Chronic Obstructive Pulmonary Disease By: Chantel Berenyi 2-16-12.
30
Chronic Obstructive Pulmonary Disease By: Chantel Berenyi 2-16-12
-
Upload
julian-carsey -
Category
Documents
-
view
216 -
download
0
Transcript of Chronic Obstructive Pulmonary Disease By: Chantel Berenyi 2-16-12.
Chronic Obstructive Pulmonary Disease
By: Chantel Berenyi2-16-12

Why I chose COPD?
o Internship at McKay-Dee Hospital in Cardiac Rehab
o Career path
Drag picture to placeholder or click icon to add

Overview
What is COPD? Disease Prevalence Signs & Symptoms Diagnosis Tests & Evaluations Complications Treatment
Effects on exercise response
Effects of medications on exercise
Effects of training Exercise testing Exercise prescription Summary &
conclusions
COPD is defined as a chronic inflammatory disease of the
lung that is characterized by progressive and irreversible
airflow limitation
There are two main forms (most have a combination):
Chronic bronchitis: involves a long-term cough with
mucus
Inflammations of bronchial tubes
Irritations of cilia in bronchial-lining
Airways become clogged by debris
Heavy secretion of mucus
http://www.youtube.com/watch?v=o7mgL-xupRQ&feature=
related
What is COPD?

Emphysema: involves destruction of the lungs over
time
Alveoli lose elasticity (flabby balloon)
Alveoli over expand to compensate, causing the
to rupture and form cysts
CO2 cannot be expelled properly with damaged
alveoli
Stagnant air develops causing shortness of breath
http://www.youtube.com/watch?v=lmZZlkrSu5o
What is COPD?

Causes of CODP
SMOKING (leading cause) 80% of individuals with COPD
are current or former smokers
Environmental factors Secondhand smoke & pollution
Exposure to certain gases or fumes
Frequent use of cooking fire w/o ventilation
Lack of the protein “alpha-1 antitrypsin”

Projected to be the world’s third most important cause of
mortality by 2020
An estimated 24 million Americans have COPD
kills more than 120,000 Americans each year—that’s 1 death
every 4 minutes
An estimated 64 million people have COPD worldwide (2004)
More than 3 million people worldwide died of COPD in 2005
The disease now affects men and women almost equally
Total deaths from COPD are projected to increase by >30% in
the next 10 yrs
Prevalence

http://www.cdc.gov/copd/data.htm

Signs & Symptoms
Cough, with or without mucus
Fatigue Weak quadriceps muscles Low body weight Cachexia Many respiratory infections Shortness of breath
(dyspnea) that gets worse with mild activity
Trouble catching breath Wheezing

Best test for COPD- spirometry (FEV1/FVC) FEV1 (forced expiratory volume in one second) Involves the
amount of air which can be forcibly exhaled from lungs in the first
second of a forced exhalation
FVC (forced vital capacity) Involves blowing out as hard as possible
after taking the deepest breath possible into a small machine that
tests lung capacity
COPD= <.70
http://www.youtube.com/watch?v=kiQcbXK7f5c
Using a stethoscope- listen to lungs
X-ray and CT scans of lungs (but can still look normal)
Blood tests- measure amounts of oxygen and carbon dioxide
in blood
Diagnosing COPD

Spirometry
No cure for COPD Stop smoking- best way to slow down lung damage Medications:
Inhalers (bronchodilators) Ipratropium (Atrovent) Tiotropium (Spiriva) Salmeterol (Serevent) Formoterol (Foradil) Albuterol
Inhaled steroids- reduce lung inflammation Anti-inflammatory medication
Montelukast (Singulair) Roflimulast
Treatment for COPD
Severe cases or during flare-ups:
Steroids by mouth or through a vein
Bronchodilators through a nebulizer
Oxygen therapy
Assistance during breathing from a machine
Antibiotics (infections can make COPD worse)
Treatment for COPD
May need oxygen therapy at home or constantly in oxygen in blood is too low (< SpO₂ 80%)
Pulmonary rehabilitation Can teach you to breath differently allowing you
to stay active
Strengthen the lungs
Help maintain muscular strength in legs
Treatment for COPD
Exacerbations: increase in coughing, shortness of breath and/or amount or color of mucus coughed up
More frequent lung infections (pneumonia)
Increased risk of osteoporosis
Depression or anxiety (reduction in independence)
Problems with loosing too much weight
Heart failure (right side of heart)
A collapsed lung
Sleep problems (not enough oxygen)
Complications
Hyperinflation (crucial aspect): impeded exhalation, incomplete lung emptying, and air trapping
When exercising: Dynamic hyperinflation is superimposed on static hyperinflation
Reduction in inspiratory capacity
Smaller tidal volume
Increased elastic and threshold work of breathing
Dynamic hyperinflation is directly linked to breathlessness
Effects on Exercise Response

Exercise limited by cardiovascular factors: Deconditioned
Impaired left ventricle function (low SpO2)
Reduced pulmonary blood flow (low SpO2)
Lactic acid accumulation at low work rates
(peripheral muscle deconditioning)
Increased CO2 output (bicarbonate buffering)
Increased ventilator requirement
Effects on Exercise Response
Study conducted on the effects of walking on COPD patients Evaluated the cardiac and respiratory responses as well as
electrical activity of lower limb muscles during walking 6 min walk test Walking distance & speed were significantly lower in COPD patients However, COPD patients walked at a higher % of peak VO2 Surface EMG data taken on muscles were about same for both
Specifically the vastus lateralis & rectus femoris were more fatigued
CONCLUSIONs: 6 min walk test was performed at a relatively higher intensity in
patients with COPD compared with healthy controls Walking cause those with COPD to be more vulnerable to muscle
fatigue
Effects of Walking
Review of 18 controlled trials conducted to see if resistance training improves elements of performance of daily activities
Found effects favoring the addition of 12 weeks of progressive resistance training exercise to aerobic exercise for increases in LBM
Progressive Resistance Exercise showed no effect on oxygen uptake
Found an improvement in walking distance in field-walking tests
Found an improvement in timed stair-climbing performance
Found overall improvements in arm & leg muscle strength
Effects of Progressive Resistance Exercise

Conducted to see the hemodynamic adaption during high-intensity intermittent exercise in COPD patients
30 min exercise session, alternating a 4 min work set at first ventilatory threshold with a 1 min set at 90% of maximal tolerated power output
Found an increase in VO2, cardiac output & ventilation during first minutes of exercise, but remained STABLE thereafter
Pulmonary arterial pressure increased from rest and significantly decreased thereafter
Total pulmonary vascular resistance decreased from rest to the end of the test
CONCLUSION: High intensity 1 min bouts of work of intermittent work
exercise are well tolerated w/o pushing pulmonary arterial pressure too high
Effects of Intermittent Exercise

Beta2-adrenoceptor agonists: Relax bronchial smooth muscle & produce
bronchodilation
Methylxanthines: Produce bronchodilation & CNS stimulation
Thiazide diuretics: Control fluid retention
Glucocorticoids (steroids): Reduce inflammation & improve pulmonary function
Effects of Medications
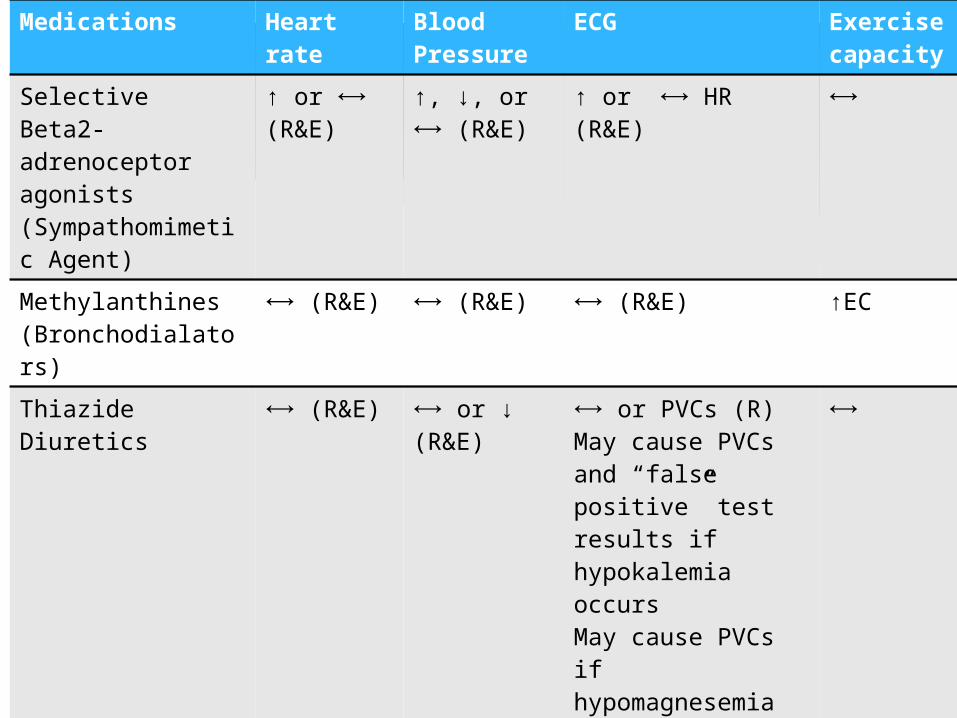
Medications Heart rate
Blood Pressure
ECG Exercise capacity
Selective Beta2-adrenoceptor agonists (Sympathomimetic Agent)
↑ or ⟷ (R&E)
↑, ↓, or ⟷ (R&E)
↑ or ⟷ HR (R&E) ⟷
Methylanthines (Bronchodialators)
⟷ (R&E) ⟷ (R&E) ⟷ (R&E) ↑EC
Thiazide Diuretics ⟷ (R&E) ⟷ or ↓ (R&E)
⟷ or PVCs (R) May cause PVCs and “false positive” test results if hypokalemia occursMay cause PVCs if hypomagnesemia occurs (E)
⟷
Glucocorticoids (steroids)
⟷ (R&E) ⟷ (R&E) ⟷ (R&E) ⟷
Antidepressants ↑ or ⟷ (R&E)
↓or ⟷ (R&E)
Variable (R)
Assessment of physiological function: Cardiopulmonary capacity Pulmonary function Determination of arterial blood gases/ arterial O2 saturation
(direct/indirect) Modifications:
Extended stages Smaller increments Slower progression Example: Naughton Protocol- only speed not grade increases
every 2 min instead of every 3 min 6 minute walk test
Popular for assessing functional exercise capacity Walking is usually best, COPD patients usually lack muscle
strength for stationary cycling & arm ergometry may cause increased dyspnea
Exercise Testing for COPD
Almost any level of physical activity can improve oxygen utilization, work capacity and anxiety
Benefits of exercise Cardiovascular reconditioning Reduced ventilatory requirement at a given work rate Improved ventilatory efficiency Reduced hyperinflation Desensitization to dyspnea Increased muscle strength Improved flexibility Improved body composition Better balance Enhanced body image
Effects of Exercise Training
Recommended mode of exercise: walking, cycling, swimming or conditioning exercises (tai chi)
enjoyable & improves ability to perform daily activities Oxygen administered if SpO2 < 88%
Goal is have SpO2 >90% during exercise Modifications to duration & frequency might be
necessary 5-10 min sessions vs. 20-30 min
6 week exercise program w/ group intervention is helpful
Rehabilitation exercises should be LIFELONG COPD patients are at risk for relapsing
Exercise Programming


COPD is a chronic inflammatory disease of the
lung that is characterized by progressive and
irreversible airflow limitation (no cure)
COPD is usually a combination of Bronchitis &
Emphysema
An estimated 24 million Americans have COPD
Smoking is the leading cause of COPD
Best test for COPD- spirometry
Conclusions

Inhalers, steroids & anti-inflammatory medication are
used to help off set symptoms
Hyperinflation is a crucial aspect of COPD
Progressive resistance & intermittent exercise can be
beneficial
Walking may improve endurance better than cycling
6 min walk test is most popular for testing COPD patients
Numerous benefits of exercise
Rehabilitation should be a lifelong process
Conclusions

Durstine, Larry J., Moore, Geoffrey E., Painter, Partricia L., & Roberts, Scott O. (2009). ACSM’s Exercise Management for Persons With Chronic Diseases and Disabilities. Champaign, IL: Human Kinetics.
LifeExtension (2011). Chronic Obstructive Pulmonary Disease, Emphysema and Chronic Bronchitis. Retrieved from http://www.lef.org/protocols/respiratory/copd_01.htm
Lonsdorfer-Wolf, E., Bougault, V., Doutreleau, S., Charloux, A., Lonsdorfer, J., & Oswald-Mammosser, M. (2004). Intermittent exercise test in chronic obstructive pulmonary disease patients: how do the pulmonary hemodynamics adapt?. Medicine & Science In Sports & Exercise, 36(12), 2032-2039.
Marquis, N., Debigare R, Bouyer L, et. al. 2009. Physiology of walking in patients with moderate to severe chronic obstructive pulmonary disease. Med. Sci. Sports Exerc. 41:1540-1548.
O'Shea, S., Taylor, N., & Paratz, J. (2009). Progressive resistance exercise improves muscle strength and may improve elements of performance of daily activities for people with COPD: a systematic review. Chest, 136(5), 1269-1283. doi:10.1378/chest.09-0029
The Credit Valley Hospital (2011). Screening for COPD. Retrieved from http://www.cvh-on.ca/podcasting/video.php
Thompson, Walter R., Gordon, Neil F., & Pescatello, Linda S. (2009) ACSM’s Guidelines for Exercise Testing and Prescription, 8th edition.
WebMD. (2011) COPD-Ongoing Concerns. Retrieved from http://www.webmd.com/lung/copd/tc/chronic-obstructive-pulmonary-disease-copd-ongoing-concerns
World Health Organization (2011). Chronic Obstructive Pulmonary Disease (COPD). Retrieved from http://www.who.int/mediacentre/factsheets/fs315/en/index.html
References

ANY QUESTIONS??