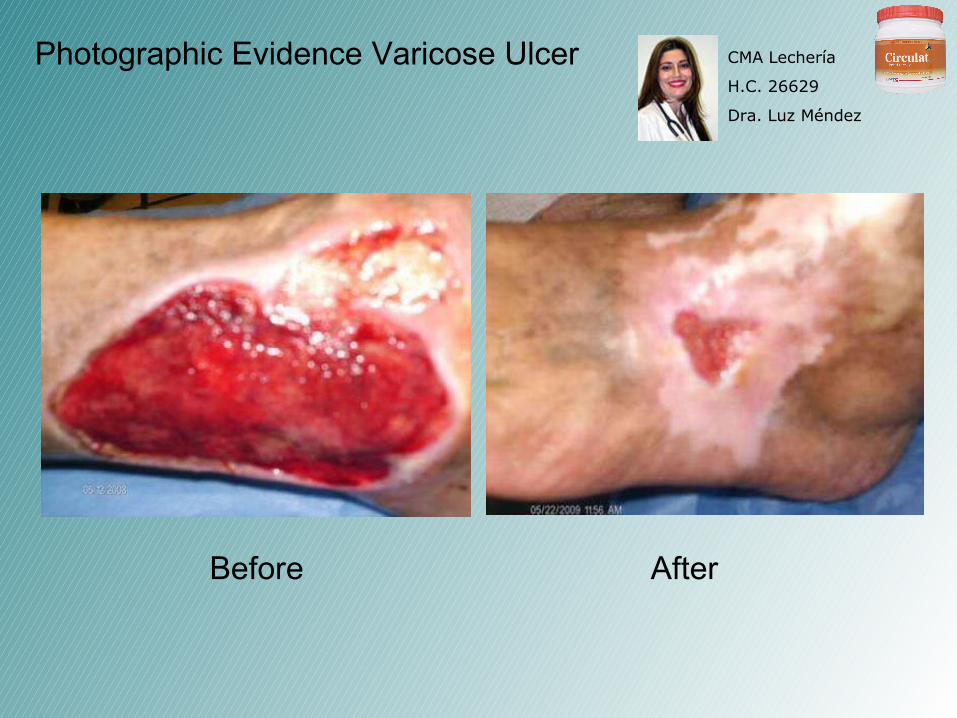
CMA Lechería
H.C. 26629
Dra. Luz Méndez
Photographic Evidence Varicose Ulcer
Before After

CMA SabanaGrande
H.C: 57.394
Dra.: Runi Molina
Photographic Evidence Varicose Ulcer
Before After

CMA Sabana Grande
H.C. 30.195
Dra. Runi Molina
Photographic Evidence Varicose Ulcer
Before
After

CMA Barquisimeto
H.C. 28.212
Dr. Rolando Sequera
Photographic Evidence Varicose Ulcer
Before
After

CMA Lechería
H.C. 26.213
Dra. Magaly Tinoco
Photographic Evidence Varicose Ulcer
Before After

CMA Lechería
H.C. 18970
Dr. Nerio Villalobos
Photographic Evidence Varicose Ulcer
Before After

CMA Lechería
H.C. 19.121
Dra. Mª Osorio
Photographic Evidence Varicose Ulcer
Before After

CMA Lechería
H.C. 12.316
Dr. Wilfredo Sánchez
Photographic Evidence Varicose Ulcer
Before
After

CMA Sabana Grande
H.C. 57.943
Dra. Edith González
Photographic Evidence Varicose Ulcer
Before After

CIRCULAT Study in Chronic Ischemic
Heart Disease
Patrick J. Lynch, 2006

Background: Endothelial Damage
NORMAL ARTERY ATHEROSCLEROTIC PLAQUENARROWED ARTERY
ENDOTHELIUM
SMOOTH MUSCLE
SMOOTH MUSCLECELLS
MACROPHAGESTRANSFORMED
INTO FOAM CELLSLIPIDS, CALCIUM
CELLULAR DEBRIS
FIBROUS CAP.
ENDOTHELIUMDAMAGE
ENDOTHELIALDYSFUNCTION
MECHANICALSTREESS
HYPERTENSION
VASOCONSTRICTION
PERIPHERALVASCULAR RESISTANCE

Relevant Mortality Rates in Venezuela

Chronic Ischemic Heart
Disease GSPECT Assessment
(Independant Lab)
Treadmill
Imaging

Chronic Ischemic Heart
Disease GSPECT Assessment
(Independant Lab)
Assessment

GSPECT Cardio-Diagnostic Imaging(Source: www.yale.edu/imaging/)
Annualized Cardiac Events Risk
Treatment Implications(majority of patients)
<1% risk of cardiac deathand MI
Risk factor modification (RFM) in addition to current regimen
Low risk of cardiac death; Intermediate risk of MI
Aggressive RFM/medicaltreatment
Intermediate-to-high riskof both cardiac death/MI
Catheterization (possiblerevascularization)/RFM
Normal Mildly Normal Moderately / Severely Abnormal
anterior
inferior
septal lat
anterior
inferior
base apex
apex
latseptal
base
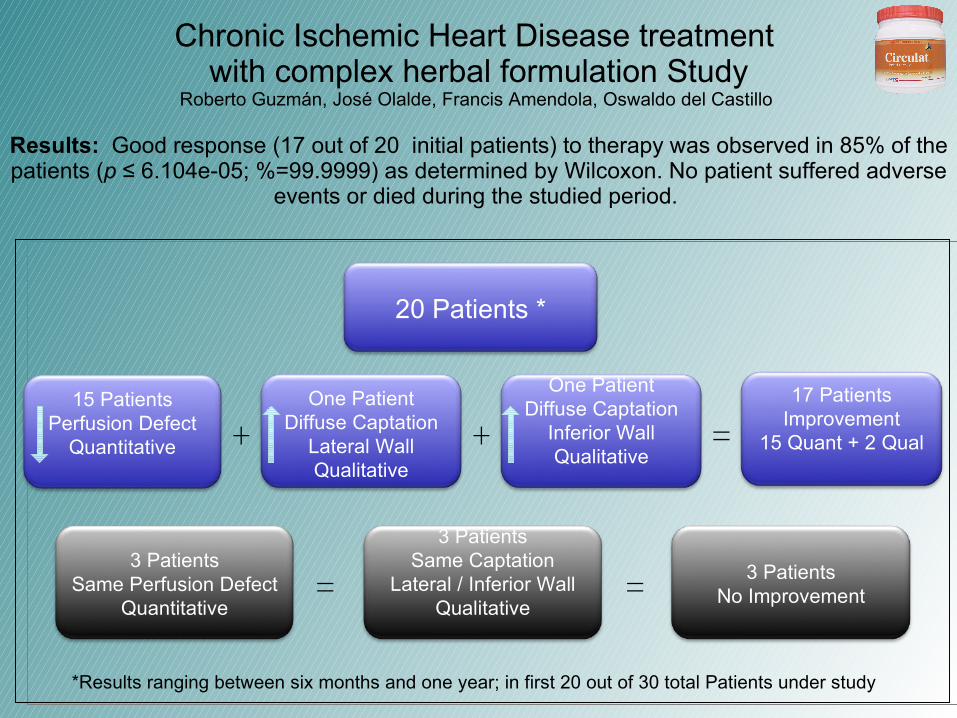
Chronic Ischemic Heart Disease treatment with complex herbal formulation Study
Roberto Guzmán, José Olalde, Francis Amendola, Oswaldo del Castillo
Results: Good response (17 out of 20 initial patients) to therapy was observed in 85% of the patients (p ≤ 6.104e-05; %=99.9999) as determined by Wilcoxon. No patient suffered adverse
events or died during the studied period.
*Results ranging between six months and one year; in first 20 out of 30 total Patients under study
One PatientDiffuse Captation
Lateral WallQualitative
20 Patients *
3 PatientsSame Perfusion Defect
Quantitative
One PatientDiffuse Captation
Inferior WallQualitative
15 PatientsPerfusion Defect
Quantitative
3 PatientsSame Captation
Lateral / Inferior WallQualitative
17 PatientsImprovement
15 Quant + 2 Qual+ + =
3 PatientsNo Improvement= =

Study Aditional Hightlights (1)

Study Aditional Hightlights (2)

PD%: 40
29 APR 2009
16 SEP2009
PD%: Post–Effort Perfusion Damage Percentage
GSPECT Image
PD%: 35
Control
6 months
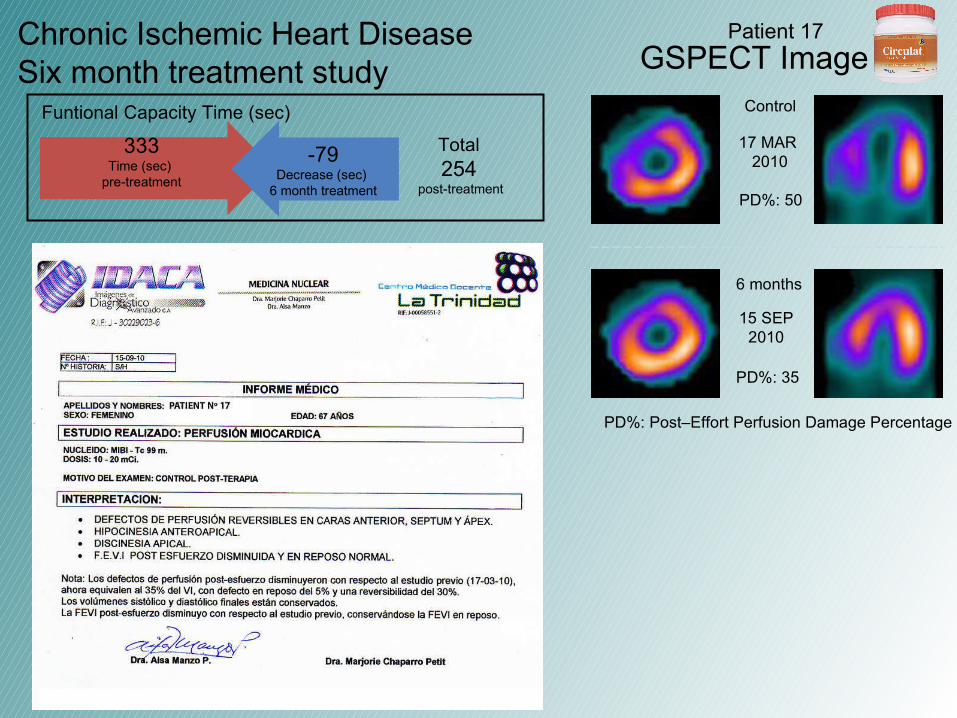
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Total452
post-treatment
386Time (sec)
pre-treatment
66Increase (sec)
6 month treatment
Patient 1

PD%: 45
13 MAY 2009
28 OCT2009
GSPECT Image
PD%: 30
Control
6 months
PD%: Post–Effort Perfusion Damage Percentage
7 JUL2010
PD%: 15
One year
Chronic Ischemic Heart Disease One year treatment study
Funtional Capacity Time (sec)
Patient unable to carry out the test due physical limitations
Patient 2

GSPECT Image
PD%: 20
20 MAY 2009
28 OCT2009
PD%: 10
Control
6 months
PD%: Post–Effort Perfusion Damage Percentage
16 JUN2010
PD%: 10
One year
Chronic Ischemic Heart Disease One year treatment study
Funtional Capacity Time (sec)
Total442
post-treatment
366Time (sec)
pre-treatment
76Increase (sec)
6 month treatment
Patient 3

GSPECT Image
PD%: 70
03 JUN 2009
11 NOV2009
PD%: 60
Control
6 months
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Total200
post-treatment
155Time (sec)
pre-treatment
45Increase (sec)
6 month treatment
Patient 4

GSPECT Image
PD%: 30
06 MAY 2009
07 OCT2009
PD%: 25
Control
6 months
09 JUL2010
PD%: 0
One year
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease One year treatment study
Funtional Capacity Time (sec)
Total615
post-treatment
486Time (sec)
pre-treatment
81Increase (sec)
6 month treatment
48Increase (sec)
1 year treatment
Patient 5
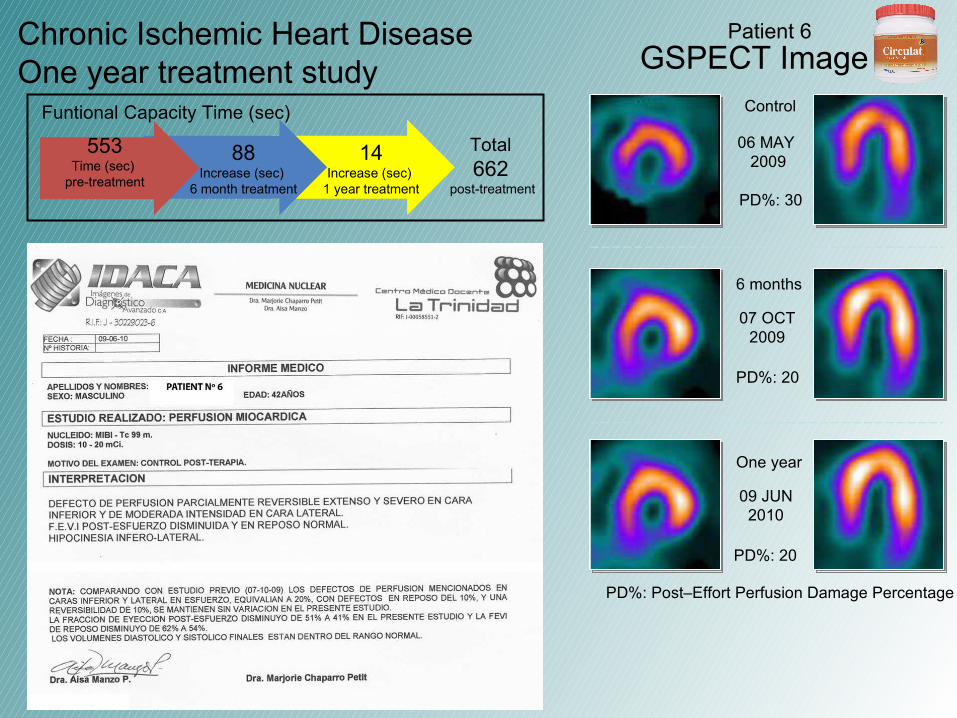
GSPECT Image
PD%: 30
06 MAY 2009
07 OCT2009
PD%: 20
Control
6 months
09 JUN2010
PD%: 20
One year
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease One year treatment study
Funtional Capacity Time (sec)
Total662
post-treatment
553Time (sec)
pre-treatment
88Increase (sec)
6 month treatment
14Increase (sec)
1 year treatment
Patient 6

PD%: 15
29 APR 2009
16 SEP2009
PD%: Post–Effort Perfusion Damage Percentage
GSPECT Image
PD%: 15
Control
6 months
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Total609
post-treatment
555Time (sec)
pre-treatment
54Increase (sec)
6 month treatment
Patient 7

PD%: 10
14 JUL 2009
11 NOV2009
GSPECT Image
PD%: 5
Control
6 months
28 JUL2010
PD%: 5
One year
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease One year treatment study
Funtional Capacity Time (sec)
Total491
post-treatment
433Time (sec)
pre-treatment
68Increase (sec)
6 month treatment
-10Decrease (sec) 1 year treatment
Patient 8

PD%: 20
14 JUL 2009
11 NOV2009
PD%: 20
Control
6 months
04 AGO2010
PD%: 20
One year
PD%: Post–Effort Perfusion Damage Percentage
GSPECT ImageChronic Ischemic Heart Disease One year treatment study
Funtional Capacity Time (sec)
Total676
post-treatment
516Time (sec)
pre-treatment
132Increase (sec)
6 month treatment
28Increase (sec)
1 year treatment
Patient 9

PD%: 60
13 MAY 2009
07 OCT2009
GSPECT Image
PD%: 35
Control
6 months
02 JUN2010
PD%: 20
One year
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease One year treatment study
Funtional Capacity Time (sec)
Total428
post-treatment
339Time (sec)
pre-treatment
89Increase (sec)
6 month treatment
Patient 10

PD%: 25
12 AGO 2009
08 DEC2009
PD%: Post–Effort Perfusion Damage Percentage
GSPECT Image
PD%: 15
Control
6 months
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Total373
post-treatment
323Time (sec)
pre-treatment
50Increase (sec)
6 month treatment
Patient 11

PD%: 15
14 JUL 2009
02 DEC2009
GSPECT Image
PD%: 0
Control
6 months
04 AGO2010
PD%: 0
One year
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease One year treatment study
Funtional Capacity Time (sec)
Total570
post-treatment
432Time (sec)
pre-treatment
83Increase (sec)
6 month treatment
55Increase (sec)
1 year treatment
Patient 12

PD%: 25
23 JUL 2009
02 DEC2009
PD%: Post–Effort Perfusion Damage Percentage
GSPECT Image
PD%: 20
Control
6 months
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Patient unable to carry out the test due physical limitations
Patient 13

GSPECT Image
PD%: 70
11 MAR 2010
15 SEP2010
PD%: 55
Control
6 months
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Total235
post-treatment
209Time (sec)
pre-treatment
26Increase (sec)
6 month treatment
Patient 14

GSPECT Image
PD%: 95
04 MAR 2010
15 SEP2010
PD%: 90
Control
6 months
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Patient unable to carry out the test due physical limitations
Patient 15

GSPECT Image
PD%: 35
10 MAR 2010
1 SEP2010
PD%: 35
Control
6 months
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Patient unable to carry out the test due physical limitations
Patient 16*
* Slight Qualitative Perfusion Improvement determined by diffuse radioisotope captation in lateral wall
GSPECT Image
PD%: 50
17 MAR 2010
15 SEP2010
PD%: 35
Control
6 months
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Total254
post-treatment
333Time (sec)
pre-treatment
-79Decrease (sec)
6 month treatment
Patient 17

GSPECT Image
PD%: 50
17 MAR 2010
06 SEP2010
PD%: 35
Control
6 months
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Total549
post-treatment
479Time (sec)
pre-treatment
70Increase (sec)
6 month treatment
Patient 18

GSPECT Image
PD%: 45
03 MAR 2010
01 SEP2010
PD%: 45
Control
6 months
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Total620
post-treatment
610Time (sec)
pre-treatment
10Increase (sec)
6 month treatment
Patient 19*
* Important Qualitative Perfusion Improvement determined by diffuse radioisotope captation in inferior wall

GSPECT Image
PD%: 15
10 MAR2010
15 SEP2010
PD%: 15
Control
6 months
PD%: Post–Effort Perfusion Damage Percentage
Chronic Ischemic Heart Disease Six month treatment study
Funtional Capacity Time (sec)
Patient unable to carry out the test due physical limitations
Patient 20

Cardiac Stent Alternatives: Associated Risk

Stem cells: Future Alternative ?
CIRCULAT IP Protection
USA Patent: Circulatory Disorders and Diabetes
Russian Patent: Method of elaboration; Circulatory Disorders and Diabetes
Mexican Patent: Circulatory Disorders and Diabetes
17 International patents (12/USA; 4/Russia; 1/Mexico)

Early results in the administration of CIRCULAT have shown it to be therapeutically efficacious, accessible and safe in the treatment of chronic ischemic heart disease.
Evidence of CIRCULAT’s efficacy was determined by state-of-the-art Gamma Single Photon Emission Computerized Tomography (GSPECT) images.
CIRCULAT is the only known orally administered treatment capable of obtaining myocardial reperfusion in chronic ischemic heart disease.
Conclusions
Next Steps
• Carry out joint phase 3 study with interested party;
• Increase numbers of patients (thirty/one hundred);
• Extend length of study (two year scenario);
• Request IP protection (in CEE) through Ischemic Cardiopathy Patent in US (PCT);
• Disseminate results of studies, seek partner and licensing and/or joint venture agreement.

Description of Circulat

Panax ginsengPfaffia paniculata
Panax quinquefolius Leuzea carthamoides
Eleutherococcus senticosus
Echinacea spp.Rhodiola rosea Grifola frondosaPetiveria alliaceaUncaria tomentosa Ganoderma lucidumSutherlandia frutescens Harpagophytum procumbens
Ginkgo bilobaHydrocotile asiaticaVaccinium myrtillus
Tabebuia avellandedae
Ruscus aculeatusAngelica sinensis Crataegus oxyacanthaHydrastis canadensisCroton lechleri
CIRCULAT is a High Pressure Liquid Chromatography fingerprinted complex formula of standardized herbal extracts, designed for circulatory disorders. Its components act synergistically
to increase the system’s survival potential (health) reducing its entropy and producing an endogenous curative tendency, without adverse effects.
CIRCULAT

Potential Synergetic Contribution
Po
ten
tial
Syn
erg
etic
Co
ntr
ibu
tio
n (
SC
)
Number of active principles (n)Number of active principles (n)
The synergetic potential of a complex herbal formulation -such as CIRCULAT- is provided by the interactions of the active principles present in each phytoceutical and can be mathematically
expressed by SC value below.

US FREE SALES CERTIFICATE



VENEZUELAN PHARMACOPEIA

GUIA SPILVA - CIRCUFORTE

VENEZUELAN FDA CERTIFICATION AS A NATURAL MEDICINE




Origin & Philosophical Background

Systemic Medicine(origin)
• Systemic Theory (ST), is published in eCAM (Oxford University Press, March, June, Sept. and Dec. 2005).
• ST stipulates that health is based on three factors:
E Functional organic energy reserve;
I Level of active biological intelligence;
O Integrity of its structure or organization.
• From ST a treatment strategy is derived denominated Systemic Medicine (SM).
• SM is a novel bio-systems approach for the treatment of chronic degenerative diseases.
• SM establishes principles for the elaboration of synergistic complex herbal formulations - such as CIRCULAT- which improve health by decreasing the body’s entropy.

Circulat187 genes
I52
E44
O14
45
OrganizationFraction
IntelligenceFraction
Common to 2 or 3 Fractions
EnergyFraction
CIRCULAT’s Synergistic -Gene Modulating- Capacity
+ + + = modulates 155 genes∑= modulates 187 genes; while ( )
The formulation modulates 32 additional genes than the sum of formulas’ individual fractions

International Publications eCAM: Part I, II and III. Systemic Theory & Systemic Medicine (2005).
eCAM: Part IV. The Praxis (2005). Investigación Clínica Sept. 2005 (vol. 46, sup. 2). Phytotherapy Research: Gene Expression (2007).
Phytotherapy Research: Diabetic Foot (2008). Phytopharm 2010 (Abstracts Book) Ischemic Cardiopathy.


















