Chronic Invasive Aspergillosis in Apparently Immunocompetent Hosts
11
723 Chronic Invasive Aspergillosis in Apparently Immunocompetent Hosts M. Karim, M. Alam, A. A. Shah, R. Ahmed, From the Department of Medicine (Infectious Diseases Services) and the and H. Sheikh Departments of Microbiology, Neurosurgery, and Pathology, Aga Khan University Hospital, Karachi, Pakistan Seventeen cases of invasive aspergillosis occurring since 1987 in apparently immunologically normal hosts have been reviewed: 9 of invasive sinus aspergillosis, 2 of isolated brain abscesses, 3 of pneumonia (1 in a patient who developed mediastinitis), 2 of lymph node aspergillosis, and 1 of osteomyelitis of the foot. Two of the 9 patients with sinus aspergillosis died; the rest were stable up to March 1993. They responded initially to combined surgical and medical therapy. Both patients with brain abscesses survived following surgery, but one had neurological sequelae. Both patients with pneumonia were well following therapy with amphotericin B; one also received itraconazole. The patient with mediastinitis died, but this disease was diagnosed late. The patients with lymph node involvement were lost to follow-up, as was the patient with osteomyelitis. Invasive aspergillosis may be common in Pakistan. Greater awareness would allow earlier diagnosis and therapy, thereby improving the outcome. Aspergillus species are ubiquitous fungi usually acquired by inhalation of airborne spores. Host factors are important in pre- venting disease. Invasive aspergillosis in patients with granulo- cyte dysfunction and after corticosteroid, antibiotic, or cancer chemotherapy is well documented. Both neutrophils and macro- phages are important in host defense: macrophages are effective against conidia, and neutrophils against hyphae [1-4]. Most patients with invasive aspergillosis have dysfunction of one or both of these systems. Recently, several reports of invasive aspergillosis in patients without apparent defects in their immune system have been published [5-11] . We therefore reviewed all cases of invasive fungal disease diagnosed histo- pathologically at the Aga Khan University Hospital (Karachi, Pakistan). Those patients with culture-proven aspergillosis who were admitted since 1987 and had no apparent immune dys- function are described here in detail (table 1). Materials and Methods Case Findings and Criteria for Inclusion The Aga Khan University Hospital is a tertiary care facility to which patients are referred from all over Pakistan. The records regarding all tissue-invasive fungal infections detected in histopathology specimens submitted to the Aga Khan Labo- ratory since 1987 were reviewed. Culture-positive cases (see Mycology section) were identified, and the medical records of those admitted to the hospital were obtained for a retrospective Received 6 June 1996; revised 27 September 1996. Reprints or correspondence: (present address): Dr. Michele Karim, Rockefel- ler University, Bronx Building, 1230 York Avenue, New York, New York 10021 Clinical Infectious Diseases 1997; 24:723-33 © 1997 by The University of Chicago. All rights reserved. 1058-4838/97/2404-0025$02.00 analysis of invasive fungal infection in apparently immuno- competent hosts (table 1). Seventeen cases were identified: 9 of invasive sinusitis, 2 of lymph node involvement, 3 of pulmonary involvement (1 in a patient with subsequently diagnosed granulomatous mediastin- itis), 2 of brain abscesses, and 1 of osteomyelitis. All patients with invasive aspergillosis had been seen by an infectious dis- ease specialist during their hospitalization. Patients were reported as presumptively immunocompetent if they had not received steroids or cytotoxic medication and had no diagnosed condition associated with immunosuppres- sion, i.e., cancer, HIV infection, or congenital immunodefi- ciency, as was ascertained from their records. Among patients available for follow-up, none had developed HIV-related dis- ease or a malignancy until March 1993. HIV testing by ELISA and phagocytic function tests were not performed for all pa- tients because of the cost involved. Mycology All specimens were streaked onto the surface of two Sabou- raud dextrose agar plates (Oxoid, Basingstoke, U.K.), a plate of Sabouraud chloramphenicol agar (containing 0.5 g of chlor- amphenicol per liter), and a Mycosel agar plate (Becton Dickin- son, Cockeysville, MD) containing cycloheximide (Actidione; Upjohn, Kalamazoo, MI). AFPA agar (Aspergillus flavus/ Aspergillus parasiticus agar, Oxoid code CM 731, Oxoid) was used to observe characteristic pigment production to aid in distinguishing A. flavus from other species of Aspergillus. All plates were incubated for up to 4 weeks [13]. Results Characteristics of Patients As shown in table 1, the majority of patients in this series were young (mean age, 25.8 years; range, 8-47 years); nine Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023 by guest on 16 February 2018
Transcript of Chronic Invasive Aspergillosis in Apparently Immunocompetent Hosts

723
Chronic Invasive Aspergillosis in Apparently Immunocompetent Hosts
M. Karim, M. Alam, A. A. Shah, R. Ahmed, From the Department of Medicine (Infectious Diseases Services) and the
and H. Sheikh
Departments of Microbiology, Neurosurgery, and Pathology, Aga KhanUniversity Hospital, Karachi, Pakistan
Seventeen cases of invasive aspergillosis occurring since 1987 in apparently immunologicallynormal hosts have been reviewed: 9 of invasive sinus aspergillosis, 2 of isolated brain abscesses, 3of pneumonia (1 in a patient who developed mediastinitis), 2 of lymph node aspergillosis, and 1 ofosteomyelitis of the foot. Two of the 9 patients with sinus aspergillosis died; the rest were stable upto March 1993. They responded initially to combined surgical and medical therapy. Both patientswith brain abscesses survived following surgery, but one had neurological sequelae. Both patientswith pneumonia were well following therapy with amphotericin B; one also received itraconazole.The patient with mediastinitis died, but this disease was diagnosed late. The patients with lymphnode involvement were lost to follow-up, as was the patient with osteomyelitis. Invasive aspergillosismay be common in Pakistan. Greater awareness would allow earlier diagnosis and therapy, therebyimproving the outcome.
Aspergillus species are ubiquitous fungi usually acquired byinhalation of airborne spores. Host factors are important in pre-venting disease. Invasive aspergillosis in patients with granulo-cyte dysfunction and after corticosteroid, antibiotic, or cancerchemotherapy is well documented. Both neutrophils and macro-phages are important in host defense: macrophages are effectiveagainst conidia, and neutrophils against hyphae [1-4].
Most patients with invasive aspergillosis have dysfunctionof one or both of these systems. Recently, several reports ofinvasive aspergillosis in patients without apparent defects intheir immune system have been published [5-11] . We thereforereviewed all cases of invasive fungal disease diagnosed histo-pathologically at the Aga Khan University Hospital (Karachi,Pakistan). Those patients with culture-proven aspergillosis whowere admitted since 1987 and had no apparent immune dys-function are described here in detail (table 1).
Materials and Methods
Case Findings and Criteria for Inclusion
The Aga Khan University Hospital is a tertiary care facilityto which patients are referred from all over Pakistan. Therecords regarding all tissue-invasive fungal infections detectedin histopathology specimens submitted to the Aga Khan Labo-ratory since 1987 were reviewed. Culture-positive cases (seeMycology section) were identified, and the medical records ofthose admitted to the hospital were obtained for a retrospective
Received 6 June 1996; revised 27 September 1996.Reprints or correspondence: (present address): Dr. Michele Karim, Rockefel-
ler University, Bronx Building, 1230 York Avenue, New York, New York10021
Clinical Infectious Diseases 1997; 24:723-33© 1997 by The University of Chicago. All rights reserved.1058-4838/97/2404-0025$02.00
analysis of invasive fungal infection in apparently immuno-competent hosts (table 1).
Seventeen cases were identified: 9 of invasive sinusitis, 2 oflymph node involvement, 3 of pulmonary involvement (1 in apatient with subsequently diagnosed granulomatous mediastin-itis), 2 of brain abscesses, and 1 of osteomyelitis. All patientswith invasive aspergillosis had been seen by an infectious dis-ease specialist during their hospitalization.
Patients were reported as presumptively immunocompetentif they had not received steroids or cytotoxic medication andhad no diagnosed condition associated with immunosuppres-sion, i.e., cancer, HIV infection, or congenital immunodefi-ciency, as was ascertained from their records. Among patientsavailable for follow-up, none had developed HIV-related dis-ease or a malignancy until March 1993. HIV testing by ELISAand phagocytic function tests were not performed for all pa-tients because of the cost involved.
Mycology
All specimens were streaked onto the surface of two Sabou-raud dextrose agar plates (Oxoid, Basingstoke, U.K.), a plateof Sabouraud chloramphenicol agar (containing 0.5 g of chlor-amphenicol per liter), and a Mycosel agar plate (Becton Dickin-son, Cockeysville, MD) containing cycloheximide (Actidione;Upjohn, Kalamazoo, MI). AFPA agar (Aspergillus flavus/Aspergillus parasiticus agar, Oxoid code CM 731, Oxoid) wasused to observe characteristic pigment production to aid indistinguishing A. flavus from other species of Aspergillus. Allplates were incubated for up to 4 weeks [13].
Results
Characteristics of Patients
As shown in table 1, the majority of patients in this serieswere young (mean age, 25.8 years; range, 8-47 years); nine
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018

724 Karim et al. CID 1997;24 (April)
Table 1. Characteristics of the 17 apparently immunocompetent patients with chronic invasive aspergillosis whose cases were reviewedretrospectively.
History and presentingcomplaints
Examination and test findings
Clinical Laboratory Radiographic CT
Sino-orbital aspergillosis for6 y; loss of vision in L eyesince bilateralethmoidectomy in 1989; Rxwith AmB (1 g) in 1989;no risk factors
T, 37.2; proptosisin R eye; novision in L eye
WBCs, 9,200 (64% N,30% Lym, 5% E,1% M); Cr, 0.9
Chest: normal Destruction of postsphenoidand optic canal areas,with bony erosion ofMCF and sella turcica
Bilateral nasal obstruction andpolyps for 8 y, withswelling around L eye and
T, 38.0; broadeningof nasal bridge;light perception
WBCs, 1,900 (80% N,15% Lym, 4% E,1% M); Cr, 1.0;
Fibrocalcific areas inapex of L lung;healed
Opacified paranasal sinuseswith destruction of MCFand sella turcica
loss of vision;polypectomies in 1982-84;
only in L eye CSF: Glu, 42; Pr,593; cells, 340/mm3
tuberculosis
Aspergillus flavus isolatedfrom polyps excised in
(100%lymphocytes)
1987; no risk factorsNasal stuffiness and recurrent
polyposis for prior 4 y;polypectomies in 1987 and
T, 37.0; polyps inboth nostrils(more in L) and
WBCs, 9,200 (39% N,30% Lym, 30% E,1% M); ESR, 18;
Linear densitiespresent at R apex;fibrocalcific
Posttreatment: bonyinvolvement of medialwall of L maxilla
1990; no risk factors thin, waterynasal secretions
Cr, 1.3; TB, 0.6;ALT, 20; AST, 21;
density, LUL
ALP, 47; IgE, 1,000IU/mL
Headache and R proptosis andpain, R nasal obstructionand pain in submandibularnode; biopsy 2 y previouslyshowed fungal disease; norisk factors
T, 37.0; firm, fixedsubmandibularnodes,tenderness, Reye; R nasalpolyp
WBCs, 8,900 (70% N,22% Lym, 6% E,2% M); Cr, 1.1
Chest: normal Mass infiltrating R maxilla,with extension in R orbitand R temporal andfrontal lobes
Rhinorrhea for 10 y and painover the paranasal sinuses;no risk factors
T, 37.2 WBCs, 8,200 Chest: normal Maxillary sinusopacification
Nasal blockage, R rhinorrhea,and occasional frontalheadache for 2 y; diplopiaand decreased vision in Reye; no risk factors
T, 36.8; Rproptosis
WBCs, 8,400 (67% N,31% Lym, 1% E,1% M); ESR, 41;Cr, 1.8; CSF: Glu,91; Pr, 54; cells, 2/mm3 ; BMC neg
Haziness of sinuses;chest: normal
Bulging of dura
Recurrent polyposis; T, 37.0; polyps in WBCs, 10,100 (71% Postinflammatory Bony involvement of floorunderwent Caldwell-Luc L nasal cavity N, 25% Lym, 3% scarring, RUL and of L orbit and medialprocedure, partial E, 1% M); ESR, 16; RML; wallethmoidectomy,polypectomy; no riskfactors
Cr, 0.9 opacification ofall sinuses
Nasal obstruction anddischarge (L > R),sneezing, intermittent Lfacial puffiness and
T, 36.2; nasalseptum grosslydeflected to R;polyp in L side
WBCs, 6,700 (60% N,35% Lym, 3% E,2% N); Cr, 1.2
Opacification of Lmaxillary sinusand nasal cavity,L ethmoid and
Involvement of paranasalsinuses, with bonydestruction of Lpostorbital wall; no
lacrimation; 2 surgeries(1986, 1990); no riskfactors
sphenoid; chest:normal
intracranial involvement
L facial pain, swelling of eye,and headaches for 6 mo;previous injury to Ltemporal region neareyebrow; no risk factors
T, 36.2; grossproptosis on L;no vision, L eye;ophthalmoplegia,swelling,tenderness on Lside of face
WBCs, 12,200 (76%N, 22% Lym, 1%E, 1% M); Cr, 1.0
Chest: normal MRI showed mass in Lmaxillary sinus,extending into sphenoid
NOTE. Abbreviations and terms (units of measure and/or normal values): ACE = angiotensin-converting enzyme (8-52); albumin (3.2-5.0 g/dL); ALP = alkalinephosphatase (28-124 IU/L); ALT = alanine aminotransferase (0-55 IU/L); AmB = amphotericin B; AST = aspartate aminotransferase (IU/L); ATT = antituberculoustherapy; BMC = bone marrow culture; Cr = creatinine level (0.85-1.35 mg/dL); DB = direct bilirubin level (0-0.15 mg/dL); E = eosinophils (0.1%-0.06%);ESR = erythrocyte sedimentation rate (mm/h); Flu = fluconazole; globulin (1.9-3.65 g/dL); Glu = glucose (mg/dL); Hx = history; IgA (0.16-1.7 g/L); IgE (10-180IU/mL); IgG (5.5-12.0 g/L); Itra = itraconazole; L = left (sided); LLL = left lower lobe; LUL = left upper lobe; Lym = lymphocytes (20%-45%); M = monocytes(0.02%-10%); MCF = middle cranial fossa; N = neutrophils (40%-75%); neg = negative; Pr = protein (g/dL); R = right (sided); RML = tight middle lobe;RUL = right upper lobe; Rx = treated or treatment; T = temperature (°C); TB = total bilirubin (0.2-1.25 mg/dL); WBCs (4-10.0 X 109/mm3).
Case no./age (y), sex
1/21, M
2/16, F
3/27, F
4/22, F
5/33, M
6/26, F
7/38, F
8/17, F
9/28, F
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018

CID 1997;24 (April)
Aspergillosis in Apparently Immunocompetent Hosts 725
Table 1. (Continued)
Therapy Pathological finding(s) (source)Culture isolate(s)
(type of specimen)Comments on follow-up and
outcome
External ethmoidectomy; 1.2 g AmB Septate fungal hyphae (ethmoid Aspergillus flavus (tissue) Long Hx of aspergillus infection of(1 mg/[kg • d]) tissue and tissues from upper
nasal wall)sinuses; lost to follow-up (went toEngland for reconstructivesurgery)
External ethmoidectomy,sphenoidectomy; 250 mg AmB
Septate hyphae invading frontallobe; inflammatorygranulation tissue
A. flavus (frontal lobe ofbrain)
Postoperative loss of vision in L eyeand pneumocephalus withprogressive loss of vision;underwent ventricular drainage andlater developed disseminatedintravascular coagulation,hypotension, and presumed sepsis;died despite Rx with antibiotics
Caldwell-Luc procedure; Mixed allergic and A. flavus (sinus tissue) Well up to last visit except chestethmoidectomy; sphenoidectomy; inflammatory pattern (R and radiograph showed fibrocalcificnasal polypectomy L nasal cavity tissue) densities in LUL and shadowing in
RUL consistent withaspergillosis
Craniotomy, ethmoidectomy; 3 g Granulomas with septate Aspergillus fumigatus Symptoms continued despite repeatedAmB (1 mg/[kg • d]) and Itra (400 hyphae (brain tissue) (brain and sinus tissue); craniotomy; hospitalized untilmg q.d. for 14 d) Pseudallescheria boydii death
(sinus tissue)
R Caldwell-Luc procedure, Lintranasal antrostomy
Acute and chronicinflammatory cells andoccasional septate hyphae
A. flavus (tissue) Well up to last visit
(mucosal tissue shavings)Bilateral external ethmoidectomy,
sphenoidectomy, and bilateralEosinophils, bony fragments,
septate hyphae (polypoidalA. flavus (polyp removed
at surgery)Postoperative radiograph showed R
maxillary haziness; well on lastmaxillary antrostomy; 300 mgAmB (1 mg/[kg • d])
tissue) follow-up visit but still had frontalheadaches
Intranasal ethmoidectomy,sphenoidectomy, and L external
Granulation tissue, necrotic andseptate fungal hyphae
A. flavus, Klebsiella
pneumoniae, and
CT repeated; well up to last visit
ethmoidectomy (ethmoid tissue) Staphylococcus aureus
(sinus tissues)
R Caldwell-Luc and L polypectomy,then L external ethmoidectomy, L
Acute and chronicinflammatory cells (polypoid
A. flavus (polypoid tissue) Followed up in clinicpostoperatively; recurrent
transnasal sphenoidectomy,ethmoidectomy, L Caldwell-Luc;1.5 g AmB (1 mg/[kg • d])
tissue); no granulomas seen headaches; CT performed andshowed extensive paranasalinvolvement and bony destructionof posterior wall of L orbit
L orbital exenteration, external Chronic granulomatous A. flavus (tissue) MRI repeated; still complains ofethmoidectomy, sphenoidectomy,and parasellar exploration; 800mg AmB (1 mg/[kg • d])
inflammation with septatehyphae (sphenoid andpostorbital region tissue)
facial tenderness
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018

726 Karim et al. CID 1997;24 (April)
Table 1. (Continued)
Examination and test findingsCase no./age (y), sex
10/32, M
11/40, M
12/24, M
13/8, F
14/47, M
15/8, F
16/31, M
17/21, M
History and presentingcomplaints Clinical Laboratory Radiographic CT
Headache and reduced vision, T, 37.0; WBCs, 10,200 (74% Chest: normal Contrast-enhancing lesionproceeding to loss of vision papilledema, L N, 24% Lym, 1% in R frontal lobein L eye in previous 4 eye E, 1% M); Cr, 1.5months; no risk factors
Hx of transient L hemiparesis T, 37.0; alert, WBCs, 8,500 (83% N, Old healed 1.5-cm enhancing lesion, Rand seizures; fits and loss oriented, no 16% Lym, 1% E, inflammatory postparietal lobe, withof consciousness in 1987; focal 5% M); ESR, 6; Cr, lesion in R apex, edema; calcified upperno risk factors neurological 1.0 probably from retroperitoneal nodes in
deficit tuberculosis abdomenOccasional hemoptysis for 1 y T, 36.6; clubbing WBCs, 17,300 (75% Cavitary lesion, Not done
and cough for 10 y; present; N, 20% Lym, 4% RUL; 4-cmirregular ATT therapy; bronchial patch E, 1% M); ESR, 8; fungus ball andex-smoker; long Hx of in RUL Cr, 1.2; nitroblue tubular density,rhinorrhea and asthmatic tetrazolium RLL; two softepisodes reduction, tissue lesions in L
neutrophil mid zone nearchemotaxis neg; hilum and inHIV neg postbasal segment,
LLL; sinusesclear.
Cough and fever for 7 mo; T, 37.2 WBCs, 10.7 (54% N, Old tuberculosis Not donedyspnea for 2 mo; 30% Lym, 13% E, lesions; bulls ontuberculosis diagnosed 3% M); ESR, 35; R side with air-radiographically (R hilar TB, 0.8; ALT, 18; fluid levels; bullashadowing); no risk factors y-glutamyl also on L side
transferase, 21 U/L;Cr, 1.0
Shortness of breath and mild T, 37.0 WBCs, 6,500 (70% N, Interstitial lung Interstitial lung fibrosiscough with clear sputum 26% Lym, 2% E, fibrosis, prominentfor 4 y, increased over 2% M); ESR, 20; nodesprior 1 y; Rx ATT for 6 Cr, 0.9; TB, 1.2;mo without improvement ALT, 14;
Sarcoidosis? ACE,41.1
Recurrent fever, cough, T, 37.4; L otitis WBCs, 26,300 (52% Pneumonitis in both Not donemultiple lymph node externa; weight, N, 30% Lym, 15% lung fields (moreswellings, and poor weight 14 kg; diffuse E, 3% M); ESR, on R)gain for prior 3 y; previous bronchi, RUL; 131; TB, 0.3; ALT,biopsy of R cervical lymph liver, 3 cm; 22; ALP, 90; totalnode showed caseating spleen, 2 cm Pr, 9.7; albumin,granulomas and septate 3.0; globulin, 6.7;fungal hyphae bone marrow:
normal precursorcells; HIV neg
Mild hemoptysis for 2 y; T, 38.0 WBCs, 8,900 (74% N, Opacified R Not donerecent weight loss; given 22% Lym, 2% M, hemithorax;ATT for 6 mo with no 2% E) pleural-effusionimprovement; no risk density in L hilumfactors
Chronic draining sinus in L T, 36.6; six WBCs, 9,500; IgM, Destruction of 5th Not donefoot, with yellow pus, for discharging 2.61 g/L (0.4-0.95) metatarsal, erosion6 y; excised and cauterized sinuses on of 3rd and 4th2 mo previously; no risk dorsum of R metatarsals; chest:factors foot, with yellow normal
pus
NOTE. Abbreviations and terms (units of measure and/or normal values): ACE = angiotensin-converting enzyme (8-52 IU/L); albumin (3.2-5.0 g/dL); ALP =alkaline phosphatase (28-124 IU/L); ALT = alanine aminotransferase (0-55 IU/L); AmB = amphotericin B; AST = aspartate aminotransferase (IU/L); ATT =antituberculous therapy; BMC = bone marrow culture; Cr = creatinine level (0.85-1.35 mg/dL); DB = direct bilirubin level (0-0.15 mg/dL); E = eosinophils (0.01%-0.06%); ESR = erythrocyte sedimentation rate (mm/h); Flu = fluconazole; globulin (1.9-3.65 g/dL); Glu = glucose (mg/dL); Hx = history; IgA (0.16-1.7 g/L); IgE(10-180 IU/mL); IgG (5.5-12.0 g/L); Itra = itraconazole; L = left (sided); LLL = left lower lobe; LUL = left upper lobe; Lym = lymphocytes (20%-45%); M =monocytes (0.02%-10%); MCF = middle cranial fossa; N = neutrophils (40%-75%); neg = negative; Pr = protein (g/dL); R = right (sided); RML = right middlelobe; RUL = right upper lobe; Rx = treated or treatment; T = temperature (°C); TB = total bilirubin (0.2-1.25 mg/dL); WBCs (4-10.0 X 109/mm3).
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018

CID 1997;24 (April)
Aspergillosis in Apparently Immunocompetent Hosts 727
Table 1. (Continued)
Therapy Pathological finding(s) (source)Culture isolate(s)
(type of specimen)Comments on follow-up and
outcome
Craniotomy; 1.5 g AmB (1 Granulation tissue with fungal A. fumigatus (tissue) Vision in L eye; well up to lastmg/[kg • d]) hyphae visit
Corticectomy with postparietal Abscess, septate branching A. flavus (brain tissue) Followed up in clinics; receivingosteoplastic flap; 500 mg AmB (1mg/[kg • d])
hyphae phenytoin
Posterolateral thoracotomy, RUL Septate hyphae, acute Aspergillus niger (fungus Symptoms returned (3 mo after Rx)lobectomy; Flu (600 mg q.d. for inflammatory changes ball removed from lung with dyspnea hemoptysis and12 d), Itra (200 mg q.d. until (fungus ball removed from and [repeatedly] fever; Rx with 3 g AmB (1 mg/afebrile 3 mo later) lung) sputum) [kg • d]), followed by Itra (200
mg q.d.), and symptoms abated;radiograph showed pneumonia inR base and LLL lingula andhilum
R anterolateral thoracotomy withbullectomy; 1 g AmB (1 mg/
Extensive necrosis, eosinophils,multinuclated cells, and
A. fumigatus,
StreptococcusDischarged while receiving ATT and
cloxacillin; doing well[kg • d]) septate hyphae (lung tissue) pneumoniae (lung
tissue); cultures neg fortuberculosis and acid-fast bacilli
Mediastinotomy, open lung biopsy Granulomas, hyphae (hilarlymph node specimen)
A. flavus (biopsiedmediastinal lesion);mycobacterial culturesneg
Lost to follow-up
Lymph node biopsy; 1 g AmB(1 mg/[kg • d])
Noncaseating granulomas withhyphae (biopsied axillary
A. fumigatus (lymph nodetissue); all bacterial and
Nitroblue tetrazolium reduction,neutrophil chemotaxis study
lymph node) mycobacterial culturesneg
normal; IgA, 2.62 g/L; IgG, 46.0g/L; lost to follow-up
Mediastinal lesion biopsy; AmB,100 mg only (1 mg/[kg • d])
Chronic granulomatousinflammation and hyphae
A. fumigatus (biopsiedlesion); all bacterialand mycobacterialcultures neg
Extensive postoperative hemoptysis,died 2 d after surgery
Local exploration and curettage of Chronic pyogenic A. fumigatus (tissue); all Repeated debridement, in attempt towound; 1,226 mg of AmB (1 granulomatous inflammation bacterial and clear infection, yielded muchmg/[kg • d]) and branching septate mycobacterial cultures improvement; after 1 y of such
hyphae neg treatment, lost to follow-up
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018

728 Karim et al. CID 1997;24 (April)
were female and eight were male. All patients with aspergillarsinusitis (cases 1-9) had a long history of rhinitis (figure 1).One patient with pulmonary aspergillosis (case 12) had a longhistory of asthma and also had a history of treated tuberculosis.Another patient (case 13) had fibrotic changes evident on achest radiograph that were suggestive of pulmonary tuberculo-sis, as did patients 2, 3, 7, and 11. In one patient (case 16),tuberculosis was suspected; however, there was no response toantituberculosis therapy, all mycobacterial cultures were nega-tive, and the patient had mediastinal involvement with Asper-
gillus fumigatus.Two patients presented with lymph node aspergillosis (cases
14 and 15) (figure 2). In one case (case 14), interstitial pulmo-nary fibrosis evident on a chest radiograph suggested underly-ing sarcoidosis. Levels of angiotensin-converting enzymeswere not elevated, however. The patient was lost to follow-up,but during hospitalization no other evidence of immunosup-pression was noted, i.e., a history of recurrent infections or thepresence of oral thrush on examination. Bacterial and mycobac-terial cultures of sputum and lymph nodes were negative.
In the second case (case 15), chest radiographic findingswere suggestive of aspergillar pneumonia. Bacterial and myco-bacterial cultures of sputum and lymph nodes were negative.Lymph node cultures yielded only A. fumigatus. Two patients(cases 10 and 11) had isolated brain abscesses (figure 3). Nopulmonary or other source was detected. From the single patientwith osteomyelitis of the foot (case 17), A. fumigatus wasisolated; no other system appeared involved.
Laboratory Tests
WBC counts ranged from 6,500/mm 3 to 26,300/mm3 , witha mean of 11,165/mm 3 . Differential counts were available forall patients (table 1) except in cases 5 and 17. In the cases inwhich the erythrocyte sedimentation rate was available, it wasnot markedly elevated, except in case 15, in which it was 131mm/h. Renal and liver function tests were not performed forall patients, as they otherwise appeared well, without stigmataof liver or renal disease. When these tests were performed, theresults were normal (table 1).
Immunologic Parameters
HIV testing was negative in cases 12 and 15 but was notperformed in the other cases. Results of nitroblue tetrazoliumtests and neutrophil chemotaxis studies were also normal forthese two patients. In case 15 serum protein immunoelectropho-resis demonstrated an elevated level of IgG, but otherwise thefindings were normal.
Outcome
Two patients with intracranial extension of sinus aspergillo-sis died despite aggressive combined surgical and medical ther-apy with up to 3 g of amphotericin B. Patient 2 had receivedonly 250 mg of amphotericin when she died of postoperativecomplications. All other patients with invasive sinus diseaserequired further follow-up, as residual disease and recurrentdisease were common. However, none had developed recurrentinfections, oral thrush, or lymphadenopathy or had evidenceof renal or liver disease on follow-up.
Patient 12, who had asthma and pneumonia, did not respondto up to 3 g of amphotericin B and developed new pulmonaryinfiltrates. Considerable improvement was noted followingtherapy with a 200 mg/d dosage of itraconazole (figure 4). Case16 was misdiagnosed as tuberculosis. Only after 6 months ofineffective therapy did a mediastinal biopsy yield an Aspergil-lus species. The patient had received 100 mg of amphotericinB when he died of massive hemoptysis soon after surgery.
The two patients with isolated brain abscesses did well aftersurgery and adjuvant therapy with amphotericin B. The patientswith lymph node aspergillosis and osteomyelitis were lost tofollow-up.
Figure 1. A CT scan (direct coronal section) revealed an inflam-matory mass in the sphenoid sinus and posterior aspect of the leftmaxillary antrum, with destruction of its lateral wall, in this patientwith aspergillosis (case 8).
Discussion
Invasive Aspergillus in immunocompromised hosts is welldocumented, and the species is second only to Candida spe-cies as an opportunistic fungal pathogen [14, 15]. Conditionsknown to predispose to invasion include qualitative or quanti-tative neutrophil defects; cytotoxic drug, corticosteroid, orprolonged antibiotic administration; and possibly underlyinglung disease and cell-mediated immune dysfunction related
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018

CID 1997;24 (April) Aspergillosis in Apparently Immunocompetent Hosts 729
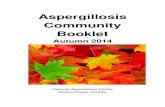
Figure 2. Multiple granulomas ina lymph node of a patient with asper-gillosis (case 15). Aspergillus organ-isms with septated hyphae wereidentified (arrow). (Original magni-fication, X 380; stain, hematoxylinand eosin.)
to recent viral infection [8, 16-19]. In addition, several casesinvolving patients with severe liver or renal disease havebeen described [20].
Invasive aspergillosis in apparently immunocompetent
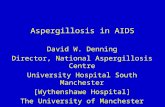
Figure 3. A CT with contrast showed an enhancing lesion in theright frontal lobe, with a small amount of surrounding edema andmidline shift, in this patient with aspergillosis (case 10).
hosts has previously been described (particularly as sinusitisand pulmonary disease). Allergic responses to the fungusappear to play a significant role in pathogenesis. Patientswith allergic sinusitis, initially described by Katzenstein etal. [21], and bronchopulmonary aspergillosis are increasinglyreported in the literature. Allergic reactions also occur inpatients with aspergillar infection in their paranasal sinusesor ectatic bronchi [21, 22]. Perhaps less well-recognized isthe development of invasive aspergillosis in such patients. Acertain subset of patients with no other evident risk factorsgo on to develop invasive sinus or pulmonary disease afterseveral months or years [23-30].
Almost all of our patients with invasive sinus disease wereatopic and had long histories of allergic rhinitis and nasalpolyps (table 1). In addition, one of our patients with invasivepulmonary disease had a long history of asthma. However,atopy was not specifically mentioned in several of the largestseries of invasive sinusitis reported from the Sudan, whereheavy environmental exposure was thought to be causative.Described patients in the Sudan were usually asymptomaticand presented with unilateral proptosis of gradual progressionover months [31]. Our patients all had headache, most com-plained of intermittent fever and nasal discharge for monthsbefore presenting, and several had had nasal polypectomies orother surgery (table 1, cases 1-9).
Two cases of intracranial extension of paranasal sinus asper-gillosis over a 10-year period in the Birmingham area of En-gland were noted by Oates et al., an interval reflecting howrare the condition is in the developed world [32]. One patientwas a Sudanese and the second a patient from Zambia. In bothof these cases, as well as those reported from the Sudan and
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018

730 Karim et al. CID 1997;24 (April)
Figure 4. A chest radiograph showed a large, well-defined infiltratein the right base and prominent left hilum in case 12.
our cases of invasive sinus disease, A. flavus was the speciesresponsible.
Although A. fumigatus has been described as the most com-mon cause of aspergillosis, A. flavus is more common in inva-sive disease, particularly in lesions beginning in the paranasalsinuses [33-37]. Aspergillar meningitis often is due to exten-sion of aspergillar sinusitis, resulting in chronic basilar menin-gitis [38]. Cultures are usually negative. In one patient withsinus disease (case 2), initial CSF analysis demonstrated anelevated cell count and protein level.
We have described two cases of isolated brain abscesses.Intracranial abscesses without other apparent sources may fol-low intravenous drug abuse or occur sporadically via hematoge-nous spread from an occult, probably pulmonary, source. Morecommonly, CNS involvement occurs by direct extension ofinvasive aspergillar infection and may follow head trauma[39-41]. In our patients there was no evidence of direct inva-sion and no history of intravenous drug use.
Karam and Griffin reviewed invasive pulmonary aspergillo-sis in immunocompetent hosts [5]. Among 25 patients withdefinite invasive pulmonary disease, 4 had a history of alcohol-
ism, 3 had a history of influenza A, and only 1 had a history ofasthma; 46.9% of patients were apparently healthy. Antecedentviral infection was not noted in our patients who reportedprolonged symptoms at presentation.
An asthmatic patient with no history of steroid use developedextensive pulmonary aspergillosis after resection of an aspergil-loma (case 12). In a previously reported case [9], disseminatedaspergillosis involving the myocardium and brain occurredafter resection of an aspergilloma. This patient, however, hada history of alcohol and drug use as well as tuberculosis, andthe clinical condition rapidly deteriorated until death occurredon the 28th postoperative day; this contrasts with the moreindolent presentation of our case 12.
Alcohol use may induce neutrophil dysfunction sufficientlyenough to predispose a patient to invasive aspergillosis [42].None of our patients reported alcohol or drug use. Alcohol useis uncommon in Pakistan, and significant renal or liver diseasewas not noted in our patients.
Aspergillar infection of the lymph nodes is uncommon, oc-curring with dissemination and in chronic granulomatous dis-ease [43]. We have described two patients from whom Asper-gillus species were recovered by culture of lymph nodespecimens (cases 14 and 15); pathology demonstrated granu-loma formation (figure 2). In one series of 64 granulomatouslymph nodes, Aspergillus species were not identified [44].Granulomas were initially noted in one of our patients (case14); later cultures of the lymph node yielded A. flavus. In thesecond patient (case 15), an 8-year-old girl, the findings ofseveral nitroblue tetrazolium reduction tests made the presenceof underlying chronic granulomatous disease, which is knownto predispose to invasive aspergillosis, less likely. Eosinophiliawas not noted in our patients.
Mediastinal invasion with Aspergillus species is extremelyrare [45] but occurred in one of our patients (case 16). He hadinitial pneumonia and empyema unresponsive to antituberculo-sis therapy; all bacterial and mycobacterial cultures remainednegative. Subsequent mediastinoscopy and biopsy demon-strated hyphae, and cultures yielded A. fumigatus. The etiologyof granulomatous mediastinitis is not established in most in-stances; a review of 77 patients proved that only for 3 (2 withhistoplasmosis and 1 with tuberculosis) could the responsibleorganism be determined [46].
Pulmonary aspergillosis followed tuberculosis in two ofour patients. In an adult asthmatic (case 12), an aspergil-loma occurred in a presumptive tuberculous cavity. Thepatient had a history of response to antituberculosis ther-apy. In an 8-year-old girl, tuberculosis was evident on achest radiograph before she presented with an empyema,which subsequently yielded an Aspergillus species. Under-lying lung disease has been described as a predisposingfactor for invasive aspergillosis [17, 18]. It is difficult toexclude associated phagocytic impairment as a factor in thesetting of tuberculosis. Several other patients (cases 2, 3,7, and 11) had evidence of old, probably healed tuberculosis
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018

CID 1997;24 (April) Aspergillosis in Apparently Immunocompetent Hosts 731
on chest radiographs. In summary, the majority of patientsdescribed had underlying abnormalities in the areas of in-volvment, which probably predisposed to colonization withAspergillus species before invasive disease set in.
The pathology of invasive aspergillosis depends on the host.As has been described with regard to immunocompetent pa-tients, granuloma with multinucleated giant cells is the predom-inant histopathologic feature. This was seen in our patients(figure 2) and has been noted in the literature. Vascular invasionusually occurs in immunocompromised patients [47]. Gefter etal. [47] have previously reported a chronic cavitary form ofpulmonary aspergillosis that may occur with mild immunosup-pression or underlying lung disease. They referred to this formas "semiinvasive." The pathology is distinct: extensive lungdestruction can occur despite the lack of vascular invasion [48].
CT and MRI are important noninvasive methods for evaluat-ing invasive fungal disease. The CT appearance of intracranialaspergillosis may be nonspecific and may contribute to thedifficulty in diagnosis. Beal et al. described low-attenuationlesions showing variable degrees of contrast-enhanced masseffect [38]. Dense concretions within a paranasal sinus massare said to be pathognomonic of an aspergillar granuloma [49].
MRI may be superior; aspergilloma is distinctive in returninga very low T2 signal, attributed to the high content of ironand manganese in fungal tissue [50]. In invasive pulmonaryaspergillosis, a CT halo or multiple small inflammatory massesmay be seen [51, 52]. Gefter et al. described the radiographicspectrum of "semiinvasive aspergillosis" as early pulmonaryconsolidation and pleural thickening; as cavitation develops, a"crescent sign" may be seen [48] .
The best chemotherapeutic approach to chronic necrotizingpulmonary aspergillosis is not known, but intravenous ampho-tericin B is effective [53]. Herbert and Bayer stressed the widestrain-to-strain variability in susceptibility to amphotericin Bin vitro and the higher minimal fungistatic concentrations ofA. flavus as compared with those of A. fumigatus [47]. How-ever, correlation between in vitro susceptibility and in vivoresponse does not always occur [53].
Denning et al. noted that for 35% of Aspergillus isolatestested, the MIC of amphotericin was ktg/mL, a level usuallyconsidered resistant. Eighteen of 21 patients evaluated re-sponded to itraconazole [54]. In our case 12, a patient withpulmonary aspergillosis, clearing of pulmonary infiltrates oc-curred after therapy for itraconazole. In a subsequent reviewof 2,121 cases of therapy for invasive aspergillosis [55], Den-ning and Stevens noted an overall response rate of 55% toamphotericin B. In one series, the conditions of several patientswith apparent chronic necrotizing pulmonary aspergillosisfailed to improve with intravenous amphotericin B therapy butresponded to intracavitary amphotericin B [55].
Surgical treatment alone appeared satisfactory for the major-ity of nonimmunocompromised patients with aspergillar sinus-itis, specifically maxillary sinusitis. However, surgical andmedical therapy failed in three cases, of which two involved
sphenoid sinus disease. Other patients with sphenoid diseasedid well with surgery alone [56, 57]. In the series reportedfrom the Sudan, most patients responded to surgery [31]. Allour patients with sinus disease required repeated and extensivesurgery, as well as therapy with amphotericin B. Two of thesenine patients (table 1) died, one was lost to follow-up, andseveral others had residual disease.
In 33 assessable cases of cerebral aspergillosis, mostly in-volving immunocompromised patients, Denning and Stevens[55] noted an overall 24% response to therapy; mortality wasnearly 100% among immunocompromised patients. Our pa-tients with isolated brain abscesses (cases 10 and 11) survivedafter surgery, although one had severe neurological sequelae,as noted in previous cases [38-41]. Surgery alone may beadequate for well-encapsulated single lesions in less immuno-compromised patients.
Bone aspergillosis often follows trauma or surgery, as inone of our patients. The patient required repeated surgery overseveral months, as well as therapy with amphotericin B. Sec-ondary infection with invasive Aspergillus in a previously in-fected foot cannot be excluded. As suggested in the literature,combined medical and surgical therapy is indicated. Amongresponders in one series, 59% underwent a combination ofmedical and surgical therapy [58].
Although immunologic data were not available for most ofour patients, no clinical evidence of immunosuppression wasnoted during presentation or in subsequent follow-up visits inpatients who were available for follow-up. HIV testing wasnot done, except in cases 12 and 15. AIDS is present in Paki-stan; the World Health Organization had reported 52 cases asof May 1995. However, invasive aspergillosis is not commonin patients with AIDS [59]. In a literature review, additionaland known predisposing risk factors for invasive aspergillo-sis —i.e., neutropenia, corticosteroid use, or intravenous druguse were noted in 79% of cases involving HIV-infected pa-tients.
The frequency of cases presenting to the Aga Khan Univer-sity Hospital appears unusual. As suggested, several factorsmay be responsible, including the susceptibility of hosts withsubtle phagocytic defects from occult liver disease, tuberculo-sis, atopy, or other possible unknown socioeconomic factors.The description of a selective neutrophil defect in eradicationof Aspergillus species suggests that other specific unidentifiedfactors may be required for killing this fungus [60, 61]. Inaddition, a more virulent subtype of Aspergillus or heavy envi-ronmental exposure may be responsible. Recognition of theincreased prevalence of invasive aspergillosis is necessary indeveloping countries, where facilities for isolation of Aspergil-lus species may not be readily available.
References
1. Washburn RG, Gallin JI, Bennett JE. Oxidative killing of Aspergillus
proceeds by parallel myeloperoxidase-dependent and independent path-ways. Infect Immun 1987; 55:2088-92.
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018

732 Karim et al. CID 1997; 24 (April)
2. Bennett JE. Role of the phagocyte in host defense against aspergillosis.In: Vanden Bossche H, Mackenzie DWR, Cauwenbergh G, eds. Asper-gillus and aspergillosis. New York: Plenum Press, 1988:115.
3. Schaffner A, Douglas H, Braude A. Selective protection against conidia bymononuclear and against mycelia by PMN in resistance to Aspergillus. JClin Invest 1982; 69:617-31.
4. Kan VL, Bennett JE. Lectin-like attachment sites on murine pulmonaryalveolar macrophages bind Aspergillus fumigatus conidia. J Infect Dis1988;158:407-14.
5. Karam GH, Griffin FM Jr. Invasive pulmonary aspergillosis in nonimmu-nocompromised, nonneutropenic hosts. Rev Infect Dis 1986; 8:357-63.
6. Finegold SM, Will D, Murray FJ. Aspergillosis, a review and report oftwelve cases. Am J Med 1959;27:463-82.
7. Hillerdal G, Benson L, Lindgren A, Hjertquist SO. Disseminated pulmo-nary aspergillosis in a previously healthy young woman. Scand J InfectDis 1984;16:217-22.
8. Fisher JJ, Walker DH. Invasive pulmonary aspergillosis associated withinfluenza. JAMA 1979;241:1493-4.
9. Rosenberg RS, Creviston SA, Schonfeld AJ. Invasive aspergillosis compli-cating resection of pulmonary aspergilloma in a non-immunocompro-mised host. Am Rev Respir Dis 1982;126:1113-5.
10. Cooper JAD, Weinbaum DL, Aldrich TK, Mandell GL. Invasive aspergil-losis of the lung and pericardium in a non-immunocompromised 33year old man. Am J Med 1981;71:903-7.
11. D'Silva H, Burke JF Jr, Cho SY. Disseminated aspergillosis in a presum-ably immunocompetent host. JAMA 1982;248:1495-7.
12. Deleted in proof13. Pfaller MA, Fromtling RA. Mycology. In: Manual of clinical microbiol-
ogy. 6th ed. Washington, DC: American Society for Microbiology,1995:697.
14. Bodey GP. Infections in cancer patients. Cancer Treat Rev 1975; 2:89-128.
15. Armstrong D. Infectious complications in cancer patients treated withchemical immunosuppressive agents. Transplant Proc 1973;5:1245-8.
16. Young RC, Bennett JE, Vogel CL, Carbone PP, DeVita VT. Aspergillosis:the spectrum of the disease in 98 patients. Medicine 1970;49:147-73.
17. Rinaldi MG. Invasive aspergillosis. Rev Infect Dis 1983; 5:1061-77.18. Kallenbach J, Dusheiko J, Block CS, Bethlehem B, Koomhof HJ, Zin S.
Aspergillus pneumonia-a cluster of four cases in an intensive careunit. S Afr J 1977; 52:919-23.
19. Wiest PM, Flanigan T, Salata RA, Shlaes DM, Katzman M, LedermanMM. Serious infectious complications of corticosteroid therapy forCOPD. Chest 1989;95:1180-4.
20. Park GR, Drummond GB, Lamb D, et al. Disseminated aspergillosis oc-curring in patients with respiratory, renal and hepatic failure. Lancet1982; 2(8291):179-83.
21. Katzenstein AL, Sale SR, Greenberger PA. Allergic aspergillus sinusitis:a newly recognized form of sinusitis. J Allergy Clin Immunol 1983;72:89-93.
22. Safirstein BH, D' Souza MF, Simon G. Five year follow-up of allergicbronchopulmonary aspergillosis. Am Rev Respir Dis 1973;108:450-9.
23. Meeker DP, Gephardt GN, Cordasco EM Jr, Wiedemann HP. Hypersensi-tivity pneumonitis versus invasive pulmonary aspergillosis: two caseswith unusual pathologic findings and review of the literature. Am RevRespir Dis 1991;143:431-6.
24. Binder RE, Faling LJ, Pugatch RD, Mahasaen C, Snider GL. Chronicnecrotizing pulmonary aspergillosis: a discrete clinical entity. Medicine(Baltimore) 1982; 61:109-24.
25. McGill TJ, Simpson G, Healy GB. Fulminant aspergillosis of the noseand paranasal sinuses: a new clinical entity. Laryngoscope 1980; 90:748-54.
26. Lowe J, Bradley J. Cerebral and orbital aspergillus infection due to invasiveaspergillosis of the ethmoid sinus. J Clin Pathol 1986; 39:774-8.
27. Miglets AW, Saunders WH, Ayers L. Aspergillosis of the sphenoid sinus.Arch Otolaryngol 1978;104:47-50.
28. Yu VL, Wagner GE, Shadomy S. Sino-orbital aspergillosis treated withcombination antifungal therapy: successful therapy after failure withamphotericin B and surgery. JAMA 1980;244:814-5.
29. Gourley DS, Whisman BA, Jorgensen NL, Martin ME, Reid MJ. Allergicbipolar sinusitis: clinical and immunopathologic characteristics. J Al-lergy Clin Immunol 1990; 85:583-91.
30. Karim M, Sheikh H, Alam M, Sheikh Y. Disseminated bipolar infec-tion in an asthmatic patient: case report. Clin Infect Dis 1993; 17:248-53.
31. Milosev B, Mabgoub EIS, Abdel AAL, El Hassan AM. Primary aspergil-loma of paranasal sinuses in the Sudan. Br J Surg 1969; 56:132-7.
32. Oates J, Clark DR, Chiodini P. Intracranial extension of paranasal sinusaspergillosis. J Laryngol Otol 1987; 101:188-90.
33. Young RC, Jennings A, Bennett JE. Species identification of invasiveaspergillosis in man. Am Clin Pathol 1972; 58:554-7.
34. Green WR, Font RL, Zimmerman LE. Aspergillosis of the orbit: reportof ten cases and review of the literature. Arch Ophthalmol 1969; 82:302-13.
35. DeFoer C, Fossion E, Vaillant JM. Sinus aspergillosis. J CraniomaxillofacSurg 1990; 18:33 -40.
36. Bassiouny A, Maher A, Bucci TJ, Moawad MK, Hendawy DS. Non-invasive antromycosis. J Laryngol Otol 1982;96:215-28.
37. Bahadur S, Kacher SK, D' Souza B, Shopra P. Paranasal sinus aspergillosis.J Laryngol Otol 1983;97:863-7.
38. Beal MF, O'Carroll CP, Kleinman GM, Grossman RI. Aspergillosis ofthe nervous system. Neurology 1982;32:473-9.
39. Walsh TJ, Hier DB, Caplan LR. Aspergillosis of the central nervous sys-tem: clinicopathological analysis of 17 patients. Ann Neurol 1985;18:574-82.
40. Salaki JS, Louria DB, Chmel H. Fungal and yeast infections of the centralnervous system: a clinical review. Medicine (Baltimore) 1984; 63:108 -32.
41. Mohandas S, Ahuja GK, Sood VP, Virmani V. Aspergillosis of the centralnervous system, J Neurol Sci 1978; 38:229-33.
42. Ascah KJ, Hyland RH, Hutcheon MA, et al. Invasive aspergillosis in ahealthy patient. Can Med Assoc J 1984; 131:332-5.
43. Elgefors B, Haugstvedt S, Brorsson JE, Esbjorner E. Disseminated asper-gillosis treated with amphotericin B and surgery in a boy with chronicgranulomatous disease. Infection 1980; 8:174-6.
44. Woodward BH, Rosenberg SI, Farham R, et al. Incidence and nature ofprimary granulomatous inflammation in surgically removed material.Am J Surg Pathol 1982; 6:119-29.
45. Ahmad M, Weinstein AJ, Hughes JA, Cosgrove DE. Granulomatous medi-astinitis due to Aspergillus flavus in a non-immunocompromised patient.Am J Med 1981; 70:887-90.
46. Schowengerdt CG, Suyemoto R, Main FB. Granulomatous and fibrousmediastinitis: a review and analysis of 180 cases. J Thorac CardiovascSurg 1969; 57:365.
47. Herbert PA, Bayer AS. Fungal pneumonia (part 4): invasive pulmonaryaspergillosis. Chest 1981; 80:220-5.
48. Gefter WB, Weingrad TR, Epstein DM, Ochs RH, Miller WT. Semi-invasive pulmonary aspergillosis: a new look at the spectrum of aspergil-lus infections of the lung. Radiology 1981;140:313-21.
49. Kopp W, Fotter R, Steiner H, Beaufort F, Stammberger H. Aspergillosisof the paranasal sinuses. Radiology 1985; 156:715-6.
50. Zinreich SJ, Kennedy DW, Malat J, et al. Fungal sinusitis: diagnosis withCT and MR imaging. Radiology 1988; 169:439-44.
51. Sider L, Davis T. Pulmonary aspergillosis: unusual radiographic appear-ance. Radiol 1987;162:657-9.
52. Herold CJ, Kramer J, Sertl K, Kalhs P, Mallek R, Imhof H. Invasivepulmonary aspergillosis: evaluation with MR imaging. Radiol 1989;173:717-21.
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018

CID 1997; 24 (April) Aspergillosis in Apparently Immunocompetent Hosts 733
53. Christiansen KJ, Bernard EM, Gold JWM, Armstrong D. Distribution andactivity of amphotericin B in humans. J Infect Dis 1985; 152:1037-43.
54. Denning DW, Stevens DA, Tucker RM, Hanson LH. Treatment of invasiveaspergillosis with itraconazole. Am J Med 1989; 86:791-800.
55. Denning DW, Stevens DA. Antifungal and surgical treatment of invasiveaspergillosis: review of 2,121 published cases [erratum appears in RevInfect Dis 1991; 13:345]. Rev Infect Dis 1990; 12:1147-201.
56. Sekhar LN, Dujovny M, Rao GR. Carotid-cavernous sinus thrombosis causedby Aspergillus fumigatus: case report. J Neurosurg 1980; 52:120-5.
57. Lavelle WG. Aspergillosis of the sphenoid sinus. Ear Nose Throat J 1988;67:266-9.
58. Tack KJ, Rhame FS, Brown B, Thompson RC Jr. Aspergillus osteomyeli-tis: report of four cases and review of the literature. Am J Med 1982;73:295-300.
59. Singh N, Yu VL, Rihs JD. Invasive aspergillosis in AIDS. South Med J1991; 84:822-7.
60. Fietta A. Sacchi F, Mangiarotti P, Manara G, Gialdroni Grassi G. Defectivephagocyte Aspergillus killing associated with recurrent pulmonary as-pergillus infections. Infection 1984; 12(1):10-3.
61. Pagani A, Spalla R, Ferrari FA, et al. Defective Aspergillus killing byneutrophil leukocytes in a case of systemic aspergillosis. Clin Exp Im-munol 1981; 43:201-7.
Downloaded from https://academic.oup.com/cid/article-abstract/24/4/723/440023by gueston 16 February 2018