
Chronic Kidney Diseas2013 · 10/4/2013 1 Chronic Kidney Disease Evaluation, Classification, and...
26
10/4/2013 1 Chronic Kidney Disease Evaluation, Classification, and Management Ohnn Nahm, M.D. Samaritan Health Services CKD: Questions • What is the public health problem associated with CKD? • What is the working definition of CKD? • What are the stages of CKD? • What are the simplest and most accurate ways of estimating GFR and proteinuria? • What are the complications of CKD? • What are the goals for management of CKD? • When should I refer CKD patients to nephrologists? Goals • Learn the close association between CKD and CVD • Introduce the most up-to-date and accurate way of estimating GFR • Review the most important complications of CKD • Provide goals for the prevention and the management of CKD
Transcript of Chronic Kidney Diseas2013 · 10/4/2013 1 Chronic Kidney Disease Evaluation, Classification, and...

10/4/2013
1
Chronic Kidney DiseaseEvaluation, Classification, and Management
Ohnn Nahm, M.D.Samaritan Health Services
CKD: Questions
• What is the public health problem associated with CKD?• What is the working definition of CKD?• What are the stages of CKD?• What are the simplest and most accurate ways of
estimating GFR and proteinuria?• What are the complications of CKD?• What are the goals for management of CKD?• When should I refer CKD patients to nephrologists?
Goals• Learn the close association between CKD
and CVD• Introduce the most up-to-date and
accurate way of estimating GFR• Review the most important complications
of CKD• Provide goals for the prevention and the
management of CKD

10/4/2013
2
CKD: Questions
• What is the public health problem associated with CKD?
• What is the working definition of CKD?• What are the stages of CKD?• What are the simplest and most accurate ways of
estimating GFR and proteinuria?• What are complications of CKD?• What are the goals for prevention of CKD?• When should I refer CKD patients to nephrologists?
CKD: The ProblemThere is a rising incidence and prevalence of ESKD, with poor outcomes and high cost
• The number of ESKD patients is estimated to be 651,330in 2010
• The total cost of the ESKD Program was $35.3 billion in 2007
• Hemodialysis costs $72,000 per year per patient• The annual mortality of HD patients in the US is nearly
25%• Prevalence of CKD has increased from 10% in 1988-1994
to 13% in 1999-2004, corresponding to 26.3 million people in 2000
The Prevalence of ESKD: 651,330 ESKD Patients in 2010
United States Renal Data System (USRDS) Annual Report, 2008http://www.usrds.org

10/4/2013
3
1. Coresh J, Selvin E, Stevens L, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298(17):2038-2047. 2. U.S. Renal Data System. USRDS 2006 Annual Data Report: Atlas of End-Stage Renal Disease in the United States. Bethesda, MD:
National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2007.
Approximately 26 Million People in the U.S. Have Chronic Kidney Disease (CKD)
The CKD Epidemic
McCullough . Rev Cardiovasc Med. 2002;3:71-76.
Epidemic Drivers
� Accelerated atherosclerosis� Increased AMI mortality� Procedural complications� Incident diastolic CHF� Increased heart failure
mortality� Increased risk of arrhythmias
DiabetesHypertension
CKD
Obesity
Prevalence of ESRD in the U.S.
Primary Disease Numbers of patients with ESRD
Diabetes 100,892
Hypertension 72,961
Glomerulonephritis 52,229
Polycystic Kidney Disease 13,992
Other Known Causes 40,012
Unknown 23,997
USRDS 2000 Annual Data Report
10/4/2013
4
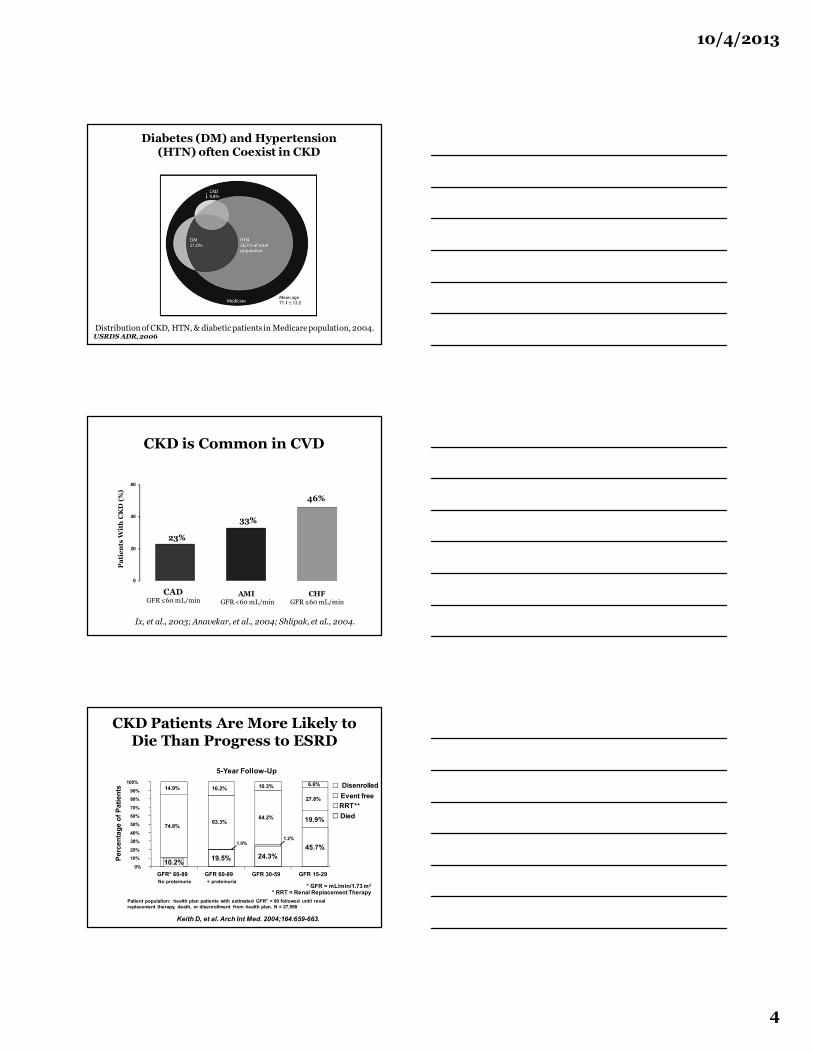
Diabetes (DM) and Hypertension (HTN) often Coexist in CKD
USRDS ADR, 2006Distribution of CKD, HTN, & diabetic patients in Medicare population, 2004.
CKD is Common in CVD
Ix, et al., 2003; Anavekar, et al., 2004; Shlipak, et al., 2004.
0
20
40
60
CADGFR ≤60 mL/min
AMI GFR <60 mL/min
CHFGFR ≤60 mL/min
23%
46%
33%
Pat
ien
ts W
ith
CK
D (
%)
CKD Patients Are More Likely to Die Than Progress to ESRD
Keith D, et al. Arch Int Med. 2004;164:659-663.
5-Year Follow-Up
45.7%24.3%19.5%10.2%
19.9%
1.2%1.0%
27.8%
64.2%63.3%
74.8%
10.3%16.2%14.9%6.6%
0%
10%20%
30%40%
50%60%70%
80%90%
100%
GFR* 60-89No proteinuria
GFR 60-89+ proteinuria
GFR 30-59 GFR 15-29
Perc
enta
ge o
f Pat
ient
s DisenrolledEvent freeRRT**Died
Patient population: health plan patients with estimated GFR* < 90 followed until renal replacement therapy, death, or disenrollment from health plan. N = 27,998
* GFR = mL/min/1.73 m2
* RRT = Renal Replacement Therapy

10/4/2013
5
Cardiovascular Mortality in the General Population (NCHS) and in ESKD Treated by
Dialysis (USRDS)
Association of eGFR with All-Cause and Cardiovascular Mortality
Chronic Kidney Disease Prognosis Consortium*Lancet 2010; 375: 2073–81
CKD: Questions
• What is the public health problem associated with CKD?• What is the working definition of CKD?• What are the stages of CKD?• What are the simplest and most accurate ways of
estimating GFR and proteinuria?• What are complications of CKD?• What are goals for prevention of CKD?• When should I refer CKD patients to nephrologists?

10/4/2013
6
K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease
National Kidney Foundation 2002
• Definition and classification of the stages of chronic kidney disease (CKD)
• Evaluation of laboratory measurements for the clinical assessment of CKD
• Association of the level of kidney function with complications of CKD
• Stratification of the risk for the risk of kidney function and development of cardiovascular disease
Definition and Stages of CKD
• The presence of CKD should be establishedbased on kidney damage and level of kidney function(GFR) irrespective of diagnosis
• Among patients with CKD, the stage of disease should be assigned based on the levels of kidney functionirrespective of diagnosis
K/DOQI CKD Classification, 2002
Definition of CKD1. Kidney damage for ≥ 3 months, with or without
decreased GFR, as manifested by either pathologic abnormalities or markers of kidney disease, including abnormalities in the blood or urine, or abnormalities in imaging tests
2. GFR less than 60 ml/min/1.73 m2 for ≥ 3 months, with or without kidney damage
* The principal marker of kidney damage is persistent proteinuria ( urinary albumin excretion > 30 mg/day )

10/4/2013
7
Definition of Kidney Failure vs. End Stage Renal Disease (ESRD)
• Kidney failure (based primarily on disease severity)GFR < 15 ml/min/1.73 m2 or treated by dialysisDoes not include kidney transplant recipients unless they meet the criteria above
• ESRD (based primarily on decision for treatment)Administrative term in U.S., including satisfying conditions for coverage by Medicare ESRD Program Treatment by dialysis or kidney transplant within 3 yearsDoes not include patients with uremia who are not treated
CKD: ClassificationK/DOQI, 2002
Stage DescriptionGFR
(ml/min/1.73 m2)
1 Kidney damage with normal or ↑ GFR ≥ 90
2Kidney damage with mild
↓ GFR60-89
3 Moderate ↓ GFR 30-59
4Severe ↓ GFR
15-29
5 Kidney failure < 15 or Dialysis
10/4/2013
8
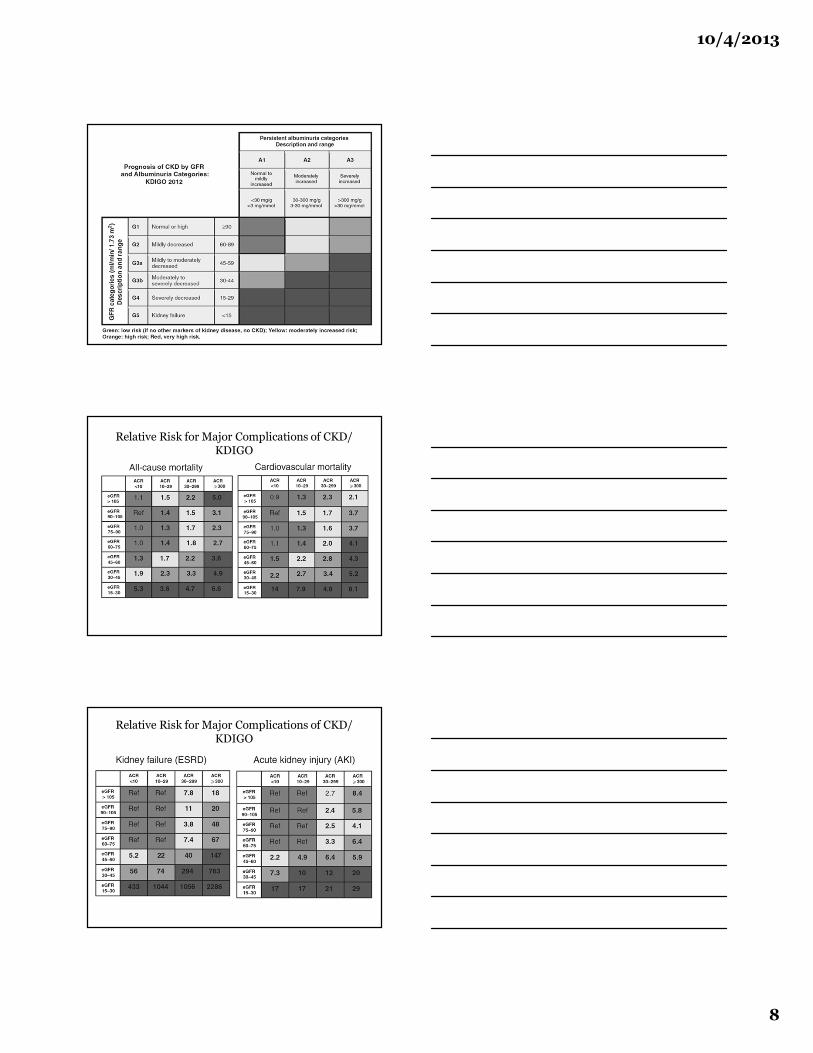
Relative Risk for Major Complications of CKD/ KDIGO
Relative Risk for Major Complications of CKD/ KDIGO

10/4/2013
9
CKD: Questions
• What is the public health problem associated with CKD?• What is the working definition of CKD?• What are the stages of CKD?• What are the simplest and most accurate ways
of estimating GFR and proteinuria?• What are complications of CKD?• What are goals for prevention of CKD?• When should I refer CKD patients to nephrologists?
Estimation of GFR
• GFR is the best overall index of the level of kidney function
• GFR has been estimated from creatinine clearance, serum creatinine concentration, and prediction equations
• The following equations provide useful estimates of GFR:In children: Schwartz and Counahan-Barrat equationsIn adults: CKD-EPI, MDRD Study, Cystatin C-EPI, and Cockcroft-Gault equations
GFR: Definition“Volume of plasma per unit time that is cleared of
substance by renal excretion”

10/4/2013
10
Factors Affecting Serum Creatinine Concentration
Condition Effect Mechanism/Comment
Kidney Disease Increase Decreased GFR
Reduced muscle mass Decrease Reduced creatinine generation: women, elderly, malnutrition
Ingestion of cooked meat
Increase Transient increase in creatinine generation
Trimethoprim, cimetidine
Increase Inhibition of tubular secretion
Flucytosine, some cephalosporins
Increase Positive interference with assay
Ketoacidosis Increase Positive interference with assay
The Perils of Using Serum Creatinine to “Guess” Level of Kidney Function
Never use the serum creatinine concentration alone to assess the level of kidney function!

10/4/2013
11
Estimation of GFR: Prediction Equations
• MDRD Equation (abbreviated)
GFR (mL/min per 1.73 m2) = 186 × (SCr)-1.154 × (Age)-0.203
× (0.742 if female) × (1.210 if African-American)Levy et al., Annals of Internal Medicine. Vol. 130, 1999
• CKD-EPI EquationGFR = 141 x [min(Scr/κ),1)α x max(Scr/κ),1)-1.209 ] x Age-0.993 x 1.018
[if female] x [1.157 if Black]Levey et al Annals of Internal Medicine. 2009; 150: 604 612
• Cockcroft-Gault Equation(140-Age) × Weight
72 × SCr× (0.85 if female)CCr =
Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI)
• Goal: Develop and validate improved estimating equations
– Diverse dataset of individuals with & without kidney disease, and across range of measured GFR and age
– Additional surrogates for non-GFR determinants
• Inclusion criteria: study population >250; availability of serum samples; quality control data
• Final studies– Category 1: 10 studies; equation development (random selection of
2/3 of data) and internal validation (remaining 1/3 of data) – Category 2: 16 studies; external validation
Levey et al Ann Int Med 2009; 150: 604 612
0
2
4
6
8
10
12
Per
cent
Estimated GFR (ml/min/1.73 m2)
MDRDCKD-EPI
60-8952.2%35.4%
15-290.4%0.4%
30-597.8%6.3%
90-11933.8%48.3%
150-1790.5%0.0%
120-1495.2%9.5%
180+0.1%0.0%
Comparison of distribution of estimated GFR for MDRD Study and CKD-EPI equations (NHANES 1999-2004)
Levey et al Ann Int Med 2009; 150: 604 612

10/4/2013
12
Estimation of GFR: Prediction Equations: Summary
• MDRD Study equation is less accurate in the population with normal or near normal GFR
• CKD-EPI equation is as accurate as MDRD study equation among individuals with GFR less than 60 ml/min and more accurate in those with higher GFR
• CKD-EPI equation results in a lower prevalence of CKD and more accurate risk prediction for adverse outcomes compared to the MDRD Study equation
• CKD-EPI equation will most likely replace MDRD Study equation in the future.
Among adults, the CKD-EPI Equation provides the most accurate estimate of GFR. It is easy to implement and a GFR calculator is available online.
http://www.kidney.org/professionals/kdoqi/gfr_calculator.cfm
Proteinuria is bad!

10/4/2013
13
Proteinuria and Relative Risk for Cardiovascular Disease
Association of of Albuminuria with All-Cause and Cardiovascular Mortality
Chronic Kidney Disease Prognosis Consortium*Lancet 2010; 375: 2073–81
Annual CV Death Rates in Diabetic Patients with Various Stages of CKD
Urinary Albumin Excretion (mg/day)
Annual Death Rate (%)
< 150 mg 0.7
150-300 mg 2.0
> 300 mg 3.5
> 300 mg and renal replacement therapy
12.1
The United Kingdom Prospective Diabetes Study (UKPDS 64).Kidney International 63:225-232, 2003
10/4/2013
14
Assessment of Proteinuria
• Normal Individuals excrete small amount of protein in their urine
• Persistently increased protein excretion is usually a marker for kidney damage
• Types of protein excreted depends on kidney diseaseAlbumin: diabetes, hypertension, glomerular diseaseLow molecular weight globulins: tubulointerstitial disease
Proteinuria: Terminology
• AlbuminuriaIncreased excretion of albumin
• MicroalbuminuriaIncreased albumin excretion below level of detection by tests for total protein
• ProteinuriaIncreased urinary excretion of protein including albumin and other specific proteins
Proteinuria: Measurement
• 24-hour urine collection
• Urine dipstick
• Spot urine: protein-to-creatinine ratio, albumin-to-creatinine ratio
10/4/2013
15
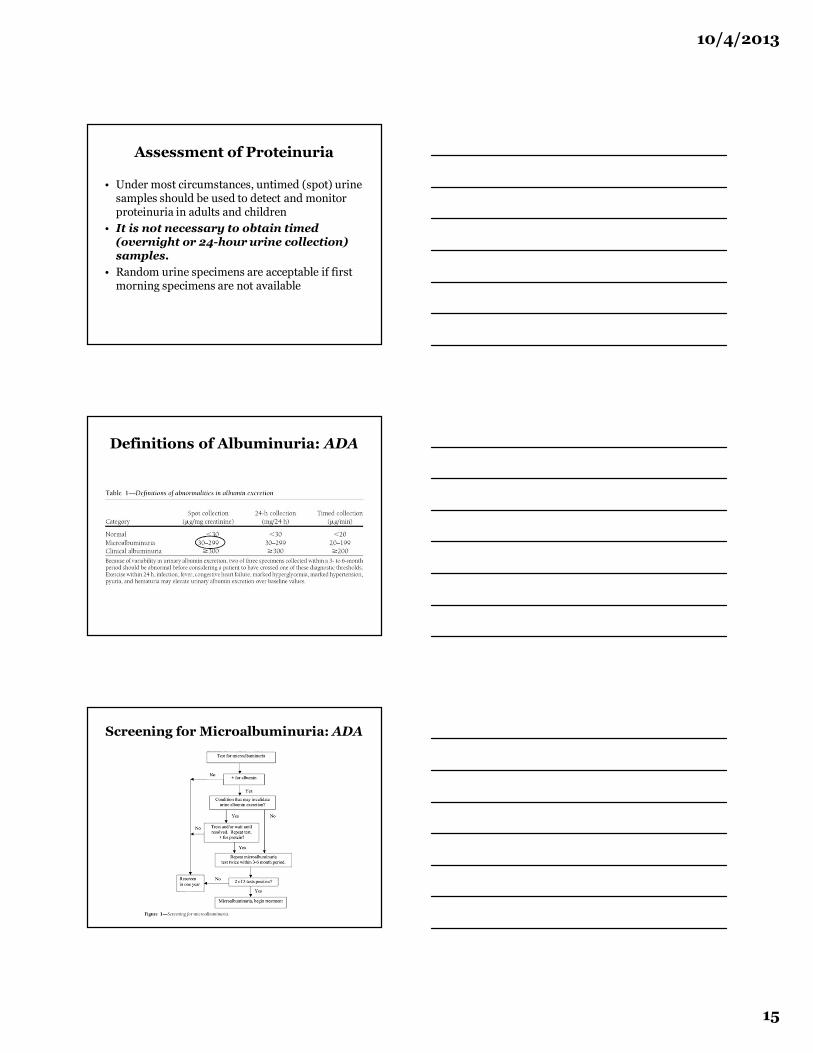
Assessment of Proteinuria
• Under most circumstances, untimed (spot) urine samples should be used to detect and monitor proteinuria in adults and children
• It is not necessary to obtain timed (overnight or 24-hour urine collection) samples.
• Random urine specimens are acceptable if first morning specimens are not available
Definitions of Albuminuria: ADA
Screening for Microalbuminuria: ADA
10/4/2013
16
Screening for Albuminuria in Diabetes: ADA
• Screening for microalbuminuria should be performed at diagnosis in patients with type 2 diabetes
• Screening for microalbuminuria should begin after 5 years’ disease duration in patients with type 1 diabetes
• After the initial screening and in the absence of previously demonstrated microalbuminuria, a test for the presence of microalbumin should be performed annually
“All patients with increased risk for developing CKD should undergo testing to identify markers of kidney disease and to estimate GFR.”
“JNC7 and ADA guidelines recommend testing adults with hypertension and diabetes for GFR and albuminuria.”
Markers of CKD Other Than Proteinuria
Abnormalities in urine sediments• Red blood cells• White blood cells• CastsAbnormalities of kidney imaging studies• Arterial stenosis• Asymmetry• Cysts• Obstruction• Size• Scarring

10/4/2013
17
Management of CKD
• Treatment of reversible causes of kidney dysfunction
• Preventing or slowing the progression of kidney disease
• Preventing cardiovascular disease• Treatment of the complications of kidney
dysfunction• Identification of adequate preparation of the
patient in whom kidney replacement therapy will be required
CKD: Questions
• What is the public health problem associated with CKD?• What is the working definition of CKD?• What are the stages of CKD?• What are the simplest and most accurate ways of
estimating GFR and proteinuria?• What are complications of CKD?• What are goals for prevention of CKD?• When should I refer CKD patients to nephrologists?
Association of Complication with CKD in Adults
• Hypertension• Anemia• Metabolic acidosis and hyperkalemia• CKD-Mineral Bone Disorder (MBD)• Neurological changes• Functioning and well-being• Malnutrition
10/4/2013
18
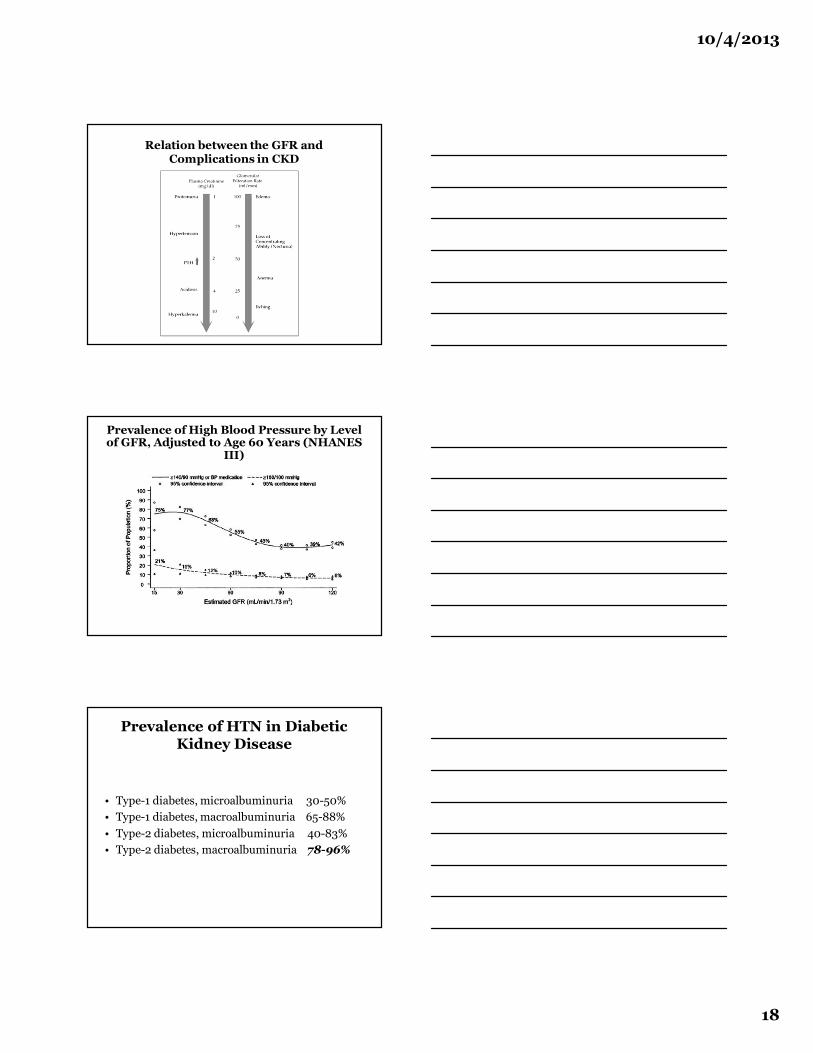
Relation between the GFR and Complications in CKD
Prevalence of High Blood Pressure by Level of GFR, Adjusted to Age 60 Years (NHANES
III)
Prevalence of HTN in Diabetic Kidney Disease
• Type-1 diabetes, microalbuminuria 30-50%• Type-1 diabetes, macroalbuminuria 65-88%• Type-2 diabetes, microalbuminuria 40-83%• Type-2 diabetes, macroalbuminuria 78-96%
10/4/2013
19
Association of CKD and Hypertension
• High blood pressure is both a cause and complication of CKD, develops early and is associated with adverse outcomes:Loss of kidney functionDevelopment of cardiovascular disease
• Blood pressure should be closely monitored and treated with specific agents and to target BP levels
Pathogenic Mechanisms of HTN in CKD
• Pre-existing essential hypertension• Extracellular fluid volume expansion• Renin-angiotensin aldosterone system activation• Increased sympathetic activity• Alteration of endothelin-derived factors• Erythropoietin administration• Increased PTH secretion• Renal vascular disease and renal artery stenosis• Cyclosporine, tacrolimus, and corticosteroid
Principles of Hypertension Treatment in CKD
Optimal blood pressure is the single most important measure to prevent progression of chronic kidney disease
Treat BP < 130/80 mmHg in patients with diabetes or CKD associated with significant proteinuria.
Treat BP < 140/90 mmHg in patients with diabetes and CKD without significant proteinuria
There was no benefit of aggressive blood pressure control in non-proteinuric CKDAppel LJ, et al "Intensive blood-pressure control in hypertensive chronic kidney disease" N Engl J Med 2010; 363: 918-29.

10/4/2013
20
Other Strategies for Renal Protection
• Protein restriction• Statin therapy• Smoking cessation• Treatment of chronic metabolic acidosis
Strategy for the Prevention of Diabetic Nephropathy
• Blood pressure control: < 130/80 mmHg• Microalbuminuria: Either an ACE inhibitor or ARB can
be used in patients with microalbuminria with or without hypertension
• Proteinuria: Treatment may be aimed at reducing proteinuria by at least 30-40%
• Dual therapy: Increased risk of AKI, hyperkalemia, and increased mortality in ONTARGET trial. Do NOT use combination therapy with ACE inhibitors and ARBs!
Adjusted Prevalence in Adults of Low Hemoglobin by GFR (NHANES III)
10/4/2013
21
Erythropoietin in CKD Patients
• Erythropoietin deficiency is the primary cause of anemia in chronic kidney disease
• Anemia in CKD is associated with fatigue, depression, dyspnea, and LVH.
• EPO should be given to the CKD patients with severe symptomatic anemia (HGB less than 9 g/dL)
• The target hemoglobin concentration is 9 to 11 g/dL.
There is increased risk of adverse cardiovascular outcome and cancer death if HGB is targeted above 13 g/dLCHOIR, CREAT, TREAT trial
Chronic Kidney Disease-Mineral Bone Disorder: CKD-MBD
A systemic disorder of mineral and bone metabolism due to CKD manifested by one or more of the following:
• Abnormalities of calcium, phosphorous, or vitamin D metabolism.
• Abnormalities in bone turnover, mineralization, volume, and linear growth, or strength
• Vascular and other soft tissue calcification
Chronic Kidney Disease-Mineral Bone Disorder: CKD-MBD
• Bone disease and disorders of calcium, phosphorous, and vitamin D metabolism develop during the early course of chronic kidney disease
• Patients with GFR<60 mL/min/1.73 m2 should be evaluated for bone disease and disorders of calcium and phosphorous
• PTH levels are elevated in patients with decreased GFR and likely the earliest marker of abnormal bone mineral metabolism

10/4/2013
22
K/DOQI Target Labs for Bone and Mineral Metabolism in CKD Stages III and IV*
Parameter RecommendationiPTH level for Stage 3 (opinion-based) 35-70 pg/mL
iPTH level for Stage 4 (opinion-based) 70-110 pg/mL
Calcium level (corrected for serum albumin) 8.4-10.2 mg/dL
Phosphorus level 2.7-4.6 mg/dL
Calcium-phosphorus product
25-hydroxy vitamin D
<55 mg2/dL2
>30 ng/mL
NKF. Am J Kidney Dis. 2003;42(4 suppl 3):S1-S201; Zisman AL et al. Am J Nephrol.2007;27:36-43.
*Currently undergoing revision by KDIGO
CKD: Questions
• What is the public health problem associated with CKD?• What is the working definition of CKD?• What are the stages of CKD?• What are the simplest and most accurate ways of
estimating GFR and proteinuria?• What are complications of CKD?• What are goals for prevention of CKD?• When should I refer CKD patients to nephrologists?
Early Treatment Can Make a Difference
100
10
0
No Treatment
Current Treatment
Early Treatment
4 7 9 11
Time (years)
Kidney FailureGFR
(m
L/m
in/
1.7
32)

10/4/2013
23
Treatments to Slow the Progression of CKD “The Earlier, the Better”
Diabetic Kidney Disease
Nondiabetic Kidney Disease
Renal Disease in Transplant
Strict glycemic control
Yes NA NA
ACE-inhibitors or ARBs
Yes Yes (greater effect if proteinuria present)
Yes
Strict blood pressure control
Yes< 130/80 mmHg
Yes< 140/90 mmHg
Not tested
There is no specific level of GFR at which ACE inhibitors or ARBs should be discontinued
Prevention of Progression of diabetic kidney disease
• Achieve normotension with therapy regimen including ACE-inhibitor or an ARB (130/80 mmHg)
• Salt restriction ( <2 g/d), recommended protein intake (0.8 to 1.0 g/kg/day)
• Tight glycemic control (target HbA1C < 7.0%)• Cessation of smoking• Control of dyslipidemia (target LDL < 100
mg/dL)• Avoidance of nephrotoxic medications
Frequent Causes of Acute Decline in GFR in CKD
• Volume depletion• Intravenous contrast• Selected antimicrobial agents• Nonsteroidal anti-inflammatory agents,
including COX-2 inhibitors• ACE inhibitors and ARBs• Cyclosporine and FK506• Obstruction

10/4/2013
24
CKD: Questions
• What is the public health problem associated with CKD and diabetic nephropathy?
• What is the working definition of CKD?• What are the stages of CKD?• What are the simplest and most accurate ways of
estimating GFR and proteinuria?• What are complications of CKD?• What are goals for prevention of CKD and diabetic
nephropathy?• When should I refer CKD patients to
nephrologists?
The Potential Benefits of Early Referral to Nephrologists
• Timely placement of appropriate dialysis access: preparation of access placement should be initiated at GFR less than 30 mL/min 1.73 m2
• Earlier initiation of dialysis• Lower morbidity and improved rehabilitation• Less frequent and shorter hospitalization• Lower cost• Improved survival
Late Referral to a Nephrologist is:
• A very common problem in the US• Associated with a greater prevalence of poor
outcome predictors, including anemia, hypoalbuminemia, and hyperphosphatemia
• Associated with suboptimal care in pre-ESKD period, especially underuse of erythropoietin and lack of AV access at ESKD start
• Contribute significantly to increased mortality independent of other known mortality predictors
10/4/2013
25
Jungers P, Zingraff J, Albouze G, et al: Late referral to maintenance dialysis: detrimental consequences. Nephrol Dial Transpl 8: 1089-1093, 1993., Hakim RM, Lazarus JM: Initiation of Dialysis. J Am Soc Nephrol 6: 1319-1328, 1995.
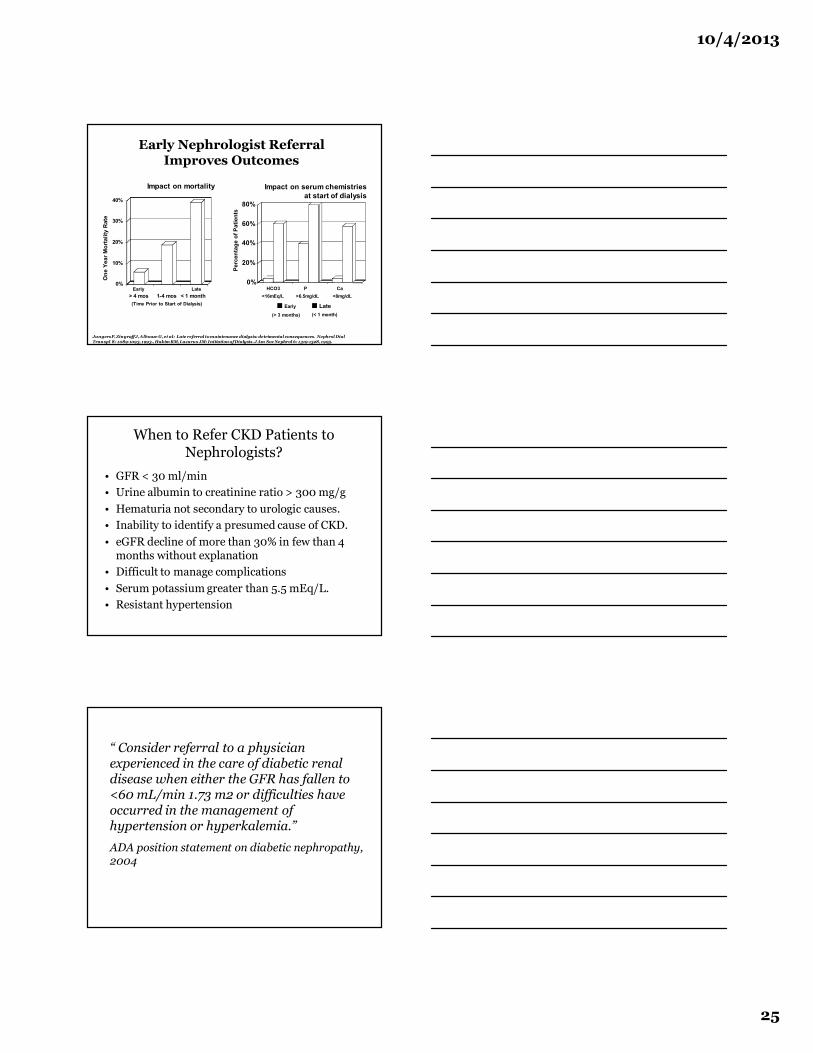
Early Nephrologist Referral Improves Outcomes
Impact on mortality
0%
10%
20%
30%
40%
One
Yea
r Mor
talit
y R
ate
< 1 month1-4 mos> 4 mos(Time Prior to Start of Dialysis)
0%
20%
40%
60%
80%
Perc
enta
ge o
f Pat
ient
s
HCO3 <16mEq/L
P >6.5mg/dL
Ca <8mg/dL
Impact on serum chemistries at start of dialysis
¢ Early ¢ Late
Early Late
(> 3 months) (< 1 month)
When to Refer CKD Patients to Nephrologists?
• GFR < 30 ml/min• Urine albumin to creatinine ratio > 300 mg/g• Hematuria not secondary to urologic causes. • Inability to identify a presumed cause of CKD. • eGFR decline of more than 30% in few than 4
months without explanation• Difficult to manage complications• Serum potassium greater than 5.5 mEq/L. • Resistant hypertension
“ Consider referral to a physician experienced in the care of diabetic renal disease when either the GFR has fallen to <60 mL/min 1.73 m2 or difficulties have occurred in the management of hypertension or hyperkalemia.”
ADA position statement on diabetic nephropathy, 2004

10/4/2013
26
“Patients with CKD should be referred to a specialist for consultation and co-management if the patient’s personal physician can not adequately evaluate and treat the patient. A nephrologist should participate in the care of patients with a GFR less than 30 mL/min 1.73 m2.”
NKF CKD guidelines, 2002










