Chronic inflammation & repair
23
-
Upload
simba-syed -
Category
Technology
-
view
529 -
download
3
description
KMU (IPM&R)
Transcript of Chronic inflammation & repair


Chronic inflammationChronic inflammation Difficult to defineDifficult to define Inflammation of prolonged duration in Inflammation of prolonged duration in
which active inflammation, tissue injury which active inflammation, tissue injury and the healing proceed simultaneouslyand the healing proceed simultaneously
Occurs in:Occurs in:– Persistent infections - AFB, fungi, TreponemesPersistent infections - AFB, fungi, Treponemes
Low toxicityLow toxicity Delayed hypersensitivityDelayed hypersensitivity Granulomatous inflammationGranulomatous inflammation
– Prolonged exposure potentially toxic agentsProlonged exposure potentially toxic agents SilicaSilica Toxic plasma lipids Toxic plasma lipids atherosclerosis atherosclerosis
– Autoimmunity - RA, lupus Autoimmunity - RA, lupus

Chronic inflammation is Chronic inflammation is characterized by:characterized by:
Infiltration with mononuclear cells Infiltration with mononuclear cells (macrophages, lymphocytes & plasma (macrophages, lymphocytes & plasma cells)cells)
Tissue destructionTissue destruction Repair involving angiogenesis and Repair involving angiogenesis and
fibrosisfibrosis Macrophage is the Macrophage is the prima donna prima donna of of
chronic inflammationchronic inflammation

Key macrophage events
1. Recruitment from circulation
2. Local Proliferation
3. Immobilization
4. Differentiation (microglia, kupffer, alveolar macrophage, osteoclasts).
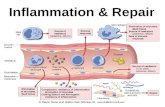
Macrophageprominent role due the large repertoire of
products it can produce when activated Tox. O2
Proteases Collagenases Chemotx factors Coag factors AA metabolites NO PDGF FGF TGF-
Tox. O2
Proteases Collagenases Chemotx factors Coag factors AA metabolites NO PDGF FGF TGF-

Note that the Note that the activated activated macrophage macrophage releases releases products that products that are similar to are similar to those those released by released by PMNsPMNs

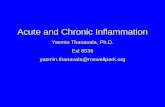
AntigenPresentation to T cells
AntigenPresentation to T cells
Lymphocyte
ActivatedLymphocyte
Macrophage
Activated macrophage
IFN-
IL-1 TNF-
Other inflammatory mediators
Other inflammatory mediators

Granulomatous Granulomatous InflammationInflammation
Aggregations of Aggregations of activated, modified activated, modified (epitheliod) (epitheliod) appearanceappearance
Granuloma – focal Granuloma – focal collection of collection of granulomatous granulomatous inflammation inflammation
BacteriaBacteria– TuberculosisTuberculosis– LeprosyLeprosy
ParasitesParasites– SchistosomiasisSchistosomiasis
FungiFungi– HistoplasmosisHistoplasmosis– BlastomycosisBlastomycosis
Metal/DustMetal/Dust– BerylliosisBerylliosis– SilicosisSilicosis
Foreign bodyForeign body– SplinterSplinter– SutureSuture– Graft materialGraft material
SarcoidosisSarcoidosis

GranulomaGranuloma


RepairRepair
Regeneration of injured tissue by Regeneration of injured tissue by parenchymal cells of the same typeparenchymal cells of the same type
Replacement by connective tissueReplacement by connective tissue Starts as early as 24 hoursStarts as early as 24 hours Granulation tissue at 3 - 5 daysGranulation tissue at 3 - 5 days Four Components:Four Components:
– AngiogenesisAngiogenesis– Migration and proliferation of fibroblastsMigration and proliferation of fibroblasts– Deposition of extracellular matrix (ECM)Deposition of extracellular matrix (ECM)– Remodeling (Maturation & organization of Remodeling (Maturation & organization of
fibrous tissue)fibrous tissue)

Proliferative PotentialProliferative Potential
Labile cells - continuously dividing Labile cells - continuously dividing – Epidermis, mucosal epithelium, GI tract Epidermis, mucosal epithelium, GI tract
epithelium etcepithelium etc Stable cells - low level of replicationStable cells - low level of replication
– Hepatocytes, renal tubular epithelium, Hepatocytes, renal tubular epithelium, pancreatic acinipancreatic acini
Permanent cells - never dividePermanent cells - never divide– Nerve cells, cardiac myocytes, skeletal Nerve cells, cardiac myocytes, skeletal
musclemuscle

Components of the processComponents of the processof fibrosisof fibrosis
Angiogenesis - New vessels budding Angiogenesis - New vessels budding from oldfrom old
Fibrosis, consisting of emigration and Fibrosis, consisting of emigration and proliferation of fibroblasts and proliferation of fibroblasts and deposition of ECMdeposition of ECM
Scar remodeling, tightly regulated by Scar remodeling, tightly regulated by proteases and protease inhibitorsproteases and protease inhibitors

Tissue RemodelingTissue Remodeling
Balance of deposition vs. degradationBalance of deposition vs. degradation Zn-dependent matrix metalloproteinasesZn-dependent matrix metalloproteinases
– Interstitial collagenases Interstitial collagenases type I, II, III type I, II, III collagencollagen
– Gelatinase Gelatinase type IV collagen & fibronectin type IV collagen & fibronectin– Stromelysins Stromelysins variety of ECM variety of ECM– Membrane-bound matrix metalloproteinases Membrane-bound matrix metalloproteinases
(MBMM)(MBMM)– Tissue inhibitors of metalloproteinase (TIMP)Tissue inhibitors of metalloproteinase (TIMP)

Scar remodeling Scar remodeling is regulated by is regulated by
metalloproteinasmetalloproteinases and their es and their
inhibitorsinhibitors
Tissue inhibitors of metalloproteinase

Wound healingWound healing Complex but orderly phenomenon Complex but orderly phenomenon
number of processesnumber of processes Induction of acute inflammatory response Induction of acute inflammatory response
by an initial injuryby an initial injury Regeneration of parenchymal cells Regeneration of parenchymal cells Migration and proliferation of both Migration and proliferation of both
parenchymal and connective tissue cellsparenchymal and connective tissue cells Synthesis of ECM proteinsSynthesis of ECM proteins Remodeling of connective tissue and Remodeling of connective tissue and
parenchymal components to restore parenchymal components to restore tissue functiontissue function
Remodeling of connective tissue to Remodeling of connective tissue to achieve wound strengthachieve wound strength

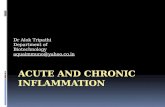
Healing by first intention Healing by first intention (primary union) (primary union)
Clean, uninfected, surgical incision with sutures:Clean, uninfected, surgical incision with sutures:
1.1. Blood clot formsBlood clot forms2.2. < 24 hours – PMNs appear< 24 hours – PMNs appear3.3. 24-48 hrs cut edges of epidermis thicken 24-48 hrs cut edges of epidermis thicken
from from basal cell hyperplasia, and epithelium basal cell hyperplasia, and epithelium
migratesmigrates for unionfor union4. By day 3 – PMN’s replaced by macrophages.4. By day 3 – PMN’s replaced by macrophages. Granulation tissue invades & collagen at Granulation tissue invades & collagen at
margins.margins.

Healing by first intention Healing by first intention (primary union) (primary union)
5.5. Incision filled with granulation tissue.Incision filled with granulation tissue. Maximal neovascularization & collagen Maximal neovascularization & collagen
bridges gap. Epidermis covers & is mature.bridges gap. Epidermis covers & is mature.6.6. One weekOne week – After suture removal wound – After suture removal wound
strength only strength only 10%10% (compared with unwounded (compared with unwounded skin)skin)
7.7. Second week – Continued collagen deposition Second week – Continued collagen deposition and fibroblast proliferation. PMNs gone.and fibroblast proliferation. PMNs gone.
8.8. First month – Scar with cellular connective First month – Scar with cellular connective tissue and no inflammatory cells. Regressed tissue and no inflammatory cells. Regressed vascular channels.vascular channels.
9.9. Third monthThird month – – 70-80%70-80% of maximum strength. of maximum strength.

Healing by first Healing by first intentionintention

Healing by second intention Healing by second intention (separated)(separated)
Large tissue defect to fill common Large tissue defect to fill common denominatordenominator
Differs from primary union in several Differs from primary union in several ways:ways:– More fibrin, more debris More fibrin, more debris more intense more intense
inflammationinflammation– More granulation tissue is formedMore granulation tissue is formed– Wound contraction aided by Wound contraction aided by
myofibroblastsmyofibroblasts

Healing by second Healing by second intention:intention:
Larger injury, abscess, Larger injury, abscess, infarction.infarction.
Process is similar butProcess is similar butresults in much larger results in much larger scar and then primary scar and then primary
unionunion

Factors that influence Factors that influence healinghealing
Nutrition - vitamin CNutrition - vitamin C Metabolic status – diabetes hindersMetabolic status – diabetes hinders Circulatory statusCirculatory status Hormones – steroids/glucocorticoids inhibitHormones – steroids/glucocorticoids inhibit InfectionInfection Mechanical stressMechanical stress Foreign bodiesForeign bodies Size, locations and type of the woundSize, locations and type of the wound
Whether a wound heals by primary or Whether a wound heals by primary or secondary union is determined by the secondary union is determined by the nature of the wound, rather than by the nature of the wound, rather than by the healing process itselfhealing process itself

















![Skin Inflammation, [Acute, Suppurative, Chronic, Chronic ... · Skin – Inflammation, [Acute, Suppurative, Chronic, Chronic Active, Granulomatous] presence of mononuclear cells (lymphocytes,](https://static.fdocuments.us/doc/165x107/5f0eb0c97e708231d44075f1/skin-inflammation-acute-suppurative-chronic-chronic-skin-a-inflammation.jpg)