Chronic Pain and Therapeutics 101
34
Chronic Pain and Therapeutics 101 Jeffrey Fudin, PharmD, DAAPM, FCCP, FASHP Remitigate, LLC 357 Delaware Avenue #214 Delmar, NY 12054 Cell Phone: 518-588-5651 http://www.paidr.com Topic Areas: Aspects of chronic and neuropathic pain: etiology; incidence and prevalence; principal symptoms and signs; nature and range of functional impairments; prognosis; current therapies; medical, functional, social, environmental Support issues; Describe areas in which adaptive neurotechnologies could play a role in diagnosis, treatment, and/or support. Participants; Mostly neuroscience and engineering grad students. There will be a few med students and residents. Suggested Readings in order of importance: 1. Kubotera N, Fudin J. Pain Management for Pharmacists – Concepts and Definitions. CE Program of The University of Connecticut School of Pharmacy and Drug Topics. Drug Topics. 2013 April; 52-61. 2. Zorn KE, Fudin J. Treatment of Neuropathic Pain: the Role of Unique Opioid Agents. Practical Pain Management. 2011 May; 11 (4): 26-33. 3. McCarberg B, Bainbridge JL, Fudin J. Optimizing Chronic Pain Management: Integrating Pharmacokinetics and Pharmacodynamics. (CME: The University of Kentucky College of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.) 4. Sasu-Tenkoramaa J, Fudin J. Neuropathy in the Cancer Patient: Causes and Cures. Practical Pain Management. 2013 April; 13(3):53-67.
Transcript of Chronic Pain and Therapeutics 101

Chronic Pain and Therapeutics 101
Jeffrey Fudin, PharmD, DAAPM, FCCP, FASHP
Remitigate, LLC
357 Delaware Avenue #214
Delmar, NY 12054
Cell Phone: 518-588-5651
http://www.paidr.com
Topic Areas:
Aspects of chronic and neuropathic pain: etiology; incidence and prevalence; principal
symptoms and signs; nature and range of functional impairments; prognosis; current
therapies; medical, functional, social, environmental
Support issues; Describe areas in which adaptive neurotechnologies could play a role in
diagnosis, treatment, and/or support.
Participants; Mostly neuroscience and engineering grad students. There will be a few med
students and residents.
Suggested Readings in order of importance:
1. Kubotera N, Fudin J. Pain Management for Pharmacists – Concepts and Definitions. CE
Program of The University of Connecticut School of Pharmacy and Drug Topics. Drug Topics. 2013
April; 52-61.
2. Zorn KE, Fudin J. Treatment of Neuropathic Pain: the Role of Unique Opioid Agents. Practical
Pain Management. 2011 May; 11 (4): 26-33.
3. McCarberg B, Bainbridge JL, Fudin J. Optimizing Chronic Pain Management: Integrating
Pharmacokinetics and Pharmacodynamics. (CME: The University of Kentucky College of Pharmacy
is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing
pharmacy education.)
4. Sasu-Tenkoramaa J, Fudin J. Neuropathy in the Cancer Patient: Causes and Cures. Practical Pain
Management. 2013 April; 13(3):53-67.

7/21/2016
1
Jeffrey Fudin, B.S., Pharm.D., FCCP, FASHPDiplomate, Academy of Integrative Pain Management (AIPM)
President and Director, Scientific and Clinical Affairs, REMITIGATE LLCClinical Pharmacy Specialist & PGY2 Pain Residency Director; Stratton VA Medical Center
Adjunct Affiliations;Albany College of Pharmacy & Health Sciences,
Western New England University College of Pharmacy, UCONN School of Pharmacy
www.paindr.com
Chronic Pain and Therapeutics 101Short Course on Adaptive Neurotechnologies
Topic Areas
Initial Topic Areas
• Aspects of chronic and neuropathic pain: etiology; incidence and prevalence; principal symptoms and signs; nature and range of functional impairments; prognosis; current therapies; medical, functional, social, environmental
• Support issues; Describe areas in which adaptive neurotechnologies could play a role in diagnosis, treatment, and/or support.
Focus
• Pharmacotherapeutics (pros, cons, unmet needs)
Participants
• Mostly neuroscience and engineering grad students. There will be a few med students and residents.

7/21/2016
2
Learning Objectives
1. Identify the prevalence of pain and understand medication‐related morbidity and mortality.
2. Define acute chronic pain, analgesia, nociceptor, noxious stimulus, and pain threshold.
3. Differentiate neuropathic, somatic, and visceral pain.
4. Categorize medications that are useful for pain including opioids, NSAIDs, antidepressants, anticonvulsants, and others.
5. Summarize medication therapeutic advantages and complexities, and be familiar with political and medical pitfalls of the various medications used to treat pain.
In 2013, the CDC identified approximately this number of persons as dying from prescription opioids:
A. 8,000
B. 9,000
C. 16,000
D. 18,000

7/21/2016
3
A. 8,000
B. 9,000
C. 16,000
D. 18,000
In 2013, the CDC identified approximately this number of persons as dying from NSAID‐related GI bleeds:
What drug categories are first line agents for neuropathic pain?
A. Antidepressants
B. Anticonvulsants
C. NSAIDs
D. Opioids

7/21/2016
4
U.S. Prescription Opioid‐Related Deaths
• Approximately 16,000 deaths in 2013 from Rx opioids
• Approximately 9,000 deaths in 2013 from heroin
• According to the CDC:
• ~85% unintentional ≈ 13,600 deaths
• ~37 unintentional deaths/day
• ~1 unintentional death every 40 minutes
• Children/infant deaths
• ~3,300 in 2014 (down from 5,187 in 2004)
Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep. 2015;64(1):32. National Vital Statistics Reports. 2015;64(2). www.cdc.gov/nchs/.Chen LH, et al. QuickStats: Rates of Deaths from Drug Poisoning and Drug Poisoning Involving Opioid Analgesics—United States, 1999–2013. MMWR Morb Mortal Wkly Rep 2015;64:32. (http://origin.glb.cdc.gov/mmwr/preview/mmwrhtml/mm6401a10.htm?s_cid=mm6401a10_w)
Utilization of Healthcare Resource• Over 50% of ED visits for opioid‐induced respiratory
depression (OIRD) and overdose result in admission/hospitalization
• Average length of stay is about 3.6 days• Average hospital charges: $30,000 per patient per
visit• Up to 10% of ED visits for OIRD and overdose result
in near‐fatal events requiring mechanical ventilation• 22% are discharged to another institution (nursing
home or rehabilitation center) following ED stay and admission $$$$
Hasegawa K, et al. Mayo Clin Proc. 2014;89(4):462‐471. Healthcare Cost and Utilization Project (HCUP); Agency for Healthcare Research and Quality. HCUP Databases. www.hcup‐us.ahrq.gov/databases.jsp. Yokell MA, et al. JAMA Intern Med. 2014;174(12):2034‐2037.

7/21/2016
5
Therapeutic Drug Classes v Pain Type
• Somatic Pain
– NSAIDs, steroids, opioids, SNRIs
• Visceral Pain
– NSAIDs, opioids
• Neuropathic Pain
– Anticonvulsants, antidepressants, opioids (limited)
Multiple Types of Pain
Adapted from: Woolf CJ. Ann Intern Med. 2004;140:441-451.*Chong MS, Bajwa ZH. J Pain Symptom Manage. 2003;25:S4-S11.
A. Nociceptive Pain
B. Inflammatory Pain
C. Neuropathic Pain
D. Noninflammatory/Non-neuropathic pain
Noxious peripheral
stimuli
Peripheral nerve damage
No known tissue or nerve damage
Abnormal central processing
Multiple mechanisms
Brain
Brain
Brain
Brain
Inflammation
• Patients may experience multiple pain states simultaneously*

7/21/2016
6
Rational PolypharmacyAdvantages
• Reduction in pain intensity• Reduction in RX toxicity & SEs• Improved efficacy• Possible improvement in surgical
outcome & decreased LOS?
Disadvantages
• Requires knowledge of drugs, PK data, & pharmacodynamics
• Every analgesic has its own unique adverse event profile
• May increase drug-drug interactions
1. Sinatra RS. Ann Meeting Cleveland Soc of Anesthesiology. Nov 2010.2. Kehlet H and Wilmore DW. Am J Surg. 2002;183:630‐41.
12

7/21/2016
7

7/21/2016
8
DF
PL
-745
,337
rofe
coxi
bN
S-3
98et
odol
acm
elox
icam
nim
esul
ide
cele
coxi
bto
mox
ipro
ldi
clof
enac
suli
ndac
sulp
hide
piro
xica
mm
eclo
fena
mat
edi
flun
isal
nifl
umic
acid
sodi
um s
alic
ylat
efe
nopr
ofen
zom
epir
acin
dom
etha
cin
tolm
etin
napr
oxen
ibup
rofe
nam
pyro
neke
topr
ofen
aspi
rin
flur
bipr
ofen
supr
ofen
keto
rola
c
0
20
40
60
80
100%
inhi
biti
on C
OX
-1 w
hen
CO
X-2
inhi
bite
d by
80%
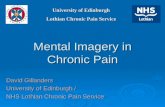
Relationship between 80% (‘therapeutic’) inhibition of COX-2 and inhibition of COX-1 in an in vitro human whole blood
assay
Warner et al, PNAS 1999; 96:7563-7568
Relative COX-2 Specificity
See http://paindr.com/wp-content/uploads/2012/05/COX-2_specificity.pdf
Abnormal, not unpleasant sensations(eg, tingling)
Paresthesias
Abnormal, unpleasant sensations (eg, shooting, lancinating, burning)
Dysesthesias
Persistent burning pain, shocklike pain
Spontaneous pain
DescriptionSymptom
Spontaneous Symptoms
Baron. Baron. ClinClin J Pain.J Pain. 2000;16(2 suppl):S122000;16(2 suppl):S12--S20; International Association for the Study of Pain S20; International Association for the Study of Pain Website. Website. Available at: Available at: http://www.iasphttp://www.iasp--pain.org/termspain.org/terms--p.htmlp.html. Accessed September 30, 2004.. Accessed September 30, 2004.

7/21/2016
9
Stimulus-Evoked Symptoms
Explosive response to normally painful stimulus
Hyperpathia
Heightened response to normally painful stimulus
Hyperalgesia
Painful response to nonpainful stimulus
Allodynia
DefinitionSymptom
International Association for the Study of Pain Web site. International Association for the Study of Pain Web site. Available at: Available at: http://www.iasphttp://www.iasp--pain.org/termspain.org/terms--p.htmlp.html. Accessed September 30, 2004.. Accessed September 30, 2004.
Limiting Calcium Influx Can Temper Hyperexcitable Neurons
• Limit amount of Ca2+ entering presynaptic neuron upon excitation
• Allow enough Ca2+ for normal nerve function• Two pharmacologic strategies
− Block Ca2+ channels− Modulate channels without blocking (allosteric)

7/21/2016
10
Mechanisms of Neuropathic Pain: Central Sensitization
• Peripheral nociceptor inputs trigger molecular changes in central neurons
• Long-lasting changes may result from − Altered receptor expression− Inhibitory interneuron death
Modification of GABA, glycine receptors
NMDA and AMPA receptor activation
Reduce effect of inhibition
Lower firing threshold
GABA = GABA = --aminobutyric acid; NMDA = aminobutyric acid; NMDA = NN--methylmethyl--DD--aspartate; aspartate; AMPA = AMPA = --aminoamino--33--hydroxylhydroxyl--55--methylmethyl--44--isoxazolepropionate.isoxazolepropionate.
Woolf, Salter. Woolf, Salter. ScienceScience. 2000. 2000;288:1765;288:1765--17681768. .
Overview
• Etiology and Pathogenesis
• Tricyclic Antidepressants
• SSRIs, SNRIs, SARIs, MOAIs
• Drug Interactions (iso‐enzyme metabolism)
• Anti‐convulsants
• Anti‐arrhythmic
• Topicals

7/21/2016
11
Pathogenesis related to DM
• Poorly controlled hypergylcemia.
• Accumulation of sorbitol in nerve cells.
• Decrease in nerve free myoinositol and dcreased activity of nerve sodium‐potassium adenosine triphosphate.
• Increased nonenzymatic peripheral nerve glycosylation.
• Nerve hypoxia.
Other Causes‐1
• Diseases
– A.I.D.S.
– Herpes Simplex Virus
– Syphilis
– Sclerotic/Connective Tissue Disorders
• Back/Tissue Injury
• Iatrogenic Causes

7/21/2016
12
Differential Diagnosis
• Organic Peripheral Neuropathy
• B‐12
• Porphyria
• Heavy Metal poisoning
• Collagen Disease
• Cancer
• Lymphoma
• Diabetes
Tricyclic Antidepressants• Amitriptyline• Imipramine• Nortriptyline• Desipramine• Clomipramine• Doxepin• Trimipramine• Amoxapine• Protriptyline
BaldessariniBaldessarini. In: . In: Goodman & GilmanGoodman & Gilman’’s The Pharmacological Basis of Therapeuticss The Pharmacological Basis of Therapeutics. 10th ed. 2001.. 10th ed. 2001.
Amitriptyline
CHCH2CH2N(CH3)2
•HCl
Mechanism of Action

7/21/2016
13
Tricyclic Antidepressants: Positive Controlled Trials
Max et al. Max et al. Neurology.Neurology. 19871987;37:589;37:589--596596; Max et al. ; Max et al. N Engl J Med.N Engl J Med. 19921992;326:1250;326:1250--12561256; ; SindrupSindrup et al. et al. Br J Clin Br J Clin PharmacolPharmacol.. 19901990;30:683;30:683--691691; Max et al. ; Max et al. Pain. Pain. 19911991;45:3;45:3--99; Watson et al. ; Watson et al. Neurology.Neurology. 19821982;32:671;32:671--673673; Max ; Max et al. et al. Neurology.Neurology. 1988;1988;38:142738:1427--14321432; Graff; Graff--Radford et al. Radford et al. ClinClin J Pain. 2J Pain. 2000000;16:188;16:188--192192; ; KishoreKishore--Kumar et al. Kumar et al. ClinClin PharmacolPharmacol Ther.Ther. 19901990;47:305;47:305--312312; Raja et al. ; Raja et al. Neurology.Neurology. 20022002;59:1015;59:1015--10211021..
Pain relief1226Desipramine (12.5-250, PBO)Kishore-Kumar
Raja
Graff-Radford
Max
Watson
PHN
Max
Sindrup
Max
Max
Painful DPN
Study
Nortriptyline (10-160, PBO)
Amitriptyline (12.5-200, PBO)
Amitriptyline (12.5-150, PBO)
Amitriptyline (12.5, PBO)
Desipramine (12.5-250, PBO)
Desipramine (50 or 200, PBO), Clomipramine (50 or 75, PBO)
Desipramine (12.5-150, PBO), Amitriptyline (12.5-150, PBO)
Amitriptyline (25-150, PBO)
Agent (mg/d)
76
49
58
24
20
26
108
29
N
24
8
12
8
12
6
14
12
Weeks
Pain intensity, relief; cognitive function
Pain intensity
Pain relief
Pain relief
Pain relief
Neuropathy symptoms
Pain relief
Pain relief
Primary End Point
Tricyclic Antidepressants: Adverse Effects• Most common adverse effects
− Sedation− Anticholinergic effects
• Dry mouth• Blurred vision• Increased intraocular
pressure• Mydriasis (pupil dilation)• Constipation• Paralytic ileus• Urinary retention• Delayed micturition• Urinary tract dilation• Hyperpyrexia • Sinus tachycardia
• Often have unacceptable side effects in the elderly
Drug Facts & Comparisons. 2004; AGS Panel on Persistent Pain in Drug Facts & Comparisons. 2004; AGS Panel on Persistent Pain in Older Persons. Older Persons. J Am J Am GeriatrGeriatr Soc.Soc.20022002;50(suppl):S205;50(suppl):S205--S224S224..
!

7/21/2016
14
SE/Problems of TCAs
• adverse behavior effects
• anticholinergic
• seizures (highest w/ maprotiline)
• autonomic side effects
• cardiac side effects
• lag time = 3‐5 days
• troublesome SEs (addressed by SSRIs)
• narrow therapeutic index
Pharmacological tx PN w/ TCAs
Dose [mg] Amine Effects Sedation Anticholinergic
3 Amine TCA
Amitriptyline [Elavil] 25-300 NE > 5HT 3 3
Clomipramine [Anafranil] 25-300 5HT 2 3
Doxepin [Sinequan] 25-300 NE > 5HT 3 2
Imipramine [Tofranil] 25-300 NE > 5HT 2 2
Trimipramine [Surmontil] 25-300 NE > 5HT 3 3
2 Amine TCA
Amoxapine [Asendin] 50-600 NE 1 1
Desipramine [Norpramin] 25-300 NE 0.5 1
Maprotiline [Ludiomil] 25-225 NE 2 2
Protriptyline [Vivactil] 10-60 NE 0.5 2
Nortriptyline [Pamelor] 25-250 NE 1 1

7/21/2016
15
Serotonin Reuptake Inhibitors
Fluoxetine [Prozac] 5-80 5HT 0.5 0
Fluvoxamine [Luvox] 50-300 5HT 0.5 0
Paroxetine [Paxil] 10-50 5HT 0.5 0.5
Citalopram [Celexa] 10-60 5HT 0.5 0
Sertraline [Zoloft] 50-200 5HT 0.5 0
Escitalopram [Lexapro] 10-20 5HT 0.5 0
Atypical Antidepressants
Venlafaxine [Effexor] 25-375 5HT > NE 0 0
Duloxetine [Cymbalta] 20-120 5HT > NE 0 0
Bupropion [Wellbutrin] 100-450 NE, DA 0 0
Nefazodone [Serzone] 100-600 5HT > NE 3 0
Trazodone [Desyrel] 50-600 5HT > NE 3 0
Mirtazapine [Remeron] 15-45 NE [?] 3 0
MAOIs
Nardil (phenelzine) 45-90mg NE,DA,5-HT 1 0
Selegiline (Eldepryl) 5-20mg NE?,DA?,5-HT 0 0
Parnate (Tranylcypromine) 30-60mg NE,DA,5-HT 1 0
Anti-depressants, continued
TRAMADOL V TAPENTADOL

7/21/2016
16
Is Tapentadol (Nucynta®) a Glorified Tramadol?
Properties Tramadol Tapentadol
Mu BindingAffinity
6000x less than morphine
18x less than morphine
Metabolism Significant CYP450
Conjugation, O‐Glucuronide
Drug Interactions
See above See above
NeuroamineActivity
5‐HT / NE NE
Boglish P. Fudin J. As The Expert: Is Tapentadol a Glorified Tramadol? Practical Pain Management. 2016 Jan-Feb; 16(1): 19-20.

7/21/2016
17
Anticonvulsants• First generation
− Phenytoin− Phenobarbital− Primidone− Ethosuximide− Carbamazepine− Valproic acid
• Second generation− Gabapentin− Lamotrigine− Topiramate− Tiagabine− Levetiracetam− Oxcarbazepine− Zonisamide− Felbamate
Carbamazepine Gabapentin
McNamara. In: McNamara. In: Goodman & GilmanGoodman & Gilman’’s The Pharmacological Basis of Therapeutics. s The Pharmacological Basis of Therapeutics. 10th ed.10th ed. 2001; 2001; PhysiciansPhysicians’’ Desk ReferenceDesk Reference®®. 59th ed. 2005; Neurontin. 59th ed. 2005; Neurontin®® (gabapentin) [package insert]. New York, NY: (gabapentin) [package insert]. New York, NY: Pfizer Inc; 2004. Pfizer Inc; 2004.
N
CONH2 CH2CO2H
CH2NH2

7/21/2016
18
Anticonvulsants: Positive Controlled Trials
Wilton. Wilton. S S AfrAfr Med JMed J. 1974. 1974;48:869;48:869--872872; ; RullRull et al. et al. DiabetologiaDiabetologia. 1969. 1969;5:215;5:215--218218; ; BackonjaBackonja et al. et al. JAMA.JAMA.19981998;280:1831;280:1831--18361836; Eisenberg et al. ; Eisenberg et al. NeurologyNeurology. 2001. 2001;57:505;57:505--509509; Rice, ; Rice, MatonMaton. . Pain.Pain. 20012001;94:215;94:215--224224; ; Rowbotham et al. Rowbotham et al. JAMA.JAMA. 19981998;280:1837;280:1837--18421842..
Rowbotham
Rice
PHN
Eisenberg
Backonja
Rull
Wilton
Painful DPN
Study
Gabapentin (300-3600, PBO)
Gabapentin (1800 or 2400, PBO)
Lamotrigine (25-400, PBO)
Gabapentin (900-3600, PBO)
Carbamazepine (600, PBO)
Carbamazepine (600, PBO)
Agent (mg/d)
229
334
59
165
30
40
N
8
7
6
8
6
4
Weeks
Mean daily pain
Mean daily pain
Pain intensity
Daily pain severity
Neuropathy symptoms
Pain relief
Primary End Point
Anticonvulsants: Safety and Adverse Events
*Frequency not specified; †adverse events occurring in 5% of patients and with at least twice the incidence of placebo group; ‡postherpetic neuralgia; §adjunctive therapy in adults with epilepsy.
Physicians’ Desk ReferencePhysicians’ Desk Reference®®. 59th ed. 2005; Neurontin. 59th ed. 2005; Neurontin®® (gabapentin) [package insert]. New York, NY: (gabapentin) [package insert]. New York, NY: Pfizer Inc; 2004.Pfizer Inc; 2004.
Severe rash including Stevens-Johnson syndrome
NoneAplastic anemia and agranulocytosis
Black box warnings
VomitingDyspepsiaDizzinessAtaxiaSomnolenceIncoordinationInsomniaRashDiplopiaBlurred vision
DizzinessSomnolencePeripheral edema
DizzinessDrowsinessNauseaUnsteadinessVomiting
Most common adverse events
Not currently indicated
PHNTrigeminal neuralgiaNeuropathic pain indication
Lamotrigine†§Gabapentin†‡Carbamazepine*

7/21/2016
19
Pharmacology: Gabapentin &

7/21/2016
20
Gabapentin: Mechanism of Action
• Interacts with 2- subunit of voltage-gated Ca2+
channels• In animal models
− Prevents allodynia and hyperalgesia− Prevents pain-related responses in models of
neuropathic pain − Decreases pain-related responses after peripheral
inflammation• Relevance of these models to human pain is
not known
NeurontinNeurontin®® (gabapentin) [package insert]. New York, NY: Pfizer Inc; 2004.(gabapentin) [package insert]. New York, NY: Pfizer Inc; 2004.
Pharmacokinetic Properties of Gabapentin• Few drug-drug interactions• Not protein bound or hepatically metabolized• No blood level monitoring or liver function testing required
Dosage adjustment is recommended in patients with compromised reDosage adjustment is recommended in patients with compromised renal function and those undergoing nal function and those undergoing hemodialysis.hemodialysis. See full prescribing information for instructions on proper adjuSee full prescribing information for instructions on proper adjustments. stments. In general, dose selection for an elderly patient should be cautIn general, dose selection for an elderly patient should be cautious, usually starting at ious, usually starting at the lower end of the dosing range, reflecting the greater frequethe lower end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, ncy of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug thor cardiac function, and of concomitant disease or other drug therapy.erapy.
Half-life
5-7 hours
Protein Binding
<3% bound
Bioavailability Metabolism Excretion
Approximately60%
(300 mg TID)
Not appreciably metabolized
Renal
NeurontinNeurontin®® (gabapentin) [package insert]. New York, NY: Pfizer Inc; 2004.(gabapentin) [package insert]. New York, NY: Pfizer Inc; 2004.
!

7/21/2016
21
CO2H
Pregabalin: Predictable Response Versus Gabapentin
High BioavailabilityHigh BioavailabilityHigh BioavailabilityLinear PK ProfileLinear PK ProfileLinear PK Profile
Pregabalin Gabapentin
All doses
90%
900 mg, 60%
1200 mg, 47%
2400 mg, 34%
3600 mg, 33%
1800 mg Recommended
dose
LyricaLyrica®® (pregabalin) Capsules CV [package(pregabalin) Capsules CV [package insert]. New York, NY: Pfizer Inc; 2005insert]. New York, NY: Pfizer Inc; 2005; Neurontin; Neurontin®® (gabapentin) (gabapentin) [package insert]. New York, NY: Pfizer Inc; 2004; [package insert]. New York, NY: Pfizer Inc; 2004; WescheWesche, , BockbraderBockbrader. . Presented at: 24th Annual Scientific Presented at: 24th Annual Scientific Meeting of the American Pain Society; 2005.Meeting of the American Pain Society; 2005.
Dose (mg/d)Dose (mg/d)
0 600 1200 1800 2400 3000 3600 4200 48000
2
4
6
8
10
12
14
16
18
Pregabalin
GabapentinSte
ady
Sta
te C
Ste
ady
Sta
te C
ma
xm
ax
(( μμg/
mL)
g/m
L)

7/21/2016
22
Pharmacokinetics & Drug Interactions
Important Considerations when Prescribing RXs for Neuropathy
Terminology
• Inducer
• Inhibitor
• Substrate
• What is Genetic Polymorphism?

7/21/2016
23
CYP450 Nomenclature
• Cytochrome is designated CYP
• CYP (#) ‐ # identifying the enzyme family
• CYP (#) (A,C) ‐ Subfamily designation
• CYP (#) (A,C) (#) ‐ Individual enzyme(this is based on when enzyme was discovered
• EXAMPLES:
– CYP3A4, CYP2D6, CYP1A2

7/21/2016
24
Argoff CE. Clinical implications of opioid pharmacogenetics. Clin J Pain. 2010;26(1):S16‐S20.Belle DJ, Singh H. Genetic factors in drug metabolism. Am Fam Physician. 2008;77(11):1553‐1560.
Individual Response to Treatment
Pharmacogenetics
How the drug affects the
body
How the body alters the drug
Personalizing Medication with Pharmacogenetic
(PGT) Interpretation
48

7/21/2016
25
PGT Variability & Response
• General population has 40‐60% phenotype variability
• CYP450 enzymes most frequently involved– CYP2D6, CYP2C19, CYP2C9, CYP3A4, CYP1A2, CYP2E1
• Genetic differences impact 25% of all drugs
1. Cavallari LH, Limdi NA. Warfarin pharmacogenomics. Curr Opin Mol Ther. 2009 Jun;11(3):243-51. 2. Lynch T, Price A. The effect of cytochrome P450 metabolism on drug response, interactions and
adverse effects. Am Fam Physician. 2007; 76(3):391-6.3. Ma JD, Lee KC, Kuo GM. Clinical application of pharmacogenomics. J Pharm Pract. 2012
Aug;25(4):417–27.
Phenotypes and Variants
• Allele Variations
– wild:wild vs variant:wild vs wild:variant
• Poor Metabolizer (PM)
– DDDD → M
• Intermediate Metabolizer (IM)
– DDDD → MMm
• Extensive Metabolizer (EM)
– DDDD → MMM
• Ultra Rapid Metabolizer (UM)
– DDDD → MMMMmmm

7/21/2016
26
Opioid Chemistry and Cross‐sensitivity
51
Medication Metabolism
Phase of Metabolism
Key Enzymes InvolvedExamples: Opioid Medication Metabolized
Phase I Cytochrome P450 (CYP450)Examples: CYP2D6, CYP2C19, CYP2B6, CYP2C9, CYP3A4 & CYP3A5
Codeine, hydrocodone, oxycodone, tramadol, fentanyl, methadone, buprenorphine
Phase II Uridine 5'‐diphospho‐
glucuronosyltransferase (UDP‐glucuronosyltransferase, UGT)Examples: UGT2B7 & 2B15
Morphine, oxymorphone, hydromorphone, tapentadol
Smith HS. Opioid metabolism. Mayo Clin Proc. 2009;84(7):613‐624.

7/21/2016
27
http://www.arupconsult.com/assets/graphics/OpiatesAndOpiodMetabolism.jpg
Methadone Statistics(CDC 2012)
2% of prescriptions for opioid analgesics are for methadone
Methadone accounts for nearly 1 in 3 prescription opioid overdose deaths in the U.S., 6X times the number in 2009
http://www.cdc.gov/features/vitalsigns/methadoneoverdoses/

7/21/2016
28
Important Sub‐pops, Pharmacogenetics
Gerber JG et al. Stereoselective Metabolism of Methadone N‐Demethylation by Cytochrome P4502B6 and 2C19. CHIRALITY 2004;16:36‐44.
CYP3A4
R‐methadoneParent Drug
EDDP inactive metabolite
S: Sorrowing outcome. (Cardiotoxic effects, QT prolongation with potential of Torsade de pointes
CYP2B6
S‐methadoneParent Drug
EDDP inactive metabolite
R: Responsible for analgesia
55
CYP2B6 demonstrates selectively metabalizes S‐enantiomerPotential risk?
(+/‐) % Variation (Compared to Manual Calculation)1
‐33%
‐55%
+100%
+242%
VARIOUSOPIOIDS
FENTA
NYL
METH
ADONE
0%
RISKS:Underdose &Withdrawal
RISKS:Overdose & Death
1. Shaw K, Fudin J. Evaluation and Comparison of Online Equianalgesic Opioid Dose Conversion Calculators. Practical Pain Management. 2013 August; 13(7):61-66. PPM 2013

7/21/2016
29
Fudin J, Marcoux MD, Fudin JA. Mathematical Model For Methadone Conversion Examined. Practical Pain Management. Sept. 2012. 46-51.
Fudin J, Marcoux MD, Fudin JA. Mathematical Model For Methadone Conversion Examined. Practical Pain Management. Sept. 2012. 46-51.

7/21/2016
30
Met
hado
ne (
mg)
Morphine (mg)
Equianalgesic Dose of Morphine to Methadone
300mg Morphine = 60mg Methadone
302.5mg Morphine = 30mg Methadone
Fudin J, Marcoux MD, Fudin JA. Mathematical Model For Methadone Conversion Examined. Practical Pain Management. 2012 September; 12(8): 46-51.
Variability in Opioid Equivalence Survey
• Sept 13 thru Dec 31, 2013, 411 Respondents
• RPhs, MD/DOs, NPs, PAs
• Convert to Daily MEQ:
– Hydrocodone 80mg; Fentanyl 75mcg/hr; Methadone 40mg; Oxycodone 120mg; Hydromorphone 48mg
319
Rennick A, Atkinson TJ, Cimino NM, Strassels SA, McPherson ML, Fudin J. Variability in Opioid Equivalence Calculations. (2015) Pain Medicine. Early release version available at http://authorservices.wiley.com/bauthor/onlineLibraryTPS.asp?DOI=10.1111/pme.12920&ArticleID=4251185 (last accessed 9/25/2015).

7/21/2016
31
The most outrageous conversions
Rennick A, Atkinson TJ, Cimino NM, Strassels SA, McPherson ML, Fudin J. Variability in Opioid Equivalence Calculations. (2015) Pain Medicine. Early release version available at http://authorservices.wiley.com/bauthor/onlineLibraryTPS.asp?DOI=10.1111/pme.12920&ArticleID=4251185 (last accessed 9/25/2015).
Political Unrest & Recent Changes
• Tramadol is now Schedule IV
• Hydrocodone combos change to Schedule II
• VA Opioid Initiative & Opioid Consents
• Oh, so misunderstood!
– Zohydro ER® Blogs on PainDr.com
• ZOHYDRO: What weighs more – A pound of feathers or a pound of hydrocodone?
• Zohydro : Rogue State Politics & A Law Enforcement Perspective
• When Politicians Play Doctor
http://paindr.com/blog/

7/21/2016
32
http://www.cdc.gov/drugoverdose/pdf/calculating_total_daily_dose‐a.pdf
Recent CDC Guidelines:Who Should I Target for In‐Home Naloxone?
Opioid Monitoring• Urine Drug Testing (Presumptive v definitive testing)
• Serum testing
• Pharmacogenetics testing
• Opioid Consents
• PDMP monitoring
• Careful titration
• In‐home naloxone education
• etc.

7/21/2016
33
Conclusions
• Not all “pain medications” are efficacious for neuropathic pain
• Rational Polypharmacy is only rational if benefits outweigh risks
• Most prescribers are grossly under‐educated in pain therapeutics and lack the time to safely initiate and monitor patients
• Alternative pain treatment need to be considered alone and combined with appropriate therapies.