Chondrosarcoma of the petrous bone: a challenging clinical ...manuscript, we present a brief...
7
Page 1 of 7 Critical review Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY) Competing interests: none declared. Conflict of interests: none declared. All authors contributed to the conception, design, and preparation of the manuscript, as well as read and approved the final manuscript. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. For citation purposes: Maslehaty H, Petridis AK, Kinzel A, Binay Y, Scholz M. Chondrosarcoma of the petrous bone: a challenging clinical entity. Head Neck Oncol. 2013 Feb 06;5(2):13. Chondrosarcoma of the petrous bone: a challenging clinical entity H Maslehaty 1† , AK Petridis 1† , A Kinzel 1 , Y Binay 1 , M Scholz 1 * Abstract Skull base chondrosarcomas are challenging lesions to treat. In this manuscript, we present a brief over- view about this clinical entity. Further- more, we present an illustrated case with chondrosarcoma of the petrous bone and highlight microsurgical treat- ment options. Introduction Skull base tumours are challenging, and neurosurgeons and ENT specialists probably find these lesions the most difficult to treat. During the last decade, many novel techniques such as endoscopy have been introduced in our clinical armamentarium. This manuscript focuses on the chondro- sarcomas of the petrous bone and presents an illustrative case, giving a current overview of the natural his- tory, diagnosis and multimodal treat- ment strategies. Epidemiology Intracranial chondrosarcomas are most common skull base lesions, whereby extra-skeletal occurrence including falcine, parasagittal, parasellar and in the choroid plexus have also described 1–6 . These tumours arise usually de novo; however, an associa- tion with Maffucci syndrome, Olliers and Paget’s diseases have also been described in the literature 6–8 . The incidence of primary intracra- nial chondrosarcomas is estimated to be <0.16% of all intracranial tumours and 6% of all skull base lesions 3–5,7 . The origin of skeletal chondrosarco- mas is uncertain. Some authors postu- late derivation from undifferentiated cells from cartilaginous synchon- droses 9–11 . Extra-skeletal chondrosar- comas are believed to arise from pluripotent cells of the meninges, parenchyma and choroid plexus 3,6 . Histological subtypes Histologically, three subtypes are dif- ferentiated: classic, myxoid and mes- enchymal. Each subtype is associated with different incidence and prognosis. Microscopically, mesenchymal chon- drosarcomas appear with a densely cellular stroma of anaplastic cells with associated lacunas of neoplastic chon- drocytes and hyaline cartilage. Further characteristic findings of chondrosar- comas are collagen and cytoplasmic glycogen deposits. The mesenchymal subtype was found to be a more malignant type with a higher tendency for recurrence, metastasis and increased vascularity. The myxoid type is charac- terized by streaks of chondrocytes in a myxoid matrix and has an inter- mediate histological position. The classic type is well differentiated with minor mesenchymal tissue 3,5,6,9 . The mesenchymal type occurs more frequently in younger (20–30 years) and the classical subtype in elderly patients (60–70 years) 3,4,12 . However, chondrosarcomas can occur at any age. A literature review by Korten and co-workers revealed occurrence of these tumours in patients aged 3 months to 76 years 4 . Tumour grading is determined by the classification of the World Health Organization (WHO) into three grades. Grade I tumours are well differentiated and grade II tumours are moderately differentiated. Grade III lesions, how- ever, are poorly differentiated and are highly malignant. Chondrosarcomas tend to grow rapidly with consecutive compres- sion and dislocation of the surround- ing brain structures. Furthermore, these tumours are characterized by their infiltrative behaviour, which lead to progressive neurological complaints such as headache and impaired vision 8,12 . Neuroimaging Characteristic neuroimaging findings of cartilaginous tumours—more specifically chondrosarcomas—are calcifications in varying degrees. On computed tomography (CT) scans, these tumours appear as isodense to hyperdense lesions, with heterogene- ous enhancement 3 . Even if distinct calcification is missing within the tumour, T1-weighted images show low signal intensity, which can be construed as cartilage lacunas. The classic type chondrosarcoma is a slow growing tumour. According to this biological behaviour, these tumours appear as extra-axial lesions with good delimitation to the sur- rounding brain tissue with retained cerebrospinal fluid (CSF) margin, even in infiltrative tumours. This circumstance is best shown on T2-weighted magnetic resonance imaging (MRI) sequences, in that these tumours appear strongly hyper- intense. On the other hand, chondro- sarcomas appear hypointense on T1-weighted images. The affection of the bony structures such as “pres- sure erosion” is best shown on CT scanning 3,13 . Since chondrosarcomas are usually low or avascular tumours, application of contrast agents may lead to mild enhancement. Some authors describe the “honeycomb” pattern 3,14 . However, some tumours can present with a high vascularization pattern and may mimic vascular tumours * Corresponding author Email: [email protected] † These authors contributed equally to this study. 1 Department of Neurosurgery, Klinikum Duisburg, Academic Teaching Hospital of University Essen-Duisburg, Germany
Transcript of Chondrosarcoma of the petrous bone: a challenging clinical ...manuscript, we present a brief...

Page 1 of 7
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Maslehaty H, Petridis AK, Kinzel A, Binay Y, Scholz M. Chondrosarcoma of the petrous bone: a challenging clinical entity. Head Neck Oncol. 2013 Feb 06;5(2):13.
Chondrosarcoma of the petrous bone: a challenging clinical entityH Maslehaty1†, AK Petridis1†, A Kinzel1, Y Binay1, M Scholz1*
AbstractSkull base chondrosarcomas are challenging lesions to treat. In this manuscript, we present a brief over-view about this clinical entity. Further-more, we present an illustrated case with chondrosarcoma of the petrous bone and highlight microsurgical treat-ment options.
IntroductionSkull base tumours are challenging, and neurosurgeons and ENT specialists probably find these lesions the most difficult to treat. During the last decade, many novel techniques such as endoscopy have been introduced in our clinical armamentarium. This manuscript focuses on the chondro-sarcomas of the petrous bone and presents an illustrative case, giving a current overview of the natural his-tory, diagnosis and multimodal treat-ment strategies.
EpidemiologyIntracranial chondrosarcomas are most common skull base lesions, whereby extra-skeletal occurrence including falcine, parasagittal, parasellar and in the choroid plexus have also described1–6. These tumours arise usually de novo; however, an associa-tion with Maffucci syndrome, Olliers and Paget’s diseases have also been described in the literature6–8.
The incidence of primary intracra-nial chondrosarcomas is estimated to be <0.16% of all intracranial tumours and 6% of all skull base lesions3–5,7.
The origin of skeletal chondrosarco-mas is uncertain. Some authors postu-late derivation from undifferentiated cells from cartilaginous synchon-droses9–11. Extra-skeletal chondrosar-comas are believed to arise from pluripotent cells of the meninges, parenchyma and choroid plexus3,6.
Histological subtypesHistologically, three subtypes are dif-ferentiated: classic, myxoid and mes-enchymal. Each subtype is associated with different incidence and prognosis. Microscopically, mesenchymal chon-drosarcomas appear with a densely cellular stroma of anaplastic cells with associated lacunas of neoplastic chon-drocytes and hyaline cartilage. Further characteristic findings of chondrosar-comas are collagen and cytoplasmic glycogen deposits. The mesenchymal subtype was found to be a more malignant type with a higher tendency for recurrence, metastasis and increased vascularity. The myxoid type is charac-terized by streaks of chondrocytes in a myxoid matrix and has an inter-mediate histological position. The classic type is well differentiated with minor mesenchymal tissue3,5,6,9. The mesenchymal type occurs more frequently in younger (20–30 years) and the classical subtype in elderly patients (60–70 years)3,4,12. However, chondrosarcomas can occur at any age. A literature review by Korten and co-workers revealed occurrence of these tumours in patients aged 3 months to 76 years4.
Tumour grading is determined by the classification of the World Health Organization (WHO) into three grades. Grade I tumours are well differentiated and grade II tumours are moderately differentiated. Grade III lesions, how-ever, are poorly differentiated and are highly malignant.
Chondrosarcomas tend to grow rapidly with consecutive compres-sion and dislocation of the surround-ing brain structures. Furthermore, these tumours are characterized by their infiltrative behaviour, which lead to progressive neurological complaints such as headache and impaired vision8,12.
NeuroimagingCharacteristic neuroimaging findings of cartilaginous tumours—more specifically chondrosarcomas—are calcifications in varying degrees. On computed tomography (CT) scans, these tumours appear as isodense to hyperdense lesions, with heterogene-ous enhancement3. Even if distinct calcification is missing within the tumour, T1-weighted images show low signal intensity, which can be construed as cartilage lacunas.
The classic type chondrosarcoma is a slow growing tumour. According to this biological behaviour, these tumours appear as extra-axial lesions with good delimitation to the sur-rounding brain tissue with retained cerebrospinal fluid (CSF) margin, even in infiltrative tumours. This circumstance is best shown on T2-weighted magnetic resonance imaging (MRI) sequences, in that these tumours appear strongly hyper-intense. On the other hand, chondro-sarcomas appear hypointense on T1-weighted images. The affection of the bony structures such as “pres-sure erosion” is best shown on CT scanning3,13. Since chondrosarcomas are usually low or avascular tumours, application of contrast agents may lead to mild enhancement. Some authors describe the “honeycomb” pattern3,14. However, some tumours can present with a high vascularization pattern and may mimic vascular tumours
* Corresponding authorEmail: [email protected]† These authors contributed equally to this study.1 Department of Neurosurgery, Klinikum
Duisburg, Academic Teaching Hospital of University Essen-Duisburg, Germany
Page 2 of 7
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Maslehaty H, Petridis AK, Kinzel A, Binay Y, Scholz M. Chondrosarcoma of the petrous bone: a challenging clinical entity. Head Neck Oncol. 2013 Feb 06;5(2):13.
such as hemangiopericitomas3. Despite the typical neuroimaging findings of chondrosarcomas, meningiomas and metastases have to be differentiated.
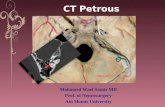
Illustrative caseA 26-years-old male patient presented with left sided abducens nerve palsy, atrophy of the left half of the tongue and progressive headaches since three months. On examination, the patient additionally presented uvula deviation to the left side and dysphagia without hearing impairments. Neuroimaging with cranial MRI and CT showed a tumour of the petrous apex, which extended to the posterior fossa right up to the foramen magnum (Figure 1).
After evaluation of the images, it was clear to us that the tumour had to be treated by combination of two approaches. The first surgical approach was retrosigmoid suboccipital to remove the tumour of the posterior fossa. The first reason for performing this surgery was the clinical symp-tomatology of the patient, i.e. double
vision related to the abducens nerve palsy. The second delayed approach was subtemporal extradural with the necessity of an additional petrous apicectomy to remove the tumour adjacent to the petrous bone to obtain gross tumour resection. Prior to sur-gery, a lumbar drainage was placed to reduce CSF and enable slight eleva-tion of the temporal lobe. During this surgical intervention, a navigation system with previously obtained CT data was used.
Figure 2 shows the cranial CT images after the retrosigmoidal and Figure 3 shows the post-operative CT after the subtemporal approach. The tumour is with exception of a small part in the petrous bone completely removed. In the post-operative course, the abdu-cens palsy declined completely.
Histologically, the tumour was diag-nosed as a chondrosarcoma grade II with extended osteodestructive growth and focally myxoid components. The proliferation index was less than 1% (Figure 4).
Since complete tumour resection was not possible, a heavy ion radia-tion therapy was performed post-operatively. The patient did not suffer any additional neurological deteriora-tion after treatment without proven tumour growth in the follow-up exam-inations (follow-up of 16 months).
Surgical approaches and anatomical structuresThere are different types of approaches to treat chondrosarcomas in the middle cranial fossa, depending on the extent of the tumours and neces-sity to protect cranial nerves, espe-cially the cochlear nerve. Therefore, the most suitable surgical strategy needs to be determined on a case-by-case basis, considering the neuroimaging findings carefully. To obtain the best surgical result, neurosurgeons have to be familiar with the anatomical structures of the skull base. Subse-quently, the most important anatomi-cal landmarks are recapitulated to make surgical understanding easier. The following descriptions are based on the findings of Wanibuchi, Friedman and Fukushima as well as on the illustrations of Sanna, Sekhar and Yaşargil16–19. The two main approaches to tumours of the petrous bone are subtemporal and retrosigmoidal. By application of each approach, different parts and angles of the area of interest are visible.
Retrosigmoidal approachThe overview of anatomical structures through a right-sided retrosigmoidal approach is displayed in Figure 5. From this point of view, looking over the cerebellum, the relationship between the trochlear nerve and superior cerebellar artery (SCA) as well as the relationship between the SCA and trigeminal nerve is visible. The fifth cranial nerve impresses as a really strong nerve close to the SCA. Next to the trigeminal nerve, the so-called acousticofacial bundle (AFB) can be identified, which contains the facial nerve, acoustic nerve, as well as the
Figure 1: Chondrosarcoma of the petrous apex and posterior fossa. (a) CT scan illustrates the posterior fossa part of the tumour (arrows). This tumour part can be removed by a retrosigmoidal approach. (b) Tumours that cannot be reached through the retrosigmoidal approach as they are present on the os petrosum are shown. This part can be approached through the subtemporal approach (arrows).

Page 3 of 7
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Maslehaty H, Petridis AK, Kinzel A, Binay Y, Scholz M. Chondrosarcoma of the petrous bone: a challenging clinical entity. Head Neck Oncol. 2013 Feb 06;5(2):13.
vestibular nerve. Behind the AFB, but still very close to it, the abducens nerve can be encountered. This nerve is accompanied a short way by the anterior inferior cerebellar artery (AICA). The AICA overlays the glos-sopharyngeal nerve at the lateral margin of this image section.
After angling the microscope inferi-orly, the lower cranial nerves become visible. Beginning at the glossopharyn-geal nerve, the vagus nerve can be demonstrated in the direct neighbour-hood. The vertebral artery is nestling between the hypoglossal nerve. On its
top, the verterbral artery gets in contact with the acessory nerve.
Subtemporal extradural approachThe subtemporal extradural approach, which is used in our illustrated case, is a widely used approach for extra-dural lesions. Preoperative lumbar CSF drainage provides better retrac-tion of the temporal lobe and better exposure of the anatomical structures. After temporal craniotomy, the dura is dissected from bone and middle meningeal artery (MMA), as the first anatomical landmark is visible. Further
dissection of the dura is done by following the MMA to the foramen spinosum. Rostral to the foramen spinosum, the foramen ovale appears with the third branch of the trigemi-nal nerve (V3, maxillary nerve). Caudal to the foramen ovale and spinosum, the petrous part of internal carotid artery (ICA) is visible, which is usually covered by a thin bone layer. The greater petrosal nerve (GPN) runs medially to the ICA, which can be followed to the arcuate eminence as another anatomical landmark, which indicates the internal auditory mea-tus. After dissection of all anatomical landmarks, the petrous apex is visi-ble and petrous apicectomy can be performed.
For drilling, the knowledge of the course of the petrous part of ICA and GPN is important. Mortini and co-workers defined the pentagonal post-trigeminal area, which is marked out by ganglion gasseri, ICA, cochlea, internal auditory canal and superior petrosal sinus. The authors termed the angle between the ganglion gasseri and superior petrosal sinus as the key point at which drilling should start to avoid damage to the surrounding anatomical structures20. The ana-tomical structures are displayed in Figure 6.
Subtemporal intradural approachThe subtemporal intradural approach provides a closer look to the struc-tures, which are not visible by the retrosigmoidal approach. Combina-tion of both approaches enables an overview of the adjacent structures of the petrous bone in intradural lesions. After retraction of the temporal lobe, anatomical structures are visible very clearly (Figure 7). The ICA and optic nerve, which passes behind the artery, can be easily identified. Branches of the ICA, in terms of the posterior commu-nicating artery, as well as the poste-rior cerebral artery, run horizontally and nearly parallel to the temporal lobe. The pituitary stalk is underlying the posterior communicating artery.
Figure 2: Tumour removal through a retrosigmoidal approach. (a) The tumour was partially removed by a retrosigmoidal approach. The posterior part of the petrosal bone was drilled to remove the tumour tissue (arrow), and the tumour was removed from the caudal cranial nerves, the abducens and cranial nerves VII/VIII. (b) The carotid artery can be visualized in its petrous part (arrow). (c) The sigmoid sinus entering the jugular foramen is shown with an arrow. ICA is shown in (b) and (c) in close proximity to the tumour. (d) In the bone window of the CCT part of the petrous bone is drilled (white arrow). (e) The subtemporal part of the tumour is still present as it is seen in this contrast-enhanced MRI of the brain. (f) In this MRI image, the limits of tumour removal are shown by white arrows. The green arrow indicates cranial nerves VII and VIII, the blue arrow shows the labyrinth and the red arrow shows the cochlea, which could be left intact during surgery. (g) MRI shows the remaining tumour, which was then removed with a subtemporal approach combined with a petrosal appicectomy (white arrows).

Page 4 of 7
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Maslehaty H, Petridis AK, Kinzel A, Binay Y, Scholz M. Chondrosarcoma of the petrous bone: a challenging clinical entity. Head Neck Oncol. 2013 Feb 06;5(2):13.
Close to the pituitary stalk, both optic nerves cross each other. The basilar artery can be identified above the ipsi-lateral oculomotor nerve. The arched branch is the superior cerebellar artery, which is running straight ahead to the trochlear nerve at the lateral margin of this image.
Endoscopic approachesSurgical resection should be the aim and can be achieved by microsurgical as well as endoscopic techniques. In the clivus, for example, endoscopic techniques have become more and more familiar in the resection of tumorous lesions in greater skull base centres, because they provide mini-mally invasive approaches to deep-seated lesions. Combination of classical microscopic and endoscopic techniques can increase of the quality and expan-sion of the field of application of surgical procedures21–27.
Adjuvant therapySince gross or total tumour resection of skull base chondrosarcomas is not possible in every case, adjuvant therapy models, in terms of post-operative irradiation, can enable tumour control. However, the efficacy of the presented treatment modalities is controversial.
Iyer and co-workers performed stereotactic radiosurgery (SRS) in 22 patients with skull base chondrosar-comas. The median dose was 15.0 Gy. Seven patients died at the 75 months follow-up as a result of tumour pro-gression. The authors postulated that patients >40 years without prior radio-therapy may benefit from early SRS after microsurgical tumour resection28.
Hauptman et al. reviewed the data of 13 patients with skull-based chordomas and chondrosarcomas, treated with linear accelerator ste-reotactic radiotherapy (SRT) or SRS. Under consideration of possible radi-ation-induced complications such as endocrinopathy, cranial neuropathy and visual impairments, the authors concluded that SRT or SRS are safe
Figure 3: Additional tumour removal after a subtemporal approach and petrosal apicectomy. (a) After the second surgery, the remaining tumour was removed by a subtemporal approach. The carotid artery was freed from tumour and a petrosal apicectomy was performed. (b) To reach the tumour tissue, labyrinth and cochlea still remained intact.
Figure 4: Histopathological images. (a) Staining for S100 protein with positive findings. (b) Haematoxylin and eosin staining. (c) Low reaction in Ki-67 staining. (d) Negative findings in cytoceratine-MNF 116 staining.

Page 5 of 7
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Maslehaty H, Petridis AK, Kinzel A, Binay Y, Scholz M. Chondrosarcoma of the petrous bone: a challenging clinical entity. Head Neck Oncol. 2013 Feb 06;5(2):13.
as an adjuvant therapy after surgical tumour resection29.
A systematic review of the literature concerning proton therapy after maximal surgical resection of skull base chondrosarcomas by Amichetti
and co-workers revealed a very high probability of medium- and long-term tumour control without the risk of sig-nificant complications30.
Tabarkiewitz and co-workers treated one patient with dendritic cell based
immunotherapy. Despite their encour-aging in vitro results on chondrosar-coma cells, this therapeutical approach remains experimental and needs further investigation31.
Förander and co-workers investi-gated the therapeutical efficacy of combination of microsurgery and Gamma Knife surgery for intracranial chondrosarcomas in nine patients. The authors concluded that local tumour control in combination of these two treatment modalities could be achieved in low-grade chondrosar-comas. On the other hand, tumour control was not satisfactory in the mesenchymal tumour type32.
Nonetheless, a review of 60 cases of intracranial chondrosarcomas by Gay and co-workers summarized that chondrosarcomas do not show a dose-response after radiotherapy. Adjuvant radiotherapy seems to increase the disease-free survival, but has no influ-ence on the total survival time. In con-trast, proton beam therapy seems to increase the survival, whereby the success of this treatment is highly dependent on the resection status of the tumours12.
PrognosisSince chondrosarcomas are malig-nant tumours with an aggressive infil-trative behaviour, the grade of surgical resection is the key for recurrence-free survival. Brackmann and Teufert analysed the long-term outcome of eight patients with skull-based chon-drosarcomas and concluded that gross total tumour resection should be achieved with adjuvant proton beam therapy to obtain the longest possible disease-free survival32.
Bloch and co-workers determined the prognosis of patients with chon-drosarcomas depending on different factors. The authors pointed out that the extent of tumour resection, the his-topathological pattern and the applica-tion of adjuvant radiotherapy are the most significant predictive factors. The overall 5-year mortality was estimated to be 11%, with an average survival
Figure 5: Right-sided retrosigmoidal approach; IV: trochlear nerve, SCA: superior cerebellar artery, V: trigeminal nerve, AFB: acousticofacial bundle, VI: abducens nerve, AICA: anterior inferior cerebellar artery, IX: glossopharyngeal nerve.
Figure 6: Right-sided subtemporal extradural approach; MMA: middle meningeal artery, ICA: internal carotid artery, IAM: Projection of internal auditory meatus, GPN: greater petrosal nerve, V3: maxillary nerve.

Page 6 of 7
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Maslehaty H, Petridis AK, Kinzel A, Binay Y, Scholz M. Chondrosarcoma of the petrous bone: a challenging clinical entity. Head Neck Oncol. 2013 Feb 06;5(2):13.
time of 53.7%8. Gay and co-workers determined the overall recurrence-free survival to be 80% at 3 years and 76% at 5 years. Patients with recur-rence had a lower survival rate of 51% at 2 years and 26% at 3 years. In agreement with other studies, the authors confirm that the histopatho-logical mesenchymal type is the most aggressive and is associated with low-est survival rates12.
References1. Arpino L, Capuano C, Gravina M, Franco A. Parasellar myxoid chondro-sarcoma: a rare variant of cranial chon-drosarcoma. J Neurosurg Sci. 2011 Dec; 55(4):387–9.2. Boccardo M, Bavaresco E, Sola S, Vitali A. Parafalcine chondrosarcoma: report of a case and review of the literature. J Neurosurg Sci. 2009 Sep;53(3):137–40. 3. Kothary N, Law M, Cha S, Zagzag D. Conventional and perfusion MR imaging of parafalcine chondrosarcoma. AJNR Am J Neuroradiol. 2003 Feb;24(2):245–8.4. Korten AG, ter Berg HJ, Spincemaille GH, van der Laan RT, Van de Wel AM. Intracranial chondrosarcoma: review of the literature and report of 15 cases. J Neurol Neurosurg Psychiatry. 1998;65:88–92.
5. Oruckaptan HH, Berker M, Soylemezoglu F, Ozcan OE. Parafalcine chondrosarcoma: an unusual localization for a classical vari-ant: case report and review of the literature. Surg Neurol. 2001 Mar;55(3):174–9.6. Park JH, Kim MJ, Kim CJ, Kim JH. Intracranial extraskeletal myxoid chon-drosarcoma: case report and literature review. J Korean Neurosurg Soc. 2012 Sep;52(3):246–9.7. Bloch OG, Jian BJ, Yang I, Han SJ, Aranda D, Ahn BJ, et al. Cranial chondrosarcoma and recurrence. Skull Base. 2010 May; 20(3):149–56.8. Bloch OG, Jian BJ, Yang I, Han SJ, Aranda D, Ahn BJ, et al. A systematic review of intracranial chondrosarcoma and survival. J Clin Neurosci. 2009 Dec; 16(12):1547–51.9. Hassounah M, Al-Mefty O, Akhtar M, Jinkins JR, Fox JL. Primary cranial and intracranial chondrosarcoma: a survey. Acta Neurochir (Wien). 1985;78(3-4):123–32.10. Rapidis AD, Archondakis G, Anteriotis D, Skouteris CA. Chondrosarcomas of the skull base: review of the literature and report of two cases. J Craniomaxillofac Surg. 1997;25:322–7.11. Scheithauer BW, Rubinstein LJ. Menin-geal mesenchymal chondrosarcoma: report of 8 cases with review of the literature. Cancer. 1978;42(6):2744–52.
12. Gay E, Sekhar LN, Rubinstein E, Wright DC, Sen C, Janecka IP, et al. Chordomas and chondrosarcomas of the cranial base: results and follow-up of 60 patients. Neurosurgery. 1995 May;36(5): 887–97.13. Chen Y, Wang X, Guo L, Li Y, Deng S, Liu Y, et al. Radiological features and pathology of extraskeletal mesenchymal chondrosarcoma. Clin Imaging. 2012 Jul–Aug;36(4):365–70.14. Lee YY, Van Tassel P, Raymond AK. Intracranial dural chondrosarcoma. AJNR Am J Neuroradiol. 1988 Nov–Dec;9(6): 1189–93.15. Koutourousiou M, Gardner PA, Tormenti MJ, Henry SL, Stefko ST, Kassam AB, et al. Endoscopic endonasal approach for resection of cranial base chordomas: outcomes and learning curve. Neurosurgery. 2012 Sep;71(3):614–24.16. Sanna M, Mancini F, Russo A, Taibah A, Falcioni M, Di Trapani G. Atlas of Acoustic Neurinoma Microsurgery. Stuttgart– New York: Georg Thieme Medical Publish-ers; 1998. p. 142–75.17. Sekhar LN, Janecka IP. Surgery of cranial base tumors. Philadelphia: Lippincott Williams & Wilkins; 1993. p. 124–9.18. Wanibuchi M, Friedman Allan H, Fukushima T. Photo-atlas of skull base dis-section. Stuttgart–New York; Georg Thieme Medical Publishers; 2009. p. 293–311.19. Yasargil MG, Smith RD, Young PH, Teddy PJ. Microneurosurgery in 4 Volumes. Stuttgart–New York; Georg Thieme Medical Publishers; 1984. p. 237.20. Mortini P, Mandelli C, Gerevini S, Giovanelli M. Exposure of the petrous segment of the internal carotid artery through the extradural subtemporal mid-dle cranial fossa approach: a systematic anatomical study. Skull Base. 2001 Aug; 11(3):177–87.21. Chatrath P, Nouraei SA, De Cordova J, Patel M, Saleh HA. Endonasal endo-scopic approach to the petrous apex: an image-guided quantitative anatomical study. Clin Otolaryngol. 2007 Aug;32(4): 255–60.22. de Notaris M, Cavallo LM, Prats- Galino A, Esposito I, Benet A, Poblete J, et al. Endoscopic endonasal transclival approach and retrosigmoid approach to the clival and petroclival regions. Neu-rosurgery. 2009 Dec;65(6 Suppl):42–50.23. Frank G, Sciarretta V, Calbucci F, Farneti G, Mazzatenta D, Pasquini E. The endoscopic transnasal transsphenoidal
Figure 7: Right-sided subtemporal intradural approach; ICA: internal carotid artery, Pcom: posterior communicating artery, NIII: oculomotor nerve, BA: basilar artery, PCA: posterior cerebral artery, Heubner: recurrent artery of Heubner, A1: A1-segment of right anterior cerebral artery, Acom: anterior communicating artery.

Page 7 of 7
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Maslehaty H, Petridis AK, Kinzel A, Binay Y, Scholz M. Chondrosarcoma of the petrous bone: a challenging clinical entity. Head Neck Oncol. 2013 Feb 06;5(2):13.
approach for the treatment of cranial base chordomas and chondrosarcomas. Neurosurgery. 2006 Jul;59(1 Suppl): ONS50–7.24. Gagliardi F, Boari N, Roberti F, Gragnaniello C, Biglioli F, Caputy AJ, et al. Extradural subtemporal transzygomatic approach to the clival and paraclival region with endoscopic assist. J Craniofac Surg. 2012 Sep;23(5):1468–75.25. Prabhu K, Kurien M, Chacko AG. Endoscopic transsphenoidal approach to petrous apex cholesterol granulomas. Br J Neurosurg. 2010 Dec;24(6):688–91.26. Zanation AM, Snyderman CH, Carrau RL, Gardner PA, Prevedello DM, Kassam AB. Endoscopic endonasal surgery for petrous
apex lesions. Laryngoscope. 2009 Jan; 119(1):19–25.27. Iyer A, Kano H, Kondziolka D, Liu X, Niranjan A, Flickinger JC, et al. Stereotactic radiosurgery for intracranial chondrosar-coma. J Neurooncol. 2012 Jul;108(3): 535–42.28. Hauptman JS, Barkhoudarian G, Safaee M, Gorgulho A, Tenn S, Agazaryan N, et al. Challenges in linear accelerator radiother-apy for chordomas and chondrosarcomas of the skull base: focus on complications. Int J Radiat Oncol Biol Phys. 2012 Jun; 83(2):542–51.29. Amichetti M, Amelio D, Cianchetti M, Enrici RM, Minniti G. A systematic review of proton therapy in the treatment of
chondrosarcoma of the skull base. Neuro-surg Rev. 2010 Apr;33(2):155–65. Review.30. Tabarkiewicz J, Radej S, Hus I, Wasiak M, Wdowiak P, Giannopoulos K, et al. Den-dritic cells based immunotherapy of patient with chondrosarcoma–case report. Folia Histochem Cytobiol. 2008;46(2):165–70.31. Förander P, Rähn T, Kihlström L, Ulfarsson E, Mathiesen T. Combination of microsurgery and Gamma Knife surgery for the treatment of intracranial chondrosar-comas. J Neurosurg. 2006 Dec;105 Suppl: 18–25.32. Brackmann DE, Teufert KB. Chondro-sarcoma of the skull base: long-term follow-up. Otol Neurotol. 2006 Oct;27(7): 981–91.


![Chondrosarcoma of the Foot: A Rare Occurrence in the ... · chondrosarcoma, and mesenchymal chondrosarcoma [2]. Chondrosarcomas are most frequently found in men between the ages of](https://static.fdocuments.us/doc/165x107/5f3b1db0e636c85ef24c91bb/chondrosarcoma-of-the-foot-a-rare-occurrence-in-the-chondrosarcoma-and-mesenchymal.jpg)