CHRONIC HEPATITIS B - NATAP - HIV · CHRONIC HEPATITIS B Promising New Treatments Ed Gane NZ Liver...
47
CHRONIC HEPATITIS B Promising New Treatments Ed Gane NZ Liver Transplant Unit Auckland Hospital
Transcript of CHRONIC HEPATITIS B - NATAP - HIV · CHRONIC HEPATITIS B Promising New Treatments Ed Gane NZ Liver...

CHRONIC HEPATITIS B Promising New Treatments
Ed Gane NZ Liver Transplant Unit
Auckland Hospital

Goals of treatment in CHB:
APASL Consensus Statement 2005
“The ultimate long-term goal is prevention
of cirrhosis, decompensation and HCC,
and prolong survival.
Sustained viral suppression is the key to
the reduction or prevention of hepatic
injury and disease progression.
Therefore, the primary goal of treatment
for chronic hepatitis B is to eliminate or
permanently suppress HBV….. ”
Liaw YF et al. Liver Int 2005
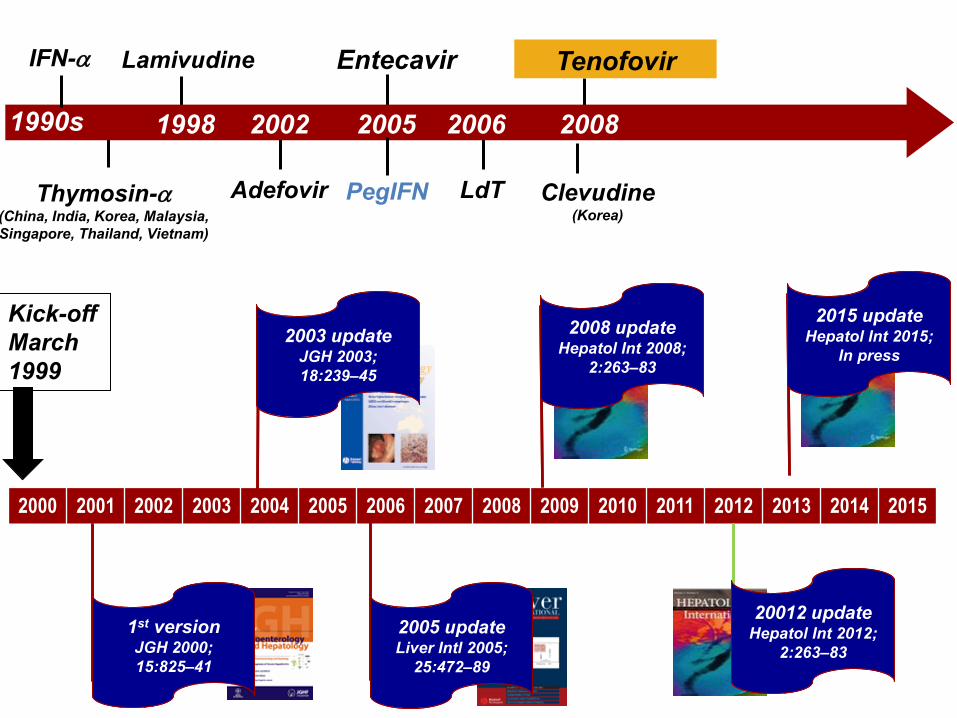
2015 update
May2015
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
2008 update Hepatol Int 2008;
2:263–83
2008 update Hepatol Int 2008;
2:263–83
2003 update JGH 2003;
18:239–45
2003 update JGH 2003;
18:239–45
1st version JGH 2000;
15:825–41
1st version JGH 2000;
15:825–41
2005 update Liver Intl 2005;
25:472–89
2005 update Liver Intl 2005;
25:472–89
Kick-off
March
1999
20012 update Hepatol Int 2012;
2:263–83
20012 update Hepatol Int 2012;
2:263–83
Thymosin- (China, India, Korea, Malaysia,
Singapore, Thailand, Vietnam)
Lamivudine
Adefovir PegIFN LdT
Tenofovir
1990s
Entecavir IFN-
2002 2006 1998 2005 2008
Clevudine (Korea)
2015 update Hepatol Int 2015;
In press
2015 update Hepatol Int 2015;
In press

Two randomized, double-blind, controlled trials in
HBeAg- (Study 102) and HBeAg+ (Study 103) CHB 1-3
– Rollover to open-label TDF at Week 48
– FTC allowed after Wk 72 if persistent viremia (DNA ≥69 IU/mL)
Chronic
HBV
patients
(HBeAg-
and
HBeAg+)
TDF 300 m g
( n= 250 , 17 6 )
ADV 10 mg
(n=125, 90)
Open - l a b e l TD F 30 0 m g Q D
8 5 4 3 0 1 2 Study Year
Biopsies
4
TDF 300 mg
(n=250, 176)
Benefits of Long-term Oral Antiviral Therapy:
Tenofovir in Studies 102 (HBeAg-) and 103 (HBeAg+)
1. Marcellin P, et al. J Hepatol. 2014 Jul 18; DOI: 10.1016/j.jhep.2014.07.019 (ePub ahead of print).

Benefits of Long-term Oral Antiviral Therapy:
Viral Suppression (Observed)
5
99.6% overall response at Year 8
98% overall response at Year 8
Weeks Weeks
TDF-TDF
ADV-TDF
TDF-TDF
ADV-TDF
HBeAg- Patients HBeAg+ Patients
99.6% 98%
1. Marcellin P, et al. J Hepatol. 2014 Jul 18; DOI: 10.1016/j.jhep.2014.07.019 (ePub ahead of print).

Patients in Long-term Tenofovir Studies 102/103
‒ 348 had liver biopsies at baseline, 1 and 5 years
Marcellin P, et al. The Lancet 2013; 381(9865): 468-475.
Ishak Fibrosis
Scores
Pe
rce
nta
ge
of
pa
tie
nts
0
10
20
30
40
50
60
70
80
90
100
Baseline Year 1 Year 5
P < 0.001
P < 0.001
0
.
6
5
4
3
2
1
0
Benefits of Long-term Oral Antiviral Therapy:
Fibrosis Regression over 5 years
28% 7%
18%

PLASMA
TFV X Tenofovir
(TFV)
GUT
HEPATOCYTE
A new Oral Antiviral: Tenofovir Alafenamide (TAF) Novel Prodrug of Tenofovir
7
TFV-MP
TFV-DP
TFV TDF TFV Tenofovir
disoproxil fumarate
(TDF)
– Enhances delivery of active drug (TFV-DP) to hepatocytes1
– Lower dose reduces circulating TFV levels >90% 2,3
– Lower risk of extrahepatic toxicity
TFV
Tenofovir
alafenamide (TAF)
TAF

Tenofovir Alafenamide (TAF)
– Improved safety profile vs TDF in HIV patients4:
1. Babusis D, et al. Mol Pharmaceutics. 2013;10:459-66; 2. Markowitz M, et al. J Antimicrob Chemother. 2014;69:1362-9 ;
3. Agarwal K et al. J Hepatology 2015;62:533-40; 4. Sax P, et al. JAIDS 2014;67:52-8 8
Me
dia
n ∆
(Q
1,
Q3
) C
LC
r (m
L/m
in)
Time (Week)
Me
an
% ∆
in H
ip B
MD
TAF*
TDF*
Time (Week)
TAF*
TDF*
*p <0.001 *p=0.041
Loss of Bone Density Renal Dysfunction
3 6 9 1 2 1 5 1 8 2 1 2 4 2 7 3 0
-1 5
-1 2
-9
-6
-3
0
T A F 2 5 m g (n = 1 0 )
Me
an
Ch
an
ge
Fro
m
Ba
se
lin
e
CrC
L (
mL
/min
/1.7
3m
2)
T D F 3 0 0 m g (n = 1 0 )
S tu d y D a y
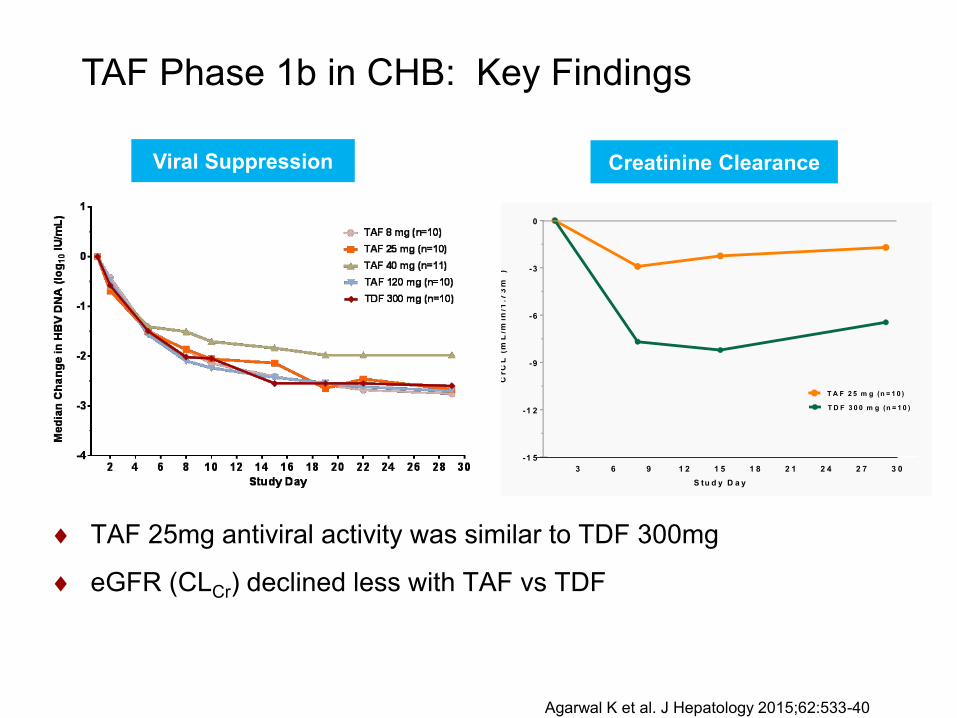
TAF Phase 1b in CHB: Key Findings
Creatinine Clearance Viral Suppression
TAF 25mg antiviral activity was similar to TDF 300mg
eGFR (CLCr) declined less with TAF vs TDF
Agarwal K et al. J Hepatology 2015;62:533-40

TAF HBV Phase IIII Study Design
Two phase 3, randomized, double-blind studies
Primary endpoint (non-inferiority margin of 10%)
– HBV DNA < 29 IU/mL at Week 48
Key secondary safety endpoints
– Bone mineral density at Week 48
– Renal parameters at Week 48
TAF 25mg
TDF 300mg
Open-label
2:1 TAF
25 mg
Study 108
HBeAg- (N=390)
Study 110
HBeAg+ (N=864)
Primary Endpoint
48 144 96 0 Week

1. High cost
2. Risk of viral rebound flares liver failure Non-adherence Emergence of resistance
3. Direct toxicity of oral antivirals Tenofovirbone disease, nephrotoxicity Entecavir risk of mutagenesis? Adefovir/Lamivudine risk of HCC
• A181T truncated S c-Raf-1/MAP kinase pathway
Disadvantages of Long-term Oral Antiviral Therapy
Yeh et al. BMC Cancer 2011, 11:398 -408
Hildt E, et al Recent Results Cancer Res 1998;154:315-29
Warner N, et al. Hepatology 2008; 48; 88-98
Confidential
Therapeutic Goal: Finite course of Therapy
Absence of HBV DNA and antigens
Cessation of all treatment
Finite treatment duration

13
TDF-Continue
TDF-Stop
Primary endpoint:
HBsAg loss by Wk 144
Wk 0 Wk 48 Wk 144
1:1
Ran
dom
iza
tion
CHB patients • HBeAg-negative
• ≥4 yrs TDF therapy
• noncirrhotic
Randomized N=45
TDF-Stop n=21
TDF-Continue n=21
Week 48 TDF-Restart
n=3
Week 48 TDF-Stop
n=18
Week 48 TDF-Continue
n=21
Withdrew consent n=3
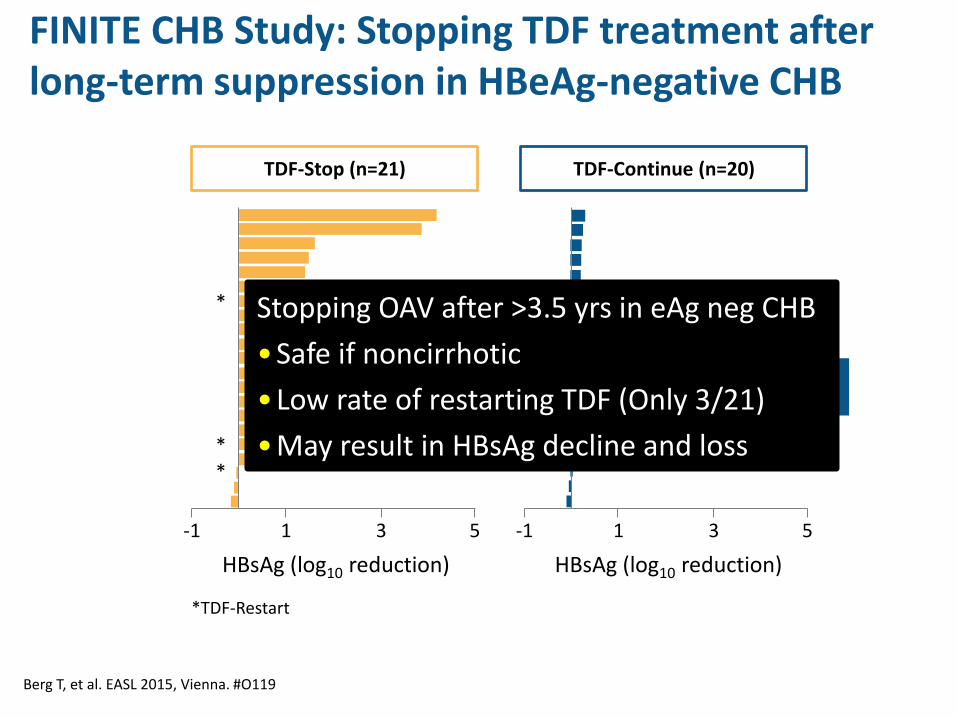
FINITE CHB Study: Stopping TDF treatment after
long-term suppression in HBeAg-negative CHB
Berg T, et al. EASL 205, Vienna. #O119

Berg T, et al. EASL 2015, Vienna. #O119
TDF-Stop (n=21)
Patients requiring TDF re-initiation (n=3) Time TDF was restarted
HB
V D
NA
(lo
g 10 IU
/mL)
Weeks from baseline
4
0
5
6
7
8
9
10
3
2
1
20 40 0 A
LT (
U/L
)
Weeks from baseline
200
0
300
400
500
1000
100
20 40 0
559 U/L 983 U/L
FINITE CHB Study: Stopping TDF treatment after long-term suppression in HBeAg-negative CHB
Berg T, et al. EASL 2015, Vienna. #O119
TDF-Stop (n=21) TDF-Continue (n=20)
1 3 5 -1
HBsAg (log10 reduction)
HBsAg reduction: mean 0.77log10
HBsAg loss in 2 pts (10%)
HBV DNA <2000 iu/mL in 14 (67%)
1 3 5 -1
HBsAg (log10 reduction)
* *
*
*TDF-Restart
FINITE CHB Study: Stopping TDF treatment after long-term suppression in HBeAg-negative CHB
HBsAg reduction: mean 0.11log10
HBsAg loss in no patients
Stopping OAV after >3.5 yrs in eAg neg CHB
•Safe if noncirrhotic
•Low rate of restarting TDF (Only 3/21)
•May result in HBsAg decline and loss

HBV CURE

New Targets for HBV “Cure”
Fabien Zoulim, and David Durantel Cold Spring Harb
Perspect Med 2015;5:a021501
cccDNA silencing Inhibit protein translation by siRNA • Arrowhead • Tekmira • Alnylam • GSK
Core inhibitors • Novira • Bayer • Assembly • Gilead • Janssen • Roche RT Pol Inhibitors
• Nucleotide analogues • Non-Nuc analogues • RNAseH inhibitrs
Entry Inhibitors
• Myrcludex
Immunodulators TLR agonists T-cell vaccines PD-1/PD-L1 blockade
HBsAg release Inhibitor • NAP

Fabien Zoulim, and David Durantel Cold Spring Harb
Perspect Med 2015;5:a021501
Core inhibitors • Novira • Bayer • Assembly • Gilead • Janssen • Roche
New Targets for HBV “Cure”

HBV Core Inhibitors Can Disrupt Multiple Steps Required for HBV Replication and Persistence
19

20
NVR 3-778 binds to HBV core & induces formation of abnormal capsids
NVR 3-778: Preclinical Profile
• NVR 3-778 induces rapid mis-assembly of HBV core
• NVR 3-778 is a potent inhibitor of HBV replication in standard HBV-producing call line HepG2.2.15: – EC50 = 0.24 μM, EC90 = 0.62 μM, similar to NUCs
• in vitro activity against HBV genotypes A, B, C and D
• Preclinical toxicology supports clinical testing:
– Negative genotoxicity assessments
– No organ toxicity in animal studies
• Oral administration
21

22
A; 50 mg
fasted dose
B; 150 mg
I
C; 400 mg
D; 800 mg
E; 14 day multidose
200 mg QD x 14 days
determined by SRC review of cohort A-D data
E2; optional 28 day multidose
Dose / frequency to be determined
SR
C
SR
C
SR
C
SR
C
SR
C
[SRC REVIEW ]
[SRC REVIEW]
[REVIEW after day 16]
[SRC REVIEW]
[SRC REVIEW]
Cohorts A-D: • Single doses after overnight fast, Day 1
• 7 days’ evaluations (inpatient days -1 to 4)
Food effect assessment with Cohort A • Subjects received a 2nd 50 mg dose with food
after washout
Cohort E multi-dose • 200 mg QD x 14 days
• Doses fasted
Healthy Volunteers • M or F, ages 18-65
• BMI 18-32 kg/m2
• 8 subjects/cohort
• Randomized 6:2, active:placebo
NOT DONE
NVR 3-778: Phase 1 MAD study in Healthy Subjects

23
Predictable dose-related exposure with little variability PK supports once daily oral dosing 200mg QD exceed inhibitory concentrations in HepG2 Doses 200 mg may afford continuous HBV inhibition
NO treatment-related AEs or Lab abnormalities
NVR 3-778: Phase 1 MAD study in Healthy Subjects

(i) Phase 1b MonoRx Dose-Ranging in HBeAg+ Patients (nuc-naïve)
F: 100 mg x 28 d
G: 200 mg x 28 d
I: >400 mg dose, or BD dosing
H: 400 mg x 28 d
Staggered initiation, Interim safety reviews at Week 2 for each cohort
NVR 3-778 Phase 1b Trial Design
24
Safety, PK, Preliminary Efficacy Initial NVR 3-778 3 monoRx dose cohorts Randomized 10:2 (active:placebo) 28 days treatment, with 28 days follow-up 4th monoRx cohort higher/lower dose
(ii) 28-day Phase 1b Combination Assessment(s)
pegIFN
NVR 3-778 + pegIFN
Randomize 24 pts 1:1
Nuc (TNF or ETV)
NVR 3-778 + Nuc
Randomize 24 pts 1:1
by protocol amendment
NVR 3-778 assessed at maximal effect dose, in combination regimens

Fabien Zoulim, and David Durantel Cold Spring Harb
Perspect Med 2015;5:a021501
Entry Inhibitors
• Myrcludex
HBsAg release Inhibitor • NAP
New Targets for HBV “Cure”

Entry Inhibitors in CHB
Urban et al. Gastroenterology 2014; 147: 48-64
• Myrcludex B is synthetic N-acylated preS1 lipopeptide which
blocks receptor functions of NTCP and virus entry
• Ongoing clinical studies in HBV and HDV infection

Nucleic Acid Polymers (NAPs) in CHB
• NAPs are oligonucleotides that interact with multiple intracellular amphipathic targets
• NAPs have multiple anti-HBV mechanisms – Block HBV entry – Post-entry activity
• Blocks subviral particle (SVP) formation – Restore host immune response
• NAPs may also have anti-delta effects – block HDV entry – Block HDV production from a SVP-related assembly
mechanism – “liberated” anti-HBs directly target HDV

Nucleic Acid Polymers (NAPs) (i) HBeAg+ CHB
10
8
6
4
4
6
8
10
LLD LLD
BL 12 20–24 IM f/u
HB
V D
NA
(lo
g cp
m)
HB
V R
NA
(log cp
m)
Responders (n=9)
Jansen L, et al. EASL 2015, Vienna. #O114
12 HBeAg+ pts in Moldova
Rep 2139-Ca IV 500mg weekly
Continued for 20-38 weeks
9 responded (fall in HBV DNA)
REP 2139-Ca
Entecavir
Add-on F/u
20–24 wks 13–26 wks 21 wks (range 7–27)
HBsAg non-responders (n=3)
HBsAg responders (n=9)
BL 12 20–24 IM add-on f/u
LLD
0
2
4
6 600
400
200
0
An
ti-HB
s
HB
sAg
(lo
g IU
/mL)
BL 12 20–24 IM f/u
REP 2139-Ca
At f/u, 4/9 patients had HBsAg <0.05 IU/mL and anti-HBs+
Long-term safety?
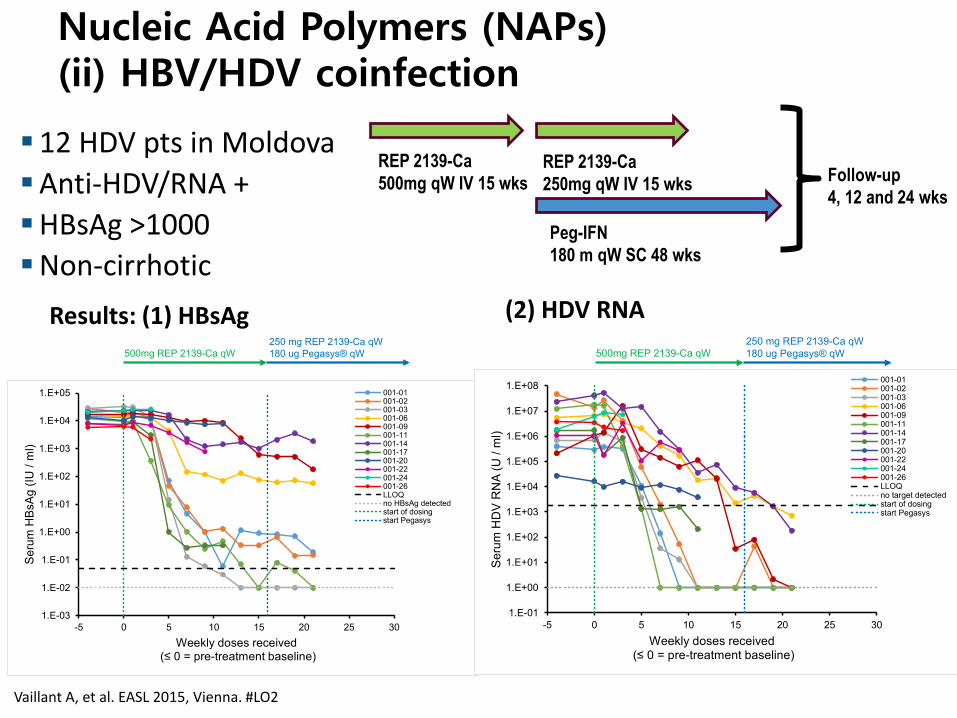
REP 2139-Ca
500mg qW IV 15 wks REP 2139-Ca
250mg qW IV 15 wks
Peg-IFN
180 m qW SC 48 wks
Follow-up
4, 12 and 24 wks
Nucleic Acid Polymers (NAPs) (ii) HBV/HDV coinfection
12 HDV pts in Moldova
Anti-HDV/RNA +
HBsAg >1000
Non-cirrhotic
500mg REP 2139-Ca qW
250 mg REP 2139-Ca qW
180 ug Pegasys® qW
1.E-03
1.E-02
1.E-01
1.E+00
1.E+01
1.E+02
1.E+03
1.E+04
1.E+05
-5 0 5 10 15 20 25 30
Se
rum
HB
sA
g (
IU /
ml)
Weekly doses received(≤ 0 = pre-treatment baseline)
001-01001-02001-03001-06001-09001-11001-14001-17001-20001-22001-24001-26LLOQno HBsAg detectedstart of dosingstart Pegasys
500mg REP 2139-Ca qW
250 mg REP 2139-Ca qW
180 ug Pegasys® qW
1.E-01
1.E+00
1.E+01
1.E+02
1.E+03
1.E+04
1.E+05
1.E+06
1.E+07
1.E+08
-5 0 5 10 15 20 25 30
Se
rum
HD
V R
NA
(U
/ m
l)
Weekly doses received(≤ 0 = pre-treatment baseline)
001-01001-02001-03001-06001-09001-11001-14001-17001-20001-22001-24001-26LLOQno target detectedstart of dosingstart Pegasys
Vaillant A, et al. EASL 2015, Vienna. #LO2
Results: (1) HBsAg (2) HDV RNA

Prenylation Inhibitors for HDV
*J. Glenn et al., J Virol. 1998 Nov;72(11):9303-6.
*J. Glenn et al., Science. 1992 May 29;256(5061):1331-3.
post-translational modification via inhibition of farnesyltransferase
(prenylation, site-specific lipid modification of proteins)
Preventing prenylation abolishes virus particle formation.
Review: Hughes, Wedemeyer, Harrison Lancet 2011

-3.5
-3
-2.5
-2
-1.5
-1
-0.5
0
0 5 10 15 20 25 30 35 40 45
LNF 100 mg BID + PEG IFN 180 mcg QW
LNF 100 mg BID + RTN 100 mg QD
HIDIT-2: PEG IFN ± tenofovir QD (N=91)
Me
an
VL C
ha
ng
e (
Lo
g IU
/mL
)
Week
(N=3)
(N=3)
Yurdaydin et al., O118 EASL 2015 Dahari et al., LP36 EASL 2015 Yurdaydin et al., O118 EASL 2015 Dahari et al., LP36 EASL 2015
15 HDV pts in Turkey treated with oral lonafarnib for 8 weeks
–200/300mg bid vs. 100mg bid +PEG vs. 100mg OD + ritonavir
Ritonavir boosting increased efficacy and reduced GI side-effects
Log decline HDV RNA
Prenylation Inhibitors in HDV coinfection Lonafarnib

Fabien Zoulim, and David Durantel Cold Spring Harb
Perspect Med 2015;5:a021501
New Targets for HBV “Cure” Immunodulators TLR agonists T-cell vaccines PD-1/PD-L1 blockade

Slide 33 Confidential
Strategies of Immune Modulation for CHB
Adaptive Immunity1-3
M X Large S (env) Core
GS-4774
1. Fisicaro P, et al. Gastroenterology 2012;143:1576-85; 2. Liu J, et. al. PLOS Pathogens 2014; 10; 1; 3. Martinet J, et
al. Gastroenterology 2012;143:1586-96; 4. Xu N, et al. Inflamm Res 2012;61:997-1004; 5. Vincent IE, et al.
PLoS One 2011;6:e26315.
HBV T-cell Vaccine

Day 1 8 15 29 85
GS-4774
(10 YU, 40 YU or 80 YU) Weekly
Immunology
Assessment
GS-4774
Administration
GS-4774
(10 YU, 40 YU or 80 YU) Monthly
57 36
GS-4774: Phase 1 Study in Healthy Volunteers
Lymphocyte Proliferation Assay (LPA)
• Immunogenicity to HBsAg, HBcAg and HBx
• Well tolerated with mild injection site reactions
Gaggar A, et al. Vaccine. 2014;32:4925-31
Slide 35 Confidential
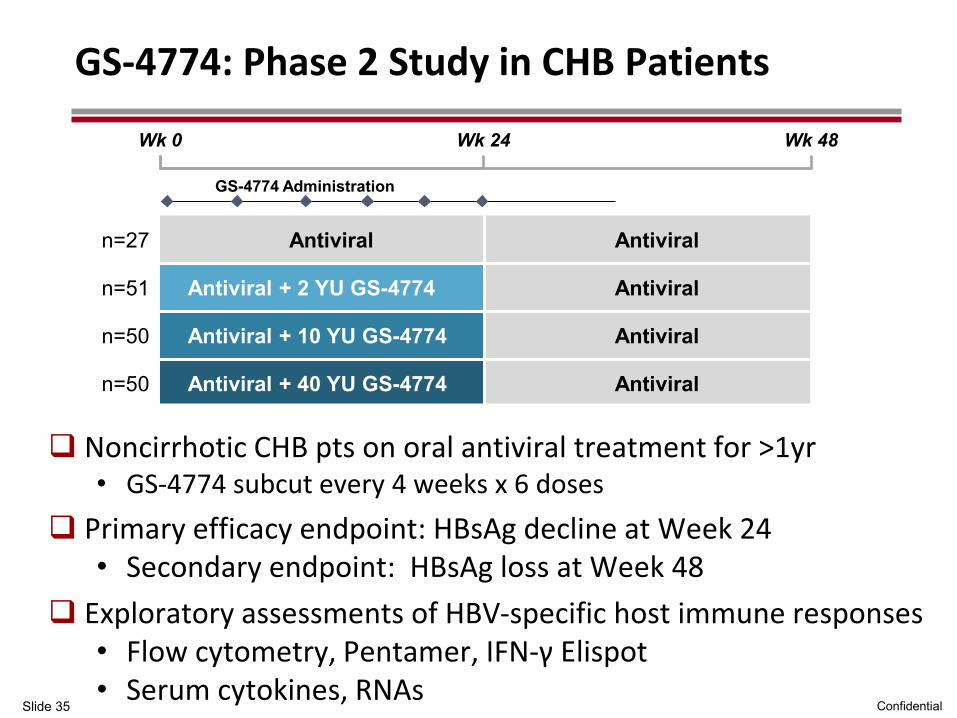
n=27 Antiviral Antiviral
n=51 Antiviral + 2 YU GS-4774 Antiviral
n=50 Antiviral + 10 YU GS-4774 Antiviral
n=50 Antiviral + 40 YU GS-4774 Antiviral
GS-4774: Phase 2 Study in CHB Patients
Noncirrhotic CHB pts on oral antiviral treatment for >1yr • GS-4774 subcut every 4 weeks x 6 doses
Primary efficacy endpoint: HBsAg decline at Week 24 • Secondary endpoint: HBsAg loss at Week 48
Exploratory assessments of HBV-specific host immune responses • Flow cytometry, Pentamer, IFN-γ Elispot • Serum cytokines, RNAs
Wk 0 Wk 24 Wk 48
GS-4774 Administration

Slide 36 Confidential
Strategies of Immune Modulation for CHB
Innate Immunity4,5
GS-9620
(Oral TLR-7 Agonist)
1. Fisicaro P, et al. Gastroenterology 2012;143:1576-85; 2. Liu J, et. al. PLOS Pathogens 2014; 10; 1; 3. Martinet J, et
al. Gastroenterology 2012;143:1586-96; 4. Xu N, et al. Inflamm Res 2012;61:997-1004; 5. Vincent IE, et al.
PLoS One 2011;6:e26315.
TLR-7/8 Agonist)

Toll-like Receptor 7 (TLR7) for HBV
NK IFN-
CD8+
APCs
IFN-α
Innate Immunity - Kill infected cells - Antiviral cytokines (e.g. IFN-γ)
Adaptive immunity - Kill infected cells - Antiviral cytokines (e.g. IFN-γ) - Neutralizing antibodies
Antiviral cytokines
Intrahepatic TLR7+ Cells
B cells
pDCs
B cell
IFN-α
IL-6
pDC, Plasmacytoid dendritic cell
APC, Antigen presenting cell.
IFN, interferon
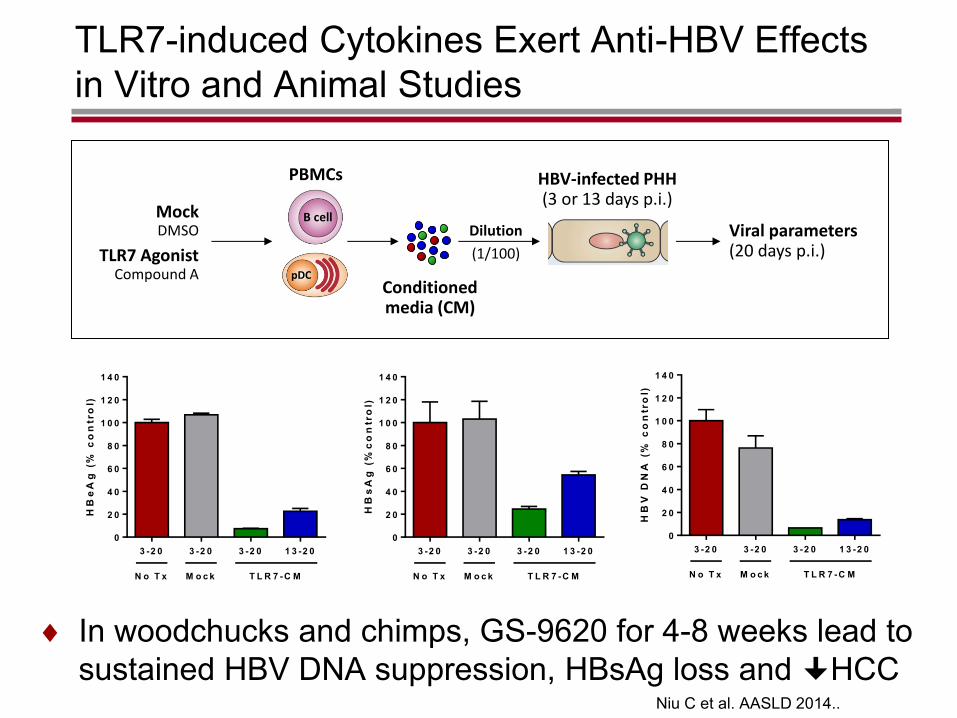
TLR7-induced Cytokines Exert Anti-HBV Effects
in Vitro and Animal Studies
Niu C et al. AASLD 2014..
Viral parameters (20 days p.i.)
HBV-infected PHH (3 or 13 days p.i.)
Dilution
(1/100) TLR7 Agonist Compound A
PBMCs
pDC
B cell Mock DMSO
Conditioned media (CM)
HB
eA
g (
% c
on
tro
l)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
HB
sA
g (
%c
on
tro
l)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
Nu
cle
i c
ou
nt
(% c
on
tro
l)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
D a y s (p .i.)
HB
V D
NA
(%
co
ntr
ol)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
HB
V R
NA
(%
co
ntr
ol)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
AK
ac
tiv
ity
(%
co
ntr
ol)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
D a y s (p .i.)
HB
eA
g (
% c
on
tro
l)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
HB
sA
g (
%c
on
tro
l)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
Nu
cle
i c
ou
nt
(% c
on
tro
l)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
D a y s (p .i.)
HB
V D
NA
(%
co
ntr
ol)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
HB
V R
NA
(%
co
ntr
ol)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
AK
ac
tiv
ity
(%
co
ntr
ol)
3 -2 0 3 -2 0 3 -2 0 1 3 -2 0
0
2 0
4 0
6 0
8 0
1 0 0
1 2 0
1 4 0
N o T x M o c k T L R 7 -C M
D a y s (p .i.)
In woodchucks and chimps, GS-9620 for 4-8 weeks lead to
sustained HBV DNA suppression, HBsAg loss and HCC

GS-9620 Phase 1 SAD/MAD study in CHB Patients
ISG15 (mRNA) Induction
(b) 2 Doses (Day 1 and 8)
Time (hr)
ISG
15 m
RN
A
mean
fo
ld c
han
ge
0 24 48 72 96 120 144 168 192 216 240 264 288 312 3360.25
0.5
1
2
4
8
16
32
64
128
Time (hr)
ISG
15 m
RN
A
mean
fo
ld c
han
ge
0 24 48 72 96 120 144 168 192 216 240 264 288 312 3360.25
0.5
1
2
4
8
16
32
64
128 Treatment-Naïve Patients Virally Suppressed Patients
GS-9620 dosing
T im e (h r )
ISG
15
me
an
fo
ld c
ha
ng
e g
en
e e
xp
re
ss
ion
0 2 4 4 8 7 2 9 6 1 2 0 1 4 4 1 6 8
0 .2 5
0 .5
1
2
4
8
1 6
3 2
6 4
1 2 8
T im e (h r )
ISG
15
me
an
fo
ld c
ha
ng
e g
en
e e
xp
res
sio
n
0 2 4 4 8 7 2 9 6 1 2 0 1 4 4 1 6 8
0 .2 5
0 .5
1
2
4
8
1 6
3 2
6 4
1 2 8Treatment-Naïve Patients Virally Suppressed Patients
(a) Single Dose
Gane EJ, et al. J Hepatol 2015 (in press)
Safety – Safe and well tolerated,
– No systemic IFN, no flares, no cytopenias
Phase II study: 150 pts with 4-12 weekly doses

HBV “Cure” is the aim!
Fabien Zoulim, and David Durantel Cold Spring Harb
Perspect Med 2015;5:a021501
cccDNA silencing

Can we eliminate cccDNA?
• cccDNA is the transcription template for all mRNAs, and is responsible for chronicity in an infected cell and rebound after OAV withdrawal.
• cccDNA is the reservoir which prevents cure
• cccDNA formation utilises the host cell’s own nuclear enzyme/DNA repair machinery
• Strategies which could eliminate cccDNA include
– cccDNA silencing by specific small molecules but against virus not host targets to avoid toxicity
– cccDNA depletion through increased hepatocyte turnover (but potential risk of hepatocarcinogenesis)
– cccDNA cleavage through by CRISPR-Cas9 nucleases

• Guide RNA sequences deliver Cas9 nuclease to conserved regions within HBV cccDNA, induce ds DNA breaks cccDNA, gene expression and DNA replication
ORF Targets
S 35
C 27
X 28
P 126
www.nature.com/scientificreports.DOI:1038/srep10833

• Has potential to eliminate persistent HBV infection but will need to target EVERY infected hepatocyte
• Need safe and effective in vivo drug delivery system (AAV vector) • Extensive genome-wide profiling to exclude off-target Cas-9 cutting
(but little homology between HBV and human DNA)
Rel
ativ
e cc
cDN
A
Rel
ativ
e H
BV
DN
A
www.nature.com/scientificreports.DOI:1038/srep10833

HBV CURE Conclusions
• Viral suppression with oral antiviral therapy can prevent disease progression and liver-related complications
• Current duration of OAV is lifelong with high cost and risk of breakthrough from non-adherence/resistance
• Future therapies will aim to induce HBsAg loss and enable discontinuation of long-term therapy
• Ultimate goal of CHB management will be to develop a new targeted therapy which can provide “HBV Cure” after a finite duration of treatment

HBV CURE: Conclusions
• HBV Cure programs stem from better understanding of HBV lifecycle and identification of new targets
• Several promising candidates already in preclinical and early clinical development
• Target patient population still undefined wrt phase of HBV infection, stage of disease, suppressed on OAV vs. treatment naïve vs. “immune tolerant”
• Safety will be the priority for these new therapies, in order to avoid severe hepatitis flares and other toxicity
• Convenient administration important (oral, subcut)
• HBV cure will ultimately require combinations which inactivate cccDNA and restore host immune responses

46
CD8+
T cell
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
HBV Virion
~10 ng/ml
HBV Sphere
~100 g/ml
HBV Filament
~1 g/ml
LHBsAg
HBsAg
MHBsAg
~1%
~90%
~10%
~5%
~85%
~10%
~10%
~80%
~10%
HIGH
COPY #
LOW
COPY #
B cell
Deplete or silence
cccDNA
Activate
antiviral
immunity
CONFIDENTIAL
HBV CURE: A Multi-Step Approach
NUCs Core inhibitors siRNAs

Special thanks to
Professor Stephen Locarnini, VIDRL
Dr W Ray Kim, Mayo Clinic
Dr Brian McMahon, Alaska
John Hornell, Chris Moyes, Helen Purcell, Hepatitis Foundation NZ