Ciccone Pharmacokinetics Article 1995

of 9
-
Upload
jason-mileski -
Category
Documents
-
view
222 -
download
0
Transcript of Ciccone Pharmacokinetics Article 1995
-
8/2/2019 Ciccone Pharmacokinetics Article 1995
1/9
Basic Pharmacokinetics and the PotentialEffect of Physical Therapy Interventions onPharmacokinetic Variables I
Pharmacokinetics involves the factors that influence drug absorption, distribu-tion, and elimination. Phamzacokinetic variables determine how a specijicdose of a drug will eventually reach talget tissues and exert a response. Variousfactors can influence normal pharmacokinetics, including exercise, applicationof physical agents, and massage. mese intmentions produce hemodynamicand other physiologic changes that can potentially alter drug disposition withinthe body. f ie magnitude and speczjic type of phamzacokinetic changes, how-etler, are highly variable depending on the specijic intervention and the drug inquestion. Physical therapy interuentions seem to have tho greatestpotential toaffect absorption and distribution of drugs that are administered by transder-ma1 techniques or by subcutaneous and intramuscular injections. Research isneeded to determine exactly how physical therapy interventions can affect thephamacokinetics of various medications, and how the clinical efects of thesemedications are afected by altered drug disposition. [Ciccone CD. Basic phar-macokinetics and the potential effect of physical therapy interventions on phar-macokinetic z~ariables. hys ?her. 199 ;75343-351 IKeyWords: Exais e, general; Phamzacokinetics; Phamzacology.
A fundamental concept in pharmacol-ogy is that a drug must reach specifictissues in the body at a sdicient con-centration to exert therapeutic effectswithout causing excessive harmful ortoxic effects. Pharmacokinetics is thebasic area of pharmacology that dealswith drug administration, absorption,distribution, tissue binding, metabo-lism, and excretion.' Pharmacokmeticproperties of a medication need to beknown so that an appropriate amountof the drug can be adrmnistered toreach target tissues and produce thera-peutic responses in a fairly predictableand timely manner.Pharrnacokinetic variables are deter-mined for therapeutic drugs to provide
an idea of how each drug is absorbed,distributed, metabolized, and so on.These variables are typically examinedduring drug testing in asymptomaticvolunteers or in patients who havediseases that will not directly affect thepharmacokinetic variables. There are anumber of factors, however, that canalter drug disposition, thus altering thenormal pharmacokinetic profile for adrug. Factors such as disease, age,diet, genetic variations, and drug inter-actions have all been noted to causechanges in the way specific drugs aredealt with in the b0dy.~-4 n addition,there may be interventions used byphysical therapists that can changepharmacokinetic effects and alter theresponse to certain drugs.
?he purpose of this article is to reviewsome basic pharmacokinetic principlesthat describe how drugs are absorbed,distributed, and eliminated from thebody. The possible effects that inter-ventions such as exercise, physicalagents, and manual techniques mayhave on these variables will beaddressed.
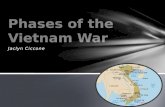
Pharmacokinetic VariablesPharmacokinetics involves the com-plex interaction of multiple factors,including drug administration, absorp-tion, distribution, and elirnination.3The interrelationships among thesevariables are illustrated schematicallyin the Figure. It is beyond the scopeof this article to address each of thesefactors independently. There are, how-
CD Ciccone, PhD, PT, is Associate Professor, Department of Physical Therapy, School of Health ever) three primary that canScience and Human Performance, Ithaca College, Ithaca, NY, 14850 (USA). be used to describe the pharrnacoki-12 / 343 Physical Therapy / Volume 75, Number 5 /May 1995
-
8/2/2019 Ciccone Pharmacokinetics Article 1995
2/9
ADMINISTRATION
LTJI ABSORPTION IBIOAVAILABILITY - - DISTRIBUTION
I(CONCENTRATION INI I SYSTEMIC CIRCULATIONCLEARANCE - - - W
tELIMINATION:- metabolism- excretion
- target tissues- other tissues
Figure. Schematic representation of the interrelationships among spec$cphannaco-kinetic jizctors. Breeprimay parametem (bioavailahility, volume of distribution, andclearance) are used to quantify these interrelationships at the points indicated by thedashed czrrozus.netic profile of a certain drug. These orally. A drug administered orally, forvariables are bioavailability, volume of example, would be considered 50%distribution (V,), and clearance. Each bioavailable if a 100-mg oral doseof these primary variables is described results in 50 mg of the drug actuallyhere. reaching the bloodstream.
Bioatailability is commonly definedas the fraction or percentage of activemedication that reaches the systemiccirculation following administration byany route.5 Drugs that are adminis-tered intravenously are considered10096 bioavailable because they aredelivered directly into the blood-stream. This concept, therefore, is notvery useful for describing the bioavail-ability of drugs administered intrave-nously. Bioavailability is more helpfulin accounting for the absorption ofdrugs that are administered by otherroutes, especially those administered
The Table lists values for bioavailabil-ity of some common medicationsfollowing oral administration inasymptomatic adults. Bioavailability ofdrugs administered by other routes,including transdermal administrationand subcutaneous and intramuscularinjections, can also be calculated de-pending on how much of the drugultimately reaches the systemic circula-tion. Regardless of the route of admin-istration. the bioavailability of anymedication can be altered by fac~orsthat increase or decrease the amountof drug that is absorbed from theadministration site and transported tothe bloodstream. This fact can necessi-
tate altering the dosage or route ofadministration to avoid untowardeffects because of changes in theplasma levels of the drug.Bioavailability of orally administereddrugs may increase, for example, inpatients with liver disease.5 Drugsabsorbed from the gastrointestinal trapass through the liver before reachingthe systemic circulation (first-passeffect), and a portion of the adminis-tered dose is normally destroyed byhepatic first-pass metabolism. If theliver is damaged, bioavailability willincrease because a relatively greaterportion of the dose will reach thesystemic circulation, and lower dos-ages may be needed to offset thisincreased bioavailabiity. Likewise,bioavailability may be increased ifdrugs are injected into or near exerciing mu ~c le .~xercise may cause in-creased absorption from an intramus-cular or subcutaneous injection site,resulting in increased appearance ofthe drug in the systemic circulation.The implications of increased bioavaiability are explored in more detail latein this article.Volume of DistributionVolume of distribution is used to indicate how a systemic dose of a medication is ultimately dispersed throughouthe body.5 Volume of distribution isdetermined by the ratio of how muchdrug appears in the plasma relative tothe total amount of drug administeredThis ratio is calculated as follows:
Amount of drug administered(1)v', = Plasma concentrationCalculation of Vdyields a parameterthat is compared with total body wa-ter. A typical 70-kg person has a totalbody water of approximately 42 L. Ifthe calculated V is approximatelyequal to 42, the drug is distributeduniformly throughout the body tissueA Lrd that is substantially less than 42indicates that the drug is retained inthe bloodstream. This typically occurswhen the drug binds to some intravascular constituent such as albumin orother plasma proteins. A V, that is
-
8/2/2019 Ciccone Pharmacokinetics Article 1995
3/9
able. Pharm ucokinetic Purameters for Some C omm on Medicationfsubstantially greater than 42 indicatesthat the drug is sequestered outside ofthe vascular comparrment by bindingto some extravascular tissue such asskeletal muscle.ral Volume ofBioavailability Distributionb Clearanceb(% I (L) (mumin) Values for V of some common medi-cations are listed in the Table. Again,factors that affect Vd can have impor-tant implications on the amount ofdrug that reaches the target tissue. Areduction in plasma proteins, for in-stance, can have dramatic effects on adrug with a small V, that is normallyretained in the bloodstream. Nonste-roidal anti-inflammatory drugs (aspirin,ibuprofen, and so on) typically have alow V because these drugs bindextensively to plasma proteins such asalbumin. A reduction in plasma pro-teins secondary to liver disease ornutritional deficits would increase theV, of these drugs because the drugwould not be retained in the circula-tion and would be distributed moreextensively throughout the body. Thisgreater distribution would also resultin larger quantities of the drug reach-ing the extravascular tissues, whichcould produce harmful effects if theseconcentrations reach toxic levels.
~ -
91 2354.320.9
Dose dependent7.721.4
Clearance
miprarnineithium
ethotrexaterednisone
Clearance is the rate at which theactive form of the drug is removed oreliminated from the body. Eliminationtypically occurs by die combinedprocesses of drug metabolism (whichtakes place prirnady in the liver) anddrug excretion (which takes placeprimarily in the kidneys).' Eliminationby other organs, including the lungs,skin, and gastrointestinal tract, can alsocontribute to drug clearance. Systemicclearance, therefore, is the cumulativeability of the liver, kidneys, and va~i-ous other tissues to eliminate a drugfrom the body.Clearance of a drug by a specific or-gan (CL,,,,) can be calculated asfollows:
data in Gilman AG, Rall 7W,Nies AS, Taylor P, eds. 7h e Phamacological Ci-C,of Therapeutics.8th ed . New York, r \ ! : Pergamon Press; 1990. (2 ) CLO, = Qx-Parameters based on a typical 70-kg person. Ci
to transdermal administration.
-
8/2/2019 Ciccone Pharmacokinetics Article 1995
4/9
where Q is the blood flow to theorgan, Ci is the concentration of drugentering the organ, and C, is the con-centration of drug exiting the organ.The ratio created by the differencebetween Ci and C divided by C, isalso termed the extraction ratio (ER)because this parameter indicates howwell the organ can remove the drugfrom the bloodstream. Hence, thisequation illustrates that the ability ofan organ to clear a drug from thebody is dependent on taro primaryfactors: the amount of blood reachingthe organ (Q) and the ability of theorgan to extract the drug from thebloodstream (ER). Factors that altereither Q or ER will affect the clearanceof a drug.Drugs can also be classified as high-extraction or low-extraction drugsdepending on how they are clearedby the primary organ responsible forclearing each drug, usually the liver.5High-extraction drugs have a high ERin a particular organ and undergoextensive elimination by that organ.Clearance of high-extraction drugs isalso said to be flowdependent be-cause the rate-limiting factor in elimi-nation is the amount of blood flowthat delivers the drug to the organ.Lowextraction drugs have a smallerER because the organ is less able toclear the drug from the bloodstream.Clearance of these drugs is less sensi-tive to changes in organ perfusion, butany further reduction in the organ'smetabolic capacity due to disease orthe presence of other drugs can causedramatic changes in clearance of low-extraction drugs. The relevance ofhigh-extraction and low-extractiondrugs during specific interventionssuch as exercise will be discussed laterin this article.E M f Exercise onPhamacokineticsExercise can produce dramaticchanges in the pharmacokinetic vari-ables of certain drugs, resulting inaltered clinical responses because theamount of drug reaching the blood-stream and ultimately reaching targettissues is excessively high or exces-
sively low.6s7 The magnitude of thesechanges is dependent on factors thatpertain to the characteristics of eachdrug as well as exercise-related factorssuch as exercise intensity, mode, andduration. Only the effects of an exer-cise bout on pharmacokinetics arereviewed here because the changesproduced by a single exercise boutcan cause sudden changes in pharma-cokinetics that may have an immediateimpact on patients who are exercisingduring physical therapy. Exercise train-ing can also produce changes in phar-macokinetics, but these changes tendto occur over a longer period of timeand cause a slower and fairly predict-able change in the patient's responseto certain medications. For more infor-mation about the effects of exercisetraining, the reader is referred to areview on this topic by D~ss ing .~Effect on Exemise onBioavailabilityExercise can affect bioavailability byaltering drug absorption at the site ofdrug administration. Exercise can affectabsorption in two primary ways. First,increased tissue heat during exercisewill increase kinetic molecular move-ment and thus increase diffusion ofdrug molecules across biologicalmembranes. Second, drug dispersionaway from the drug delivery site canbe increased or decreased, dependingon whether exercise increases or de-creases blood flow to the site of drugadministration. These two factors,therefore, must be considered alongwith the drug administration route todetermine whether an exercise boutwill increase or decrease bioavailabil-ity. Exercise may produce opposingeffects on absorption of orally adminis-tered drugs, for instance, because theincreased kinetic movement of thedrug across the gastrointestinal mu-cosa may be offset by the reduction insplanchnic blood flow commonly seenduring moderate- to high-intensityexercise."Studies that have examined the effectof exercise on bioavailability followingoral drug administration have pro-duced conflicting results. In a study of10 patients with Parkinson s disease, a
dose of levodopa was administeredorally du m g a bout of exercise on acycle ergometer.1 Levodopa absorp-tion was delayed in 5 patients, wasincreased in 3 patients, and was un-changed in 2 patients. Another studyexamined the effects of the absorptioof midazolam (a sedative-hypnoticagent) during 50 minutes of treadmilrunning in 16asymptomatic volun-teers." The authors stated that mida-zolam absorption was impaired durinexercise because the amount of drugappearing in the plasma (peak plasmconcentration) was significantly lowethan during a control, nonexerciseperiod. In that same study, the phar-macokinetics of ephedrine (a decon-gestanthronchodilator) were not significantly affected by the exercisebout. Peak plasma concentrations ofthree different antibacterial drugs (sufamethizole, tetracycline, and doxycycline) were all s im ca nt ly increasedin asymptomatic volunteers undergo-ing 4 hours of moderate exercise,12and the absorption of digoxin (a car-diac glycoside used to treat heart fdilure) was reported to increase duringhours of intennittent cycling exerciseperformed at moderate intensity.lgConversely,3 hours of moderate,intermittent exercise ( 5 minutes ofexercise,5 minutes of rest) did notalter the plasma concentration of quiidine (an antiarrhythmic), salicylate Canti-i&ammatory/anaIgesic), or sul-fadirnidine (an antibacterial). 4 Henceexercise can produce variable effectson bioavailability following oral ad-ministration, and these effea areprobably dependent on the characteristics of the drug and the intensity,duration, and type of exercise bout.
The effect of exercise on systemicbioavailability following subcutaneouor intramuscular injection is somewhmore predictable. Absorption is geneally increased when drugs are injecteinto or near actively exercising mus-c l e ~ . ~his observation may be ex-plained by the fact that transmem-brane diffusion and blood flow areboth increased in exercising tissuesand the drug is absorbed more quickand dispersed more rapidly away frothe injection site and into the systemcirculation. There is also some evi-
Physical Therapy /Volume 75, Numbt
-
8/2/2019 Ciccone Pharmacokinetics Article 1995
5/9
f subcutane-concomitant in-
exercising tissues
absorption.15The opposite effectif drugs are injected intocising tissues, and absorption
if blood is shuntedf injection and
bioavailability of in-ted drugs can have important clini-
ations because the injected
well-ented with insulin adrninistra-
in patients with diabetes melli-l7 Exercise involving an
hus increases systemic bioavail-Ls.l5-'7 A sudden increase in
be h a h l be-hypoglycemic
ise because exercise works syn-ically with insulin to reduce
fac~orindependently.l8J9 Patients
therefore select injection sites
ay have to alter the exer-gimen so that the exercising
at are administered trans-e transdermal absorption because
skin temperature andsed skin hydration secondary to
" Absorption will also beif exercise causes an in-
in cutaneous blood flow, al-amount of cutaneous vaso-
ple who are hypovolemic and exercis-ing in extreme heat.20*21The clinical implications of increasedtransdermal administration are numer-ous, especially considering that moreand more drugs are being adminis-tered through transdermal patches.Plasma concentrations of medicationssuch as nitroglycerin have been ob-served to increase as much as three-fold in asymptomatic volunteers un-dergoing cycling exercise whilewearing a nitroglycerin pat~h.~O,~lhisoccurrence could have beneficialeffects if the increased plasma nitro-glycerin concentration helps offset anincreased tendency for exercise-induced anginal artacks. Conversely,negative effects would be seen if theincreased plasma nitroglycerin potenti-ates exercise-induced vasodilation,thus leading to excessive hypotension.Additional research is needed to deter-mine the potential effect5 of changesin systemic bioavallability caused byexercise in patients receiving nitroglyc-erin and other medications (estrogen,nicotine) through transdermal patches.The effect of exercise on transdermalbioavailability also has implications fordrugs administered through ionto-phoresis and phonophoresis. Exerciseinvolving the administration site couldtheoretically increase the amount ofdrug delivery if exercise is performedimmediately before or after ionto-phoretic or phonophoretic treatment.No studies are available, however, todocument this phenomenon. Likewise,increased blood flow to the site ofdelivery may be counterproductive ifthe goal of transdermal administrationis to focus drug delivery to a specificstructure such as a tendon or bursa.lncreased regional blood flow maycause the drug to be dispersed awayfrom the delivery site, thus negatingthe desired local effect. Again, the lackof research in this area makes it diffi-cult to determine whether exercisewould have a counterproductive effecton local drug disposition because ofan increased washout from the site ofapplication.
Finally, exercise can increase the rateof absorption and bioavailability of
drugs that are administered by inhala-tion, including antiasthmaticshron-chodilators such as terbutaline. Onestudy noted that inhalation of terhutal-ine just prior to a bout of stationarycycling caused an increase in the rateof appearance of the drug in theplasma and an increase in peakplasma concentrations of this dn1g.24This effect was attributed to a concom-itant increase in pulmonary blood flowand increased movement of drugacross the alveolar membranes. Thiseffect might be advantageous becausethe moderate increase in plasma druglevels seen during exercise couldoffset an increase in the tendency forexercise to initiate an asthma attack.More research is needed to determinewhether the increased bioavailabilityof inhaled antiasthmatic drugs duringexercise is clinically beneficial as evi-denced lly a decrease in exercise-induced asthma.Effect of Exemise on DmgDistributionExercise has been reported to cause adecrease in the V of certain medica-tions, indicating that the plasma con-centration of the drug is increased."An exercise-induceddecrease in Vdhas been observed for several orallyadministered drugs such as the cal-cium channel blocker verapamil,25 thecardiac beta-blocker pr0pranolo1,25-2~the antiasthmatic agent the0phylline,2~and the central nervous system stimu-lant ~affeine .~9xercise also decreasedthe V of atropine (an anticholinergicagent) when this drug was adminis-tered by intramuscular injection.30sj1The observed decrease in Vd seenwith these drugs may be caused tosome extent by the effect of exerciseon other pharmacokinetic variables.For instance, an increase in bio-availibility combined with a decreasein drug clearance could account forincreased plasma drug levels, thusdecreasing Vd. This fact would beespecially true for dn ~gshat tend tobe retained in the plasma, that is,drugs that tend to have a low V un-der normal (nonexercise) conditions.The decrease in Vd seen with certaindnigs may also be caused by the re-
Physical Therapy / Volume 75, Number 5 /May 1995
-
8/2/2019 Ciccone Pharmacokinetics Article 1995
6/9
distribution of blood flow and plasmavolume that occurs during an exercisebout. Plasma volume may decrease byas much as 12% to 18%during exer-cise,32,33and this decrease will cause arelative increase in the concentrationof drugs located in the bloodstream.The decrease in V of some drugs,however, is not fully explained bychanges in plasma volume, and therapid decrease in Vdobserved fordrugs such as propranolol has beenattributed to other factors, such asincreased entry of the drug into thebloodstream after the drug is displacedfrom extravascular binding sites.3"Regardless of the exact mechanism,exercise can cause a relative increasein intravascular concentration of cer-tain drugs, as evidenced by a decreasein the Vdof these agents.Conversely,Vdmay increase for somedrugs during exercise, indicating thatmore of the drug is drawn out of thebloodstream and into extravasculartissues. The most common example isdigoxin, which binds to the cell mem-brane of skeletal m~scle.35.3~xerciseappears to increase the affinity ofskeletal muscle binding sites fordigoxin, thus causing plasma digoxinconcentration to decrease and muscleconcentration to in~rease.35,3~Volume of distribution for a givendrug can increase or decrease, de-pending on a number of factors suchas the binding properties of the drugand concomitant changes in otherpharmacokinetic variables duringexercise. The intensity and duration ofthe exercise bout are also factors thatcan influenceV,, as evidenced by thefact that the Vd for propranolol andverapamil was not altered duringprolonged (7-hour), intermittent sub-maximal exerci~e.3~,39If V, does change during exercise, theclinical implications of these changesare often unclear. A decrease in the Vdcould mean that more drug is beingsequestered in the bloodstream andless drug is available to reach extravas-cular target tissues. Aspirin and similarnonsteroidal anti-inflammatory drugs,for instance, would be less effective ifthey are retained excessively in the
vascular compartment and are notable to reach peripheral tissues suchas an arthritic joint. Conversely, anincrease in V could mean that drugsreach the peripheral tissues moreextensively than expected, and thisfact could precipitate adverse effects ifdrug concentrations at the target tis-sues are excessively high. Increaseddigoxin concentrations could reach themyocardium, for example, thus in-creasing the possibility of cardiotoxiceffects. Thus, exercise clearly can affectthe distribution of certain medications,but it remains to be seen whetherthese particular pharmacokineticchanges ultimately cause clinicalproblems.Effect of Exetcise on D N ~Clearance
Exercise produces transient changes inliver function that could potentiallyalter hepatic drug clearance. Hepaticblood flow decreases progressively asexercise intensity increases, with he-patic perfusion being reduced by asmuch as 50%when exercise intensityapproaches 7@/0 of maximal oxygenuptake.9A decrease in hepatic perfu-sion during exercise can potentiallydecrease the clearance of drugs thatare metabolized in the liver, especiallyhigh-extraction drugs.RRecall thatmetabolism of high-extraction drugs isessentially dependent on delivery ofthe drug via the bloodstream; hence,clearance of these drugs should bedecreased if hepatic perfusion de-creases during exercise. Low-extraction drugs will probably not beaffected as greatly during exercisebecause clearance of these drugs isdependent on the metabolic capacityof the liver rather than on hepaticblood flow.8Given the rather pronounced effect ofexercise on hepatic perfusion, exerciseshould produce predictable declines inthe clearance of drugs that undergoextensive hepatic metabolism. Only alimited number of studies have investi-gated this phenomenon, however, andthese studies have generally failed todiscern any dramatic reduction inhepatic clearance even with high-extraction drugs such as verapamil
and propranol01.38~39t is not clearhow hepatic clearance can remainunchanged during exercise, although adecrease in hepatic clearance may bemasked during exercise by other fac-tors such as increased nonhepaticclearance and changes in other phar-macokinetic variables (absorption anddistribution). Nonetheless, additionalresearch is needed to determine con-clusively whether exercise produceschanges in the hepatic clearance ofvarious medications, especially high-extraction drugs.The kidney also undergoes transientchanges during exercise that can affectdrug clearance. Renal blood flow andglomerular filtration rate decrease byas much as 65% and 300!, espectively,at higher exerciseClearance of drugs that undergo flow-dependent elimination by the kidneys(high-extraction drugs), therefore, canbe decreased during exercise becauseless of the drug is reaching thenephron." Other changes in renalfunction, including decreased secre-tion of drugs into the renal tubule andincreased reabsorption of acidic drugsfrom the tubule, can contribute to anexercise-induced decrease in renaldrug clearance.6A limited number of studies haveinvestigated the effects of exercise onrenal drug clearance, and these studieshave typically shown reductions inrenal clearance ranging from 8% to84% depending on the particular drugand the mode and intensity of theexercise bout.*+45 Thus, an exercbe-induced decrease in renal eliminationseems fairly predictable and consistentwith what would be expected consid-ering the changes in renal hemody-narnics and filtration that are known tooccur during exercise. Still, additionalresearch is needed to determine theextent that these decreases in renaldrug clearance can cause subsequentalterations in the clinical response tospecdic drugs.Summary of Exercise E i k t sExercise produces complex changes inthe pharmacokinetics of certain drugs,which can alter the amount of drug
Physical Therapy / Volume 75, Number 5 / May 1995
-
8/2/2019 Ciccone Pharmacokinetics Article 1995
7/9
hese changes, however,highly variable, depending on
each drug; the route of drug admin-is
An exception,d bioavailability of dmgs adminis-
is) will typically be in-if the site of a h s t r a t i o n is
vely involved in the exercise bout.
if anyin the clinical response is
of Physical Agents on
systemically administered drugs byecting factors such as local blood
f a drug to a specific tissuee (tendon, muscle, bursa, and so
ct drugryotherapy site. Although drug
heating and cooling agents have
assume that delivery of system-lly administered drugs to the tissues
thermal agents will be
locally by intramuscular or subcutane-ous injection. Application of local heatto the site of drug administration willalmost certainly increase dispersion ofthe drug away from the delivery site.This increased dispersion may causeuntoward effects because the drug isdelivered too rapidly into the systemiccirculation and the plasma concentra-tion increases more rapidly thanwould occur without heating. Applica-tion of heat over the site of subcutane-ous insulin injection, for example,would accelerate absorption into thebloodstream, thus potentially causingexcessive insulin effects and hypogly-cemia. Application of heat over thesite of these types of injection shouldprobably be avoided, although thereare really no definitive research studiesthat support this belief.Locally applied heat and cold alsohave the potential to alter transdermaldrug lunetics, but these effects arepoorly understood. It has been shownthat systemic absorption of ionto-phoretically administered drugs can beincreased or decreased in the presenceof drugs that produce local vasodila-tion or vasoconstriction, resp ecti ~el y. ~It seems reasonable, therefore, thatthermal agents that produce simdarvasoactive effects will also influenceabsorption of drugs applied by ionto-phoresis or phonophoresis. Applica-tion of local heat, for instance, couldbe used to intentiondlly increase thesystemic absorption of locally applieddrugs if the desired effect is to increasethe systemic bioavailability of thesemedications.Anecdotal reports have also suggestedthat applying heat after iontophoresisor phonophoresis may be beneficialbecause the drug will be dispersedmore readily within the subcutaneoustissues due to increased local bloodflow. This rationale seems question-able, however, if the goal of transder-ma1 application is to focus the drug toa specific subcutaneous tissue or struc-ture. Increasing local tissue perfusionwould cause a washout of the drugfrom the administration site, thus ne-gating the benefit of local transdermaldelivery. Again, there is no experimen-tal research to document the positive
or negative effects of local heat follow-ing transdermal delivery, but the po-tential washout effect should certainlybe considered if local heat is applieddirectly after transdermal delivery.The effects of other physical agentssuch as electrotherapeutic devices onpharmacokietics are not known.Certain types of electrical stimulationof skeletal muscle will increase localheat and blood flow, and this effectcan potentially increase drug deliveryto the stimulated muscle. Again, it isnot known whether this effect is suffi-cient to cause a meaningful increase inlocal drug delivery. Conversely, awashout effect may be caused if thestimulated muscle was used as a sitefor depot injection of a slow-releasedrug formulation, and stimulation ofthe injected muscle should probablybe avoided.Eltects of Manual Techniqueson PhannacokineticsManual techniques, including massage,can increase drug absorption fromlocal subcutaneous injection sites. Thiseffect has been documented withinsulin absorption, where externalmassage has been shown to increasethe disappearance of insulin from theinjection site and thus increase plasmainsulin con~entration.~~nterestingly,this effect has been observed in theabsence of any simultaneous increasein subcutaneous blood flow, suggest-ing that massage increases insulinabsorption through some type of me-chanical effect on local t i s s ~ e s . ~heincreased absorption produced bymassage can have clinical implicationsif plasma drug levels are increased tothe point where untoward effects (eg,hypoglycemia) begin to occur.The effect of massage on delivery ofsystemically administered drugs tolocal tissues is not known. Massagecould conceivably increase drug deliv-ery to the massaged tissues by increas-ing local blood flow or by some typeof mechanical "milking" effect. Theextent to which massage can increasedelivery to specific tissues andwhether this has any clinical relevanceis unclear.
Physical Therapy / Volume 75, Number 5 /May 1995
-
8/2/2019 Ciccone Pharmacokinetics Article 1995
8/9
SummaryPharmacolunetics involves the pro-cesses that affect drug dispositionwithin the body. Certain pharmacoki-netic variables such as bioavailability,V,, and clearance must be known toestimate the proper dosing regimenthat will enable a drug to reach itstarget tissue at an appropriate thera-peutic concentration. Certain physicaltherapy interventions have the poten-tial to produce transient changes inthe pharmacokinetic profile of certaindrugs so that the clinical response tothe drug is altered. In particular, exer-cise, thermal agents, and massage canaffect the disposition of certain agentsby altering one or more pharmacoki-netic variables. This seems especiallytrue for drugs that are administeredlocally by transdermal techniques orby subcutaneous or intramuscularinjection. Exercise, local heat, or mas-sage of the ah s t r a t i o n site canpotentially increase absorption of adrug, causing a relative increase insystemic bioavailability. This increasedbioavailability can increase the inci-dence of side effects, because theplasma concentrations may increasemore quickly and to a greater extentthan expected.
Clinicians, therefore, should be awareof the need to modlfy certain treat-ments so that the effect on local drugabsorption, distribution, and metabo-lism is minimized. Likewise, exerciseand other physical therapy interven-tion can cause physiological changesthat could alter the disposition ofsystemically administered drugs, andthe possibility that these interventionsmay have an impact on pharmacoki-netics should always be consideredwhen a patient exhibits any untowarddrug response.
References1 Benet LZ, Mitchell JR, Sheiner LB. Introduc-tion. In: Gilman AG, Rall TW, Nies AS, TaylorP, eds. The Pharmacological Basis of 7hera-peutics. 8th ed . New York, NY: PergamonPress; 1990.2 Levy RH, Bauer LA. Basic pharmacokinetics.7he r Drug M onit. 1986;8:47-58.
3 Pang KS, Xu X, St Pierre MV. Determinantsof metabolite disposition. Ann Rev PhannacolToxicol. 1992;32:625669.4 Perucca E, Grimaldi R, Crema A. Interpreta-tion of drug levels in acute and chronic dis-ease states. Clin Phannacokinet. 1985;10:498-513.5 Benet LZ. Pharmacokinetics: absorption,distribution, and elimination. In: Katzung BG,ed . Basic and Clinical Pharmacology. 5th ed.East Norwalk, Conn: Appleton & Lange; 1992.6 Van Baak MA. Influence of exercise on thepharmacokinetics of drugs. Clin Phannacoki-net. 1990;19:32-43.7 Sweeney GD. Drugs: some basic concepts.Med Sci Sports E3Cerc. 1981;13:247-251.8 Dossing M. Efect of acute a nd chronic ex-ercise on hepatic drug metabolism. Clin Phar-macokinet. 1985;10:426-431.9 Rowell LB. Human cardiovascular adjust-ments to exercise and thermal stress. Physio-logic Rev. 1974;54:75-159.10 Carter JH, Nutt JG, Woodward WR. Theefect of exercise on levodopa absorption.Neurology. 1992;42:2042-2045.11 Stromberg C, Vanakoski J, Olkkola KT,et al. Exercise alters the pharmacokinetics ofmidazolam. Clin Pharmacol 7her. 1992;51:527-532.12 Ylitalo P, Hinkka H, Neuvonen PJ. Effectof exercise on the serum level and urinaryexcretion of tetracycline, doxycycline and sul-famethizole. Eur J Clin P hannacol . 1977;12:367-373.13 Jogestrand T, Andersson K. Efect of physi-cal exercise on th e pharmacokinetics ofdigoxin during maintenance treatment.J Cardiovasc Pharmacol. 1989;14:73-76.14 Aslaksen A, Aanderud L. Drug absor ptionduring physical exercise. Br J Clin Phannacol.1980;10:385385.15 Fernqvist E, Linde B, Ostman J, Gunnars-son R. Efects of physical exercise on insulinabsorption in insulin-dependent diabetics: acomparison between human and porcine in-sulin. Clin Physiol. 1986;6:489-498.16 Koivisto VA, Felig P. Effects of leg exerciseon insulin absorption in diabetic patients.N Engl J Med. 1978;298:79-83.17 Thow JC, Johnson AB, Antsiferov M,Home PD. Exercise augments the absorptionof isophane (NPH) insulin. Diabet Med. 1989;6:342-345.18 Mikines KJ, Sonne B, Farrell PA, et al. Ef-fect of physical exercise on sensitivity andresponsiveness to insulin in humans.Am JPhysiol. 1988;254:E248-E259.19 Richter EA, Mikines KJ, Galbo H, Kiens B.Efect of exercise on insulin action in humanmuscle. J Appl Physiol. 1989;66:876-885.20 Nadel ER. Recent advances in temperatureregulation during exercise in humans. FedBOC.985;44:2286-2292,21 Smolander J, Kolari P, Korhonen 0 , lmari-nen R. Skin blood flow during incrementalexercise in a thermoneutral and hot dry envi-ronment. Ezcr J Appl Physiol. 1987;56:275280.22 Barkve TF, Langseth-Manrique K, Bre-desen JE, Gjesdal K. Increased uptake oftransdermal glyceryl trinitrate during physicalexercise and during high ambient tempera-ture. Am Heart J. 1986;112:537-541.23 Weber S, de Lauture D, Rey E, et al. Theefects of moderate sustained exercise o n the
pharmacokinetics of nitroglycerine. B r j C lPhannacol . 1987;23:105105.24 Schmekel B, Borgstrom L, Wollmer P. Eercise increases the rate of absorption of inhaled terbutaline. Chest. 1992;101:742-74525 Van Baak MA, Mooij JM, Schifers PM. Eercise and the pharmacokinetics of propran101, verapamil, and atenolol. Eur J Clin Phamacol . 1992;43:547-550.26 Henry JA, Iliopoulou A, Kaye CM, et alChanges in plasma concentrations of acebulol, propranolol a nd indomethacin duringphysical exercise. Life Sci. 1981;28:19251927 Hurwitz GA, Webb JG, Walle T, et al.Exercise-induced increments in plasma levof propranolol and noradrenaline. Br J ClinPhannacol . 1983;16:599-608.28 Schlaefer F, Engelberg I, Kaplanski J,Danon A. Efect of exercise and environmeheat on theophylline kinetics. Respiration.1984;45:438-442.29 Collomp K, Anselme F, Audran M, et alEffects of moderate exercise on the pharmakinetics of cafeine. Eur J Clin Phannacol.1991;40:279-282.30 Kamimori GH, Smallridge RC, RedmondDP, et al. The ef ect of exercise on atropinepharmacokinetics. EurJ Clin Phannacol.1990;39:395-397.31 Mund ie TG, Pamplin CL, PhillipsYY,Smallridge RC. Efect of exercise in sheep othe absorption of intramuscular atropine sufate. Phannacology. 1988;37:132-136.32 Costill DL, FinkWJ. Plasma volumechanges following exercise and thermal dedration. J Appl Physiol. 1974;37:521-525.33 Harrison MH, Edwards RJ, Leitch DR. Effect of exercise and thermal stress on plasmvolume. J Appl Physiol. 1975;39:925-331.34 Powis G , Snow DH. The effects of exerand adrenaline infusion upon the blood leof propranolol and antipyrine in the horseJ Phannacol E rp 7her. 1978;205:725-731.35 Joretag T, Jogestrand T. Physical exercisand binding of digoxin to skeletal muscle:effect of activation frequency. Eur J Clin Phmacol . 1984;27:567-570.36 Joretag T, Jogestrand T. Physical exerciand digoxin binding to skeletal muscle: reltion to exercise intensity. Eur J Clin Phanncol. 1983;25:585-588.37 Jogestrand T, Sundqvist K. Efect of phycal exercise on the digoxin concentrations skeletal muscle and serum in man. ClinPhysiol. 1981;1:99-104.38 Arends BG, Bohm ROB, van KemenadeJE, et al. Influence of physical exercise on pharmacokinetics of propran olol. Eur J CliPhannacol. 1986;31:375-377.39 Mooy J, Arends B, van Kemenade J, et Influence of prolonged submaximal exercion the pharmacokinetics of verapamil in hmans. J Cardiovasc Pharmacol. 1986;8:940942.40 Castenfors J. Renal function during prolonged exercise. Ann NYA cad Sc i. 1977;3151-159.41 Grimby G. Renal clearances during prolonged supine exercise at diferent loads.J Appl Physiol. 1965;20:1294-1298.42 Poortmans JR. Exercise an d renal functExerc Sport Sci Rev. 1977;5:255-294.
Physical Therapy / Volume 75, Number 5 / May 1995
-
8/2/2019 Ciccone Pharmacokinetics Article 1995
9/9
G, Winer N, Cohen I. adimidine and procainamide. IntJ Clin Pbar- subcutaneously injected insulin preparations.of exercise on renal clearance of ateno- macol lher Toxicol. 1985;23:548-553. Diabetes Care. 1982;5:77-91.Pbannaceutical Sci. 1980;69:344 345. 46 Singh P, Maibach HI. Transdermal 48 Linde B. Dissociation of insulin absorption
RD , Side11FR. Effects of heat and iontophoresis: pharmacokinetic consider- and blood flow during massage of a subcuta-ations. Clin Pbannacobinet. 1994;26:327-334. neous injection site. Diabetes Care. 1986;9:Clin Pbannacol lher. 1973;14:8389. 47 Berger M, Cuppers HJ, Hegner H, et al. 570-574.
P, Hinkka H. Effect of exercise o n Absorption kinetics and biologic effects of
2
Call for ReviewersPhysical Therapy is currently seeking qualified individuals to serve asmanuscript reviewers, Reviewers should have:Ixtensive experience in area(s) of content expertiseIxperience as authors of articles published in peer-reviewed ournalsFamiliarity with peer review is essential,If you are interested in becoming a reviewer for the Journal, please senda cover letter and a copy of your curriculum vitae to:EditorPhysical Therapy1111 North Fairfax StreetAlexandria, VA 22314-1488Interested in becoming involved, but not sure you have thetime to review manuscripts? The Journal is also looking for articleabstracters and book/software/videotape reviewers. Send us aletter expressing your interest and stating your general areasof expertise, along with a copy of your curriculum vitae,We look forward to hearing from you.
351 Physical Therapy / Volume 7 5 , Number 5 /May 1995