Cine MR CSF Flow Study in Hydrocephalus · 2016-12-26 · Hye-Young Choi. et al : Cine MR CSF Flow...
8
J Korean Radiol 1997; 37: 415-422 Cine MR CSF Flow Study in Hydrocephalus : What are the Valuable Parameters?1 Hye-Young Choi, M.D., Myung-Hyun Kim , M.D .2 PU rpose : To evaluate the changes in diagnosis of intracranial cerebrospinal fluid (CSF) dynamics in the hydrocephalus , we studied the various parameters of cine phase contrast (PC) magnetic resonance (MR) CSF flow images in cases of acutely progressive hydrocephalus , comparing them with those in normal CSF circulation. Materials and Methods : The MR images were obtained with a 1. 5T (GE Signa , GE Medical Systems , Milwaukee , USA) unit using the 2 dimensional cine PC sequence with peripheral gating and gradient recalled echo imaging in ten cases ofnon-obstruc- tive hydrocephalus(NOH) , three of obstructive hydrocephalus(OH) , and ten controls. The time-echo time- fli p angle employed were 50 to 80 msec-ll to 15 msec-12 to 15 degrees. Temporal velocity information relating to cervical pericord CSF spaces, third and fourth ventricles , and the aqueduct were plotted as wave forms which were then analyzed for configuration, amplitude parameters(Vmax, Vmin, Vdif) , and temporal parameters(R-S , R-SMV , R-D , R-DMV). The statistical significance of each parameter was examined using the paired t-test. All patients with OH underwent endoscopic third ventriculostomy , whereas all with NOH underwent shunting procedures. Resu Its : In five ROIs , distinct reproducible configuration features were obtained at aqueduct and cervical pericord spaces , but not at ventricular levels. We determined the statistically significant differences between controls and hydrocephalus patients using temporaL rather than amplitude parameters. In NOH, the graph showed R-DMV shortening (p < 0.01) at the anterior cervical pericord space. In OH, there were R-DMV shortening (p < 0.05) was seen at the anterior cervical pericord space, and R-DMV shortening (p < 0.02) at the posterior cervical pericord space. In one case ofOH, a typi- cal change of configuration , mirror image , was obtained at aqueduct leveL and in all OH cases, the level of obstruction could be determined. Conclusion : The results of cine PC MR CSF flow study may be valuable for points for determining the level of obstruction , explaining the cause of hydrocephalus , diagnosing OH, and deciding the need for shunting procedures ; decisions would be based on an analysis of in vivo images, curve configuration , and phase shift of the vel- ocity curve. In the diagnosis of acutely progressive . hydrocephalus , termporal parameters are nore important than those relat Index Words : Brain , hydrocephalus Brain , MR Magnetic resonance(MR) , ciue study ' Department ofDiagnostic Radiology , Ewha Medical Research Center ' Department of Neurosurgery , Division of Neurology , Ewha medical Research Ce nt er , of Medicine , Ewha Womans University Received May 9, 1997 ; Accepted August 6 , 1997 Address reprint requests to : Myung-Hyu n Kim , M.D., Depart ment of Neuro- surgery, Ew ha Womans Universit y Mokdong Hospital , Mok-6- dong ' 911-1. Yangcheon- ku , Seo uI1 58-710, Korea . Tel. 82-2-650-5038 Fax.8 2-2 -6 49 -5 59 3 Intracranial and intraspinal cere brospinal fluid (CSF) flow was evaluated by means of the cardiac gated gradient echo magnetic resonance (MR) technique (1-6). During systole there is downward (caudal) flow of CSF in the aqueduct of Sylvius , the foramen of - 415 -
Transcript of Cine MR CSF Flow Study in Hydrocephalus · 2016-12-26 · Hye-Young Choi. et al : Cine MR CSF Flow...

J Korean Radiol S∞ 1997; 37: 415-422
Cine MR CSF Flow Study in Hydrocephalus : What are the Valuable Parameters?1
Hye-Young Choi, M.D., Myung-Hyun Kim, M.D .2
PU rpose : To evaluate the changes in diagnosis of intracranial cerebrospinal fluid (CSF) dynamics in the hydrocephalus, we studied the various parameters of cine phase contrast (PC) magnetic resonance (MR) CSF flow images in cases of acutely progressive hydrocephalus , comparing them with those in normal CSF circulation.
Materials and Methods : The MR images were obtained with a 1. 5T (GE Signa, GE Medical Systems, Milwaukee, USA) unit using the 2 dimensional cine PC sequence with peripheral gating and gradient recalled echo imaging in ten cases ofnon-obstructive hydrocephalus(NOH), three of obstructive hydrocephalus(OH), and ten controls. The time-echo time- fli p angle employed were 50 to 80 msec-ll to 15 msec-12 to 15 degrees. Temporal velocity information relating to cervical pericord CSF spaces, third and fourth ventricles, and the aqueduct were plotted as wave forms which were then analyzed for configuration, amplitude parameters(Vmax, Vmin, Vdif), and temporal parameters(R-S , R-SMV, R-D, R-DMV). The statistical significance of each parameter was examined using the paired t-test. All patients with OH underwent endoscopic third ventriculostomy, whereas all with NOH underwent shunting procedures.
Resu Its : In five ROIs, distinct reproducible configuration features were obtained at aqueduct and cervical pericord spaces, but not at ventricular levels. We determined the statistically significant differences between controls and hydrocephalus patients using temporaL rather than amplitude parameters. In NOH, the graph showed R-DMV shortening (p < 0.01) at the anterior cervical pericord space. In OH, there were R-DMV shortening (p < 0.05) was seen at the anterior cervical pericord space, and R-DMV shortening (p < 0 .02) at the posterior cervical pericord space . In one case ofOH, a typical change of configuration, mirror image, was obtained at aqueduct leveL and in all OH cases, the level of obstruction could be determined.
Conclusion : The results of cine PC MR CSF flow study may be valuable for points for determining the level of obstruction, explaining the cause of hydrocephalus, diagnosing OH, and deciding the need for shunting procedures ; decisions would be based on an analysis of in vivo images, curve configuration, and phase shift of the velocity curve. In the diagnosis of acutely progressive . hydrocephalus, termporal parameters are nore important than those relat
Index Words : Brain, hydrocephalus Brain, MR Magnetic resonance(MR) , ciue study
'Department ofDiagnostic Rad iology , Ewha Medical Research Center ' Department of Neurosurgery , Division of Neurology , Ewha medical Research Center , C이lege of Medicine, Ewha Womans University 。 l 논문은 1995학년도이화여자대학교교내연구비 지원에 의하여 이루어진것임
Received May 9, 1997 ; Accepted August 6 , 1997 Address reprint requests to : Myung-Hyun Kim , M.D ., Department of Neurosurgery, Ew ha Womans University Mokdong Hospital , Mok-6-dong ' 911-1. Yangcheon-ku, SeouI1 58-710, Korea . Tel. 82-2-650-5038 Fax.82-2-649-5 593
Intracranial and intraspinal cerebrospinal fluid (CSF) flow was evaluated by means of the cardiac gated gradient echo magnetic resonance (MR) technique (1-6). During systole there is downward (caudal) flow of CSF in the aqueduct of Sylvius, the foramen of
- 415 -

et al : Cine MR CSF Flow Study in Hydroceph헤us Hye-Young Choi.
eter of the skull at the level of the measurement of maximum bifrontal distance} was about 0.32 in NOH, and 0.40 in OH. We also examined ten healthy volunteers (six men and four women) aged 25 - 50 (mean, 30.4}years, none ofwhom had any prior history of neurological disease; none was taking medication, and in all, brain MRI was norma l.
Using a 1. 5 (Signa, General Electrics, U.S.A.) superconducting magnet, head and spine cine MR images were obtained in a mid-sagittal plane and in multiple axial planes. All the CSF flow studies were peripheral gated and used a reduced flip angle (15 degrees) gradient echo technique with a TR determined by the patient’s R-to-R interval, a TE of 15 ms, and a section thickness of 5 mm. Multiple images (“cine frames ") in the same plane were obtained during an R-to-R interval, starting immediately after the R-wave with successive images acquired at 40 ms intervals to within about 200 ms of the next R-wave. Clearly, with a slower heart rate, more frames would be obtainable. Images were acquired following 2 to 4 excitations, on a 192 X 256 matrix and displayed on a 512 X 512 matrix. The information was then displayed in a 'real time' closed loop cine format. Patients with cardiac arrhythmias are not ideal candidates for gated studies because oftheir varying R-to-R interval.
The qualitative cine studies were examined for evidence of marked signal void within various CSF pathways indicative of pulsating and rapidly flowing CSF. Intracranially, we examined axial CSF flow primarily at the aqueduct of Sylvius, the third and , fourth ventricle, and the dorsal and ventral subarachnoid
Magendie, the basal cisterns and the dorsal and ventral subarachnoid spaces, while during diastole, upward (cranial) flow of CSF is seen. Quantitative evaluation of CSF flow via phase reconstruction permits a more precise mapping of the intracranial and intraspinal flow patterns, and it is more sensitive in detecting fluid motion and allows calculation of CSF velocity(5}. In conditions which result in alterations of flow , cine MR dramatically shows either obstruction or excessively turbulent flow within the CSF pathways.
This investigation was performed to characterize and to quantify normal CSF flow at key locations in the intracranial and spinal neuraxis by means of a phase-contrast cine MR pulse sequence. This important basic information may be useful for understanding altered physiology in disease states such as the various forms ofhydrocephalus.
Methods
Ten patients(seven men and three women}aged lO - 71(mean, 47.6}years with non-obstructive hydrocephah뼈NO아H퍼-I},’ three males aged 1- 60(mean, 35 .3} years with obstructive hydrocephalus (OH) were included in this study. All NOH patients underwent ventriculoperitoneal (VP) shunting procedures, and a11 OH patients underwent endoscopic third ventriculostomy . All fulfilled the fo11owing diagnostic criteria: a history of progressive dementia, gait disturbance and/or urinary urgency or incontinence, and hydrocephalus on CT and MRI(Table 1}. Mean Evans index (maximum bifrontal distance/maximum inner diam-
Table 1. Clinical Summary ofObstructive and Non-obstructive Hydrocephalus Patients.
Etiology GOS l
2
3
4
5
6
7
8
9
0
l
14
3
----
v m v v v v v v v v v v v
Operation
찌 찌 찌
앤 맺
m?
m?
m갱 맨 맨 m갱 맨 맨
@
@
m
m m m m m m m m m m
,비 띠 띠
u
u
u
u
u
u
u
u
u
u
’κ -κ ι
-m
’해 ’m ,m ’m ‘m
찌 때 ’m
’m @
““
때
w w w mq
w w mn
w w w m m m
띠 띠 띠
1j
1j
1j
Evansindex
0.3 2 0. 34 0.39 0.3 0.29 0.29 0.3 0.29 0.31 0.32 0.52 0.34 0.35
meningitis menmgItis menmgltls
hemorrhage hemorrhage unknown
hemorrhage hemorrhage hemorrhage unknown congenital cbll tumor cbll tumor
Diagnosis
뻐 m… …m
mμ
mm
mm
m m m m H
H
H
K K
K
K
K
m “ k
m “ 。
。
。
Age m m
끄 표 %
이α 개 %
이 기 l
%
ω
Sex M
M
M
M
M
M
M
F
F
F
M
M
M
Case
GOS, Glasgow outcome scale(I dead , 11 vegetative, 111 severely disabled , IV moderately disabled, V normal); M; male; F, female ; NOH, non-obstructive hydrocephalus; OH, obstructive hydrocephalus ; cblL cerebellum; VP shunting, ventriculoperitoneal shunting; 3ra ventriculostomy, third ventriculostomy
- 416 -

J Korean Radiol S∞ 1997; 37: 415-422
spaces at the cervico-medu11ary junction. CSF pathways were judged to be patent whenever a normal f10w void was observed during a portion of the gated cycle. The analysis of phase-contrast images alone was not sufficient to assess the subtle physiologic details of the CSF f1ow. Further precision can be achieved by plotting the temporal velocity information from images as a waveform(CSF f10w waveform)(6). The fo11owing scans were performed in a11 ten volunteers and 13 patients : 1) sagittal Tl -weighted locater(SOO/l S/2 [repetition time /echo time/excitations], 5-mm scan thickness); 2) sagittal midline CSF study to include the aqueduc t,
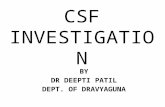
third and fourth ventricle , and cervical subarachnoid spaces to the level of C-4; 3) axial CSF study through the third ventricle, the inferior collicular level of the aqueduct, the fourth ventricle, and the dorsal and ventral subarachnoid spaces at the cervico-medu11ary junction. The region ofinterest for the precord CSF was at C2 body leveL and for postcord CSF, at approximately C-l. The waveforms of a11 the CSF and the blood f10w studies were plotted, with velocities in millimeters per second on the y-axis and fractions of the cardiac cycle on the x-axis. Fractions of the cardiac cycle were chosen in order to normalize subjects with different heart rates. The fo11owing amplitude and temporal parameters(A and B, respectively) were also evaluated : A) maximum CSF systolic velocity(Vmax), maximum CSF diastolic velocity(Vmin), and the difference between Vmax and Vmin (Vdi터. B) cardiac R-wave to the onset ofCSF systole(R-S), R-wave to maximum systolic velocity(R-MSV), R-wave to the onset of CSF diastole (R-D), and R-wave to maximum diastolic velocity (R-MDV). The measurements R-S and R-D for CSF f10w
]
뼈키
1 ‘ R.P >, \
~ 50 I ‘ \ \
윤 : R.SMV 、o -•-••- '--> 、
R.S
“ ‘
딩) -5 0 I ν
100 I
; Vdif -• 50
2 00 ι ... t . I Vmin
250
P hase
Fig. 1. The graph showing CSF flow wave and the meaning of vanous parameters. Vmax. maximum systolic velocity; Vmin, maximum diasolic velocity; V dif, difference of Vmax-Vmin ; R-S, R wave to onset of CSF systole; R-MSV , R wave to maximum systolic velocity; R-D , R wave to onset of CSF diastole; R-MDV, R wave to maximum diastolic velocity
waveforms were obtained at time points at which zero velocity was noted(Fig. 1). The results of volunteers were compared with those of patients by using the paired t test or Mann Whitney rank sum test
Results
Normal intracranial CSF flow
Qualitative Assessment Velocity changes in the frontal horns of the lateral
ventricles were minimal and did not show a clear oscillatory pattern. Variable directions and velocities of CSF flow within the posterior third ventricle were observed and occasional f10w at the level of the foramen of Monro was seen. The veloci ty profile of CSF in the aqueduct was similar to that of CSF in the foramen of Monro, but velocities in the aqueduct were greater.
Peak systolic flow occurred at 2S. 2 % d uring the cardiac cycle(from one cardiac R-wave to the next R-wave) , whereas peak diastolic flow occurred at 74.4 %(Fig. 2) . Flow was simultaneously reserved in the foramen of Monro and aqueduct at 56 % during the cycle. Mean peak signal changes were nearly equivalent during the systolic and diastolic phases: 204(SD = 124) and 212(SD = 131), respectively. The fourth ventricle served as a mixing chamber for CSF exiting the ventricular system and CSF f10wing in from the cisterna magna, which itself was the other major site for the mixing of CSF. The systolic and diastolic phases could be identified but were less we11 defined than those of the other areas studied. Craniocaudal and caudocranial flow could often be detected simultaneously . Because of the anatomy and mixing characteristics, pulsation
. m
%
o
g
빼
~{}a∞Z잉}Zi -s:이-a -150
200
.;>50
Phasε
Fig. 2. The mean CSF f10w wave showing different phase shift at various ROI in normal persons. ant. SAS or post.
SAS, the CSF flow wave of pericord spaces precede that of aqueduct.
- 417-

Hye-Young Choi. et al : Cine MR CSF Flow Study in Hydrocephalus
amplitude had little meaning in this location. CSF pulsation dynamics in the cervical spine showed we11-defined systolic and diastolic components. Peak velocity during CSF systole occurred at 3 % (SD = 3.1 %) during the cardiac cycle , and peak diastolic velocity occurred at 66.5 %(SD = 5.2 %). It is noteworthy that peak systolic velocity in the cervical subarachnoid space preceded this velocity in the foramen of Monro and aqueduct by 22.2 % of the cardiac cycle(Fig. 2). Mean peak signal intensity in the anterolateral recess was 145.1(SD = 53.3), while peak diastolic signal intensity was 187 .7(SD = 60.8). The velocities in the subarachnoid space were variable because of the various compartments formed by dorsal and ventral roots , the dentate ligament, and dorsal arachnoid septations(Fig . 3). Velocities dorsal to the cervical cord were lower and more variable in some patients, no flow was detected dorsal to the cord except during peak systole and diastole. In these flow compartments, however, the timing ofvelocity changes, was uniform.
Quantitative Assessment Flow was bidirectionaL which a11 extraventricular
and aqueductal CSF flow waveforms showing distinct CSF systolic and diastolic components . Extraventricular CSF flow waveforms were characterized by relatively narrow systolic peaks and broad diastolic troughs , the diastolic slopes were less steep than the systolic . Aqueductal CSF flow waveforms differed from those of the extraventricular CSF compartments
A B
c D
in that the systolic peaks were broader than the dias tolic troughs. Considerable variations in amplitude parameters (Vmax and Vmin) were seen with wide ranges between maximum and minimum values. The onset ofthe craniocaudal flow (R-S) in the postcord CSF space was either simultaneous with or earlier than that in the precord space(1.4 %). The onset of craniocaudal flow in the pericord spaces was always earlier than in the aqueduct(P < 0.05), that of caudocranial flow in the postcord space was earlier than in the precord space(P < 0.005), and that of caudocranial flow in pericord spaces was always earlier than in the aqueduct(P < O. 0001)(Fig. 2) .
The results of the configuration, amplitude, and temporal analysis ofthe CSF flow waveforms were considered separately . Their configuration was distinctive , and slightly different between the extraventric ular spaces and the aqueduct and we observed wide variations in the maximum systolic and diastolic velocity values of CSF flow . Similar observations have been previously documented(3, 5). We decided that the most valuable parameters were temporaL and were at the level of aqueduct and pericord spaces, since these showed relatively constant flow , and we compared controls and patients on the basis of these o bservations.
Changes in intracranial CSF flow
In patients with hydrocephalus, CSF flow patterns varied according to the underlying cause of ventricle
Fig. 3. Axial velocity-encoded images of upper cervicallevel in normal per-
‘ son. Systolic peak f10w (white) is seen in 3A, and diastolic peak f10w (black) is seen in 3C. Invertion of sytolic to diastolic or diastolic to systolic f10w is seen in 3B or 3D(Note signal changes starts at the periphery of cervical pericord spaces. Dentate ligaments is seen in lateral part of pericord spaces.)
- 418 -

J Korean Radiol Soc 1997; 37 : 415 - 422
enlargement.
Non-obstr uctive hyd rocepha lus (NOH) In terms of the results of qualitative an alysis or
patterns of wave configuration, where were no re markable differences between normal controls and NOH patients. Considerable variation in 없nplitude parameters (Vmax, Vmin , and Vdif) was seen, however, with a wide range between maximum and minimum values, and this variation was too wide to compare the parameters of the volunteers with those of patients. on analysis of temporal parameters, only R-DMV was senn to be significantly different between volunteers and patients, and this variation occurred at the level of the anterior cervical subarachnoid space(p < 0.01).
Obstructive hyd rocephalus (OH ) The level of obstruction was qualitatively visible. In
one case, wave configuration was typically reversed in the form of a mirror image. There was no significant difference in amplitude parameters, but with regard to temporal parameters, R-DMV at the level of the anterior cervical subarachnoid space (p < 0.05) and R-DMV at the level of the posterior cervical subarachnoid space (p < 0.02) were significantly different (Table 2)
D iscuss ion
Although some fundamental features of CSF flow
physiology have been recognized for some time(7, 8), the use of MR imaging techniques has led to a more detailed understanding of CSF motion(9 - 12). The flow dynamics of CSF are primarily dictated by fast pulsatile motion driven by pulsation ofthe intracranial carotid and vertebrobasilar arteries (13 , 14) and the “ bulk" or slow f10w of CSF(15 - 18). With recent advances in MR imaging techniques, the direction and velocity of some f10ws can be detected not only visually, but also quantitatively. Furthermore, it now has become possible to obtain information on the motion pattern, direction and absolute value of motion velocity in CSF in vivo(S , 19). Sine, however, the pure bulk flow ofCSF is very slow and may always be modified by fast to-and-fro motion, MR imaging has as yet not been applied to an analysis of CSF bulk flow. Radio-cisternography, developed by DiChiro et al. (20), still remains the most popular method of stud ying CSF bulk f1ow. Previous MR imaging studies ofCSF pulsatile motion by other researchers(S , 13) reported the rate of CSF pulsatile motion to be 18 - 36 mm/s(2l) or 10. 9 - S2 .4mm/s(5) in the ventral subarachnoid space and 13 - 25 mm/s(l) in the dorsal. Considering that such arterial formations as the basilar artery and the circle of Willis in the ventral side ofthe brain stem may serve as generators of CSF pulsatility( 13, 14), it is not surprising that these f10w studies indicate that CSF moves faster in the ventral subarachnoid space than in the dorsal spac.
CSF f10w waveforms, representing the f10w within a small region of interest, have distinct configurations and temporal patterns . The analysis of the flow
Table 2. Summary ofVariable Parameters and Statistical Significance.
Amplitude parameter Temporal parameter
Vmax Vmin Vdif R- SMV R- D R- DMV R- S
Aqueduct normal 53.2 - 70.7 124.9 0.25 0.51 0.74 0.95 NOH 43.9 - 56.5 100.4 0.26 0.54 0.77 0.96 OH 60.2 - 66.3 126.5 0.08 0.34 0.66 0.86
ant. pericord normal 50 .4 - 46.6 97 0.03 0.31 0.67 0.9 NOH 45 .7 - 57.8 103.5 0.01 0.24 0.49** 0.76 OH 54.6 - 42.1 96.7 0.04 0.2 0.6* 0.88
post. pericord normal 47.7 - 49.8 97.5 0.04 0.21 0.62 0.88 NOH 35.5 - 44 95.8 0.07 0.29 0.81 0.87 OH 52 - 46.2 96.4 0.04 0.19 0.56* 0.91
NOH, non-obstructive hydrocephalus ; OH, obstructive hydrocephalus; ant. or post. pericord , anterior or posterior cervical pericord space; Vmax, maximal systolic velocity ; Vmin, minimal diastolic velocity; Vdif. difference of Vmax-Vmin; R--SMV , R-wave to maximum systolic velocity ; R-D, R-wave to the onset of diastolic flow; R-S , R-wave to the onset of systolic f1ow ; R-DMV, R-wave to maximum diastolic velocity *, * * statistically significant values (p < 0.05) by paired t-test.
- 419 -

Hye-Young Choi, et al : Cine MR CSF Flow Study in Hydrocephalus
waveform appears to be reliab1e, reproducib1e, and sensitive(6). Craniocauda1 and caudocrania1 postcord CSF flow occurs either simu1taneous1y with or earlier than the precord CSF flow. Pericord CSF flow in either direction precedes that in the prepontine cistern, the interpeduncu1ar cistern, and the aqueduc t. Prior research concerning CSF pressure waveforms indicates that the configuration and amplitude of these depend on arteria1 input, compliance of the crania1 contents, and venous outflow(22, 23).
Our preliminary experience indicates however, that 1arge variations in norma1 velocities shou1d be expected in a11 CSF spaces. The probab1e reasons for these norma1 variations are multip1e but most probab1y relate to the size ofnearby vascu1ature, the compliance of surrounding brain/spina1 cord tissue, the anatomy of the CSF containing spaces, the vo1ume and vascu-1arity of the choroid p1exus, and the systemic hemodynamics(S). The distensibility of the venous structures must a1so influence the effects of pu1se waves, as Du Bou1ay has pointed out(24). Velocity measurements in the basa1 cisterns and the upper cer vica1 subarachnoid space are thought to be more re liab1e than those obtained from sma11er spaces such as the aqueduct of Sy1vius(S). Bidirectiona1 nonsynchronous flow can, in addition, be observed , and can be noticed in many segments ofthe CSF pathway.
It appears that for the detection of fluid flow cine MR is more sensitive than static MR imaging. Specifica11y, Sherman (2S) reported a varying incidence of flow voids in the aqueduct and the foramen of Magendie, and these depended on the degree of ventricu1omega1y. When this was not present, an aqueduct flow void was noted in 67 % ofthe cases and a foramen Magendie flow void in 39 %. These percentages increased with increasing ventricu1omega1y. Our clinica1 materia1s show that using the cine MR technique, as described above, these structures are routinely seen. It is emphasized however, that the degree of flow vo이l벼d in the foramen 0아fMa앵gen띠1띠dieno야rmally varies from pa따t디ient to pa따t디ient, a r.삶ac야t which relates to i따 t않 s size and 10cat더ion re1ative to the mid-sagitta1 p1ane(S).
The clinica1 significance of this technique is apparent when one is either trying to assess whether surgica1 intervention may be efficacious or when one wishes to assess the patterns of flow during an MR examination aimed at improving d1ag
entricu1ar communicating hydrocepha1us is present. Even when aqueducta1 compression is suspected be cause of a mass 1esion, cine MR can determine whether ventricu1omega1y is a consequence of aqueducta1 kinking or compression. This can be of some importance when deciding whether ventricu1omega1y is main1y a result of treatment or occurs either partly or main1y on a mechanica1 basis(S). Cine MR can be he1pfu1 in determining the 1eve1 of obstruction in cases of comp1ex hydrocepha1us, i. e. where any one of mu1-tip1e adhesions or masses cou1d exp1ain the presence of ventricu1omega1y.
Many authors have shown that peak cauda1 and rostra1 flow in the aqueduct is significantly higher in patients with NOH than in hea1thy vo1unteers. This has been suggested in previous studies using the flow void (26) and velocity-sensitive phase methods(S , 22,
27). Barkhof et a1. (27) noted increased CSF ve10city and flow vo1ume in the cerebra1 aqueduct of patients with NOH, but the diagnostic criteria for hydrocepha1us were not specified . Using a phase-contrast method with retrospective cardiac gating, Nitz et a1. (28) found a tendency towards higher flow ve10cities and vo1umetric flow rates in NPH. In a recent study, Brad1ey et a1. (29) suggested that the findings of norma1 aqueduct CSF dynamics in patients in whom NPH is suspected probab1y indicates that they havecentra1 atrophy rather than NPH, and shou1d not be shunted.
Unfortunate1y, our results showed substantia1 variation of amplitude parameters (velocity changes) in norma1 subjects and patients, and thus did not provide important information about hydrocepha1us. We observed wide variations in maximum systolic and diastolic velocity va1ues of CSF flow , and similar observations have been previous1y documented(3, S) Earlier experiments have shown changes in the tempora1 parameters of CSF pressure waveforms with altered craniospina1 dynamics(6 - 8), and we therefore believe that the tempora1 par없neters of flow waveforms may have clinica1 applications. In both NOH and OH, R-DMVs were significant1y shorter (p < 0.01 , P < O.OS , respective1y) at the anterior pericord space, but R-DMV was significant1y shorter only in OH(p < 0.02) at the posterior pericord space. This indicates that there are considerab1e changes in the configuration of flow-waves , especially in phase shifting; these may be explained by early diastolic recoil due to increased extraventricu
-420 -

J Korean Radiol Soc 1997;37:415-422
other pathological conditions take into account the re
lationship between circadian variation and CSF pro
duction, which is minimal around noon and reaches a
maximum just after midnight(30). All measurements in
the present study were all performed during the after
noon and hence probably re f1ect an intermediate level
of prod uction
Several limitations of this study should be noted.
First, the number of patients, especially those with
negative CSF f10w study findings who underwent
shunt formation, is small; second, the study is retro
spective; third, although the at blinding of chart
reviews was attempted , this was not always possible
because of information about the CSF f10w study
already written in the physician ’s notes; fourth ,
although this phase- contrast technique is excellent for
quantitating laminar f10w (31) it may result in substan
tial underestimation of turbulent flow , especially in
patients with hyperdynamic CSF flow. Despite these
shortcomings, it is thought that the quantitative CSF
f10w study is a useful method ofpredicting response to
shunting in patients with hydrocephalus and in the
work-up ofsuch patients, may be considered the test of
choice after clinical evaluation and routine imaging.
References
l. Akihiko w , Sumio K, Kiyoshi S. Characteristics of cerebro
spinal fluid circulation in infants as detected with MR velocity imaging. Child' 5 Nerv Syst 1995; 11 : 227-230
2. Bradley WG , Scalzo D, Queralt J , Nitz WN, et al. Normal-Press
ure Hydrocephalus: Evaluation with Cerbrospinal Fluid Flow
Measurements at MR imaging Radiology 1996; 198 : 523-529
3. Enzmann DR, Pelc NJ. Normal flow pattern of intracranial and
spinal cerebrospinal fluid defined with phase-contrast cine MR imaging. Radiology 1991; 178: 467-474
4. Gideon P, Stahlberg F, Thomsen C, Gjerris F, Sorensen PS,
Henriksen O. Cerbrospianl Fluid Flow and production in
patients with normal pressure hydrocephalus studied by MRI
Neuroradiology 1994; 36: 210-215 5. Quencer RM , Donovan Post MJ , Hinks RS. Cine MRI in the
evaluation of normal and abnormal CSF flow: intracranial and intraspinal studies. Neuroradiology 1990; 32 ‘ 37 1-391
6. Refeeque A, Bogdan AR, W이pert SM. Analysis of Cerebro
spinal Fluid Flow Waveforms with Gated Phase-Contrast MR
Velocity Measurements. AJN R 1995; 16 : 389-400
7. Nitta M, Hasegawa Y, Nagai H. Conduction time of the pulse
through the brain in increased intracranial pressure. Neurochiru앵ia 1982; 25: 186-187
8. Portnoy HD, Chopp M. In commentary on Daley ML, Gallo AE,
Gehling GF, et al. Fluctuations of intracranial pressure associated with the cardiac cycle. Neurosurgerγ 1982; 11:
617-621
9. Citrin CM , Sherman J L, Gangarosa RE, Scanlon D. Physiology
of the CSF flow void sign: modification by cardiac gating. AJNR 1987; 7: 1021-1024
10. Edelman RR , Wedeen VJ , Davis KR, et al. Multiphasic MR
- 421
imaging: a new method for direct imaging of pulsatile CSF flow. Radiology 1986; 161 : 779-783
I l. Malko JA, Hoffman JC, McClees EC, Davis PC, Braun IF. A
phantom stud y of intracranial CSF signal loss due to pulsatile motion. AJN R 1988; 9 : 83-89
12. Szeverenyi NM, Kiwddwe SA, Cacayorin ED. Correction of CSF
motion artifact on MR images of the brain and spine by pulse
sequence modification ’ clinical evaluation. AJN R 1988; 9 : 1069-1074
13. Adolpgh RJ , Fukusuni H, Fowler NO. Origin of cerebrospinal
fluid pulsation. Am J Physiol 1967; 212 ’ 840-846
14. Hamit HF, Beall AC, De Bakey Me. Hemodynamic inf1uences
upon brain and cerebrospinal f1uid pulsations and pressure. J
Trauma 1965; 5: 174-184
15. Bauer FK, Yuhl ET. Myelography by means of 131-1. The
mye/oscintigram Neurolo양I 1953; 3: 341-346 16. Bell RL. Isotope transfer test for diagnosis of ventriculo
subarachnoid block. J Neurosurg 1957; 64: 674-679
17. Chon SN, French LA. Systemic absorption and urinary ex
cretion of RISA from subarachnoid space ‘ Neurology 1955; 5 555-557
18. Cutler RWP. Formation and absorption of cerebrospinal fluid in
man. Brain 1968; 91 : 707-720
19. Ohara S, Matsumoto T, Nagai H, Banno T. Observation of CSF
pulsatile flow in MRI: the signal void phenomenon. Neurol Surg
1987; 39: 991-996
20. DeChiro G. Observations on the circulation of the cerebrospinal
fluid. Acta Radio/ 1966; 15: 988-1002
2l. Ridgway JP, Turnbull LW , Smith MA . Demonstration of pulsa
tile cerebrospinal fluid f10w using magnetic resonance phase
imaging. B J Radiol 1987; 60: 423-427 22. Cordoso ER, Rowan JO, Galbrath S. Analysis of the cerebro
spinal fluid pulse wave in intracranial pressure. J Neurosurg
1983; 59: 817-821
23. Portnoy HD, Chopp M, Branch C, Shannon MR. Cerebrospinal
fluid pulse waveform as an indicator of cerebral auto regulation.
J Neurosurg 1982; 56; 666-678
24. DuBoulay GH ‘ Pulsatile movements in the CSF pathways. Br J
Radiol 1966; 39 ‘ 255-262
25. Sherman JL, Citrin CM , Gangarosa RE, Bowen BJ. the MR ap
pearance of CSF f10w in patients with ventriculomegaly. AJNR
1986; 7: 1025-1031
26. Bradley WG , Kortman KE , Burgoyne B. Flowing cerebrospinal
fluid in normal and hydrocephalic states: appearance on MR
images. Radiology 1986 ; 159: 611-616 27. Barkhof F, Kouwenhoven M, Valk J , Sprenger M. Quantitative
MR flow analysis in the cerbral aqueduct: controls vs com
municating hydrocephalus(abstr) ‘ In: Book of abstracts; Society
of Magnetic Resonance in Medicine Berkeley, Cali f, Society of
Magnetic Resonance in Medicin

Hye-Young Choi. et al : Cine MR CSF Flow Study in Hydrocephalus
31‘ Mullin WJ, Atkinson D, Hashemi RH, Yu J, Bradley WG. High resolution quantitative assessment of aqueductal CSF motion by
phase contrast MRI technique: correlation with p비satile flow phantom. Radiology 1993; 183: 459-466
대한빙시선의학호|지 1997; 37: 415-422
뇌수종 환자에서 뇌척수액 역동학 검사:가치가 있는 변수는 무엇인가?1
1 이화여자대학교 의과대학 진단방사선과학교실
2이화여자대학교 의과대학 신경외과학교실
최 혜 영 · 검 명 현2
목 적 저자들은 급성으로 진행되는 교통성 또는 폐쇄성 뇌수종 환자들에서 뇌척수액 역동학 검사의 의의를
알아보고자하였다.
대상 및 방법 : 검사대상은 교통성 뇌수종 10예, 폐쇄성 뇌수종 3예, 그리고 정상 대조군 10예였다. 각각에서 1.
5T( GE , Signa, USA)의 자기공명 촬영기를 이용하여 심장박동을 기준으로 R-R interval당 167~ 의 이차원적
영상을 소급적 방법으로 얻었다. 촬영부위는 제3뇌실, Sylvius관, 제 4뇌실 및 전후방 경추부 지주막하 수조였으
며, 각 부위에서 촬영한 영상들을 분석하고, 위상차에 따른 자기 신호 정도로 표시해 도표로 나타냈다. 도표의
모양,수축기 빛 이완기에서의 파고와시점을분석하여 수축기와 이완기의 최대 파고및 그차이,수축기와이완
기의 시점 및 각각으로의 이행 시기의 시점 등 7개의 지표들을 얻어 이를 통계 처리하여 환자군과 정상 대조군
을비교하였다.
결 과 ’ 각 예에서 얻은 5부위의 촬영 결과를 분석한 결과 제3뇌실 및 제4뇌실에서의 측정치는 개인차가 심하
여 제외되었다. Sylvius관과 전후방 경추부 지주막하 수조에서 얻은 7개의 지표 중 수축기 빛 이완기의 파고에
관게된 3개의 지표들(amplitude parameters)보다 수축기와 이완기의 시점 및 각각으로의 이행 시기의 시점에
관계된 4개의 지표들(temporal parameters)이 의미 있게 나타났다. 교통성 뇌수종에서는 정상 대조군에 비해
전방 경추부 지주막하 수조에서의 이완기 최대점 도달시기가 더 빠르게 나타났고(p<0.02) , 폐쇄성 뇌수종에서
는 전방 경추부 지주막하 수조에서의 이완기의 최대점 도달시기가 더 빠르게 나타났고(p<0.05) 후방 경추부 지
주막하 수조에서의 이완기의 최대점 도달시기도 더 빠르게 나타났다.(p<O.02) 또한 폐쇄성 뇌수종에서 그 폐쇄
부위를 정확하게 알수있였다.
결 론 자기공명 영화촬영술을 이용한 뇌척수액 역동학 검사는 영상분석, 파형분석, 그리고 파형의 위상차의
변화 등을 통해 뇌수종에서 폐쇄 부위를 알려주고, 뇌수종의 원인 규명과 진단, 나아가서 수술 여부를 결정하는
데 큰 도움이 될 것으로 사료된다. 급성으로 진행되는 뇌수종의 진단에 있어서 amplitude parameter보다는
temporal parameter가 의미 있었으며 temporal parameter 중에서도 이완기의 최대점 도달시기가 가장 의미
있는것으로나타났다.
” “







![Dr Winkler ASNI presentation [Read-Only] Annual Meeting/Handouts/Dr_Winkler_ASNI... · 1/11/2013 8 Normal CSF Flow • CSF Exchange between the Lateral and the 3rd Ventricles through](https://static.fdocuments.us/doc/165x107/5b4d98eb7f8b9a0a418b4a0f/dr-winkler-asni-presentation-read-only-annual-meetinghandoutsdrwinklerasni.jpg)