chronic urticaria
124
Updates in Chronic Urticaria Management BY PROF. ASHRAF OKBA HEAD OF THE DEPARTMENT OF IMMUNOLOGY AND ALLERGY AIN SHAMS UNIVERSITY
-
Upload
ashraf-okba -
Category
Health & Medicine
-
view
152 -
download
1
Transcript of chronic urticaria

Updates in Chronic Urticaria Management
BY
PROF. ASHRAF OKBA
HEAD OF THE DEPARTMENT OF
IMMUNOLOGY AND ALLERGY
AIN SHAMS UNIVERSITY
Agenda
2
Introduction and definitions
Prevalence
Mast cell and urticaria pathogenesis
Diagnosis
Urticaria burden
Assessment of disease severity and patient quality of life
Guidelines updates in urticaria treatment
Urticaria is a disease characterized by thedevelopment of wheals (hives), angioedema, or both.
Urticaria Definition:
Acute urticaria is defined as the occurrence of spontaneouswheals, angioedema, or both for <6 weeks, while in chronicurticaria symptoms last for more than 6 weeks.
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
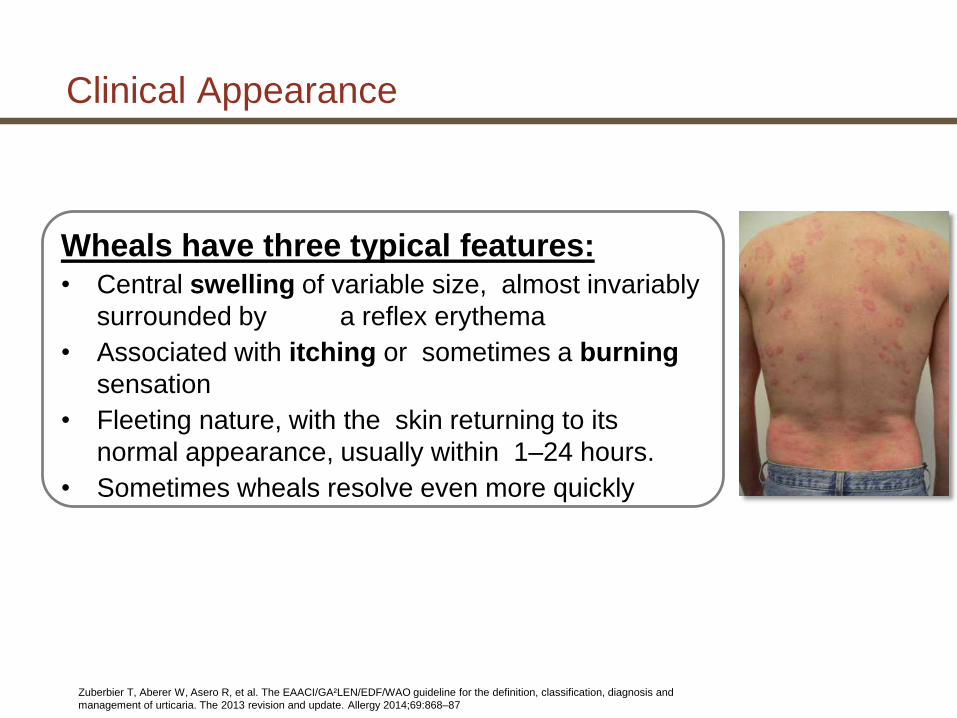
Clinical Appearance
Wheals have three typical features:• Central swelling of variable size, almost invariably
surrounded by a reflex erythema
• Associated with itching or sometimes a burning
sensation
• Fleeting nature, with the skin returning to its
normal appearance, usually within 1–24 hours.
• Sometimes wheals resolve even more quickly
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87

Angioedema Definition
• /an·gio·ede·ma/ a vascular reaction involving the deep dermis or subcut
aneous or submucosal tissues,representing localized edema caused by
dilatation and increased permeability of the capillaries,
• Sometimes pain rather than itching.
• Frequent involvement below mucous membranes
• Its resolution is slower than that for wheals and can take up to 72
hours 1
• Angioedema most often involves the
eyelids , lips, tongue, genitalia,
hands and feet with the larynx ,
gastrointestinal and urinary bladder
being less commonly affected.
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
Angio-oedema of the lip (a) during and (b) 3
days after an attack. (Courtesy of St John’s
Institute of Dermatology, London, UK.)
7
Acute Urticaria: ˂ 6 Weeks
Chronic Urticaria: ≥ 6 Weeks
Classification of Urticarias
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
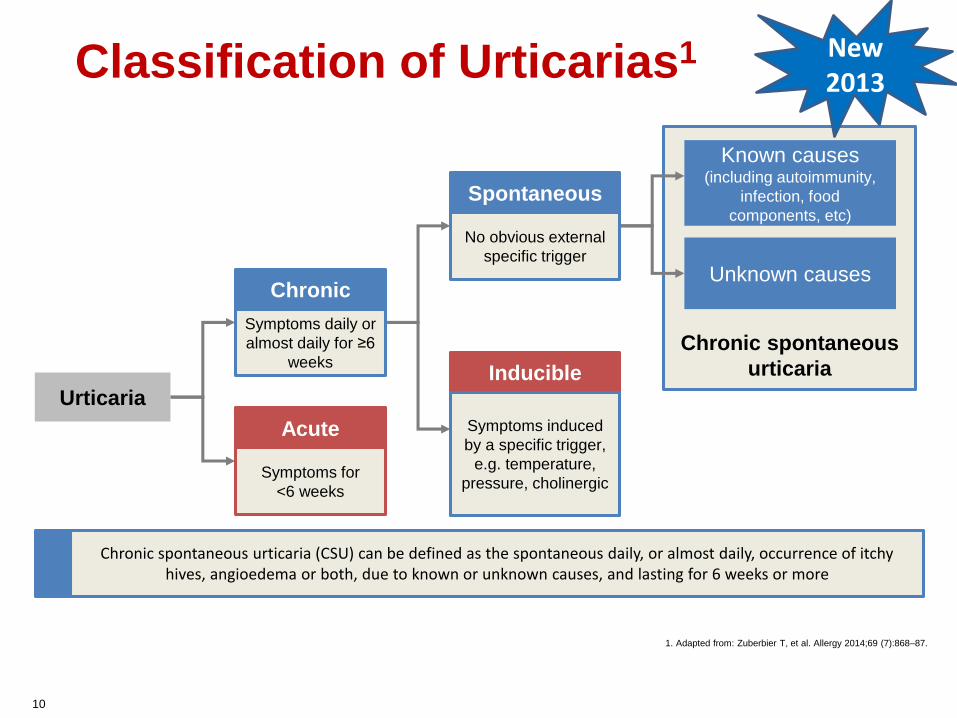
Classification of Urticarias1
1. Adapted from: Zuberbier T, et al. Allergy 2014;69 (7):868–87.
Chronic spontaneous
urticaria
Chronic
Acute
Spontaneous
InducibleUrticaria
Known causes (including autoimmunity,
infection, food
components, etc)
Unknown causes
Chronic spontaneous urticaria (CSU) can be defined as the spontaneous daily, or almost daily, occurrence of itchy hives, angioedema or both, due to known or unknown causes, and lasting for 6 weeks or more
Symptoms daily or
almost daily for ≥6
weeks
No obvious external
specific trigger
Symptoms for
<6 weeks
Symptoms induced
by a specific trigger,
e.g. temperature,
pressure, cholinergic
10
New2013

Chronic Urticaria: What is in Name?
Is it chronic urticaria, chronic idiopathic urticaria, or chronic spontaneous urticaria?
The term chronic indicates that urticaria is present for more than 6 weeks.
The cause of chronic urticaria is known in approximately 25% of patients (refers primarily to those with physically inducible urticarias)
Kaplan AP. Therapy of chronic urticaria: a simple, modern approach. Ann Allergy Asthma Immunol.2014 (Article in press)
For CSU, the cause of the spontaneous urticariasapproaches zero because the etiology is not known even though there is an association with autoimmunity in approximately 45% of patients and,
The term spontaneous rather than idiopathic emphasizes that it is endogenous rather than exogenous and non inducible rather than inducible.
Chronic Urticaria: What is in Name?
Kaplan AP. Therapy of chronic urticaria: a simple, modern approach. Ann Allergy Asthma
Immunol.2014 (Article in press)
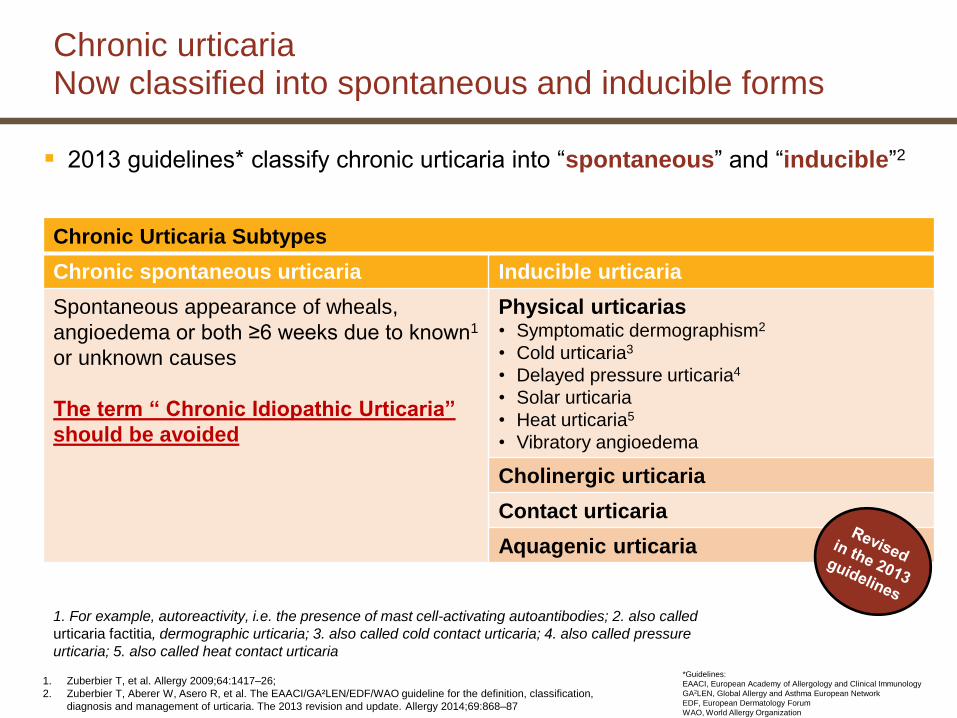
Chronic urticariaNow classified into spontaneous and inducible forms
2013 guidelines* classify chronic urticaria into “spontaneous” and “inducible”2
Chronic Urticaria Subtypes
Chronic spontaneous urticaria Inducible urticaria
Spontaneous appearance of wheals,
angioedema or both ≥6 weeks due to known1
or unknown causes
The term “ Chronic Idiopathic Urticaria”
should be avoided
Physical urticarias• Symptomatic dermographism2
• Cold urticaria3
• Delayed pressure urticaria4
• Solar urticaria
• Heat urticaria5
• Vibratory angioedema
Cholinergic urticaria
Contact urticaria
Aquagenic urticaria
1. For example, autoreactivity, i.e. the presence of mast cell-activating autoantibodies; 2. also called
urticaria factitia, dermographic urticaria; 3. also called cold contact urticaria; 4. also called pressure
urticaria; 5. also called heat contact urticaria
*Guidelines:
EAACI, European Academy of Allergology and Clinical Immunology
GA2LEN, Global Allergy and Asthma European Network
EDF, European Dermatology Forum
WAO, World Allergy Organization
1. Zuberbier T, et al. Allergy 2009;64:1417–26;
2. Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification,
diagnosis and management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87

Prevalence of Urticaria
Estimated to occur in 15-23% of the population
Up to 40% of patients who have chronic urticaria longer than six months will still have urticaria 10 years later
Approximately 40% of patients with chronic urticaria have angioedema
All age groups can be affected, however the peak incidence is seen between 20 and 40 years of age. i.e, patients are primarily affected during important years of their working age.
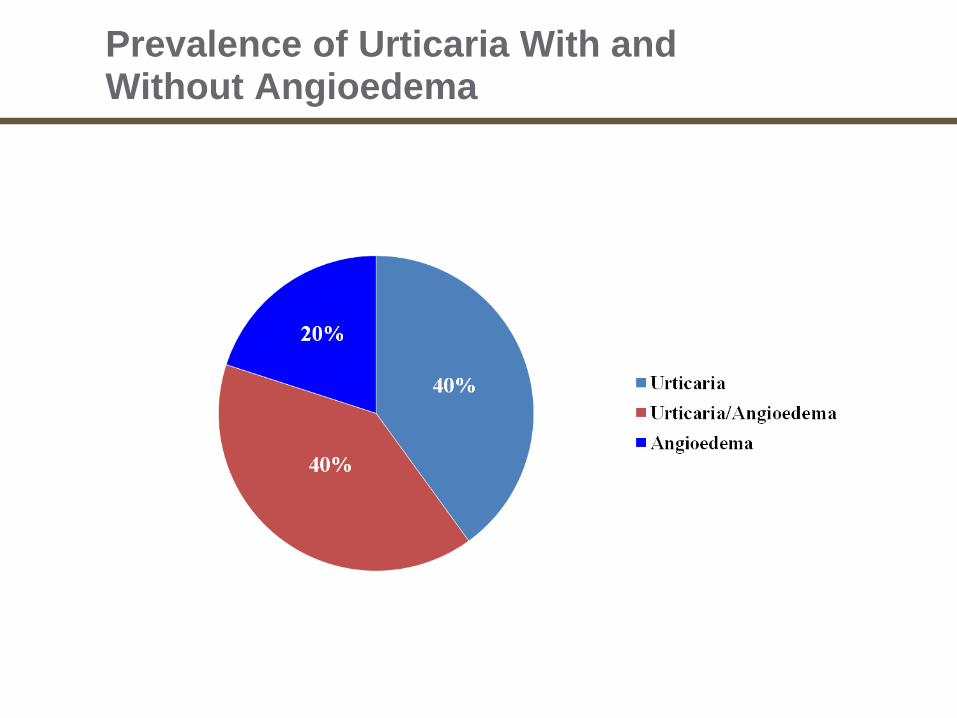
Prevalence of Urticaria With and Without Angioedema

Urticaria
Acute urticaria refers to hives lasting less than six weeks; in approximately 15-20% of cases an inciting cause can be identified
Chronic urticaria refers to hives lasting longer than 6-8 weeks; identification of a cause is less than 5%

Chronic spontaneous Urticaria is by far the most common subtype of all forms of non-acute Urticaria.1
The duration of CSU varies greatly from patient to patient, with some individuals suffering irritating symptoms such as pruritus far decades.2
2- A/fergol et lmmunopatho/2001; 29(4): 129-132
1- Allergy 2011; 66: 317–330.
Prevalence and Burden

1616
Frequency of angioedema in selected patients with chronic spontaneous urticaria
n, number of patients/subjects; NR, not reported.
*Authors examined patients with all types of urticaria.
†Authors do not distinguish between chronic spontaneous urticaria and other
forms of nonacute urticaria.
‡Authors examined the total population.
Maurer M, Weller K, Bindslev-Jensen C, Giménez-Arnau A, Bousquet PJ, et al. Unmet clinical needs in chronic spontaneous urticaria. A GA²LEN task force report. Allergy. 2011 Mar;66(3):317-30

In most cases, the duration of CSU is estimated to be 1–5 years1
However, for some patients the disease can last longer, sometimes more than 25 years1
Year 25
Years since diagnosis
Another 20% will resolve
(with or without treatment)
within 5 years of onset2
50% will resolve (with or
without treatment) within
6 months of onset2
Another 20% will resolve
(with or without treatment)
within 3 years of onset2
Another <2% will resolve
(with or without treatment)
within 25 years2
Duration of Chronic Urticaria
Year 1 Year 2 Year 3 Year 4 Year 5
1. Maurer M, et al. Allergy 2011;66:317–30;
2. Beltrani VS. Clin Rev Allergy Immunol 2002;23:147–69
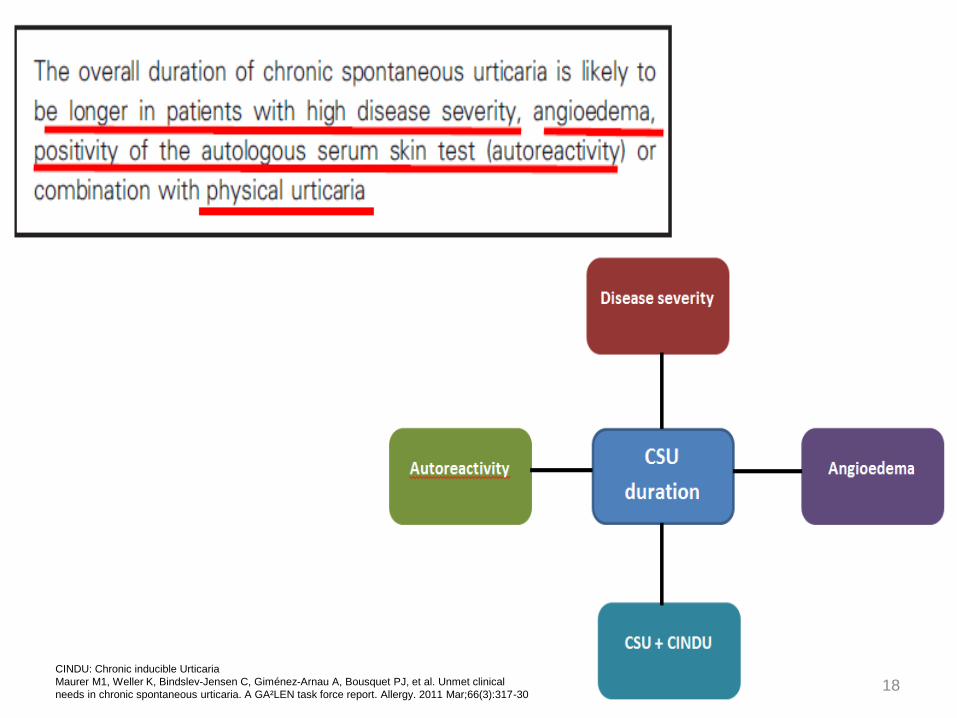
18CINDU: Chronic inducible Urticaria
Maurer M1, Weller K, Bindslev-Jensen C, Giménez-Arnau A, Bousquet PJ, et al. Unmet clinical
needs in chronic spontaneous urticaria. A GA²LEN task force report. Allergy. 2011 Mar;66(3):317-30
19
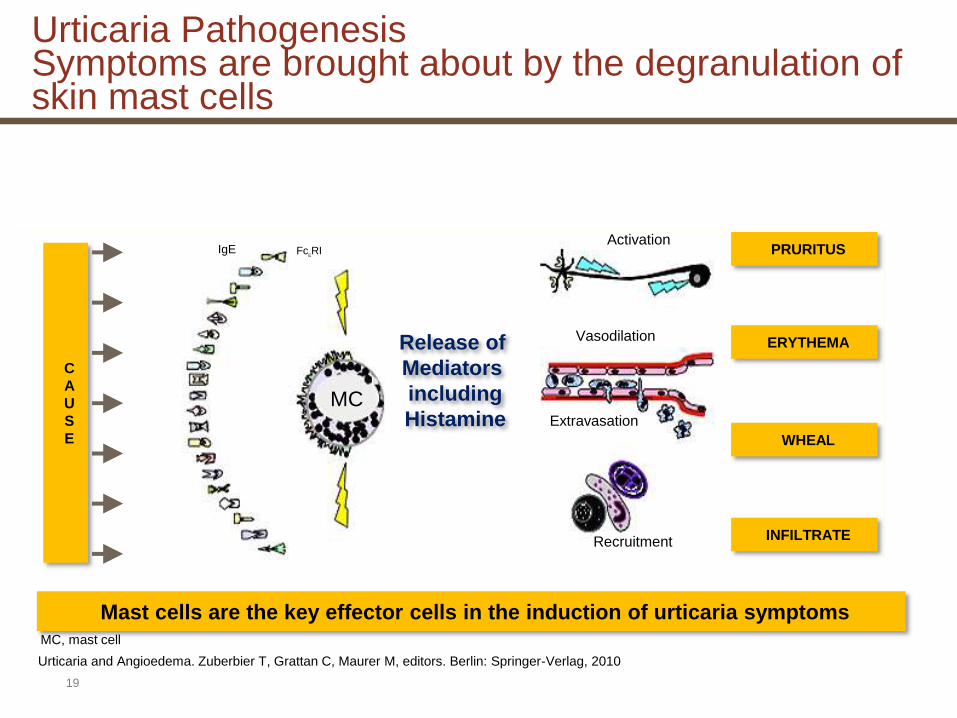
MC
Release of
Mediators
including
Histamine
PRURITUS
ERYTHEMA
WHEAL
INFILTRATE
Activation
Vasodilation
Extravasation
Recruitment
C
A
U
S
E
Mast cells are the key effector cells in the induction of urticaria symptoms
Urticaria and Angioedema. Zuberbier T, Grattan C, Maurer M, editors. Berlin: Springer-Verlag, 2010
MC, mast cell
Urticaria PathogenesisSymptoms are brought about by the degranulation of skin mast cells
IgE FceRI

1. Altrichter S, et al. PLoS One 2011;6:e14794;
2. Hide M, et al. N Engl J Med 1993;328:1599−604
Mast cells in some patients are activated by autoallergic or autoimmune mechanisms1
• histamine-releasing immunoglobulin G (IgG) autoantibodies against the high-affinity immunoglogulin E (IgE) receptor (FcεRI) or IgE itself are present in the circulation,2 and IgE autoantibodies may also be present1
Auto-allergy
allergen
1.Autoantigen/autoallergen
3. endogenous anti-IgE
antibody
Auto-immunity
2. anti-FcεRI
1.IgE against self
Allergy
MC
IgE
FcεRI
Pathophysiology of urticariaMast cell stimulation
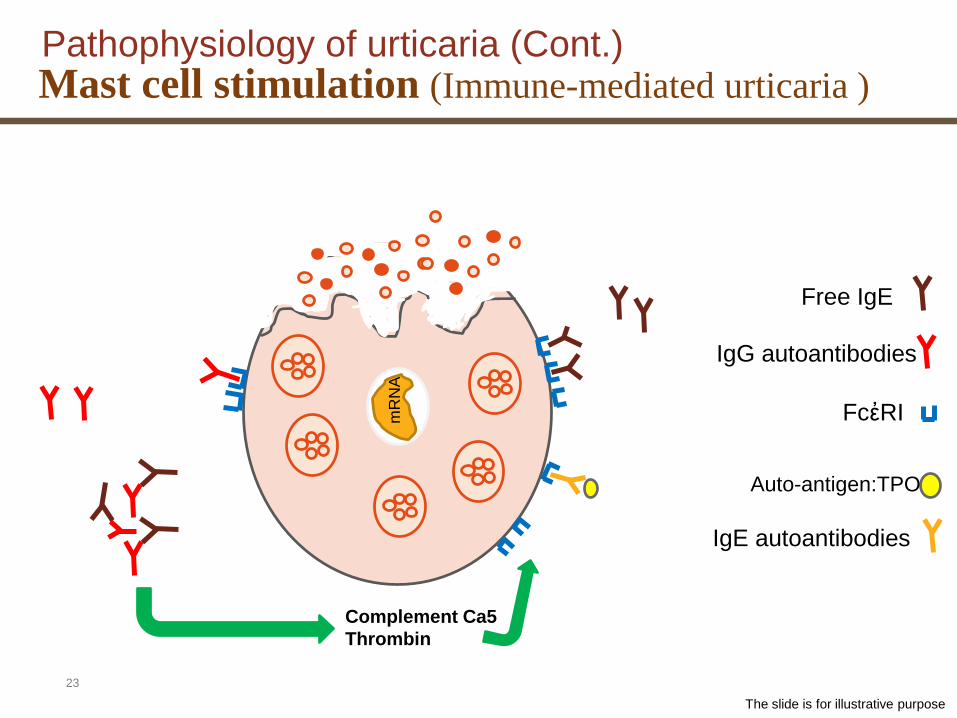
Several mechanisms of mast cell activation in CU have been identified:
• For example, IgG autoantibodies directed against IgE can cause cross-linking of mast cell– bound IgE and subsequent mast cell degranulation.
• Another subgroup of patients with CU exhibits IgG autoantibodies directed against the a-subunit of the high-affinity IgE receptor FceRI on mast cells.
• Recently identified, a subgroup of patients with CU who exhibit IgE autoantibodies against thyroperoxidase (TPO), and IgE antibodies against TPO (IgE– anti-TPO)–positive patients with CU exhibit significantly higher IgG–anti-TPO levels and lymphocyte counts, as well as decreased C4 complement levels
CU: Chronic urticaria
(J Allergy Clin Immunol 2011;128:202-9.)
Pathophysiology of urticaria (Cont.) Mast cell stimulation

22
Complement Ca5
Thrombin
FcἐRI
IgG autoantibodies
Auto-antigen:TPO
IgE autoantibodies
mR
NA
Free IgE
Pathophysiology of urticaria (Cont.) Mast cell stimulation
The slide is for illustrative purpose
23
Complement Ca5
Thrombin
FcἐRI
Free IgE
IgG autoantibodies
Auto-antigen:TPO
IgE autoantibodies
mR
NA
Pathophysiology of urticaria (Cont.) Mast cell stimulation (Immune-mediated urticaria )
The slide is for illustrative purpose

Maurer M1, Weller K, Bindslev-Jensen C, Giménez-Arnau A, Bousquet PJ, et al. Unmet clinical needs in chronic spontaneous urticaria. A GA²LEN task force report. Allergy. 2011 Mar;66(3):317-30 24
Diagnosis of urticaria
• It is important to remember that not all possible causative factors need to be investigated in all patients and the
first step in diagnosis is a thorough history:
25Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87

2626
1. Time of onset of disease
2. Frequency and duration of wheals
3. Diurnal variation
4. Occurrence in relation to weekends,
holidays, and foreign travel
5. Shape, size, and distribution of
wheals
6. Associated angioedema
7. Associated subjective symptoms of
lesion, e.g. itch, pain
8. Family and personal history
regarding urticaria, atopy
9. Previous or current allergies,
infections, internal diseases, or other
possible causes
10. Psychosomatic and psychiatric
diseases
11. Surgical implantations and events during
surgery.
12. Gastric/intestinal problems (stool, flatulence).
13. Induction by physical agents or exercise.
14. Use of drugs (NSAIDs, injections,
immunizations, hormones, laxatives,
suppositories, ear and eye drops, and alternative
remedies).
15. Observed correlation to food.
16. Relationship to the menstrual cycle.
17. Smoking habits.
18. Type of work.
19. Hobbies.
20. Stress (eustress and distress).
21. Quality of life related to urticaria and emotional
Impact.
22. Previous therapy and response to therapy.
The first step in diagnosis is a thorough historyQuestions should be asked regarding the following items:
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
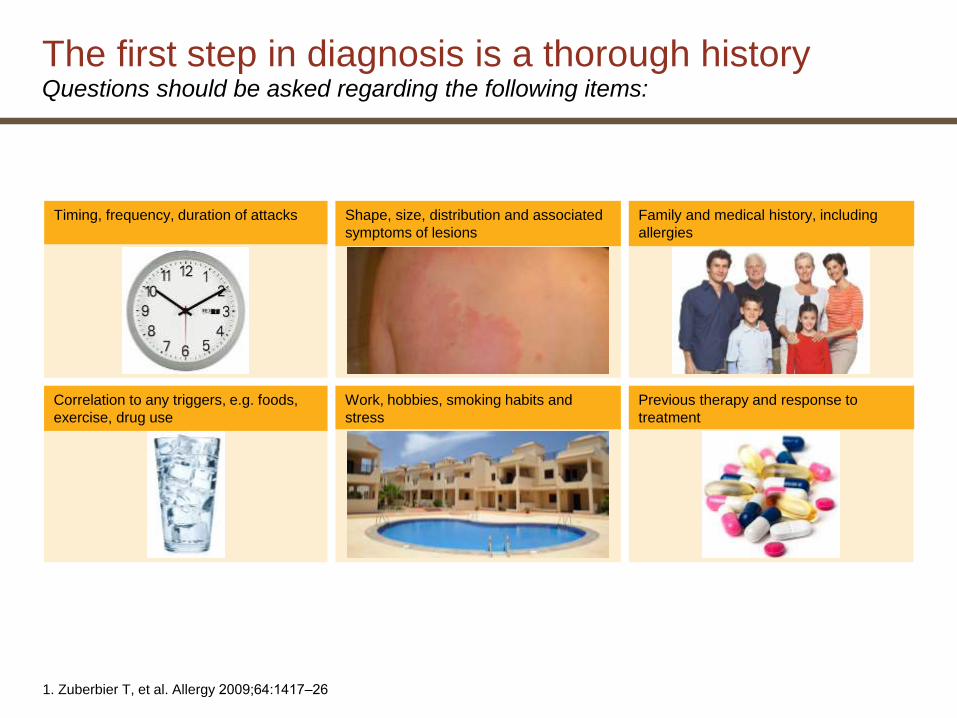
1. Zuberbier T, et al. Allergy 2009;64:1417‒26
Timing, frequency, duration of attacks Shape, size, distribution and associated
symptoms of lesions
Family and medical history, including
allergies
Correlation to any triggers, e.g. foods,
exercise, drug use
Work, hobbies, smoking habits and
stress
Previous therapy and response to
treatment
The first step in diagnosis is a thorough historyQuestions should be asked regarding the following items:

2828
The second step of the diagnosis is the physical examination of the patient.
This should include:
A diagnostic provocation test including drug, food, and physical tests where it is indicated by history.
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87

Physical examination
1. Zuberbier T, et al. Allergy 2009;64:1417‒26
Tests to identify triggers: these should be performed where indicated by history to
diagnose inducible urticaria subtypes1

3030
Routine diagnostic tests (recommended)
Extended diagnostic program* (suggested based
on history only)
Cold urticaria Cold provocation and threshold test
(ice cube, cold water, cold wind)
Differential blood count and ESR or CRP cryoproteins
rule out other diseases, especially infections
Delayed
pressure
urticaria
Pressure test and threshold test None
Heat urticaria Heat provocation and threshold test None
Solar urticaria UV and visible light of different
wavelengths
and threshold test
Rule out other light-induced dermatoses
Symptomatic
dermographism
Elicit dermographism and threshold
test (dermographometer)
Differential blood count, ESR or CRP
Vibratory
Angioedema
Test with, for example, vortex None
Aquagenic
urticaria
Wet cloths at body temperature
applied for 20 min
None
Cholinergic
urticaria
Exercise and hot bath provocation None
Contact
urticaria
Cutaneous provocation test. Skin
tests with immediate readings, for
example prick test
None
*Depending on suspected cause.
Zuberbier T, Aberer W, Asero R, et al. Allergy 2014;69:868–87
Recommended diagnostic tests for frequent urticaria subtypes
For Chronic inducible urticaria
3131
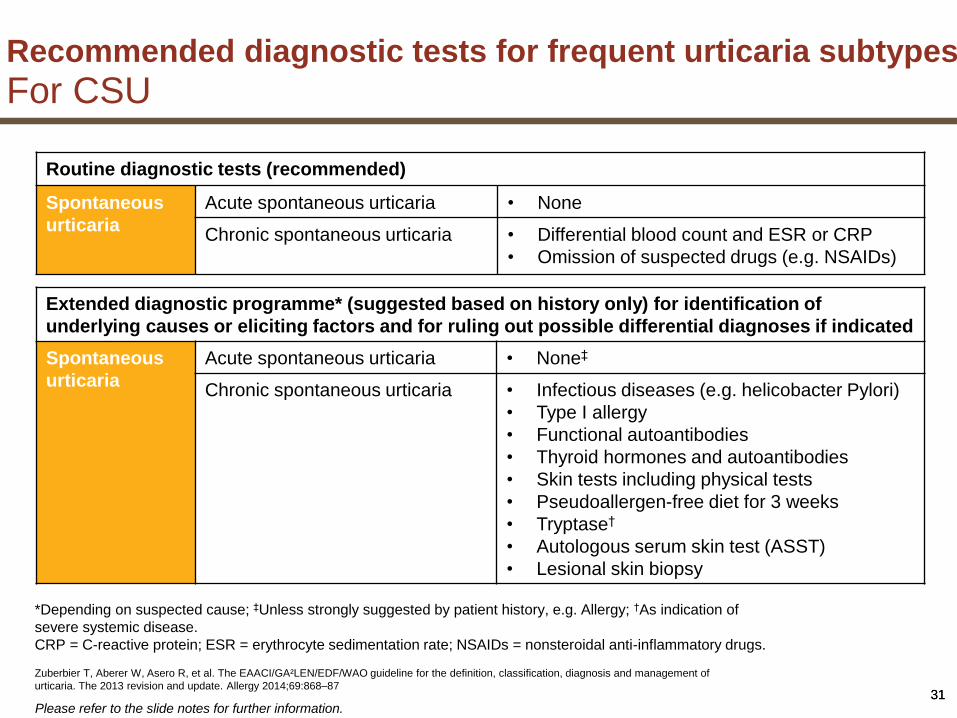
Recommended diagnostic tests for frequent urticaria subtypes
For CSU
Routine diagnostic tests (recommended)
Spontaneous
urticaria
Acute spontaneous urticaria • None
Chronic spontaneous urticaria • Differential blood count and ESR or CRP
• Omission of suspected drugs (e.g. NSAIDs)
Extended diagnostic programme* (suggested based on history only) for identification of
underlying causes or eliciting factors and for ruling out possible differential diagnoses if indicated
Spontaneous
urticaria
Acute spontaneous urticaria • None‡
Chronic spontaneous urticaria • Infectious diseases (e.g. helicobacter Pylori)
• Type I allergy
• Functional autoantibodies
• Thyroid hormones and autoantibodies
• Skin tests including physical tests
• Pseudoallergen-free diet for 3 weeks
• Tryptase†
• Autologous serum skin test (ASST)
• Lesional skin biopsy
*Depending on suspected cause; ‡Unless strongly suggested by patient history, e.g. Allergy; †As indication of
severe systemic disease.
CRP = C-reactive protein; ESR = erythrocyte sedimentation rate; NSAIDs = nonsteroidal anti-inflammatory drugs.
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of
urticaria. The 2013 revision and update. Allergy 2014;69:868–87
Please refer to the slide notes for further information.
3232
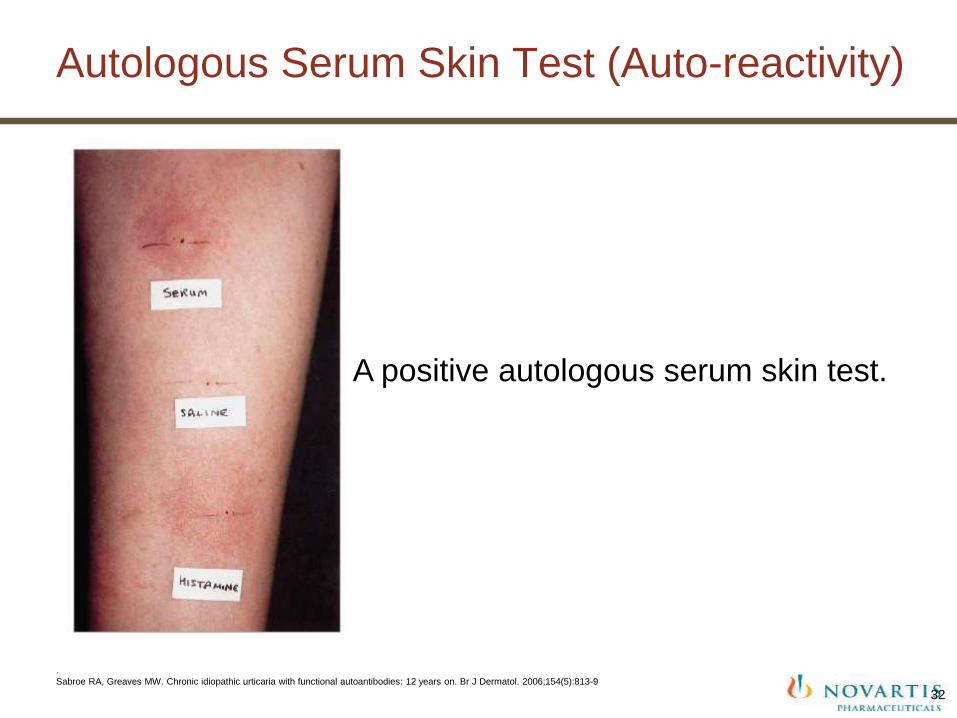
Autologous Serum Skin Test (Auto-reactivity)
A positive autologous serum skin test.
.
Sabroe RA, Greaves MW. Chronic idiopathic urticaria with functional autoantibodies: 12 years on. Br J Dermatol. 2006;154(5):813-9

ASST positivity and disease activity/severity
Approximately one third of CSU patients show a positive response against their own serum in the autologous serum skin test (ASST)1
• autoantibodies against the high-affinity IgE receptor or against IgE itself can be detected in some of these patients1
• patients with autoimmune CSU appear to have more severe disease2
- more severe clinical features have been reported, including more wheals, larger wheal size, higher itch scores3– 5
- longer duration of disease5–7
- higher requirement for antihistamine medication7
1. Maurer, M et al. Allergy 2011;66:317–30; 2. Kozel MMA, Sabroe RA. Drugs 2004;64:2515–36; 3. Sabroe RA, et al. J Am Acad Dermatol 1999;40:443–50; 4. Caproni M, et al. Acta Derm Venereol 2004;84:288–90; 5. Alyasin S, et al. South Med J 2011;104:111–5; 6. Konstantinou GN, et al. Allergy 2009;64:1256–68; 7. Staubach P, et al. Dermatology 2006;212:150–9

• Should routine diagnostic measures be performed in acute urticaria?
• We recommend against any routine diagnostic measures in acute urticaria (strong recommendation/clinical consensus).
34Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
• Should routine diagnostic measures be performed in chronic spontaneous urticaria?
• We recommend for only very limited routine diagnostic measures in chronic spontaneous urticaria (strong recommendation/ clinical consensus).
35Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87

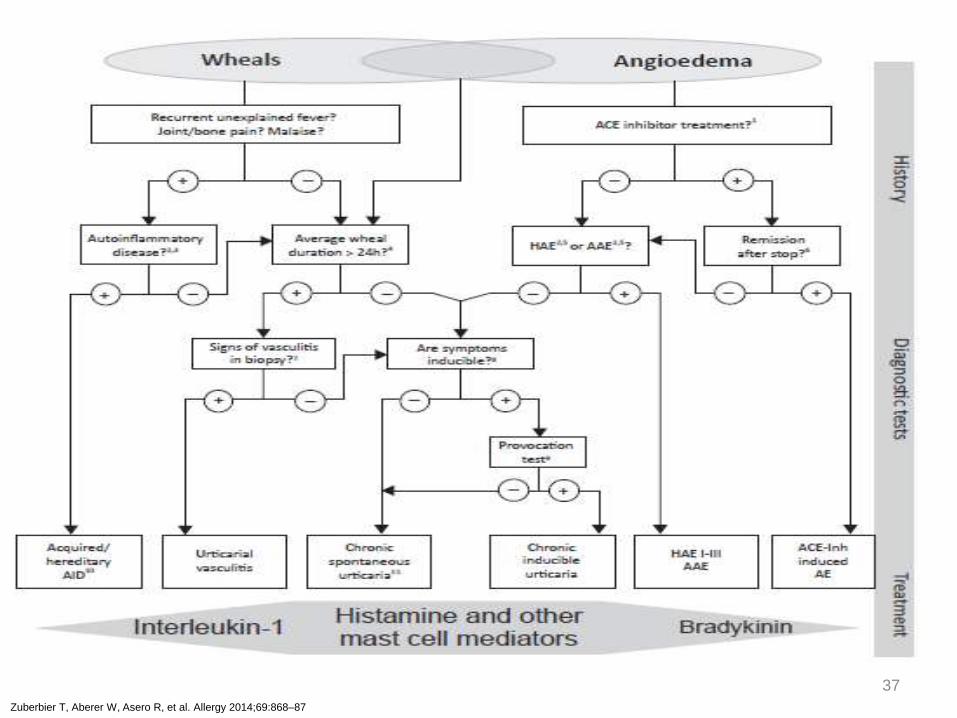
Diagnostic algorithm for patients presenting with wheals,
angioedema, orboth
36
37
Zuberbier T, Aberer W, Asero R, et al. Allergy 2014;69:868–87

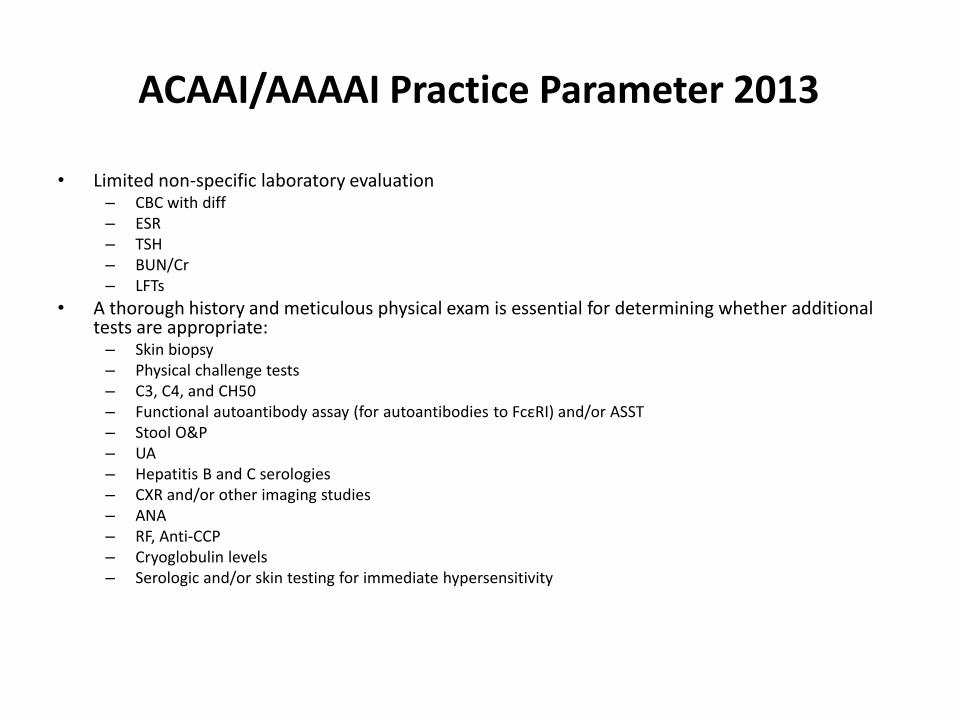
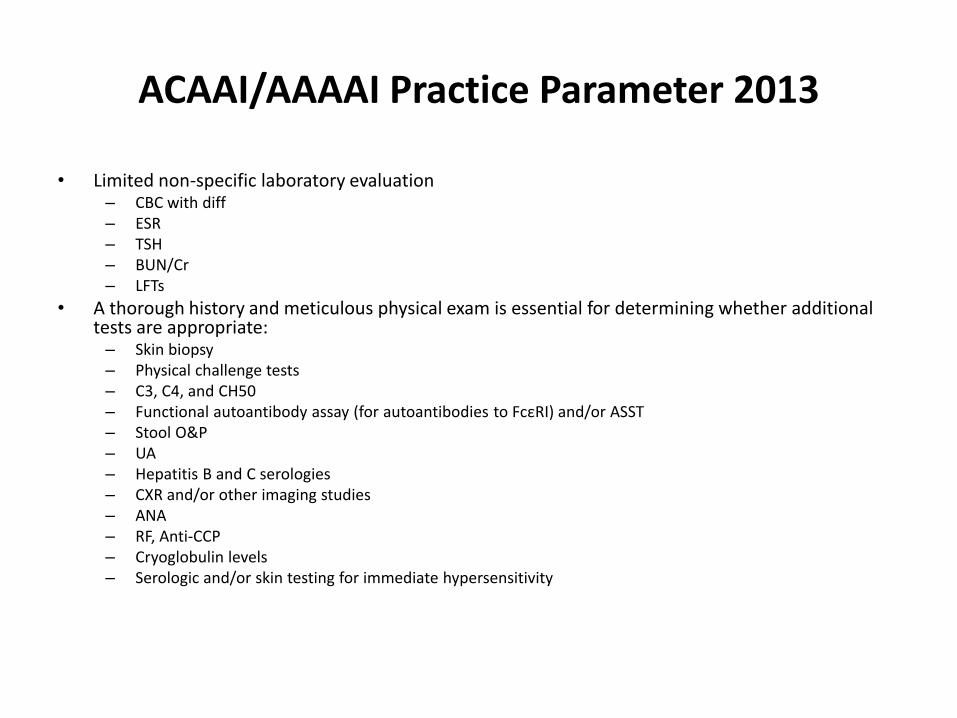
ACAAI/AAAAI Practice Parameter 2013
• Limited non-specific laboratory evaluation– CBC with diff– ESR– TSH– BUN/Cr– LFTs
• A thorough history and meticulous physical exam is essential for determining whether additional tests are appropriate:
– Skin biopsy– Physical challenge tests– C3, C4, and CH50– Functional autoantibody assay (for autoantibodies to FcεRI) and/or ASST– Stool O&P– UA– Hepatitis B and C serologies– CXR and/or other imaging studies– ANA– RF, Anti-CCP– Cryoglobulin levels– Serologic and/or skin testing for immediate hypersensitivity

WAO Guideline 2012
• History/physical examTime of onset– Frequency and duration of wheals– Presence of diurnal variation– Shape, size, and distribution of wheals– Associated angioedema– Family and personal history of urticaria– Atopy– Medications (NSAIDs, hormones, laxatives, immunizations)– Observed correlation with food and stress
• Diagnostic studiesCBC/diff– LFTs– ESR, CRP– Screening for thyroid autoimmunity "may be considered" (Anti-Tg, Anti-TPO)– Physical urticaria testing– Role of H. pylori is controversial, and the evidence is weak– Skin biopsy may be needed to confirm urticarial vasculitis or Schnitzler syndrome

Kaplan
• CBC/diff - high eosinophil counts might trigger a stool examination for ova and parasites
• CRP or ESR• TSH/FT4, anti-TPO, anti-TG antibodies - may be useful because so many CU
patients are found to be hypothyroid and are then treated with a thyroid hormone• Other tests
– Routine food allergy skin testing - not recommended– ANA - not recommended in the absence of symptoms (other than urticaria) that might suggest
the presence of SLE– Anti-IgE/anti-IgE receptor antibodies - of theoretical interest, but none of the treatment
modalities distinguish patients with the antibodies from those without them– Skin biopsy - when the diagnosis is not clear or when a vasculitis is suspected or at least needs
to be ruled out• Examples of circumstances where a skin biopsy should be performed would be the presence of fever,
concomitant petechiae or palpable purpura, lesions that fade with bruising, individual lesions lasting >24 h (and certainly >36 h), or prominent arthralgia
• ANA, C3, C4, and C1q binding assay for circulating immune complexes and cryoglobulin determination would be included
•

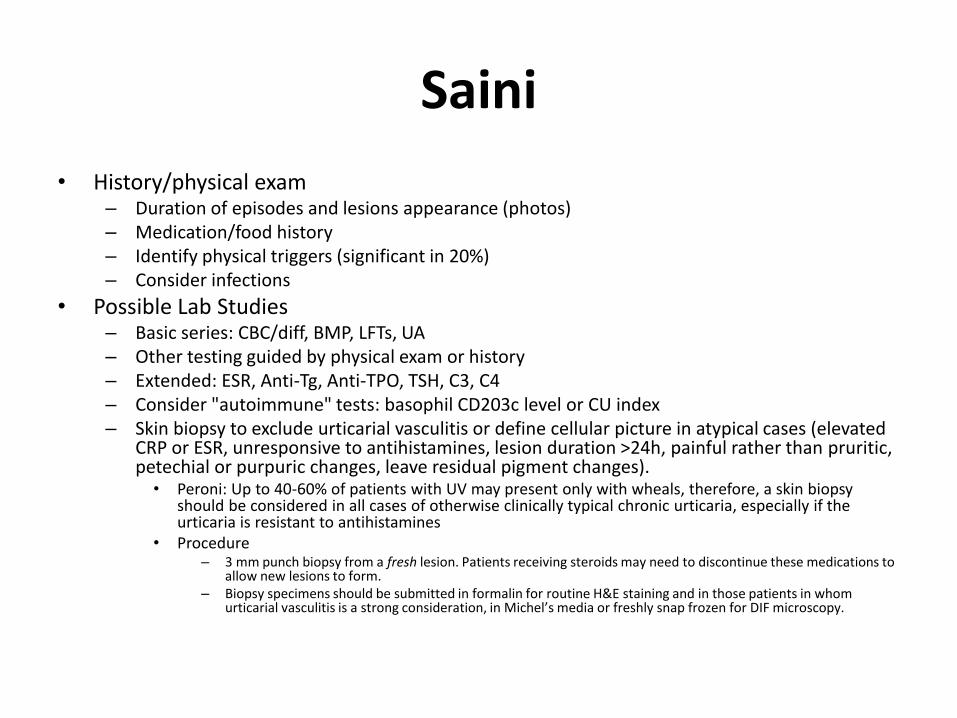
Saini
• History/physical exam– Duration of episodes and lesions appearance (photos)– Medication/food history– Identify physical triggers (significant in 20%)– Consider infections
• Possible Lab Studies– Basic series: CBC/diff, BMP, LFTs, UA– Other testing guided by physical exam or history– Extended: ESR, Anti-Tg, Anti-TPO, TSH, C3, C4– Consider "autoimmune" tests: basophil CD203c level or CU index– Skin biopsy to exclude urticarial vasculitis or define cellular picture in atypical cases (elevated
CRP or ESR, unresponsive to antihistamines, lesion duration >24h, painful rather than pruritic, petechial or purpuric changes, leave residual pigment changes).
• Peroni: Up to 40-60% of patients with UV may present only with wheals, therefore, a skin biopsy should be considered in all cases of otherwise clinically typical chronic urticaria, especially if the urticaria is resistant to antihistamines
• Procedure– 3 mm punch biopsy from a fresh lesion. Patients receiving steroids may need to discontinue these medications to
allow new lesions to form.– Biopsy specimens should be submitted in formalin for routine H&E staining and in those patients in whom
urticarial vasculitis is a strong consideration, in Michel’s media or freshly snap frozen for DIF microscopy.

Bernstein
• History/physical exam• Evaluate for evidence of physical urticarias, dermatographism• Initial testing
– CBC/diff– ESR– TSH– LFTs– UA– Allergy skin testing is not indicated in the initial evaluation of urticaria
• Testing for refractory cases– C4– Anti-Tg, Anti-TPO– H. pylori antibodies– Hepatitis panel– Consider autologous serum skin test– Consider skin biopsy if urticaria are atypical, not evanescent
Dreyfus
• Initial testing– TSH, Anti-Tg– CBC/diff– SPEP– LFTs– Hepatitis titers– H. pylori IgG, IgM and titers for other infectious illness - if suggested by history– ANA and anti-DNA anti-bodies - if history or exam suggestive of vasculitis– C1INH level and function, C2, C4 - if angioedema present– Chromagranin A or urine catecholamines - if significant flushing, carcinoid features– Tryptase - if significant component of anaphylaxis with urticaria, angioedema– CXR and PFT - if associated respiratory symptoms such as cough, wheezing– Total immunoglobulin levels, B/T cell subsets - if history suggestive of parasitic infection,
chronic infection– Pregnancy testing - if relevant age and sex– Serum basophil activation or histamine release in vitro and/or autologous skin testing - not
required but may be useful to confirm diagnosis

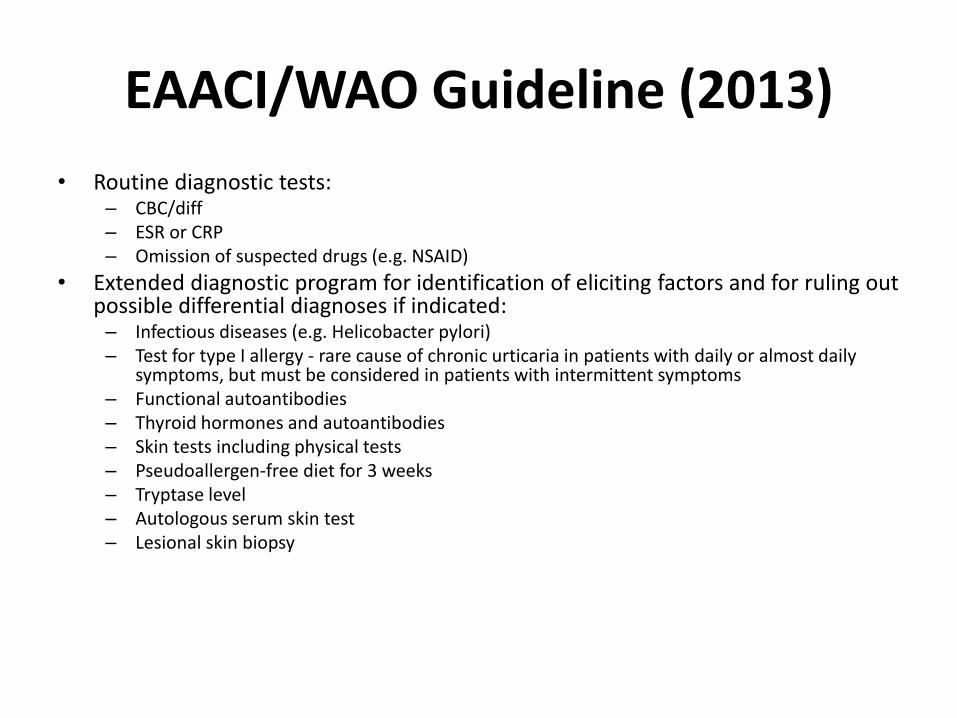
EAACI/WAO Guideline (2013)
• Routine diagnostic tests:– CBC/diff– ESR or CRP– Omission of suspected drugs (e.g. NSAID)
• Extended diagnostic program for identification of eliciting factors and for ruling out possible differential diagnoses if indicated:
– Infectious diseases (e.g. Helicobacter pylori)– Test for type I allergy - rare cause of chronic urticaria in patients with daily or almost daily
symptoms, but must be considered in patients with intermittent symptoms– Functional autoantibodies– Thyroid hormones and autoantibodies– Skin tests including physical tests– Pseudoallergen-free diet for 3 weeks– Tryptase level– Autologous serum skin test– Lesional skin biopsy
Diagnostic Approach for Children (Boguniewicz)
• Routine testing– Allergy testing– CBC/diff– ESR– LFTs– TSH, FT4, anti-Tg, anti-TPO
• Extended testing for selected patients– Hepatitis serology– Complement levels– ANA and specific autoimmune testing– EBV testing– Stool ova and parasites– Skin biopsy if vasculitis or mastocytosis are suspected
• Children whose CU persists should have yearly re-evaluation to rule-out late onset autoimmune disease
•

Specialized Lab Testing for Urticaria
• CU Index - patient's serum is added to healthy donor basophils and quantity of histamine release is measured. The reference range for a healthy non-CU population is <10. Values ≥10 indicate that basophils were stimulated by patient serum to release histamine (the larger the value the more histamine released).
– In one study, 23% of healthy controls vs. 57% of CU patients had a positive CU index– Positive CU Index associated with more severe CIU
• Anti-FcεR1 (high affinity IgE receptor) IgG antibody- by Western blot, direct measurement of IgEreceptor autoantibodies
– These antibodies may not correlate with disease activity and have been identified in other autoimmune diseases (even in the absence of urticaria), including pemphigus vulgaris, SLE, dermatomyositis, and pemphigoid, suggesting that these antibodies may represent an epiphenomenon.
• Anti-IgE IgG antibody• Basophil CD203c levels - by flow cytometry, indirect measure of autoantibodies to IgE receptor
which result in basophil activation.• Anti-C1q antibody - Patients with hypocoplementemic urticarial vasculitis syndrome (HUVS) usually
have autoantibodies reactive with the collagen-like region of the C1q molecule, and can develop angioedema.
•
Additional Testing Notes
• D-dimer - elevated D-dimer may be a biomarker of antihistamine-resistant chronic urticaria (Asero)
– This subtype may respond to anticoagulation with tranexamic acid and low molecular weight heparin
• Wedi - careful search for at least infections with H. pylori, strep, and perhaps also staph and yersinia should be included in the work-up of severely affected patients; our routine work-up includes:
– Helicobacter pylori monoclonal stool antigen test– Serology for strep (ASO, anti-DNase B), staph (antistaphylolysin), yersinia (IgA, IgG,
immunoblot). If an infection is identified, it should be appropriately treated and it should be checked whether eradication has been achieved.
• Initial evaluation for autoinflammatory syndromes (e.g. CAPS) should include:– CBC/diff - to screen for neutrophilia– CRP, ESR– ANA - help rule out autoimmune disease– UA - screen for proteinuria which suggests renal amyloidosis– Serum amyloid A level - inflammation marker and screening parameter for amyloidosis– Gene mutation analysis if specific diagnosis suspected (e.g. CAPS)
49
Urticaria Burden

Impact of chronic spontaneous urticaria on the patients
In addition to the classical clinical symptoms like pruritus, whealing and the occurrence of angioedema, many other factors are of major importance for patients with chronic spontaneous urticaria these include:
1. The unpredictability of the attacks.
2. Lack of quality sleep (due to pruritus).
3. Fatigue caused by treatment.
4. Side-effects.
5. Cosmetic disfigurement.
Quality of life
Allergy 2011; 66: 317–330.50
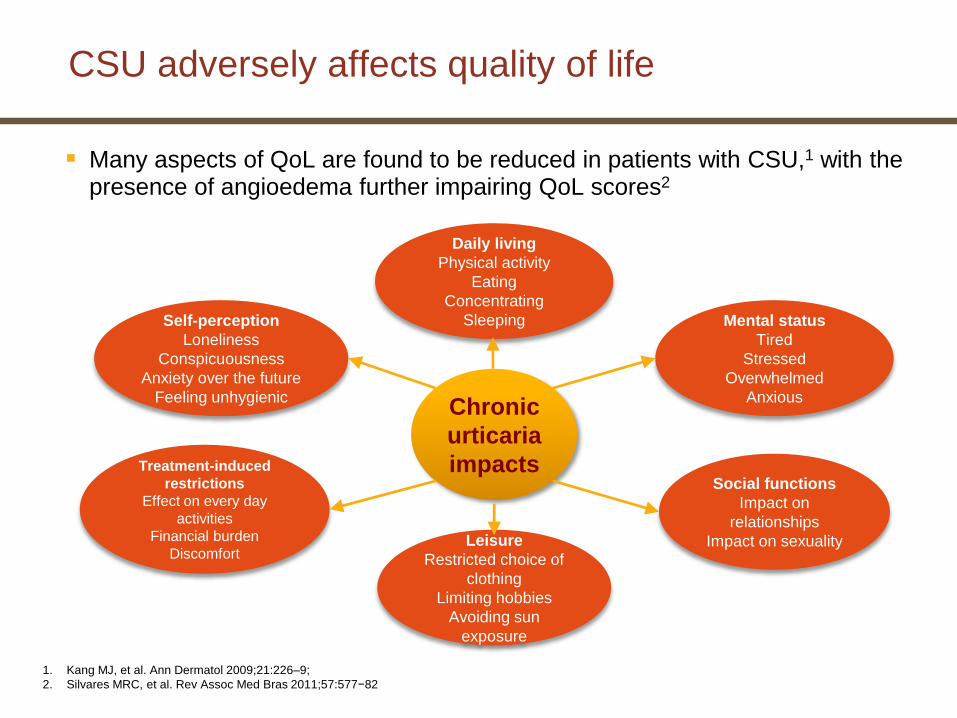
CSU adversely affects quality of life
Many aspects of QoL are found to be reduced in patients with CSU,1 with the presence of angioedema further impairing QoL scores2
Mental status
Tired
Stressed
Overwhelmed
Anxious
Daily living
Physical activity
Eating
Concentrating
Sleeping
Leisure
Restricted choice of
clothing
Limiting hobbies
Avoiding sun
exposure
Self-perception
Loneliness
Conspicuousness
Anxiety over the future
Feeling unhygienic
Treatment-induced
restrictions
Effect on every day
activities
Financial burden
Discomfort
Social functions
Impact on
relationships
Impact on sexuality
Chronic
urticaria
impacts
1. Kang MJ, et al. Ann Dermatol 2009;21:226–9;
2. Silvares MRC, et al. Rev Assoc Med Bras 2011;57:577−82
Maurer M1, Weller K, Bindslev-Jensen C, Giménez-Arnau A, Bousquet PJ, et al. Unmet clinical needs in chronic spontaneous urticaria. A GA²LEN task force report. Allergy. 2011 Mar;66(3):317-30 53

5454
Patients with CU feel similarly lacking in energy, socially isolated, and emotionally upset as the patients with heart disease
Comparison of the NHP (part I) scores in patients with chronic urticaria (CU, n 5 134)
and in patients with ischemic heart disease (IHD, n 5 98) awaiting coronary artery bypass
grafting. (From O’Donnell BF, Lawlor F, Simpson J, et al. The impact of chronic urticaria on
the quality of life. Br J Dermatol 1997;136(2):200;
O’Donnell BF. Urticaria: Impact on Quality of Life and Economic Cost. Immunol Allergy Clin N Am 2014; 34: 89–104

Socioeconomic burden
The socioeconomic cost of Chronic urticaria is high in terms of direct medical costs and indirect costs, such as lost wages because of absences from work
0
50
100
150
200
250
300
Direct costs/patient/year ($US)
Laboratory
Outpatient visits
ED/hospital visits
Medication
Direct costs include laboratory costs, outpatient visits, emergency department (ED)/hospital visits, and
medication
Indirect costs include income lost because of travel to outpatient visits and work absenteeism
0
50
100
150
200
250
300
Indirect costs/patient/year in lost wages ($US)
Travel tooutpatient visit
Absence fromwork
Based on a CSU prevalence of 0.04% among the US population, estimated mean total
indirect and direct costs would be $244 million per year
DeLong LK, et al. Arch Dermatol 2008;144:35−9
$U
S
$U
S

How to assess disease activity and quality of life?
56
Disease activity
Quality of life
UAS AAS
CU-Q2ol AE-Qol
Wheal Angioedema

5757
Disease activity in spontaneous urticaria should be assessed using the UAS7
The UAS7 is a validated method for assessing disease activity
A modification to the UAS7, in which signs and symptoms are assessed two times per day, has also been validated
Score Wheals Pruritus
0 None None
1 Mild (<20 wheals/24 hours) Mild (present, but not annoying or troublesome)
2 Moderate (20–50 wheals/24 hours) Moderate (troublesome, but does not interfere with
normal daily activity or sleep)
3 Intense (>50 wheals/24 hours or
large confluent areas of wheals)
Intense (severe pruritus, which is sufficiently
troublesome to interfere with normal daily activity or
sleep)
Sum of score: 0–6 for each day is summarized over one week (maximum 42)
Urticaria activity score
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of
urticaria. The 2013 revision and update. Allergy 2014;69:868–87

Treatment of Urticaria

63
Goal of treatment
Should treatment aim at complete symptom control in urticaria?
We recommend aiming for complete symptom control in urticaria as safely as possible (strong recommendation/clinical consensus following the WHO constitution in conformity with the Charter of the United Nations).
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and management
of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
6464
Chronic urticaria is a mast cell-dependent disease and should be managed accordingly
In CU, partly unknown stimuli cause mast cells to release their mediators leading to small (wheals) or larger and deeper (angioedema) edema of the skin
The therapeutic approach is universal and based on the same principles as in other mast-cell dependent diseases:1,2
1. Elimination/avoidance of the cause or trigger/stimulus
2. Symptomatic pharmacological treatment by reducing mast cell mediator release and/or the effect of these mediators at the target organ
3. Inducing tolerance
Management algorithms for CU should take account of:2
• Variation in symptoms from one patient to another
• Need to step up or step down treatment
• Differences between easy-to-treat and refractory patients
CU = chronic urticaria.
1. Zuberbier T, et al. EAACI/GA2LEN/EDF/WAO guideline: management of urticaria. Allergy 2009;64:1427–1443
2. Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
6565
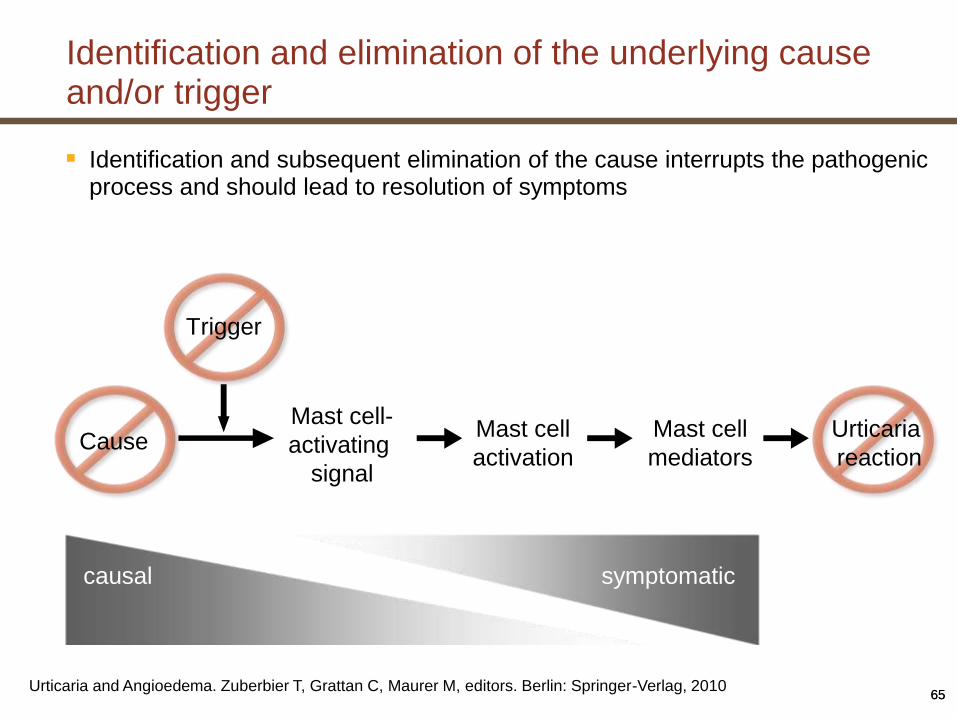
Identification and elimination of the underlying cause and/or trigger
Identification and subsequent elimination of the cause interrupts the pathogenic process and should lead to resolution of symptoms
Urticaria and Angioedema. Zuberbier T, Grattan C, Maurer M, editors. Berlin: Springer-Verlag, 2010
Trigger
CauseMast cell-
activating
signal
Mast cell
activation
Mast cell
mediators
Urticaria
reaction
causal symptomatic

Elimination or avoidance of the cause or trigger/stimulus requires an exact diagnosis
Drugs
When such agents are suspected in the course of diagnosis, they should be omitted entirely or substituted by another class of agents if indispensable
Drugs causing non-allergic hypersensitivity reactions (e.g. NSAIDs) cannot only elicit, but can also aggravate pre-existing CSU, so that elimination in the latter case will only improve symptoms in some patients
Physical stimuli
Avoidance is desirable but not always simple
Eradication of infections and treatment of inflammatory processes
CSU is often associated with inflammatory or infectious diseases
Infections should be treated appropriately, but it is unclear whether they have significant causative role
Reduction of functional autoantibodies
There is little experience in the reduction of functional autoantibodies with plasmaphoresis in CSU
Such treatment should be reserved for patients unresponsive to all other forms of treatment
Dietary management
IgE-mediated food allergy is rarely the underlying cause of CSU
Pseudoallergic reactions to foods have been seen in some patients with CSU
In such cases, diet low in pseudoallergens should be implemented for ≥3–6 months
CU = chronic urticaria; CSU = chronic spontaneous urticaria; NSAID = non-steroidal anti-inflammatory drug.
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
Induction of tolerance may be useful in some urticaria subtypes
Inducing tolerance may be effective in cold, cholinergic and solar urticaria
Tolerance only lasts for a few days, so consistent daily exposure is required
• This may not be tolerated by patients (e.g. in the case of cold baths for cold urticaria)
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of
urticaria. The 2013 revision and update. Allergy 2014;69:868–87
6868
Trigger
CauseMast cell-
activating
signal
Mast cell
activation
Mast cell
mediators
Urticaria
reaction
symptomatic
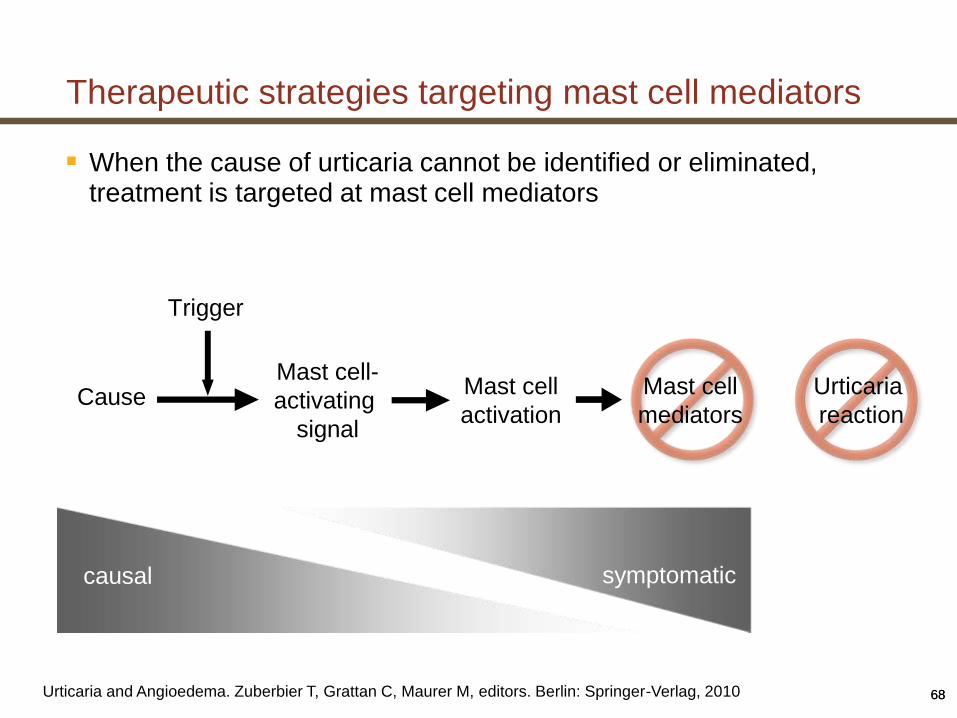
Therapeutic strategies targeting mast cell mediators
When the cause of urticaria cannot be identified or eliminated, treatment is targeted at mast cell mediators
Urticaria and Angioedema. Zuberbier T, Grattan C, Maurer M, editors. Berlin: Springer-Verlag, 2010
causal

Guidelines Recommendations Toward Urticaria Management
*The order of third-line treatments does not reflect preference.
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification,
diagnosis and management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
First line:
Modern second-generation antihistamines
Second line:
Increase dosage up to fourfold of modern second-generation antihistamines
Third line:
Add on to second-line*: omalizumab or ciclosporin A or montelukast
Short course (maximum 10 days) of corticosteroids may also be used at all times if
exacerbations demand this
If symptoms persist after 2 weeks
If symptoms persist after 1–4 further weeks
69

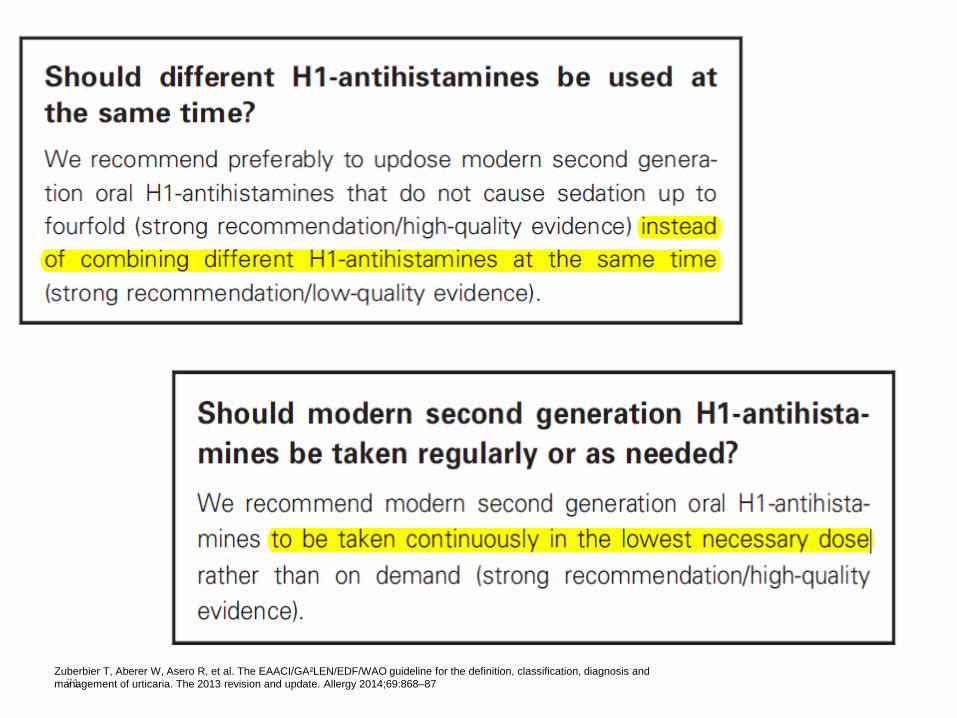
Continuous treatment with H1-antihistamines is central to the management of CU
Many symptoms of urticaria are mediated primarily by histamine
• Histamine H1 receptors are located on endothelial cells and sensory nerves
• H1-antihistamines stabilize these receptors in an inactive state
In some cases, other mast cell mediators (PAF, leukotrienes, cytokines) are also involved and a pronounced cellular infiltrate including basophils, lymphocytes and eosinophils may be observed
• Such cases may respond to a brief course of corticosteroids and may be relatively refractory to H1-antihistamines
Use of first-generation (sedating) antihistamines is not recommended for routine management of urticaria
Modern second-generation H1-antihistamines should be considered as the first-line treatment for urticaria
• Up-dosing (up to 4× licensed dose) is the second-line option
PAF = platelet activating factor.
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
71Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87

72
Up to 50% of CSU patients have an inadequate response to H1-antihistamines at licensed doses.1,2
1. Maurer M, et al. Allergy 2011;66:317–30.
2. Weller K, et al. J Eur Acad Dermatol venereol 2013;27:43-50
How do you help your H1-antihistamines refractory patients?

Ciclosporin A has a moderate, direct effect on mast cell mediator release
• Shown to be effective in double-blind placebo-controlled studies
• Efficacy in combination with modern second generation H1-antihistamines has been shown in placebo-controlled trials and open controlled trials
• Not recommended as standard treatment due to high incidence of adverse effects
• Recommended only use in severe disease refractory to any dose of antihistamine
Information on ciclosporin A and corticosteroids is similar to that in the 2009 guidelines;
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
Treatment of antihistamine-refractory patients:
Ciclosporin A
LTRAs are associated with a low level of evidence for efficacy in urticaria
• The best evidence is for montelukast
In urticaria, topical corticosteroids are not helpful (with the possible exception of pressure urticaria on the soles of the feet [low evidence])
• If systemic corticosteroids are used, doses between 20–50 mg/day are required
• Adverse effects occur during on long-term use
• There is a strong recommendation against long-term use of corticosteroids outside specialist clinics
• In many countries, corticosteroids are not licenced for use in urticaria
Description of LTRAs has been changed since 2009 and now notes that the best evidence is for montelukast.
LTRA = leukotriene receptor antagonist.
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
Treatment of antihistamine-refractory patients:
LTRAs and corticosteroids

Omalizumab (anti-IgE) has now been shown to be very effective in the treatment for CSU, both in case reports and case series as well as in double-blind placebo-controlled studies in antihistamine refractory selected patients.
75
Treatment of antihistamine-refractory patients:Omalizumab
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
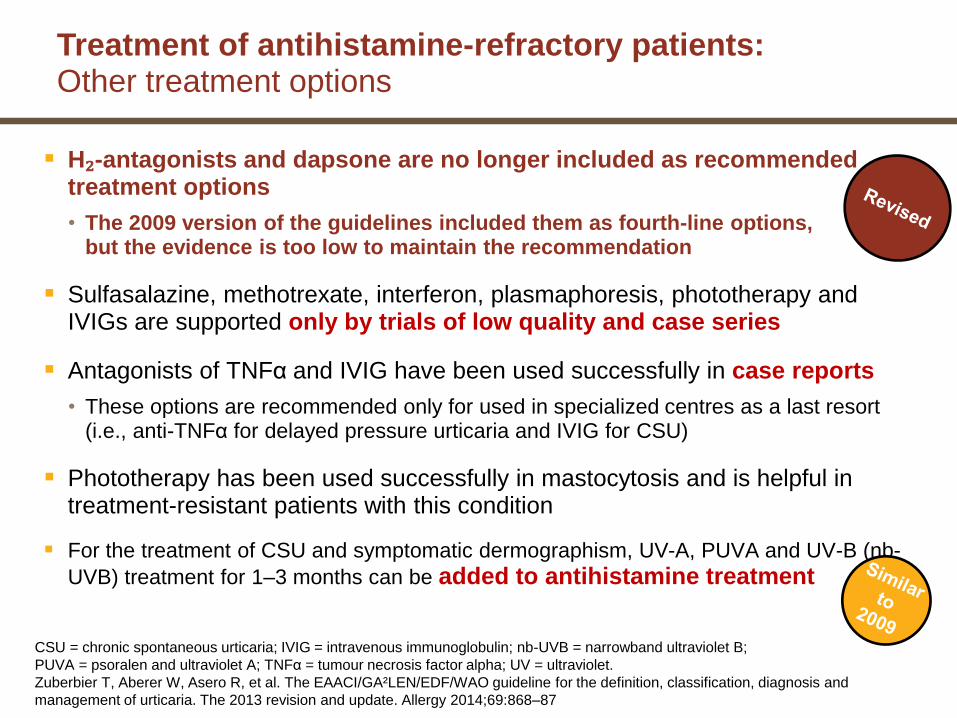
Treatment of antihistamine-refractory patients:Other treatment options
H₂-antagonists and dapsone are no longer included as recommended treatment options
• The 2009 version of the guidelines included them as fourth-line options, but the evidence is too low to maintain the recommendation
Sulfasalazine, methotrexate, interferon, plasmaphoresis, phototherapy and IVIGs are supported only by trials of low quality and case series
Antagonists of TNFα and IVIG have been used successfully in case reports
• These options are recommended only for used in specialized centres as a last resort (i.e., anti-TNFα for delayed pressure urticaria and IVIG for CSU)
Phototherapy has been used successfully in mastocytosis and is helpful in treatment-resistant patients with this condition
For the treatment of CSU and symptomatic dermographism, UV-A, PUVA and UV-B (nb-
UVB) treatment for 1–3 months can be added to antihistamine treatment
CSU = chronic spontaneous urticaria; IVIG = intravenous immunoglobulin; nb-UVB = narrowband ultraviolet B;
PUVA = psoralen and ultraviolet A; TNFα = tumour necrosis factor alpha; UV = ultraviolet.
Zuberbier T, Aberer W, Asero R, et al. The EAACI/GA²LEN/EDF/WAO guideline for the definition, classification, diagnosis and
management of urticaria. The 2013 revision and update. Allergy 2014;69:868–87
Maurer.M, Magerl M, Metz M, Zuberbier.T, et al.Revisions to the international guidelines on the diagnosis and therapy of chronic urticaria. Journal of German Society of
Dermatology. 2013. DOI: 10.1111/ddg.12194

78
79
Thank You

80
Diagnostic Approach

ACAAI/AAAAI Practice Parameter 2013
• Limited non-specific laboratory evaluation– CBC with diff– ESR– TSH– BUN/Cr– LFTs
• A thorough history and meticulous physical exam is essential for determining whether additional tests are appropriate:
– Skin biopsy– Physical challenge tests– C3, C4, and CH50– Functional autoantibody assay (for autoantibodies to FcεRI) and/or ASST– Stool O&P– UA– Hepatitis B and C serologies– CXR and/or other imaging studies– ANA– RF, Anti-CCP– Cryoglobulin levels– Serologic and/or skin testing for immediate hypersensitivity

WAO Guideline 2012
• History/physical examTime of onset– Frequency and duration of wheals– Presence of diurnal variation– Shape, size, and distribution of wheals– Associated angioedema– Family and personal history of urticaria– Atopy– Medications (NSAIDs, hormones, laxatives, immunizations)– Observed correlation with food and stress
• Diagnostic studiesCBC/diff– LFTs– ESR, CRP– Screening for thyroid autoimmunity "may be considered" (Anti-Tg, Anti-TPO)– Physical urticaria testing– Role of H. pylori is controversial, and the evidence is weak– Skin biopsy may be needed to confirm urticarial vasculitis or Schnitzler syndrome

Kaplan
• CBC/diff - high eosinophil counts might trigger a stool examination for ova and parasites
• CRP or ESR• TSH/FT4, anti-TPO, anti-TG antibodies - may be useful because so many CU
patients are found to be hypothyroid and are then treated with a thyroid hormone• Other tests
– Routine food allergy skin testing - not recommended– ANA - not recommended in the absence of symptoms (other than urticaria) that might suggest
the presence of SLE– Anti-IgE/anti-IgE receptor antibodies - of theoretical interest, but none of the treatment
modalities distinguish patients with the antibodies from those without them– Skin biopsy - when the diagnosis is not clear or when a vasculitis is suspected or at least needs
to be ruled out• Examples of circumstances where a skin biopsy should be performed would be the presence of fever,
concomitant petechiae or palpable purpura, lesions that fade with bruising, individual lesions lasting >24 h (and certainly >36 h), or prominent arthralgia
• ANA, C3, C4, and C1q binding assay for circulating immune complexes and cryoglobulin determination would be included
•
Saini
• History/physical exam– Duration of episodes and lesions appearance (photos)– Medication/food history– Identify physical triggers (significant in 20%)– Consider infections
• Possible Lab Studies– Basic series: CBC/diff, BMP, LFTs, UA– Other testing guided by physical exam or history– Extended: ESR, Anti-Tg, Anti-TPO, TSH, C3, C4– Consider "autoimmune" tests: basophil CD203c level or CU index– Skin biopsy to exclude urticarial vasculitis or define cellular picture in atypical cases (elevated
CRP or ESR, unresponsive to antihistamines, lesion duration >24h, painful rather than pruritic, petechial or purpuric changes, leave residual pigment changes).
• Peroni: Up to 40-60% of patients with UV may present only with wheals, therefore, a skin biopsy should be considered in all cases of otherwise clinically typical chronic urticaria, especially if the urticaria is resistant to antihistamines
• Procedure– 3 mm punch biopsy from a fresh lesion. Patients receiving steroids may need to discontinue these medications to
allow new lesions to form.– Biopsy specimens should be submitted in formalin for routine H&E staining and in those patients in whom
urticarial vasculitis is a strong consideration, in Michel’s media or freshly snap frozen for DIF microscopy.

Bernstein
• History/physical exam• Evaluate for evidence of physical urticarias, dermatographism• Initial testing
– CBC/diff– ESR– TSH– LFTs– UA– Allergy skin testing is not indicated in the initial evaluation of urticaria
• Testing for refractory cases– C4– Anti-Tg, Anti-TPO– H. pylori antibodies– Hepatitis panel– Consider autologous serum skin test– Consider skin biopsy if urticaria are atypical, not evanescent

Dreyfus
• Initial testing– TSH, Anti-Tg– CBC/diff– SPEP– LFTs– Hepatitis titers– H. pylori IgG, IgM and titers for other infectious illness - if suggested by history– ANA and anti-DNA anti-bodies - if history or exam suggestive of vasculitis– C1INH level and function, C2, C4 - if angioedema present– Chromagranin A or urine catecholamines - if significant flushing, carcinoid features– Tryptase - if significant component of anaphylaxis with urticaria, angioedema– CXR and PFT - if associated respiratory symptoms such as cough, wheezing– Total immunoglobulin levels, B/T cell subsets - if history suggestive of parasitic infection,
chronic infection– Pregnancy testing - if relevant age and sex– Serum basophil activation or histamine release in vitro and/or autologous skin testing - not
required but may be useful to confirm diagnosis
EAACI/WAO Guideline (2013)
• Routine diagnostic tests:– CBC/diff– ESR or CRP– Omission of suspected drugs (e.g. NSAID)
• Extended diagnostic program for identification of eliciting factors and for ruling out possible differential diagnoses if indicated:
– Infectious diseases (e.g. Helicobacter pylori)– Test for type I allergy - rare cause of chronic urticaria in patients with daily or almost daily
symptoms, but must be considered in patients with intermittent symptoms– Functional autoantibodies– Thyroid hormones and autoantibodies– Skin tests including physical tests– Pseudoallergen-free diet for 3 weeks– Tryptase level– Autologous serum skin test– Lesional skin biopsy

Diagnostic Approach for Children (Boguniewicz)
• Routine testing– Allergy testing– CBC/diff– ESR– LFTs– TSH, FT4, anti-Tg, anti-TPO
• Extended testing for selected patients– Hepatitis serology– Complement levels– ANA and specific autoimmune testing– EBV testing– Stool ova and parasites– Skin biopsy if vasculitis or mastocytosis are suspected
• Children whose CU persists should have yearly re-evaluation to rule-out late onset autoimmune disease
•

Specialized Lab Testing for Urticaria
• CU Index - patient's serum is added to healthy donor basophils and quantity of histamine release is measured. The reference range for a healthy non-CU population is <10. Values ≥10 indicate that basophils were stimulated by patient serum to release histamine (the larger the value the more histamine released).
– In one study, 23% of healthy controls vs. 57% of CU patients had a positive CU index– Positive CU Index associated with more severe CIU
• Anti-FcεR1 (high affinity IgE receptor) IgG antibody- by Western blot, direct measurement of IgEreceptor autoantibodies
– These antibodies may not correlate with disease activity and have been identified in other autoimmune diseases (even in the absence of urticaria), including pemphigus vulgaris, SLE, dermatomyositis, and pemphigoid, suggesting that these antibodies may represent an epiphenomenon.
• Anti-IgE IgG antibody• Basophil CD203c levels - by flow cytometry, indirect measure of autoantibodies to IgE receptor
which result in basophil activation.• Anti-C1q antibody - Patients with hypocoplementemic urticarial vasculitis syndrome (HUVS) usually
have autoantibodies reactive with the collagen-like region of the C1q molecule, and can develop angioedema.
•

Additional Testing Notes
• D-dimer - elevated D-dimer may be a biomarker of antihistamine-resistant chronic urticaria (Asero)
– This subtype may respond to anticoagulation with tranexamic acid and low molecular weight heparin
• Wedi - careful search for at least infections with H. pylori, strep, and perhaps also staph and yersinia should be included in the work-up of severely affected patients; our routine work-up includes:
– Helicobacter pylori monoclonal stool antigen test– Serology for strep (ASO, anti-DNase B), staph (antistaphylolysin), yersinia (IgA, IgG,
immunoblot). If an infection is identified, it should be appropriately treated and it should be checked whether eradication has been achieved.
• Initial evaluation for autoinflammatory syndromes (e.g. CAPS) should include:– CBC/diff - to screen for neutrophilia– CRP, ESR– ANA - help rule out autoimmune disease– UA - screen for proteinuria which suggests renal amyloidosis– Serum amyloid A level - inflammation marker and screening parameter for amyloidosis– Gene mutation analysis if specific diagnosis suspected (e.g. CAPS)

93

Chronic infection and chronic urticaria
• Chronic infection — in most cases it is not clear whether the two processes are related, occur simultaneously by chance, or are influenced by medications– The following infections reported to be associated with urticaria, with
improvement after infection resolved:• Parasitic
– Ascaris, Ancylostoma, Strongyloides, Filaria, Giardia lamblia, Entamoeba spp, Blastocystisspp, Echinococcus, Schistosoma, Trichinella,Toxocara, and Fasciola
– Anisakis simplex (a sea fish nematode) has been reported as possible cause of recurrent acute urticaria in areas of the world where uncooked fish is eaten frequently
• Bacterial: H. pylori, Streptococcus spp, Staphylococcus spp, Yersiniaenterocolitica, Mycoplasma pneumonia
– In a meta-analysis, rate of CU remission when H. pylori was eradicated was 30.9% vs. 21.7% when not
• Viral: hepatitis C, CMV, EBV, norovirus, parvovirus B19• Unspecified organisms: tonsillitis, sinusitis, dental infection, UTI• Fungal: The existence of an ‘id’ reaction with urticaria secondary to a fungal
infection is no longer considered tenable (Kaplan)

Malignancy and chronic urticaria
• Lymphoproliferative disease/malignancy — rarely have simple urticaria, typically have lesions consistent with urticarial vasculitis, and present with other systemic symptoms– Schnitzler's syndrome - onset in 50's, monoclonal IgM or
IgG gammopathy with recurrent fever, weight loss, bone pain, myalgias/arthralgias, lymphadenopathy, and non-pruritc urticaria that may become pruritic. May be due to circulating immune complexes and complement activation, anakinra (IL-1R antagonist) effective.
– Also reported with B-cell lymphomas, Hodgkins, CML, lung/colorectal/liver carcinomas
Back up slides about Role of Omalizumab in CSU
97

98
Emerging a New Standard of Care for
Refractory CSU Patients
Xolair® (omalizumab)
Treatment of antihistamine-refractory patients (cont’d)

How do you help yourrefractory CSU patients when…?
99
Up to 50% of CSU patients have an inadequate response to H1-antihistamines at licensed doses.1,2
Beyond Omalizumab, there are no other licensed treatment options.1
Until now, there has been no standard of care for these refractory CSU patients.1
1. Maurer M, et al. Allergy 2011;66:317–30.
2. Weller K, et al. J Eur Acad Dermatol venereol 2013;27:43-50

Now you can change the lives ofrefractory CSU patients with
Omalizumab
100
Introduction to Omalizumab
Xolair® (omalizumab) is a recombinant DNA-derived humanized monoclonal antibody that selectively binds to human immunoglobulin E (lgE).
Xolair® 300mg (2x150mg/4 weeks) injection is indicated for adults and adolescents (12 years of age and above) with chronic spontaneous urticaria refractory to standard of care.
Xolair BPI, 2014
In Allergic Asthma:
Xolair has been listed in the Egyptian market for more than 6 years, and indicated for
adults and children (6 years of age and above) with moderate to severe persistent allergic
asthma whose symptoms are inadequately controlled with inhaled corticosteroids (ICS).
Xolair has been shown to decrease the incidence of asthma exacerbations in these
patients. Safety and efficacy have not been established in other allergic conditions.

Apart from reducing free IgE levels, the additional mechanisms by which omalizumab works in patients with CSU remains unclear.
Reports describe patients with CSU as having abnormal basophil function, including:1
• Decreased responsiveness to stimuli acting through the IgE receptor (50% of patients),
• Blood basopenia, and
• Recruitment of basophils into skin lesions.
With successful therapy, blood basopenia and FcεRIfunction began to return to normal levels.1
1021. Vonakis BM, Saini SS. New concepts in chronic urticaria. Curr Opin Immunol 2008;20:709-16.
Omalizumab Mode of Action:

In previous studies, omalizumab reduced free IgE levels within hours after administration and down regulates FcεRI on blood basophils within 2 weeks;
A study of human cutaneous mast cells indicates a down regulatory effect in 3 to 4 weeks.1,2
However, in individual patients the time course of symptom control does not necessarily follow these parameters.
103
1. Beck LA, Marcotte GV, MacGlashan D, Togias A, Saini S. Omalizumab-induced reductions in mast cell FcεRI expression and function. J Allergy Clin Immunol 2004;114:527-30.
2. Gomez G, Jogie-Brahim S, Shima M, Schwartz LB. Omalizumab reverses the phenotypic and functional effects of IgE-enhanced FcεRI on human skin mast cells. J Immunol 2007;179:1353-61.
Omalizumab Mode of Action
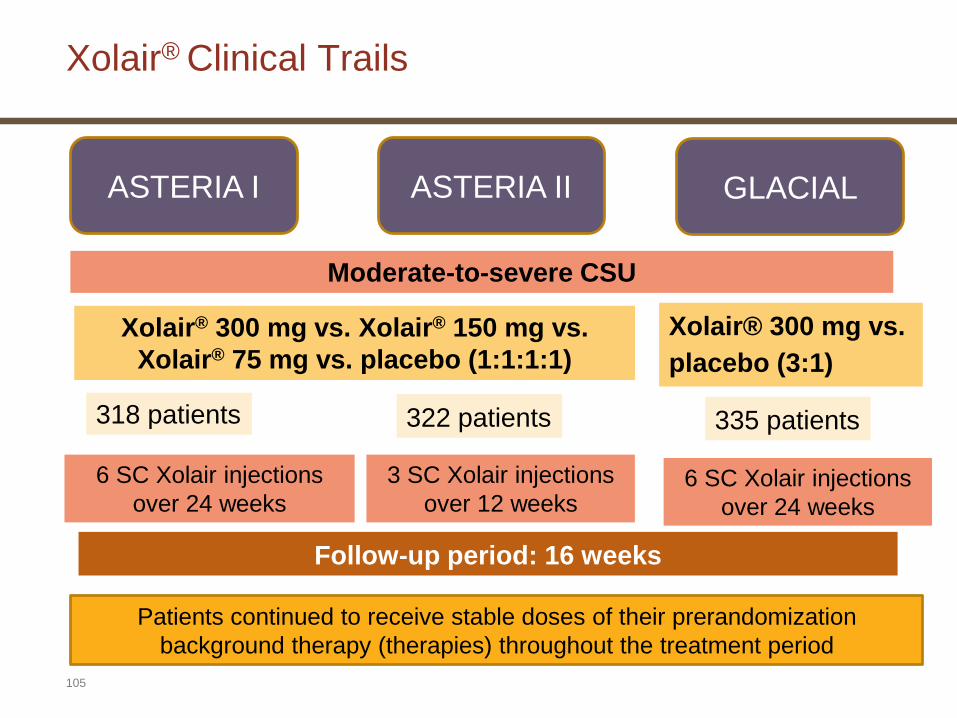
Xolair® Clinical Trails
105
6 SC Xolair injections
over 24 weeks
ASTERIA I ASTERIA II GLACIAL
Xolair® 300 mg vs. Xolair® 150 mg vs.
Xolair® 75 mg vs. placebo (1:1:1:1)
Moderate-to-severe CSU
Follow-up period: 16 weeks
Xolair® 300 mg vs.
placebo (3:1)
318 patients 322 patients 335 patients
3 SC Xolair injections
over 12 weeks6 SC Xolair injections
over 24 weeks
Patients continued to receive stable doses of their prerandomization
background therapy (therapies) throughout the treatment period

Patient baseline demographics (mITT population): ASTERIA II and GLACIAL*
*Please refer to the manuscripts for a full list of patient baseline demographic data;
Data are means (SDs) unless otherwise stated;†Measured in 78 patients in the placebo group.
CIU=chronic idiopathic urticaria; CSU=chronic spontaneous urticaria; DLQI=Dermatology Life
Quality Index; mITT=modified intention to treat; OMA=omalizumab; SD=standard deviation;
UAS=urticaria activity score; UAS7=weekly urticaria activity score.
1. Maurer M, et al. N Engl J Med 2013;
2. Kaplan A, et al. J Allergy Clin Immunol 2013.
Characteristic ASTERIA II1 GLACIAL2
Placebo
(n=79)
OMA 75 mg
(n=82)
OMA 150 mg
(n=82)
OMA 300 mg
(n=79)
Placebo
(n=83)
OMA 300 mg
(n=252)
Age, years 43.1 12.5 39.7 15.0 43.0 13.2 44.3 13.7 44.3 14.7 42.7 13.9
Female sex, no. (%) 55 (70) 61 (74) 65 (79) 63 (80) 55 (66.3) 186 (73.8)
Race (white), no. (%) 70 (89) 64 (78) 70 (85) 68 (86) 75 (90.4) 223 (88.5)
Body mass index (kg/m2) 30.0 7.7 30.2 7.7 30.0 7.3 29.0 6.3 31.0 9.6 29.4 7.1
Time since diagnosis of CSU,
years
Mean
Median
7.2 10.7
3.3
5.3 7.1
2.5
7.2 8.9
3.9
6.1 7.3
3.5
8.8 11.2
4.1
7.0 8.8
3.4
No. of previous CSU medications 4.4 2.9 4.1 2.1 4.5 3.2 4.3 2.5 6.4 2.9 5.9 2.5
In-clinic UAS 5.3 0.7 5.4 0.8 5.3 0.7 5.3 0.7 5.2 0.8 5.2 0.8
UAS7 31.0 6.6 30.7 6.9 31.4 7.0 29.5 6.9 30.2 6.7 31.2 6.6
Weekly itch severity score 14.0 3.4 14.0 3.7 14.2 4.1 13.7 3.5 13.8 3.6 14.0 3.6
Weekly no. of hives score 17.0 4.2 16.8 4.2 17.1 4.1 15.8 4.6 16.4 4.6 17.1 4.2
Overall DLQI score 12.6 5.9† 12.6 6.5 13.0 6.1 12.7 6.4
Presence of angioedema, no (%) 30 (38) 31 (38) 38 (46) 32 (41) 41 (49.4) 137 (54.4)

Objectives of the 3 clinical trials
107
− Evaluation of the efficacyof Omalizumab compared with placebo in patients who remained symptomatic despite H1-antihistamine therapy (at licensed doses.)
− Safety and tolerability were evaluated as secondary objectives.
GLACIAL ASTERIA I and ASTERIA II
− Evaluation of the safety of Omalizumab compared with placebo in CSU patients who remained symptomatic despite treatment with H1-antihistamines at up to 4 times the approved dose plus H2-antihistamines, leukotriene receptor antagonists, or both.
− Efficacy was assessed as a secondary objective.

Primary and secondary endpoints
Asteria I
N=318
Asteria II
N=322
Glacial
N=335
Primary
endpoint
Change from baseline to Week 12 in weekly
Itch Severity Score (ISS)Safety
Secondary
endpoints
At Week 12:
• Change from baseline in UAS7
• Change from baseline in weekly # of hives score
• Time to MID (≥5 points) response in weekly ISS
• Proportion of patients with UAS7 ≤6
• Proportion of weekly ISS MID responders
• Change from baseline in weekly size of largest
hive score
• Change from baseline in DLQI
• Proportion of angioedema-free days from Week 4
to Week 12 of therapy
• Proportion of Complete Responders (UAS7=0)*
Same as Asteria I
and Asteria II
primary and
secondary endpoints
*Exploratory endpoint in Asteria II. DLQI, Dermatology Life Quality Index, UAS7, urticaria activity score over 7 days.
MID: minimal important difference
Summary for results of
Omalizumab 300 mg vs Placebo in
Phase III Programme in CSU
110
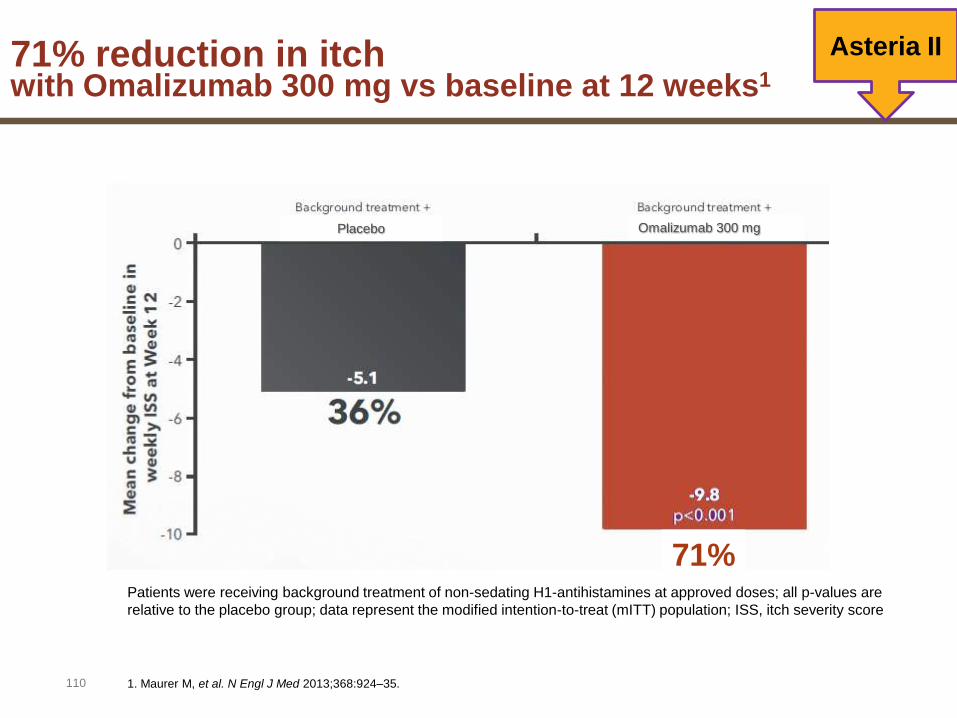
71% reduction in itch with Omalizumab 300 mg vs baseline at 12 weeks1
Asteria II
Patients were receiving background treatment of non-sedating H1-antihistamines at approved doses; all p-values are
relative to the placebo group; data represent the modified intention-to-treat (mITT) population; ISS, itch severity score
1. Maurer M, et al. N Engl J Med 2013;368:924–35.
Omalizumab 300 mgPlacebo
71%

111
Omalizumab 300 mgPlacebo
Patients were receiving background treatment of non-sedating H1-antihistamines at approved doses; all p-values are
relative to the placebo group; data represent the modified intention-to-treat (mITT) population; ISS, itch severity score
67% reduction in itch with Omalizumab 300 mg vs baseline at 12 weeks1,2
Asteria I
1. Saini SS, et al. Ann Allergy Asthma Immunol 2013;111 (Suppl. 5):A18.
2. Rosén K, et al. Allergy 2013;68 (Suppl. 97):259.
67%

62% reduction in itch with Omalizumab 300 mg vs baseline at 12 weeks1
112
Glacial
Patients were receiving background treatment of non-sedating H1-antihistamines (up to 4x the approved dose)
plus H2-antihistamines and/or leukotriene-receptor antagonists; all p-values are relative to the placebo group;
data represent the modified intention-to-treat (mITT) population; ISS, itch severity score
1. Kaplan A, et al. J Allergy Clin Immunol 2013;132:101–9
29%
Omalizumab 300 mgPlacebo
62%
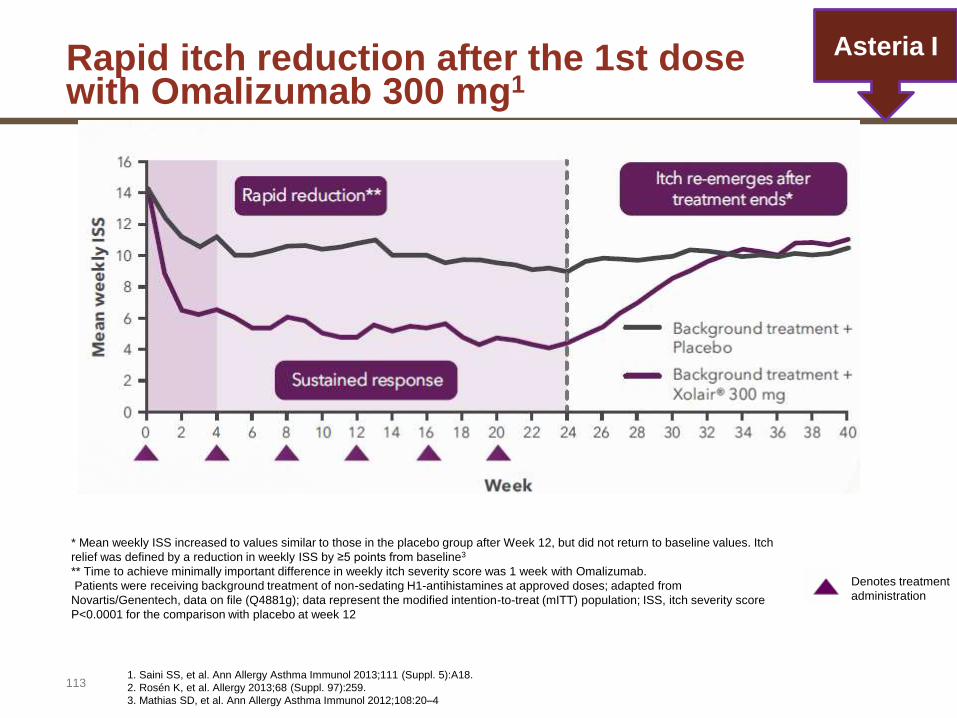
Rapid itch reduction after the 1st dosewith Omalizumab 300 mg1
113
Asteria I
1. Saini SS, et al. Ann Allergy Asthma Immunol 2013;111 (Suppl. 5):A18.
2. Rosén K, et al. Allergy 2013;68 (Suppl. 97):259.
3. Mathias SD, et al. Ann Allergy Asthma Immunol 2012;108:20–4
* Mean weekly ISS increased to values similar to those in the placebo group after Week 12, but did not return to baseline values. Itch
relief was defined by a reduction in weekly ISS by ≥5 points from baseline3
** Time to achieve minimally important difference in weekly itch severity score was 1 week with Omalizumab.
Patients were receiving background treatment of non-sedating H1-antihistamines at approved doses; adapted from
Novartis/Genentech, data on file (Q4881g); data represent the modified intention-to-treat (mITT) population; ISS, itch severity score
P<0.0001 for the comparison with placebo at week 12
Denotes treatment
administration
114
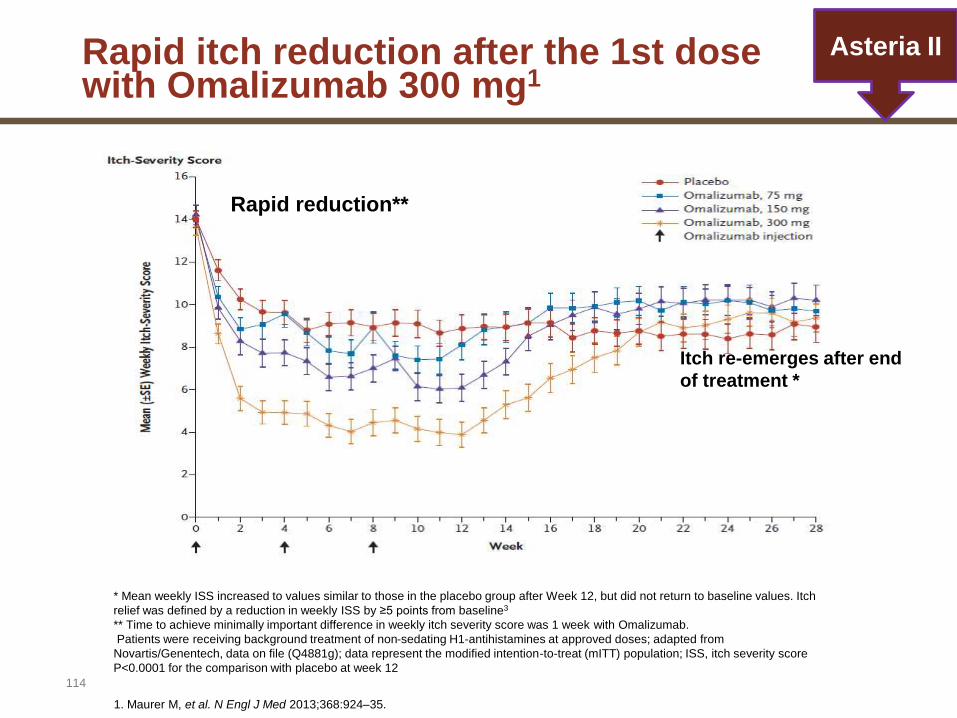
Asteria II
* Mean weekly ISS increased to values similar to those in the placebo group after Week 12, but did not return to baseline values. Itch
relief was defined by a reduction in weekly ISS by ≥5 points from baseline3
** Time to achieve minimally important difference in weekly itch severity score was 1 week with Omalizumab.
Patients were receiving background treatment of non-sedating H1-antihistamines at approved doses; adapted from
Novartis/Genentech, data on file (Q4881g); data represent the modified intention-to-treat (mITT) population; ISS, itch severity score
P<0.0001 for the comparison with placebo at week 12
1. Maurer M, et al. N Engl J Med 2013;368:924–35.
Rapid itch reduction after the 1st dosewith Omalizumab 300 mg1
Rapid reduction**
Itch re-emerges after end
of treatment *

115
Rapid itch reduction after the 1st dosewith Omalizumab 300 mg2
* Mean weekly ISS increased to values similar to those in the placebo group after Week 12, but did not return to baseline values. Itch relief was defined by a
reduction in weekly ISS by ≥5 points from baseline6
** Time to achieve minimally important difference in weekly itch severity score was 2 weeks with Omalizumab.2
Patients were receiving background treatment of non-sedating H1-antihistamines (up to 4x the approved dose) plus H2-antihistamines and/or leukotriene-
receptor antagonists. Data represent the modified intention-to-treat (mITT) population; ISS, itch severity score.
P <.001 for the comparison with placebo at week 12
Mean change from baseline in weekly ISS by study week (baseline observation carried forward
method, modified intention-to-treat population).
Itch re-emerges after end of
treatment *
Rapid reduction**
....
....
..........
............
...
......Discontinuation of Omalizumab
adapted from Kaplan A, et al. 2013
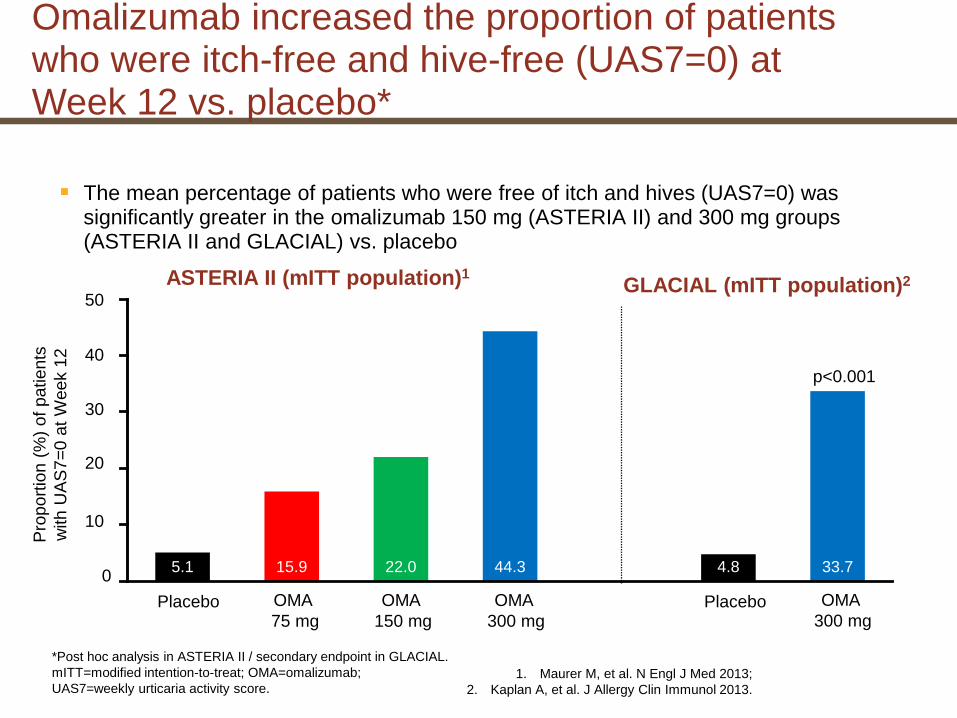
Omalizumab increased the proportion of patients who were itch-free and hive-free (UAS7=0) at Week 12 vs. placebo*
The mean percentage of patients who were free of itch and hives (UAS7=0) was significantly greater in the omalizumab 150 mg (ASTERIA II) and 300 mg groups (ASTERIA II and GLACIAL) vs. placebo
ASTERIA II (mITT population)1GLACIAL (mITT population)2
0
10
20
50
5.1 15.9 22.0 44.3 4.8 33.7
Pro
po
rtio
n (
%)
of
pa
tie
nts
with U
AS
7=
0 a
t W
eek 1
2
22.0
44.340
30
1. Maurer M, et al. N Engl J Med 2013;
2. Kaplan A, et al. J Allergy Clin Immunol 2013.
*Post hoc analysis in ASTERIA II / secondary endpoint in GLACIAL.
mITT=modified intention-to-treat; OMA=omalizumab;
UAS7=weekly urticaria activity score.
p<0.001
OMA
300 mgPlaceboPlacebo OMA
75 mg
OMA
150 mg
OMA
300 mg
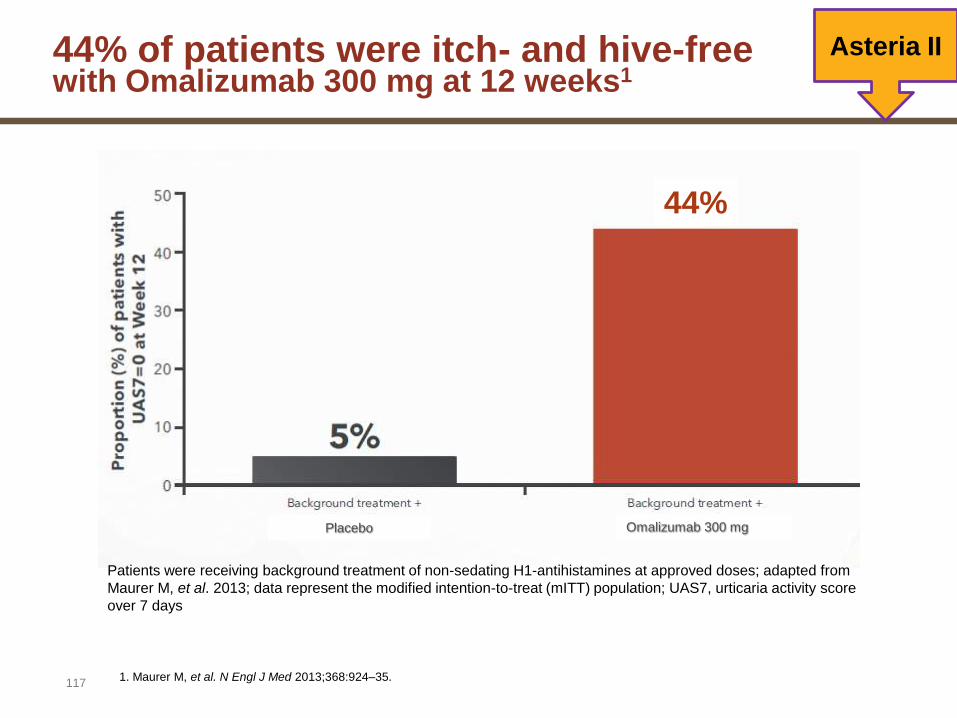
44% of patients were itch- and hive-freewith Omalizumab 300 mg at 12 weeks1
117
Omalizumab 300 mgPlacebo
Patients were receiving background treatment of non-sedating H1-antihistamines at approved doses; adapted from
Maurer M, et al. 2013; data represent the modified intention-to-treat (mITT) population; UAS7, urticaria activity score
over 7 days
1. Maurer M, et al. N Engl J Med 2013;368:924–35.
Asteria II
44%

Omalizumab significantly increased the proportion of patients who were well controlled (UAS7≤6) at Week 12*
A significantly higher proportion of patients in the omalizumab 150 mg (ASTERIA II) and 300 mg groups (ASTERIA II and GLACIAL) had symptoms which were well-controlled (UAS7≤6) vs. placebo
0
15
30
45
60
75
90
19 27 43 66 12.0 52.4
Pro
port
ion (
%)
of
patients
with
UA
S7≤6 a
t W
eek 1
2
42.7
65.8
p<0.05
p<0.05
*Secondary endpoint in ASTERIA II and GLACIAL.
mITT=modified intention-to-treat; OMA=omalizumab;
UAS7=weekly urticaria activity score.
ASTERIA II (mITT population)1 GLACIAL (mITT population)2
1. Maurer M, et al. N Engl J Med 2013;
2. Kaplan A, et al. J Allergy Clin Immunol 2013.
p<0.001
OMA
300 mgPlaceboPlacebo OMA
75 mg
OMA
150 mg
OMA
300 mg
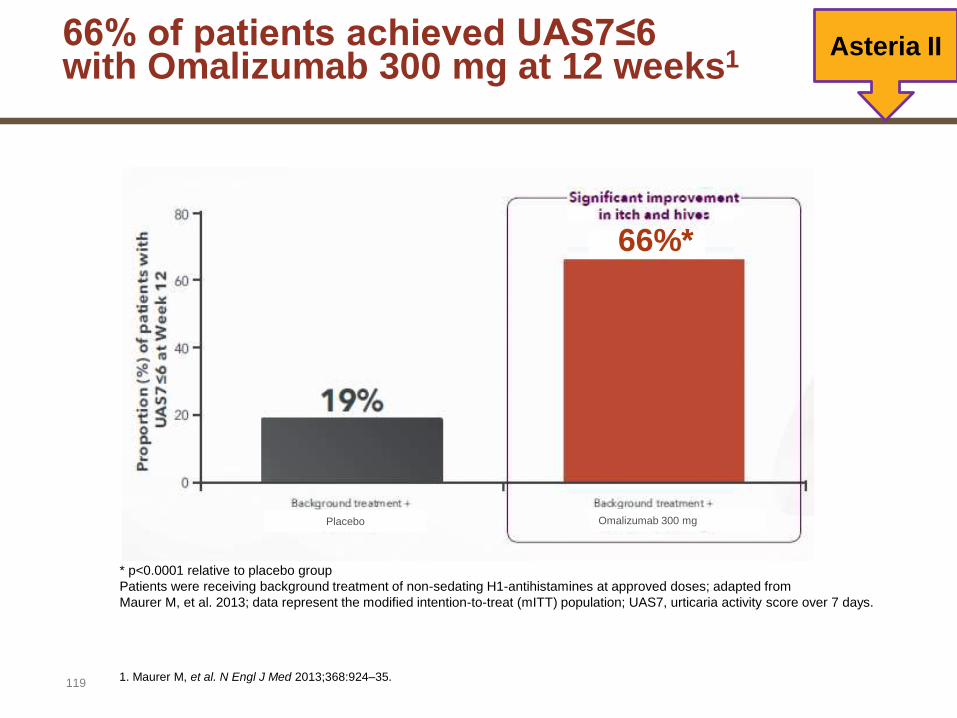
66% of patients achieved UAS7≤6with Omalizumab 300 mg at 12 weeks1
119
Asteria II
1. Maurer M, et al. N Engl J Med 2013;368:924–35.
66%*
Omalizumab 300 mgPlacebo
* p<0.0001 relative to placebo group
Patients were receiving background treatment of non-sedating H1-antihistamines at approved doses; adapted from
Maurer M, et al. 2013; data represent the modified intention-to-treat (mITT) population; UAS7, urticaria activity score over 7 days.

Omalizumab significantly improved QoL (DLQI)* at Week 12 vs. placebo
*Secondary endpoint in ASTERIA II and GLACIAL.
DLQI=Dermatology Life Quality Index; mITT=modified intention-to-treat population;
OMA=omalizumab; QoL=quality-of-life.
1. Maurer M, et al. N Engl J Med 2013;
2. Kaplan A, et al. J Allergy Clin Immunol 2013.
–15
–10
–5
0
–8.3
–10.2
Change f
rom
baselin
e in
DLQ
I score
at
Week 1
2
p<0.001
p=0.02
ASTERIA II (mITT population)1 GLACIAL (mITT population)2
Significant improvements in QoL (measured using DLQI) seen with omalizumab 150 mg (ASTERIA II) and 300 mg (ASTERIA II and GLACIAL) vs. placebo
PlaceboOMA
75 mg
OMA
150 mg
OMA
300 mg
OMA
300 mgPlacebo
–6.1 –7.5 –8.3 –10.2 –5.1 –9.7
p<0.001

80% reduction in DLQI scorewith Omalizumab 300 mg vs baseline at 12 weeks1
121
Omalizumab 300 mgPlacebo
48%
80%
Asteria II
Patients were receiving background treatment of non-sedating H1-antihistamines at approved doses; all p-values are
relative to the placebo group; data represent the modified intention-to-treat (mITT) population; DLQI, Dermatology Life
Quality Index.
1. Maurer M, et al. N Engl J Med 2013;368:924–35.
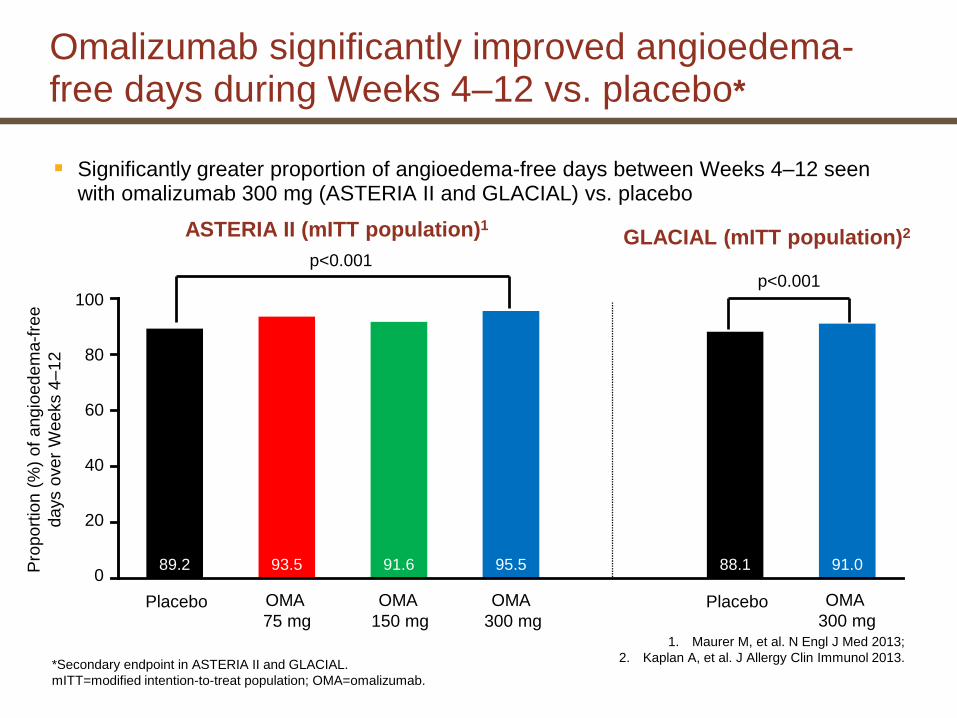
Omalizumab significantly improved angioedema-free days during Weeks 4–12 vs. placebo*
Significantly greater proportion of angioedema-free days between Weeks 4–12 seen with omalizumab 300 mg (ASTERIA II and GLACIAL) vs. placebo
1. Maurer M, et al. N Engl J Med 2013;
2. Kaplan A, et al. J Allergy Clin Immunol 2013.
ASTERIA II (mITT population)1GLACIAL (mITT population)2
*Secondary endpoint in ASTERIA II and GLACIAL.
mITT=modified intention-to-treat population; OMA=omalizumab.
0
20
40
60
80
100
89.2 93.5 91.6 95.5 88.1 91.0Pro
port
ion (
%)
of
ang
ioe
dem
a-f
ree
days o
ver
Weeks 4
–12
91.6
p<0.001
OMA
300 mgPlaceboPlacebo OMA
75 mg
OMA
150 mg
OMA
300 mg
p<0.001

76% reduction in weekly hives scorewith Omalizumab 300 mg vs baseline at 12 weeks1
123
Omalizumab 300 mgPlacebo
76%
Patients were receiving background treatment of non-sedating H1-antihistamines at approved doses; all p-values are relative to the placebo
group; adapted from Maurer M, et al. 2013; data represent the modified intention-to-treat(mITT) population
Asteria II
1. Maurer M, et al. N Engl J Med 2013;368:924–35.

Xolair® safety was investigated in over 700 patients in the CSU Phase III clinical program1
124
Overall incidences of adverse reactions were similar between Omalizumab and placebo patients. 2
1. Xolair Basic Prescribing Information
2. Kaplan A, et al. J Allergy Clin Immunol 2013;132:101–9
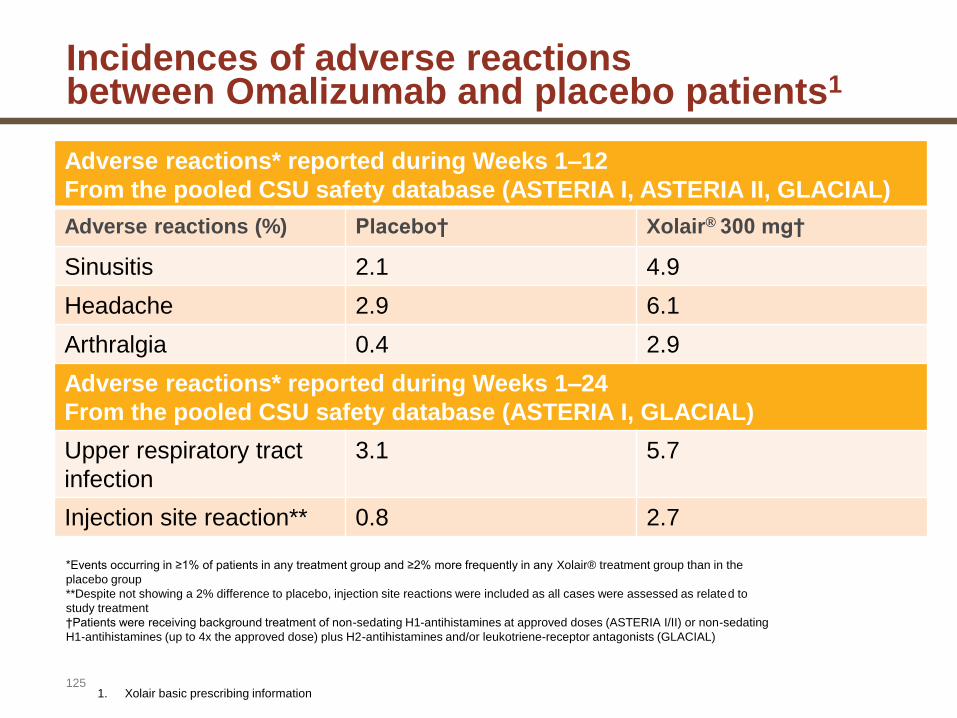
Incidences of adverse reactionsbetween Omalizumab and placebo patients1
125
Adverse reactions* reported during Weeks 1–12
From the pooled CSU safety database (ASTERIA I, ASTERIA II, GLACIAL)
Adverse reactions (%) Placebo† Xolair® 300 mg†
Sinusitis 2.1 4.9
Headache 2.9 6.1
Arthralgia 0.4 2.9
Adverse reactions* reported during Weeks 1–24
From the pooled CSU safety database (ASTERIA I, GLACIAL)
Upper respiratory tract
infection
3.1 5.7
Injection site reaction** 0.8 2.7
1. Xolair basic prescribing information
*Events occurring in ≥1% of patients in any treatment group and ≥2% more frequently in any Xolair® treatment group than in the
placebo group
**Despite not showing a 2% difference to placebo, injection site reactions were included as all cases were assessed as related to
study treatment
†Patients were receiving background treatment of non-sedating H1-antihistamines at approved doses (ASTERIA I/II) or non-sedating
H1-antihistamines (up to 4x the approved dose) plus H2-antihistamines and/or leukotriene-receptor antagonists (GLACIAL)
Xolair® has an established safety profilebased on long-term use in severe allergic asthma
126
Safety evaluated in >9,300 subjects receiving Omalizumab in clinical programs.1
Omalizumab has >400,000 patient years’ experience, since US approval in 2003, and EU approval in 2005.1
In the US, Xolair® is licensed for adults and adolescents (≥12 years of age) with moderate to severe persistent allergic asthma.2
In the EU, Xolair® is licensed for adults and adolescents (≥6 years of age) with severe persistent allergic asthma.3
Xolair® is now approved in >90 countries, including the EU.1
1. Sixteenth Periodic Safety Update Report (PSUR) dated 15.02.2013. Novartis data on file.
2. Xolair® US summary of product characteristics 2014.
3. Xolair® EU summary of product characteristics 2014.
Contraindication
127
Hypersensitivity to the active substance or to any of the excipients.
Xolair® Basic Prescribing information

Warnings and precautions 1
128
Allergic reactions:
• Anaphylactic reactions and other allergic reactions: Frequency rare. Medication for the treatment of anaphylactic reactions should be available immediately.
• Patients should be informed that such reactions are possible and prompt medical attention should be sought if allergic reactions occur.
Serum sickness and serum sickness-like reactions: Frequency rare.
Antihistamines and corticosteroids may be useful for preventing or treating this disorder, and patients should be advised to report any suspected
symptom.
Parasitic infections:
• Patients with high risk of helminth infection show a slight increase in infection rate.
• If patients do not respond to recommended anti-helminth treatment, discontinuation of Xolair® should be considered
Xolair® Basic Prescribing information

129
Patients should be observed following administration of Xolair® 300mg CSU:
• In more than 700 Omalizumab-treated patients enrolled in the Phase III trials, there were no cases of Omalizumab-related anaphylaxis1-4
Asthma1
• In patients with severe allergic asthma, anaphylaxis was rare (≥1/10,000 to <1/1,000) in previous clinical trials. Onset was usually within 2 hours of the first or subsequent injections, but may occur later.
Patients should be informed that such reactions are possible.1
1. Xolair basic prescribing information
2. Maurer M, et al. N Engl J Med 2013;368:924–35.
3. Kaplan A, et al. J Allergy Clin Immunol 2013;132:101–9
4. Saini SS, et al. Ann Allergy Asthma Immunol 2013;111 (Suppl. 5):A18.
Warnings and precautions 1

Omalizumab has a simple dosing schedule1
130
1. Xolair Basic Prescribing Information
2. Zuberbier T, et al. Allergy 2014 (in press).
The recommended dose is 300 mg(2x 150 mg) every
four weeks through subcutaneous administration.
– Clinical trial experience of long-term treatment beyond
6 months in this indication is limited.
– Prescribers are advised to periodically reassess the need for
continued therapy.
Recently updated international guidelines recommend
Omalizumab for patients inadequately controlled with
H1-antihistamines.2
With Omalizumab 300mg:
131
1
2
No need to determine baseline IgE levels.1
No need to calculate the dose based on patient’s
body weight. 1
1. Xolair Basic Prescribing Information
Xolair® provides improvement in itch severity independent of
patient’s weight or IgE levels1
There was no correlation between patients’ baseline IgE
levels/weight and response to Xolair®